")
Back to Journals » Risk Management and Healthcare Policy » Volume 17
Health Disparities Among Family Decision-Makers in China: An Ordered Probit Analysis of the China Family Panel Studies
Authors Zhang S, Huang Y , Wang X, Wang H
Received 23 October 2023
Accepted for publication 15 March 2024
Published 19 March 2024 Volume 2024:17 Pages 635—647
DOI https://doi.org/10.2147/RMHP.S443930
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gulsum Kubra Kaya
Songbiao Zhang,1 Yuxuan Huang,1 Xining Wang,1 Huilin Wang1,2
1School of Business, Hunan University of Science and Technology, Xiangtan, Hunan Province, People’s Republic of China; 2Moray House School of Education and Sport, The University of Edinburgh, Edinburgh, Scotland, UK
Correspondence: Huilin Wang, Moray House School of Education and Sport, the University of Edinburgh, Edinburgh, Scotland, UK, Email [email protected]
Purpose: The family decision-makers serve as the backbone of the family, and their health status warrants consideration. This study aims to explore how the health status of this group of people, namely the family decision-making group, is affected, and to delve into the mechanisms of influence based on this. The goal is to provide reliable evidence and strategies for the health management of the family decision-makers group, contributing to the achievement of the “Healthy China 2030” Planning Outline.
Patients and Methods: Drawing on data from the China Family Panel Studies (CFPS), this study utilizes an Ordered Probit Model to analyze and compare the health status of family decision-makers and non-decision-makers.
Results: The findings indicate that decision-makers tend to experience poorer health outcomes than other family members, with increased pressure related to decision-making identified as a significant contributor to their declining health. Heterogeneity analysis reveals that the negative effect is less pronounced in households with higher net worth but more pronounced in those with more significant housing, education, and medical spending pressures. Moreover, this study analysis highlights that enhancing individual or family socioeconomic status can alleviate the adverse health effects experienced by family decision-makers.
Conclusion: The study reveals the presence of certain health adverse effects among family decision-makers. The implications drawn from this research hold significance for the health management of this demographic, underscoring the necessity for tailored interventions aimed at addressing the distinctive challenges confronted by this group.
Keywords: family decision makers, health, pressure, socioeconomic status
Introduction
As the economy and society develop, people’s living standards steadily improve, leading to a growing desire for a better quality of life. As a result, health has received significant attention and extensive discussion worldwide as a critical aspect of well-being. Moreover, as an essential component of human capital,1 health is fundamental in promoting family happiness and social development. However, numerous factors impact residents’ health, and the effects on different population groups can vary significantly. Therefore, governments must research various population groups to formulate effective countermeasures to clarify each influencing factor’s underlying mechanisms.
In the “Healthy China 2030” Planning Outline, the Chinese government has prioritized the health of its citizens as a fundamental objective for achieving a healthy nation. The plan recognizes the need to address health issues among key groups such as women, children, the elderly, people with disabilities, and low-income. It emphasizes the importance of strengthening health services for these populations, which includes implementing safety plans for maternal and child health, promoting the construction of medical and health service systems for older adults, and formulating regulations on disability prevention and rehabilitation for disabled individuals. These measures aim to reduce health disparities among different groups and promote universal health coverage, thus advancing social equity. However, this study has revealed that family decision-makers lack corresponding measures and guarantees to support their health and well-being.
Based on existing research, scholars have shown greater attention to the health status of vulnerable groups such as women, children, older adults, people with disabilities, and low-income earners.
For older adults, studies have shown that marriage can enable both partners to care for each other, thereby promoting the health status of older adults.2 Social participation significantly improves the self-rated health of older adults by changing health behaviors and accessing health resources, with more significant effects on the health status of older adults.3 The health status of elderly parents is more conducive to improvement with their children’s higher income and education levels.4 Additionally, subjective social support significantly impacts the health of rural older adults.5
For children, Case, Fertig6 tracked a group of children from childhood to adulthood and found that those with poor health received less education and had poorer health as adults. In a study by Wang,7 notable health disparities were observed among three distinct groups of children in China, namely rural children, urban children, and migrant children. Furthermore, the father’s educational attainment was found to play a compensatory role in addressing these health disparities among children. Another influential factor impacting the health of children and adolescents, particularly their mental well-being, is the influence of social media, as evidenced by the research conducted by Richards, Caldwell.8
Furthermore, studies have shown that low-income residents face significant health maintenance disadvantages.9 Multiple studies have consistently demonstrated that individuals belonging to low-income groups often exhibit unhealthy eating behaviors, which undoubtedly serve as a significant determinant of their health status, consequently contributing to the existence of health disparities when compared to their high-income counterparts.10 Nevertheless, it is noteworthy that income inequality exerts a more profound detrimental influence on the self-rated health of low-income individuals, exacerbating the prevailing health inequalities within society.11
Socioeconomic status significantly influences the risk of disease among Chinese women, particularly within the female demographic. Notably, education emerges as the foremost protective factor among this group.12 Wu 13 found that switching household cooking from solid to clean fuels improved women’s self-rated and other-rated health. The health effect of changing from clean cooking fuels for women aged 46 and over was more significant than that for women aged 45 and under14 used the modified Multidimensional Energy Poverty Index (MEPI) to measure and monitor multidimensional energy poverty. They found a significant negative causal relationship between multidimensional energy poverty and women’s health.
Research findings indicate that individuals with disabilities generally experience inferior oral health compared to their non-disabled counterparts. Irrespective of the specific type of disability, disabled individuals exhibit a greater prevalence of dental caries issues than those without disabilities.15 Holm, Sainio16 studied the impact of the COVID-19 pandemic on the social and mental health of disabled people. They found that those with mobility and cognitive disabilities believed more often than non-disabled people that the pandemic had reduced their hope for the future. Likewise, Mitchell, Ryder17 found that people with disabilities are often affected by socioeconomic disadvantage and suffer worse health outcomes than non-disabled people.
In current health research, relatively little attention has been paid to dominant groups such as family decision-makers. Traditional Chinese family values emphasize the importance of the family, considering it as the fundamental unit of society and the foundation for individual growth and social stability. Within these values, affection and a sense of responsibility hold an extremely important position, with family members caring for and helping each other, each bearing their own responsibilities. However, the division of labor within the family varies, and thus the responsibilities and pressures faced are also different. As the backbone of the family, family decision-makers play a crucial role in determining the efficient allocation of family resources and the well-being of family members. However, there is a lack of clear understanding of the health status of this group within the academic community. From a self-interest perspective, family decision-makers can allocate limited family resources to improve their health and benefit from greater freedom in the allocation process.18 Moreover, family decision-makers gain more respect from family members and experience greater psychological satisfaction, which can positively affect their physical and mental health. Additionally, family decision-makers receive more care and attention from family members to ensure the stability and normal functioning of the family, which further benefits their health. These are potential benefits of being a family decision-maker on health status, defined as positive effects in this study. However, from a grand perspective, higher family status brings more responsibilities and pressure. As a result, family decision-makers may need to engage in more complex mental or physical work to improve the entire family’s welfare, which may adversely affect their health. Additionally, Chinese families face increasing pressure due to rising housing, education, and medical expenses. High housing prices have forced many families to take on significant housing loans, while the increasing cost of education has made it a substantial part of the family’s expenses. Finally, the high cost of medical expenses requires families to save more as a precaution against illness, putting additional pressure on family decision-makers. Chronic stress has been found to have detrimental effects on health through its influence on the rate of cellular aging.19 All the above are potential adverse effects of being a family decision-maker on health status, defined as adverse effects in this study.
In the process of promoting “Healthy China”, family decision-makers are undoubtedly a group that cannot be overlooked. However, given that serving as a decision-maker in the family has two opposing effects on residents’ health, and there is currently no research exploring which effect dominates. To address this gap, this study aims to study the impact of having decision-making power in the family on residents’ health status and to delve into the mechanisms of influence. We aim to reduce family health disparities and promote health equity by proposing effective interventions for this group. Utilizing data from the China Family Panel Studies (CFPS), this study employs an Ordered Probit Model to compare and analyze differences in health status between family decision-makers and non-decision-makers.
This study makes several contributions. Firstly, conducting a comparative analysis of the health status differences between family decision-makers and non-decision-makers broadens the research perspective on family decision-makers. Secondly, this study discovers that family decision-makers experience more significant pressure than non-decision-makers, negatively affecting their health status. This finding provides theoretical and empirical support for the health management of family decision-makers. Thirdly, the study’s results indicate that enhancing the socioeconomic status of individuals or families can partially mitigate the adverse health effects experienced by family decision-makers. This finding offers a valuable reference for promoting the population’s overall health from the social status perspective.
Materials and Methods
Study Design
The China Social Science Survey Center at Peking University conducted this cross-sectional study, establishing the China Family Panel Studies (CFPS) database. This survey aims to reflect the changes in Chinese society, economy, population, education, and health by tracking data across three levels: individuals, families, and communities. It particularly focuses on issues related to the economic and non-economic well-being of Chinese residents, primarily including three sub-databases: the Family Member Relationship Database (famconf), the Family Economy Database (famecon), and the Individual Database (person). Moreover, the CFPS sample is a multi-stage probability sample drawn using implicit stratification methods, covering 25 provinces/cities/autonomous regions, which provides good representativeness and well satisfies the objectives of this study.
Study Population
Our research subjects include both family decision-makers and non-decision-makers. Based on the design of the CFPS questionnaire, the inclusion criteria are set to identify families with identifiable decision-makers for significant events, while families that cannot identify decision-makers for significant events are excluded.
Sample Size
Based on the results of variable selection, we merged the three CFPS databases and eliminated missing values from the variables to obtain a valid analytical sample for our study, totaling 5,678 sample observations. This includes 1,814 family decision-makers and 3,864 non-decision-makers. In the robustness checks that follow, we also applied a top and bottom 1% winsorization to continuous variables to eliminate extreme values.
Variable Setting
Dependent Variable
The dependent variable used in this study is individual health status, measured by subjective self-assessment. This variable is a direct and widely used physiological health indicator in the social sciences. The questionnaire measures residents’ health status by asking, “How do you assess your own health condition?” Respondents’ answers are categorized as “unhealthy”, “average”, “relatively healthy”, “healthy”, and “very healthy”, and are assigned integer values from 1 to 5, respectively. Within the sample, the average level of self-rated health among respondents is 2.74, which is below the “relatively healthy” level. Self-rated health is a comprehensive measure considering disease severity, family history of disease, and overall health status.20,21 This reliable and valid measurement approach conforms to psychometric principles. Therefore, we use self-rated health as the primary measure of health status and employ other health-related variables as explanatory variables in robustness tests.
Independent Variable
In the CFPS questionnaire, respondents were asked, “Who primarily makes the decisions in your family when encountering significant events (such as building or buying a house, moving, children’s education, etc.)?” The answer provided by the respondent is the personal identification number corresponding to the family decision-maker. If the personal identification number corresponding to the family decision-maker matches that of the respondent, we classify them as a family decision-maker, assigning a value of 1; otherwise, they are assigned a value of 0.
Control Variable
Based on previous research results,22,23 this study controls for other variables that could potentially affect the health of residents, including age (the age of the respondent), gender (with males assigned a value of 1 and females a value of 0), marriage status (with those who are married or cohabiting assigned a value of 1, and all others a value of 0), education level (with values assigned as follows: no schooling = 0, elementary school = 6, junior high school = 9, senior high school/technical secondary school/vocational high school = 12, junior college/technical school = 15, undergraduate = 16, master’s = 19, and doctorate = 22), exercise frequency (ranging from 1 to 5, corresponding to: never, once a month, two or three times a month, two or three times a week, almost every day), sleep duration (in hours), smoking (with respondents who smoked in the past month assigned a value of 1, and those who did not a value of 0), income (logarithm of per capita household income), and urban residence (with those living in urban areas assigned a value of 1, and those in rural areas a value of 0). Additionally, this study introduces province dummy variables in the regression analysis to account for differences in household economic characteristics resulting from regional disparities.
Measurement Model Setting
Individual health status is a discrete ordinal variable, and this study follows the common practice in domestic and international literature by employing an ordered probit model (abbreviated as “Oprobit”) for regression analysis. The Oprobit model treats individual health status as an ordinal variable, requiring the use of latent variables to derive maximum likelihood estimators. Specifically, the model estimated in this article is as follows:

In formula (1),  represents the latent variable for individual health status.
represents the latent variable for individual health status.  is the core explanatory variable, indicating whether an individual holds decision-making power within the family.
is the core explanatory variable, indicating whether an individual holds decision-making power within the family.  is the control variable matrix, and
is the control variable matrix, and  is the random disturbance item, with
is the random disturbance item, with  ,
,  and
and  being the parameters to be estimated. Although
being the parameters to be estimated. Although  is an unobservable latent variable, it has the following relationship with individual health status:
is an unobservable latent variable, it has the following relationship with individual health status:

As shown in equation (2),  represents the individuals health status. When
represents the individuals health status. When  is below the threshold value C1, the resident feels unhealthy (
is below the threshold value C1, the resident feels unhealthy ( ); when it is above C1 but below C2, the resident perceives their health status as average (
); when it is above C1 but below C2, the resident perceives their health status as average ( ); and so forth, when
); and so forth, when  is above C4, the resident feels very healthy (
is above C4, the resident feels very healthy ( ). Furthermore, when
). Furthermore, when  follows a standard normal distribution, the likelihood function of the sample can be derived from equation (2), and the maximum likelihood estimators can be obtained, resulting in the Oprobit model. Since the coefficients estimated by the Oprobit model can only provide limited information in terms of significance and direction, the analysis presented later in this article reports the marginal effects of the explanatory variables on residents health status.
follows a standard normal distribution, the likelihood function of the sample can be derived from equation (2), and the maximum likelihood estimators can be obtained, resulting in the Oprobit model. Since the coefficients estimated by the Oprobit model can only provide limited information in terms of significance and direction, the analysis presented later in this article reports the marginal effects of the explanatory variables on residents health status.
Data Analysis
Data were checked for completeness and consistency, and coded by the principal investigator. Next, they were exported to Stata version 16 for analysis. Initially, in the descriptive analysis, the mean and median values of all variables were calculated for the full sample, the family decision-makers sample, and the non-family decision-makers sample. Subsequently, using the Oprobit model, baseline regression results were provided through stepwise regression, and robustness checks were conducted on this basis by handling extreme values, adding control variables, and replacing dependent variables. Furthermore, an in-depth study of the mechanisms of influence was conducted, and this mechanism was further verified while analyzing heterogeneity. Finally, interaction terms were introduced to explore potential moderating effects. All tests were two-tailed, with a significance level set at 0.05. The results were presented in both text and table formats.
Results
Descriptive Statistics
For comparative purposes, Table 1 provides descriptive statistics for the total sample, the family decision-maker sample, and the non family decision-maker sample, consisting of 5,678, 1,814, and 3,864 observations, respectively. The mean residents’ health status values in the three samples were 2.74, 2.44, and 2.88, respectively. Descriptive statistics show that the health status of family decision-makers is below average and even lower than that of other family members who are not decision-makers in significant events, providing a straightforward comparison.
 |
Table 1 Descriptive Statistics |
Table 1 Descriptive statistics (See the end of the manuscript)
Benchmark Regression
To ensure the robustness of the results, this study employs the method of gradually adding control variables in the regression. The empirical analysis results using Stata/MP17.0 are presented in Table 2. As depicted in Table 2, column (1) shows that when only the provincial dummy variables are controlled, the impact of household decision-makers on residents’ health status is significantly negative at the 1% level, preliminarily revealing the relationship between the two variables. Columns (2) and (3) gradually add control variables, and the direction and significance of the core explanatory variable remain unchanged. The baseline regression results indicate that, on the whole, the negative effect of having decision-making power in the family on residents’ health status is greater than the positive effect, meaning that the health status of family decision-makers is worse than that of non-decision-makers. Specifically, compared to the non-decision-maker group, the health status of family decision-makers is 1.58 percentage points worse. This may also indicate that most decision-makers in Chinese families are altruistic individuals who quietly endure more significant pressure from the family, which, in turn, affects their health.
 |
Table 2 Benchmark Regression |
In terms of control variables, on average, for each unit increase in the Age variable, Health decreases by 0.3%; in terms of Gender, males have a Health status 1.44 percentage points better than females; in terms of Marriage, married or cohabiting residents have a Health status 3.31% worse than unmarried residents; for each unit increase in the Education variable, Health increases by 0.23%; for each unit increase in the Exercise variable, Health increases by 0.55%; for each unit increase in the Sleep variable, health status increases by 0.36%; for each unit increase in the Income variable, Health increases by 0.74%. Additionally, the variables Smoking and Urban have negative and positive impacts on Health, respectively, but both are not significant at the 5% statistical level.
Table 2 Benchmark regression (See the end of the manuscript.)
Robustness Check
Dealing with Extreme Values
Addressing extreme values in the sample is essential as they may significantly affect the regression results. To mitigate this issue, this study excluded samples with residents aged below 20 and above 80 years and applied a shrinkage of 1% to all continuous variables. The regression results after handling extreme values are presented in column (1) of Table 3 and are consistent with the baseline regression results in Table 2.
 |
Table 3 Robustness Check |
Controlling for Having Health Insurance Variable
There is ample evidence to suggest that having medical insurance can reduce out-of-pocket medical expenses, improve access to medical services, and significantly impact.24 As such, this study includes a dummy variable for “having medical insurance” in the model to control its effects further. As a result, the regression results in column (2) of Table 3 remain robust.
Substitution of Explained Variables
Due to the potential subjectivity of self-assessed health status among residents, there may be discrepancies between their perception of personal health and actual health status. To address this issue, this study employs an alternative indicator (whether hospitalized in the past 12 months, yes = 1, no = 0) to measure health status. The Probit model regression results are presented in column (3) of Table 3. The results demonstrate a significantly positive average marginal effect of family decision-makers at the 1% level, indicating that the probability of family decision-makers being hospitalized in the past year is 3.81% higher than that of other family members. This finding confirms that the adverse health effects of family decision-makers remain robust across various model specifications, further supporting the study’s conclusions.
Table 3 Robustness check (See the end of the manuscript.)
Mechanism Test
In this study, household decision-makers are considered the backbone of the household, bearing the majority of household pressure, which can negatively impact the health of residents. The level of depression experienced by family decision-makers is used as an indicator of the family’s stress, which reflects their overall welfare.25–27 Column (1) of Table 4 reveals that household decision-makers face a significantly higher-pressure level than other family members, averaging a 65.07% increase in pressure. Column (2) of Table 4 presents the regression results after controlling for pressure indicators. After controlling for residents’ pressure levels, the average marginal effect of household decision-makers on emotional self-rated health significantly decreases, and the significance level reduces from 1% to 5%. This indicates that being the household’s decision-maker affects residents’ health by increasing pressure levels. Therefore, household decision-makers experience more pressure than non-decision-makers, which is detrimental to their health.
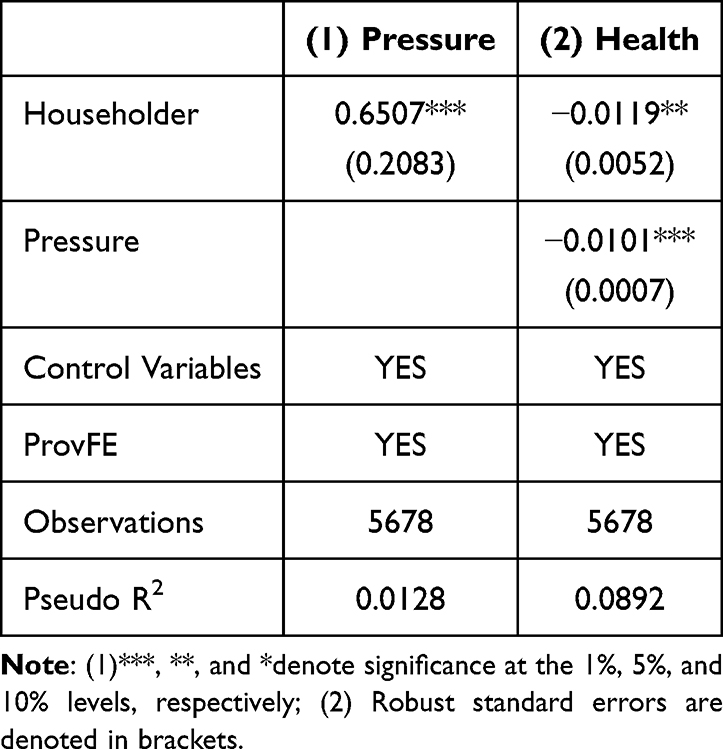 |
Table 4 Mechanism Test |
Table 4 Mechanism test (See the end of the manuscript.)
Heterogeneity Analysis
Regression by Sample of Household Net Assets
The level of net assets is an essential factor that determines the economic pressure of a family. To examine the relationship between net assets and the impact of household decision-makers on residents’ health status, we classified samples into high-net-worth families (whose net assets are higher than the median level) and low-net-worth families (whose net assets are lower than the median level). Sub-sample regression results are presented in Table 5, columns (1) and (2). This study finds that in high-net-worth families, the average marginal effect of family decision-makers is significantly lower and no longer significant compared with samples with lower net assets. This suggests that the pressure faced by household decision-makers in families with higher net worth is relatively low, and the negative impact on their health status is relatively weak.
 |
Table 5 Regression Results of Heterogeneity of Net Household Assets |
Table 5 Regression results of heterogeneity of net household assets (See the end of the manuscript.)
Regression by Sample by the Primary Source of Pressure
To examine household decision-makers’ impact on residents’ health status under different family pressure levels, this study conducted sub-sample regressions based on housing difficulties, education expenditures, and medical expenditures. The regression results are presented in Table 6. Firstly, the samples were divided into families with more significant and less housing pressure. The results show that family decision-makers’ negative average marginal effect on residents’ pressure is more important in families with more substantial housing pressure. Similarly, in families with higher education expenditure pressure, the impact of household decision-makers on residents’ health status remains significantly negative. Conversely, this effect is no longer significant in families with less education expenditure pressure. Moreover, the sub-sample regression based on medical expenditures reveals a lower significance level of the negative impact of household decision-makers on residents’ health status in families with lower medical expenditure pressure. Interestingly, household decision-makers’ negative effect on residents’ health status is slightly higher in families with less medical expenditure pressure. This may be attributed to the fact that more significant medical expenditure pressure leads to more medical expenditure, which benefits the health status of residents and thus alleviates the negative impact of medical expenditure pressure.
 |
Table 6 Heterogeneity Regression Results of Primary Sources of Family Pressure |
In summary, this study finds that household decision-makers have a more significant negative impact on the health status of residents in families with greater pressure levels. In contrast, their influence is more minor and less important in families with less pressure levels. These results further support that household decision-makers experience more significant pressure, adversely affecting their health outcomes.
Table 6 Heterogeneity regression results of primary sources of family pressure (See the end of the manuscript.)
Expanded Analysis
The inequitably distributed social structures and resources are in large part responsible for the health inequality.28 Therefore, socioeconomic status can undoubtedly have a significant impact on the health status of individuals, and numerous studies have confirmed its positive impact on personal health.29,30 Socioeconomic status determines people’s working and living environments and access to various health products and services.31 Furthermore, it influences people’s psychological state and perception of the outside world. These material and psychological factors jointly affect people’s behavior and exposure to various pathogenic factors, ultimately influencing their health outcomes.
The present study investigates whether the adverse health effects experienced by household decision-makers are influenced by their socioeconomic status. Since subjective social status can better capture socioeconomic status information than objective measures, it has more substantial predictive power for physical and mental health.32,33 Therefore, this study constructed subjective social status indicators using respondents’ responses to “your local social status” and “your family’s local social status”. Higher scores on a scale of 1 to 5 indicate a higher social status of the individual or family in the local area. The regression results in Table 7 incorporate an interaction term between family decision-makers and socioeconomic status.
 |
Table 7 Moderating Effect of Socioeconomic Status |
Consistent with the baseline regression, the study finds that household decision-makers significantly negatively impact residents’ health status. The interaction terms between family decision-makers and personal and family social status are very favorable at the 1% level, indicating that the adverse health effects of family decision-makers are related to the local social group of individuals and families. Specifically, the negative health effects are weaker for families with higher personal or family social status.
Table 7 Moderating effect of socioeconomic status (See the end of the manuscript.)
Discussion
Ensuring individuals’ health and well-being is paramount as it impacts a family’s prosperity and shapes a nation’s future. Vulnerable groups such as older adults, women, children, and people with disabilities face more significant health risks and challenges. If their medical needs are not met, they may fall into a vicious cycle of “vulnerable-unhealthy-more vulnerable”. Health issues concerning vulnerable groups have garnered significant attention from the academic community, and many studies34–39 have proposed effective measures for their health management.
In promoting the health of the entire population, the health problems of family decision-makers need to be given more attention. On the one hand, family decision-makers have an advantage in allocating limited resources within the family. Therefore, they can use more family resources to improve their health status due to their self-interest.18 Additionally, they have greater discretion in utilizing family resources, which may positively impact their health. However, on the other hand, family decision-makers typically have higher family status, which leads to greater family responsibilities and pressures, potentially resulting in adverse effects on their health status.19
As such, the positive and negative effects on the health status of family decision-makers and the size of these effects determine their overall impact on health. Interestingly, our empirical analysis of the health status of Chinese family decision-makers revealed that the adverse health effects on Chinese family decision-makers are likely to be greater due to the influence of the spirit of altruism inherent and family responsibility awareness in Chinese culture. Specifically, the health status of family decision-makers is 1.58 percentage points worse than that of non-decision-makers. In the heterogeneity tests, we found that compared to non-decision-makers, decision-makers in families with greater housing pressure have a 4.16% worse health status, those in families with greater educational expenditure pressure have a 2.57% worse health status, and those in families with greater medical expenditure pressure have a 1.43% worse health status. However, compared to families with greater pressures from housing, education, and medical expenses, decision-makers in families with less pressure have a worse health status than non-decision-makers, but both the degree and significance are significantly reduced. We also analyzed the moderating effect, which found that the socioeconomic status of individuals and families can moderate the adverse health effects of family decision makers.
Family decision-makers have historically been considered privileged, so their health concerns have been overlooked. However, the findings of this study provide a reliable empirical foundation for managing the health of family decision makers, which can contribute to the achievement of the national health goal. Chinese families face increased pressure from education, housing, and medical expenses, primarily affecting family decision makers. Therefore, firstly, China should continue to push for full coverage of basic medical insurance while vigorously promoting supplemental medical insurances, such as major illness insurance, to prevent residents from falling into or returning to poverty due to illness and to increase the utilization rate of medical services. Secondly, the country should actively implement the “double reduction policy” in compulsory education to reduce the burden of educational expenses on families, enabling parents to be relieved from the heavy burden of family education. Finally, China should address the rapid increase in housing prices and provide subsidies to financially struggling families needing housing, breaking the dilemma of most people struggling to buy a house throughout their lives.
China is currently in a period of accelerated social development and transformation, and social differentiation is likely to persist. Given that the socioeconomic status of individuals and families can effectively mitigate the negative impact of the health status of family decision makers, social public policy needs to be adjusted. Health policy should focus on social equity and reducing social status gaps.
Despite the significant contributions of this study, certain limitations exist. Firstly, the research results are based on cross-sectional data, which may result in reverse causality issues that could affect the outcomes. For example, family members may volunteer to serve as family decision-makers to improve their health. Future research should consider using longitudinal data to address this limitation. Secondly, in the present study, the health status assessment relies on the residents’ subjective self-evaluation. However, the subjective self-assessment of health may not accurately measure the health status of residents. It is worth considering a multidimensional approach for a more comprehensive understanding of health status.
Conclusions
The present study offers several significant findings. Firstly, our results indicate that serving as a family decision-maker has a negative impact on residents’ health status, with family decision-makers experiencing a 1.58% decrease in their health status compared to other family members. Secondly, household decision-makers are exposed to higher stress levels, which is the main reason behind their poorer health status. Thirdly, we found that the effect of family decision-makers’ health status on residents’ health is not uniform. For example, in samples with higher net assets, the family decision-maker’s health status is relatively weak. In contrast, in samples with high housing, education, and medical expenditure pressures, the negative impact of the family decision-maker’s health status is more significant. Finally, our study also shows that individual or family socioeconomic status can mitigate the adverse health effects associated with being a family decision-maker to some extent.
Data Sharing Statement
Publicly available datasets were analyzed in this study. The data can be found at: https://opendata.pku.edu.cn/dataverse/CFPS.
Ethics Approval and Informed Consent
The studies involving human participants were reviewed and approved by the School of Business at Hunan University of Science and Technology. Informed consent was obtained from all respondents prior to their participation in the study. Additionally, this research was conducted in compliance with the standards outlined in the Declaration of Helsinki for human research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Science Foundation of China (Project No. 42101172) and the Hunan Provincial Philosophy and Social Science Foundation (Project No. 22YBA133).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Grossman M. On the concept of health capital and the demand for health. J Political Econ. 1972;80(2):223–255. doi:10.1086/259880
2. Fuhrer R, Sa S. How gender affects patterns of social relations and their impact on health: a comparison of one or multiple sources of support from “close persons”. Soc sci med. 2002;54(5):811–825. doi:10.1016/S0277-9536(01)00111-3
3. Liu J, Rozelle S, Xu Q, Yu N, Zhou T. Social engagement and elderly health in china: evidence from the china health and retirement longitudinal survey (CHARLS). Int J Environ Res Public Health. 2019;16(2):278. doi:10.3390/ijerph16020278
4. Pr Z, Liu Y. The higher the children’s achievements, the better the elderly health? Evidence from China. Front Public Health. 2022;10:10.
5. Zhuori N, Cai Y, Yan Y, Cui Y, Zhao M. Does social support affect the health of the elderly in rural China? A meta-analysis approach. Int J Environ Res Public Health. 2019;16(18):3471. doi:10.3390/ijerph16183471
6. Case A, Fertig A, Paxson C. The lasting impact of childhood health and circumstance. J Health Econommic. 2005;24(2):365–389. doi:10.1016/j.jhealeco.2004.09.008
7. Wang D. Reduction but not elimination: health inequalities among urban, migrant, and rural children in China-The moderating effect of the fathers’ education level. BMC Public Health. 2019;19(1):1219. doi:10.1186/s12889-019-7522-6
8. Richards D, Ph C, Go H. Impact of social media on the health of children and young people. J Paediatr Child Health. 2015;51(12):1152–1157. doi:10.1111/jpc.13023
9. Kawachi I. A glossary for health inequalities. J Epidemiol Community Health. 2002;56(9):647–652. doi:10.1136/jech.56.9.647
10. Na A, Thangiah N, Tt S, Ha M. Does a low-income urban population practise healthy dietary habits? International Health. 2018;10(2):108–115. doi:10.1093/inthealth/ihy001
11. Cai W, Deng Y, Zhang Q, Yang H, Huo X. Does income inequality impair health? Evidence from rural China. Agriculture. 2021;11(3):203. doi:10.3390/AGRICULTURE11030203
12. Yin H, Wu Q, Cui Y, et al. Socioeconomic status and prevalence of chronic non-communicable diseases in Chinese women: a structural equation modelling approach. BMJ Open. 2017;7(8):e014402. doi:10.1136/bmjopen-2016-014402
13. Wu S. The health impact of household cooking fuel choice on women: evidence from China. Sustainability. 2021;13(21):12080. doi:10.3390/SU132112080
14. Abbas K, Xu D, Li S, Baz K. Health implications of household multidimensional energy poverty for women: a structural equation modeling technique. Energy Build. 2021;234:110661. doi:10.1016/J.ENBUILD.2020.110661
15. J-y L, K-c L, S-y K, H-r P, Y-j K, B-h J. Oral health status of the disabled compared with that of the non-disabled in Korea: a propensity score matching analysis. PLoS One. 2019;14(1):e0208246. doi:10.1371/journal.pone.0208246
16. Me H, Sainio P, Parikka S, Koskinen S. The effects of the COVID-19 pandemic on the psychosocial well-being of people with disabilities. Disabil Health J. 2022;15(2):101224. doi:10.1016/J.DHJO.2021.101224
17. Mitchell RJ, Ryder T, Matar K, Lystad RP, Clay‐Williams R, Braithwaite J. An overview of systematic reviews to determine the impact of socio-environmental factors on health outcomes of people with disabilities. Health Soc Care Commun. 2022;30(4):1254–1274. doi:10.1111/HSC.13665
18. Chiappori P, Fortin B, Lacroix G. Marriage market, divorce legislation, and household labor supply. J Political Econ. 2002;110(1):37–72. doi:10.1086/324385
19. Epel ES, Blackburn EH, Lin J, et al. Accelerated telomere shortening in response to life stress. Proc Natl Acad Sci. 2004;101(49):17312–17315. doi:10.1073/pnas.0407162101
20. Kf F, Mm F. Utility of health data from social surveys: is there a gold standard for measuring morbidity? Am Sociological Rev. 1999;64(2):303–315. doi:10.2307/2657534
21. Darviri C, Ak A, Tigani X, Ec A. Lifestyle and self-rated health: a cross-sectional study of 3,601 citizens of Athens, Greece. BMC Public Health. 2011;11(1):619. doi:10.1186/1471-2458-11-619
22. Bian Z, Qu X, Ying H, Liu X. Are COVID-19 mitigation measures reducing preterm birth rate in China? BMJ Global Health. 2021;6(8):e006359. doi:10.1136/bmjgh-2021-006359
23. Yue D, Chen X, Zhu Y, Macinko J, Meng Q. Reductions in under-5 mortality and public health improvements of the China healthy cities (Counties) initiative: a nationwide quasi-experimental study. BMJ Global Health. 2022;7(3):e007154. doi:10.1136/bmjgh-2021-007154
24. Card D, Dobkin C, Maestas N. Does medicare save lives?*. Q J Econ. 2009;124(2):597–636. doi:10.1162/QJEC.2009.124.2.597
25. Brown S, Taylor K, Wheatley PS. Debt and distress: evaluating the psychological cost of credit. J Economic Psych. 2005;26(5):642–663. doi:10.1016/j.joep.2005.01.002
26. Bridges S, Disney R. Debt and depression. J Health Econommic. 2010;29(3):388–403. doi:10.1016/j.jhealeco.2010.02.003
27. Gathergood J. Debt and depression: causal links and social norm effects*. Econ J. 2012;122(563):1094–1114. doi:10.1016/j.jhealeco.2010.02.003
28. Valles SA. A pluralistic and socially responsible philosophy of epidemiology field should actively engage with social determinants of health and health disparities. Synthese. 2021;198(10):2589–2611. doi:10.1007/s11229-019-02161-5
29. Bg L, Phelan J. Social conditions as fundamental causes of disease. J Health Social Behav. 1995;Spec No:80–94. doi:10.2307/2626958
30. Me H, Waite LJ. Health in household context: living arrangements and health in late middle age. J Health Social Behav. 2002;43(1):1–21. doi:10.2307/3090242
31. Foster H, Polz P, Mair F, Gill J, Ca O. Understanding the influence of socioeconomic status on the association between combinations of lifestyle factors and adverse health outcomes: a systematic review protocol. BMJ Open. 2021;11(5):e042212. doi:10.1136/bmjopen-2020-042212
32. Singh-Manoux A, Mg M, Ne A. Does subjective social status predict health and change in health status better than objective status? Psych med. 2005;67(6):855–861. doi:10.1097/01.psy.0000188434.52941.a0
33. Sakurai K, Kawakami N, Yamaoka K, Ishikawa H, Hashimoto H. The impact of subjective and objective social status on psychological distress among men and women in Japan. Soc sci med. 2010;70(11):1832–1839. doi:10.1016/j.socscimed.2010.01.019
34. Puig-Barrachina V, Malmusi D, Jm M, Benach J. Monitoring social determinants of health inequalities: the impact of unemployment among vulnerable groups. Int J Health Serv. 2011;41(3):459–482. doi:10.2190/HS.41.3.d
35. Davies J, McKenna M, Bayley J, Denner K, Young H. Using engagement in sustainable construction to improve mental health and social connection in disadvantaged and hard to reach groups: a new green care approach. J Ment Health. 2020;29(3):350–357. doi:10.1080/09638237.2020.1714001
36. Chen J, Hao S, Wu Y. Housing and health in vulnerable social groups: an overview and bibliometric analysis. Reviews Environ Health. 2022;37(2):267–279. doi:10.1515/reveh-2020-0167
37. Mehl KR. The medical model of “obesity” and the values behind the guise of health. Synthese. 2023;201(6):215. doi:10.1007/s11229-023-04209-z
38. Wang Q, Que YZ, Wan XY, Prevalence LCQ. Risk factors, and impact on life of female urinary incontinence: an epidemiological survey of 9584 women in a region of southeastern China. Risk Manage Healthc Policy. 2023;16:1477–1487. doi:10.2147/RMHP.S421488
39. Chen Q, Tian W, Zheng L, Li T. Safeguarding the right to health of the elderly in rural china: a legal analysis. Risk Manage Healthc Policy. 2023;16:1621–1632. doi:10.2147/RMHP.S420954
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.