")
Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 16
Gout Knowledge: A Survey of Australian Outpatients with Gout
Authors Chin A, Adams RJ , Gill TK , Hill CL
Received 12 September 2023
Accepted for publication 9 November 2023
Published 13 January 2024 Volume 2024:16 Pages 1—7
DOI https://doi.org/10.2147/OARRR.S435692
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Chuan-Ju Liu
Athena Chin,1 Robert J Adams,2 Tiffany K Gill,3 Catherine L Hill1,4
1Rheumatology Unit, The Queen Elizabeth Hospital, Woodville South, South Australia, Australia; 2Flinders Health and Medical Research Institute – Sleep Health, Flinders University, Bedford Park, South Australia, Australia; 3Adelaide Medical School, University of Adelaide, Adelaide, South Australia, Australia; 4Discipline of Medicine, University of Adelaide, Adelaide, South Australia, Australia
Correspondence: Athena Chin, Email [email protected]
Background: The prevalence of gout has increased in the Western societies due to ageing and increasing BMI. Recently, lifestyle and dietary factors have been linked in epidemiological studies with an alteration of the risk of gout; however, there remains a lack of data on patient knowledge of these factors. The purpose of this survey-based study was to determine the knowledge of gout and its treatment both in the community and specialist care settings.
Methods: Participants were recruited from a hospital rheumatology outpatient department, consumer organization and a random sample of participants from a population-based cohort who had self-reported gout in South Australia. Participants completed a survey regarding basic demographics, the Single Item Literacy Screener, use of medication and diet for treatment of their gout and knowledge of gout.
Results: Seventy-four people were recruited (87% male) with a mean age of 66 years (range 35– 88). The mean duration of gout was 16.6 years (range 0– 60). On screening with SILS, 19.0% were identified as having limited reading ability. Most gout was managed by the family practitioner (81.1%) and/or rheumatologist (18.9%). In regard to current gout medications, 52.7% were taking allopurinol, 17.6% colchicine, 9.5% non-steroidal anti-inflammatory drugs, 6.8% prednisolone and 5.4% herbal preparations. For further information regarding gout, participants would most commonly approach their general practitioner (85.1%). Most participants correctly identified certain triggers to gout attacks and almost half of participants (41.9%) reported that they had altered their diet due to gout. Conversely, participants often incorrectly identified common risk or protective factors for gout.
Conclusion: Gout remains a common, yet undertreated, chronic condition. Our study highlights a lack of knowledge amongst patients of risk and protective factors in relation to gout. The increasing prevalence of gout within the population indicates a need to improve education and understanding among those with the condition.
Keywords: gout, patient knowledge, risk factors, protective factors
Introduction
The prevalence of gout has increased globally,1 due to a combination of ageing and increasing prevalence of obesity. This increasing burden of gout has led a call to optimize treatment and management of gout at individual, community and national levels.2,3 Recently,4 lifestyle and dietary factors (such as weight gain, sugary beverages, fruit juice, low fat dairy products) have been linked in epidemiological studies to a modification of risk of gout,5–7 though patient knowledge of these factors is not common.8 In addition, adherence to urate lowering therapy, such as allopurinol, in patients with gout is often low (10–46%), resulting in frequent failure to meet serum uric acid (SUA) targets which are crucial to successful gout management.9,10 Adequate knowledge of gout treatment is likely to enhance adherence, and personalised education with nurse-led programs may facilitate this.11,12
The aim of this study was to determine the knowledge of gout and its treatment among people with gout both in the Australian community and specialist care settings to ultimately allow better provision of improved educational materials for people with gout.
Methods
Participants with gout were recruited three different settings from a hospital rheumatology outpatient department, Arthritis South Australia (a community-based consumer organisation) and a random sample of participants from a population-based cohort study (North West Adelaide Health Study, NWAHS) who had self-reported medically diagnosed gout. The NWAHS is a longitudinal population-based cohort study, and further details of methodology have been described elsewhere.13 In brief, the NWAHS has had three main stages of data collection which have involved questionnaires and a clinic assessment. These were in 1999–2003 (Stage 1), 2004–2006 (Stage 2) and in 2008–2010 (Stage 3). In Stage 3 of the NWAHS, participants were asked “Have you been told by a doctor that you have gout?”. Potential participants for the current study were identified from the NWAHS database in the following manner. A random sample of those who replied positively to this question were identified were contacted and asked to complete the survey. This study complies with the Declaration of Helsinki.
Participants were given a survey regarding basic demographics (age, sex, education levels), the Single Item Literacy Screener (SILS),14 use of medication and diet for treatment of their gout and knowledge of gout (including precipitating factors and management of gout). The survey was developed by a rheumatologist and an epidemiologist (Supplementary Material 1). The survey aimed to test the patient’s knowledge of medication use in the setting of acute gout, knowledge of precipitants and risk factors for gout. In addition, participants were asked whether they had changed their diet due to gout and an open-ended question about dietary changes that they had made.
The study was approved by the Committee for the Ethics of Human Research of the North Western Adelaide Health Service (The Queen Elizabeth Hospital). Each participant gave written informed consent.
Results
Seventy-four participants completed the survey (Supplementary Material 1). Overall, n=19 participants were recruited from a hospital rheumatology outpatient department, n=8 from Arthritis South Australia and n=47 from the random sample of participants from NWAHS who had self-reported gout.
Participant characteristics are shown in Table 1. The participants were predominantly male (86.5%) with mean age of 65.8 years (range 35–88). The mean duration of gout was 16.6 years (range 0–60). On screening with SILS, 19.0% were identified as having limited reading ability. The highest education attainment was primary school (9.5%), secondary school (45.9%) and post-school qualifications (44.6%). For the majority, gout was managed by the general practitioner (81.1%) and/or rheumatologist (18.9%) with 9.5% responding that no doctor was involved in their gout management. With regard to the use of gout medications currently, 52.7% were taking allopurinol, 17.6% colchicine, 9.5% non-steroidal anti-inflammatory drugs (NSAIDs), 6.8% prednisolone and 5.4% herbal preparations. In addition, 16.2% stated that they had previously taken allopurinol and 24.3% colchicine. For acute attacks, a variety of medications were utilized (47.3% NSAIDs, 36.5% colchicine, 9.5% corticosteroids and 23.0% acetaminophen).
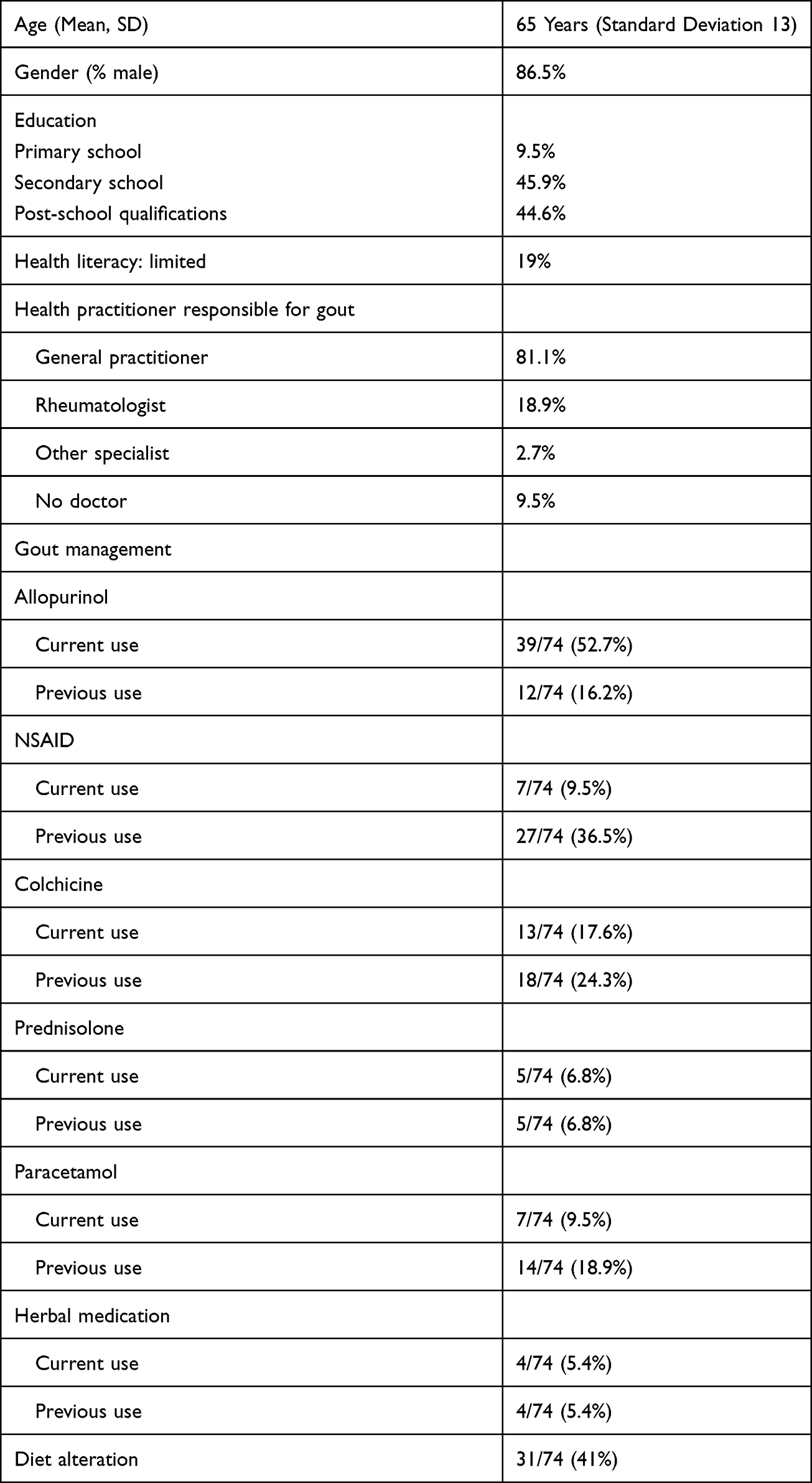 |
Table 1 Baseline Characteristics (n = 74) |
For those who were currently or had previously taken allopurinol (n=51), 82.4% took it daily. As reflected in Table 2, while the majority of participants were aware of the association between uric acid and gout (90.5%), only 55.4% knew that allopurinol reduces uric acid. Although only 7.8% stated that they ceased allopurinol during an acute flare, 52.4% did not state what they did in this situation. For these patients, 49% felt that allopurinol improves their gout, whereupon 5.9% believed it makes gout worse.
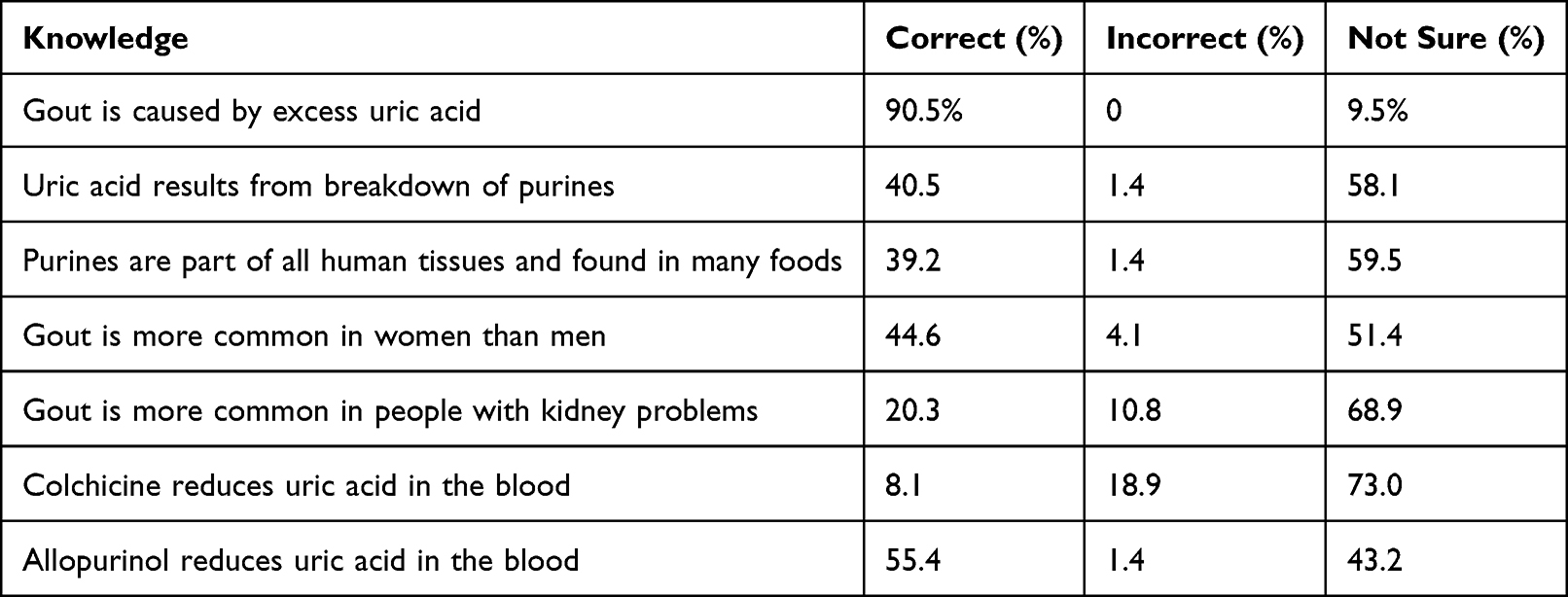 |
Table 2 Knowledge of Gout |
For information regarding gout, participants would approach their general practitioner (85.1%), the Internet (33.8%), local consumer organisation (Arthritis SA) (20.3%) or family/friends (12.2%).
Almost half of participants (41.9%) reported that they had altered their diet due to gout. The primary changes made were related to reducing “acidic food” (primarily tomatoes and citrus), reducing seafood/shellfish intake, reducing red meat intake and alcohol intake.
Most participants correctly identified certain triggers to gout attacks such as excess alcohol and certain purine foods (such as seafood) (Table 3). However, common risk or protective factors for gout were often not correctly identified by participants (eg being overweight, fruit juice, carbonated drinks, low fat dairy products, caffeine-containing beverages) (Table 4). For example, only 40.5% of participants responded that being overweight increased the risk of developing gout.
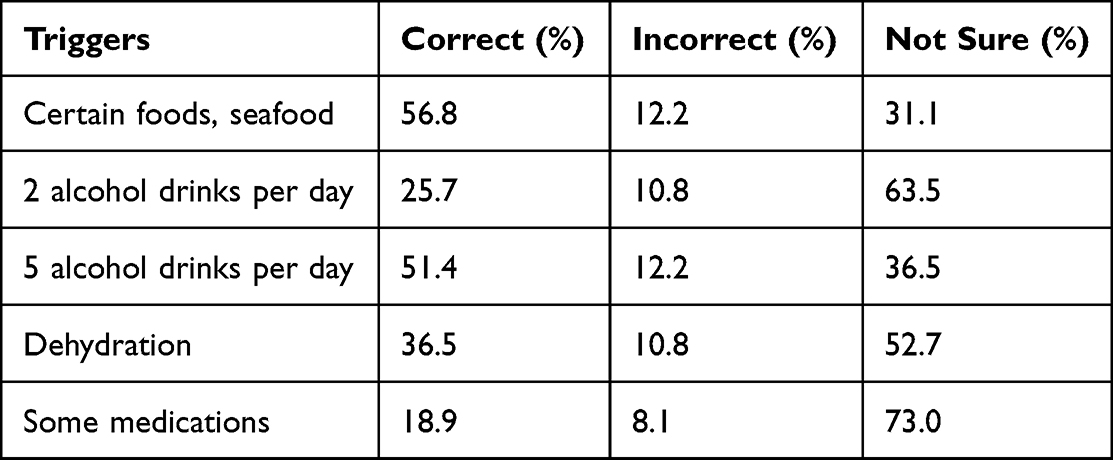 |
Table 3 Knowledge of Triggers of Gout Attacks |
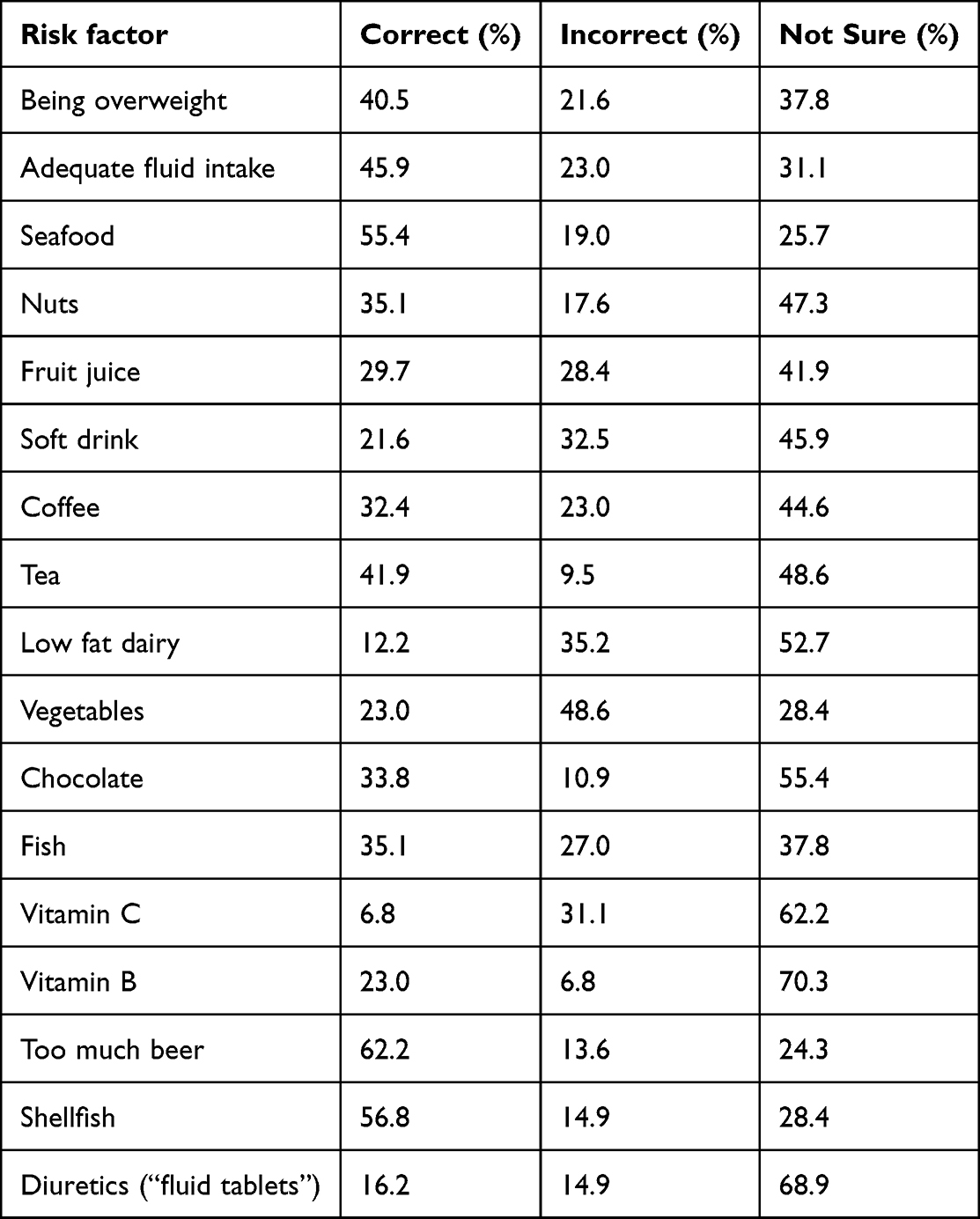 |
Table 4 Knowledge of Risk Factors for Gout |
Discussion
This study which included people with gout from a variety of settings demonstrated that there was lack of awareness of risk factors and protective factors in relation to gout. This supports previous studies suggesting deficits in patient knowledge of dietary triggers of gout, which was seen to be worse in those with active disease.8 It highlights the need to improve education and understanding among those with this chronic condition, which can be debilitating with significant socioeconomic impact.15
This study is strengthened by the inclusion of patients from a variety of settings, including hospital care and the community. Overall, there were similar levels of understanding between the groups of respondents coming from different settings and with different primary treating clinicians. Limitations of this study include potential for self-selection given that participants responding to the survey may reflect a higher health literacy than the general population. A larger study with translated versions of the survey could be utilized in the future to broadening inclusion of patients from different cultural backgrounds and primary languages.
Provision of personalized information and informed shared decision-making in a nurse-led care program in the UK has been found to be efficacious and cost-effective in management of gout with education a primary focus of the trial.12 Use of a gout knowledge survey at gout onset would allow clinicians to determine a patient’s initial knowledge of gout and its management, and subsequently provide individually tailored education. Recently, a novel intervention has been developed using patients as “story-tellers” to improve gout knowledge and medication adherence.16 The development of such innovative modalities for improvement in gout care, particularly those that provide individualized and culturally appropriate material, are required.
In other diseases which require self-management of acute attacks such as asthma, action plans are given to aid patients with direction of how to manage them. Consideration of action plans could be considered in gout.
The concept of treating to a target uric acid level is now well recognized among rheumatologists, and widely accepted as a crucial strategy in managing gout effectively.17,18 Despite this, only approximately half of the patients in our study were receiving urate-lowering therapy, suggesting the need for increased distribution of information and guidelines in the community. A previous longitudinal study has also revealed that medication adherence rates were lower in patients with gout, compared to other chronic conditions.19 Fostering patient education and engagement about current and target serum uric acid levels may therefore increase successful utilization of urate-lowering therapy.
Recent studies have emphasized the role of diet as a risk factor for gout; whereupon alcohol and purine-rich foods such as meat and seafood increase the incidence of gout,6 and increased dairy product consumption has been associated with decreased risk of development of gout.5 However, a recent randomized clinical trial in Australia did not demonstrate any additional benefit on lowering serum uric acid levels at 6 months by providing education on diet,20 noting all these patients were already receiving appropriate urate-lowering therapy.
Conclusion
There is a lack of awareness of risk and protective factors in relation to gout among gout sufferers. This condition can have potentially crippling impacts for individuals, and an increasing prevalence of gout within our population reflects a need to improve education and understanding among patients and their treating clinicians.
Acknowledgments
This article has been reviewed for scientific content and consistency of data interpretation by chief investigators of the North West Adelaide Health Study (NWAHS). The NWAHS team are most grateful for the generosity of the cohort participants in the giving of their time and effort to the study. The NWAHS team also is very appreciative of the work of the clinic, recruiting and research support staff for their substantial contribution to the success of the study.
We thank Ms Jude Sowden for her help with the administration of the survey.
Disclosure
Professor Robert Adams reports grants from National Health and Medical Research Council, grants from The Hospital Research Foundation, grants from ResMed Foundation, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Collaborators. GDaH. Global, regional, and national disability-adjusted life-years (DALYs) for 315 diseases and injuries and healthy life expectancy (HALE), 1990–2015: a systematic analysis for the global burden of disease study 2015. Lancet. 2016;388(10053):1603–1658. doi:10.1016/S0140-6736(16)31460-X
2. Doherty M, Jansen TL, Nuki G, et al. Gout: why is this curable disease so seldom cured? Ann Rheum Dis. 2012;71(11):1765–1770. doi:10.1136/annrheumdis-2012-201687
3. Kuo CF, Grainge MJ, Mallen C, Zhang W, Doherty M. Rising burden of gout in the UK but continuing suboptimal management: a nationwide population study. Ann Rheum Dis. 2015;74(4):661–667. doi:10.1136/annrheumdis-2013-204463
4. Smith E, Hoy D, Cross M, et al. The global burden of gout: estimates from the global burden of disease 2010 study. Ann Rheum Dis. 2014;73(8):1470–1476. doi:10.1136/annrheumdis-2013-204647
5. Choi HK, Atkinson K, Karlson EW, Willett W, Curhan G. Purine-rich foods, dairy and protein intake, and the risk of gout in men. N Engl J Med. 2004;350(11):1093–1103. doi:10.1056/NEJMoa035700
6. Choi HK, Atkinson K, Karlson EW, Willett W, Curhan G. Alcohol intake and risk of incident gout in men: a prospective study. Lancet. 2004;363(9417):1277–1281. doi:10.1016/S0140-6736(04)16000-5
7. Moi JH, Sriranganathan MK, Edwards CJ, Buchbinder R. Lifestyle interventions for chronic gout. Cochrane Database Syst Rev. 2013;2013(5):Cd010039. doi:10.1002/14651858.CD010039.pub2
8. Harrold LR, Mazor KM, Peterson D, Naz N, Firneno C, Yood RA. Patients’ knowledge and beliefs concerning gout and its treatment: a population based study. BMC Musculoskelet Disord. 2012;13(1):180. doi:10.1186/1471-2474-13-180
9. Rashid N, Coburn BW, Wu YL, et al. Modifiable factors associated with allopurinol adherence and outcomes among patients with gout in an integrated healthcare system. J Rheumatol. 2015;42(3):504–512. doi:10.3899/jrheum.140588
10. De Vera MA, Marcotte G, Rai S, Galo JS, Bhole V. Medication adherence in gout: a systematic review. Arthritis Care Res. 2014;66(10):1551–1559. doi:10.1002/acr.22336
11. Fuller A, Jenkins W, Doherty M, Abhishek A. Nurse-led care is preferred over GP-led care of gout and improves gout outcomes: results of Nottingham gout treatment trial follow-up study. Rheumatology. 2020;59(3):575–579. doi:10.1093/rheumatology/kez333
12. Doherty M, Jenkins W, Richardson H, et al. Efficacy and cost-effectiveness of nurse-led care involving education and engagement of patients and a treat-to-target urate-lowering strategy versus usual care for gout: a randomised controlled trial. Lancet. 2018;392(10156):1403–1412. doi:10.1016/S0140-6736(18)32158-5
13. Grant JF, Chittleborough CR, Taylor AW, et al. The north west Adelaide health study: detailed methods and baseline segmentation of a cohort for selected chronic diseases. Epidemiol Perspect Innov. 2006;3(1):4. doi:10.1186/1742-5573-3-4
14. Morris NS, MacLean CD, Chew LD, Littenberg B. The single item literacy screener: evaluation of a brief instrument to identify limited reading ability. BMC Fam Pract. 2006;7(1):21. doi:10.1186/1471-2296-7-21
15. Coleman W, Spencer D, Wong P, Manolios N. An enquiry into the crippling gout affecting pacific islander and maori men in western Sydney. Int J Rheum Dis. 2021;24(11):1394–1401. doi:10.1111/1756-185X.14222
16. Jackson LE, Saag KG, Chiriboga G, et al. A multi-step approach to develop a “storytelling” intervention to improve patient gout knowledge and improve outpatient follow-up. Contemp Clin Trials Commun. 2023;33:101149. doi:10.1016/j.conctc.2023.101149
17. Juraschek SP, Kovell LC, Miller ER, Gelber AC. Gout, urate-lowering therapy, and uric acid levels among adults in the United States. Arthritis Care Res. 2015;67(4):588–592. doi:10.1002/acr.22469
18. Richette P, Doherty M, Pascual E, et al. 2016 updated EULAR evidence-based recommendations for the management of gout. Ann Rheum Dis. 2017;76(1):29–42. doi:10.1136/annrheumdis-2016-209707
19. Briesacher BA, Andrade SE, Fouayzi H, Chan KA. Comparison of drug adherence rates among patients with seven different medical conditions. Pharmacotherapy. 2008;28(4):437–443. doi:10.1592/phco.28.4.437
20. Holland R, McGill NW. Comprehensive dietary education in treated gout patients does not further improve serum urate. Intern Med J. 2015;45(2):189–194. doi:10.1111/imj.12661
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.