")
Back to Journals » Risk Management and Healthcare Policy » Volume 17
Health Technology Assessment: Evaluation of 7 Glucagon-Like Peptide-1 Receptor Agonists for the Treatment of Type 2 Diabetes Mellitus
Authors Xie Z , Hu J, Li M, Hu X , Chen J
Received 20 December 2023
Accepted for publication 17 April 2024
Published 23 April 2024 Volume 2024:17 Pages 1053—1067
DOI https://doi.org/10.2147/RMHP.S455897
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Zeyu Xie, Jia Hu, Mengting Li, Xiao Hu, Jisheng Chen
Key Specialty of Clinical Pharmacy, The First Affiliated Hospital of Guangdong Pharmaceutical University, Guangzhou, People’s Republic of China
Correspondence: Jisheng Chen, Key Specialty of Clinical Pharmacy, The First Affiliated Hospital of Guangdong Pharmaceutical University, Guangzhou, 510080, People’s Republic of China, Tel +86 20-87622305, Fax +86 20-61321967, Email [email protected]
Purpose: This study provides a reference for healthcare organizations in the selection and rational use of glucagon-like peptide-1 receptor agonists (GLP-1RAs), based on the Rapid Guide for Drug Evaluation and Selection in Chinese Medical Institutions (Second Edition).
Methods: According to the Rapid Guide for Drug Evaluation and Selection in Chinese Medical Institutions (Second Edition) released in 2023, relevant databases such as PubMed, Cochrane, and Embase, drug labels, and clinical guidelines were searched for drug information. We systematically evaluated 7 GLP-1RAs marketed in China for safety, efficacy, economy, pharmacological properties, and other attributes using a percentage scoring method.
Results: The final assessment result scores from highest to lowest were semaglutide (71.5 points), dulaglutide (68.9 points), liraglutide (68.7 points), exenatide (62.5 points), lixisenatide (59.9 points), polyethylene glycol loxenatide (55.9 points), and benaglutide (45.1 points).
Conclusion: When a healthcare organization introduces GLP-1RAs to their hospital, they can refer to the assessment results and use the top three recommended medications: semaglutide, dulaglutide, and liraglutide.
Keywords: glucagon-like peptide-1 receptor agonist, health technology assessment, type 2 diabetes mellitus, drug evaluation
Introduction
Hospital-based health technology assessment (HB-HTA) refers to the comprehensive and systematic evaluation of relevant health technologies based on the actual needs of hospitals, using the principles and methods of evidence-based medicine and health technology assessment to make rapid decisions about the selection, acquisition, and use of new technologies to improve health equity and is a commonly used policy analysis tool internationally.1,2
The incidence of diabetes is increasing due to changes in diet and lifestyle. Type 2 diabetes mellitus (T2DM) accounts for approximately 98% of diabetes diagnoses globally, although the exact proportion varies greatly from country to country.3 It is estimated that 530 million adults worldwide have diabetes, with a global prevalence of 10.5% among adults aged 20–79 years.4,5 The prevalence of diabetes among adults aged 20–79 years in China increased by 71.1%, from 4.7% in 1990 to 8.0% in 2019. Furthermore, the prevalence of diabetes among adults aged 20–79 in China is projected to increase from 8.2% to 9.7% in 2020–2030 compared with 2019. These statistics highlight the severity of the T2DM epidemic in China.
According to a 2016 report, over 1.9 billion adults aged 18 or older were overweight worldwide, with more than 650 million being obese. The report also found that 39% of adults aged 18 or older were overweight and 13% were obese.6 Overweight and obesity are significant risk factors for developing T2DM.7 Patients with T2DM are frequently overweight or obese, and obesity exacerbates the risk of cardiovascular disease in these patients. Weight reduction can help delay the progression of prediabetes to T2DM. Furthermore, Diabetes is a risk factor for cardiovascular disease, which is the leading cause of death in patients with diabetes.8 Patients with diabetes have a 2–4 times higher risk of cardiovascular disease compared to those without diabetes.9 Most patients diagnosed with T2DM are between 50 and 60 years old and are at a high risk for atherosclerotic cardiovascular disease (ASCVD) if they are aged 40 or older.
GLP-1RAs is currently widely used in clinical practice due to its significant benefits. It has been shown to reduce body weight, reduce the risk of ASCVD, and improve atherosclerosis and lipids, in addition to its significant glucose-lowering effects. The 2023 American Diabetes Association guidelines recommend GLP-1RAs or sodium-glucose cotransporter-2 inhibitors (SGLT-2i) with cardiovascular benefits as one of the indispensable medications for the treatment of T2DM, along with significant weight loss, in addition to metformin therapy.10 There are several drugs available for treating T2DM, including 7 GLP-1RAs injections that have been marketed in China to date. Additionally, an oral form of GLP-1RAs, as well as a GIP and GLP-1 dual agonist (tirzepatide), will also be marketed in China. This may pose challenges for healthcare organizations screening GLP-1RAs for introduction into their hospitals, particularly for those without the capacity to conduct drug evaluations independently. Therefore, given the wide range of GLP-1RAs currently available on the market, scientific evaluation and drug selection can ensure that healthcare organizations introduce advantageous drugs in a timely manner. This is conducive to guaranteeing that patients receive safe, effective, economical, and appropriate drug therapy. The objective of this study was to assess 7 GLP-1RAs that marketed in China based on the “2023 Rapid Guidelines for Drug Evaluation and Selection in Chinese Healthcare Organizations (Second Edition)”,11 so as to provide a reference for healthcare organizations in introducing and rationalizing the use of GLP-1RAs.
Methods
Evaluation Basis
Based on the “Rapid Guidelines for Drug Evaluation and Selection in Chinese Medical Institutions (Second Edition)” published in 2023,11 and applying a percentage assessment model to evaluate 7 GLP-1RAs. In terms of pharmacological properties, the main evaluation of the drug’s pharmacological effects, in vivo processes, whether the pharmacology and methods of use are clear, the length of the drug’s expiration date and storage requirements. In terms of drug effectiveness, the main evaluation is the clinical effectiveness of the drug, the recommendation level of relevant authoritative professional information such as clinical guidelines or expert consensus. Regarding safety, the evaluation mainly focuses on adverse events, drug use in special populations, and drug interactions. In terms of economics, the drug’s average daily therapeutic cost is being evaluated. Information on the availability of drugs is evaluated.
Data Source
Drug labels, drug registration information, some government websites (eg, American Food and Drug Administration (FDA), National Medical Products Administration (NMPA) provide safety information. English databases PubMed, Embase, and Cochrane Library, as well as Chinese databases Chinese Biomedical Sciences (CBM) and China National Knowledge Infrastructure (CNKI), were searched for systematic evaluations, meta-analyses, and real-world studies on the safety and efficacy of GLP-1RAs in treating T2DM. High-quality guidelines for the treatment of type 2 diabetes issued by an authoritative organization within 5 years (eg, American Diabetes Association). Search terms: semaglutide, liraglutide, PEX 168, exenatide, lixisenatide, dulaglutide, benaglutide, glucagon-like peptide-1 receptor agonist.
Evaluated Drug and Contents
The 7 GLP-1RAs marketed in China are exenatide injection, liraglutide injection, lixisenatide injection, benaglutide injection, dulaglutide injection, polyethylene glycol (PEG) loxenatide injection, and semaglutide injection. The evaluation of the 7 GLP-1RAs included an assessment of their pharmacologic properties (28%), efficacy (27%), safety (25%), economy (10%), and other attributes (10%). Table 1 displays the basic information on the 7 GLP-1RAs marketed in China.
 |
Table 1 The 7 GLP-1RA Basic Information |
Analysis and Evaluation
Drugs included in the evaluation were assigned a score according to the drug evaluation guidelines based on evidence collected by searching relevant databases.11 If no scoring breakdown rules exist, experts in the field are invited to refine them. The evaluation was conducted by two clinical pharmacists independently. In case of conflicting results, experts in the relevant fields were invited to discuss the evaluation results. The evaluation results will eventually be used to select medicines for medical institutions and make decisions about clinical medication programs.
Results
Pharmacological Properties (28%)
Pharmacological Effects and in vivo Processes
7 GLP-1RAs with obvious clinical efficacy, clear and innovative mechanism of action, all scoring 5 points; at the same time, the in vivo process, pharmacokinetic parameters are complete, scoring 5 points.
Pharmacy and the Use of Drugs
The ingredients and excipients of the 7 GLP-1RAs are clearly defined; the dosage forms are all subcutaneous/intramuscular injections, and to avoid serious gastrointestinal adverse events, it is necessary to start with a low dosage and gradually increase the dosage during use. In terms of specifications and packaging, all 7 GLP-1RAs are compatible with clinical use and dosage can be adjusted. In terms of administration frequency, exenatide was given twice daily, benaglutide three times daily, liraglutide and lixisenatide once daily, and dulaglutide, PEG loxenatide, and semaglutide once weekly. In addition, in terms of ease of use, all patients treated with GLP-1RAs need to be trained by a healthcare provider.
Drug Storage Conditions and Expiration Dates
All 7 GLP-1RAs must be refrigerated for storage. Exenatide, lixisenatide, and semaglutide have an expiration date of 36 months, while liraglutide has an expiration date of 30 months. PEG loxenatide, benaglutide, and dulaglutide have an expiration date of 24 months. Table 2 displays the results of the pharmacologic properties evaluations for the 7 GLP-1RAs.
 |
Table 2 Pharmacological Properties Score Results |
Efficacy (27%)
Indications
The approved indications for all 7 GLP-1RAs in China are for glycemic control in adult patients with T2DM. Based on the Chinese Lipid Management Guidelines 2023,12 patients who are diagnosed with T2DM and are aged 40 years or older can be considered a high-risk group for ASCVD. Liraglutide, dulaglutide, and semaglutide have been shown to reduce the risk of major cardiovascular in adult patients with T2DM and are clinically indicated/sub selected, scoring 3 points. Exenatide, lixisenatide, benaglutide, and PEG loxenatide scored 1 point for having a neutral profile of major cardiovascular benefit or for having no studies, and being the clinically More drugs available.
Guideline Recommendations
Guidelines and expert consensus on the clinical use of GLP-1RAs suggest that GLP-1RAs reduce cardiovascular risk in T2DM (eg, 2020 Chinese Guidelines for the Prevention and Control of Type 2 Diabetes Mellitus, 2022 Chinese Clinical Guidelines for the Prevention and Control of Type 2 Diabetes Mellitus in the Elderly, and 2023 American Diabetes Association Standards for the Medical Diagnosis and Treatment of Diabetes Mellitus). The recommendations of the guidelines and expert consensus are shown in Table 3.
Table 3 recommends liraglutide, dulaglutide, and semaglutide for the treatment of T2DM combined with CVD, with a grade of recommendation of I A and a score of 12. Exenatide and lixisenatide are mentioned as neutral for CVD in guidelines and expert consensus, with neutral results from the cardiovascular outcomes (CVOT) study. In the 2019 ESC/EASD Guidelines, lixisenatide and exenatide are mentioned as neutral in terms of their effect on the risk of hospitalization for HF and may be considered for the treatment of T2DM combined with HF, with a grade of recommendation of IIb. Benaglutide and PEG loxenatide are no guideline or expert consensus recommendations and lack of data from the CVOT study, both scored 6 points.
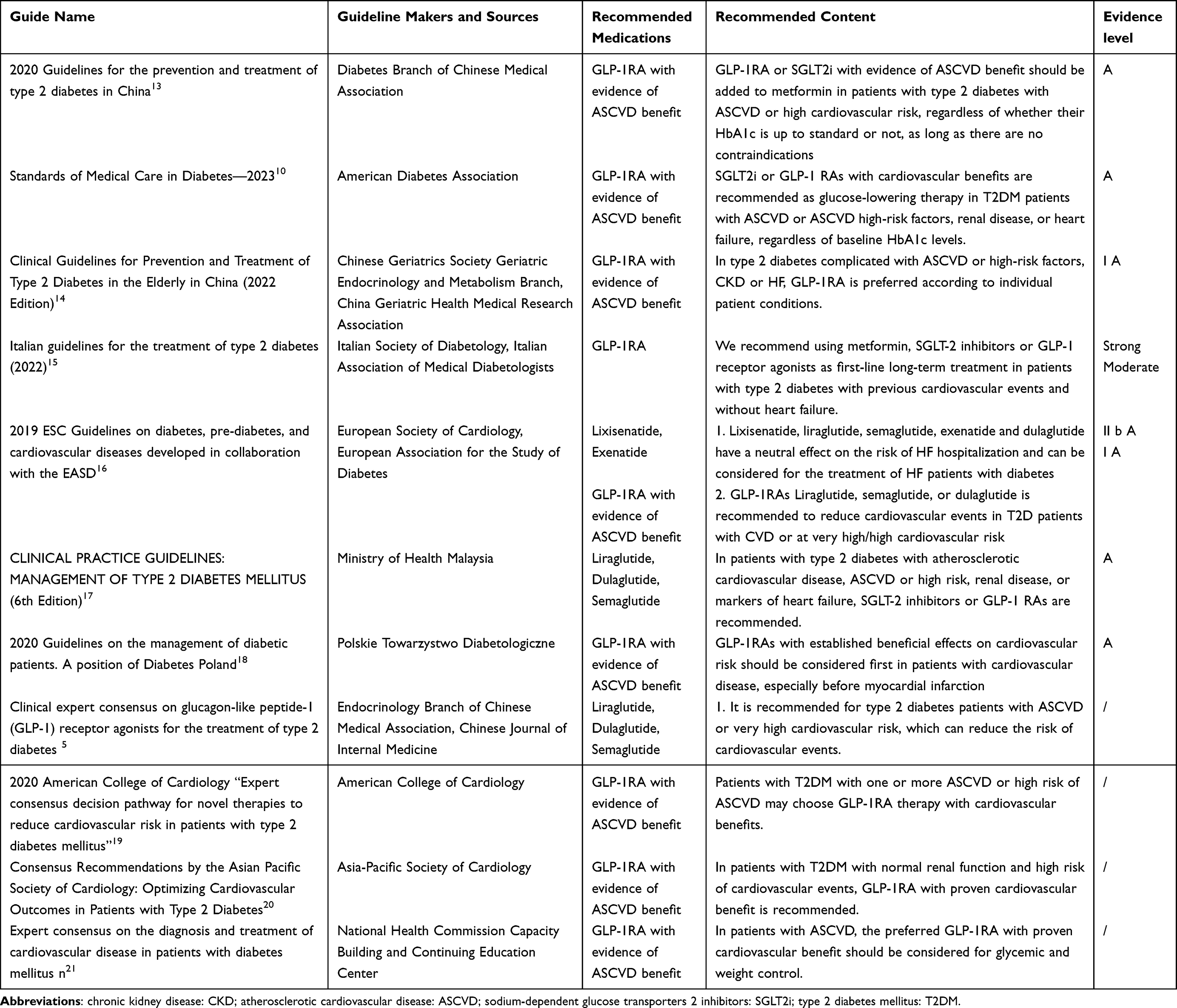 |
Table 3 Recommendations in Domestic and Foreign Guides and Consensus |
Clinical Efficacy
The primary endpoint efficacy indicator was HbA1c (6 points). Secondary efficacy endpoints included weight loss (2 points) and risk of cardiovascular benefit (2 points). The class of drugs’ highest indicator of improved efficacy is considered to have a perfect score.
The results of the basic information on HbA1c reduction, weight loss, and cardiovascular benefits of the 7 GLP-1RAs are shown in Table 4. The study was conducted by searching PubMed and Cochrane Library Medical Database. The meta-analysis study by Tsapas, Apostolos et al22 evaluated the HbA1c lowering effects of different glucose-lowering agents, including 5 GLP-1RAs, through 453 trials that assessed nine antidiabetic interventions from 21 drug classes. Shi-Shen et al23 conducted a meta-analysis of polyethylene glycol loxenatide, which included the percentage of HbA1c reduction and weight loss. Xia, Lin et al24 also conducted a meta-analysis, which included 36 RCTs with a total of 11,126 patients comparing the effect of 8 GLP-1RAs on weight loss in patients with T2DM. Additionally, the drug label did not provide any study data on weight loss for benaglutide. Similarly, there was no significant difference in weight loss between PEG loxenatide and placebo. Furthermore, there were no study data available on CVOT for either benaglutide or PEG loxenatide.
 |
Table 4 The Results of HbA1c Reduction, Weight Loss, and Cardiovascular Benefits of the 7 GLP-1 RAs |
The results of HbA1c reduction, weight loss, and cardiovascular benefits of the 7 GLP-1 RAs are shown in Table 4, it can be seen that semaglutide reduced HbA1c the most (−1.33%) among 7 GLP-1 RAs, scoring 6 points. Dulaglutide, PEG loxenatide, and liraglutide lowered HbA1C in essentially similar and all scored 4 points. In the term of weight loss and cardiovascular benefit, semaglutide also had a significant weight reduction advantage (−4.27 kg) and a cardiovascular benefit, scoring 4 points.
Overall, on the primary outcome endpoint (HbA1c), exenatide, liraglutide, lixisenatide, benaglutide, dulaglutide, PEG loxenatide, and semaglutide scored 3, 4, 2, 1, 4, 4, and 6, respectively. At the secondary outcome endpoint (weight loss + cardiovascular benefit), the scores for exenatide, liraglutide, lixisenatide, benaglutide, dulaglutide, PEG loxenatide, and semaglutide were 2, 3, 1.5, 0, 2.5, 0, and 4, respectively. The efficacy scores result of the 7 GLP-1RAs are shown in Table 5.
 |
Table 5 Efficacy Score Results |
Safety
Adverse Events
The most common adverse events of the 7 GLP-1RAs were gastrointestinal reactions, which were mild to moderate, with an incidence of >10%, all of which were scored as 1 point. Mild to moderate adverse events (eg, hypoglycemia, gastrointestinal, injection site reactions, etc.) were noted for both benaglutide and PEG Loxenatide. In addition, the incidence of serious adverse events ranged from 0.01% to <0.1%, scoring 4 points. The incidence of serious adverse events (eg, necrotizing or hemorrhagic pancreatitis, acute kidney damage and renal failure, anaphylactic reactions, and hypoglycemic aspects) for exenatide, liraglutide, and dulaglutide ranged from 0.01% to <0.1%, scoring 4 points. The incidence of serious adverse events (eg, severe hypoglycemia, severe allergic reactions, and acute pancreatitis) was between 0.1% and <1% for both lixisenatide and semaglutide, scoring 3 points.
Special Populations
Liraglutide has been approved by the FDA for the treatment of patients with T2DM over the age of 10 years, scoring 0.7. None of the other GLP-1RAs are recommended for use in the pediatric population. None of the 7 GLP-1RAs are recommended in pregnant and breastfeeding populations. In the elderly population, all 7 GLP-1RAs were available, scoring 1 point. In terms of renal dysfunction, exenatide, benaglutide, and PEG loxenatide had no relevant research data, scoring 0 points. Lixisenatide and dulaglutide could be used, scoring 3 points. Liraglutide and semaglutide could be used for mild to moderate renal dysfunction, scoring 2 points. In terms of liver function abnormalities, exenatide, lixisenatide, PEG loxenatide, and semaglutide can be used in mild to moderate, scoring 2 points; liraglutide and dulaglutide can be used in mild, moderate, and severe, scoring 3 points; and benaglutide is not recommended for patients with liver function abnormalities, scoring 0 points.
Drug Interactions
All 7 GLP-1RAs delay gastric emptying, affecting the rate of absorption of drugs absorbed via the gastrointestinal tract, and caution should be exercised in combining with other oral medications to avoid affecting their onset of action, scoring 1 point;
Other
Special dosing warnings were present for all 7 GLP-1RAs, all scoring 0 point. The adverse events that occurred with the 7 GLP-1RAs were largely reversible, scoring 0.5 point. In terms of teratogenicity and carcinogenicity, according to the drug labels, liraglutide, dulaglutide, lixisenatide, and semaglutide are teratogenic and carcinogenic, scoring 0 points; benaglutide is not teratogenic but lacks data from carcinogenicity studies, scoring 0.5 points; PEG loxenatide is not teratogenic but is carcinogenic, scoring 0.5 points; exenatide is not teratogenic or carcinogenic, scoring 1 point. The safety scores result of the 7 GLP-1RAs are shown in Table 6.
 |
Table 6 Safety Score Results |
Economy
All 7 GLP-1RAs were nationally negotiated drugs, and the prices of the target drugs were finally obtained by referring to the latest negotiated drug prices of the National Health Insurance (2024). The basic economy Information of 7 GLP-1RAs are shown in Table 7. The economy score results are shown in Table 8.
 |
Table 7 The Basic Economy Information of 7 GLP-1RA |
 |
Table 8 Economy Score Results |
Other Attributes
National Health Insurance and National Essential Drug Characteristics
All 7 GLP-1RAs are in Class B of the National Health Insurance and all have payment restrictions. Liraglutide is included in the National Essential Drug Catalog and has no Δ requirement, and the other 6 GLP-1RAs are not included in the National Essential Drug Catalog.
National Centralized Drug Procurement and Original Research Drugs
All 7 GLP-1RAs are originator drugs, all scored 1 point. In addition, none of the GLP-1RAs are national centralized drug procurement drugs, scoring 0 points.
Market and Business Characteristics
The other 5 GLP-1RAs are available in the United States, Europe, and Japan, except for benaglutide and PEG loxenatide, which are currently available only in China. The manufacturers of exenatide, liraglutide, lixisenatide, dulaglutide, and semaglutide are among the top 50 pharmaceutical companies in terms of global sales and are ranked 9th, 15th, 8th, 13th, and 15th, respectively (2022 rankings). PEG loxenatide is ranked 31st in the list of the top 100 pharmaceutical industry of the Ministry of Industry and Information Technology of China. Benaglutide is not in the list of the top 100 pharmaceutical industry in China and World’s top 50 pharmaceutical companies. The other attributes score results are shown in Table 9.
 |
Table 9 Other Attributes Score Results |
Final Scoring Results for the Five Dimensions of the 7 GLP-1RAs
Table 10 displays the final scores for the 7 GLP-1RAs evaluated. The top three GLP-1RAs were obtained by semaglutide, dulaglutide and liraglutide. Meanwhile, they were significantly better than other GLP-1RAs in terms of efficacy.
 |
Table 10 Final Score Results for the 7 GLP-1RAs |
Discussions
The results of this study showed that the 7 GLP-1RAs were ranked from highest to lowest as semaglutide, dulaglutide, liraglutide, exenatide, lixisenatide, PEG loxenatide, and benalutide. The top 3 rankings of semaglutide (71.5 points), dulaglutide (68.9 points), and liraglutide (68.7 points) were used as preferred drugs.
In addition to being effective and safe, GLP-1RAs provide weight loss and cardiovascular benefits.25 In terms of weight loss, the FDA has approved the use of semaglutide 2.4 mg and liraglutide 3.0 mg for weight management in patients with overweight or obesity. Studies have shown26 that weight loss of up to 12.47 kg and 5.24 kg, respectively, can be achieved after more than 20 weeks of treatment with semaglutide 2.4 mg and liraglutide 3.0 mg. In addition, tirzepatide 15 mg showed greater reductions in glycated hemoglobin and body weight compared with semaglutide. All current hypoglycemic agents with cardiovascular benefit are liraglutide, dulaglutide, and semaglutide for GLP-1RAs, and empagliflozin, canagliflozin, and dapagliflozin for SGLT-2i, respectively.27,28 Meanwhile, adequate vitamin D supplementation may improve insulin resistance in T2DM, as the average age of diabetics is 50–60 years.29 In clinical practice, it is crucial to select a GLP-1RA with cardiovascular efficacy, good glucose lowering and weight loss according to the patient’s condition and needs.
The study conducted by Qiu Bo et al30 on health technology assessment has been implemented in their region and is now being adopted in other regions of China to provide guidance to healthcare organizations on drug selection based on this guideline. The current evaluation of the 7 GLP-1 RAs was based on the second version of the guideline, which is consistent with the previous evaluation of the first version, which recommended semaglutide (71.00 points), dulaglutide (68.75 points), and liraglutide (67.50 points) as the recommended drugs.31 With further updates to the guidelines and support from other high-quality evidence-based medicine, the results of the two assessments are consistent, indicating that the results of this health technology assessment are reliable, and representative.
The American diabetes association guidelines (2023) and the Chinese guidelines for the prevention and treatment of type 2 diabetes (2020) recommend that among people with type 2 diabetes who have established atherosclerotic cardiovascular disease or established kidney disease, a SGLT-2i or GLP-1RA with demonstrated cardiovascular disease benefit is recommended as part of the comprehensive cardiovascular risk reduction and/or glucose-lowering regimens. Liraglutide, semaglutide and dulaglutide have been shown to be GLP-1RAs with cardiovascular benefit. The results of this study show that the results based on the current evaluation are consistent with the recommended results of the guidelines.
The aim of this study was to conduct an objective and rapid evaluation of 7 GLP-1RAs that have been marketed in China to alleviate the selection pressure of medical institutions due to the large number of varieties and to provide an evidence-based basis for selecting drugs. Meanwhile, the study can also provide drug selection recommendations and methodological references for healthcare organizations in other countries, especially in other countries with low and middle incomes or a low level of healthcare. However, there are several limitations to this study: First, this study is a rapid assessment, not a comprehensive. Healthcare organization must take into account its own hospital and local practices when introducing GLP-1RAs. Second, with the updating of evidence-based medicine, the extension of the clinical application period of drugs, the price changes brought about by the tendering and purchasing of drugs, the adjustment of the national essential drug list, the adjustment of the national health insurance list, and the development of drug manufacturers, the changes will further affect our evaluation indexes and results. Therefore, evaluators must update their evaluations in a timely manner to avoid bias in evaluation results.
This study needs more adequate evidence of evidence-based medicine (eg, real-world multicenter clinical data, high-quality meta-analysis, etc.) to make the evaluation results more comprehensive and representative. At the same time, in order to make this guideline more convincing and representative, the weights of each index and evaluation criteria need to be optimized through continuous practice.
Conclusions
7 GLP-1RAs that have been marketed in China were objectively evaluated according to the drug evaluation guidelines, and the evaluation results can provide a reference for medical institutions to select GLP-1RAs drugs. When a healthcare organization introduces a GLP-1RAs, the top three ranked drugs, semaglutide, dulaglutide and liraglutide, can be used as recommended drugs based on the evaluation results.
Acknowledgments
We would like to thank all of the author that participated in the present study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Project funded by the Central Financial Government’s Subsidy Fund for Improving Medical Service Protection Capacity, No. Z155080000004. Guangzhou Municipal People’s Livelihood Science and Technology Research Program Project, No. 201803010096. China Association for Pharmaceutical Education 2023 Special Project on Health Technology Assessment of Clinical Medication, No. 2023WSJSPGZXKT-43. Guangdong Hospital Pharmacy Research Fund-Special Fund for Comprehensive Clinical Evaluation of Drugs (No. 2022-1115-12).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Men P, Tang H, Zhai S. Steps and methods of pharmaceutical health technology assessment. China Medi Insurance. 2015;10(3):57–59.
2. Lanting L, Jinlan F, Lin X, et al. Dilemma and way out of health technology assessment in Chinese hospitals. China Hospl Manag. 2019;39(02):7–10.
3. Green A, Hede SM, Patterson CC, et al. Type 1 diabetes in 2017: global estimates of incident and prevalent cases in children and adults. Diabetology. 2021;64:2741. doi:10.1007/s00125-021-05571-8
4. IDF Diabetes Atlas; 2021. Available fromhttps://diabetesatlas.org/atlas/tenth-edition/.
5. Ong KL, Stafford LK, McLaughlin SA, et al. Global, regional, and national burden of diabetes from 1990 to 2021, with projections of prevalence to 2050: a systematic analysis for the Global burden of disease study 2021. Lancet. 2023;402:203.
6. World Health Organization. Obesity and overweight [OL]. Available from: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
7. Gavin JR 3rd, Rodbard HW, Fox KM, et al. Association of overweight and obesity with health status, weight management, and exercise behaviors among individuals with type 2 diabetes mellitus or with cardiometabolic risk factors. Risk Manag Healthc Policy. 2009;2:1–7. PMID: 22312203; PMCID: PMC3270907. doi:10.2147/RMHP.S4562
8. Shi R, Niu Z, Wu B, et al. Study on the risk factors for hyperuricaemia and related vascular complications in patients with type 2 diabetes mellitus. Risk Manag Healthc Policy. 2020;13:1661–1675. PMID: 33061700; PMCID: PMC7518772. doi:10.2147/RMHP.S255042
9. Yanzhen ZHAO, Jing DU. Research progress of GLP-1 receptor agonists in the treatment of type 2 diabetes mellitus[J]. Geriatrics Research. 2021;2(03):55–60.
10. ElSayed NA, Aleppo G. 9. Pharmacologic approaches to glycemic treatment: standards of care in diabetes—2023. Diabetes Care. 2023;46(Supplement_1):S140–S157. doi:10.2337/dc23-S009
11. Zhigang ZH, Zhanjun DO, Jianping LIU. A rapid guide to drug evaluation and selection in Chinese medical institutions. Medicine Herald. 2023;42(04):447–456.
12. Wang Z, Liu J, Jianjun L, et al. Guidelines for lipid management in China (2023). Chin J Circu. 2023;38(03):237–271.
13. Diabetes Branch of Chinese Medical Association. Guidelines for the prevention and treatment of type 2 diabetes in China (2020 Edition). Intl J Endocrinology Metab. 2021;41(05):482–548.
14. Prevention D, Treatment of Clinical Guidelines Writing Group. Clinical guidelines for prevention and treatment of type 2 diabetes in the elderly in China (2022 Edition). Chin J Diabet. 2022;30(01):2–51.
15. Mannucci E, Candido R, Monache LD, et al. Italian guidelines for the treatment of type 2 diabetes. Nutr Metab Cardiovasc Dis. 2022;59(5):579–622. doi:10.1016/j.numecd.2022.01.027
16. Cosentino F, Grant PJ, Aboyans V, et al.; ESC Scientific Document Group. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur Heart J. 2020;41(2):255–323. PMID: 31497854. doi:10.1093/eurheartj/ehz486
17. Doyle-Delgado K, Chamberlain JJ, Shubrook J H, et al. Pharmacologic approaches to glycemic treatment of type 2 diabetes: synopsis of the 2020 American diabetes association’s standards of medical care in diabetes clinical guideline[J]. Ann Internal Med. 2020;173(10):813–821. doi:10.7326/M20-2470
18. Araszkiewicz A, Bandurska-Stankiewicz E, Budzyński A, et al. 2020 Guidelines on the management of diabetic patients. A position of Diabetes Poland. Clinical Diabet. 2020;9(1):1–101.
19. Gong S, Gao M, Yang H. Interpretation of the 2020 American college of cardiology’s “expert consensus decision path for new treatments to reduce cardiovascular risk in patients with type 2 diabetes”: lowering blood sugar should protect the heart. Chinese General Practice Med. 2021;24(05):509–516.
20. Tan JWC, Sim D, Ako J, et al. Consensus recommendations by the Asian pacific society of cardiology: optimising cardiovascular outcomes in patients with type 2 diabetes. European Cardiol Review. 2021;16. doi:10.15420/ecr.2020.52
21. Center for Capacity Building and Continuing Education of the National Health Commission, Yihong S, Kang C, Xin C, et al. Expert consensus on the diagnosis and treatment of cardiovascular disease in diabetic patients [J]. Chinese J Int Med. 2021;60(5):421–437. doi:10.3760/cma.j.cn112138-20201208-00999
22. Tsapas A. Comparative effectiveness of glucose-lowering drugs for type 2 diabetes: a systematic review and network meta-analysis. Ann Internal Med. 2020;173(4):278–286. doi:10.7326/M20-0864
23. Shen S, Cong W, Changdong D, et al. Systematic evaluation of the efficacy and safety of polyethylene glycol losenatide in the treatment of type 2 diabetes mellitus. Chin J Hospital Pharm. 2021;41(17):1703–1709. doi:10.13286/j.1001-5213.2021.17.02
24. Xia L, Shen T, Dong W, et al. Comparative efficacy and safety of 8 GLP-1RAs in patients with type 2 diabetes: a network meta-analysis. Diabetes Res Clin Pract. 2021;177:108904. doi:10.1016/j.diabres.2021.108904
25. Jing G. Research progress of glucagon-like peptide-1 receptor agonists in cardiovascular complications of type 2 diabetes mellitus[J]. Modern Diag Therap. 2020;31(19):3041–3042+3190.
26. Xie Z, Yang S, Deng W, et al. Efficacy and safety of liraglutide and semaglutide on weight loss in people with obesity or overweight: a systematic review. Clin Epidemiol. 2022;14:1463–1476. doi:10.2147/CLEP.S391819
27. Yanlan L, Aiwen H, Guanxu C, et al. Cardiovascular benefit of SGLT-2 inhibitors and GLP-1 receptor agonists in the treatment of type 2 diabetes: a systematic review and reticulated Meta-analysis[J]. J Pharm Pract. 2022;40(04):354–358.
28. Xie C, Zhou J. Recent research progress on the evidence and mechanism of cardiovascular benefit of SGLT2 inhibitors in type 2 diabetes mellitus population. Mod med health. 2021;37(15):2599–2604.
29. Zhao H, Tang Y, Zheng C, et al. Vitamin D status is independently associated with insulin resistance in patients with type 2 diabetes mellitus. Risk Manag Healthc Policy. 2021;14:1393–1399. PMID: 33854388; PMCID: PMC8039193. doi:10.2147/RMHP.S299963
30. Qiu B, Xiao L, Haotian Y, et al. Application of hospital health technology assessment in the selection and evaluation of sulfonylureas[J]. Chinese J Pharmacy. 2021;56(02):153–161.
31. Xie Z, Li J, Yang S, et al. A health technology assessment based on Chinese guidelines: glucagon-like peptide-1 receptor agonist in the treatment of type 2 diabetes complicated with cardiovascular disease. Therap Clinil Risk Manag. 2022;18:889–900. doi:10.2147/TCRM.S375067
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.