")
Back to Journals » International Journal of Women's Health » Volume 16
Gender and Drug Use Discrimination Among People Who Inject Drugs: An Intersectional Approach Using the COSINUS Cohort
Authors Anwar I , Faye A, Pereira Gonçalves J, Briand Madrid L, Maradan G, Lalanne L, Jauffret-Roustide M, Auriacombe M, Roux P
Received 4 November 2023
Accepted for publication 25 February 2024
Published 12 March 2024 Volume 2024:16 Pages 451—462
DOI https://doi.org/10.2147/IJWH.S448147
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Ilhame Anwar,1 Aissatou Faye,1 Jessica Pereira Gonçalves,1 Laélia Briand Madrid,1 Gwenaëlle Maradan,2 Laurence Lalanne,3,4,* Marie Jauffret-Roustide,5– 7,* Marc Auriacombe,8– 10,* Perrine Roux1
1Aix Marseille Univ, Inserm, IRD, SESSTIM, Sciences Economiques & Sociales de la Santé & Traitement de l’Information Médicale, ISSPAM, Marseille, France; 2ORS PACA, Observatoire régional de la santé Provence-Alpes-Côte d’Azur, Marseille, France; 3INSERM 1114, Department of Psychiatry and Addictology, University Hospital of Strasbourg, Fédération de Médecine Translationnelle de Strasbourg (FMTS), Strasbourg, 67000, France; 4Department of Psychiatry and Addictology, University Hospital of Strasbourg, Fédération de Médecine Translationnelle de Strasbourg (FMTS), Strasbourg, 67000, France; 5CERMES3 (Inserm U988/UMR CNRS 8211/EHESS/Paris Descartes University), Paris, France; 6British Columbia Center on Substance Use, Vancouver, Canada; 7Baldy Center on Law and Social Policy, Buffalo University, New York, NY, USA; 8Univ. Bordeaux, Bordeaux, France; 9Addiction Team (Laboratoire de psychiatrie)/SANPSY, CNRS USR 3413, Bordeaux, France; 10Pôle Addictologie, CH Charles Perrens and CHU de Bordeaux, Bordeaux, France
*These authors contributed equally to this work
Correspondence: Ilhame Anwar, Sciences Economiques et Sociales de la Santé et Traitement de l’Information Médicale (SESSTIM), Faculté des sciences médicales et paramédicales, 27 Bd Jean Moulin 13385 Marseille Cedex 5, Marseille, France, Email [email protected]
Purpose: Injection drug use is strongly associated with stigmatization by loved ones, healthcare providers, and society in general. This stigmatization can have negative consequences on the health of people who inject drugs (PWID) and limit their access to care. Women who inject drugs face greater stigma than men because of gendered social norms and the intersectional effect between gender and drug use identities. For this analysis, we aimed to study discrimination - which is closely linked to stigmatization - experienced by PWID, considering the intersectionality between drug use discrimination and gender discrimination in the French context.
Methods: We used data from the COSINUS cohort study, conducted between June 2016 and May 2019 in four French cities. We selected 427 of the 665 PWID who regularly injected drugs enrolled in COSINUS, at three months of follow-up, and performed multivariable logistic regression to identify factors associated with self-reported drug use discrimination.
Results: Women comprised 20.6% of the study sample. Sixty-nine percent of the participants declared drug use discrimination and 15% gender discrimination. In the multivariable regression analysis, PWID who had hurried injection out of fear of being seen were almost twice as likely to have experienced drug use discrimination (OR [95% CI]: 1.77 [1.15, 2.74], p = 0.010). Likewise, women experiencing gender discrimination were almost three times as likely to have experienced drug use discrimination (OR [95% CI]: 2.84 [1.07,7.56], p=0.037).
Conclusion: Women who inject drugs experienced gender and drug use intersectional discrimination. This could be a reason for the low attendance rates of women in healthcare settings. In addition, discrimination negatively impacted injection drug use practices (eg, hurried injection), particularly for people with unstable housing who injected in public spaces. We recommend introducing adapted services in healthcare facilities for women who inject drugs, and creating a favorable social and physical environment for all PWID in order to improve their health and access to care.
Keywords: gender, injection drug use, intersectionality, discrimination
Introduction
Drug use, and particularly injection drug use, is strongly associated with stigmatization by loved ones, healthcare providers, and society in general.1 Stigma is defined as social disapproval of someone because of a specific attribute.2 Stigma may lead to discrimination, the latter being defined as treating someone unfairly because of a specific attribute,2 such as drug use or gender in the context of this article. Stigma can take different forms such as internalized stigma, where people who inject drugs (PWID) accept others’ negative views of them and devaluate themselves, and enacted stigma, which is related to negative experiences in healthcare settings such as dismissive attitudes, mistreatment and discrimination by care providers.3 Some PWID adopt strategies to avoid these situations by staying away from healthcare settings, delaying care, and concealing their injection practices.4 Experiencing discrimination is one of the several barriers PWID face in terms of accessing healthcare. Specifically, it leads to limited use of healthcare and harm reduction services.5 This can have negative consequences on PWID physical and mental health, such as adopting injection risky behaviors (eg, reusing injecting equipment), avoiding medical care despite having injection related-complications, a poor health-related quality of life, and difficulties engaging in treatment programs.5,6
Women who inject drugs face greater stigma than men because of gendered social norms and the intersectional effect of gender and drug use identities.7 This intersectional stigma has an impact on women’s health and on access to care, which can explain their under-representation with respect to men who inject drugs in healthcare and harm reduction settings.8 Some women who attend these services hide their injection practices from healthcare providers while others prefer not to attend, and delay care as much as possible.9 Moreover, women experience more physical and sexual violence than men, which also contributes to their reluctance to use harm reduction services.10
In Western Europe, women who inject drugs represent approximately 30% of all PWID.11 In France, of the approximately 130,000 known PWID in 2019,12 women accounted for 18%.11 Compared to men, women who inject drugs are more exposed to hepatitis C virus (HCV) and HIV infections and have poorer mental health.10
We aimed to study discrimination experienced by PWID in France, while taking into account the intersectionality between drug use and gender. More specifically, we investigated whether women who experienced gender discrimination were more likely to also experience discrimination because of their drug use.
Materials and Methods
COSINUS is a multi-site longitudinal cohort study conducted in France between June 2016 and May 2019 in four cities (Paris, Strasbourg, Marseille, Bordeaux).13 The main objective was to assess the effectiveness of drug consumption rooms (DCR) on PWID health (HIV and HCV risk practices, other health issues).14,15 Eligibility criteria were as follows: being 18 years of age or older, French speaking, regular use of illegal drugs or prescribed medication, injecting at least once in the previous month, and providing informed consent to participate. The study’s 665 participants were recruited in the two DCR currently in France, one in Strasbourg and one in Paris, as well as harm reduction services in these two cities and in Bordeaux and Marseille. They were followed for 12 months and completed face-to-face questionnaires administered by trained interviewers at enrolment (M0), 3 months (M3), 6 months (M6), and 12 months (M12). Ethical approval was provided by the Institutional Review Board (IRB00003888) of the French institute of medical research and health (opinion number: 14–166). This study was completed in accordance with the 1964 Helsinki declaration. More detailed information on the study protocol is available elsewhere.13
For the present analysis, we selected COSINUS participants at M3 (n=430) as the question regarding experience of discrimination was only contained in the M3 questionnaire. Of these, 427 had available data on this theme.
The main outcome, “drug use discrimination”, was created as a dichotomous variable (“yes” vs “no”) using the question “During your lifetime, have you ever been discriminated against, been prevented from doing something, been hassled, or felt inferior because of your drug use?”. Participants who answered “Do not know” (n=3) were classified in the “no” category.
Independent variables were as follows: sociodemographic and socioeconomic data (city of interview, age, gender, education level, country of birth, living with a partner, having a family member who used drugs, type of housing, employment, receiving social welfare allowance, food aid, and health insurance), drug use practices (time since first injection, daily opioid use, daily stimulant use, daily injection, injection-body site risk level (see below), hurrying injection out of fear of being seen, and places for injecting), health characteristics (being currently on opioid agonist therapy (OAT), harmful alcohol consumption, attending a DCR, and HCV status), and finally, two discrimination data variables (experiencing gender discrimination (total population), and experiencing gender discrimination according to gender “gender discrimination-gender”). The “gender discrimination” variable was constructed using the same question as that for the main outcome: “During your lifetime, have you ever been discriminated against, been prevented from doing something, been hassled, or felt inferior because of your gender?”. The “gender discrimination-gender” variable was constructed using four categories which combined gender and gender-based discrimination as follows: (1) Non-discriminated men, (2) Discriminated men, (3) Non-discriminated women and (4) Discriminated women.
The “injection-body site risk level” variable (see above) was classified into three categories: low, medium, and high. To construct this variable, we first created a score combining injection site recommendation type (“recommended”, ie, the arm; “not recommended”, ie, the hand, wrist, foot, leg and muscles; and “dangerous”, ie, the groin, neck, armpit, breast and sexual organ) and the frequency of injection in these areas based on two questions; the first asked which parts of the body the PWID had injected into at least once, while the second asked which part (note: singular) of the body they most frequently injected into. Scoring was as follows: 1 (PWID most frequently injected in a recommended area); 2 (PWID most frequently injected in a recommended area AND injected in a non-recommended area at least once); 3 (PWID most frequently injected in a recommended area AND injected in a dangerous area at least once); 4 (PWID most frequently injected in a non-recommended area AND injected in a recommended area at least once); 5 (PWID most frequently injected in a non-recommended area AND injected in a dangerous area at least once); 6 (PWID most frequently injected in a dangerous area). From these scores, we then created the three categories, with the score 1 reflecting low risk, 2,3, and 4 medium risk, and 5 and 6 high risk.
Furthermore, the variable “HCV status” (see above) was created as a dichotomous variable considering those who currently had HCV versus those who did not, those who were HCV cured, and those unaware of their HCV status.
We compared participants who declared drug use discrimination with those who did not using the Chi-square test for categorical data. To identify factors associated with drug use discrimination, we performed univariable logistic regressions to identify eligible variables for the multivariable model with a threshold p-value <0.25. We then performed multivariable logistic regression using a backward stepwise procedure in order to only keep variables with a p-value <0.05 in the final model.
Results
Women comprised 20.6% of the study sample and median age was 39 years (interquartile range (IQR): 32–46) (Table 1). Approximately 69% and 15% declared drug use and gender discrimination, respectively. More specifically, 6.6% of men and 8.9% of women had experienced gender discrimination (“gender discrimination-gender” variable).
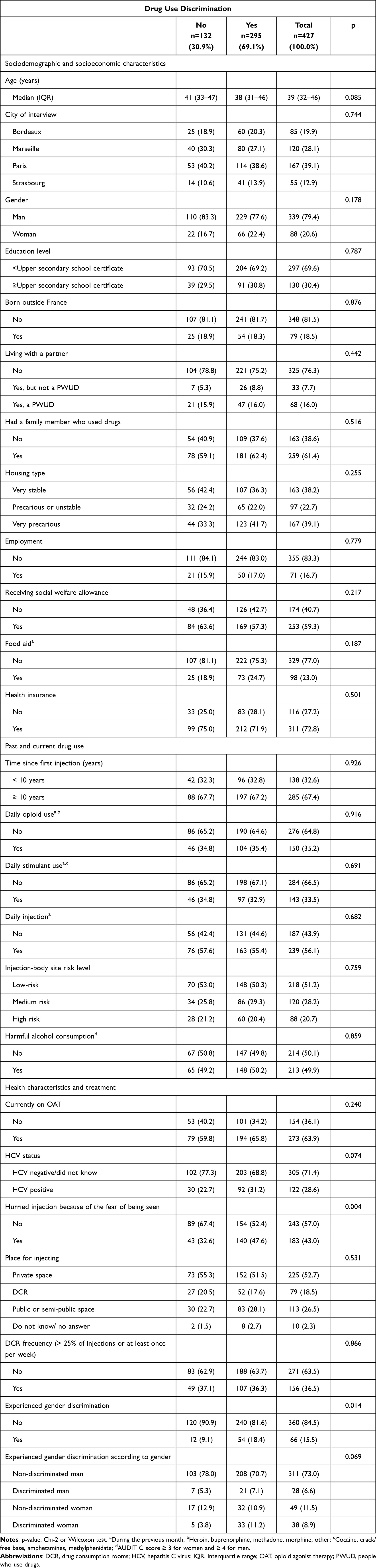 |
Table 1 Descriptive Analyses of Study Sample (n=427) |
Participants who declared drug use discrimination were slightly younger than those who did not. Moreover, they were more likely to i) have hurried injection out of fear of being seen, ii) be HCV positive at the time of the survey, and iii) declare gender discrimination. The latter was especially true for women.
Table 2 presents the results of the univariable and multivariable regression analyses. In the latter, PWID who had hurried injection were almost twice as likely to have experienced drug use discrimination (OR [95% CI]: 1.77 [1.15,2.74], p = 0.010). Gender-discriminated women were almost three times as likely to have also experienced drug use discrimination (OR [95% CI]: 2.84 [1.07,7.56], p=0.037) compared to men not gender discriminated.
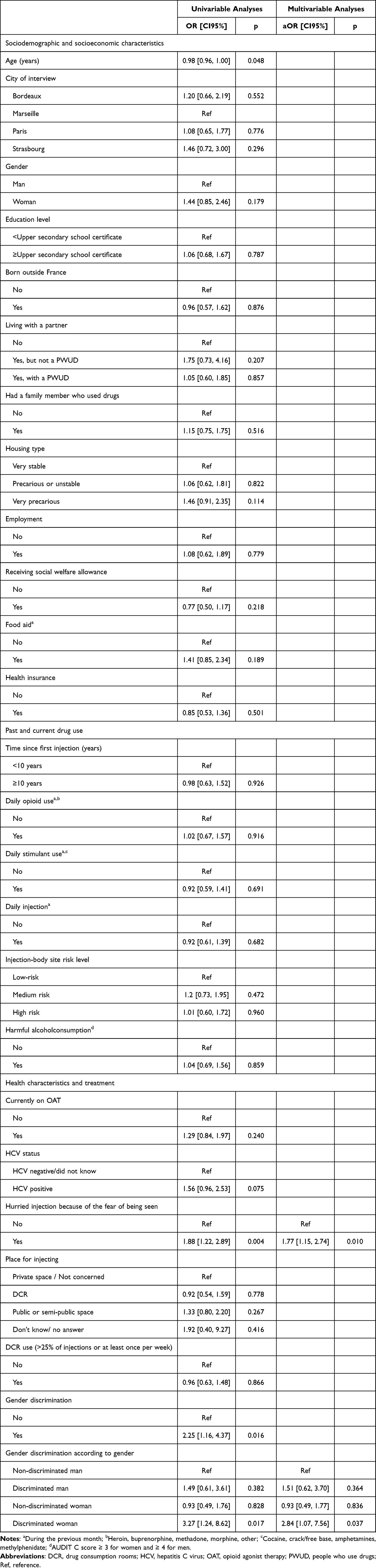 |
Table 2 Univariable and Multivariable Logistic Regression Analyses (n=427) |
Discussion
The main finding of our analyses is that gender discrimination in women was associated with more drug use discrimination than in men not gender discriminated. No impact of gender discrimination was found for men in our analyses.
More specifically, women who inject drugs in our sample experienced gender and drug use intersectional stigma, also called “double stigma”. This intersectional stigma stems from the expectations of society in general concerning womanhood, and the stereotype that women who inject drugs engage in prostitution.7 It is present in healthcare and harm reduction settings, and prevents women from utilizing related services, including sexual health services.16 It is often related to patient-perceived discriminatory actions and attitudes by healthcare providers, such as mistreatment, poor quality of care, and patient shaming arising from providers’ prejudices against women.7,17,18 Furthermore, past experience of discrimination in healthcare settings represents a significant barrier to accessing health services for women who inject drugs.7,9 Specifically, these women implement strategies to avoid stigma and discrimination in healthcare settings, such as not disclosing their injection practices, not attending appointments, delaying healthcare,9 and injecting in hidden spaces out of fear that their drug use will become public.19 All these strategies can negatively impact their health. Moreover, some women who inject drugs may fear possible harassment by men in healthcare settings.18 Indeed, women who inject drugs are more likely to have experienced physical, sexual or psychological violence than their male counterparts. This gender-based violence, stemming from the stigmatization and distribution of gendered social roles, also creates difficulties for women to seek help and to utilize health services.16 In harm reduction settings, the consequence of this violence is that women are prevented from being able to feel at ease or safe in the centers’ reception spaces.19,20 This could be one reason why women who inject drugs represent such a hard-to-reach population, not only for harm reduction services but for researchers and public health interventions. A trustful relationship with providers could attenuate this stigma, thereby fostering attendance in healthcare and harm reduction services.18 Furthermore, it is important to provide suitable multidisciplinary support for women experiencing violence in harm reduction settings.19 This could include, among other things, training care providers in the management of gender-based violence, developing protocols for the management of violence in harm reduction facilities, and improving networking with other professionals consulting women20,21 with a view to better meeting this population’s complex needs.
Gender-equity in healthcare facilities must be promoted.22 To tackle the current inequity in care for women who inject drugs, it is important to create safe, stigma-free spaces to facilitate their access to harm reduction services. By protecting women’s privacy and safety, dedicated “women-only” spaces in harm reduction centers help to improve program attendance and access to social and health services.21,23 Specifically, these spaces limit the reproduction of gendered power relations, and enable the development of peer support as well as knowledge sharing concerning drug use between women. They also provide women with the opportunity to verbalize the violence they have experienced, thereby fostering empowerment.20,23 In France, structural developments should involve the roll-out of more women-only centers, providing women-only sessions during opening hours (this already exists in some harm reduction centers for support on gynecology and pregnancy),24 and increasing the offer of sexual and reproductive health services.18 Proposing child care services in such spaces could also be useful, given that mothers are usually the primary provider for children.19
Another interesting result from our study is that hurried injection out of fear of being seen was associated with drug use discrimination, independent of gender. As described in the “risk environment” approach,25 an unfavorable environment can increase vulnerability to drug-related harms for PWID. A previous study found that PWID who experienced frequent discrimination were not only more likely to report drug-related harms (overdoses, infections, and abscesses), but also poorer wellbeing.26 This finding suggests that our result on hurried injection may reflect previous experiences of discrimination related to the stigma surrounding drug injection, which may have had a negative impact on PWID drug use practices. Hurried injection prevents PWID from adopting safer injecting practices (eg, cleaning site before injection, injecting into the arm instead of a non-recommended or dangerous site, slow injection to avoid overdose). Specifically, it can lead to skin and soft tissue infections which in turn bring about further complications such as bone and joint infections, infective endocarditis and sepsis.27 Moreover, most PWID in our study sample experienced social precarity and had unstable housing. Homeless PWID experience discrimination more frequently in public spaces because of the lack of safe spaces to inject. This can reinforce their vulnerability to drug-related harms and increase risky injecting behaviors. All these elements highlight the need to open more DCR, which have already been associated with a reduction in abscess and overdose rates.14
Our study has limitations. First, there is possible social desirability bias due to the mode of questionnaire administration. However, a previous study found good validity and reliability of self-reports in terms of drug use in PWID.28 Second, although our sample size was sufficient to guarantee study power, few women (20%) were included, which reflects other studies on drug use. Nevertheless, the association between drug use and gender discrimination in women which we found was significant despite this small percentage. Finally, we did not use a validated scale to measure gender or drug use discrimination. Nonetheless, our method helped us to capture individual experiences of intersectional discrimination in PWID.29
Conclusion
Using components of the intersectional approach, our main result highlighted a positive association between drug use discrimination and gender discrimination in women. Healthcare and harm reduction facilities should provide tailored services for women who inject drugs. A second result is that persons who hurried injection were more likely to experience drug use discrimination. More generally, it is important to create a favorable social and physical environment (ie, by reducing injection-related stigma and creating safe spaces for injection) for all PWID in order to improve PWID health and access to care. The intersectionality approach used in our analyses could be complemented by qualitative studies in order to better understand the various dimensions of intersectional stigma and discrimination experienced by PWID, in particular women.
Abbreviations
aOR, Adjusted Odds Ratio; DCR, drug consumption rooms; HCV, hepatitis C virus; IQR, interquartile range; OAT, opioid agonist therapy; OR, Odds ratio; PWID, people who inject drugs; PWUD, people who use drugs.
Data Sharing Statement
The dataset used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The ethical approval has been received from the Institutional Review Board (IRB00003888) of the French institute of medical research and health (opinion number: 14–166). This research was completed in accordance with the 1964 Helsinki declaration, and all participants provided informed consent prior to their inclusion.
Acknowledgments
We thank all the research participants and the members of the COSINUS scientific committee (Henri-Jean Aubin, Patrizia Carrieri, Nerkassen Chau, Jean-Marie Danion, Maurice Dematteis, Laurent Karila and Thomas Kerr), the Ethical Review Committee, the French Institute for Public Health Research (IRESP) and the IRESP scientific committee (Marc Bardou, Christian Ben-Lakhdar, Eric Breton, Olivier Cottencin, Helene Donnadieu-Rigole, Xavier Laqueille, Jennifer O’Loughlin, Christophe Tzourio et Frank Zobel). We also thank the Public Health Doctoral Network of EHESP for funding Ilhame Anwar’s PhD. Finally, our thanks to Jude Sweeney (Milan, Italy) for the English revision and copyediting of our manuscript.
We also thank the COSINUS study group: Marc Auriacombe, Cyril Berenger, Gilles Bertoia, Laélia Briand Madrid, Maria Patrizia Carrieri, Isabelle Célérier, Carole Chauvin, Manon Chevalier, Jean-Marie Danion, Sébastien de Dinechin, Cécile Denis, Natascia Grelli, Marie Gutowski, Naomi Hamelin, Marie Jauffret-Roustide, Charlotte Kervran, Sébastien Kirchherr, Laurence Lalanne, Mireille Le Breton, Gwenaëlle Maradan, Sarah Moriceau, Perrine Roux and Antoine Vilotitch.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded in full by the French Government Addiction Agency MILDECA (The inter-ministerial mission to fight against drugs and addictive practices). The funder had no role in the study design, analysis, preparation of the manuscript, or the decision to submit the paper for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Seear K. Addressing alcohol and other drug stigma: where to next? Drug Alcohol Rev. 2020;39(2):109–113. doi:10.1111/dar.13028
2. Earnshaw VA, Chaudoir SR. From conceptualizing to measuring HIV stigma: a review of HIV stigma mechanism measures. AIDS Behav. 2009;13(6):1160–1177. doi:10.1007/s10461-009-9593-3
3. Muncan B, Walters SM, Ezell J, Ompad DC. “They look at us like junkies”: influences of drug use stigma on the healthcare engagement of people who inject drugs in New York City. Harm Reduct J. 2020;17(1):53. doi:10.1186/s12954-020-00399-8
4. Biancarelli DL, Biello KB, Childs E, et al. Strategies used by people who inject drugs to avoid stigma in healthcare settings. Drug Alcohol Depend. 2019;198:80–86. doi:10.1016/j.drugalcdep.2019.01.037
5. Couto E, Cruz C, Salom C, Maravilla J, Alati R. Mental and physical health correlates of discrimination against people who inject drugs: a systematic review. J Stud Alcohol Drugs. 2018;79(3):350–360. doi:10.15288/jsad.2018.79.350
6. Paquette CE, Syvertsen JL, Pollini RA. Stigma at every turn: health services experiences among people who inject drugs. Int J Drug Policy. 2018;57:104–110. doi:10.1016/j.drugpo.2018.04.004
7. Meyers SA, Earnshaw VA, D’Ambrosio B, Courchesne N, Werb D, Smith LR. The intersection of gender and drug use-related stigma: a mixed methods systematic review and synthesis of the literature. Drug Alcohol Depend. 2021;223:108706. doi:10.1016/j.drugalcdep.2021.108706
8. Cadet-Taïrou A, Janssen É, Guilbaud F. Profils et pratiques des usagers reçus en CAARUD en 2019. Tendances. 2020;142:4.
9. Brener L, Cama E, Broady T, et al. Experiences of stigma and subsequent reduced access to health care among women who inject drugs. Drug Alcohol Rev. 2024. doi:10.1111/dar.13806
10. Iversen J, Page K, Madden A, Maher L. HIV, HCV and health-related harms among women who inject drugs: implications for prevention and treatment. J Acquir Immune Defic Syndr. 2015;69(1):S176–S181. doi:10.1097/QAI.0000000000000659
11. Degenhardt L, Peacock A, Colledge S, et al. Global prevalence of injecting drug use and sociodemographic characteristics and prevalence of HIV, HBV, and HCV in people who inject drugs: a multistage systematic review. Lancet Glob Health. 2017;5(12):e1192–e1207. doi:10.1016/S2214-109X(17)30375-3
12. Observatoire français des drogues et des tendances addictives [Drugs and Addictions, Key Data 2022]. Drogues et addictions, chiffres clés 2022 - 9e édition; 2022: 8.
13. Auriacombe M, Roux P, Briand Madrid L, et al. Impact of drug consumption rooms on risk practices and access to care in people who inject drugs in France: the COSINUS prospective cohort study protocol. BMJ Open. 2019;9(2):e023683. doi:10.1136/bmjopen-2018-023683
14. Roux P, Jauffret-Roustide M, Donadille C, et al. Impact of drug consumption rooms on non-fatal overdoses, abscesses and emergency department visits in people who inject drugs in France: results from the COSINUS cohort. Int J Epidemiol. 2022:dyac120. doi:10.1093/ije/dyac120
15. Lalanne L, Roux P, Donadille C, et al. Drug consumption rooms are effective to reduce at-risk practices associated with HIV/HCV infections among people who inject drugs: results from the COSINUS cohort study. Addict Abingdon Engl. 2024;119(1):180–199. doi:10.1111/add.16320
16. Medina-Perucha L, Scott J, Chapman S, Barnett J, Dack C, Family H. A qualitative study on intersectional stigma and sexual health among women on opioid substitution treatment in England: implications for research, policy and practice. Soc Sci Med. 2019;222:315–322. doi:10.1016/j.socscimed.2019.01.022
17. Ayon S, Ndimbii J, Jeneby F, et al. Barriers and facilitators of access to HIV, harm reduction and sexual and reproductive health services by women who inject drugs: role of community-based outreach and drop-in centers. AIDS Care. 2018;30(4):480–487. doi:10.1080/09540121.2017.1394965
18. Värmå Falk M, Strömdahl S, Ekström AM, et al. A qualitative study of facilitators and barriers to participate in a needle exchange program for women who inject drugs. Harm Reduction Journal. 2020;17(1):84. doi:10.1186/s12954-020-00425-9
19. Shirley-Beavan S, Roig A, Burke-Shyne N, Daniels C, Csak R. Women and barriers to harm reduction services: a literature review and initial findings from a qualitative study in Barcelona, Spain. Harm Reduct J. 2020;17(1):1–13. doi:10.1186/s12954-020-00429-5
20. Schmitt F. L’accès des femmes aux CAARUD: une discrimination négative indirecte. In: Espaces genrés des drogues: parcours dans l’intimité, la fête et la réduction des risques. Le Bord de l’eau. 2022: 71–98. Available from: https://shs.hal.science/halshs-03664595.
21. Fédération bruxelloise des Institutions pour Toxicomanes. Femmes* Genre et Assuétudes - Synthèse Des Constats de Terrain et Recommandations de La FEDITO BXL; 2023: 35.
22. Gupta GR, Oomman N, Grown C, et al. Gender equality and gender norms: framing the opportunities for health. Lancet Lond Engl. 2019;393(10190):2550–2562. doi:10.1016/S0140-6736(19)30651-8
23. Boyd J, Lavalley J, Czechaczek S et al. “Bed Bugs and Beyond”: an ethnographic analysis of North America’s first women-only supervised drug consumption site [Female-oriented programmes in addiction care: Results from the Ad-femina survey]. Int J Drug Policy. 2020;78:102733. doi:10.1016/j.drugpo.2020.102733
24. Mutatayi C. Résultats de l’enquête Ad-femina: accueil spécifique des femmes en addictologie [Female-oriented programmes in addiction care: Results from the Ad-femina survey]. Tendances. 2019;130:6.
25. Rhodes T. The ‘risk environment’: a framework for understanding and reducing drug-related harm. Int J Drug Policy. 2002;13(2):85–94. doi:10.1016/S0955-3959(02)00007-5
26. Couto E, Cruz C, Salom CL, et al. Frequent experience of discrimination among people who inject drugs: links with health and wellbeing. Drug Alcohol Depend. 2018;190:188–194. doi:10.1016/j.drugalcdep.2018.06.009
27. Larney S, Peacock A, Mathers BM, Hickman M, Degenhardt L. A systematic review of injecting-related injury and disease among people who inject drugs. Drug Alcohol Depend. 2017;171:39–49. doi:10.1016/j.drugalcdep.2016.11.029
28. Darke S. Self-report among injecting drug users: a review. Drug Alcohol Depend. 1998;51(3):253–263. doi:10.1016/S0376-8716(98)00028-3
29. Else-Quest NM, Hyde JS. Intersectionality in quantitative psychological research: ii. methods and techniques. Psychol Women Q. 2016;40(3):319–336. doi:10.1177/0361684316647953
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.