")
Back to Journals » International Medical Case Reports Journal » Volume 12
Growing teratoma syndrome with porta hepatis involvement – a case report
Authors Abdulraheem EA, Sait MK , Sait KH , Anfinan NM , Elkadi OR
Received 29 August 2018
Accepted for publication 1 February 2019
Published 22 March 2019 Volume 2019:12 Pages 75—78
DOI https://doi.org/10.2147/IMCRJ.S185572
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Ronald Prineas
Ekhlas Ahmed Abdulraheem,1 Maram K Sait,2 Khalid H Sait,2 Nisreen M Anfinan,1 Osama R Elkadi3
1Department of Obstetrics and Gynecology, Gynecology Oncology Unit, Faculty of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia; 2Faculty of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia; 3Department of Pathology, Drexel University College of Medicine, PA, USA
Abstract: Growing teratoma syndrome is a rare entity of tumors, it arises seldomly from ovarian and testicular carcinoma. It presents with disseminating masses of mature teratoma during or following chemotherapy of malignant germ cell tumors. We are reporting a 19-year old presented with recurrent left ovarian mass and supra renal large mass close to the porta hepatis was seen on magnetic resonance imaging. This patient was treated 3 years ago for stage I immature teratoma with left ovarian cystectomy and chemotherapy. Surgical excision of the left ovary and the abdominal mass required meticulous dissection, and the mass was shaved off the porta hepatis with no intraoperative or postoperative complications. Pathology showed mature teratoma. She has no recurrent 5 years after treatment. To the best of our knowledge, this is the first case report describing close relation of growing teratoma syndrome to the porta hepatis, no such case report like this has been reported in our region.
Keywords: malignant germ cell tumor, porta hepatis, growing teratoma syndrome
Introduction
Growing teratoma syndrome (GTS) is a rare condition, which presents as metastasizing large masses of mature teratoma during or after chemotherapy of non-seminomatous germ cell tumors (NSGCTs) of ovary or testis.1,2 The description of this clinical entity was introduced in literature by Carr et al3 in 1981, who described a process of benign differentiation of testicular teratocarcinoma. That was followed by the introduction of the current terminology of this syndrome in 1982 by Logothetis. He reported a group of six cases of NSGCTs that transformed to benign growing masses after disease-free interval following appropriate chemotherapy and normalization of tumor markers.4 This condition has been detected in both ovarian and testicular NSGCTs, and the incidence is 1.9%–7.6%.5
We presented a case of recurrent mature teratoma in the ovary and the upper abdomen close to the porta hepatis after treatment for immature ovarian teratoma with cystectomy and chemotherapy.
Case presentation
A 19-year-old woman had left ovarian cystectomy and received two cycles of bleomycin, etoposide, and platinum chemotherapy for the diagnosis of stage I immature teratoma. She did not continue the treatment and lost a follow-up because of financial reason. Thirty months after last chemotherapy, she presented to our care for the first time with the complain of abdominal distention and discomfort for 4 months. On examination showed pelvic mass as well as large 12×10×8 cm right mass in the right upper abdomen. Magnetic resonance imaging scan of pelvis and abdomen revealed left ovarian mass 10×8×7 cm and a large well-defined suprarenal mass that measured 12×10×8.3 cm displacing the right kidney inferiorly and inferior the right lobe of liver and close to the porta hepatis (Figure 1). Both masses showed evidence of cystic changes, fatty component, and calcification. The previous histopathology was reviewed in our center, and it was consistent with immature teratoma, grade 3 (Figure 2). Her complete blood count and liver function test were normal. The Ca-125 level was 47 U/mL; alpha-fetoprotein and LDH and HCG were normal. Surgery was performed through vertical abdominal incision. Left oophorectomy was performed because the left ovary was occupied by a large friable tumor mass that measured 10×12×8 cm. Another large mass was identified; it measured about 13 cm and extended between superior surface of right suprarenal gland and inferior surface of the liver. The mass was closely related to the gall bladder and was partially enveloping porta hepatis. The tumor was gently mobilized and dissected through a clear plane and shaved carefully from the porta hepatis. Patient left with no residual disease. The operative time was 5 hours, and the blood loss was 1 L. The patient had an uneventful postoperative course with total 5 days of hospital stay. Histopathological examination of resected masses revealed mature teratoma (Figure 3). The patient was followed up for 48 months with no evidence of disease recurrence.
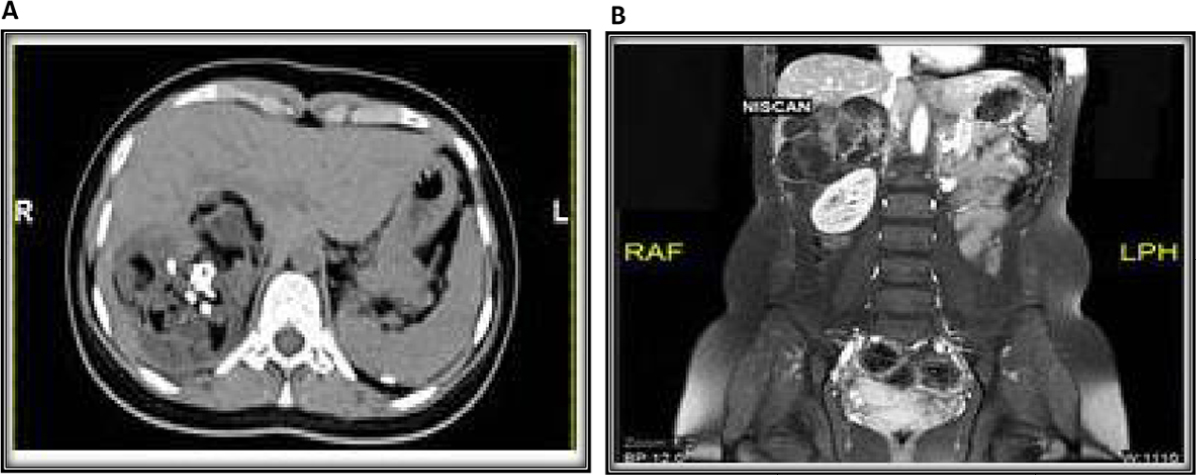 | Figure 1 (A, B) Magnetic resonance imaging scan of abdomen revealed a large well-defined suprarenal mass that measured 12×10×8.3 cm displacing the right kidney inferiorly and inferior the right lobe of liver and close to the porta hepatis, with evidence of cystic changes, fatty component, and calcification. |
 | Figure 2 Histopathology of the initial left ovarian tumor demonstrating immature teratoma composed of mixed immature and mature elements including (A) primitive neuroepithelial elements with rosettes formation (H&E, 4×), (B) focal immature cartilaginous elements (H&E, 4×), and (C) benign mature epithelial elements forming papillary structures adjacent to mature neuroglial tissue (H&E, 4×). |
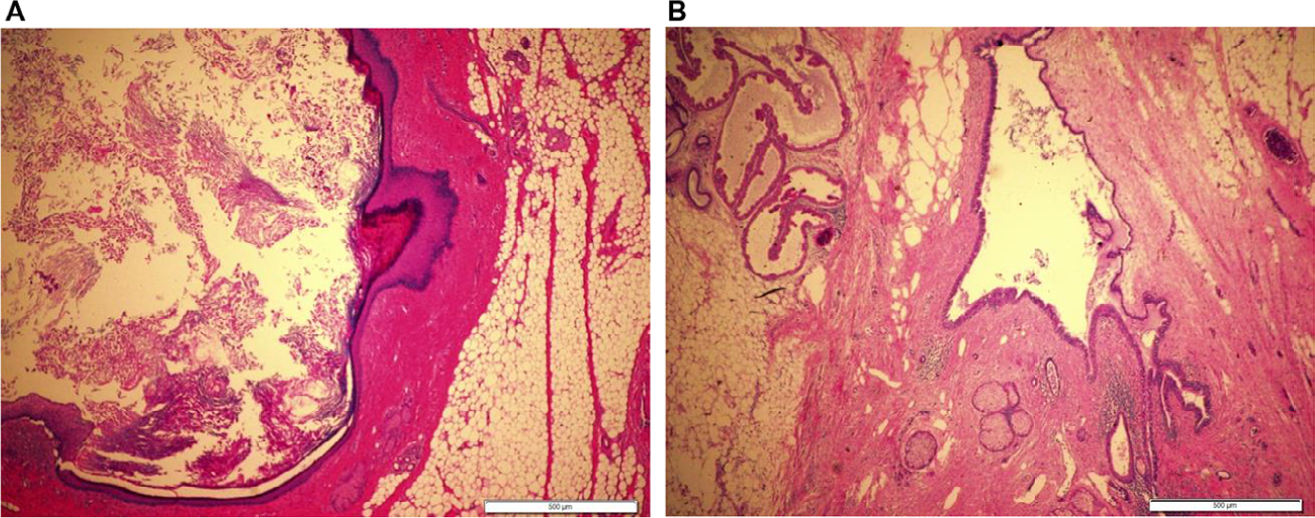 | Figure 3 Histopathology of the recurrent tumor revealed heterogeneous mature elements including (A) epidermal cyst lined by mature keratinized squamous epithelium and filled with keratinous debris (H&E, 4×), (B) dermoid cyst lined by benign squamous epithelium surrounded by mature fibroadipose tissue with embedded adnexal glands (H&E, 4×). |
Discussion
The etiology of GTS is not well understood but several postulations are quoted: 1) chemotherapy induced selective elimination of malignant cells with sparing of mature elements that eventually grow as migrating mature teratoma, 2) chemotherapy induced evolution of malignant cells to benign tissue, described as “chemotherapeutic retroconversion” by DiSaia et al,6 and 3) spontaneous evolution of malignant cells to benign ones, aided by prolongation of the disease course as a result of the treatment.7 A similar phenomenon reported in some cases in which ganglioneuroblastoma and neuroblastoma – malignant embryonic tumors of sympathetic nerve cells – had fully differentiated to ganglioneuroma, a mature benign tumor after radiation therapy.8
The diagnosis of GTS should meet the following three criteria: 1) history of definite diagnosis of NSGCT, 2) normal tumor markers, and 3) radiological evidence of growing lesions during or after chemotherapy. Surgery is the mainstay of treatment, and the outcome is dependent on the stage of size and the location of GTS.1
The retroperitoneum is the most common site of involvement; other anatomical locations reported in literature are the pelvis, mediastinum, lungs, lymph nodes, brain, and the liver.5
Our patient had a supra renal mass, inferior to the liver and partially involved the porta hepatis together with recurrent ovarian mass almost 3 years after ovarian cystectomy and chemotherapy for immature teratoma.
Literature review over 38 years characterized the patients mean age of diagnosis and mean tumor size. It demonstrated that the median age for NSGCTs diagnosis was 22 years, median tumor size of GTS was 8.6 cm (range 1–25 cm), and median time interval from primary treatment to diagnosis of GTS was 26.6 month.9
The standard therapy for GTS is complete surgical resection, since this disease is resistant to chemotherapy or radiotherapy. The risk of recurrence after total resection is low and measures only 0%–4% vs 72%–83% for partial resection.10
The surgical approach could be challenging especially for bulky tumor attached to vascular or visceral structures, as technical difficulties subsequently increase the incidence of intraoperative complications. Serious intraoperative complications associated with GTS are aortic and ureteral injury. Common postoperative complications are ileus, acute pancreatitis, chylous ascites, and sepsis.10 Complete surgical resection is advocated even with involvement of vital structures, and anticipation of reconstructive procedures is a must. Furthermore, special consideration should be given during anesthesia for cases with giant masses associated with respiratory compromise.11
In our case, there was no major operative difficulty in the surgical approach for our case, meticulous dissection of the mass in proximity to porta hepatis and right suprarenal gland was performed with no complications. Although the mass was closely related to the inferior surface of right lobe of liver, there was no parenchymal involvement. In literature review, GTS has been presented in two patients as intraparenchymal liver masses both underwent surgical excision and had uneventful follow-up.12 A more aggressive hepatic involvement of GTS was reported in one case where extensive teratoma growth replaced the entire liver and the patient underwent a successful liver transplantation.13
Conclusion
Clinical or radiological encounters of rapidly growing masses in patients treated for malignant germ cell tumors should raise the question about the probability of GTS diagnosis, especially if associated with normal tumor makers. The prognosis of GTS is favorable with early recognition and prompt surgical intervention. To the best of our knowledge, this is the first case report describing close relation of GTS to the porta hepatis, no such reports about GTS have been reported in our region.
Ethical approval and informed consent
Ethical approval for this study was obtained from the Unit of Biomedical Ethics, Faculty of Medicine. King Abdulaziz University Hospital. The patient provides both verbal informed consent and written informed consent for the publication of the case details and any images in the open access journal.
Disclosure
The authors report no conflicts of interest in this work.
References
Gorbatiy V, Spiess PE, Pisters LL. The growing teratoma syndrome: current review of the literature. Indian J Urol. 2009;25(2):186–189. | ||
Kato N, Uchigasaki S, Fukase M. How does secondary neoplasm arise from mature teratomas in growing teratoma syndrome of the ovary? A report of two cases. Pathol Int. 2013;63(12):607–610. | ||
Carr BI, Gilchrist KW, Carbone PP. The variable transformation in metastases from testicular germ cell tumors: the need for selective biopsy. J Urol. 1981;126(1):52–54. | ||
Logothetis CJ, Samuels ML, Trindade A, Johnson DE. The growing teratoma syndrome. Cancer. 1982;50(8):1629–1635. | ||
Kataria SP, Varshney AN, Nagar M, Mandal AK, Jha V. Growing teratoma syndrome. Indian J Surg Oncol. 2017;8(1):46–50. | ||
DiSaia PJ, Saltz A, Kagan AR, Morrow CP. Chemotherapeutic retroconversion of immature teratoma of the ovary. Obstet Gynecol. 1977;49(3):346–350. | ||
Hong WK, Wittes RE, Hajdu ST, Cvitkovic E, Whitmore WF, Golbey RB. The evolution of mature teratoma from malignant testicular tumors. Cancer. 1977;40(6):2987–2992. | ||
Dyke PC, Mulkey DA. Maturation of ganglioneuroblastoma to ganglioneuroma. Cancer. 1967;20(8):1343–1349. | ||
Li S, Liu Z, Dong C, et al. Growing teratoma syndrome secondary to ovarian giant immature teratoma in an adolescent girl: a case report and literature review. Medicine (Baltimore). 2016;95(7):e2647. | ||
Spiess PE, Kassouf W, Brown GA, et al. Surgical management of growing teratoma syndrome: the M. D. Anderson cancer center experience. J Urol. 2007;177(4):1330–1334. | ||
Ohashi N, Imai H, Tobita T, Ishii H, Baba H. Anesthetic management in a patient with giant growing teratoma syndrome: a case report. J Med Case Rep. 2014;8(1):32. | ||
Lorusso D, Malaguti P, Trivellizzi IN, Scambia G. Unusual liver locations of growing teratoma syndrome in ovarian malignant germ cell tumors. Gynecol Oncol Case Rep. 2011;1(1):24–25. | ||
Kapoor V, Ferris JV, Rajendiran S. Growing teratoma syndrome of the liver: treatment with living related donor liver transplantation. AJR Am J Roentgenol. 2003;181(3):839–841. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.