")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 17
Gestational Diabetes Mellitus Subtypes Classified by Oral Glucose Tolerance Test and Maternal and Perinatal Outcomes: Results of a Mexican Multicenter Prospective Cohort Study “Cuido Mi Embarazo”
Authors Ortega-Montiel J , Martinez-Juarez LA , Montoya A , Morales-Juárez L, Gallardo-Rincón H, Galicia-Hernández V, Garcia-Cerde R , Ríos-Blancas MJ , Álvarez-Hernández DA , Lomelin-Gascon J, Martínez-Silva G, Illescas-Correa LM, Diaz Martinez DA, Magos Vázquez FJ , Vargas Ávila E, Carmona-Ramos MC, Mújica‐Rosales R , Reyes-Muñoz E , Tapia-Conyer R
Received 2 December 2023
Accepted for publication 16 March 2024
Published 26 March 2024 Volume 2024:17 Pages 1491—1502
DOI https://doi.org/10.2147/DMSO.S450939
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Janinne Ortega-Montiel,1 Luis A Martinez-Juarez,1,2 Alejandra Montoya,1 Linda Morales-Juárez,3 Héctor Gallardo-Rincón,1,4 Victoria Galicia-Hernández,1 Rodrigo Garcia-Cerde,1 María Jesus Ríos-Blancas,1 Diego-Abelardo Álvarez-Hernández,1 Julieta Lomelin-Gascon,1 Gisela Martínez-Silva,1 Lucía M Illescas-Correa,5 Daniel A Diaz Martinez,6 Francisco Javier Magos Vázquez,6 Edwin Vargas Ávila,6 Ma Concepción Carmona-Ramos,7 Ricardo Mújica‐Rosales,1 Enrique Reyes-Muñoz,8 Roberto Tapia-Conyer9
1Carlos Slim Foundation, Mexico City, Mexico; 2Johns Hopkins Center for Humanitarian Health, Bloomberg School of Public Health, Baltimore, MD, USA; 3Institute for Obesity Research, Tecnológico de Monterrey, Mexico City, Mexico; 4Health Sciences University Center, University of Guadalajara, Guadalajara, Jalisco, Mexico; 5Maternal and Childhood Research Center (CIMIGEN), Mexico City, Mexico; 6Ministry of Health of the State of Guanajuato, Tamazuca, Guanajuato, Mexico; 7Ministry of Health of the State of Hidalgo, Pachuca, Hidalgo, Mexico; 8Coordinatión of Gynecological and Perinatal Endocrinology, National Institute of Perinatology Isidro Espinosa de los Reyes, Mexico City, Mexico; 9National Autonomous University of Mexico, School of Medicine, Mexico City, Mexico
Correspondence: Alejandra Montoya, Carlos Slim Foundation, Lago Zurich 245, Presa Falcon Building (Floor 20), Col. Ampliación Granada, Miguel, Hidalgo, Mexico City, 11529, Mexico, Tel +52 55 4976 0344, Email [email protected]
Purpose: This study explores the impact of gestational diabetes mellitus (GDM) subtypes classified by oral glucose tolerance test (OGTT) values on maternal and perinatal outcomes.
Patients and Methods: This multicenter prospective cohort study (May 2019–December 2022) included participants from the Mexican multicenter cohort study Cuido mi Embarazo (CME). Women were classified into four groups per 75-g 2-h OGTT: 1) normal glucose tolerance (normal OGTT), 2) GDM-Sensitivity (isolated abnormal fasting or abnormal fasting in combination with 1-h or 2-h abnormal results), 3) GDM-Secretion (isolated abnormal values at 1-h or 2-h or their combination), and 4) GDM-Mixed (three abnormal values). Cesarean delivery, neonates large for gestational age (LGA), and pre-term birth rates were among the outcomes compared. Between-group comparisons were analyzed using either the t-test, chi-square test, or Fisher’s exact test.
Results: Of 2,056 Mexican pregnant women in the CME cohort, 294 (14.3%) had GDM; 53.7%, 34.4%, and 11.9% were classified as GDM-Sensitivity, GDM-Secretion, and GDM-Mixed subtypes, respectively. Women with GDM were older (p = 0.0001) and more often multiparous (p = 0.119) vs without GDM. Cesarean delivery (63.3%; p = 0.02) and neonate LGA (10.7%; p = 0.078) were higher in the GDM-Mixed group than the overall GDM group (55.6% and 8.4%, respectively). Pre-term birth was more common in the GDM-Sensitivity group than in the overall GDM group (10.2% vs 8.5%, respectively; p=0.022). At 6 months postpartum, prediabetes was more frequent in the GDM-Sensitivity group than in the overall GDM group (31.6% vs 25.5%). Type 2 diabetes was more common in the GDM-Mixed group than in the overall GDM group (10.0% vs 3.3%).
Conclusion: GDM subtypes effectively stratified maternal and perinatal risks. GDM-Mixed subtype increased the risk of cesarean delivery, LGA, and type 2 diabetes postpartum. GDM subtypes may help personalize clinical interventions and optimize maternal and perinatal outcomes.
Keywords: Gestational Diabetes, GDM-Mixed, GDM-Secretion, GDM-Sensitivity, macrosomia, cesarean delivery, pre-term delivery
Introduction
Gestational diabetes mellitus (GDM) is a heterogeneous disease that is identified during pregnancy. It is associated with multiple physiologic changes, including alterations to glucose metabolism, adverse maternal–perinatal outcomes, and long-term cardiometabolic consequences.1,2 According to the Diabetes Atlas published by the International Diabetes Federation, the estimated global prevalence of GDM in 2021 was 16.7%, affecting an estimated 21 million births. Notably, the region encompassing North America and the Caribbean demonstrated a higher GDM prevalence of 20.7%, impacting approximately 1.3 million births.3 In Mexico, the prevalence of GDM has been reported to be between 10%–12%,4 and the multicenter cohort study Cuido mi Embarazo (CME) conducted in Mexico identified a GDM prevalence of 14%.5
At present, the clinical management of GDM follows a uniform approach for all diagnosed women, which involves the use of medication and behavioral therapy.3,6,7 However, different cases of GDM exhibit distinct phenotypes, characteristics, and associated risk factors, warranting more personalized management. Three subtypes of GDM can be defined based on the insulin defect involved.8 “GDM-Sensitivity” may be characterized by an insulin sensitivity defect, “GDM-Secretion” may be characterized as beta cell dysfunction or a defect in insulin secretion, and “GDM-Mixed” involves both a defect in insulin sensitivity and a defect in insulin secretion or beta cell dysfunction. Insulin sensitivity defects are associated with an increased risk of fetal overgrowth and GDM-associated adverse outcomes.9 Moreover, in GDM-Secretion, insulin secretion defects are often associated with an increased risk of hypoglycemia and the potential for future development of type 2 diabetes.10
A favored approach to subclassifying women with GDM involves phenotyping based on three serum glucose concentrations measured using the 2-h 75-g oral glucose tolerance test (OGTT) conducted between 24 and 28 gestational weeks.9,11 The GDM-Sensitivity phenotype presents elevated fasting glucose concentrations, the GDM-Secretion phenotype presents elevated glucose concentrations at 1 and/or 2 h post-load, and the GDM-Mixed phenotype presents both elevated fasting and 2-h post-load glucose concentrations. These manifestations reflect the underlying deterioration in glucose metabolism. The frequency of each GDM subtype is similar across different studies, with GDM-Sensitivity being the most frequent (48–51%), followed by GDM-Secretion (26–30%) and GDM-Mixed (17–20%).8,11
Previous studies have used biomarkers to classify GDM into subtypes, such as homeostatic model assessment based on fasting glucose and insulin measures, the Matsuda insulin sensitivity index, and genotyping biomarkers.12,13 Regardless of the method used, these studies have consistently identified similar groups in terms of the underlying pathways and distribution prevalence. Women with an insulin sensitivity defect (GDM-Sensitivity) often share phenotypic characteristics with those diagnosed with type 2 diabetes, particularly those with severe insulin-resistant diabetes. These phenotypic characteristics are related to overweight or obesity, altered lipid profiles (hypertriglyceridemia), family history of type 2 diabetes, and fasting hyperglycemia.14 Women with an insulin sensitivity defect have also shown a higher incidence of delivering newborns that are considered large for their gestational age, as well as pregnancy-related hypertension, but not higher cesarean delivery rates.15–17 These subtype assessments could facilitate the use of different treatment and monitoring strategies in precision medicine for GDM.
It has been observed that certain metabolic defects may occur after delivery in patients with GDM. For example, there is an elevated risk of developing prediabetes or type 2 diabetes within the first year postpartum. This risk also varies according to the GDM subtype, highlighting the importance of diabetes reclassification at 3–12 months postpartum.13,18
To our knowledge, no studies have been conducted on GDM subtypes in pregnant Mexican women. In this study, we aimed to assess the impact of GDM subtypes based on the results of the OGTT on maternal and perinatal outcomes.
Material and Methods
Study Population
The CME cohort was assessed as part of a prospective multicenter pregnancy study conducted in Mexico, which has been registered with the Research Registry (researchregistry7405).5 The study was performed in accordance with the principles of the Declaration of Helsinki. The study protocol was approved by the Research and Ethics Committees of the Secretary of Health of Hidalgo State (date: September 28, 2018; approval number: FSSA2018076) and the Secretary of Health of Guanajuato State (date: February 04, 2020; approval number: CONBIOETICA-11-CEI-003-20,190,704), and all participants provided written informed consent. Patients were recruited between May 2019 and December 2022 from six primary healthcare centers in three Mexican states: Hidalgo, Guanajuato, and Mexico City. Other studies using the data from the CME cohort study have been published previously.19–24 We analyzed the 2-h 75-g OGTT results of 2056 Mexican pregnant women between 24 and 28 weeks of gestation, without a prior diagnosis of type 2 diabetes, from the CME cohort study.
Data Collection and Laboratory Assessments
Data on sociodemographic characteristics, medical history, pre-gestational body mass index (BMI), regular antenatal visits, laboratory and ultrasound results, pregnancy resolution, and management of self-monitoring for GDM were collected and managed using REDCap electronic data capture tools.25
In accordance with the criteria set by the International Association of the Diabetes and Pregnancy Study Groups (IADPSG), patients at 24–28 weeks of gestation underwent a standard 2-h 75-g OGTT in the morning after an overnight fast lasting for at least 8 h.1 Antenatal medical attention was provided to all pregnant women according to the Mexican Official Norm: NOM-007-SSA2-2016,26 ensuring regular visits, maternal weight measurement, blood pressure monitoring, identification of pregnancy alarm signs, and collection of urine test strips for rapid testing.
Metabolic Postpartum Reclassification
All women with GDM were recommended to undergo metabolic reclassification at 6–12 weeks postpartum to screen for prediabetes or new-onset type 2 diabetes according to the 75-g OGTT results spanning a 2-h interval. The reclassification encompassed three possible scenarios: normoglycemia, prediabetes, and type 2 diabetes. For normoglycemia, the fasting glucose concentration should fall to <100 mg/dL (5.6 mmol/L), and the 2-h post-load glucose concentration should be <140 mg/dL (<7.8 mmol/L). Prediabetes was defined by a fasting glucose concentration ranging between 100 mg/dL (5.6 mmol/L) and 125 mg/dL (6.9 mmol/L), and/or a 2-h post-load concentration between 140 mg/dL (7.8 mmol/L) and 199 mg/dL (11.1 mmol/L). A diagnosis of type 2 diabetes was made if the fasting glucose concentration was ≥126 mg/dL (≥7.0 mmol/L) and/or the 2-h post-load concentration was >200 mg/dL (11.1 mmol/L).
In situations where a woman did not seek consultation between 6 and 12 weeks post-pregnancy, the reclassification was performed between 13 weeks to 1 year after delivery. This reclassification utilizes either the fasting glucose concentration or hemoglobin A1c measurements. Hemoglobin A1c-based reclassification specifies that a value of <5.7% is considered normal, prediabetes is classified between 5.7% and 6.4%, and ≥6.5% warrants a diagnosis of type 2 diabetes.27
Definitions
GDM was diagnosed following the IADPSG and American Diabetes Association criteria. According to these criteria, a diagnosis was established if any single plasma glucose measurement met or exceeded the following thresholds during the OGTT: fasting ≥92 mg/dL (5.1 mmol/L); 1-h ≥180 mg/dL (10.0 mmol/L); and 2-h ≥153 mg/dL (8.5 mmol/L).1,3
Based on the OGTT results, women diagnosed with GDM were classified into four distinct GDM subtypes; 1) normal glucose tolerance (normal OGTT values), 2) GDM-Sensitivity (elevated fasting blood glucose [first], whether this was the sole altered concentration or combined with 1-h [second] or 2-h [third] post-load glucose elevation [1, 1–2, 1–3]); 3) GDM-Secretion (elevated 1- and/or 2-h post-load glucose concentrations [2, 3, 2–3], with a normal fasting glucose concentration); and 4) GDM-Mixed (when all three glucose concentrations [fasting and two post-load concentrations] were elevated [1-2-3]).9
Macrosomia was established in neonates with a birth weight of ≥4,000 g. Women were considered multiparous if they had completed two or more deliveries. Small for gestational age (SGA) was defined as live births weighing less than the 10th percentile compared with infants of the same gestational age and sex. Large for gestational age (LGA) was defined as live births weighing more than the 90th percentile compared with infants of the same gestational age and sex.28
Statistical Analysis
Patients’ characteristics and biomarkers were compared between the GDM subtypes and the non-GDM group. Continuous variables were presented as the mean ± standard deviation, and categorical variables were presented as frequency (%).
Patients’ characteristics were compared between the non-GDM and the GDM groups, as well as among the GDM subtypes, using the t-test or analysis of variance for continuous variables and the chi-square test for categorical variables. Bonferroni-adjusted p values were generated for these pairwise comparisons. Fisher’s exact test was used to compare categorical pregnancy and perinatal outcome variables among the GDM subtypes. The linear regression model was used to examine the effect of the fasting glucose concentration on the 1-h post-load glucose concentration, and the effect of the 1-h post-load glucose concentration on the 2-h post-load glucose concentration measured with the OGTT according to the GDM subtypes. The data were analyzed using STATA software, version 17.0 (College Station, TX, USA).
Results
Baseline Characteristics According to GDM Diagnoses and Subtypes
Of the 2056 Mexican pregnant women in the CME cohort, the overall prevalence of GDM was 14.3%. Based on the OGTT results, 158 women were classified as GDM-Sensitivity (53.7%), 101 as GDM-Secretion (34.4%), and 35 as GDM-Mixed (11.9%). A scatter plot of the total fasting serum glucose and 1-h post-load glucose concentrations at the time of OGTT revealed a distribution pattern within each quadrant, which was used to identify the subtypes (Figure 1).
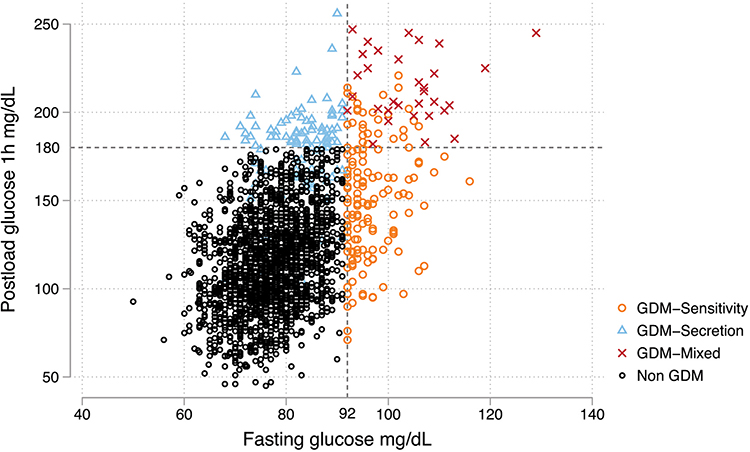 |
Figure 1 Distribution of fasting and 1-h post-load glucose concentrations in the non-GDM and GDM groups by subtype. The distribution of fasting plasma glucose (x-axis) and 1-h post-load glucose (y-axis) concentrations during the oral glucose tolerance test for each pregnant woman is shown. Each symbol represents an individual woman, with different symbols or colors indicating GDM subtypes and non-GDM. The dotted lines indicate the cut-off point for the diagnosis of GDM according to the American Diabetes Association standard. Any significant trends in the findings shown in the figure (eg, a higher proportion of GDM women above the cut-off point) are also noted. Abbreviations: GDM, gestational diabetes mellitus. |
In general, women with GDM were older than women without GDM (28.7 ± 6.5 vs 25.2 ± 6.1 years, p = 0.0001), and women with GDM-Mixed were the oldest (31.1 ± 6.5 years, p = 0.001). Women with GDM were more often multiparous (14.4% vs 11.2%, p = 0.119) and more frequently had a family history of type 2 diabetes (44.0% vs 25.2%, p = 0.0001) than women without GDM. In terms of education, no significant differences were found between the GDM and non-GDM groups. In the GDM group, 50.3% had at least basic education, and 32.6% were educated to high school level. Around 16% reported having higher education, and 1.0% had no education. Family history of type 2 diabetes was most prevalent in the GDM-Secretion group (51.0%, p = 0.0001). Regarding pre-gestational BMI, women with GDM had a higher prevalence of overweight or obesity before pregnancy than women without GDM (37.9% vs 30.9% and 30.0% vs 15.0%, respectively, p = 0.0001). However, a higher prevalence of overweight was observed in the GDM-Sensitivity (37.0%) and GDM-Secretion (43.6%) groups than in the GDM-Mixed group (25.7%) (p = 0.0001), and a higher prevalence of obesity was observed in women with GDM-Mixed (42.9%, p = 0.001) than in the other two GDM subtypes (Table 1).
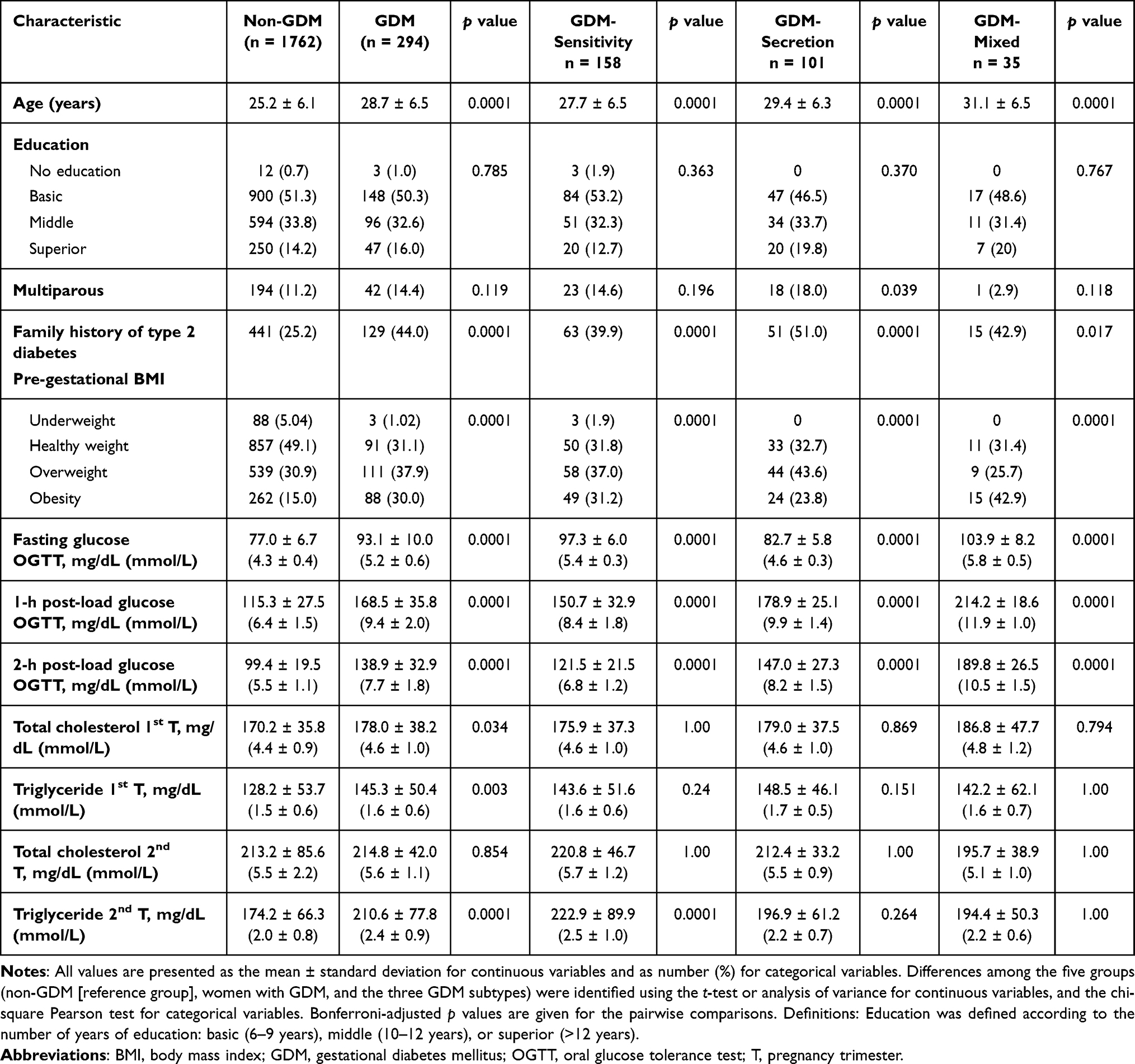 |
Table 1 Comparison of Demographic and Clinical Characteristics Among the Non-GDM, GDM, and GDM Subtype Groups |
Glucose metabolism can be assessed through all three concentrations of the OGTT (fasting, 1-h, and 2-h concentrations) among the GDM subtypes. The GDM-Sensitivity subtype was characterized by an elevated fasting glucose concentration (97.3 ± 6.0 mg/dL [5.4 ± 0.3 mmol/L]) compared with the GDM-Secretion subtype. Conversely, the GDM-Secretion subtype showed elevated 1-h and 2-h post-load glucose concentrations (178.9 ± 25.1 mg/dL [9.9 ± 1.4 mmol/L] and 147.0 ± 27.3 mg/dL [8.2 ± 1.5 mmol/L], respectively) when compared with the GDM-Sensitivity subtype. Women with the GDM-Mixed subtype demonstrated higher glucose concentrations, both fasting and post-load, than the other GDM subtypes (fasting: 103.9 ± 8.2 mg/dL [5.8 ± 0.5 mmol/L]; 1-h: 214.2 ± 18.6 mg/dL [11.9 ± 1.0 mmol/L]; 2-h: 189.8 ± 26.5 mg/dL [10.5 ± 1.5 mmol/L]; p = 0.0001).
We measured the total cholesterol (TC) concentration in 726 women (non-GDM: n = 612/GDM: n = 114) and the triglyceride (TG) concentration in 636 women (non-GDM: n = 533/GDM: n = 103) in the first trimester of pregnancy. In the second trimester, the TC concentration was measured in 792 women (non-GDM: n = 671/GDM: n = 121) and the TG concentration in 736 women (non-GDM: n = 623/GDM: n = 113). Women with GDM had higher TC and TG concentrations than women classed as non-GDM in the first trimester (TC: 178.0 ± 38.2 mg/dL [4.6 ± 1.0 mmol/L], p = 0.034; TG: 145.3 ± 50.4 mg/dL [1.6 ± 0.6 mmol/L], p = 0.003), as well as a higher TG concentration in the second trimester (TG: 210.6 ± 77.8 mg/dL [2.4 ± 0.9 mmol/L], p = 0.0001). The most significant increase in serum TG concentration from the first trimester to the second trimester was observed for the GDM-Sensitivity subtype (143.6 ± 51.6 mg/dL [1.6 ± 0.6 mmol/L] to 222.9 ± 89.9 mg/dL [2.5 ± 1.0 mmol/L], p = 0.0001), demonstrating the adverse metabolic profile of this subtype (Table 1).
We analyzed the glucose kinetics for each GDM subtype during the OGTT. Regarding the relationship between fasting serum glucose and 1-h post-load serum glucose (Figure 2A), the strongest positive correlation was observed in women with GDM-Sensitivity (b = 1.31, p = 0.02), followed by women with GDM-Secretion (b = 0.99, p = 0.02). In contrast, the correlation between the 1-hpost-load serum glucose and the 2-h post-load serum glucose (Figure 2B) remained positive for the GDM-Sensitivity subtype, albeit less pronounced (b = 0.25, p = 0.001). In contrast, the correlation in the GDM-Secretion subtype was negative (b = −0.33, p = 0.002). In the GDM-Mixed subtype, a positive correlation was observed between the 1-h post-load glucose and the 2-h post-load glucose (b = 0.61, p = 0.01), and this group tended to have higher glucose concentrations for the three measurements of the OGTT (Figure 2B).
 |
Figure 2 Relationship of fasting and post-load glucose concentrations among the GDM subtypes.The glucose kinetics for each GDM subtype during the oral glucose tolerance test are shown. Each symbol represents an individual woman, with different symbols or colors indicating different GDM subtypes. (A) shows the effect of fasting plasma glucose on 1-h post-load glucose within each GDM subtype. (B) shows the effect of 1-h post-load glucose on 2-h post-load glucose within each GDM subtype. The respective linear regression coefficients are shown, indicating the strength and direction of the relationship between the glucose concentrations, with p values shown in parentheses. Any significant trends in the findings shown in the figure (eg, a stronger relationship in certain GDM subtypes) are also highlighted. Abbreviations: GDM, gestational diabetes mellitus. |
Delivery and Perinatal Outcomes
At the time of this analysis, we had obtained data from 78.7% of mother-child binomials in our active cohort, including 77.8% without GDM and 85.0% with GDM (Table 2).
 |
Table 2 Comparison of Perinatal Outcomes Among the Non-GDM, GDM, and GDM Subtype Groups |
The prevalence of cesarean delivery was higher in women with GDM (55.6%) than in women classified as non-GDM (p = 0.0001), and higher still in women with GDM-Secretion and GDM-Mixed (60.6% and 63.3%, respectively).
We analyzed data from 1620 newborns, focusing on gestational age, SGA, LGA, and macrosomic outcomes. In the context of gestational age, both pre-term and post-term births were more prevalent in the GDM group than in the non-GDM group. Specifically, pre-term births accounted for 8.5% of the GDM group and 4.7% of the non-GDM group (p = 0.003), while post-term births accounted for 2.0% of the GDM group and 0.6% of the non-GDM group (p = 0.003). When analyzed by GDM subtype, the highest prevalence of pre-term birth was observed in the GDM-Sensitivity group (10.2%, p = 0.022), while the highest prevalence of post-term birth was observed in the GDM-Mixed group (7.1%, p = 0.0001). The prevalence of SGA was 11.9%–16.7%, with no significant differences observed among the three GDM subtypes. The prevalence of newborns with LGA was higher in the group with GDM (8.4%) than in the non-GDM group (4.0%) (p = 0.003), particularly among those with GDM-Mixed (10.7%, p = 0.078) compared with the other GDM subtypes. The prevalence of macrosomia was 2.4% in the GDM group and 0.9% in the non-GDM group (p = 0.050).
Postpartum Reclassification
For GDM postpartum reclassification, we analyzed the postpartum OGTT results of 62.6% (184 of 294) of women with GDM during the cohort follow-up. The prevalence of prediabetes was 25.5%, and the diagnosis of type 2 diabetes de novo was 3.3%. Interesting patterns were observed in the diagnosis reclassification according to GDM subtype. The highest prevalence of transition to normal glucose metabolism was seen in women with GDM-Secretion (81.2%), whereas 31.6% of women with GDM-Sensitivity remained with prediabetes. However, the most concerning outcome was observed in women with GDM-Mixed, who had the highest prevalence of reclassification to type 2 diabetes (10.0%, p = 0.197) (Table 3).
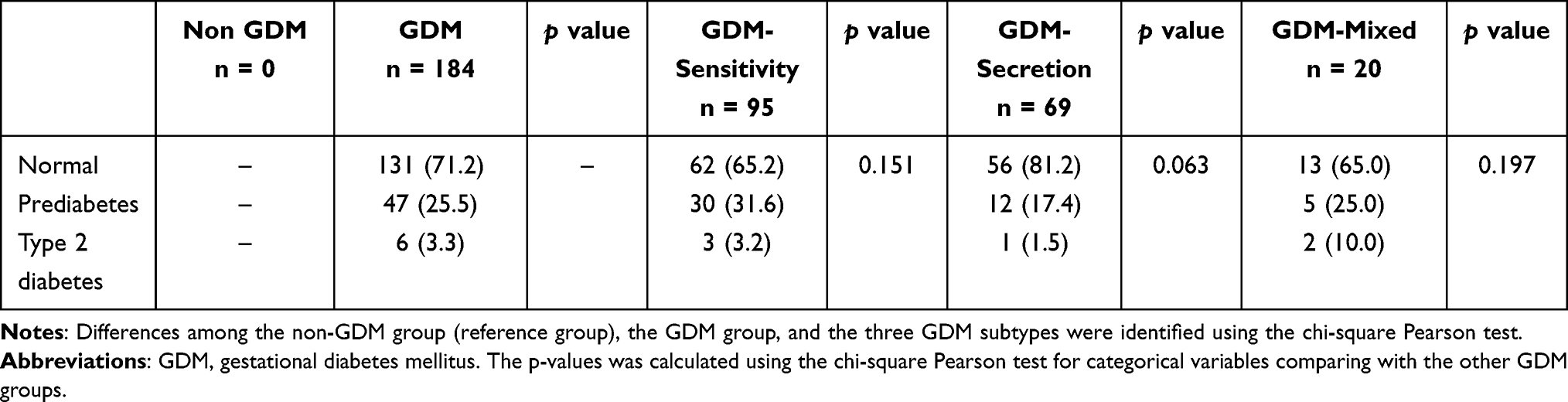 |
Table 3 Postpartum Reclassification of GDM |
Discussion
In this study, we identified the incidence of GDM subtypes according to abnormal results of OGTT among pregnant Mexican women. We observed higher rates of cesarean delivery and LGA neonates in women classified as GDM-Mixed than in the overall GDM group. Pre-term birth was more common in women classified as GDM-Sensitivity than in the overall GDM group. At 6 weeks postpartum, prediabetes was more frequent in the GDM-Sensitivity group than in the overall GDM group, whereas type 2 diabetes was more common in the GDM-Mixed group than in the overall GDM group.
More than half of the 294 women with GDM had an insulin sensitivity defect (53.7%), while 34.4% had an insulin secretion defect (GDM-Secretion). This prevalence distribution is similar to that reported by Powe et al8 in US women and by Retnakaran et al13 in Canadian women. However, we found a lower prevalence of both insulin defects (GDM-Mixed: 11.9%) than that reported by Kotzaeridi et al11 in women from Vienna and by Layton et al16 from the Gen3G cohort from Canada. The high proportion of GDM diagnoses with normal fasting glucose concentrations (GDM-Secretion 34.4%) underscores the importance of offering a complete OGTT with fasting, 1-h post-load, and 2-h post-load glucose concentration measurements.
By identifying these GDM subtypes, we observed differences in clinical risk characteristics, such as older age and family history of type 2 diabetes. Furthermore, pre-gestational BMI, which is often used as a proxy of metabolic status before pregnancy, was higher in women with GDM-Sensitivity and GDM-Mixed, showing a higher prevalence of overweight and obesity. This finding aligns with those of Li et al and Wang et al29–31 who reported that women with GDM-Dysfunction had higher pre-gestational BMI values and a higher risk of giving birth to an infant with macrosomia or an infant considered LGA. Powe et al8 presented a genotype-based approach to identify GDM subtypes, where they showed a polygenic score for type 2 diabetes in pregnant women with an insulin sensitivity defect, making them more susceptible to developing GDM with higher fasting glucose (GDM-Sensitivity).
We found that women in the GDM-Mixed group showed adverse metabolic profiles at the beginning of pregnancy compared with women classed as non-GDM or women with a single insulin defect. Regarding the maternal lipid profile, we showed that women with GDM had higher TC and TG concentrations in the first trimester, and that the elevated TG concentration persisted in the second trimester. However, there was heterogeneity among the GDM subtypes, with the highest TG concentrations observed in the GDM-Sensitivity group. This result is similar to the finding of Layton et al,16 who showed differences in high-density lipoprotein, low-density lipoprotein, and non-esterified fatty acid concentrations between GDM subtypes. However, TG concentrations have previously been demonstrated as a risk factor for the development of GDM-Resistance (odds ratio [OR] 1.8, 95% CI 1.2–2.6) and GDM-Mixed (OR 2.06, 95% CI 1.3–3.17).28
Several studies have assessed glucose metabolism in women with GDM of different physiological subtypes.32–34 Liu et al33 demonstrated the dynamic responses of glucose and insulin at different time points. Women with GDM-Mixed presented with higher glucose and insulin concentrations, similar to our findings in Figure 2. The most significant increase in glucose at 60 minutes was observed in the GDM-Resistance group. In the present study, we showed a strong positive correlation between the fasting and 1-h post-load glucose concentrations. Conversely, a more significant decrease in glucose at 120 minutes was observed in the GDM-Dysfunction group in Liu et al’s study.33 In the present study, we showed a negative correlation between the 1-h post-load and the 2-h post-load glucose concentrations in the GDM-Secretion group. This suggests that these women had better beta cell responsiveness in the late phase after the OGTT.
In the present study, women with GDM had a higher frequency of cesarean delivery than women classed as non-GDM. This trend was even more pronounced in women with GDM-Mixed (63.3%, p = 0.016). This is a common outcome described in other studies and is often associated with other maternal outcomes, such as preeclampsia and induced labor.29,34 Our results indicate that adverse maternal outcomes can also impact newborns. In our population, pre-term birth was common, with specific heterogeneity among the GDM subtypes. Moreover, we observed that the prevalence of LGA in newborns was higher in women with GDM, specifically in the GDM-Sensitivity group, which is consistent with other studies that used LGA as a perinatal outcome, where maternal obesity, hyperglycemia, and hyperinsulinemia may have contributed to the increased risk.15,33
More than half of the women in the present study developed GDM during pregnancy, largely due to risk factors that were present before conception. Only one third of GDM cases could be attributed to placental mechanisms. This highlights the clinical importance of offering personalized and timely management to minimize adverse perinatal and newborn outcomes.
Early and accurate identification of GDM subtypes is crucial for providing personalized management and enhancing maternal and perinatal outcomes. Our findings underscore the importance of considering GDM heterogeneity in clinical practice and public health. By distinguishing between GDM subtypes, clinicians can customize management interventions, such as tailored nutrition plans, exercise regimes, and adequate medication, to address the specific underlying mechanism of each GDM subtype. This personalized approach has the potential to somewhat mitigate the risks associated with GDM, including cesarean delivery, pre-term birth, and the postpartum development of type 2 diabetes.
Given the well-established risk of negative pregnancy outcomes and long-term cardiovascular complications, such as arterial hypertension, in women with GDM,18,35,36 therapeutic management should prioritize long-term metabolic monitoring. This approach would ensure that every woman diagnosed with GDM undergoes a 75-g OGTT within the first 6 months post-delivery as a mandatory policy. Our findings suggest that the metabolic trajectory of these women may vary based on the GDM subtype during pregnancy. Therefore, a comprehensive evaluation of the metabolic evolution of these women is crucial to prevent the development of chronic diseases at an early age. These diseases not only impact the individual’s quality of life, but they also place a significant burden on the healthcare system. Despite the current social and resource barriers, health systems must prioritize the implementation of these practices to provide optimal long-term care for this vulnerable population. In this study, only glucose measurements were performed; therefore, studies examining the more widespread complications of GDM, such as cardiovascular complications, should be performed in the future.
Based on our analysis, this study’s primary strengths lie in its novel approach to classifying GDM subtypes through OGTT results as this methodology enhances our understanding of distinct risk profiles while informing personalized management strategies. The multicenter, prospective cohort design, which encompasses a substantial sample size from diverse Mexican regions, ensures the robustness and generalizability of our findings. Moreover, the study underscores the importance of early and accurate GDM subtype identification in optimizing maternal and perinatal outcomes. By advocating for tailored clinical interventions, our research contributes to advancing precision medicine in GDM care, highlighting the potential for improved health outcomes in pregnant women and their infants. Together, these strengths collectively show our study’s significant contribution to the field of GDM.
However, this study has several limitations that should be considered when interpreting the findings. First, we did not follow the long-term metabolic trajectories of women with GDM, which is crucial given the established link between GDM and future cardiovascular complications. Longitudinal studies that consider the GDM subtype present during pregnancy should be conducted. Second, unlike previous studies conducted by Powe et al,8,9 we did not measure insulin during the OGTT. Nevertheless, the authors of those studies noted that glucose behavior aligns well with GDM subtypes. Finally, the present study exclusively involved Mexican women, which could limit the generalizability of the findings to other settings.
Conclusion
This analysis of the CME cohort highlighted the heterogeneity in GDM subtypes within the Mexican population, which were associated with different maternal and perinatal outcomes. The GDM-Mixed subtype was associated with a greater likelihood of cesarean delivery, LGA neonates, and type 2 diabetes postpartum, emphasizing the importance of subtype-specific clinical management of GDM and aligning with the principles of personalized medicine. Such a tailored approach could help optimize maternal and perinatal outcomes and reduce postpartum complications.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
We acknowledge the support of the Centre for Maternal and Infant Research (CIMIGEN) and the Ministry of Health of the States of Hidalgo and Guanajuato for their help in performing this study. We thank Emily Woodhouse, PhD, of Edanz (www.edanz.com) for providing editorial support, which was funded by Fundación Carlos Slim, in accordance with Good Publication Practice (GPP) 2022 guidelines (https://www.ismpp.org/gpp-2022). Parts of this work were presented at the 82nd Scientific Sessions of the American Diabetes Association, New Orleans, LA, 3–7 June 2022.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Global Health Partnership Eli Lilly and Company. The funder was not involved in the study design; collection, analysis, or interpretation of data; writing of the report; or the decision to submit the paper for publication. Carlos Slim Foundation developed the study design, analysis, and interpretation of data and was involved in writing the paper.
Disclosure
No potential conflicts of interest relevant to this article were reported.
References
1. El Sayed NA, Aleppo G, Aroda VR. American Diabetes Association, et al. Classification and diagnosis of diabetes: standards of care in diabetes-2023. Diabetes Care. 2023; 46:S19–S40.
2. Lee SM, Shivakumar M, Park JW, et al. Long-term cardiovascular outcomes of gestational diabetes mellitus: a prospective UK Biobank study. Cardiovasc Diabetol. 2022;21(1):221. doi:10.1186/s12933-022-01663-w
3. International Diabetes Federation. IDF Diabetes Atlas,
4. Medina-Pérez EA, Sánchez-Reyes TO, Hernández-Peredo AR, et al. Gestational diabetes mellitus. Diagnosis and treatment in the first level of care. Internal Med Mexico. 2017;33:91–98.
5. Gallardo-Rincón H, Lomelin-Gascon J, Martinez-Juarez LA, et al. Diagnostic accuracy of capillary blood glucometer testing for gestational diabetes. Diabetes Metab Syndr Obes. 2022;15:3855–3870. doi:10.2147/DMSO.S389420
6. Centro Nacional de Equidad de Género y Salud Reproductiva. Diabetes y embarazo: lineamiento técnico [diabetes and pregnancy: technical guidelines]. Available from: http://cnegsr.salud.gob.mx/contenidos/descargas/SMP/LineamientoDiabetesyEmbarazo.pdf.
7. McIntyre HD, Catalano P, Zhang C, Desoye G, Mathiesen ER, Damm P. Gestational diabetes mellitus. Nat Rev Dis Prim. 2019;5(1):47. doi:10.1038/s41572-019-0098-8
8. Powe CE, Hivert MF, Udler MS. Defining heterogeneity among women with gestational diabetes mellitus. Diabetes. 2020;69(10):2064–2074. doi:10.2337/dbi20-0004
9. Powe CE, Allard C, Battista MC, et al. Heterogeneous contribution of insulin sensitivity and secretion defects to gestational diabetes mellitus. Diabetes Care. 2016;39(6):1052–1055. doi:10.2337/dc15-2672
10. Homko CJ, Sivan E, Reece AE. Is there a role for oral antihyperglycemics in gestational diabetes and type 2 diabetes during pregnancy? Treat Endocrinol. 2004;3(3):133–139. doi:10.2165/00024677-200403030-00001
11. Kotzaeridi G, Blätter J, Eppel D, et al. Characteristics of gestational diabetes subtypes classified by oral glucose test values. Eur J Clin Invest. 2021;51(51):e13628. doi:10.1111/eci.13628
12. Feghali MN, Atlass J, Ribar E, Caritis SN, Simhan H, Scifres CM. 82: subtypes of gestational diabetes mellitus based on mechanisms of hyperglycemia. Am J Obstet Gynecol. 2019;220(1):S66. doi:10.1016/j.ajog.2018.11.091
13. Retnakaran R, Ye C, Hanley AJ, Connelly PW, Sermer M, Zinman B. Subtypes of gestational diabetes and future risk of pre-diabetes or diabetes. EClinicalMedicine. 2021;40:101087. doi:10.1016/j.eclinm.2021.101087
14. Ahlqvist E, Storm P, Käräjämäki A, et al. Novel subgroups of adult-onset diabetes and their association with outcomes: a data-driven cluster analysis of six variables. Lancet Diabetes Endocrinol. 2018;6(5):361–369. doi:10.1016/S2213-8587(18)30051-2
15. Selen DJ, Edelson PK, James K, et al. Physiological subtypes of gestational glucose intolerance and risk of adverse pregnancy outcomes. Am J Obstet Gynecol. 2022;226(2):241.e1–241.e14. doi:10.1016/j.ajog.2021.08.016
16. Layton J, Powe C, Allard C, et al. Maternal lipid profile differs by gestational diabetes physiologic subtype. Metab Clin Exp. 2019;91:39–42. doi:10.1016/j.metabol.2018.11.008
17. Cosson E, Bentounes SA, Nachtergaele C, et al. Prognosis associated with sub-types of hyperglycaemia in pregnancy. J Clin Med. 2021;10(17):3904. doi:10.3390/jcm10173904
18. Park S, Kim S. Women with rigorously managed overt diabetes during pregnancy do not experience adverse infant outcomes but do remain at serious risk of postpartum diabetes. Endocr J. 2015;62(4):319–327. doi:10.1507/endocrj.EJ14-0529
19. Gallardo-Rincón H, Lomelin J, Martinez-Juarez LA, et al. 1358-P: point of care OGTT for the screening of gestational diabetes: a feasible proposal for low-resource settings. Diabetes. 2020;69(Supplement_1)(Supplement_1):1358–P. doi:10.2337/db20-1358-P
20. Gallardo-Rincón H, Ortega-Montiel J, Martinez-Juarez LA, et al. 1065-P: the use of OGTT and phenotypic characteristics to identify GDM subtypes in Mexican women, an approach towards precision medicine. Diabetes. 2022;71(Supplement_1):1065–P. doi:10.2337/db22-1065-P
21. Gallardo-Rincón H, Ríos-Blancas MJ, Ortega-Montiel J, et al. MIDO GDM: an innovative artificial intelligence‑based prediction model for the development of gestational diabetes in Mexican women. Sci Rep. 2023;13(1):6992. doi:10.1038/s41598-023-34126-7
22. Martinez-Juarez LA, Lomelin J, Ortega-Montiel J, et al. 1280-PUB: the impact of proactive and personalized strategies in the self-monitoring of blood glucose in women with diabetes in pregnancy: the experience of the cohort cuido mi embarazo in Mexico. Diabetes. 2021;70(Suppl 1):1280–PUB. doi:10.2337/db21-1280-PUB
23. Martinez-Juarez LA, Gallardo-Rincón H, Montoya A, et al. 1836-PUB: the use of OGTT and phenotypic characteristics to identify GDM subtypes in Mexican women, an approach towards precision medicine. Diabetes. 2023;72(Supplement_1):1836–PUB.
24. Zulueta M, Gallardo-Rincón H, Martinez-Juarez LA, et al. Development and validation of a multivariable genotype-informed gestational diabetes prediction algorithm for clinical use in the Mexican population: insights into susceptibility mechanisms. BMJ Open Diabetes Res Care. 2023;11(2):e003046. doi:10.1136/bmjdrc-2022-003046
25. Harris PA, Taylor R, Minor BL, et al. REDCap consortium. the REDCap consortium: building an international community of software platform partners. J Biomed Inform. 2019;95:103208. doi:10.1016/j.jbi.2019.103208
26. Diario Oficial de la Federación. Norma Oficial Mexicana NOM-007-SSA2-2016, para la atención de la mujer durante el embarazo, parto y puerperio, y de la persona recién nacida. Available from: https://www.dof.gob.mx/nota_detalle.php?codigo=5432289&fecha=07/04/2016#gsc.tab=0.
27. ElSayed NA, Aleppo G, Aroda VR, et al. 15. management of diabetes in pregnancy: standards of care in diabetes—2023. Diabetes Care. 2023;46:(S254–S266).
28. Flores HS, Martínez SH. Birth weight of male and female infants born in hospitals affiliated with the instituto Mexicano del seguro social. Bol Med Hosp Infant Mex. 2012;69:30–39.
29. Li Z, Cheng Y, Wang D, et al. Incidence rate of type 2 diabetes mellitus after gestational diabetes mellitus: a systematic review and meta-analysis of 170,139 women. J Diabetes Res. 2020;2020:3076463. doi:10.1155/2020/3076463
30. Wang N, Peng Y, Wang L, et al. Risk factors screening for gestational diabetes mellitus heterogeneity in Chinese pregnant women: a case–control study. Diabetes Metab Syndr Obes. 2021;14:951–961. doi:10.2147/DMSO.S295071
31. Wang N, Song L, Sun B, et al. Contribution of gestational diabetes mellitus heterogeneity and prepregnancy body mass index to large-for-gestational-age infants—a retrospective case-control study. J Diabetes. 2021;13(4):307–317. doi:10.1111/1753-0407.13113
32. Shao B, Mo M, Xin X, et al. The interaction between prepregnancy BMI and gestational vitamin D deficiency on the risk of gestational diabetes mellitus subtypes with elevated fasting blood glucose. Clin Nutr. 2020;39(7):2265–2273. doi:10.1016/j.clnu.2019.10.015
33. Liu Y, Hou W, Meng X, et al. Heterogeneity of insulin resistance and beta cell dysfunction in gestational diabetes mellitus: a prospective cohort study of perinatal outcomes. J Transl Med. 2018;16(1):289. doi:10.1186/s12967-018-1666-5
34. Plows JF, Stanley JL, Baker PN, Reynolds CM, Vickers MH. The pathophysiology of gestational diabetes mellitus. Int J Mol Sci. 2018;19(11):3342. doi:10.3390/ijms19113342
35. Benhalima K, Van Crombrugge P, Moyson C, et al. Characteristics and pregnancy outcomes across gestational diabetes mellitus subtypes based on insulin resistance. Diabetologia. 2019;62(11):2118–2128. doi:10.1007/s00125-019-4961-7
36. Yerlikaya G, Falcone V, Stopp T, et al. To predict the requirement of pharmacotherapy by OGTT glucose levels in women with GDM classified by the IADPSG criteria. J Diabetes Res. 2018;2018:3243754. doi:10.1155/2018/3243754
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.