")
Back to Journals » Journal of Healthcare Leadership » Volume 16
Gender-Related Microaggressions in Orthopedic Surgery: A Comprehensive Survey of Women Orthopedists and Implications for Progress, Saudi Arabia
Authors Alhammadi NA, Al Jabbar I , Alahmari SA, Alqahtani RM, Alhadi WA, Alnujaymi BM, Al-Jakhaideb MM, Almoghamer HD, Alqahtani MS, Mahmood SE
Received 25 August 2023
Accepted for publication 22 November 2023
Published 8 January 2024 Volume 2024:16 Pages 29—37
DOI https://doi.org/10.2147/JHL.S437083
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Zhanming Liang
Nouf A Alhammadi,1,* Imtinan Al Jabbar,2,* Seham A Alahmari,2,* Rawan M Alqahtani,2,* Wajd A Alhadi,2,* Bayan M Alnujaymi,2,* Miran M Al-Jakhaideb,2,* Hanan D Almoghamer,2,* Manar S Alqahtani,2,* Syed Esam Mahmood3,*
1Rheumatologist and Lupus Specialist, Department of Medicine, College of Medicine, King Khalid University, Abha, Saudi Arabia; 2College of Medicine, King Khalid University, Abha, Saudi Arabia; 3Department of Family and Community Medicine, College of Medicine, King Khalid University, Abha, Saudi Arabia
*These authors contributed equally to this work
Correspondence: Syed Esam Mahmood, Department of Family and Community Medicine, College of Medicine, King Khalid University, Abha, 62529, Saudi Arabia, Email [email protected]
Background: Microaggressions are subtle and often unintentional acts that can be verbal, nonverbal, or environmental, and they convey negative messages to individuals belonging to marginalized social groups. This study aims to determine the prevalence of microaggressions experienced by female Saudi orthopaedic surgeons.
Methods: This cross-sectional study was conducted online and targeted female in orthopedic surgery across different regions of the Kingdom of Saudi Arabia. The survey was uploaded to Google Forms and distributed through social media platforms like Twitter, Instagram, and WhatsApp by well-trained data collectors.
Results: In this survey we included 96 female Saudi orthopedics. Their mean age was 27.46 ± 12.20 years. Most respondents were either residents (52.63%), or specialists (23.16%). Most participants (92.63%) were still in training or early in their careers, with the vast majority (93.68%) had their residency in Saudi Arabia. Nearly three-fifths (61.05%) have reported experiencing microaggressions as victims, 76.84%, did not see themselves as perpetrators of microaggressions, 23.16% acknowledged having engaged in such behavior. Patients or their families were reported to be involved in microaggressions in 43.16% of cases, while male surgeons and male support staff were implicated at 51.58% and 23.16%, respectively. Additionally, other male medical doctors participate in microaggressions in 33.68% of instances. Female surgeons were identified as being involved in 22.11% of microaggressions, whereas 29.47% involve female support staff.
Conclusion: The study’s outcomes can help inform strategies to promote a supportive and inclusive environment within the field of orthopaedic surgery, encouraging positive interactions and equitable opportunities for all practitioners.
Keywords: gender, microaggressions, orthopedic, surgery, Saudi Arabia
Introduction
Coined by Chester Pierce in 1970, the term “microaggression” refers to the phenomenon of “subtle, stunning, often automatic, and nonverbal exchanges which are put downs”.1 More recent research has further defined microaggressions as encompassing verbal, nonverbal, and/or environmental slights, snubs, or insults that are either intentional or (most often) unintentional, yet convey hostile, derogatory, or otherwise negative messages to target persons based on their membership in a structurally oppressed social group.2 Often, microaggressions are rooted in implicit or explicit prejudice or other stereotypes such as sexuality, race, ethnicity, gender, religious beliefs, or disability.3,4 Research demonstrates that repeated, long-term experiences of microaggressions can have damaging consequences, including decreased trust, undermining of relationships, compromised quality of care, lower self-esteem, lower self-confidence, cultural mistrust, negative views of the world, poor behavioral control, psychological distress, anxiety, and depression.5,6
An anonymous 32-item survey was administered to members of Women in Orthopaedics, United States (US) a private online group exclusively comprising female orthopaedic surgeons in practice or training. A substantial 74% of respondents reported experiencing some form of microaggression during their training, with 13% acknowledging their role as perpetrators of microaggressions against others.7 These findings provide valuable information on the prevalence and perpetrators of microaggressions in the context of female orthopaedic surgeons’ careers. Women and underrepresented minorities are most commonly the target of workplace harassment and bullying.8,9
Despite the increasing percentage of females in medical school, orthopaedic surgery continues to lag behind.10 The representation of active female orthopaedic surgeons in the US was 5% in 2015, the lowest among all areas of medicine including other surgical subspecialties. While the reasons for these low numbers are likely multifactorial, a contributing factor may be a negative workplace culture, with microaggressions potentially impacting the decision to pursue orthopaedics as a career.11 Similarly, a cross-sectional study conducted in Saudi Arabia shed light on the gender distribution within orthopedic surgery, revealing that females comprised 14.6% (37) of the total orthopedic surgeons, while males accounted for 85.4% (217). This data highlights a significant gender disparity in the field, with female representation being notably lower compared to their male counterparts.12
Given the persistent underrepresentation of women in orthopaedic surgery, this study aims to determine the prevalence of microaggressions experienced by female Saudi orthopaedic surgeons. The study hypothesis is that microaggressions are commonly experienced among Saudi women in orthopaedics, shedding light on potential factors contributing to the limited representation of females in this surgical subspecialty.
Methods
Study Design
This cross-sectional study was conducted online and targeted female in orthopedic surgery across different regions of the Kingdom of Saudi Arabia. The survey was uploaded to Google Forms and distributed through social media platforms like Twitter, Instagram, and WhatsApp by well-trained data collectors. To make the survey applicable for orthopedic training in Saudi Arabia, it was modified from a prior survey used in orthopedic training in the US by Samora et al.7 Eligible participants were females in orthopedic surgery currently training in Saudi Arabia who were able to complete the self-reported questionnaire. Males, trainees of other surgical disciplines, those training in a country other than Saudi Arabia, and those who refused to participate or did not complete the questionnaire were excluded. Informed consent was obtained from all participants.
Using G Power, the study’s required sample size was estimated with a 95% confidence level, assuming a 50% response distribution and a margin of error of ± 5%. Considering a presumed prevalence of microaggression at 74%,7 the minimum required sample size was found to be 82 participants. The study employed a non-probability convenience sampling technique, including all eligible subjects during the study period.
Data Collection
The questionnaire was designed to gather comprehensive information about participants’ experiences during their orthopedic residency and practice settings, particularly in relation to gender-based microaggressions and discriminatory behaviors. It starts by collecting basic demographic data, such as the completion year of the orthopedic residency and whether it took place in Saudi Arabia. The survey then delves into the participants’ current practice setting and specialty, allowing them to choose from a list of options, including academic, private practice, hospital employee, military, and more. Participants could also specify “Other” if their practice setting or specialty is not listed. The questionnaire addressed the prevalence of microaggressions in the orthopedic surgery environment, inquiring whether participants have experienced being a victim, perpetrator, or silent witness to such behaviors. To identify the common perpetrators of microaggressions in the orthopedic surgery field, participants were asked to rank a list of individuals, including patients and their families, support staff (both male and female), male and female surgeons, and other male/female medical doctors. The survey also examined specific scenarios during residency/fellowship training where gender-related discrimination might have occurred. Participants were asked to check all that apply from a list of statements such as questioning strengths and abilities based on gender, being told that women should not be orthopedic surgeons, facing demeaning material in lectures, and experiencing negative discussions about pregnancy and family planning. Other gender-related scenarios during training include negative comments on appearance and behaviors, being asked to do something not requested of a male counterpart, and missing training opportunities due to gender bias. Moreover, the questionnaire addressed issues related to social events, where participants could indicate if they were excluded because of their gender, and the representation of women on podiums at meetings. It also explored situations where participants were mistaken for other roles, such as nurses, representatives, or physician assistants, and how they were treated differently by staff due to their gender. Lastly, the survey focused on facilities and resources available to participants based on gender, including the provision of separate locker rooms or doctors’ lounges, the availability of resources for breastfeeding, and the sizing of lead shielding in the operating room.
Ethical Approval
The ethical committee of King Khalid University granted approval for the study. Prior to their participation, all participants provided written informed consent. The research adhered to the ethical guidelines of the Helsinki Declaration.
Statistical Analysis
In this study, data normality was assessed using the Shapiro–Wilk test. For normally distributed data, the researchers used the mean and standard deviation as descriptive statistics. On the other hand, categorical data was described using numbers and frequencies to represent the counts and proportions of each category. To perform data analysis, the researchers utilized SPSS (Statistical Package for the Social Sciences), version 26. Chi-square tests were used for statistical analysis. A p-value < 0.05 was considered statistically significant.
Results
In this survey, we included 96 female Saudi orthopedics. Their mean age was 27.46 ± 12.20 years. Most respondents were either residents (52.63%), or specialists (23.16%). Most participants (92.63%) were still in training or early in their careers, with the vast majority (93.68%) had their residency in Saudi Arabia. Notably, 38.95% were currently in training, while 37.89% work in hospital settings. In terms of specialty, General Orthopedics leads at 31.58%, but a considerable number (43.16%) have yet to choose a subspecialty. Notably, 98.95% of respondents practice orthopedics in Saudi Arabia (Table 1). Table 1 also provides insights into the regional distribution, with the “Central Region” having the highest representation at 32.65%, followed by the “Eastern Region” at 26.32%.
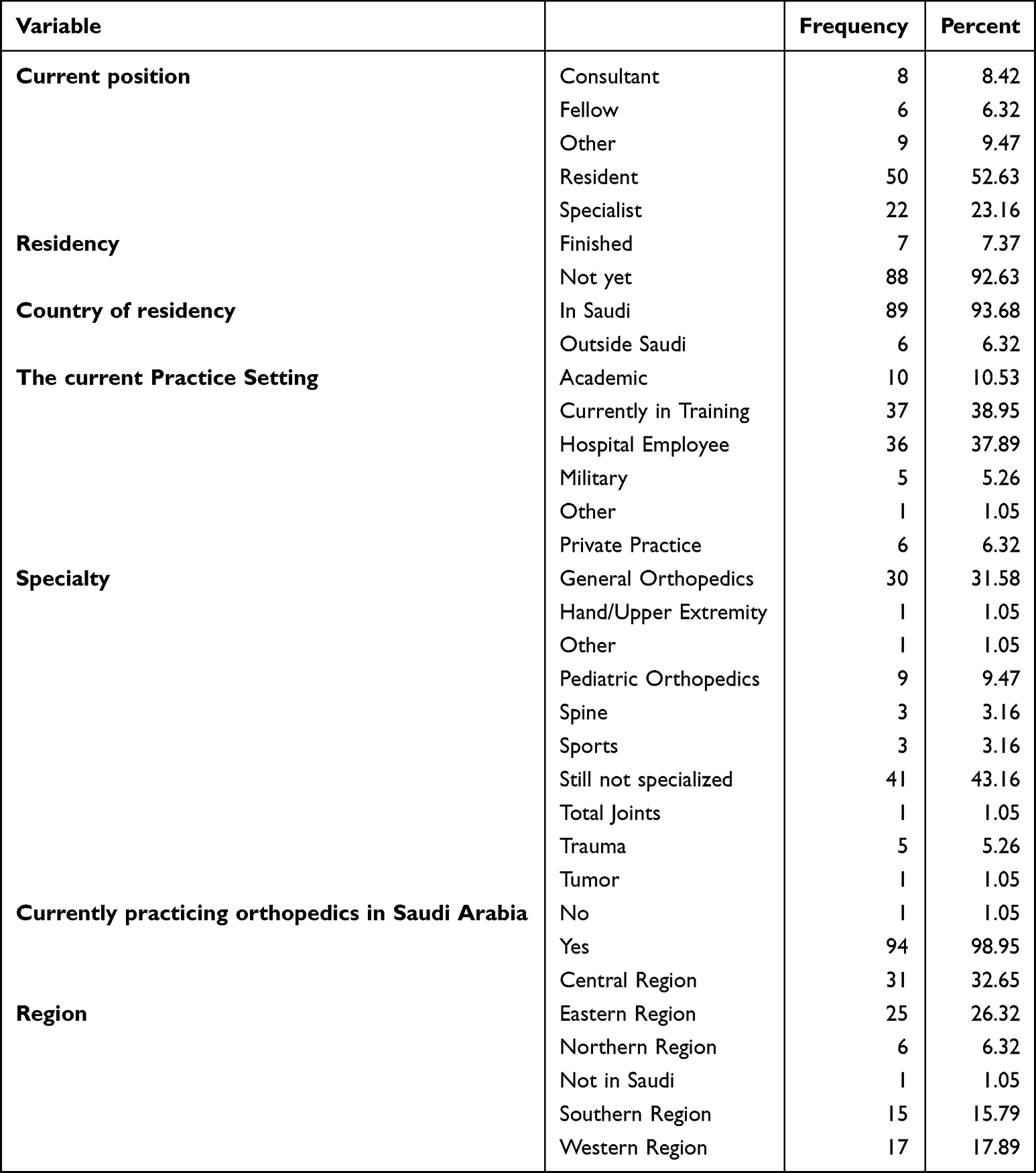 |
Table 1 Demographic and Practice Insights of Saudi Female Orthopedic Practitioners: Current Positions, Specialties, and Regional Distribution |
Figure 1 shows that 61.05% have reported experiencing microaggressions as victims. On the other hand, 38.95% claim not to have been victims of microaggressions. Notably, a substantial majority, 76.84%, did not see themselves as perpetrators of microaggressions, while 23.16% acknowledged having engaged in such behavior. Additionally, 32.63% identify as silent witnesses to microaggressions, whereas 67.37% state that they have not observed such incidents.
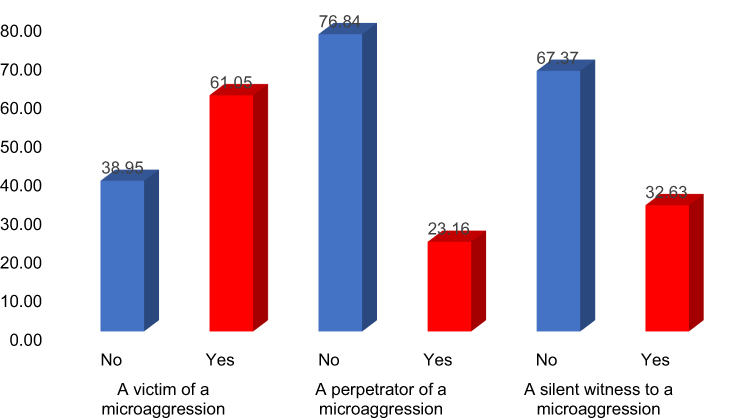 |
Figure 1 Microaggression experiences: incidences of being a victim, perpetrator, and silent witness among Saudi female orthopedics. |
Table 2 shows that there was statistically significant difference to be a silent witness to a microaggression across the Saudi Arabia region being the highest in the central region (34.48%) vs (5.17%) in the Northern region, p value 0.025. There was also difference across region regarding being aggression and a perpetrator of a microaggression however, these differences were not statistically significant.
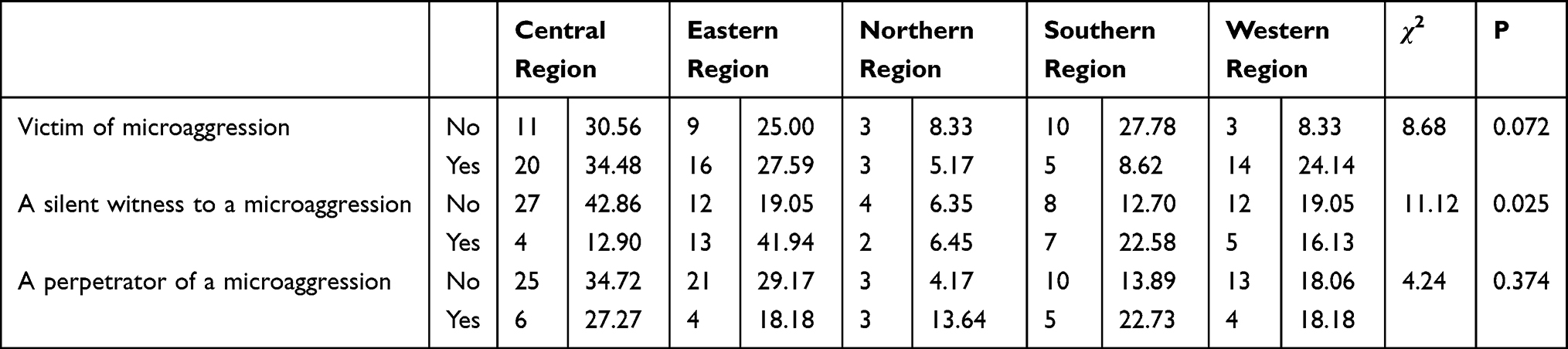 |
Table 2 Exposure to Microaggression Among Female Orthopedics Practicing in KSA |
Patients or their families were reported to be involved in microaggressions in 43.16% of cases, while male surgeons and male support staff were implicated at 51.58% and 23.16%, respectively. Additionally, other male medical doctors participate in microaggressions in 33.68% of instances. Female surgeons were identified as being involved in 22.11% of microaggressions, whereas 29.47% involve female support staff. Other female medical doctors were reported in 11.58% of cases. Notably, in most categories, most individuals (ranging from 56.84% to 88.42%) were reported not to partake in microaggressions, whereas the involvement of such behavior ranges from 11.58% to 43.16% (Table 3).
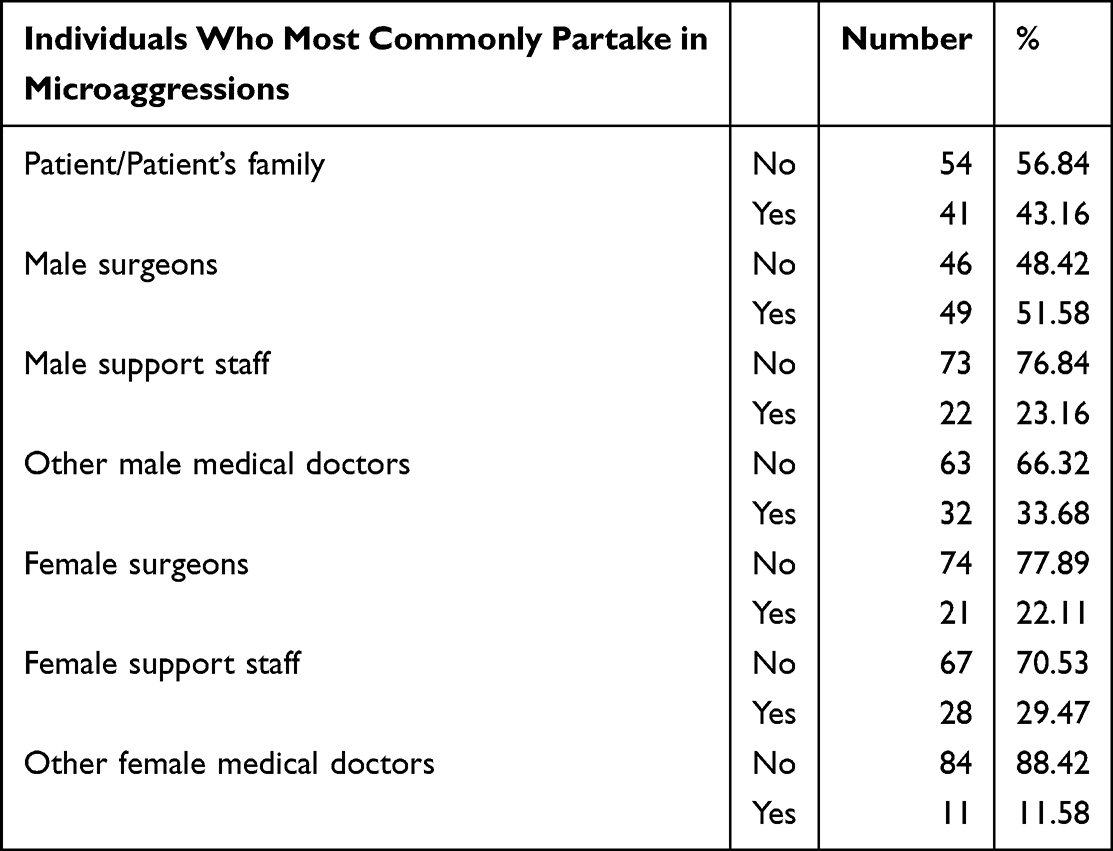 |
Table 3 Roles in Microaggressions: Identifying Individuals Most Commonly Involved in a Medical Environment |
Table 4 provides a comprehensive overview of gender-related experiences during orthopedic residency/fellowship training, shedding light on discrimination and stereotyping faced by individuals based on their gender. The data shows that a significant number of respondents experienced negative discussions related to their pregnancy and/or family planning (37.89%), their strength and ability being questioned due to gender (65.26%) and being told that women should not be orthopedic surgeons (48.42%). A substantial majority of respondents reported facing demeaning material in lectures and presentations (76.84%) and negative comments about their appearance (44.21%). Additionally, a significant portion experienced negative discussions about their way of being (69.47%) and being asked to do things not typically requested of males (53.68%). The findings also highlight challenges faced in professional settings, such as having titles excluded in introductions (18.95%) and being assumed to represent all female orthopedic surgeons (30.53%). The data further reveals instances of underrepresentation of women on podiums at meetings (18.95%) and missed training opportunities due to gender (14.74%).
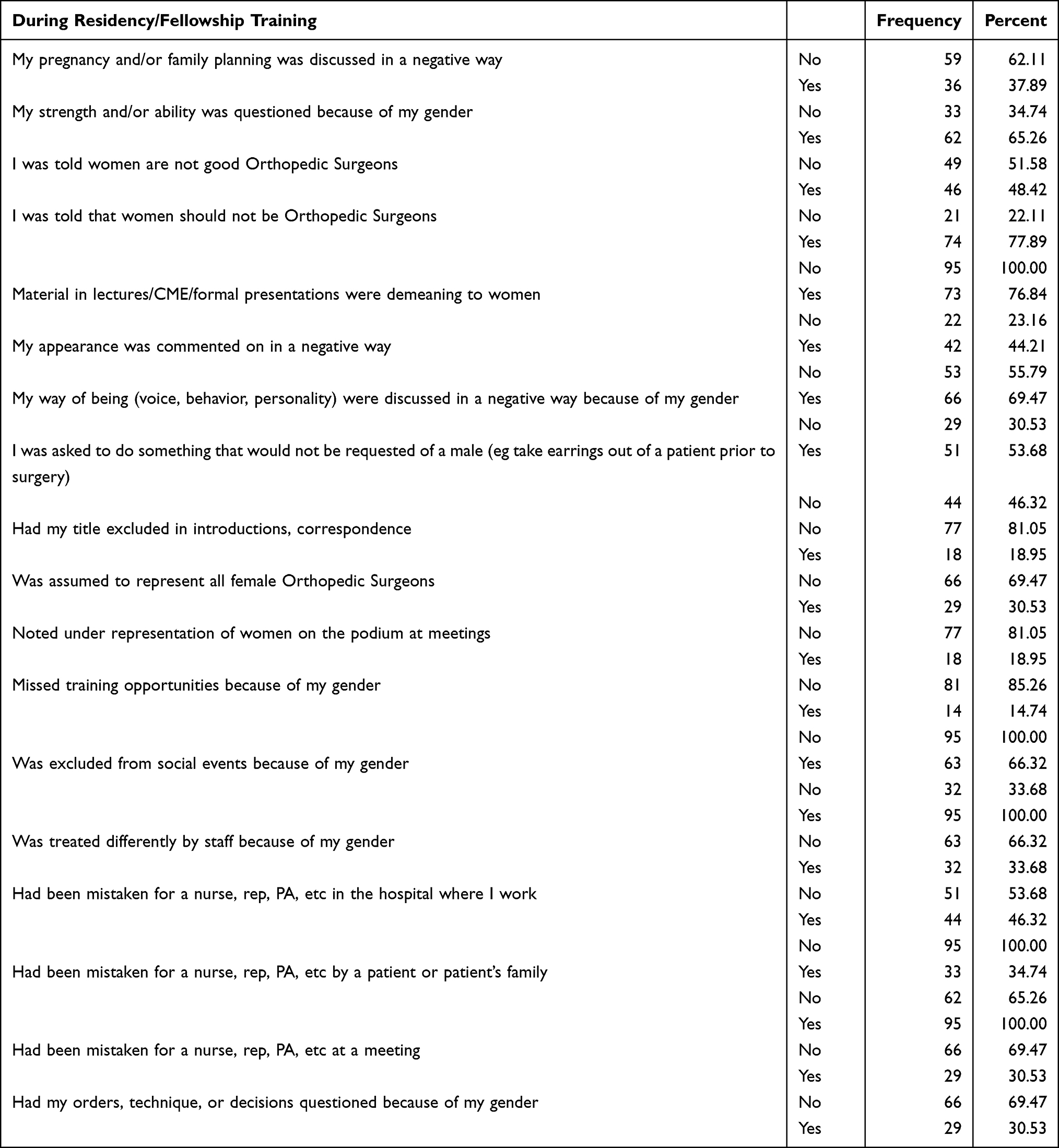 |
Table 4 Gender-Related Experiences During Orthopedic Residency/Fellowship Training: A Survey on Discrimination and Stereotyping |
Regarding social dynamics, respondents reported being excluded from social events (66.32%), treated differently by staff (33.68%), and mistaken for other roles, such as nurse, rep, or PA (46.32% to 65.26%), based on their gender. Additionally, a significant portion (30.53%) had their orders, technique, or decisions questioned because of their gender.
Figure 2 highlights gender-related disparities in locker room resources and workplace accommodations for orthopedic females. 41.1% of respondents reported experiencing fewer locker room resources due to their gender, while 38.9% were not offered a separate female locker room or doctor’s lounge like their male counterparts. Additionally, 26.3% of individuals did not have physical resources available to breastfeed while working. Furthermore, 51.6% mentioned not having lead shielding sized for their frame while working in the operating room. The data also shows that 31.6% saw signage equating the Nurse’s locker room to the Women’s locker room.
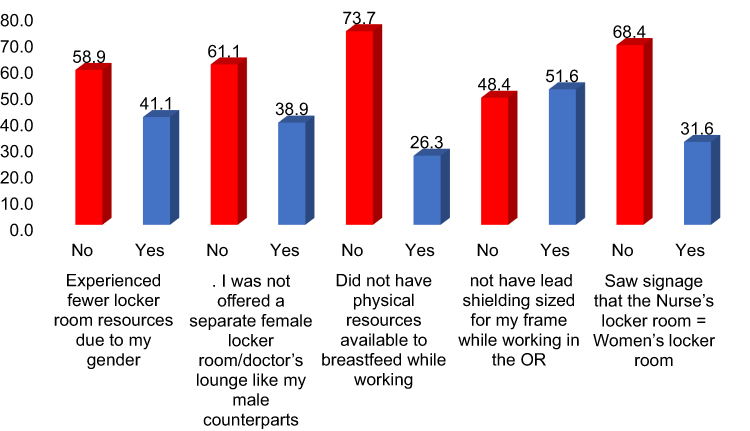 |
Figure 2 Gender-related experiences during orthopedic residency/fellowship training. |
Discussion
The study’s findings revealed that 61.05% of female trainees in orthopedic surgery reported experiencing microaggressions as victims, while 38.95% claimed not to have been victims. Moreover, 76.84% did not see themselves as perpetrators of microaggressions, while 23.16% acknowledged engaging in such behavior. A significant number (32.63%) identified as silent witnesses to microaggressions. Patients or their families were involved in 43.16% of microaggressions, followed by male surgeons (51.58%), male support staff (23.16%), and other male medical doctors (33.68%). The study also highlighted various gender-related experiences during orthopedic residency/fellowship training, with negative discussions about pregnancy and family planning, questioning of strength and ability due to gender, and being told women should not be orthopedic surgeons being notable challenges. A significant majority faced demeaning material in lectures and presentations and negative comments about appearance. Instances of underrepresentation of women at meetings and missed training opportunities due to gender were observed. Social dynamics revealed exclusion from social events and being mistaken for other roles based on gender. Additionally, workplace accommodations and resources showed disparities, with experiencing fewer locker room resources, not offered separate female facilities, and lacking resources for breastfeeding.
Similarly, based on the finding of a survey conducted among a portion of the American Academy of Orthopaedic Surgeons’ members, it was revealed that women were more prone to encountering instances of discrimination, harassment, and bullying compared to their male counterparts, with percentages of 81% and 35% respectively.11 Similar prevalence was reported by Samora et al7 (74%). A lower rate of microaggressions was reported by German healthcare professionals. Specifically, 38.1% of the respondents reported being witnesses of discrimination, while 13.5% of the participants stated that they personally experienced discrimination in their respective wards.13
In this study, participants identified male surgeons followed by patients and patients’ families as the most commonly responsible individuals for such behavior. The identification of male surgeons as frequent perpetrators highlights a potential gender disparity within the profession of orthopaedic surgery. This emphasizes the importance of addressing and mitigating any biased behaviors or attitudes that might exist within the male-dominated field. Samora et al7 reported that patients and their families were the primary perpetrators, followed closely by male surgeons and female staff. It is worth noting that the education of medical trainees, comprising medical students and residents, is shaped by their interactions with patients and their families, supervisors, nurses, peers, and other healthcare providers. These interactions can serve as valuable sources of mentorship and motivation, significantly impacting the trainees’ future career paths. However, it is essential to recognize that these same individuals can also potentially contribute to feelings of unease, stress, mistreatment, harassment, or discrimination.14
In this study, respondents encountered discrimination related to their pregnancy and family planning, had their strength and ability questioned due to gender, and faced discouraging remarks about women pursuing orthopedic surgery careers. A systematic review conducted by Morrison et al,15 highlighted that a significant number of women have observed or faced discrimination concerning pregnancy and parenthood, leading to some opting to postpone family planning decisions. Moreover, 67% of them chose to delay childbearing due to their career path in orthopedics. This study observed instances of underrepresentation of women at meetings and missed training opportunities due to gender. It also revealed social dynamics such as exclusion from social events and being mistaken for other roles based on gender. Workplace accommodations and resources showed disparities, including fewer locker room resources, lack of separate female facilities, and inadequate resources for breastfeeding. Indeed, female medical students might be encouraged to select specialties perceived as “female-friendly”, such as family medicine and pediatrics, while being discouraged from choosing surgical specialties due to societal gender stereotypes about career preferences and family–life balance.16,17 This gender disparity often persists throughout residency training and as female physicians progress to become attending physicians.18,19 Unfortunately, women in medicine may not receive equal recognition compared to their male colleagues, particularly concerning leadership roles and salary compensation.19 These disparities in recognition and compensation may be a consequence of the gendered pathways female medical students are steered towards, which tend to undervalue and offer lower pay for professions and careers dominated by women. These findings emphasize the significance of tackling gender-related challenges within orthopedic training programs. Creating an inclusive and supportive environment that values diversity and recognizes the contributions of all individuals, irrespective of their gender, is essential.19 Health-Sustainability is a useful tool for the integration of sustainable development in the high-performance strategies that managers of healthcare facilities must develop in the current context of global challenges.20
Coping strategies play a crucial role in reducing the negative cumulative effects and safeguarding one’s emotional well-being. A beneficial approach is seeking debriefing and support from a colleague at work or a loved one at home. Additionally, connecting with others who share similar experiences or forming therapeutic support groups can be considered to repair “microaggressions”, offering valuable perspective and validation of one’s experiences. Instead of solely focusing on the actions of the perpetrators, Freeman and Stewart2 adopt a victim-centered approach. Their method involves validating the victims’ experiences, ensuring that the harms they endure are not trivialized, and acknowledging the various types of harm they may encounter. According to them, none of the so-called “microaggressions” are truly insignificant to the individuals targeted.
Strengths and Limitations
The study demonstrates strengths in its comprehensive investigation of microaggressions and gender-related challenges among female orthopedic surgery in Saudi Arabia, employing a mixed-methods approach, and diverse participant pool. Nevertheless, limitations are present, including potential self-report bias, sampling bias from non-probability convenience sampling, and limited generalizability. The cross-sectional design hinders establishing causal relationships, and assumptions about the prevalence of microaggressions and the online survey format may introduce biases. Moreover, retrospective recall and cultural specificity may impact the accuracy and applicability of findings beyond Saudi Arabia’s context. Finally, the small sample size of included participants is due to the small number of females practicing orthopedics in Saudi Arabia.
Conclusions
Based on the study’s findings, it is advised to implement awareness and sensitivity training to address microaggressions and gender-related challenges experienced by Saudi female trainees in orthopedic surgery. Establishing mentorship and support programs is essential to guide and motivate female trainees throughout their training, and initiatives to enhance gender diversity within the field should be pursued. Empowering female trainees through leadership development programs can foster their participation in leadership roles. Advocating for policy reforms to ensure equal opportunities and resources for female trainees is crucial. Creating a supportive work environment, conducting research, and fostering collaboration and networking are also key factors in tackling these challenges effectively. Longitudinal studies can monitor progress and outcomes over time, while institutions must demonstrate a strong commitment to promoting inclusivity and equity for all trainees. The implementation of these recommendations would lead to substantial advancements in creating a more inclusive and equitable environment for female orthopedic surgery trainees.
Funding
The authors extend their appreciation to the Deanship of Scientific Research at King Khalid University for funding this work through large group Research Project under grant number RGP2/263/44.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Barbour FB. The Black Seventies. Boston: P. Sargent Boston; 1970.
2. Freeman L, Stewart H. Microaggressions in clinical medicine. Kennedy Inst Ethics J. 2018;28(4):411–449. doi:10.1353/ken.2018.0024
3. Sue DW, Capodilupo CM, Torino GC, et al. Racial microaggressions in everyday life: implications for clinical practice. Am Psychol. 2007;62(4):271. doi:10.1037/0003-066X.62.4.271
4. Nadal KL, Issa M-A, Leon J, et al. Sexual orientation microaggressions: “death by a thousand cuts” for lesbian, gay, and bisexual youth. J LGBT Youth. 2011;8(3):234–259. doi:10.1080/19361653.2011.584204
5. Nadal KL, Griffin KE, Wong Y, et al. The impact of racial microaggressions on mental health: counseling implications for clients of color. J Couns Dev. 2014;92(1):57–66. doi:10.1002/j.1556-6676.2014.00130.x
6. Kim PY, Kendall DL, Cheon H-S. Racial microaggressions, cultural mistrust, and mental health outcomes among asian American college students. Am J Orthopsych. 2017;87(6):663. doi:10.1037/ort0000203
7. Samora JB, Denning J, Haralabatos S, et al. Do women experience microaggressions in orthopaedic surgery? Current state and future directions from a survey of women orthopaedists. Curr Orthop Pract. 2020;31(5):503–507. doi:10.1097/BCO.0000000000000909
8. Brown J, Drury L, Raub K, et al. Workplace harassment and discrimination in gynecology: results of the AAGL member survey. J Minim Invasive Gynecol. 2019;26(5):838–846. doi:10.1016/j.jmig.2019.03.004
9. Coombs AAT, King RK. Workplace discrimination: experiences of practicing physicians. J Natl Med Assoc. 2005;97(4):467.
10. O’Brien BC, Forrest K, Wijnen‐Meijer M, ten Cate O. A global view of structures and trends in medical education. Understanding Med Educ. 2018;2018;7–22.
11. Samora JB, Van Heest A, Weber K, et al. Harassment, discrimination, and bullying in orthopaedics: a work environment and culture survey. J Am Acad Orthop Surg. 2020;28(24):e1097–e1104. doi:10.5435/JAAOS-D-19-00822
12. Alshammari AN, Shafiq M, Altayeb M, et al. Gulf cooperation council female residents in orthopedics: influences, barriers, and mental pressures: a cross-sectional study. J Musculoskelet Surg Res. 2018;2(2):51. doi:10.4103/jmsr.jmsr_5_18
13. Yolci A, Schenk L, Sonntag P-T, et al. Observed and personally experienced discrimination: findings of a cross-sectional survey of physicians and nursing staff. Hum Resour Health. 2022;20(1):83. doi:10.1186/s12960-022-00779-0
14. Fnais N, Soobiah C, Chen MH, et al. Harassment and discrimination in medical training: a systematic review and meta-analysis. Acad Med. 2014;89(5):817–827. doi:10.1097/ACM.0000000000000200
15. Morrison LJ, Abbott AG, Mack Z, et al. What are the challenges related to family planning, pregnancy, and parenthood faced by women in orthopaedic surgery? A systematic review. Clin Orthop Relat Res. 2023;481(7):1307–1318. doi:10.1097/CORR.0000000000002564
16. Hill E, Vaughan S. The only girl in the room: how paradigmatic trajectories deter female students from surgical careers. Med Educ. 2013;47(6):547–556. doi:10.1111/medu.12134
17. Drinkwater J, Tully MP, Dornan T. The effect of gender on medical students’ aspirations: a qualitative study. Med Educ. 2008;42(4):420–426. doi:10.1111/j.1365-2923.2008.03031.x
18. Frank E, Zhao Z, Sen S, et al. Gender disparities in work and parental status among early career physicians. JAMA Netw Open. 2019;2(8):e198340. doi:10.1001/jamanetworkopen.2019.8340
19. Jena AB, Olenski AR, Blumenthal DM. Sex differences in physician salary in US public medical schools. JAMA Intern Med. 2016;176(9):1294–1304. doi:10.1001/jamainternmed.2016.3284
20. Moldovan F, Moldovan L, Bataga T. Assessment of labor practices in healthcare using an innovatory framework for sustainability. Medicina. 2023;59:796.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.