")
Back to Journals » Patient Preference and Adherence » Volume 18
Health Literacy Needs of Acute Pancreatitis Patients During the Diagnosis and Treatment Process Under the Lens of the Timing It Right Theory: A Qualitative Study
Authors Su X, Ma S, Yang X, Zhang C, Chen W
Received 26 October 2023
Accepted for publication 13 February 2024
Published 26 February 2024 Volume 2024:18 Pages 507—517
DOI https://doi.org/10.2147/PPA.S444955
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Xia Su,1,2 Shuli Ma,3 Xiaoxi Yang,4 Can Zhang,1 Weiwei Chen5
1Hepatobiliary and Pancreatic Center, Clinical Medical College, Yangzhou University, Yangzhou, Jiangsu, People’s Republic of China; 2School of Nursing & Public Health, Yangzhou University, Yangzhou, Jiangsu, People’s Republic of China; 3Department of Gastroenterology, Affiliated Hospital of Nantong University, Nantong, Jiangsu, People’s Republic of China; 4School of Health and Wellness, Panzhihua University, Panzhihua, Sichuan, People’s Republic of China; 5Medical College of Yangzhou University, Yangzhou, Jiangsu, People’s Republic of China
Correspondence: Weiwei Chen, Tel +86 18051062900, Email [email protected]
Background: The incidence and recurrence rate of acute pancreatitis (AP) continues to increase worldwide. The risk of AP attack and recurrence is closely related to the patient’s health literacy. Previous studies have shown that AP patients had low levels of health literacy. Understanding patients’ experience in AP’s diagnosis and treatment process and their health literacy needs might significantly improve their health status.
Objective: This study aims to understand the experience of acute pancreatitis (AP) patients in the diagnostic and treatment process and explore their health literacy needs at various phases of this process.
Methods: This study utilized a qualitative approach based on Timing It Right theory. A purposive sampling strategy was employed to select 31 participants diagnosed with AP at various phases of the diagnosis and treatment process. These patients were selected from the Pancreatitis Treatment Centers of two tertiary hospitals in Eastern China. Subsequently, semi-structured in-depth interviews were conducted with the selected participants. The qualitative data was analyzed using the Colaizzi’s method.
Results: The themes of AP patients’ experiences and health literacy needs at various phases of the diagnosis and treatment process were presented as follows. 1. Diagnosis phase: inability to obtain disease information, psychological support seeking, and change unhealthy lifestyle; 2. Hospitalization phase: disease treatment information needs and medical professionals’ healthcare. 3. Discharge Preparation phase: fear of recurrence, individualized healthy lifestyle instruction. 4. Home Recovery phase: self-management, continuous healthcare needs, and family support.
Conclusion: AP patients’ HL needs and health-related problems vary during the diagnosis and treatment process. Medical professionals should comprehend AP patients’ changing needs and individual differences, provide continuous healthcare, and involve families in patient management. These factors support patients’ long-term self-management and preserve their overall health.
Keywords: acute pancreatitis, Timing It Right, health literacy need, qualitative study
Background
Acute pancreatitis (AP) is a gastrointestinal emergency characterized by acute onset and rapid progression by abnormal activation of pancreatic enzymes and local inflammation of the pancreas. It can cause systemic inflammatory response syndrome (SIRS), pancreatic necrosis, and organ failure.1,2 The incidence of AP is increasing year by year.3,4 According to the epidemiological statistics of European and American countries, the incidence of AP is 13–45 per 100,000 people, the second major cause of hospitalization for patients with digestive system diseases and the fifth major cause of in-hospital death.5 According to reports, the annual incidence of AP in China is 4.9–73.4 per 100,000 people.6 AP patients have complex conditions and many complications; about 10–30% of patients will have recurrent attacks.4,7 Due to repeated abdominal pain, nausea, and other symptoms, patients with recurrent AP often show negative emotions, such as anxiety and depression, which seriously affect their quality of life and pose significant challenges to their economy and work status.8
Studies have examined that the attack and recurrence of AP are closely related to the patient’s lifestyle,9 and the patient’s health literacy and self-management capability play a decisive role in their lifestyle. Health literacy (HL) refers to the capability of individuals to make health decisions about medical care, disease prevention, and health promotion based on their knowledge and capability.10 AP patients’ HL has a more direct and noticeable impact on health outcomes as a particular population. Studies have shown that poor eating habits, insufficient physical exercise, and stress in AP patients are the key factors leading to pancreatitis attacks.11 A prospective cohort study by Pang et al showed an inverse association between behavioral habits in HL and AP risk.12 Previous longitudinal survey results found that AP patients’ overall HL level was low.13 Due to the complex condition and rapid progress during the treatment, AP patients often have negative emotions such as anxiety and depression. They are eager to obtain psychological support from medical professionals.7 A longitudinal study showed that most AP patients still had unmet needs for health behavior instructions after discharge, and their health behavior capability was only slightly improved.13
The fundamental basis for improving the HL of AP patients is to scientifically and accurately assess the HL-related problems and needs of AP patients to formulate targeted intervention programs.14 However, existing studies mainly focus on the health education needs of AP, and only a few studies explored the related problems and needs of AP patients from the perspective of HL.15,16 At the same time, the HL needs changes of patients in the diagnosis and treatment process of AP are also the concerns of this study. Therefore, this study uses a qualitative approach to understand the experience of AP patients in the diagnosis and treatment process and explore the HL needs of AP patients. At the same time, using the Timing It Right (TIR) theory as a theoretical framework, the changes in the HL needs of AP patients at various phases will be further explored. TIR theory was proposed by American scholar Cameron et al.17 This theory advocates that the disease is divided into five stages, including the diagnosis phase, the stable phase, the discharge preparation phase, the adjustment phase, and the adaptation phase. It is believed that the support and needs of patients develop with the progress of the disease phase. To adapt to the dynamic needs of patients in various phases, medical professionals should provide active care to patients. This theory has been used to explore the physiological needs and nursing interventions of patients with acute respiratory distress syndrome18 and stroke,19 and the effect is significant. It is expected that the findings of this study can provide evidence for medical professionals to formulate valid and feasible intervention plans and ultimately help AP patients improve their health status.
Methods
Design
This study used a phenomenological qualitative design to understand AP patients’ experiences during the diagnosis and treatment process and explore the HL needs of AP patients at various phases.
Participants and Sampling
Purposive sampling was used to select 31 AP patients treated in the Pancreatitis Treatment Centers of 2 tertiary hospitals in Eastern China as the participants from September 2022 to March 2023. Inclusion criteria: diagnosis of AP1 for the first time, 18 to 80 years of age, talking freely and clearly, and voluntarily participating in the study. Exclusion criteria: patients with a history of severe mental disorders, other organ dysfunction, and malignant tumors will be excluded from the study. The determination of sample size followed the principle of data saturation, and the sample is enough once no new idea sparks from participants’ information.
Based on the TIR theory,8 combined with the clinical characteristics of AP and the suggestions of relevant experts in Gastroenterology, General Surgery, and Pancreatitis Treatment Center, the process of diagnosis and treatment of AP was finally divided into four phases: 1. Diagnosis phase, within 24 hours after admission; 2. Hospitalization phase; 3. Discharge Preparation phase, 1~2 days before discharge; 4. Home Recovery phase: previous studies showed that the HL of AP patients decreased after discharge, then gradually increased, and leveled13 off after about three months, suggesting that they may experience more health problems and challenges within three months after discharge, so this study set the Home Recovery phase for within three months after discharge. There was no duplication of participants in the four phases. Participants in the four phases were marked by letters A, B, C, and D, respectively.
Data Collection
The semi-structured, in-depth interviews were conducted with 31 participants. Face-to-face interviews were conducted in the hospital for participants in the Diagnosis, Hospitalization, and Discharge Preparation phases. Online interviews were conducted via telephone for participants who were at home in the Home Recovery phase.
Interview Guide
The interview guide for this study was determined through 3 stages. In stage 1, the researcher preliminarily drew up the interview guide according to the research purpose, literature review, expert suggestions, and the researcher’s clinical experience. In stage 2, two participants who met the inclusion criteria were pre-interviewed using the interview guide proposed in stage 1. In stage 3, the interview guide was revised according to the pre-interview, and the interview guide was formally confirmed after the research group discussion. The questions of the final interview guide are shown in Table 1.
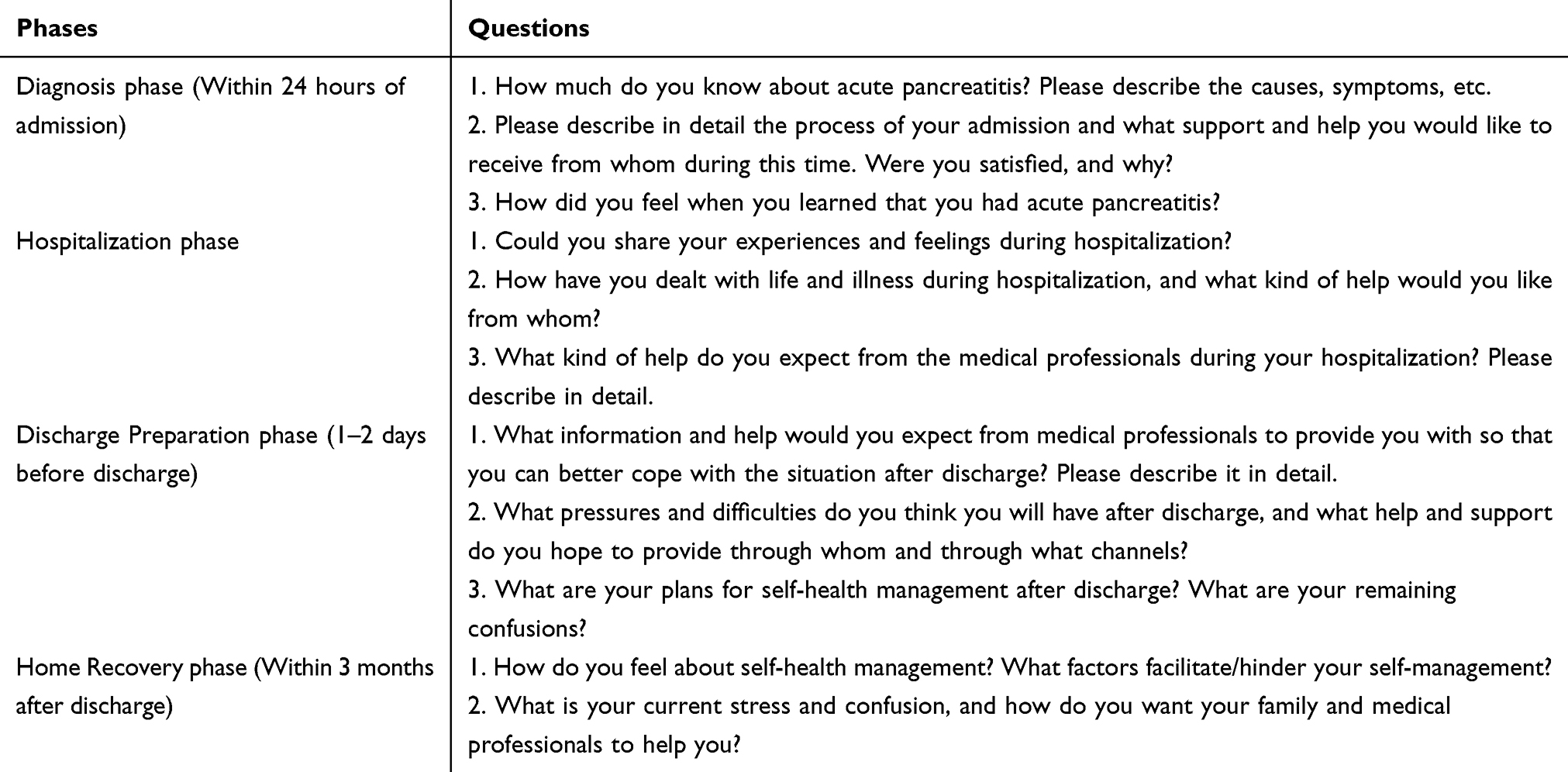 |
Table 1 The Interview Guide for Participants in the Four Various Phases |
The participants determined the time and place of the face-to-face interview. The interview was generally held in the afternoon when there were fewer treatments. The interview place was a quiet classroom or ward, and unrelated persons were absent. The privacy of participants was fully respected and protected. At the beginning of the interview, the researcher created a relaxed communication atmosphere, and each interview began with a “daily conversation”. Secondly, the researcher guided the interview according to the previously formulated interview guide and encouraged the participants to express their opinions on the problem actively. The researcher would use probing questions to explore if valuable information sparks from participants. The researcher carefully recorded the participants’ expressions, body, and language changes during the answer process, avoided excessive subjective guidance and suggestive questions, and maintained a neutral and respectful attitude. After the interview, the vague and unclear contents of the interview were inquired and verified with the participants.
Data Analysis
The audio files of the interviews were transcribed into text within 24 hours after each interview, and the transcripts were checked twice. If there were any disagreements with the contents of the transcripts among the researchers, the researcher would confirm with the participants to clarify their opinions. Nvivo 11 software was used to manage the qualitative data. Colaizzi’s method was adopted for data analysis: 1. The interviews’ transcripts should be read thoroughly to be fully understood. 2. Identify and categorize significant statements relevant to the topic being studied. 3. Meanings should be derived from the identified significant statements. 4. Organize the formulated meanings into clusters of themes. 5. Integrate findings in steps 1–4 into an exhaustive description of the topic under study. 6. Formulate statements that describe the fundamental structure of the topic. 7. Asking participants about the fundamental structure formulated to validate the findings.20 The researchers independently analyzed and coded the original data twice, and the coding process was always neutral and objective.
Ethic
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Clinical Medical College, Yangzhou University (No. 2022ky276). The purpose and significance of the study were explained to all the participants before their participation. The informed consent form was endorsed by each included participant after they were all informed about the study and volunteered to participate. Each participant was duly notified and granted permission for the data to be published anonymously, as stated on the informed consent form. Participants were also informed of the actions required for participation in the study, including the interview and record. They reserved personal rights to refuse to answer sensitive questions.
Trustworthiness
Member checking and peer debriefing were used to achieve credibility. Follow-up interviews with some participants were conducted to verify the findings by implementing member checking. Peer debriefing involves finding a peer debriefer from the research team to review and interrogate the study and data so that the findings resonate with people other than the researcher. The audit trail was used to establish the dependability of this study. The trail of materials, including the process of qualitative interview, the data, findings, and interpretations, will be examined by the auditor from the research team. A reflective journal was developed and maintained to assist the researcher in ongoing self-reflection and to help control the researcher’s bias due to personal traits.
Results
General Information of Participants
There were 31 AP patients selected to participate in the study. The number of participants in each phase was 8, 7, 6, and 10, respectively. There were 18 males and 13 females aged 18 to 72 years. General information of all the participants is shown in Table 2.
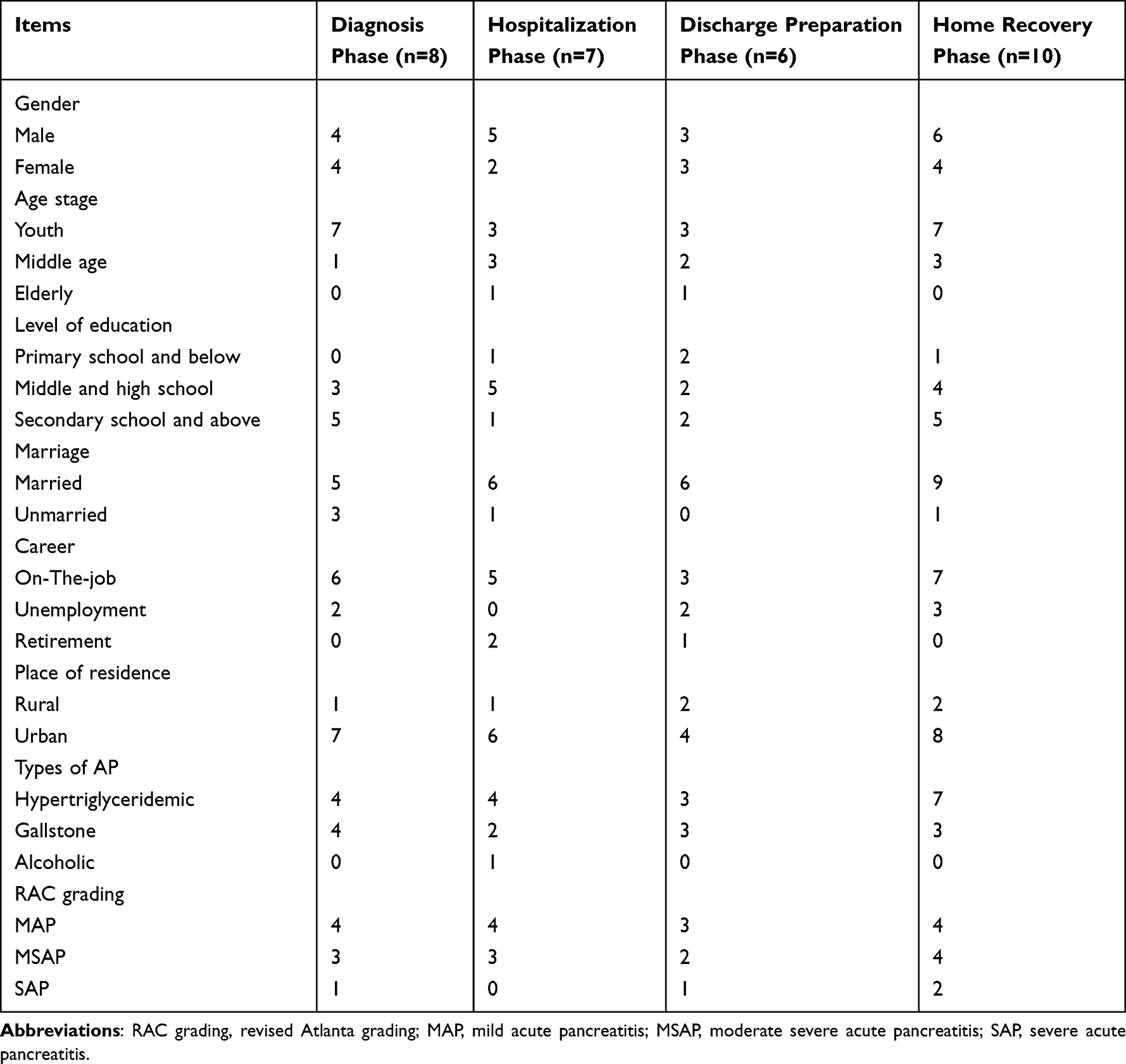 |
Table 2 General Information of 31 AP Patients in Four Phases of the Diagnosis and Treatment Process |
Themes
The study revealed themes of AP patients’ experience and HL needs at the four phases of the diagnosis and treatment process: (1) Diagnosis phase: inability to obtain disease information, psychological support seeking, and change unhealthy lifestyle; (2) Hospitalization phase: disease treatment information needs and medical professionals’ healthcare; (3) Discharge Preparation phase: fear of recurrence, individualized healthy lifestyle instruction; (4) Home Recovery phase: self-management, continuous healthcare needs, and family support.
Diagnosis Phase
Theme 1 Inability to Obtain Disease Information
Most patients lacked knowledge of AP disease and did not understand pancreatic function, pathogenesis, and clinical manifestations of pancreatitis. After patients were told they were diagnosed with pancreatitis, they would obtain relevant knowledge through informal channels such as family, friends, and Internet publicity while questioning the correctness of acquiring knowledge.
A3: I have never heard of pancreatitis before. My relatives and friends have never had pancreatitis, I do not know where the pancreas is, and I have never thought I would have this disease (sigh).
A5: I’ve never heard of pancreatitis before. Can high blood lipids cause pancreatitis? How can my blood lipids be high when I’m so young?
A6, A1: The doctor said high blood lipids caused my pancreatitis. I quickly checked on the Baidu Internet, but I still did not understand what was happening and whether the network explanation was correct.
A7: The doctor told me the pancreas is in this position (pointing to the left lower abdomen). When I first came in, I was asked if it hurt. I thought it was strange. My stomach didn’t hurt much, but my back hurt a lot. I thought it was a recurrence of disc disease.
A8: Nurse, I want to ask you, my husband died of pancreatic cancer, is my disease related to him?
Theme 2 Psychological Support Seeking
During the attack of acute pancreatitis, patients have obvious symptoms such as abdominal pain, abdominal distension, and vomiting. Due to the pain and lack of knowledge of the disease, patients often have unstable emotions such as fear, anxiety, and irritability.
A6: The doctor said that after I had pancreatitis, I felt nothing, but I searched the Internet for Baidu at that time. If I didn’t check, I didn’t know. I was lucky my husband was by my side. Otherwise, it would have been. The nurse came and gave me some comfort. I felt much better.
A6: I have never had this disease before, and I felt terrified when I came to the hospital. We felt much better after the doctors and nurses talked to us.
Theme 3 Change Unhealthy Lifestyle
The incidence of acute pancreatitis is mainly related to bad lifestyle. After admission, patients often self-reflect on their previous bad lifestyle and try adjusting themselves.
A1: If I had known that this disease hurts so much, I would not drink so much wine. I usually like to eat greasy food. I will eat less in the future.
A3: I used to like meat dishes. I’m a fast eater, like to drink Coke, and have an irregular lifestyle. Thinking about how unhealthy my lifestyle was before, I just got this disease. I need to change my lifestyle.
Hospitalization Phase
Theme 1 Disease Treatment Information Needs
Patients want maximum transparency in the treatment process to understand the details of the treatment plan and the reasons for taking the treatment measures. Patients want to be informed of specific information in time to ensure the timeliness and accuracy of the information. So they can be informed about their health status promptly and dynamically and participate in shared decision-making.
B1: I don’t feel much pain now, but the doctor still doesn’t let me eat (curls lips) and drink water. I feel dry to death. When can I eat?
B2: The test results were not updated when I checked them on my phone. The morning rounds are so short we sometimes forget to ask, and the doctor didn’t tell me what the blood test was like. I have done another CT check. Is the condition better for now?
B3: I want to ask that: they say I have a cyst here, it needs an operation to put a tube here. How long should the tube stay? How big is this operation? How do you do that? I don’t know anything.
B4: The doctor said I have gallbladder and bile duct stones and need an operation. I want to ask when to do the operation. I’ve been here for days.
Theme 2 Medical Professionals’ Healthcare
The support of medical professionals is critical for patients during AP’s diagnosis and treatment process. Patients need professional help, guidance, and advice.
B3: We have never had this disease before. The doctor let us buy Rhubarb to drink and Mirabilite for external application. How can we know without your guidance!
B5: When I came, the pain was killing me. A nurse inspected the ward at night and saw that I could not sleep at all. She told the doctor, then gave me an injection and asked me to sit with my legs for a while, then I felt much better.
B6: I didn’t know what to eat on a low-fat diet. I didn’t know the difference between a liquid and a semi-liquid diet. How would we have known if the nurse hadn’t told me?
Discharge Preparation Phase
Theme 1 Fear of Recurrence
Acute pancreatitis is prone to recurrence. When discharged from the hospital, most patients fear disease recurrence and want to obtain relevant information to prevent disease recurrence.
C1: Nurse, what I am most worried about now is what I will eat when I go home and what I can do to avoid recurrence. It hurts too much, and I don’t want to get this disease again.
C2: Nurse, how much should the blood fat be reduced? What method can lower blood fat? How often should I have a review? I do not want to come to the hospital again.
C4: A gallbladder problem causes my pancreatitis. The doctor says I need to rest before returning for the operation. Will it not recur during this period? What am I going to do?
Theme 2 Individualized Healthy Lifestyle Instruction
At this phase, the patient began to resume diet gradually. To keep the condition stable and prevent the recurrence of pancreatitis, the patient attached great importance to diet and exercise and needed to seek appropriate diet and exercise planning. They wanted specific instructions from medical professionals.
C2: Do you have any scientific recipes, such as what to eat daily? Then I will not be bothered by this issue.
C3: Can you make a plan for me? When I leave the hospital, I won’t be able to ask you any time as I do now in hospital.
C5: After I leave the hospital, do I have anything to pay attention to regarding exercise? And what about diet?
Home Recovery Phase
Theme 1 Self-Management
At this phase, patients are in the recovery stage of the disease, and they hope to improve self-management and develop healthy behaviors to avoid disease recurrence. However, limited by age, economic level, education level, and other factors, patients’ self-health management measures and levels are pretty different, and they hope to obtain diversified and suitable health management methods.
D1: I know it’s bad to overeat, and I need to live a healthier lifestyle, but that’s easier said than done!
D2: When I just left the hospital, I could eat what the doctor told me. With time going on and I felt better, I returned to eating freely and stopped monitoring my blood sugar.
D3: Do you have an electronic health management platform that can supervise me, remind me regularly, and help me manage myself well?
D5: You can organize competitions such as diet punch, exercise punch, making healthy recipes, etc., which can motivate us to implement better self-management.
D8: You can go to our community to promote the knowledge of pancreatitis. We can also learn from that.
Theme 2 Continuous Healthcare Needs
After discharge, patients need more health-related instructions and supervision from medical professionals, and their self-management ability needs to improve. Continuous healthcare support from medical professionals after patients’ discharge is crucial for them to prevent recurrence and readmission.
D1: Can you put us (patients) with pancreatitis into a communication group? This way, we can communicate more, and I can also be supervised. You can also pay more attention to us and call us more often. When I left the hospital, I felt like I was left alone.
D4: I still have a drainage tube on my stomach. I can’t deal with it; we are in the countryside, and it is not easy to come to the hospital. Can you come to my home to change my drainage bag?
Theme 3 Family Support
An unhealthy lifestyle is closely related to AP recurrence. The adjustment of lifestyle requires strong self-management of patients themselves; the support and supervision of family also play a vital role.
D3: I think the most important thing is to control my eating habits, and my family should also help and supervise me.
D6: I don’t care as much about my diet now, and sometimes my family doesn’t care as much as they did when I just got back home from the hospital, and I think I might return to my bad habits.
Discussion
This study utilized the TIR theory to understand the experience of AP patients in the diagnosis and treatment process and explore their HL needs. The results indicated that patients’ problems and HL needs varied throughout phases. The primary focus of patients’ needs throughout the Diagnosis and Hospitalization phase is acquiring knowledge about disease and treatment. Conversely, in the Discharge Preparation and Home Recovery phase, patients focused more on health instruction and self-care expertise. During the Diagnosis phase, patients were eager to receive psychological support from medical professionals. During the Hospitalization phase, patients’ requirements shifted to healthcare services provided by medical professionals. Ultimately, patients aspired to enhance their ability to independently manage their health and make necessary lifestyle adjustments throughout the Home Recovery phase. They required individualized lifestyle instructions from medical professionals.
Diagnosis Phase: Provide Patients with Accurate Information About Disease and Treatment, Offer Psychological Support, and Educate Patients in Adopting Health-Promoting Behaviors
This study revealed that following the diagnosis of acute pancreatitis, the patients had a significant deficiency in their comprehension of the disease and demonstrated a strong desire for information pertinent to the illness. This coincides with the findings of Yang Xiaoxi.13 Providing disease-related information to patients in their early treatment phase might effectively alleviate anxiety symptoms, reduce psychological pressure, mitigate uncertainty about the disease, and enhance treatment compliance.21,22 The Knowledge - Attitude - Practice theory posits that the accumulation of knowledge primarily influences individual behavior motivation. Gaining a comprehensive understanding of disease and health is beneficial for developing accurate and optimistic attitudes and beliefs, ultimately leading individuals to modify detrimental behaviors and proactively adopt healthy behaviors.23 Hence, it is imperative for medical professionals to proactively impart disease-related information and potential clinical symptoms to patients upon diagnosis to mitigate patients’ feelings of distress.
A sudden onset, intense severity, elevated mortality, and intense pain distinguish AP. This study revealed varying levels of negative emotions experienced by patients across different phases, including sad mood, anxiety, depression, irritability, and other painful emotions. These feelings were shown to be more intense during the diagnosis period. This aligns with the discoveries made by Ma.24 Prior research has indicated that competent psychological counseling can significantly alleviate patients’ negative feelings, such as sadness and anxiety. It can also raise patients’ self-efficacy, improve their compliance with treatment and nursing care, and facilitate positive changes in their health behaviors.25,26 Thus, at this point, medical professionals ought to enhance communication with patients, pay attention to their feelings, conduct psychological assessments and timely interventions, encourage patients to express their desires, provide them with individualized psychological support, and lessen their negative emotions. Family support can be engaged as necessary to strengthen patients’ faith in the treatment they receive.
Upon the AP diagnosis, the patient started examining their previous unhealthy lifestyle and expressed a wish to adopt healthy behaviors that promote health status, as the attack and the recurrence of AP are mainly associated with unhealthy lifestyle patterns. Thus, it is imperative for medical professionals to enhance health education for patients during this phase. Patients should receive individualized, one-on-one health education when the medical professional has identified the factors that support and hinder their health behavior. The educational content should be emphasized using various mediums such as videos, images, and instructional manuals. These materials should be repeated to enhance patients’ memory consolidation to the greatest extent possible. Simultaneously, it can expand patients’ access to information and assist in developing a healthy behavior attitude, and promote the adoption of a healthy lifestyle through the utilization of mobile platforms such as APPs, WeChat, and SMS.
Hospitalization Phase: Establish a Sound Medical Professional Support System that Encourages Patients to Participate in Decision-Making
Studies have shown that the participation of both medical professionals and patients in decision-making, which embodies the autonomy of patients and the modern medical concept of “patient participation in treatment decision-making”, can effectively raise the awareness of the patient’s owners, stimulate their mobility, and improve their experience and adherence.27 Therefore, during this phase, nurses can choose appropriate decision-making support tools, such as paper and video/audio-video joint support manuals, to increase patient involvement, provide guidance on treatment and communication, and improve patient understanding of treatment information.28 At the same time, this study shows that patients face a variety of stresses during treatment. These pressures arise from the complexity of the condition, the difficulty of treatment, the duration of treatment, and the uncertainty of the effect of treatment. This is consistent with the findings of Boije.29 As an important component of patient social relationships, medical personnel must provide patients with timely, multi-faceted professional support.30 At this stage, medical professionals can help patients find other social support, help them express their ideas, and build confidence in treatment. To help patients’ families adapt as quickly as possible to the role of caregivers, medical professionals need to increase professional skills training for patients’ family members.
Discharge Preparation Phase: Support Patients in Reducing their Fears of Recurrence and Create an Individualized Health Maintenance Plan
Because AP is prone to recurrence, patients who were leaving the hospital frequently showed psychological issues that fear of recurrence and require an understanding of prevention. However, diverse lifestyles, dietary practices, and different causes of acute pancreatitis have left patients uncertain regarding health management at home.31 Therefore, to reduce patients’ fear of recurrence, medical professionals must reassess their health behavior and healthy lifestyle before leaving the hospital, list dietary and environmental inducers, provide targeted guidance and health education, and collaborate with patients to develop individualized health maintenance plans. Middle-aged patients make up a more significant portion of acute pancreatitis sufferers.32 Because of their proficiency with current technology, healthcare providers can utilize the Internet to build lasting relationships with patients to motivate them to keep a healthy lifestyle after leaving the hospital and to avoid AP recurrence and complications.
Home Recovery Phase: Patients, Families, and Medical Professionals Collaborate to Motivate Patients to Adopt Healthy Behaviors
Maintaining a healthy lifestyle is of the utmost importance for preventing AP recurrence. However, most AP patients lack the self-management skills to maintain a healthy lifestyle over a prolonged period after discharge, which causes harmful behaviors like stopping taking medications and excessive eating. Only a small percentage of patients can maintain their health behaviors after discharge following the advice given during hospitalization.12 Medical professionals can use the intelligent platform to implement high-quality continuous healthcare services, enhance patient compliance and self-management skills, and comprehensively manage and supervise patients’ diets, medications, health knowledge, and other aspects after patients with acute pancreatitis are discharged from the hospital. Additionally, the Internet, smartphones, and other information technology and tools make it easier for medical professionals to communicate with patients. Medical professionals can also provide timely and efficient remote health instructions for patients, which not only solves the access difficulties posed by patients’ distance from medical professionals but also encourages the development of ongoing communication between patients. They may watch over and support one another, which is extremely helpful for fostering healthy behaviors in patients.33 Medical professionals should work with patients and families to raise consciousness about the significance of family support and participation in promoting patients’ healthy behaviors and also establish an optimal family environment that supports patients in maintaining their healthy status.
Limitations
This study is the first attempt to gain an understanding of the experience of AP patients during the diagnosis and treatment process by using a qualitative approach. Furthermore, TIR theory was used as the theoretical framework to explore the HL needs of AP patients at various phases of the process. There are certain limitations in this study. Initially, the interviews were conducted only with AP patients, and the caregivers were not included in qualitative interviews. Qualitative interviews with caregivers are desirable in the future to better comprehend AP patients’ health problems. Besides, the interview was conducted exclusively with AP patients in two tertiary hospitals in Jiangsu Province. Multiple center studies are expected to obtain more information on AP patients’ experience and HL needs during the diagnosis and treatment.
Conclusion
AP patients’ health-related problems and HL needs are different in various phases of the disease diagnosis and treatment process. Overall, in the process, patients hope to obtain disease and treatment-related knowledge, be given enough psychological support, be involved in treatment and healthcare decision-making, and improve their health behavior. Medical professionals should understand the dynamic needs of AP patients and the differences between individuals, provide patients with continuous healthcare, and encourage families to participate in patient management. These measures are essential to help patients establish sustained self-management and maintain their health status.
Abbreviations
AP, Acute Pancreatitis; HL, Health Literacy; TIR, Timing It Right.
Acknowledgments
We would like to express our gratitude to the 31 participants who generously shared their time, experience, and stories in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The National Natural Science Foundation of China (Grant No. 82004291); The 333 High-level Talents Training Project of Jiangsu Province; The Foundation Project of Medicine College of Yangzhou University (Grant No. SBLC22005, SBHL22015).
Disclosure
All authors declare no conflicts of interest in this work.
References
1. Pancreatic Surgery Group of the Surgical Society of the Chinese Medical Association. Guidelines for the diagnosis and treatment of acute pancreatitis in China (2021). Chin J Gastrointest Surg. 2021;20(07):730–739. doi:10.3760/cma.j.cn115610-20210622-00297
2. Zhuang DL. Chinese Diabetes Society. Guideline for the prevention and treatment of type 2 diabetes mellitus in China (2020 edition). Chin J Endocrinol Metab. 2021;37:311–398.
3. Wen L, Javed TA, Dobbs AK, et al. The protective effects of calcineurin on pancreatitis in mice depend on the cellular source. Gastroenterology. 2020;159(3):1036–1050.e8. doi:10.1053/j.gastro.2020.05.051
4. Lee PJ, Papachristou GI. New insights into acute pancreatitis. Nat Rev Gastroenterol Hepatol. 2019;16(8):479–496. doi:10.1038/s41575-019-0158-2
5. Yao JH, Li WM. Efficacy of ulinastatin for the treatment of patients with severe acute pancreatitis. Medicine. 2019;98(43):e17644. doi:10.1097/MD.0000000000017644
6. Boxhoorn L, Voermans RP, Bouwense SA, et al. Acute pancreatitis. Lancet. 2020;396(10252):726–734. doi:10.1016/S0140-6736(20)31310-6
7. Liu J, Zhang B. The lived experience of inpatients with acute recurrent pancreatitis: a qualitative research study from West China. Gastroenterol Nurs. 2020;43(3):249–257. doi:10.1097/SGA.0000000000000442
8. McGuire SP, Montero AM, McGreevy KA, et al. Pancreatitis associated anxiety, depression, and stress: hypothesis, definition, and intervention. Surg Open Sci. 2022;2(10):50–52. doi:10.1016/j.sopen.2022.06.005
9. Hegyi P, Párniczky A, Lerch MM, et al. International consensus guidelines for risk factors in chronic pancreatitis. Recommendations from the working group for the international consensus guidelines for chronic pancreatitis in collaboration with the International Association of Pancreatology, the American Pancreatic Association, the Japan Pancreas Society, and European Pancreatic Club. Pancreatology. 2020;20(4):579–585. doi:10.1016/j.pan.2020.03.014
10. Dumenci L, Matsuyama RK, Kuhn L, et al. On the validity of the rapid estimate of adult literacy in medicine (REALM) scale as a measure of health literacy. Commun Methods Meas. 2013;7(2):134–143. doi:10.1080/19312458.2013.789839
11. Adams RJ, Stocks NP, Wilson DH, et al. Health literacy-a new concept for general practice? Aust Fam Physician. 2009;38(3):144–147.
12. Pang Y, Kartsonaki C, Turnbull I, et al. Metabolic and lifestyle risk factors for acute pancreatitis in Chinese adults: a prospective cohort study of 0.5 million people. PLoS Med. 2018;15(8):e1002618. doi:10.1371/journal.pmed.1002618
13. Yang XX. Research on the Development and Application of Health Literacy Scale for Patients with Acute Pancreatitis. Yangzhou: Yangzhou University; 2022.
14. Gurmu DY. Level of patient health literacy and associated factors among adult admitted patients at public hospitals of West Shoa Oromia, Ethiopia. Patient Prefer Adher. 2022;16:853–859. doi:10.2147/PPA.S357741
15. Munigala S, Gardner TB, O’Reilly EM, et al. Understanding pancreatic diseases using animated pancreas patient: informing patients for better health outcomes with visual formats of learning. Pancreas. 2018;47(10):1256–1261. doi:10.1097/MPA.0000000000001178
16. Phillips AE, Faghih M, Drewes AM, et al. Psychiatric comorbidity in patients with chronic pancreatitis associates with pain and reduced quality of life. Am J Gastroenterol. 2020;115(12):2077–2085. doi:10.14309/ajg.0000000000000782
17. Cameron JI, Gignac MA. “Timing it right”: a conceptual framework for addressing the support needs of family caregivers to stroke survivors from the hospital to the home. Patient Educ Couns. 2008;70(3):305–314. doi:10.1016/j.pec.2007.10.020
18. Lee CM, Herridge MS, Matte A, et al. Education and support needs during recovery in acute respiratory distress syndrome survivors. Crit Care. 2009;13(5):R153. doi:10.1186/cc8053
19. Burns SP, Lutz BJ, Magwood GS. “Timing it Right”: needs of African American adults with stroke and their caregivers across the care continuum. Ethn Health. 2022;27(2):420–434. doi:10.1080/13557858.2019.1693512
20. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
21. Xiong S, Ding M, Li P, et al. A health education model based on knowledge, attitude, and practice used as adjunct therapy for metabolic syndrome complicated with acute pancreatitis: a case report. J Int Med Res. 2020;48(5):300060520924272. doi:10.1177/0300060520924272
22. Lavalley SA. Caregiver informational support in different patient care settings at end of life. Home Health Care Serv Q. 2018;37(2):97–112. doi:10.1080/01621424.2018.1438951
23. Graham P. Classroom-based assessment: changing knowledge and practice through preservice teacher education. Teaching Teacher Educ. 2005;21(6):607–621. doi:10.1016/j.tate.2005.05.001
24. Ma S, Yang X, He H, et al. Psychological experience of inpatients with acute pancreatitis: a qualitative study. BMJ Open. 2022;12(6):e060107. doi:10.1136/bmjopen-2021-060107
25. Chen C, Zhou Y, Wang D, et al. Anxiety, depression, and coping styles among patients with chronic pancreatitis in East China. BMC Psychiatry. 2023;23(1):212. doi:10.1186/s12888-023-04691-2
26. Pezzolato M, Spada GE, Fragale E, et al. Predictive models of psychological distress, quality of life, and adherence to medication in breast cancer patients: a scoping review. Patient Prefer Adher. 2023;17:3461–3473. doi:10.2147/PPA.S440148
27. Chang HL, Li FS, Lin CF. Factors influencing implementation of shared medical decision making in patients with cancer. Patient Prefer Adher. 2019;13:1995–2005. doi:10.2147/PPA.S217561
28. Chenel V, Mortenson WB, Guay M, Jutai JW, Auger C. Cultural adaptation and validation of patient decision aids: a scoping review. Patient Prefer Adher. 2018;12:321–332. doi:10.2147/PPA.S151833
29. Boije K, Drocic A, Engström M, et al. Patients’ perceptions of experiences of recovering from acute pancreatitis: an interview study. Gastroenterol Nurs. 2019;42(3):233–241. doi:10.1097/SGA.0000000000000375
30. Al-Noumani H, Omari O, Al-Naamani Z. Role of health literacy, social support, patient-physician relationship, and health-related quality of life in predicting medication adherence in cardiovascular diseases in Oman. Patient Prefer Adherence. 2023;17:643–652. doi:10.2147/PPA.S401666
31. Lankisch PG, Apte M, Banks PA. Acute pancreatitis. Lancet. 2015;386(9988):85–96. doi:10.1016/S0140-6736(14)60649-8
32. Lin S. Retrospective Analysis of Large Sample Data on the Pathogenetic Characteristics, Treatment and Regression of Acute Pancreatitis. Guangzhou: Southern Medical University; 2022.
33. Kistler CE, Zimmerman S, Khairat S. Health information technology challenges and innovations in long-term care. J Am Med Dir Assoc. 2021;22(5):981–983. doi:10.1016/j.jamda.2021.03.017
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.