")
Back to Journals » Nutrition and Dietary Supplements » Volume 15
Gut Microbiota Composition in Indian and Western Infants (0–24 Months): A Systematic Review
Authors Veeraraghavan B, Kesavelu D , Yadav B
Received 22 December 2022
Accepted for publication 24 March 2023
Published 6 April 2023 Volume 2023:15 Pages 25—46
DOI https://doi.org/10.2147/NDS.S402256
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Gary Johanning
Balaji Veeraraghavan,1 Dhanasekhar Kesavelu,2 Bijesh Yadav1
1Christian Medical College, Vellore, Tamil Nadu, 632004, India; 2SS Child Care, Mogappair, West Chennai, 600037, India
Correspondence: Balaji Veeraraghavan, Christian Medical College, Vellore, Tamil Nadu, 632004, India, Tel +919442210555, Email [email protected]
Abstract: Gut microbiota starts colonizing from birth and reach the adult gut microbial profile by around three years of age. There are scarce data on the gut microbial profiles of Indian infants. Moreover, there are insufficient data comparing the types of gut microbiota in Indian and Western infants, at different stages of their growth between 0 and 24 months. Also, with increasing globalization, infants of one country of origin are born in another country or travel to another country during infancy. Hence, these infants are exposed to changing environment and food practices that often causes dysbiosis or imbalance in the healthy gut microbiota profile. Dysbiosis has been linked, directly or indirectly, with many neurodevelopmental, gastrointestinal, respiratory, and other health issues. Early probiotic supplementation is associated with the return to the gut microbiota profile to a healthy state at one year and beyond. The changing global scenarios warrant the availability of a probiotic that can be used across nations. However, this is possible only if the gut microbiota profile of Indian and Western infants is similar enough to encourage the use of same probiotic in both populations. Hence, a systematic literature search was carried out to assess if the microbiota profile of the Indian and Western infants was comparable. This systematic review included 29 studies (10 Indian and 19 Western) and found that despite some differences, the gut microbiota of Indian and Western infants aged 0– 24 months are largely similar, with implications for probiotic supplementation.
Keywords: gut microbiota, Indian, Western, 0.24 months, infants
Introduction
Gut microbiota start colonizing from birth and reach the adult gut microbial profile by around three years of age.1 The terminology ‘gut microbiota’ includes bacteria, archaea, eukarya, microeukaryotes, viruses, fungi, and protozoans colonizing the gastrointestinal tract.2–4 However, the significance of archaea, eukarya and microeukaryotes in infants (0–24 months) is not well understood, and these microbiota are either reported as absent, transient, or detected in limited samples.3,5,6 Very few studies report appreciable presence of these microbiomes in infancy.7 On the other hand, bacteria constitute the major portion of gut microbiota during infancy and various taxonomic groups have been reported across studies.3,4,6,8
In a healthy infant, gut microbiota are in a state of eubiosis or harmonious commensulization towards formation of a healthy human gut.9 Right from the neonatal phase, gut microbiota play a major role metabolic (digestion and metabolism), protective (act as barrier against pathogenic microorganisms) and trophic (growth and differentiation of intestinal epithelial cells and immune system homeostasis) role.1,8,9
Any delay or disturbance in the development of the age appropriate healthy gut microbiota can lead to dysbiosis, defined as an imbalance between healthy commensal and pathogenic organisms leading to disease.1,8,10 The mode of delivery, vaginal (VD) or cesarean (CSD) is known to impact the diversity and colonization of gut microbiota and has a direct impact on infant health.11–13 Similarly, feeding practices (breastfed, bottle fed, weaning etc) affect the diversity and colonization of gut microbiota.14,15
Dysbiosis has been linked, directly or indirectly, with many neurodevelopmental, gastrointestinal, respiratory, and other health issues.8–10 Hence, it is important to prevent dysbiosis and correct it at the earliest. Probiotics are live microbiota (especially bacteria and yeast) given as a supplement to prevent and/or correct dysbiosis as they help in normalizing the gut microbiota towards eubiosis.10,16–19
Traditionally, Indians have been moving to Western world countries for better education, career and health prospects.20 Today, globalization has resulted in rampant movement of individuals from one country to another.21 The change in geographical location, local environment, diet patterns of mother and local weaning food and supplementary milk options can impact the colonization and diversity of gut microbiota in infants.14,15 Thus, these infants born in another country or travelling to another country are at risk of dysbiosis due to changes in their local environment.22 Hence, there is a need for probiotics that can correct dysbiosis across infants of different geographies. However, this is possible only if the gut microbiota profile of Indian and Western infants is similar enough to encourage the use of same probiotic in both populations.
In this context, little is known about the gut microbial profiles of Indian infants. Infant gut microbiota profiles from advanced Western world are abundant. However, data comparing the gut microbiota of Indian and Western infants is lacking.4 Hence, this systematic review was conducted to extract data on gut microbiota profile (gut bacterial profile) of Indian versus Western infant populations aged 0–24 months, compare their gut microbiota profile/composition, and assess if there are enough similarities between the gut microbiome of the two populations to encourage use of same probiotics for these infants. Since mode of delivery and feeding practices have been shown to impact the gut microbiome across geographies, we aimed to compare the gut microbiota of Indian and Western infants by mode of delivery and by feeding practices.
Methods
Aim
To compare the gut microbiota profile/composition of Indian versus the Western infants 0–24 months old. An additional aim was to see if there was any similarity between the gut microbiotas between the Indian and Western infants.
Protocol
This systematic literature review followed a pre-determined, non-registered protocol and was conducted in accordance with the ‘Preferred Reporting Items for Systematic Reviews and Meta-Analyses’ (PRISMA)23,24 guidelines. We included the articles that determined the gut microbiota of healthy Indian/Western well-nourished infants between the age of 0–24 months according to the predetermined inclusion/exclusion criteria. Even though the term “Western world” can mean different regions depending on the location of the index country, in general, the current understanding of Western world includes regions from America, Europe, Canada and Australia.25 Hence, the protocol clubbed all these countries under the “Western world” countries.
Bacteria can be classified in many ways. We used the Integrated Taxonomic Information System (IT IS) for the taxonomic classification of bacteria.26 In addition, information on the taxonomic classification was taken from the article included, if it was available.
Criteria for Including Studies
The systematic review included any clinical trial from India or Western world evaluating gut microbiota (bacteria) in healthy full-term, vaginally delivered or delivered by cesarean section, well-nourished infants aged 0–24 months. The mothers were healthy and not under any medication for any comorbid condition. Trials pulling gut microbiota data from longitudinal cohorts or population databases were included, but only the data for the 0–24 months age group was considered. Only those trials that extracted data on the fecal microbiota profile were included.
Criteria for Excluding Studies
The systematic review excluded clinical trials that evaluated the gut microbiota in preterm infants; malnourished infants; stunted infants; obese infants; or pediatric studies in age group above 24 months; or the evolution of gut microbiota during a disease, gastrointestinal disorder, neurological or metabolic disorder; or in response to an intervention (vaccine, synbiotics, supplements, antibiotics or probiotics), allergen, or a particular diet type (protein rich, carbohydrate rich, Mediterranean, etc.) Studies evaluating only oral microbiota and not fecal microbiota were also excluded. Studies reporting just the diversity index without specifying the individual bacteria, comparing Indian infants with infants of countries other than those covered under Western world, or studies analyzing the effects of different factors on the infant gut microbiota were also excluded.
Method of Literature Search and Selection of Articles
Free literature databases like MEDLINE (PubMed) were independently searched on August 1, 2022 by two investigators for English language human trials published between 1970 until July 31, 2022, using the following search terms (“infants”) AND (“gut” OR “intestinal” OR “fecal” OR “stool”) AND (“microbiota” OR “microflora” OR “microbiome”). A total of 2007 records were retrieved.
The two investigators (Dr Nidhi Gupta and Dr Kokil Mathur) independently screened the retrieved records for duplicates and removed the duplicates using a reference manager. The retrieved records were then analyzed for inclusion/exclusion by the title of the study and abstract, and then finally the 114 full texts were screened by them. The records being considered for inclusion during screening were segregated as Indian and Western depending on the country of the trial. A total of 104 were excluded after mutual discussion and deliberations.
Finally, the two investigators agreed to include 10 records through online search (two Indian and eight Western).
Since the number of retrieved studies were very few, the two investigators decided to supplement the search by manually sourcing the bibliography of the 42 excluded review articles and systematic reviews and meta-analysis and the Google Scholar. Nine studies meeting the inclusion criteria that were missed during the online search were added from the bibliography and 10 studies were added from Google Scholar.
Finally, of the 2017 records retrieved, 29 studies (10 Indian and 19 Western) met the inclusion criteria. Figure 1 outlines the detailed search and selection criteria of the records through the PRISMA flow chart. The studies were further segregated by mode of delivery and by feeding practices as outlined in the respective study inclusion criteria.
 |
Figure 1 PRISMA flow diagram for literature search and selection. Notes: Page MJ, Moher D, Bossuyt PM, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ;2021:n160. Creative Commons.24 |
The details of the 29 studies included in the systematic review are captured in Table 1. Of the 19 Western studies, 14 studies were from Europe,12,27–39 two were from America,6,40 two from Canada,41,42 and one from Australia43.
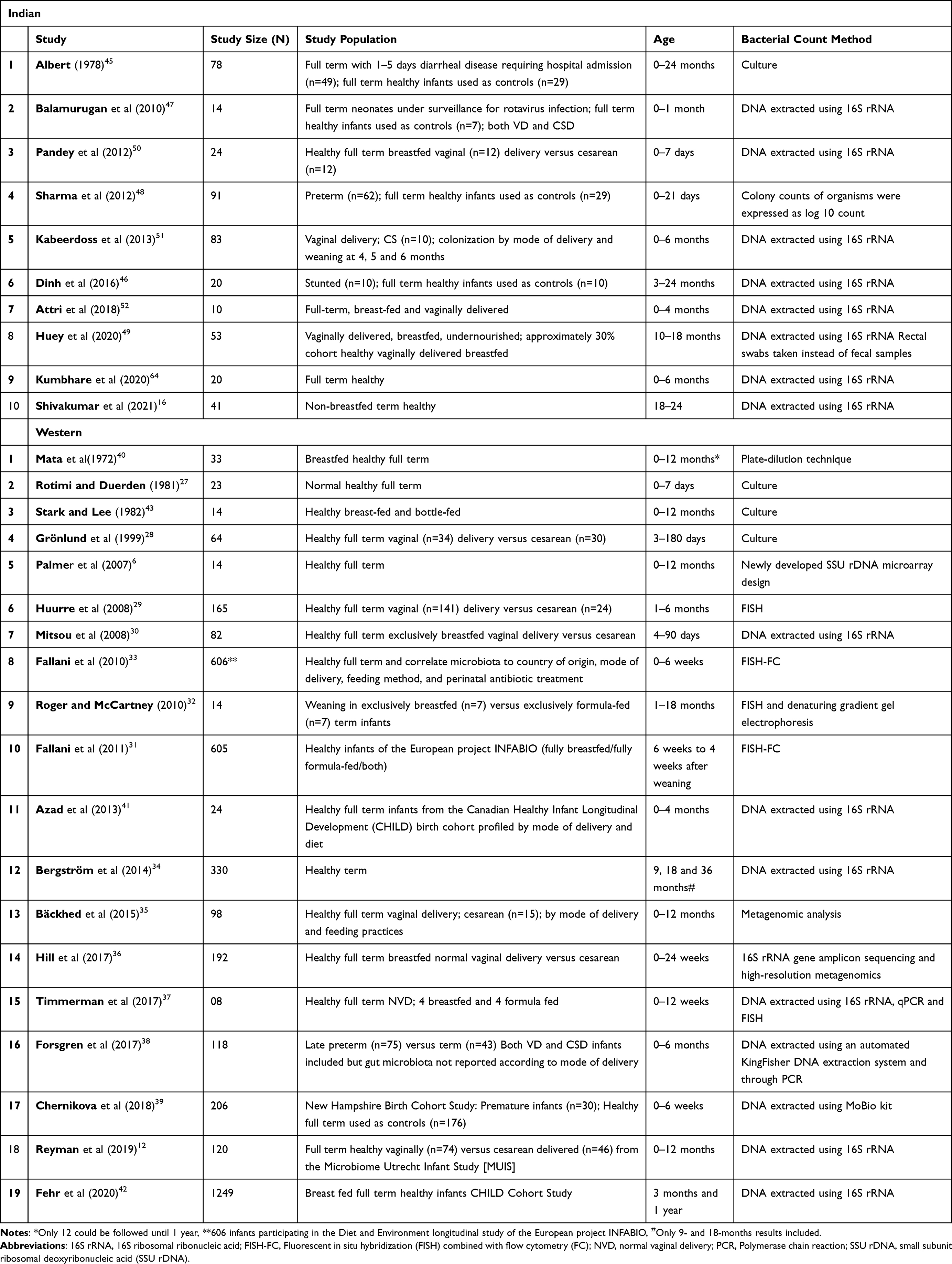 |
Table 1 Studies Included in the Systematic Review |
Quality of Evidence and Risk of Bias
Two researchers independently assessed the records using the Cochrane Collaboration’s tool for risk of bias assessment, which includes seven domains of bias stratifying the risk of bias as low, high or unclear.44 The two researchers then discussed their findings and resolved any discrepancy through discussion and consensus.
The scientific quality of individual studies included was generally high with well-designed methodology and statistical analysis. All the studies assessed the fecal microbiota in infants and clearly defined the technique used for assessing the microbiota. The infant age group, mode of delivery, and feeding practices were captured by most studies.
Data Analysis and Its Limitations
Despite the high quality of evidence of individual studies, proper statistical comparison and analysis of the studies could not be carried out due to many inconsistencies in the way the data was presented in different studies.
None of the studies compared the gut microbiota between Indian and Western infants (0–24 months). In five studies (Albert et al, Dinh et al, Sharma et al, Balamurugan et al, Chernikova et al)39,45–48 the healthy infants were not the main study population but were used as controls. The controls also differed by age as shown in Table 1. Similarly, there was no consistency in the age group considered by mode of delivery/breastfeeding/weaning as shown in Table 1. It is a known fact that the gut microbiome rapidly develops between birth and first two years of life,1 and therefore there can be marked difference in colonizations.
Further, though the method for assessing microbiota type and the bacterial count method were clearly described, the methods used across the studies were not consistent (Table 1). The various methods used were by both Indian and Western studies were culture, DNA extracted using 16S rRNA, colony counts of organisms were expressed as log 10 count, plate-dilution technique, small subunit ribosomal deoxyribonucleic acid (SSU rDNA) microarray design, fluorescent in situ hybridization (FISH), FISH combined with flow cytometry (FISH-FC), DNA extracted using MoBio kit, DNA extracted using an automated KingFisher DNA extraction system and through Polymerase chain reaction (PCR), DNA extracted using 16S rRNA, qPCR and FISH, 16S rRNA gene amplicon sequencing and high-resolution metagenomics, and metagenomic analysis. Different methods of identifying the microbiotas have their own sensitivity and specificity and thus their capability of identifying the microbiota differs. However, 14 of the 29 studies used the “DNA extracted using 16S rRNA” method and thus have the same sensitivity and specificity towards capturing the microbiota types.
The Western population was not consistent and included studies from Central America, USA, Canada, Australia, and Europe. However, 14 of the 19 studies from the Western world were from Europe, thereby ensuring that majority of the studies from the Western world were from the same region. We considered removing studies from Central America, USA, Canada, and Australia, but since a robust statistical analysis was not possible, and that there was not enough comparative European literature on gut microbiome by mode of delivery, breastfeeding and weaning practices, we decided to include these studies to understand if any inferences could be drawn regarding the similarities and differences between the gut microbiome of Indian and Western infants.
Of the two studies from America, the study by Mata et al was in indigenous Guatemalan children from Central America and the one by Palmer et al is from USA. Of the two studies from Canada, the study by Azad et al included healthy full-term infants from the Canadian Healthy Infant Longitudinal Development (CHILD) birth cohort profiled by mode of delivery and diet and the study by Fehr et al included breast fed full term healthy infants from the same CHILD Cohort Study. The study from Australia by Stark and Lee included healthy breast-fed and bottle-fed infants.
There was inconsistency in the granularity of taxonomical classification reported by the studies with as some studies reported the bacteria at phyla and family level only while other studies reported more granular data by genus and species. After extracting the data, we noted a great variation at species level between the two populations. Hence, we decided to compare the gut microbiota of the two populations at the genus level. However, we built the entire taxonomical tree (Figure 2) using the IT IS system for complete understanding.
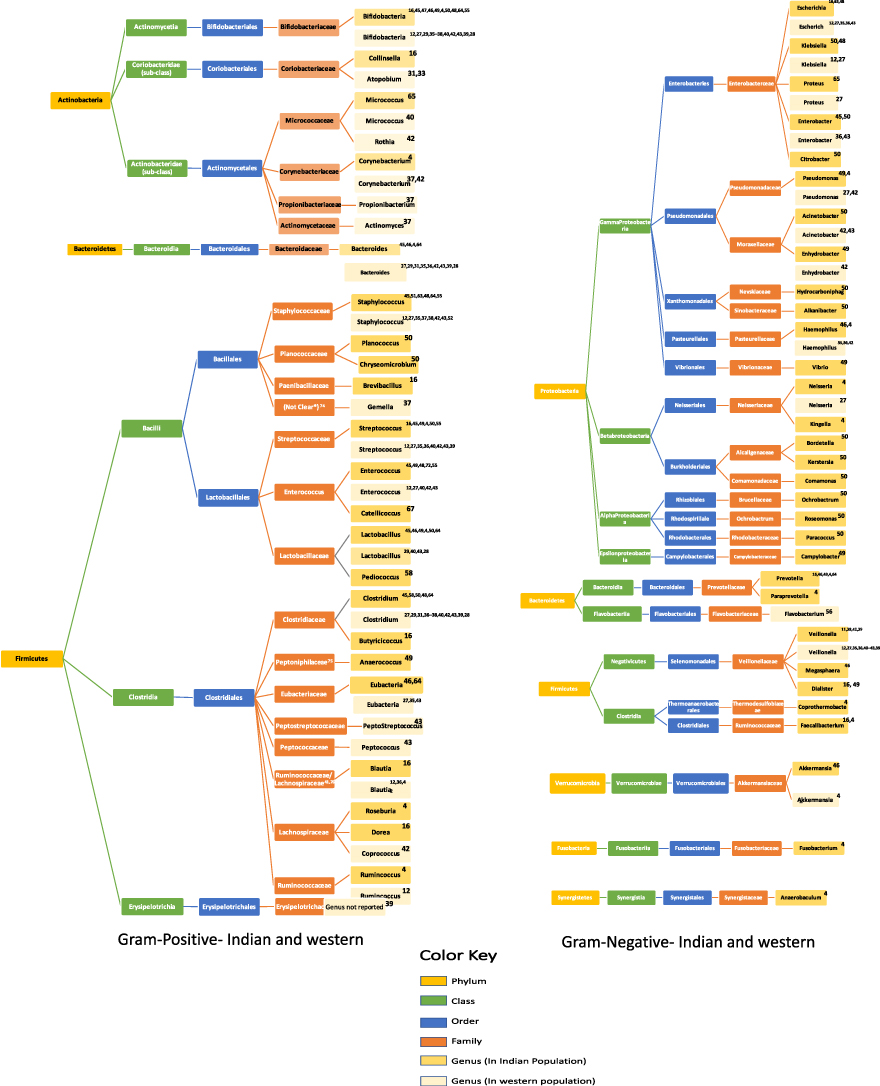 |
Figure 2 Gut microbiota according to different taxonomic groups in Indian versus Western infants. Notes: *The family of genus Gemella is not clear;65 Genus Anaerococcus is under family Peptoniphilaceae66 as per the source cited, family details were not available at Integrated Taxonomic Information System (IT IS) used by the systematic review to classify the microbiota; Genus Blautia is reported to be under two families: family Ruminococcaceae and family Lachnospiraceae.41,67 |
Therefore, due to differences in the methodology of microbiota classification, detection, and counting; differences in the country of origin; and inconsistency in age group captured in different studies by mode of delivery or feeding/weaning practices, the available data was described descriptively. The information extracted from the studies was discussed by the authors and synthesized with the goal to reach a logical conclusion.
Results
Gut Microbiota According to Different Taxonomic Groups in the Indian versus Western Population
Gut microbiota data from all the 29 studies (10 Indian and 19 Western) were available and captured in Figure 2.
Similarities in Gut Microbiota of Healthy Full-Term Indian and Western Infants
Gut microbiota of five phyla: Bacteroidetes, Firmicutes, Actinobacteria, Proteobacteria, Fusobacteria, and Verrucomicrobia, were present in both Indian and Western infants.
Proteobacteria and Firmicutes were the most represented phyla across both populations, followed by Actinobacteria.
Under the phylum Proteobacteria, order Gamma Proteobacteria was the most reported order with gram-negative Escherichia, Klebsiella, Proteus and Enterobacter reported across both populations. Genus Neisseria under the order Betabroteobacteria was reported in both the populations but by one Indian and one Western study only.
Under the phylum Firmicutes, both gram-positive and gram-negative bacteria were reported in both the populations. The orders Bacillales, Lactobacillales, and Clostridiales were present in both the Indian and Western infants. At the genus level, gram-positive Staphylococcus, Streptococcus, Enterococcus, Lactobacillus, Clostridium, Eubacteria and Blautia were reported by multiple studies for both Indian and Western infants. Of the gram-negative bacteria, genus Veillonella was reported by multiple Indian and Western studies.
Under the phylum Actinobacteria, all the classes and orders of bacteria were seen in both Indian and Western infants, with some variance in the family and genus level. The genus Bifidobacteria and Corynebacterium were reported in both Indian and Western infants, but Bifidobacteria was the most reported microbiota in both the populations by majority of the records.
Under the phylum Bacteroidetes, the gram-positive genus Bacteroides was the most reported microbiota for both Indian and Western infants. Under the phylum Verrucomicrobia, only one genus, Akkermansia, was reported, and seen in both Indian and Western infants.
Differences in Gut Microbiota of Healthy Full-Term Indian and Western Infants
Two phyla, Fusobacteria and Synergistetes were reported by Indian studies only.
Under the phylum Proteobacteria, orders Betabroteobacteria, Alpha Proteobacteria and Epsilon Proteobacteria were predominantly reported for Indian infants.
Under the phylum Firmicutes, the order Erysipelotrichales was reported in Western infants by one study only.
Under the phylum Actinobacteria, bacteria from two families (Propionibacteriaceae and Actinomycetaceae) under the order Actinomycetales were not seen in Indian infants.
Under the phylum Bacteroidetes, the gram-negative genus Prevotella and Paraprevotella were reported only in Indian infants.
Though there were differences at the genus level between the two populations, the different genus was usually reported by one Indian or Western study only (Figure 2).
Colony Percentages of Gut Microbiota in Indian versus Western Infants According to Different Taxonomic Groups
Total 11 of the 29 included studies reported gut microbiota colony counts. However, only eight (four Indian and four Western) studies reported the colony count as percentages and were included in the analysis. Three studies by Sharma et al, Kabeerdoss et al (both Indian) and Palmer et al (Western) reported colony counts by methods other than percentages and hence they were not included in the analysis of this section Sharma reported the microbiota count as mean log colony-forming unit (CFU) per gram, while Palmer and Kabeerdoss used rRNA gene copies in the range of 109 to 1010/g of stool (wet weight).
Similarities and Differences Reported at Phyla Level
When classified according to the phylum, it was seen that the colony percentage of Firmicutes (38.6–44.716,46 vs 32.01–43.86,41) and Bacteroidetes (13.8–18.916,46 vs 20.086) was similar in both the Indian and Western populations. The percentage range for the colony percentage of Firmicutes and Bacteroidetes was narrow. On the other hand, the Western infants showed almost double the highest colony percentage of Proteobacteria (46.14 vs 25.89) and Actinobacteria (36.4 vs 17.5) compared to the Indian population. However, the range of colony percentages for both Proteobacteria and Actinobacteria was very wide.
Similarities and Differences Reported at Class Level
Under the phylum Firmicutes, colony counts of classes Bacilli (9.266), Clostridia (19.976), and Mollicutes (2.796) were reported for only Western population and that too by one study only. Under the phylum Proteobacteria, bacterial count was reported for classes Gamma Proteobacteria (46.116) and Beta Proteobacteria (0.036) were reported by one Western study, and for order Aeromonadales (41.2949) was reported by one Indian study.
Similarities and Differences Reported at Family Level
Under the phylum Firmicutes, colony count for family Lachnospiraceae (8.616 vs 8–14.239,41) and Ruminococcaceae (8.516 vs 041) were reported for both Indian and Western infants, while bacterial count for family Erysipelotrichaceae was reported only for Western population (0.8–439,41).
Under the phyla Bacteroidetes and Actinobacteria bacterial count was reported for family Prevotellaceae (17.616) and Bifidobacteriaceae (816) respectively, by one Indian study only and the counts were not available for Western population.
Under the phylum Proteobacteria, bacterial count was reported for family Moritellaceae (1.1949) by one Indian study only and for family Enterobacterceae (7.4–2039,41) by two Western studies.
Similarities and Differences Reported at Genus Level
When classified according to the genus, Streptococcus, Veillonella, and Lactobacillus had similar colony percentage for both the population, while Western infants had a much higher percentage range of Bifidobacterium (15–4033,39,41 vs 0.57 −14.8516,46,48,49) and Bacteroides (11.4–1933,39 vs 6.0546) than Indian infants. Figure 3 shows the similarities and differences in bacterial count reported for both the populations.
 |
Figure 3 Colony percentages of gut microbiota in Indian and Western infants Indian; 16,46,48,49 Western6,33,39,41. |
Limitations Encountered While Comparing Colony Counts
Colony percentages of various other microbiota could not be compared due to lack of data for either Indian or Western colonization.
Further, a direct comparison of the colony percentages could not be made between Indian and Western infants as the studies had different probes for bacterial detection and included infants with different modes of delivery or feeding practices. Also, though all the infants were under 24 months, the gut microbiota profile was captured at different ages. Thus, a study could have reported a higher percentage of a particular microbiota during early infancy, which may have declined during later infancy resulting in a lower percentage being reported by another study.
Gut Microbiota in Indian versus Western Infants Classified According to Mode of Delivery
Table 2 and Table 3 compare the gut microbiota of infants during 0–24 months of life, classified according to the mode of delivery. Thirteen (four Indian and nine Western) studies met the inclusion criteria of reporting the gut microbiota by either mode of delivery or reported the gut microbiota in either VD or CSD infant population. There were no studies comparing the gut microbiota in Indian versus Western infants by mode of delivery. Only five studies (two Indian and three Western) compared the relative predominance of the gut microbiota by the mode of delivery in their respective population.30,33,41,50,51
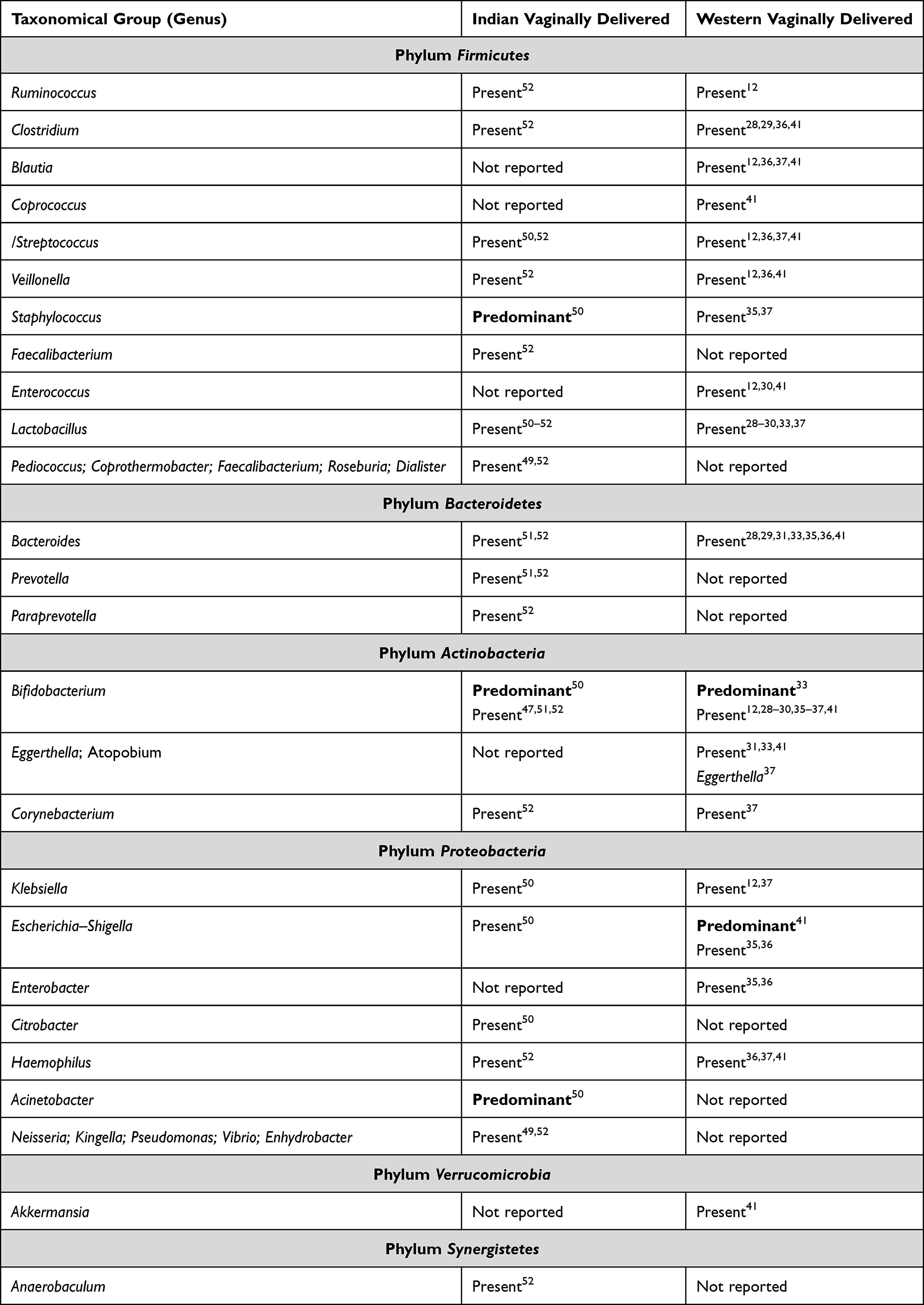 |
Table 2 Gut Microbiota (0–24 Months) in Indian and Western Vaginally Delivered Infants |
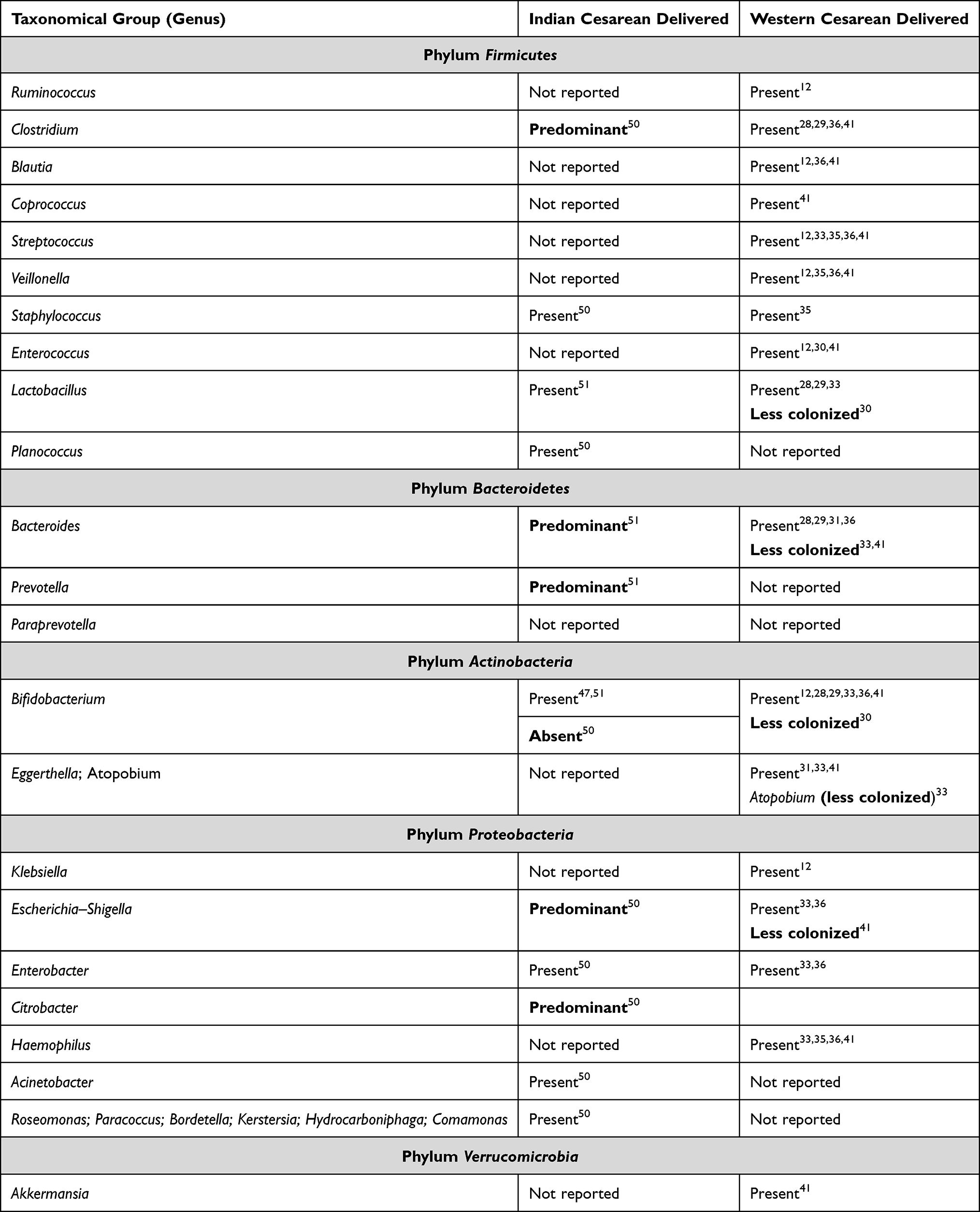 |
Table 3 Gut Microbiota (0–24 Months) in Indian and Western Cesarean Delivered Infants |
Similarities and Differences Reported in Gut Microbiota of Vaginally Delivered Infants
Table 2 shows the similarities and differences in gut microbiota profile of vaginally delivered infants of Indian vs Western population. Of the studies reporting gut microbiota in VD full-term infants Ruminococcus, Clostridium, Streptococcus, Veillonella, Staphylococcus, and Lactobacillus (Firmicutes); Bacteroides (phylum Bacteroidetes); Bifidobacterium (phylum Actinobacteria); Klebsiella, Escherichia–Shigella, and Haemophilus (phylum Proteobacteria) were reported by both Indian and Western studies.
Pandey et al (Indian; 0–7 days neonates) reported predominance of Staphylococcus, Bifidobacterium, and Acinetobacter in VD while Western studies reported predominance of Bifidobacterium (0–6 weeks infants)33 and Escherichia–Shigella (0–4 months)41 in VD infants.
Similarities and Differences Reported in Gut Microbiota of Cesarean Delivered Infants
Table 3 shows the similarities and differences in gut microbiota profile of vaginally delivered infants of Indian vs Western population. Clostridium, Staphylococcus, Lactobacillus, Bacteroides, Bifidobacterium, Escherichia–Shigella and Enterobacter were reported for both Indian and Western CSD full term infants.
For the CSD infants, Indian studies reported predominance of Clostridium,50 Bacteroides (0–6 months),51 Prevotella,51 Escherichia–Shigella50 and Citrobacter50 and absence of Bifidobacterium.50 On the other hand, Western studies reported less colonization of Bifidobacterium,30 Atopobium,33 Escherichia–Shigella41 in CSD infants.
Relative Abundance of Microbiota in Vaginal versus Caesarean Delivered Infants
Both Indian and Western studies report predominance of in Bifidobacterium VD33,50 infants and either absence or less colonization of Bifidobacterium in CSD30,50 infants. However, the over or under representation of various other gut microbiota varied.
Gut Microbiota in Indian versus Western Infants Classified According to Feeding Practices
Tables 4–6 represent the bacteria present in the gut microbiota of infants during 0–24 months of life, classified according to the feeding practices. Twelve (four Indian and eight Western) studies reported the gut microbiota by feeding practices.
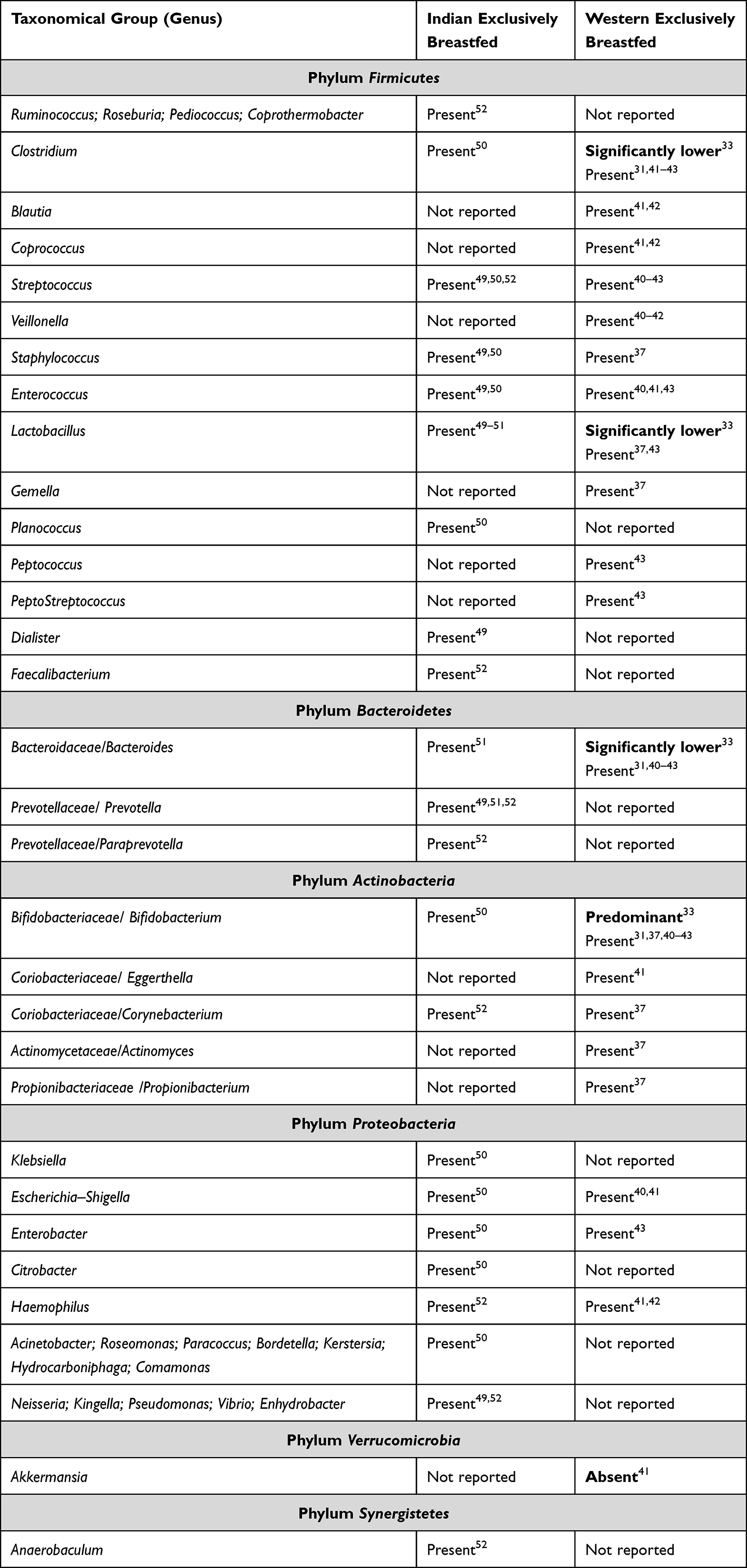 |
Table 4 Gut Microbiota (0–24 Months) in Indian and Western Exclusively Breastfed Infants |
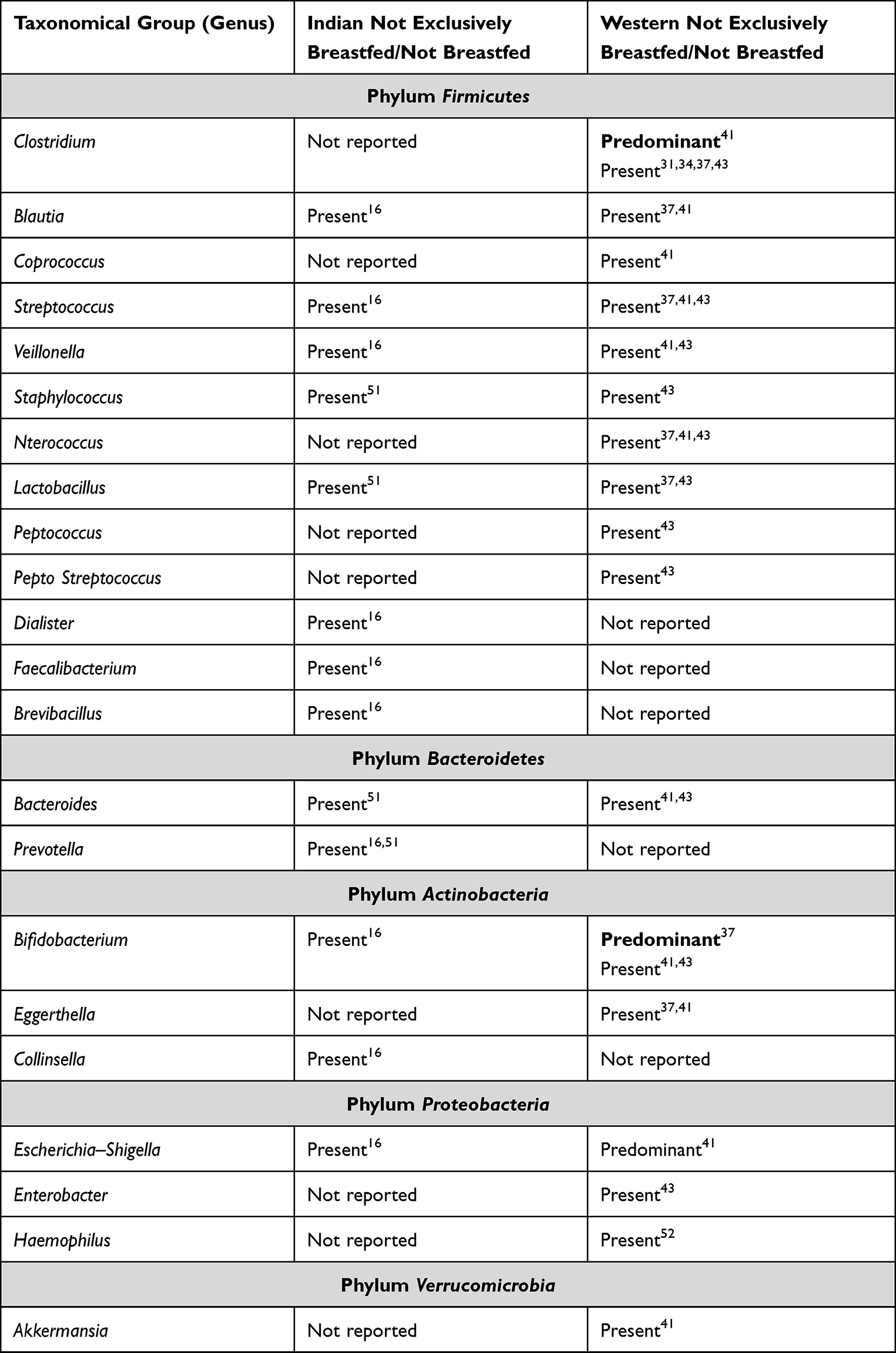 |
Table 5 Gut Microbiota (0–24 Months) in Indian and Western Not Exclusively Breastfed Infants |
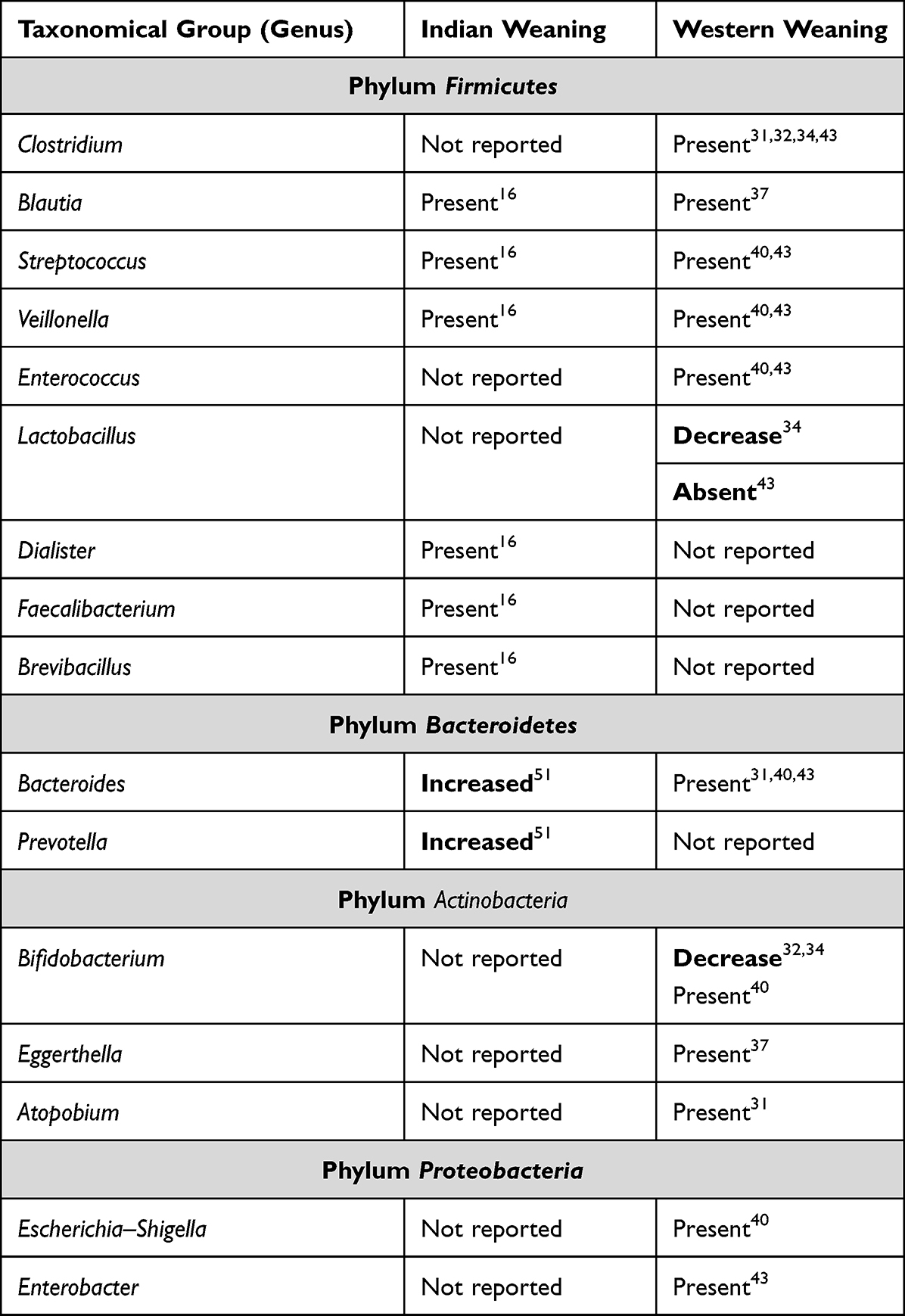 |
Table 6 Gut Microbiota (0–24 Months) in Indian and Western Infants During Weaning |
There were no studies comparing the gut microbiota in Indian versus Western infants by feeding practices. Of the Indian studies, only Kabeerdoss et al reported the gut microbiota during the weaning period. However, since Shivakumar et al reported the gut microbiota profile of 18–24 months old in infants who were not breastfed, their reported gut microbiota profile was also included in this section. On the other hand, several Western studies reported multiple genera in the infants during the weaning period.31,32,34,34,37,40
Similarities and Differences Reported in Gut Microbiota of Exclusively Breastfed Infants
Table 4 shows the similarities and differences in gut microbiota profile of exclusively breastfed infants of Indian vs Western population. Attri et al reported all the phyla in Indian exclusively breastfed infants: Firmicutes, Proteobacteria, Bacteroidetes, Actinobacteria, Verrucomicrobia, Fusobacteria, Synergistetes.52
For exclusively breastfed infants, the following gut microbiotas were reported for both Indian and Western infants: Clostridium, Streptococcus, Staphylococcus, Enterococcus, Lactobacillus (Firmicutes); Bacteroides (Bacteroidetes); Bifidobacterium, Corynebacterium (Actinobacteria); and Escherichia–Shigella, Enterobacter, Haemophilus (Proteobacteria). The differences in the gut microbiotas in exclusively breastfed infants are detailed in Table 4.
Similarities and Differences Reported in Gut Microbiota of Not Exclusively Breastfed Infants
Table 5 shows the similarities and differences in gut microbiota profile of not exclusively breastfed infants of Indian vs Western population. Seven Western and three Indian studies reported the gut microbiota profiles in not exclusively breastfed infants (formula-fed or fed with animal milk along with breastfeeding). For infants who were not exclusively breastfed, Clostridium, Blautia, Streptococcus, Staphylococcus, Veillonella, Lactobacillus (Firmicutes); Bacteroides (Bacteroidetes); Bifidobacterium (Actinobacteria); Escherichia–Shigella (Proteobacteria) were reported for both Indian and Western infants. The differences in the gut microbiotas in not exclusively breastfed infants are detailed in Table 5.
Similarities and Differences Reported in Gut Microbiota of Infants During Weaning Period
Table 6 shows the similarities and differences in gut microbiota profile of infants of Indian vs Western population during the weaning period. There was lack of Indian data during weaning period with only two studies reporting microbiota profile during weaning. Eight studies from the Western world reported microbiota profile during weaning.
Despite lack of Indian literature, both the Indian and Western infants were reported to colonize Blautia, Streptococcus, Veillonella (Firmicutes); and SeBacteroides (Bacteroidetes).
Under the phylum Firmicutes, an increase in families of Ruminococcaceae and Lachnospiraceae and decrease in families of Enterococcaceae and Lactobacillaceae were reported by Western studies.32,41 Families of Erysipelotrichaceae; Peptostreptococcaceae were also reported by a Western study.41 However, the genera details of these families were not reported. Other differences in the gut microbiotas during weaning are detailed in Table 6.
Discussion
The bacterial phyla representative of the human gut microbiota are Bacteroidetes, Firmicutes, Actinobacteria, Proteobacteria, and Verrucomicrobia.6,53 Of these, the neonatal gut microflora comprises mainly of four major phyla: Proteobacteria, Firmicutes, Actinobacteria, and Bacteroidetes.4,11 Our systematic review also concludes that gut microbiotas of the phyla Firmicutes, Proteobacteria, Actinobacteria, Bacteroidetes, and Verrucomicrobia were present in both Indian and Western infants. The phyla Fusobacteria and Synergistetes were reported for only Indian infants by a single study52 only.
Proteobacteria and Firmicutes were the most represented phyla across both populations, followed by Actinobacteria, Bacteroidetes and Verrucomicrobia. A similar representation of phyla has also been reported Asian and Western communities by a recent review article.6,41,54 However, an older review of Western studies reported Firmicutes and Bacteroidetes were the most reported phyla followed by Proteobacteria and Actinobacteria.9 The differences in the reported predominance of the phyla are driven by the research question. Xu et al and our systematic review was focused on identifying the ethnic diversity/similarity while the review by Fang et al was focused on the gut microbiota in health and neurocognitive development.
At the genera level, Staphylococcus, Streptococcus, Enterococcus, Lactobacillus, Clostridium, Eubacteria, Blautia, Veillonella (Firmicutes); Escherichia, Klebsiella, Proteus and Enterobacter (Proteobacteria); Bifidobacteria, Corynebacterium (Actinobacteria); Bacteroides (Bacteroidetes); and Akkermansia (Verrucomicrobia) were the common genera reported for both Indian and Western healthy full-term infants. While a timeline of relative abundance according to infant’s age is not possible for this systematic review due to paucity of literature, similar gut microbiotas profile has been reported for healthy full-term infants with abundance of Bifidobacterium, Bacteroides, Akkermansia, Lactobacillus, Streptococcus, Staphylococcus and Clostridium.55 The review by Yang et al too reported abundance of Clostridium, Enterococcus, Lactobacillus, and Ruminococcus (Firmicutes); Bacteroides and Prevotella (Bacteroidetes), which were the common genera we also found in Indian and Western studies.
The gut microbiota of the newborn undergoes developmental changes based on two primary independent factors, mode of delivery and feeding practices.36,41,55 The gut microbiota of VD is dominated by gut microbiota derived from the mother’s vagina while the gut microbiota of CSD is derived from maternal skin.54,56 This difference is more pronounced in the first week since birth and less visible after six months of age.11,12 Thereafter, the gut microbiotas of the VD and CSD attain almost similar profile with minor differences in the microbiotas profile along with expected delay in development and relative abundance of microbiotas in CSD as compared to VD.28,30,33,41,50,51
Since this systematic review included the microbiota profile of both VD and CSD across different timelines between 0 and 24 months age, we found that at the genera level, Clostridium, Staphylococcus Lactobacillus, Escherichia–Shigella, Bifidobacterium and Bacteroides were common to both VD and CSD infants across Indian and Western population. An earlier systematic review too found that Bifidobacteria, Bacteroides, Clostridium, and Lactobacillus genera were common in both VD and CSD from the age of 6 to 12 months of life.11
CSD infants have been reported to have a relative low abundance of Bifidobacteria and low colonization or absence of Bacteroides.56 These microbiotas are usually obtained from the mother at birth. This systematic review too reported absence50 or low colonization30 of Bifidobacteria in CSD.
Compared to VD, CSD infants have a relatively lower gut microbial diversity, primarily due to delay in colonization of Bacteroidetes.57 This systematic review too found a relatively lower genera diversity for the phylum Firmicutes and Proteobacteria in the CSD infants. However, though Bacteroides were present in both VD and CSD, the relative difference in their abundance and timeline of appearance could not be ascertained.
The microbiota profile of both exclusively breastfed and not exclusively breastfed is also similar but the timeline of appearance and their relative abundance differs.37 There is sequential colonization of intrauterine/vaginal birth associated microbiota followed by skin-derived taxa.35,37 Ethnic diversity in infant gut microbiota appears before the introduction of complementary feeding and is primarily due to geographic differences.54 This is seen to some extent between the two groups, especially at the genus level. Of the phyla common between Indian and Western exclusively breastfed infants, there was ethnic diversity at the genera level. While Ruminococcus, Roseburia, Pediococcus, Coprothermobacter, Planococcus, Dialister, Faecalibacterium, Prevotella, Paraprevotella, Vibrio, Enhydrobacter, Kingella, Neisseria, Pseudomonas, Acinetobacter, Roseomonas, Paracoccus; Bordetella, Kerstersia, Hydrocarboniphaga, Comamonas were found in Indian infants, the genera Blautia, Coprococcus, Veillonella, Gemella, Peptococcus, Eggerthella were reported in Western infants. However, in general, the Indian and Western exclusively breastfed infants had the same microbial profile Box 1.
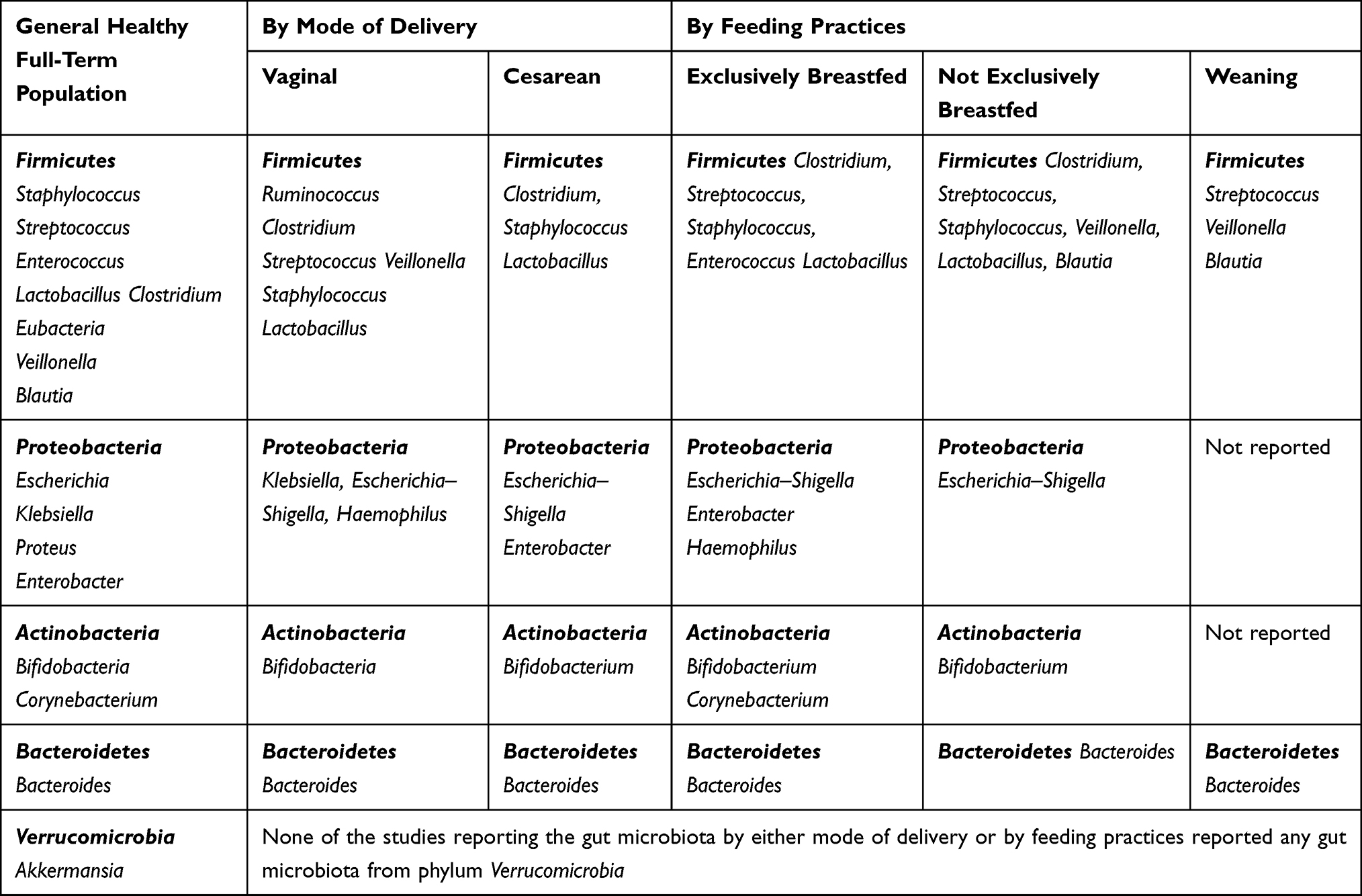 |
Box 1 Gut Microbiotas Common to Both Indian and Western Healthy Full-Term Infants |
Similarly, both Indian and Western infants not exclusively breastfed also had bacteria of several genera common among them (Box 1). Bifidobacterium can ferment milk oligosaccharides and is therefore present in abundance in infants as they are mainly fed on milk diet.54,56 This systematic review too found high colony percentages of Bifidobacterium reported from both Indian16,46,48,49 and Western33,39,41 studies.
Gut microbiota profile of infants fed on formula or animal milk is modified by the microbiotas present in these feeds.58 Staphylococcus, Streptococcus, Enterococcus and Clostridium along with Bifidobacterium have been found to dominate the gut microbiota profile of formula-fed infants. This systematic review too found these microbiotas along with Veillonella, Lactobacillus, Blautia and Bacteroides in Indian and Western infants who were not exclusively breastfed.
Complementary diet in infancy plays a major role in diversity of gut microbiota and its development into an adult gut microbiota profile.54 Thus, the gut microbiota is dominated by genera of Firmicutes and Bacteroidetes that are also found in the adults.54 This systematic review too found the genera Blautia, Streptococcus, Veillonella and Bacteroides in both Indian and Western infants during weaning period, despite differences in feeding practices during weaning between the Indian and Western infants. However, the gut microbiota composition during weaning was not well represented in this systematic review, especially for Indian studies, due to lack of data available from the studies that met the inclusion criteria.
Strengths and Limitations
The systematic review could not retrieve any literature that compares the gut microbiome between Indian and Western infants from birth to 24 months of age. For the first time, a systematic literature search revealed that gut microbiota of term healthy adequately nourished infants (0.24 months) is somewhat similar between Indian and Western population. However, direct age-wise (at birth, 6 months, 1 year and 2 years) comparisons between the Indian and Western infants were not possible because of lack of targeted time-specific literature for the two groups. Hence, this systematic review reported the comparative gut microbiota profile for the entire time-period from birth to 2 years in Indian versus Western term healthy adequately nourished infant.
Similarly, the relative abundance of a particular gut microbiota according to a specific time period was not possible due to lack of literature. Also, no statistical analysis for the relative abundance could be conducted as the samples were collected at different time periods and analyzed using different probes and methods. Despite these shortcomings, the systematic review could retrieve and report the colony percentages of the gut microbiotas for the Indian and Western infants aged 0–24 months.
The systematic review identified the need for well-designed studies that outline the minimum requirements to report the infant gut microbiota such as (but not limited to) taxonomical classification used, granularity of data to be presented, source of swab (fecal/oral), method of detection, etc. The systematic review also identified the need for comparing gut microbiota profile between Indian and Western infants based on targeted time-period and within the targeted time-period by mode of delivery and feeding practices. Another major gap identified was lack of studies, especially Indian, during the weaning period that assessed the gut microbiota profile by the weaning feeding practices. Further, we think that larger longitudinal studies are required to see the similarities and differences in the development of gut microbiota profile between Indian and Western infants.
Clinical Implications
The systemic review showed diverse phyla colonizing the infant gut in both Indian and Western infants. Usually, a highly diverse microbial profile is advantageous for optimal health.9 However, the systematic review also found colonies of harmful gut microbiotas17,18,59 such as Klebsiella, Escherichia–Shigella, Clostridium and Staphylococcus across the two populations. Probiotics containing Lactobacilli, Bifidobacteria and Streptococcus are often used to effectively alter the gut microbiota profile towards developing eubiosis.10,16–18
These protective microbiotas were commonly present across the two populations irrespective of mode of delivery and breastfeeding practices. However, included studies did show that Lactobacillus population can decrease in CSD30 and during weaning34 and Bifidobacteria can decrease in CSD.30,50 Gut dysbiosis has been reported even in breastfed infants.60
Gut dysbiosis has been linked to increased risk for allergic disease, asthma, inflammatory bowel disease (IBD), autoimmune disorders, obesity, and associated noncommunicable diseases (NCDs) like diabetes and cardiovascular disorders.61–63 The epigenetic link between gut dysbiosis and diseases can be explained through the perspective of the “Developmental Origins of Health and Disease (DOHaD)”.62 The DOHaD theory gives importance to nutrition and environmental exposures and notes that proper probiotic supplementation from birth through the infancy and early childhood can favourably modulate the gut microbiota and its products and thereby reduce the risk of diseases like IBD and NCDs.61–63
Early probiotic supplementation is associated with persistent eubiosis at one year and beyond.60 Hence, since the gut microbial profile of the Indian and Western infants is largely similar with respect to clinical implications, it can be inferred that they can be supplemented with similar probiotics during infancy (0–24 months).
Therefore, infant food supplements and probiotics which have the same composition as that of the protective infant microbiota of both Indian and Western infants can be used universally for both the populations to improve the growth, health, and development of infants as desired.
Long-term follow-up studies are required to compare the gut-microbiota and its correlation with health and disease between the Indian and Western infants. Special focus is required to see the association with IBD, NCDs and autoimmune disorders and how the gut microbiota can be effectively modulated towards health.
Author Conclusions
This systematic review found that despite some differences, the gut microbiota of Indian and Western infants aged 0–24 months are largely similar (Box 1), with implications for probiotic supplementation.
However, there are no studies comparing the gut microbiota in Indian versus Western infants (0–24 months). Hence, well-designed studies with age-specific comparative populations, and according to the same timeline of development, mode of delivery, and feeding practices can better help understand the similarities and differences in the growth, development, and diversity of the gut microbiota in both the populations. This can help in clearly identifying the window of opportunity for supplementation and intervention.
Ethics Compliance
The study was a narrative synthesis of systematic literature search and hence did not require EC approval.
Acknowledgments
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work, and have given final approval for the version to be published. The authors thank Dr. Punit Srivastava, and Dr. Kokil Mathur of Mediception Science Pvt. Ltd (www.mediception.com) for providing medical writing support in the preparation of this manuscript.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Guarner F, Malagelada J-R. Gut flora in health and disease. Lancet. 2003;361(9356):512–519. doi:10.1016/S0140-6736(03)12489-0
2. Thursby E, Juge N. Introduction to the human gut microbiota. Biochem J. 2017;474:1823–1836. doi:10.1042/BCJ20160510
3. Wampach L, Heintz-Buschart A, Hogan A, et al. Colonization and succession within the human gut microbiome by archaea, bacteria, and microeukaryotes during the first year of life. Front Microbiol. 2017. doi:10.3389/fmicb.2017.00738
4. Bharadia L, Agrawal N, Joshi N. Development and functions of the infant gut microflora: Western vs. Indian infants. Int J Pediatr. 2020;2020:e7586264. doi:10.1155/2020/7586264
5. van de Pol JAA, van Best N, Mbakwa CA, et al. Gut colonization by methanogenic archaea is associated with organic dairy consumption in children. Front Microbiol. 2017;8. doi:10.3389/fmicb.2017.00355
6. Palmer C, Bik EM, DiGiulio DB, Relman DA, Brown PO. Development of the human infant intestinal microbiota. PLoS Biol. 2007;5:e177. doi:10.1371/journal.pbio.0050177
7. Rani SB, Balamurugan R, Ramakrishna BS. Molecular analysis of the human faecal archaea in a southern Indian population. J Biosci. 2017;42:113–119. doi:10.1007/s12038-017-9668-7
8. Underwood MA, Mukhopadhyay S, Lakshminrusimha S, Bevins CL. Neonatal intestinal dysbiosis. J Perinatol. 2020;40:1597–1608. doi:10.1038/s41372-020-00829-2
9. Yang I, Corwin EJ, Brennan PA, Jordan S, Murphy JR, Dunlop A. The infant microbiome: implications for infant health and neurocognitive development. Nurs Res. 2016;65:76–88. doi:10.1097/NNR.0000000000000133
10. Walker WA. Initial intestinal colonization in the human infant and immune homeostasis. Ann Nutr Metab. 2013;63(Suppl 2):8–15. doi:10.1159/000354907
11. Rutayisire E, Huang K, Liu Y, Tao F. The mode of delivery affects the diversity and colonization pattern of the gut microbiota during the first year of infants’ life: a systematic review. BMC Gastroenterol. 2016;16:86. doi:10.1186/s12876-016-0498-0
12. Reyman M, van Houten MA, van Baarle D, et al. Impact of delivery mode-associated gut microbiota dynamics on health in the first year of life. Nat Commun. 2019;10:4997. doi:10.1038/s41467-019-13014-7
13. Zhang C, Li L, Jin B, et al. The effects of delivery mode on the gut microbiota and health: state of art. Front Microbiol. 2021;12:724449. doi:10.3389/fmicb.2021.724449
14. Laursen MF. Gut microbiota development: influence of diet from infancy to toddlerhood. ANM. 2021;77:21–34.
15. Martin R, Makino H, Yavuz AC, et al. Early-life events, including mode of delivery and type of feeding, siblings and gender, shape the developing gut microbiota. PLoS One. 2016;11:e0158498. doi:10.1371/journal.pone.0158498
16. Shivakumar N, Sivadas A, Devi S, et al. Gut microbiota profiles of young South Indian children: child sex-specific relations with growth. PLoS One. 2021;16:e0251803. doi:10.1371/journal.pone.0251803
17. Thomas DW, Greer FR. Committee on nutrition; section on gastroenterology H and nutrition. Probiotics and prebiotics in pediatrics. Pediatrics. 2010;126:1217–1231. doi:10.1542/peds.2010-2548
18. Piewngam P, Otto M. Probiotics to prevent Staphylococcus aureus disease? Gut Microbes. 2019;11:94–101. doi:10.1080/19490976.2019.1591137
19. Nazir Y, Hussain SA, Abdul Hamid A, Song Y. Probiotics and their potential preventive and therapeutic role for cancer, high serum cholesterol, and allergic and HIV diseases. Biomed Res Int. 2018;2018:e3428437. doi:10.1155/2018/3428437
20. Sharma A. Change in immigration trends – Indians now moving to new countries beyond the UK, Canada. The Financial Express. Financial Express; 2022. Available from: https://www.financialexpress.com/passport-visa/change-in-immigration-trends-indians-now-moving-to-new-countries-beyond-The-uk-canada/2448859.
21. Knobler S, Mahmoud A, Lemon S, Pray L. A World in motion: the global movement of people, products, pathogens, and power. National Academies Press (US); 2006. Available from: https://www.ncbi.nlm.nih.gov/books/NBK56593.
22. Sbihi H, Boutin RCT, Cutler C, Suen M, Finlay BB, Turvey SE. Thinking bigger: how early-life environmental exposures shape the gut microbiome and influence the development of asthma and allergic disease. Allergy. 2019;74:2103–2115. doi:10.1111/all.13812
23. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;71:105906.
24. Page MJ, Moher D, Bossuyt PM, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ;2021:n160. doi:10.1136/bmj.n160
25. World Population Review. Western Countries 2023; 2023. Available from: https://worldpopulationreview.com/country-rankings/western-countries.
26. ITIS. Integrated taxonomic information system. integrated taxonomic information system; 2022. Available from: https://www.itis.gov.
27. Rotimi VO, Duerden BI. The development of the bacterial flora in normal neonates. J Med Microbiol. 1981;14:51–62. doi:10.1099/00222615-14-1-51
28. Grönlund MM, Lehtonen OP, Eerola E, Kero P. Fecal microflora in healthy infants born by different methods of delivery: permanent changes in intestinal flora after cesarean delivery. J Pediatr Gastroenterol Nutr. 1999;28:19–25. doi:10.1097/00005176-199901000-00007
29. Huurre A, Kalliomäki M, Rautava S, Rinne M, Salminen S, Isolauri E. Mode of delivery - effects on gut microbiota and humoral immunity. Neonatology. 2008;93:236–240. doi:10.1159/000111102
30. Mitsou EK, Kirtzalidou E, Oikonomou I, Liosis G, Kyriacou A. Fecal microflora of Greek healthy neonates. Anaerobe. 2008;14:94–101. doi:10.1016/j.anaerobe.2007.11.002
31. Fallani M, Amarri S, Uusijarvi A, et al. Determinants of the human infant intestinal microbiota after the introduction of first complementary foods in infant samples from five European centres. Microbiology. 2011;157:1385–1392. doi:10.1099/mic.0.042143-0
32. Roger LC, McCartney AL. Longitudinal investigation of the faecal microbiota of healthy full-term infants using fluorescence in situ hybridization and denaturing gradient gel electrophoresis. Microbiology. 2010;156:3317–3328. doi:10.1099/mic.0.041913-0
33. Fallani M, Young D, Scott J, et al. Intestinal microbiota of 6-week-old infants across Europe: geographic influence beyond delivery mode, breast-feeding, and antibiotics. J Pediatr Gastroenterol Nutr. 2010;51:77–84. doi:10.1097/MPG.0b013e3181d1b11e
34. Bergström A, Skov TH, Bahl MI, et al. Establishment of intestinal microbiota during early life: a longitudinal, explorative study of a large cohort of Danish infants. Appl Environ Microbiol. 2014;80:2889–2900. doi:10.1128/AEM.00342-14
35. Bäckhed F, Roswall J, Peng Y, et al. Dynamics and stabilization of the human gut microbiome during the first year of life. Cell Host Microbe. 2015;17:690–703. doi:10.1016/j.chom.2015.04.004
36. Hill CJ, Lynch DB, Murphy K, et al. Evolution of gut microbiota composition from birth to 24 weeks in the INFANTMET Cohort. Microbiome. 2017;5:4. doi:10.1186/s40168-016-0213-y
37. Timmerman HM, Rutten NBMM, Boekhorst J, et al. Intestinal colonisation patterns in breastfed and formula-fed infants during the first 12 weeks of life reveal sequential microbiota signatures. Sci Rep. 2017;7:8327. doi:10.1038/s41598-017-08268-4
38. Forsgren M, Isolauri E, Salminen S, Rautava S. Late preterm birth has direct and indirect effects on infant gut microbiota development during the first six months of life. Acta Paediatr. 2017;106:1103–1109. doi:10.1111/apa.13837
39. Chernikova DA, Madan JC, Housman ML, et al. The premature infant gut microbiome during the first 6 weeks of life differs based on gestational maturity at birth. Pediatr Res. 2018;84:71–79. doi:10.1038/s41390-018-0022-z
40. Mata LJ, Mejicanos ML, Jiménez F. Studies on the indigenous gastrointestinal flora of Guatemalan children. Am J Clin Nutr. 1972;25:1380–1390. doi:10.1093/ajcn/25.12.1380
41. Azad MB, Konya T, Maughan H, et al. Gut microbiota of healthy Canadian infants: profiles by mode of delivery and infant diet at 4 months. CMAJ. 2013;185:385–394. doi:10.1503/cmaj.121189
42. Fehr K, Moossavi S, Sbihi H, et al. Breastmilk feeding practices are associated with the co-occurrence of bacteria in mothers’ milk and the infant gut: the CHILD Cohort Study. Cell Host Microbe. 2020;28:285–297.e4. doi:10.1016/j.chom.2020.06.009
43. Stark PL, Lee A. The microbial ecology of the large bowel of breast-fed and formula-fed infants during the first year of life. J Med Microbiol. 1982;15:189–203. doi:10.1099/00222615-15-2-189
44. Higgins JPT, Altman DG, Gøtzsche PC, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. doi:10.1136/bmj.d5928
45. Albert MJ, Bhat P, Rajan D, Maiya PP, Pereira SM, Baker SJY. Faecal flora of south Indian infants and young children in health and with acute gastroenteritis. J Med Microbiol. 1978;11:137–143. doi:10.1099/00222615-11-2-137
46. Dinh DM, Ramadass B, Kattula D, et al. Longitudinal analysis of the intestinal microbiota in persistently stunted young children in South India. PLoS One. 2016;11:e0155405. doi:10.1371/journal.pone.0155405
47. Balamurugan R, Magne F, Balakrishnan D, et al. Faecal bifidobacteria in Indian neonates & the effect of asymptomatic rotavirus infection during the first month of life. Indian J Med Res. 2010;132:721–727.
48. Sharma N, Chaudhry R, Panigrahi P. Quantitative and Qualitative Study of Intestinal Flora in Neonates. J Glob Infect Dis. 2012;4:188–192. doi:10.4103/0974-777X.103895
49. Huey SL, Jiang L, Fedarko MW, et al. Nutrition and the gut microbiota in 10 to 18-month-old children living in Urban Slums of Mumbai, India. mSphere. 2020;5:e00731–e00820. doi:10.1128/mSphere.00731-20
50. Pandey PK, Verma P, Kumar H, Bavdekar A, Patole MS, Shouche YS. Comparative analysis of fecal microflora of healthy full-term Indian infants born with different methods of delivery (vaginal vs cesarean): acinetobacter sp. prevalence in vaginally born infants. J Biosci. 2012;37:989–998.
51. Kabeerdoss J, Ferdous S, Balamurugan R, et al. Development of the gut microbiota in southern Indian infants from birth to 6 months: a molecular analysis. J Nutr Sci. 2013;2:e18. doi:10.1017/jns.2013.6
52. Attri S, Nagpal R, Goel G. High throughput sequence profiling of gut microbiome in Northern Indian infants during the first four months and its global comparison. Meta Gene. 2018;17:184–191. doi:10.1016/j.mgene.2018.06.011
53. MCarmen M-C, Peláez Carmen RT. Chapter 6 - laboratory simulators of the colon microbiome. In: Faintuch J, Faintuch S, editors. Microbiome and Metabolome in Diagnosis, Therapy, and Other Strategic Applications. Academic Press; 2019:61–67.
54. Xu J, Lawley B, Wong G, et al. Ethnic diversity in infant gut microbiota is apparent before the introduction of complementary diets. Gut Microbes. 2022;11:1362–1373. doi:10.1080/19490976.2020.1756150
55. Robertson RC, Manges AR, Finlay BB, Prendergast AJ. The human microbiome and child growth – first 1000 days and beyond. Trends Microbiol. 2019;27:131–147. doi:10.1016/j.tim.2018.09.008
56. Korpela K. Impact of delivery mode on infant gut microbiota. ANM. 2021;77:11–19.
57. Jakobsson HE, Abrahamsson TR, Jenmalm MC, et al. Decreased gut microbiota diversity, delayed Bacteroidetes colonisation and reduced Th1 responses in infants delivered by caesarean section. Gut. 2014;63:559–566. doi:10.1136/gutjnl-2012-303249
58. Moore RE, Townsend SD. Temporal development of the infant gut microbiome. Open Biol. 2019;9:190128. doi:10.1098/rsob.190128
59. Adlerberth I, Wold AE. Establishment of the gut microbiota in Western infants. Acta Paediatr. 2009;98:229–238. doi:10.1111/j.1651-2227.2008.01060.x
60. O’Brien CE, Meier AK, Cernioglo K, et al. Early probiotic supplementation with B. infantis in breastfed infants leads to persistent colonization at 1 year. Pediatr Res. 2022;91:627–636. doi:10.1038/s41390-020-01350-0
61. West CE, Renz H, Jenmalm MC, et al. The gut microbiota and inflammatory noncommunicable diseases: associations and potentials for gut microbiota therapies. J Allergy Clin Immunol. 2015;135:3–13; quiz 14. doi:10.1016/j.jaci.2014.11.012
62. Mejia-Leon ME, Argüelles-Lopez A, Briseño-Sahagun P, et al. Could alterations in the infant gut microbiota explain the development of noncommunicable diseases from the DOHaD perspective? IntechOpen. 2022. doi:10.5772/intechopen.105168
63. Luca FD, Shoenfeld Y. The microbiome in autoimmune diseases. Clin Exp Immunol. 2019;195:74. doi:10.1111/cei.13158
64. Kumbhare SV, Patangia DV, Mongad DS, Bora A, Bavdekar AR, Shouche YS. Gut microbial diversity during pregnancy and early infancy: an exploratory study in the Indian population. FEMS Microbiol Lett. 2020;367:fnaa022. doi:10.1093/femsle/fnaa022
65. Collins MD. The Genus Gemella. In: Dworkin M, Falkow S, Rosenberg E, Schleifer K-H, Stackebrandt E, editors. The Prokaryotes: Volume 4: Bacteria: Firmicutes, Cyanobacteria. New York, NY: Springer US; 2006:511–518.
66. Morand A, Tall ML, Kuete Yimagou E, et al. Anaerococcus urinimassiliensis sp. nov., a new bacterium isolated from human urine. Sci Rep. 2021;11:2684. doi:10.1038/s41598-021-82420-z
67. Sorbara MT, Littmann ER, Fontana E, et al. Functional and genomic variation between human-derived isolates of lachnospiraceae reveals inter- and intra-species diversity. Cell Host Microbe. 2020;28:134–146.e4. doi:10.1016/j.chom.2020.05.005
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.