")
Back to Journals » Journal of Healthcare Leadership » Volume 15
Headache Education by E-Learning Through Social Networking Services (Social Media)
Authors Katsuki M , Nanri M, Miyakoshi Y, Gobo S, Koh A, Kawamura S, Tachikawa S, Matsukawa R, Kashiwagi K, Matsuo M, Yamagishi F
Received 24 July 2023
Accepted for publication 13 October 2023
Published 1 November 2023 Volume 2023:15 Pages 285—296
DOI https://doi.org/10.2147/JHL.S432132
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pavani Rangachari
Masahito Katsuki,1,2 Maiko Nanri,3 Yuki Miyakoshi,4 Shuto Gobo,4 Akihito Koh,2 Shin Kawamura,2 Senju Tachikawa,2 Ryo Matsukawa,2 Kenta Kashiwagi,5 Mitsuhiro Matsuo,6 Fuminori Yamagishi7
1Department of Neurosurgery and Headache Outpatient, Japanese Red Cross Suwa Hospital, Nagano, Japan; 2Department of Neurosurgery, Itoigawa General Hospital, Niigata, Japan; 3Nurse-Senka, SMS Corporation, Tokyo, Japan; 4Creatone, Regnition, Saitama, Japan; 5Department of Neurology, Itoigawa General Hospital, Niigata, Japan; 6Department of Anesthesiology, Toyama University Hospital, Toyama, Japan; 7Department of Surgery, Itoigawa General Hospital, Niigata, Japan
Correspondence: Masahito Katsuki, Department of Neurosurgery, Japanese Red Cross Suwa Hospital, 5-11-50, Kogandori, Suwa, Nagano, 392-0027, Japan, Tel/Fax +81-0266-52-6111, Email [email protected]
Introduction: Headache is a common public health problem, but its burden could be avoided by raising headache awareness and the appropriate use of acute medication and prophylactic medication. Few reports on raising headache awareness in the general public have been reported, and there are no reports on headache awareness campaigns through social networking services (SNS), or social media, in Japan. We prospectively performed a headache awareness campaign from March 2022 through 2 SNS, targeting nurse and wind instrumental musicians, because they are with high headache prevalence.
Methods: Through the 2 SNS, the article and video were distributed, respectively. The article and video described the 6 important topics for the general public about headaches, which were described in the Clinical Practice Guideline for Headache Disorders 2021. Just after reading or watching them as e-learning, we performed online questionnaire sheets to investigate the awareness of the 6 topics through the 2 SNS. The awareness of the 6 topics before and after the campaign was evaluated.
Results: In the SNS nurse-senka, we obtained 1191 responses. Women comprised 94.4%, and the median (range) age was 45 (20 to 71) years old. Headache sufferers were 63.8%, but only 35.1% had consulted doctors. In the SNS Creatone, we got the response from 134 professional musicians, with 77.3% of women. The largest number of respondents were in their 20s (range 18– 60 years old). Headache sufferers were 87.9%. Of them, 36.4% had consulted doctors, 24.2% were medication-overuse headache. The ratios of individuals who were aware of the 6 topics significantly increased from 15.2%-47.0% to 80.4– 98.7% after the online questionnaire in both SNS (p < 0.001, all).
Conclusion: E-learning and online survey via SNS can improve headache awareness.
Keywords: awareness, education, medication-overuse headache, migraine, online, prevention, social networking services, social media
Introduction
Migraine is a public health problem1–9 in addition to tension-type headache (TTH)10–12 and cluster headache,13–16 and it is described in the International Classification of Headache Disorders 3rd edition (ICHD-3).17 Migraine prevalence is 0.9–9.5%.8,9,18–25 The economic and social impacts of migraine on productivity are starting to be recognized.24,26,27 Presenteeism accounts for 89% of productivity losses associated with migraines. In a four-year study of approximately 8000 employees in the US healthcare system, 22 prevalent health problems were examined for prevalence and their effects on productivity. Migraine was found to be the second most common reason for presenteeism, costing the employer about US$2 million annually.28 Migraine headaches, a disease with such high economic losses, have become preventable in recent years. Novel drugs, such as calcitonin gene-related peptide (CGRP)-related drugs, for migraine are now widely used.4,29–34 They have made migraine a fully preventable disease. Still, there was an unmet need for migraine care: 89.8% of respondents had never taken preventative medicine for headaches, and 36.5% had been hesitant to consult doctors.9,35 Most headache sufferers presumably manage the pains by taking over-the-counter (OTC) medicines.36,37 Additionally, when people with headaches consult a doctor, only neuroimaging is done to rule out organic or emergent disorders, and the diagnostic for a detailed primary headache and its treatment is inadequate. Even when diagnosing primary headaches, clinicians lack the necessary treatment understanding, which leaves patients dissatisfied.36 Inappropriately using OTC medications and insufficient headache medical resources may result in chronic migraine and medication-overuse headache (MOH).38–41 Before developing chronic migraine and MOH, appropriate preventative drugs can be used,14,15,31,32,42–45 but headache patients do not consult doctors.
By promoting headache awareness46 and the appropriate use of acute medication and preventative medication, this significant public health issue could be averted. Raising headache awareness not only among headache sufferers who routinely consult doctors but also among the general public, including headache sufferers who never come to the hospital and non-headache sufferers, is important. Many methods have been used to educate the general population about diseases, not just headaches.47–49 However, few reports on raising headache awareness of headaches in people without headaches have been reported.26,28,38,50,51 In this context, we prospectively ran a headache awareness campaign using social networking sites (SNS) as we call it in Japan, or social media, and assessed the effects of the campaign on SNS users, including both those who already had headaches and those who did not necessarily have them.
Materials and Methods
Campaign Procedure
This headache awareness campaign was held by Itoigawa General Hospital in March 2022, in partnership with SMS Corporation and Regnition. The leading target groups were nurses and wind instrumental musicians because headaches are common in nurses25,52–59 and wind instrumental musicians.60 About the former, shift workers tend to have migraine due to dysregulation of circadian rhythms.61 Migraine has a higher prevalence in workers with night shifts.62 Regarding the latter, the cultural association between music and migraine has been examined in the past.63 Also, sound hypersensitivity is often comorbid with migraine,64 and the relationship between music talent and migraine was also investigated.65 There are major SNS for nurses and wind instrumental musicians in Japan. The former one is called “nurse-senka” (https://knowledge.nurse-senka.jp/), with 1 million nurse users and 4 million page views per month. The latter one is called “Creatone” (https://www.creatone.jp/), on which more than 3000 users and professional musicians can communicate with professional musicians, and they can learn and be taught by professionals online or by e-learning videos.
This campaign emphasizes 6 important topics based on the Clinical Practice Guideline for Headache Disorders 202136 (Table 1). An article in SNS nurse-senka (https://knowledge.nurse-senka.jp/500343) and a video in SNS Creatone (https://www.youtube.com/watch?v=tkfOALn5vGU) were created, explaining the 6 topics. The article and video were made available to all users on the two SNS. Immediately after reading or viewing them as e-learning, we conducted online questionnaires to ascertain how well-versed users were in the 6 themes (Table 1) via the 2 SNS. The users read and answered them online of their own free will. We did not force any participation or answers. After a month, we again asked the users to answer the same online survey sheet and measured the awareness ratio of the 6 topics. The users did not acquire any honorarium and responded on a voluntary basis. We also asked, “why most headache sufferers do NOT consult doctors?” as choice questions.
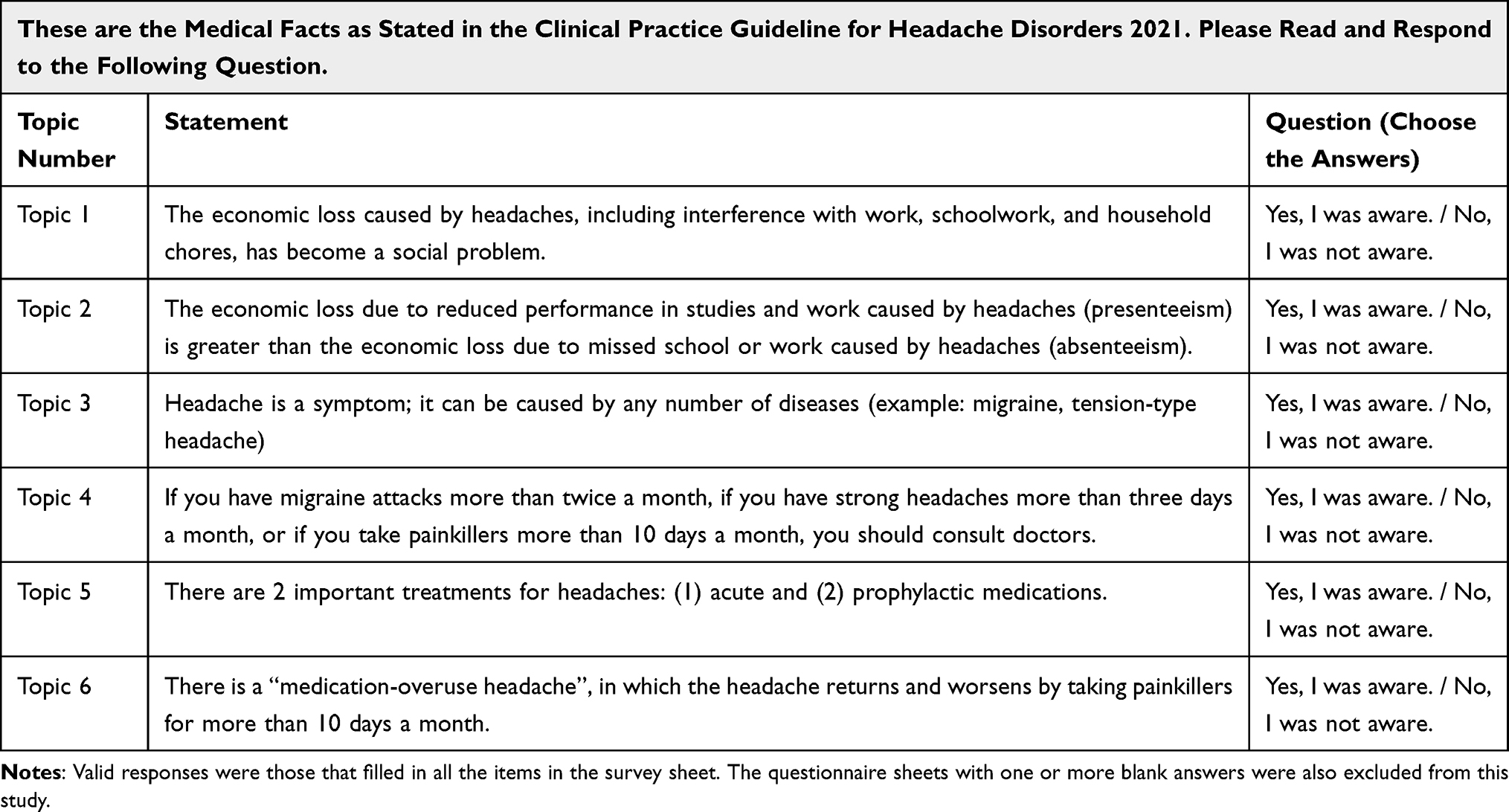 |
Table 1 Topics and Survey Sheet |
Age and headache characteristics were also collected, and headache and MOH diagnoses were made in the same way in the previous studies.18–20 The questionnaire was developed through Google Forms, and the questionnaire sheet consisted of the following items: age, sex, how many days per month a headache occurs in these 3 months or no headaches, whether your headache has been examined and diagnosed by a doctor, what acute medication you use, how many days per month you use the acute medication, use of prophylactic medication for headache, and what prophylactic medication you use. In the valid respondents, cases with headaches within the last 3 months were considered headaches sufferers. MOH was defined by referring to the ICHD-3 [2]. A case of MOH was defined as a respondent who had headaches ≥15 days per month and reported intake of non-opioid analgesic, such as acetaminophen and loxoprofen, ≥15 days per month, combination analgesic (most OTC medicines) or triptan ≥10 days per month. These case definitions approximate Criteria A and B of the ICHD-3 diagnostic criteria for MOH (code 8.2).
Google Forms can access the questionnaires. One for Creatone (https://docs.google.com/forms/d/1052wI3nn7o14_dpMVB53tkEpRrdWJxRtu323cfHZ6jQ/edit) and one for Nurse-Senka cannot be public for the company’s reasons.
Statistical Methods
Before and after the online questionnaire, the percentage of people who were aware of the six topics was compared using a Chi-square test. Statistical significance was determined as a two-tailed p 0.050. Version 28.0.0 of SPSS was utilized; it was made by IBM in New York, USA. No Bonferroni correction was used.66
Ethical Aspects
Itoigawa General Hospital Ethics Committee approved this study (approval number 2022–2, 2022–3). There were no names or other personally identifying information in the anonymous survey. The volunteers were given a copy of the online survey form that detailed the study’s objectives. If they wanted to take part in the study, they had to fill out the survey form. They were allowed not to participate if they did not want to do so by being asked to submit a blank sheet or not to try. The users did not acquire any honorarium and responded on a voluntary basis. All procedures were carried out following the Helsinki Declaration. To protect patient privacy, all identifiable patient data was removed from the database.
Results
We received 1191 responses to the SNS nurse-senka. The median (range) age was 45 (20 to 71) years old, and women made up 94.4% of the population. Only 35.1% of the 63.8% of headache sufferers had seen a doctor. One hundred and thirty-four professional musicians responded to the SNS Creatone survey, with 77.3% of them being female. The majority of responders (range: 18–60 years old) were in their 20s. There were 87.9% headache sufferers. Of them, 36.4% had seen doctors, 24.2% were MOH, and 75.9% reported that their headaches had interfered with their music performance as professionals.
Following the online survey in both SNS, the ratios of people who were aware of the six themes considerably climbed from 15.2% to 47.0% to 80.4 to 98.7% (p < 0.001, all) (Table 2). After one month, the nurse-senka group appeared to have a higher level of understanding than the Creatone group.
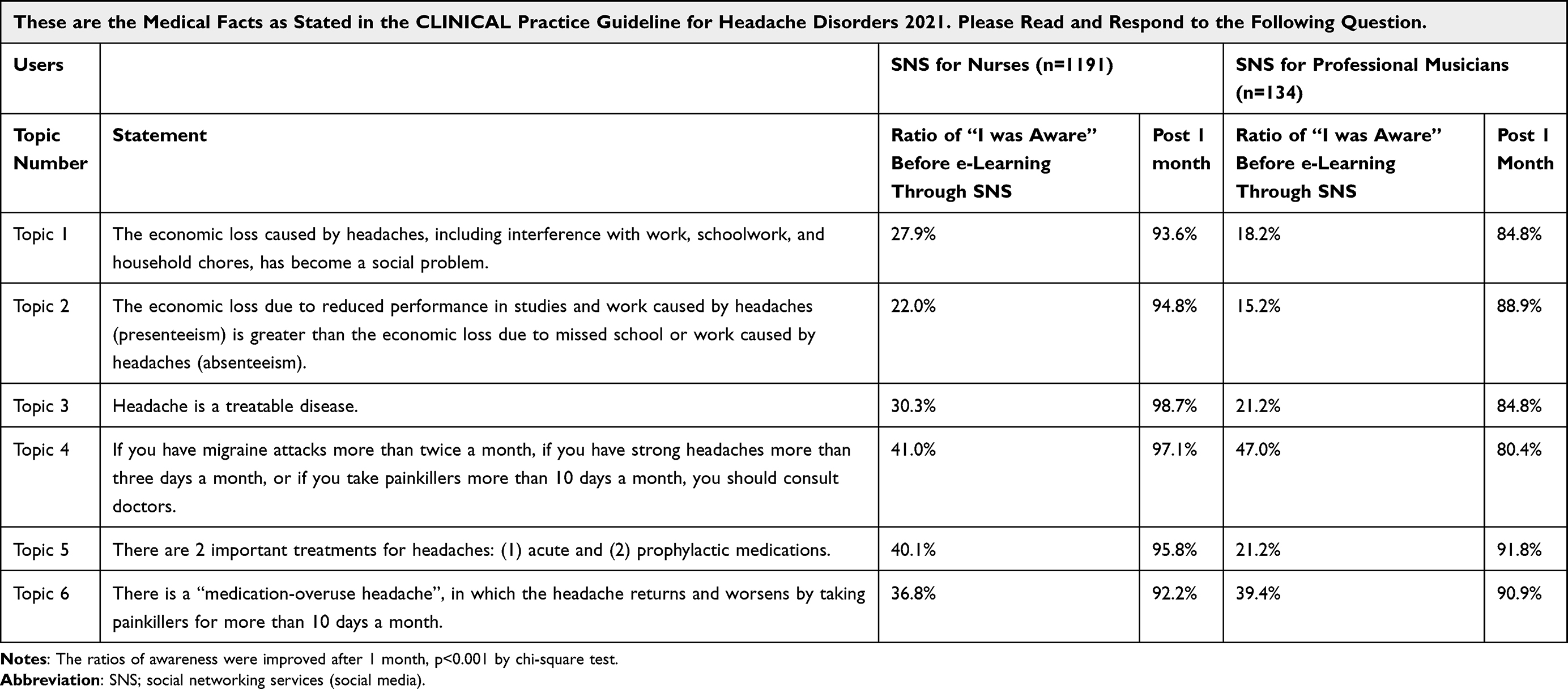 |
Table 2 Survey Results Through Social Networking Services for Nurses and Professional Musicians |
Table 3 displays the results of the survey question, “Why do most headache sufferers NOT consult doctors?” The results seemed similar in both groups. In nurse-senka, the most answered reasons were because taking time off from work or school to see a doctor would cause inconvenience to others, because I cannot take time to visit a hospital during the daytime on weekdays, and because over-the-counter medicines are sufficient, in order. Those in Creatone were because I do not think headaches are sick enough to go to the hospital, Because over-the-counter medicines are sufficient, and because my headache will go away if I just persevere, in order.
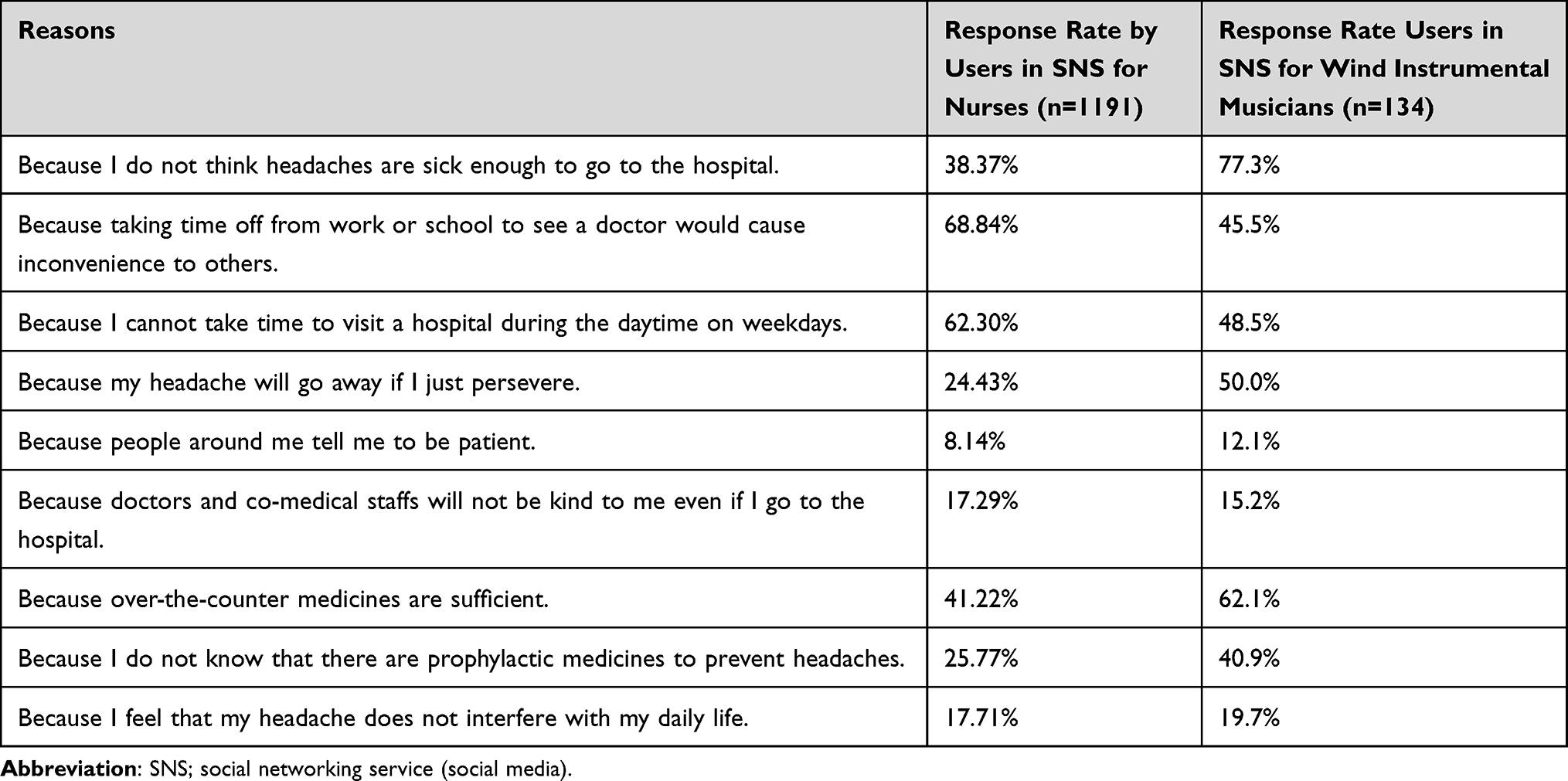 |
Table 3 The Questionnaire Results of “Why Most Headache Sufferers Do NOT Consult Doctors?” |
This awareness-raising led four of the nurses working at Japanese Red Cross Suwa Hospital to visit the headache out patients at the hospital. They are treated with prophylactic medication by our headache specialists.
Discussion
Through two SNSs, we ran this campaign to raise awareness about headaches. After the e-learning and online survey, the ratios of people who were aware of the six themes dramatically rose (p<0.001, all). According to our findings, online surveys and e-learning could increase SNS users’ awareness of headaches.
Previous Awareness Campaign
In March 2004, the World Health Organization and the Global Campaign against Headache jointly launched the initiative.67 The campaign was conceptualized in 3 steps; 1) Knowledge for awareness, 2) Awareness for action, and 3) Action for change. The details are described in Table 4. This campaign is still well underway around the world, and epidemiological surveys and educational projects for healthcare providers were conducted.2,68–71
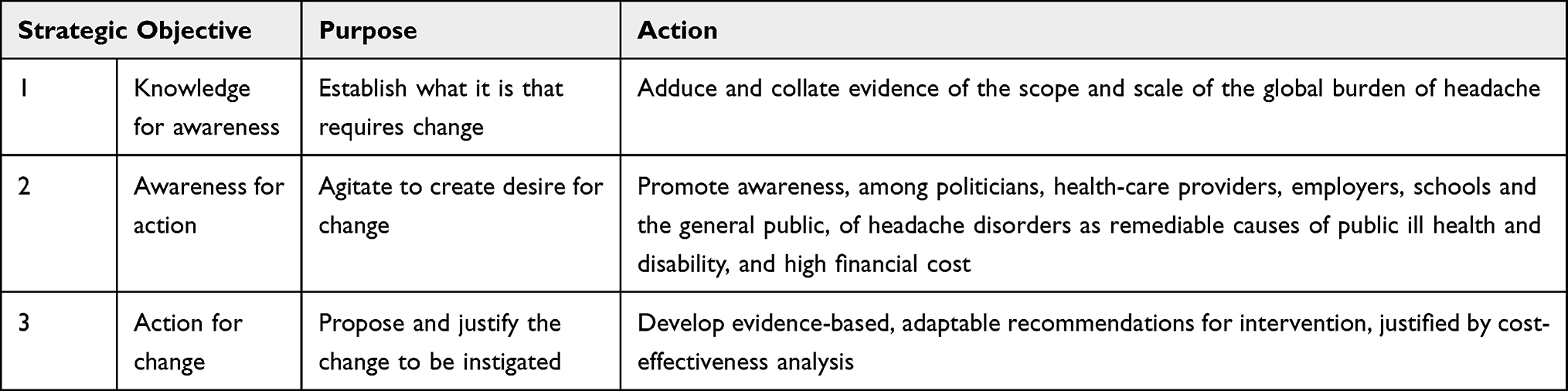 |
Table 4 The Three Strategic Objectives of the Global Campaign Against Headache |
A national MOH awareness campaign,38 university education,51 public education,50 leaflet distribution at mass vaccinations, and e-learning through schools26 are the only campaigns that have been carried out to inform the general public about headaches, despite the fact that the education program for doctors and headache sufferers has been widely implemented. But not every campaign was successful.
In 2016, a Danish national awareness campaign for MOH was performed. The target audience included the general public, general practitioners, and pharmacists. The campaign achieved significant reach and engagement, with 297,000 views of online videos, distribution of campaign materials to all 400 pharmacies, dissemination of over 28,000 leaflets, radio and television coverage reaching large audiences, publication of numerous print media articles, presence on reputable websites and online news agencies, and scientific paper publications. A survey conducted after the campaign indicated an increase in public awareness of MOH from 31% to 38%. However, this was not statistically significant.38
Here Is a report on education at a university. Through social networking sites, Lai et al51 conducted a study of the University of Birmingham undergraduate students concerning MOH in 2014. A total of 485 respondents, with nearly half having medical training, answered the survey. 372 of the 485 respondents (or 76.7%) were uninformed of the potential for MOH from routine painkiller usage for a headache. After receiving information on MOH, 364 of the 485 respondents (75.1%) said they would use fewer analgesics or seek medical advice. Additionally, 397 out of 485 people (81.8%) said OTC analgesics should have a MOH warning on the label. Although small in scale, this report is an attempt to raise awareness among the general public and is similar to our research in that it uses the Internet.
A system of education for the general public, those who suffer from headaches, and medical personnel was developed in Yekaterinburg, Russia, in 2013. In this situation, the Russian Headache Research Society conducted public education through the media, focusing on the identification of various headache types, their causes and potential preventative measures, appropriate and inappropriate medication use, and when to seek professional assistance. The article does not discuss how education affects the general public, but given that the mass media participated and that the city has a population of more than 1.3 million, we assume it was a significant effort.50 Details are not available, but a follow-up report on the effectiveness of this awareness campaign is awaited.
Before this study, we conducted the Itoigawa Headache Awareness Campaign from August 2021 to June 2022, consisting of two main interventions, and assessed their effectiveness. The campaign targeted individuals aged 15–64 in the general public. Two main interventions were implemented, supported by additional smaller interventions. Intervention 1 involved distributing leaflets and administering paper-based questionnaires on headaches during COVID-19 vaccination. Intervention 2 included on-demand e-learning and online surveys conducted through schools. Both interventions focused on six key topics outlined in the Clinical Practice Guideline for Headache Disorders 2021. Data on awareness of the topics were collected before and after each intervention. We obtained 4016 valid responses from 6382 individuals who received vaccinations in intervention 1, and 2577 responses from 594 students and 1983 parents in intervention 2, reaching a total of 6593 participants (32.2% of the working-age population in Itoigawa city). The percentage of individuals aware of the six topics significantly increased after both main interventions, ranging from 6.6% (39/594) - 40.0% (1606/4016) to 64.1% (381/594) - 92.6% (1836/1983) (p < 0.001, all). Community-based interventions, particularly during mass vaccination events where residents gather, and school-based e-learning proved to be effective methods for raising headache awareness.26 Even under the coronavirus-2019 pandemic, the awareness campaign could be performed online.
One recent successful awareness campaign is a Japanese information technology company’s internal awareness campaign. Sakai and Igarashi et al28 performed a headache education and evaluation program in the workplace of the company from 2019 to 2022. A total of 73,432 employees from the company participated in the program, with 16.7% having migraine, 40.7% experiencing TTH, and 0.5% having cluster headaches. Following the training and education, 82.9% of participants without headaches expressed a change in their attitude towards colleagues with headache disorders, and 72.5% reported an improved understanding of headaches. The educational program increased awareness of the impact of headaches on people’s lives, with the proportion of employees recognizing its significance rising from 46.8% to 70.6%. Additionally, 4.1% of participants expressed interest in virtual consultations with headache specialists, and over half of them had not previously sought medical advice for their headaches. The program resulted in an annual productivity gain of approximately 14.7 days per employee with headaches, leading to a cost-saving of $4531 per employee. These positive outcomes emphasize the value of workplace programs for migraine across all industries. As these tangible improvements in economic losses are being reported, it is essential to continue to disseminate correct information about headaches.
Thus, there are successful and unsuccessful awareness-raising activities. Further discussion is needed to determine what methods are best in the future. Instead of using mass media, consumer-generated media like weblogs and SNS have been utilized in the current complicated media ecosystem.72,73 Due to the possibility that those who do not have headaches are not interested in the burden of headaches, we assume that passively educating the general public through the media has no impact. Therefore, this headache awareness was conducted using the SNS consisting of user groups that would potentially have a high headache prevalence. Our campaigns were not mandatory; we asked for free-will participation on the SNS. We aimed to recruit as many participants as possible by targeting a population with a high headache prevalence and by explaining the 6 topics in a way that was easy to understand for nurses and wind instrumental musicians on each SNS. We may need to devise further ways to increase participation in the future, such as advertisements and point programs.
Importance of Early Medical Consultation
The notion that migraine is a progressive disease is being proposed.74,75 It is estimated that episodic migraine progresses to chronic migraine at a rate of 2.5% per year and may be underestimated due to the arbitrary 15-day period according to the migraine criteria.76 Key clinical features of migraine progression include progressive increases in the number and intensity of attacks, autonomic disturbance, and allodynia, leading to chronic migraine over time.77 Pathophysiologically, changes in hypothalamic activity, as one of the hypothesized generators of migraine,78 and diminished brainstem inhibitory process79 have been estimated as the main progression mechanisms. The factors related to migraine progression are the high frequency of migraine attacks, medication overuse, comorbid pain syndromes, and obesity.74 About 30% of chronic migraine is refractory to both preventive and acute treatment.36 Although CGRP-related agents have been reported to be effective in chronic migraine,80–84 their response rate is not comparable to that of episodic migraine. Therefore, early consultation and treatment are needed before the migraine progresses to chronic migraine.
Hirata et al85 used epidemiological surveys and questionnaires. They found that 14–38% of headache patients did not visit a hospital because of the effectiveness of OTC medicines. In contrast, some patients first visited a doctor because OTC had become ineffective (48/691, 6.9%) or because their headaches had increased in frequency (55/691, 8.0%). Also, prophylactic treatment is not well performed in Japan,9,35 and patients who would make their physicians have thought to prescribe prophylactic treatments aggressively and for whom early prophylactic treatment is prescribed may have already begun to develop chronicity from the initial consultation. If so, further educational efforts26,38 should be made, and patients should be seen while they have relatively mild episodic migraine. Also, for such severe patients, the new CGRP-related drugs can perform therapeutic effects.80,86–91 Further data accumulation is needed.
In clinical practice, patient education is important, but the long-term perspective is difficult, and patients often drop out and receive multiple medical services.92 Patients who consult multiple doctors may lack trust in their doctors and doctor-shop. It will be necessary in the future to build trust between doctors and patients and to plan treatment based on shared decision-making.93,94 As a starting point, disseminating information through social networking sites such as this one may be an easy way to spread a little correct knowledge.
Future Plan
We mention future prospects. Under the COVID-19 pandemic, our headache awareness campaign can be performed without face-to-face communication to avoid infection. Also, our materials used for awareness-raising can be installed into smartphone applications of headache diary95,96 and further dissemination and spread on SNS, which had a significant impact. Furthermore, with rapid digital transformations such as online telemedicine,97,98 treatment devices99 and electronic headache diaries as smartphone applications,95,96,100 and artificial intelligence diagnosis,101 it should be crucial to raise awareness because it will be more efficient and effective. Considering that migraine sufferers tend to be younger, this awareness campaign may be even more accepted.
Furthermore, the biopsychosocial approach to migraine and headache management will have therapeutic effects.102 Today, pharmaceutical therapies are the mainstay of migraine and headache treatment. However, because they are complex diseases, it is crucial to adopt a comprehensive strategy to address, in each person, every aspect that affects the disease’s effects and helps to prevent a long-term worsening course. In addition to pharmacological strategies, proper education about headaches, physical therapy, and massage are essential to treatment. These non-pharmacological treatments can be learned through SNS. Finally, SNS can become a place for users suffering from headaches to exchange information and learn from each other, which may lead to social care.102 Until now, patients have had the opportunity to exchange information with each other in person and to receive education from doctors.46 However, with the advancement of digitalization, social care may be created in environments such as SNS and metaverse.103
Limitations
We herein described limitations. This campaign was performed in specific SNS, so user demographics are skewed and may be difficult to generalize for all SNSs in Japan as well as other countries. Additionally, because of the data-gathering strategy used, our study may contain responder bias. As a result, the outcomes might not have represented all users. Distributing information through SNS is sometimes difficult because some users are not accustomed to using smartphones or SNS. Also, shown by the low survey collection rate, there is a possibility that some users may have ignored the campaign and survey without engaging in it. The disadvantage is the low participation rate instead of easy dissemination of information. The ratio of headache sufferers seemed high among the responders in this study. However, we did not specify the headache types among the 2 groups since this was a preliminary attempt to provide information for preventing MOH. We should specify the headache types in the next campaign in SNS. Additionally, a significant percentage of those who had no interest in headaches abstained from the e-learning and survey. It may also have been a result of worsening headaches from gazing at the screen of smartphones or computers.85,104–108 Furthermore, the review of information retention is very short at one month. We confirmed the educational effect of this campaign but could not confirm that this awareness effect was retained until, for example, 12 months. Lastly, the most important issue is the prevention of medication overuse. If this could be shown, our approach would be one route to tap into an even larger audience and work towards improving and maintaining self-management skills over the longer term. Based on the experience and reflection obtained from this study and our preliminary experience in raising awareness in the community,26 we are currently considering an awareness campaign for hundreds of thousands of people with large municipalities and companies.
Conclusions
This headache awareness campaign was carried out via online surveys and e-learning through two social networking sites. This is so because certain user groups on the SNS may have a high prevalence of headaches. One month after e-learning, the ratios of people who were aware of the six themes related to headaches dramatically increased (p<0.001, all). Our findings imply that online surveys and e-learning can raise headache awareness. The campaign’s elements can be added to mobile applications and further disseminated on social media, having a significant impact. Raising awareness will be more efficient and effective in the age of rapid digital innovations, such as online telemedicine and artificial intelligence diagnosis, and it should be a priority.
Acknowledgments
We are thankful to all medical staff.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Leonardi M. Burden of migraine: what should we say more? Neurol Sci. 2015;36(Suppl S1):1–3. doi:10.1007/s10072-015-2188-z
2. Stovner LJ, Hagen K, Linde M, Steiner TJ. The global prevalence of headache: an update, with analysis of the influences of methodological factors on prevalence estimates. J Headache Pain. 2022;23(1):34. doi:10.1186/s10194-022-01402-2
3. Vos T, Lim SS, Abbafati C, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–1222. doi:10.1016/S0140-6736(20)30925-9
4. Hashimoto Y, Komori M, Tanji Y, Ozeki A, Hirata K. Lasmiditan for single migraine attack in Japanese patients with cardiovascular risk factors: subgroup analysis of a Phase 2 randomized placebo-controlled trial. Expert Opin Drug Saf. 2022. doi:10.1080/14740338.2022.2078302
5. Suzuki K, Takeshima T, Igarashi H, et al. Impact of the COVID-19 pandemic on migraine in Japan: a multicentre cross-sectional study. J Headache Pain. 2021;22(1):53. doi:10.1186/s10194-021-01263-1
6. Takeshima T, Sakai F, Hirata K, et al. Erenumab treatment for migraine prevention in Japanese patients: efficacy and safety results from a Phase 3, randomized, double-blind, placebo-controlled study. Headache. 2021;61(6):927–935. doi:10.1111/head.14138
7. Hirata K, Sakai F, Takeshima T, et al. Efficacy and safety of erenumab in Japanese migraine patients with prior preventive treatment failure or concomitant preventive treatment: subgroup analyses of a phase 3, randomized trial. J Headache Pain. 2021;22(1):110. doi:10.1186/s10194-021-01313-8
8. Hirata K, Ueda K, Komori M, et al. Comprehensive population-based survey of migraine in Japan: results of the ObserVational Survey of the Epidemiology, tReatment, and Care Of MigrainE (OVERCOME [Japan]) study. Curr Med Res Opin. 2021;37(11):1945–1955. doi:10.1080/03007995.2021.1971179
9. Matsumori Y, Ueda K, Komori M, et al. Burden of Migraine in Japan: results of the ObserVational Survey of the Epidemiology, tReatment, and Care Of MigrainE (OVERCOME [Japan]) Study. Neurol Ther. 2022;11(1):205–222. doi:10.1007/s40120-021-00305-9
10. Suzuki N, Ishikawa Y, Gomi S, et al. Prevalence and characteristics of headaches in a socially active population working in the Tokyo metropolitan area -surveillance by an industrial health consortium. Internal Med. 2014;53(7):683–689. doi:10.2169/internalmedicine.53.1700
11. Shibata Y. [Clinical analysis of the patients with tension-type headache in whom kakkontou is effective] (Japanese). J Neurosurgery Kampo Med. 2019;5:16–18.
12. Fujimoto T, Sato T, Sato R, Ohtaki K, Asai J, Hokata H. [Treatment of tension-type headache with kakkon-to associated with guidance of a way of life] (Japanese). Pain kampo med. 2001;11:9–13.
13. Imai N, Yagi N, Kuroda R, Konishi T, Serizawa M, Kobari M. Clinical profile of cluster headaches in Japan: low prevalence of chronic cluster headache, and uncoupling of sense and behaviour of restlessness. Cephalalgia. 2011;31(5):628–633. doi:10.1177/0333102410391486
14. Imai N. [New management of cluster headache] (Japanese). Brain Nerve. 2021;73(4):347–355. doi:10.11477/mf.1416201766
15. Imai N. A cluster headache responsive to ramelteon, a selective melatonin MT1/MT2 receptor agonist. Intern Med. 2016;55(17):2483–2485. doi:10.2169/internalmedicine.55.6621
16. Imai N, Kitamura E. Differences in clinical features of cluster headache between drinkers and nondrinkers in Japan. PLoS One. 2019;14(11):e0224407. doi:10.1371/journal.pone.0224407
17. Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders. Cephalalgia. 2018;38(1):1–211. doi:10.1177/0333102417738202
18. Katsuki M, Kawahara J, Matsumori Y, et al. Questionnaire-based survey during COVID-19 vaccination on the prevalence of elderly’s migraine, chronic daily headache, and medication-overuse headache in one Japanese city—Itoigawa Hisui Study. J Clin Med. 2022;11(16):4707. doi:10.3390/jcm11164707
19. Katsuki M, Matsumori Y, Kawahara J, et al. School-based online survey on chronic headache, migraine, and medication-overuse headache prevalence among children and adolescents in Japanese one city - Itoigawa Benizuwaigani study. Clin Neurol Neurosurg. 2023;226:107610. doi:10.1016/j.clineuro.2023.107610
20. Katsuki M, Yamagishi C, Matsumori Y, et al. Questionnaire-based survey on the prevalence of medication-overuse headache in Japanese one city-Itoigawa study. Neurol Sci. 2022;43:3811–3822. doi:10.1007/s10072-021-05831-w
21. Takeshima T, Ishizaki K, Fukuhara Y, et al. Population-based door-to-door survey of migraine in Japan: the Daisen Study. J Head Face Pain. 2004;44(1):8–19. doi:10.1111/j.1526-4610.2004.04004.x
22. Sakai F, Igarashi H. Prevalence of migraine in Japan: a nationwide survey. Cephalalgia. 1997;17(1):15–22. doi:10.1046/j.1468-2982.1997.1701015.x
23. Goto M, Yokoyama K, Nozaki Y, et al. Characteristics of headaches in Japanese elementary and junior high school students: a school-based questionnaire survey. Brain Dev. 2017;39(9):791–798. doi:10.1016/j.braindev.2017.05.010
24. Shimizu T, Sakai F, Miyake H, et al. Disability, quality of life, productivity impairment and employer costs of migraine in the workplace. J Headache Pain. 2021;22(1):29. doi:10.1186/s10194-021-01243-5
25. Nadaoka T, Kanda H, Oiji A, Morioka Y, Kashiwakura M, Totsuka S. Headache and stress in a group of nurses and government administrators in Japan. Headache. 1997;37(6):386–391. doi:10.1046/j.1526-4610.1997.3706386.x
26. Katsuki M, Matsumori Y, Kawahara J, et al. Headache education by leaflet distribution during COVID‐19 vaccination and school‐based on‐demand e‐learning: itoigawa Geopark Headache Awareness Campaign. J Head Face Pain. 2023;63(3):429–440. doi:10.1111/head.14472
27. Takeshima T, Wan Q, Zhang Y, et al. Prevalence, burden, and clinical management of migraine in China, Japan, and South Korea: a comprehensive review of the literature. J Headache Pain. 2019;20(1):111. doi:10.1186/s10194-019-1062-4
28. Sakai F, Igarashi H, Yokoyama M, et al. Diagnosis, knowledge, perception, and productivity impact of headache education and clinical evaluation program in the workplace at an information technology company of more than 70,000 employees. Cephalalgia. 2023;43(4):3331024231165682. doi:10.1177/03331024231165682
29. Ambat FDF, Bentivegna E, Martelletti P. Novel migraine therapies may reduce public and personal disadvantages for people with migraine. BioDrugs. 2022;36(3):337–339. doi:10.1007/s40259-022-00532-y
30. Serra López-Matencio JM, Gago-Veiga AB, Gómez M, et al. Treatment of migraine with monoclonal antibodies. Expert Opin Biol Ther. 2022;22(6):707–716. doi:10.1080/14712598.2022.2072207
31. Sakai F, Suzuki N, Kim BK, et al. Efficacy and safety of fremanezumab for episodic migraine prevention: multicenter, randomized, double-blind, placebo-controlled, parallel-group trial in Japanese and Korean patients. Headache. 2021;61(7):1102–1111. doi:10.1111/head.14178
32. Sakai F, Takeshima T, Homma G, Tanji Y, Katagiri H, Komori M. Phase 2 randomized placebo-controlled study of lasmiditan for the acute treatment of migraine in Japanese patients. Headache. 2021;61(5):755–765. doi:10.1111/head.14122
33. Scheffler A, Schenk H, Wurthmann S, et al. CGRP antibody therapy in patients with drug resistant migraine and chronic daily headache: a real-world experience. J Headache Pain. 2021;22(1):111. doi:10.1186/s10194-021-01323-6
34. Ruscheweyh R, Broessner G, Goßrau G, et al. Effect of calcitonin gene-related peptide (-receptor) antibodies in chronic cluster headache: results from a retrospective case series support individual treatment attempts. Cephalalgia. 2020;40(14):1574–1584. doi:10.1177/0333102420949866
35. Takeshima T, Ueda K, Komori M, et al. Potential unmet needs in acute treatment of migraine in Japan: results of the OVERCOME (Japan) study. Adv Ther. 2022;39(11):5176–5190. doi:10.1007/s12325-022-02289-w
36. Headache Clinical Practice Guideline Development Committee C. 2021. [Clinical Practice Guideline for Headache Disorders 2021] (Japanese). Japanese Society of Neurology J, Japanese Headache Society J, Japanese Society of Neurological Therapeutics J, eds) Igaku-Shoin.
37. Ozeki K, Noda T, Nakamura M, Ojima T. Weather and headache onset: a large-scale study of headache medicine purchases. Int J Biometeorol. 2015;59(4):447–451. doi:10.1007/s00484-014-0859-8
38. Carlsen LN, Westergaard ML, Bisgaard M, Schytz JB, Jensen RH. National awareness campaign to prevent medication-overuse headache in Denmark. Cephalalgia. 2018;38(7):1316–1325. doi:10.1177/0333102417736898
39. Silberstein SD, Lipton RB, Dodick DW. Operational diagnostic criteria for chronic migraine: expert opinion. Headache. 2012;54(7):1258–1266. doi:10.1111/head.12407
40. Togha M, Karimitafti MJ, Ghorbani Z, et al. Characteristics and comorbidities of headache in patients over 50 years of age: a cross-sectional study. BMC Geriatr. 2022;22(1):1–10. doi:10.1186/s12877-022-03027-1
41. Huang L, Bourke D, Ranta A. The impact of an online adult headache guideline on headache referrals to the neurology clinic. Intern Med J. 2021;51(8):1251–1254. doi:10.1111/imj.14959
42. Ito Y, Mitsufuji T, Asano Y, et al. Naratriptan in the prophylactic treatment of cluster headache. Intern Med. 2017;56(19):2579–2582. doi:10.2169/internalmedicine.8865-17
43. Odaguchi H, Wakasugi A, Ito H, et al. The efficacy of goshuyuto, a typical Kampo (Japanese herbal medicine) formula, in preventing episodes of headache. Curr Med Res Opin. 2006;22(8):1587–1597. doi:10.1185/030079906X112769
44. Mitsufuji T, Yamamoto T, Miyake A, et al. [Use of yokukansan for the treatment of headaches caused by medication overuse, second report: effectiveness of administering only yokukansan] (Japanese). J Japanese Assoc Oriental Psychosomatic Medicine. 2014;29(1):84–87.
45. Mitsufuji T, Yamamoto T, Hayashi Y, Mizoi Y, Tamura N, Araki N. [Use of yokukansan for the treatment of medication overuse headache] (Japanese). J Japanese Assoc Oriental Psychosomatic Medicine. 2013;28(1):47–49.
46. Sakai F. Beat the stigma of primary headache disorders: activities of JPAC and GPAC. Neurol Clin Neurosci. 2020;8(3):128–131. doi:10.1111/ncn3.12374
47. Ohyama S, Yokota C, Miyashita F, et al. Effective education materials to advance stroke awareness without teacher participation in junior high school students. J Stroke Cerebrovasc Dis. 2015;24(11):2533–2538. doi:10.1016/j.jstrokecerebrovasdis.2015.07.001
48. Hino T, Yokota C, Nishimura K, et al. Spreading awareness of stroke through school-based education: a pooled analysis of three community-based studies. J Stroke Cerebrovasc Dis. 2018;27(7):1810–1814. doi:10.1016/j.jstrokecerebrovasdis.2018.02.008
49. Matsuzono K, Yokota C, Takekawa H, et al. Effects of stroke education of junior high school students on stroke knowledge of their parents: Tochigi project. Stroke. 2015;46(2):572–574. doi:10.1161/STROKEAHA.114.007907
50. Lebedeva ER, Olesen J, Osipova VV, Volkova LI, Tabeeva GR, Steiner TJ. The Yekaterinburg headache initiative: an interventional project, within the Global Campaign against Headache, to reduce the burden of headache in Russia. J Headache Pain. 2013;14:101. doi:10.1186/1129-2377-14-101
51. Lai JTF, Dereix JDC, Ganepola RP, et al. Should we educate about the risks of medication overuse headache? J Headache Pain. 2014;15:10. doi:10.1186/1129-2377-15-10
52. Nagai K, Hayashi K, Yasui T, et al. Disease history and risk of comorbidity in women’s life course: a comprehensive analysis of the Japan Nurses’ Health Study baseline survey. BMJ Open. 2015;5(3):e006360. doi:10.1136/bmjopen-2014-006360
53. Chen SJ, Chen CH, Chang HY. Effects of inhaling essential oil on headache-related quality of life among nurses working in emergency and critical care units. Hu Li Za Zhi. 2021;68(5):51–64. doi:10.6224/JN.202110_68(5).08
54. Diao T, Zhu J, Yu L, Ma X. Correlation analysis of vestibular symptoms and migraine and non-migraine headaches: an epidemiological survey of 708 female nurses. Front Neurosci. 2022;16:925095. doi:10.3389/fnins.2022.925095
55. Durham CF, Alden KR, Dalton JA, et al. Quality of life and productivity in nurses reporting migraine. Headache. 1998;38(6):427–435. doi:10.1046/j.1526-4610.1998.3806427.x
56. Menon B, Remadevi N. Migraine in nursing students-A study from a tertiary care center in South India. J Neurosci Rural Pract. 2021;12(1):129–132. doi:10.1055/s-0040-1721556
57. Viticchi G, Falsetti L, Pettinari P, Provinciali L, Silvestrini M, Bartolini M. Headache in a population of hospital workers. Neurol Sci. 2014;35(Suppl 1):157–158. doi:10.1007/s10072-014-1759-8
58. Bartolini M, Viticchi G, Falsetti L, et al. Migraine in health workers: working in a hospital can be considered an advantage? Neurol Sci. 2014;35(Suppl 1):27–29. doi:10.1007/s10072-014-1737-1
59. Wang Y, Xie J, Yang F, et al. The prevalence of primary headache disorders and their associated factors among nursing staff in North China. J Headache Pain. 2015;16:4. doi:10.1186/1129-2377-16-4
60. Hasegawa M, Kawai H, Nishiwaki K, et al. [The outbreak situation of the physical symptom in the musical instrument exercise of the high school brass band club student] (Japanese). Ann Rep Faculty Rehabilitation Shijonawate Gakuen Univ. 2010;6:13–18.
61. Santos IS, Griep RH, Alves MGM, et al. Job stress is associated with migraine in current workers: the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil). Eur J Pain. 2014;18(9):1290–1297. doi:10.1002/j.1532-2149.2014.489.x
62. Sandoe CH, Sasikumar S, Lay C, Lawler V. The impact of shift work on migraine: a case series and narrative review. Headache. 2019;59(9):1631–1640. doi:10.1111/head.13622
63. Roberts DL, Vargas BB. The portrayal of migraine in popular music: observations and implications. Headache. 2012;52(7):1164–1170. doi:10.1111/j.1526-4610.2012.02159.x
64. Ishikawa T, Tatsumoto M, Maki K, Mitsui M, Hasegawa H, Hirata K. Identification of everyday sounds perceived as noise by migraine patients. Intern Med. 2019;58(11):1565–1572. doi:10.2169/internalmedicine.2206-18
65. Hassler M, Gupta D. Functional brain organization, handedness, and immune vulnerability in musicians and non-musicians. Neuropsychologia. 1993;31(7):655–660. doi:10.1016/0028-3932(93)90137-o
66. Rothman KJ. No adjustments are needed for multiple comparisons. Epidemiology. 1990;1(1):43–46.
67. Steiner TJ, Birbeck GL, Jensen RH, et al. The Global Campaign turns 18: a brief review of its activities and achievements. J Headache Pain. 2022;23(1):49. doi:10.1186/s10194-022-01420-0
68. Togha M, Rafiee P, Ghorbani Z, et al. The prevalence of headache disorders in children and adolescents in Iran: a schools-based study. Cephalalgia. 2022;42(11–12):1246–1254. doi:10.1177/03331024221103814
69. Kawatu N, Wa Somwe S, Ciccone O, et al. The prevalence of primary headache disorders in children and adolescents in Zambia: a schools-based study. J Headache Pain. 2022;23(1):118. doi:10.1186/s10194-022-01477-x
70. Luvsannorov O, Anisbayar T, Davaasuren M, et al. The prevalence of headache disorders in children and adolescents in Mongolia: a nationwide schools-based study. J Headache Pain. 2020;21(1):107. doi:10.1186/s10194-020-01175-6
71. Genc D, Vaičienė-Magistris N, Zaborskis A, et al. The prevalence of headache disorders in children and adolescents in Lithuania: a schools-based study. J Headache Pain. 2020;21(1):73. doi:10.1186/s10194-020-01146-x
72. Kohda T, Nagata H. 「複合メディア環境」におけるテレビ視聴者行動 [Survey on television viewers’ behavior under ‘complex media-environment’]. J Information Media Studies. 2012;11:15–31. Japanese. doi:10.11304/jims.11.15
73. Ministry of Internal Affairs and Communications M. Available from: [The Evolving Digital Economy and Beyond Society 5.0]. Japanese; 2019. https://www.soumu.go.jp/johotsusintokei/whitepaper/ja/r01/html/nd114120.html.
74. Rattanawong W, Rapoport A, Srikiatkhachorn A. Neurobiology of migraine progression. Neurobiol Pain. 2022;12:100094. doi:10.1016/j.ynpai.2022.100094
75. Natoli J, Manack A, Dean B, et al. Global prevalence of chronic migraine: a systematic review. Cephalalgia. 2010;30(5):599–609. doi:10.1111/j.1468-2982.2009.01941.x
76. Ishii R, Schwedt TJ, Dumkrieger G, et al. Chronic versus episodic migraine: the 15-day threshold does not adequately reflect substantial differences in disability across the full spectrum of headache frequency. Headache. 2021;61(7):992–1003. doi:10.1111/head.14154
77. Torres-Ferrús M, Quintana M, Fernandez-Morales J, Alvarez-Sabin J, Pozo-Rosich P. When does chronic migraine strike? A clinical comparison of migraine according to the headache days suffered per month. Cephalalgia. 2017;37(2):104–113. doi:10.1177/0333102416636055
78. Schulte LH, Allers A, May A. Hypothalamus as a mediator of chronic migraine: evidence from high-resolution fMRI. Neurology. 2017;88(21):2011–2016. doi:10.1212/WNL.0000000000003963
79. Aurora SK, Barrodale PM, Tipton RL, Khodavirdi A. Brainstem dysfunction in chronic migraine as evidenced by neurophysiological and positron emission tomography studies. Headache. 2007;47(7):996–1003. doi:10.1111/j.1526-4610.2007.00853.x.
80. Förderreuther S, Zhang Q, Stauffer VL, Aurora SK, Láinez MJA. Preventive effects of galcanezumab in adult patients with episodic or chronic migraine are persistent: data from the phase 3, randomized, double-blind, placebo-controlled EVOLVE-1, EVOLVE-2, and REGAIN studies. J Headache Pain. 2018;19(1):121. doi:10.1186/s10194-018-0951-2
81. Lambru G, Hill B, Murphy M, Tylova I, Andreou AP. A prospective real-world analysis of erenumab in refractory chronic migraine. J Headache Pain. 2020;21(1):61. doi:10.1186/s10194-020-01127-0
82. McAllister P, Cohen JM, Campos VR, Ning X, Janka L, Barash S. Impact of fremanezumab on disability outcomes in patients with episodic and chronic migraine: a pooled analysis of phase 3 studies. J Headache Pain. 2022;23(1):112. doi:10.1186/s10194-022-01438-4
83. Barbanti P, Egeo G, Aurilia C, et al. Fremanezumab in the prevention of high-frequency episodic and chronic migraine: a 12-week, multicenter, real-life, cohort study (the FRIEND study). J Headache Pain. 2022;23(1):46. doi:10.1186/s10194-022-01396-x
84. Nahas SJ, Naegel S, Cohen JM, et al. Efficacy and safety of fremanezumab in clinical trial participants aged ≥60 years with episodic or chronic migraine: pooled results from 3 randomized, double-blind, placebo-controlled phase 3 studies. J Headache Pain. 2021;22(1):141. doi:10.1186/s10194-021-01351-2
85. Hirata K, Sano H, Kondo H, Shibasaki Y, Koga N. Clinical characteristics, medication use, and impact of primary headache on daily activities: an observational study using linked online survey and medical claims data in Japan. BMC Neurol. 2023;23(1):80. doi:10.1186/s12883-023-03122-9
86. Igarashi H, Shibata M, Ozeki A, Day KA, Matsumura T. Early onset and maintenance effect of galcanezumab in Japanese patients with episodic migraine. J Pain Res. 2021;14:3555–3564. doi:10.2147/JPR.S326905
87. Katsuki M, Kashiwagi K, Kawamura S, Tachikawa S, Koh A. One-time use of galcanezumab or fremanezumab for migraine prevention. Cureus. 2023;15(1):e34180. doi:10.7759/cureus.34180
88. Tatsuoka Y, Takeshima T, Ozeki A, Matsumura T. Treatment satisfaction of galcanezumab in Japanese patients with episodic migraine: a phase 2 randomized controlled study. Neurol Ther. 2021;10(1):265–278. doi:10.1007/s40120-021-00236-5
89. Silberstein SD, Stauffer VL, Day KA, Lipsius S, Wilson MC. Galcanezumab in episodic migraine: subgroup analyses of efficacy by high versus low frequency of migraine headaches in phase 3 studies (EVOLVE-1 & EVOLVE-2). J Headache Pain. 2019;20(1):75. doi:10.1186/s10194-019-1024-x
90. Ito Y, Mitsufuji T, Okada M, et al. Early effect of calcitonin gene-related peptide monoclonal antibodies in migraine with medication overuse: a single-center retrospective study. Intern Med. 2023. doi:10.2169/internalmedicine.1471-22
91. Ihara K, Ohtani S, Watanabe N, et al. Predicting response to CGRP-monoclonal antibodies in patients with migraine in Japan: a single-centre retrospective observational study. J Headache Pain. 2023;24(1):23. doi:10.1186/s10194-023-01556-7
92. Lau JTF, Yu A, Cheung JCK, Leung SSF. Studies on common illnesses and medical care utilization patterns of adolescents in Hong Kong. J Adolescent Health. 2000;27(6):443–452. doi:10.1016/S1054-139X(99)00075-0
93. Urtecho M, Wagner B, Wang Z, et al. A qualitative evidence synthesis of patient perspectives on migraine treatment features and outcomes. Headache. 2023;63(2):185–201. doi:10.1111/head.14430
94. Biagianti B, Grazzi L, Gambini O, et al. Decision-making deficit in chronic migraine patients with medication overuse. Neurol Sci. 2012;33(Suppl 1):S151–5. doi:10.1007/s10072-012-1071-4
95. Kato Y, Poh W, Horvath Z, Cadiou F, Shimazu T, Maruki Y. Impact of COVID-19 pandemic on migraine management in the United States: insights from migraine tracking app users. BMC Neurol. 2021;21(1):345. doi:10.1186/s12883-021-02378-3
96. Katsuki M, Tatsumoto M, Kimoto K, et al. Investigating the effects of weather on headache occurrence using a smartphone application and artificial intelligence: a retrospective observational cross-sectional study. Headache. 2023.
97. Sasaki R, Yunoki T, Nakano Y, et al. Actual telemedicine needs of Japanese patients with neurological disorders in the COVID-19 pandemic. Intern Med. 2023;62(3):365–371. doi:10.2169/internalmedicine.9702-22
98. Katsuki M. The first case series from Japan of primary headache patients treated by completely online telemedicine. Cureus. 2022;14(11):e31068. doi:10.7759/cureus.31068
99. Parlongue G, Cerdan EV, Koenig J, Williams DP. Smartphone based music intervention in the treatment of episodic migraine headaches - A pilot trial. Complement Ther Med. 2021;63:102779. doi:10.1016/j.ctim.2021.102779
100. Jonker L, Fitzgerald L, Vanderpol J, Fisher S. Digital diary app use for migraine in primary care: prospective cohort study. Clin Neurol Neurosurg. 2022;216:107225. doi:10.1016/j.clineuro.2022.107225
101. Katsuki M, Narita N, Matsumori Y, et al. Preliminary development of a deep learning-based automated primary headache diagnosis model using Japanese natural language processing of medical questionnaire. Surg Neurol Int. 2020;11:475. doi:10.25259/SNI_827_2020
102. Rosignoli C, Ornello R, Onofri A, et al. Applying a biopsychosocial model to migraine: rationale and clinical implications. J Headache Pain. 2022;23(1):100. doi:10.1186/s10194-022-01471-3
103. Adusumilli G, Kallmes KM, Kobeissi H, Kallmes DF, Heit JJ. Into the meta-verse: the decade of global knowledge sharing. Interv Neuroradiol. 2023;15910199231154704. doi:10.1177/15910199231154704
104. Berry PA. Migraine disorder: workplace implications and solutions. AAOHN J. 2007;55(2):51–56. doi:10.1177/216507990705500202
105. Yamakawa M, Tachibana A, Tatsumoto M, Okajima K, Ueda S, Hirata K. Hemodynamic responses related to intrinsically photosensitive retinal ganglion cells in migraine. Neurosci Res. 2020;160:57–64. doi:10.1016/j.neures.2019.11.011
106. Dahal HN, Kharel Sitaula R. Visual impact of digital classroom among students attending online education. J Nepal Health Res Counc. 2022;20(2):405–411. doi:10.33314/jnhrc.v20i02.4041
107. Tatsumoto M, Suzuki E, Nagata M, Suzuki K, Hirata K. Prophylactic treatment for patients with migraine using blue cut for night glass. Intern Med. 2022. doi:10.2169/internalmedicine.0132-22
108. Horiguchi H, Suzuki E, Kubo H, et al. Efficient measurements for the dynamic range of human lightness perception. Jpn J Ophthalmol. 2021;65(3):432–438. doi:10.1007/s10384-020-00808-2
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.