")
Back to Journals » Patient Preference and Adherence » Volume 18
Following Physician’s Advice in Late Life: The Roles of Health Beliefs and Health Status
Received 8 December 2023
Accepted for publication 17 January 2024
Published 20 January 2024 Volume 2024:18 Pages 217—226
DOI https://doi.org/10.2147/PPA.S409023
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Poshan Dahal, Eva Kahana
Department of Sociology, Case Western Reserve University, Cleveland, OH, USA
Correspondence: Poshan Dahal, Department of Sociology, Case Western Reserve University, 226 Mather Memorial Building, 10900 Euclid Avenue, Cleveland, OH, 44106-7124, USA, Tel +1-216-368-2000, Email [email protected]
Objective: This study aims to explore the influence of health-related locus of control beliefs such as belief in the role of health professionals in influencing patient health, cognitive functioning, and multimorbidity on adherence to physician’s recommendations among older adults.
Methods: A cross-sectional study involving older adults (N=684, age range = 71– 100 years) living in Clearwater, Florida, reported their adherence to physician’s recommendations, cognitive functioning, physical health, and health-related locus of control beliefs. Ordered Logistic regression was used.
Results: Older adults who believed that health professionals influence health and a person is likely to recover from illness because other people take good care of him/her had higher adherence to physician’s recommendations. Older adults who believed that their own action affects their health had lower odds of reporting adherence by 27%. Additionally, those with cognitive impairment had lower odds of reporting adherence by 38%. Functional limitations, multimorbidity, and self-image of health were not associated with adherence.
Conclusion: This is one of the first studies to consider the influence of locus of control beliefs on adherence of physician’s recommendations among community dwelling older adults. With the exception of one item “My good health is largely a matter of good fortune”, generally individuals with external locus of control had higher adherence. Our findings also underscore the policy and clinical significance of different health-related beliefs held by older adults.
Keywords: health behaviors, adherence, health beliefs, older adults, ordered logistic regression
Introduction
Adherence to health-related recommendations, such as medication, diet, and lifestyle changes, has profound implication for improving health outcomes.1–4 High prevalence of chronic illnesses and increased vulnerability to health issues with age make adherence to such recommendations even more important for older adults. Health-related recommendations such as medication adherence are critical since non-adherence among older adults with chronic conditions can have serious health consequences.5 Despite the importance of adherence to physician’s recommendations, studies have shown mixed results about the prevalence and predictors of non-adherence among older adults.6–10
Previous studies have identified various factors associated with patient adherence. These include knowledge or health literacy,11 cognitive function,12 patient–provider relationship,13 patient’s perception of physician,14 adverse effects of drugs or polypharmacy and lack of confidence in immediate or future benefits15 and other logistics and economic barriers.16 Some of the barriers to adherence may relate to a perceived lack of need. The older person who is in good health may not be concerned about health-related vulnerability.17 Other barriers may involve beliefs about locus of control, which refer to the extent to which people believe that they have control over their own fate.18 In this study context, it refers to the control people believe they have over their health. Prior research has focused on the role of health care provider on patient’s adherence to medical regimens and did not consider patient’s beliefs.19 Having strong internal locus of control beliefs may empower older adults to follow medical advice and thereby enhance their health. Conversely, strong external locus of control beliefs may result in aversion to focus on health behaviors and greater reliance on others.
Findings about the association between locus of control and health care utilizations among older adults are mixed.20–22 Chipperfield and Greenslade23 explored the connection between locus of control and health care utilization. They found that older adults who had low level of internal locus of control had higher use of health care services – visited physicians more often, had more laboratory tests, and stayed longer in the hospital. Hong et al,24 in a study of anti-hypertensive medication use found more adherence among individuals with higher internal locus of control and lower external locus of control. De Jesus and Xiao20 on the other hand found a weak impact of health-related locus of control on health care utilization after accounting for access to health insurance. Neither of these studies, however, explored the recommendations by care providers and adherence by the patient. Furthermore, researchers have not previously explored the different dimensions of health-related locus of control and their separate influences on adherence.
Existing literature on patient adherence points to the critical importance of adherence to medical advice especially among individuals with chronic conditions.25 A systematic review of articles about adherence by Yap et al9 found that health conditions such as impaired vision, poor physical function, and lower self rated health predicted low adherence among older adults aged 65 years and older. Perceived control and the subsequent adherence can also be the result of the individual’s comorbid conditions. Henninger et al26 in a study of community-dwelling older adults observed that individuals with more chronic conditions exhibited more external locus of control than older adults with fewer comorbid conditions. This finding further bolsters the need to understand the relationship between locus of control and adherence to physician’s recommendation.
Studies have found negative associations between regimen complexity, cognitive impairment, and medication adherence.16 Hulka et al27 observed that with greater complexity of scheduling older adult were likely to have higher errors of commission (taking drugs not prescribed by physicians) and scheduling misconceptions (taking prescribed drugs, but on the wrong schedule). Similar observation was made by Abada et al28 among community dwelling older adults with self-neglect. These researchers observed that the medication regimen complexity was a contributor to low-adherence rate. Stilley et al29 also reported similar associations between medication adherence and deficits in attention/mental flexibility and/or working memory.
Despite the importance of the need of understanding determinants of adherence to the recommendation by health care providers, such influences still are not fully unexplored16 and systematically undefined. Studies have considered different factors that can affect patient adherence to treatment and medication use such as the physician–patient relationship.19 However, the influence of patient’s own health-related beliefs on adherence has not been explored yet. Moreover, the existing literature is largely limited to medication adherence and therefore, overlooks adherence to other recommendations that can also have significant health implications. Consequently, our study sought to investigate influences on adherence to medical recommendations among older adults.
In this study, we examined the influence of multimorbidity and health-related locus of control on older adults’ adherence to health care provider’s recommendations. We hypothesized that older adults who believe that their own actions affect their health will have higher adherence to physician’s or health care provider’s recommendations than older adults who believe that their health is controlled by external forces beyond their control. We also anticipated that older adults who have more chronic conditions (and therefore need more medications and care) will have higher adherence than those with fewer chronic conditions. Furthermore, we also anticipated that individuals with cognitive impairment will have greater difficulty recalling the physicians’ recommendations and therefore will have lower adherence.
Materials and Methods
Data and Sample
Data for this study were obtained from the study of successful aging conducted by Elderly Care and Research Center.30 This study was conducted among independent, retirement community dwelling older adults living in Clearwater, Florida, USA. All the residents in these settings were over the age of 65 years and lived independently. Baseline data collection occurred in 1990. Only older adults who were living in retirement communities that provided no service were selected for the study. Anyone who was above the age of 72 years was eligible to participate, and their spouses were also eligible to be included. All residents, regardless of racial background or other demographic characteristics were eligible to participate. As it turns out, the vast majority of residents were white, reflecting the demographic profile of US retirement communities. Therefore, our sample included white older adults only. However, there were no race- based inclusion or exclusion criteria. The settings attracted predominantly residents from among older adults living up north (see Kahana, Kelley-Moore & Kahana31 for more details about the sampling procedure). Written informed consent was obtained from each participant prior to the study commencement. Ethical approval for this study was obtained from the Institutional Review Board of Case Western Reserve University. Our study also complies with the Declaration of Helsinki. For this study, we utilized data from wave 3 which was collected in 1992 since the health-related locus of control variables was measured in this wave only. We recognize that the data were collected some time ago. However, it is unlikely that the relationship between locus of control and adherence to physician’s recommendations would change over time. A total of 788 respondents were interviewed in wave 3. However, for this analysis, we excluded 104 individuals with missing information on the dependent variable. Our sample size, after excluding observations with missing information, was 684. Out of those 104 respondents with missing data, 70% were female, they had poorer health compared to our final sample. The respondents with missing data, who were excluded from the analysis, had 4 (SD = 8.09) disabilities and 4.14 (SD = 2.32) chronic conditions on average, with about 48% reporting that they have poor or fair health. It is notable that our sample was healthier than those who were excluded due to missing values. The health status of respondents was relatively better compared to older people of similar age since they were residents of an independent living retirement community that offered few services.32
Measures
Adherence to physician’s recommendations. Adherence to physician’s recommendations is our dependent variable of this study. Adherence to physician’s recommendations was measured by asking respondents “How often do you follow advice provided by your physician or medical care provider?” Responses ranged from 1 (= never) to 5 (=always). Less than 2% responded 1 (=never) and less than 1% responded 2 (= rarely). Therefore, for this analysis, along with response category 3 (=occasionally), we recoded the above categories as “less than frequently”. Our sensitivity analysis (not presented here) with the 5 categories and 4 categories (first and second categories from the 5 categories scale collapsed to form a single category: “never or rarely”) showed similar results.
Self-rated health. Respondents were asked how they rate their health in general and their responses were classified as 1 (=poor or fair), 2 (=good), and 3 (=excellent).
Total doctor visits. Respondents were asked how many times they visited a physician in the past year. On average, respondents said they had 7.34 visits (SD = 8.47) in the past year.
Cognitive impairment. This was measured using the 10-item Short Portable Mental Status Questionnaire (SPMSQ).33 Participants were asked a series of 10 questions (eg, “What year is it?” “What is the name of the President?” “What is your telephone number?” and responses to these questions were recorded as 0 (= correct, reflecting no mistakes) or 1 (= incorrect). For this analysis, responses were summed and recoded into three categories (1 = 0 or 1 incorrect, 2 = two incorrect, and 3 = three or more incorrect) where higher value indicated greater cognitive impairment.
Chronic illnesses. Respondents were asked about their health conditions in the past year. They were asked if they had hypertension, arthritis or rheumatism, glaucoma, cataracts, asthma, emphysema or bronchitis, osteoporosis, heart troubles, circulatory problems, diabetes, ulcers, liver disease, kidney disease, other urinary tract disorders, skin cancer, anemia, or stroke in the past year. Responses were recorded as 0 (= no) or 1 (= yes) for each of these conditions. For this analysis, we added the responses to create a summative scale ranging between 0 (= does not have any chronic condition) and 10 (= has all chronic conditions). On an average, respondents had 3.54 (SD=2.01) chronic conditions.
Disability. We utilized Lawton’s34 Activities of Daily Living (ADL) and Instrumental Activities of Daily Living (IADL) items to measure disability.35 ADL was measured by asking how often respondents had trouble in carrying out six different activities: bathing, dressing, and putting on shoes, getting to or using the toilet, getting in/out of bed unassisted, eating without assistance, and getting in/out of chair, during the past year. Their responses to each of these activities ranged between 0 (= never) and 3 (= always). Instrumental Activities of Daily Living (IADL) limitation were measured by asking participants how often they have trouble in carrying out six activities: “Getting yourself from room to room”, “Going out of doors”, “Walking up and down stairs”, “Doing your own housework”, Preparing your own meals’, and “Shopping for groceries”. Responses to each question ranged between 0 (= never) and 3 (= always). We added the responses to ADL and IADL limitations to construct a summative disability scale ranging between 0 (= no difficulty on any item) to 36 (= difficulty in all items all the time). A high Cronbach’s alpha (= 0.85) showed that the items used to create disability scale were strongly interrelated. In the sample, response to the disability score ranged between 0 and 33.
Health related multidimensional locus of control. Respondents were given nine different multidimensional health-related locus of control36 related statements
Luck plays a big part in determining how soon I will recover from an illness, ‘Health professionals control my health’, ‘The main thing which affects my health is what I myself do’, ‘When I recover from an illness, it’s usually because other people have been taking good care of me
“My good health is largely a matter of good fortune”, “If I get sick, it is my own behavior which determines how soon I get well again”, “If I take care of myself, I can avoid illness”, “No matter what I do, I’m likely to get sick, and “Regarding my health, I can only do what my doctor tells me to do”) and their responses were recorded in a 5-point Likert scale which ranged between 0 (= strongly disagree) to 5 (= strongly agree). Each health-related locus of control variable was entered into the model separately in order to estimate an independent effect of these individual variables on our dependent variable. Due to low interrelationship between these items, for this analysis, we treated them as separate variables.
Other covariates. Age, level of education, gender, and marital status are the other covariates used in the analysis. Marital status was recoded as 1 (= married) and 0 (= others). Education was measured in years. For this analysis, less than 2% participants who had education above 19 years were top coded at 19.
Data Analysis
Following our exploratory analysis, we employed ordered logistic regression to estimate the relationship between adherence to physician’s recommendations and the independent variables. Since the dependent variable is measured on an ordinal scale, ordered logistic regression helped us retain maximum information in the dependent variable. Analysis was performed using STATA 16, and ologit command in STATA was used to estimate models. Ordered logistic regression assumes proportional odds ratio, and we tested this assumption using the brant command in STATA. Non-significant p value (0.591) indicated that the proportional odds assumption was not violated.
Prior to moving to the multivariate models, we ran simple regression models for each health-related locus of control item to check their independent effect on our outcome variable. Only 5 out of the 9 of these items were significant predictors of adherence to the recommendations. Therefore, only items significant at the bivariate level were retained for further exploration with multivariate analysis.
At the bivariate level, four health-related locus of control variables (“Luck plays a role in how soon I will recover”; “If I get sick, it is my own behavior which determines how soon I get well again”; “If I take care of myself, I can avoid illness”; “No matter what I do, I am likely to get sick”) were not significant (not shown). We fit two models to estimate the effect of locus of control and health status on adherence to physician’s recommendations. Model 1 only has the five-health related locus of control beliefs that were significant at bivariate level. In Model 2, we added other health and disability measures and adjusted the model for other covariates.
Results
Table 1 presents the descriptive statistics of the study variables. The average age of participants was 80.70 years (SD = 4.51). The majority of the respondents were women (65.20%). The mean years of education was 13.63 years, and 46.05% respondents were married. In terms of health status, more than half of the respondents (67.98%) said that they had either “excellent health” or “good health”, and about one-fifth (21.35%) of respondents had some cognitive impairment. About one-fourth (27.78%) of respondents reported having IADL limitations. The overwhelming majority of respondents (92.54%) did not have ADL limitation (not shown in the table), which suggests that overall, most of the respondents had good functional health. Respondents reported 7.34 visits to physician in the past year and only 2.19% respondent had not visited physician in the past year. Pearson’s correlation showed a positive association between the number of physicians visits and the number of chronic conditions (r = 0.22, p < 0.000).
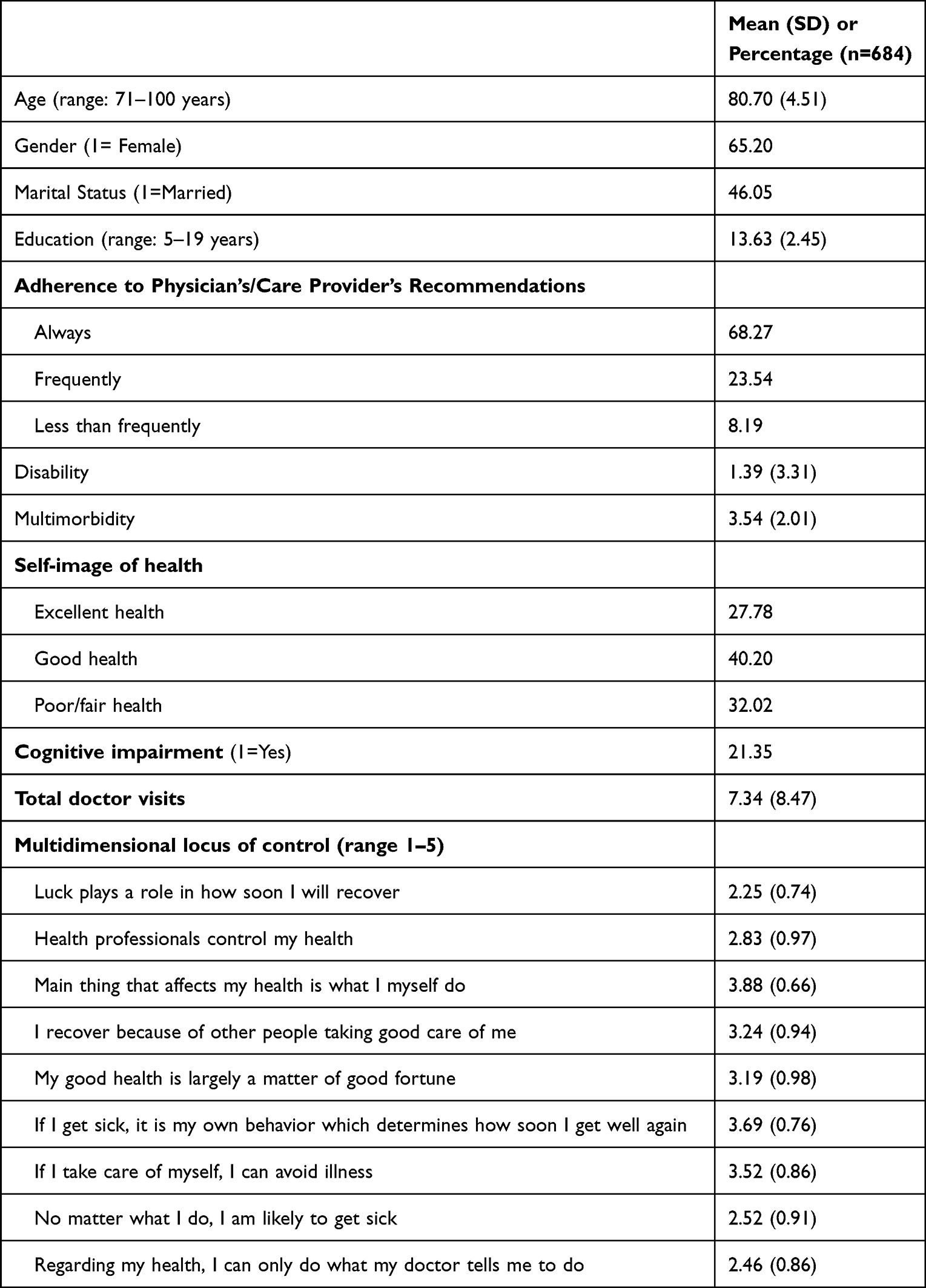 |
Table 1 Descriptive Statistics of Study Variables |
The majority of the respondents (68.27%) reported that they always follow recommendations given by their physician or health care provider, whereas only about one-fourth (23.54%) said that they follow their recommendations frequently and 8.19% said that they follow their advice less frequently. Further analysis showed that those who said that they follow physician’s recommendations less frequently, on average had 3.07 chronic conditions, which is 0.51 less compared to those who said they follow the recommendations always or frequently (3.58 and 3.58 respectively). One-way ANOVA analysis showed no difference between the mean hospital visits between those who follow physician’s recommendations always, frequently, and less frequently (F=1.17, p=0.31). Older adults who reported IADL limitation were more likely to follow the recommendations (Chi2=13.85, P<0.01), but ADL was not significantly associated with adherence (Chi2=3.43, p=0.18).
Results from Ordered logistic regression are presented in Table 2. Model 1 represents the influence of the health-related locus control variable on adherence controlling for demographic variables, while model 2 accounts for four health-related measures in addition to the variables in model 1. Model 1 suggests a statistically significant positive relationship between physician adherence and the belief that health professionals control one’s health, controlling for covariates. Older adults who think more strongly that their health is controlled by health professional had higher odds of reporting more adherence to physician recommendations (OR=1.35, p<0.001) in model 1. This association is slightly weakened but remained significant (OR=1.34, p<0.001) after controlling for health status, functional limitations, and other covariates in model 2.
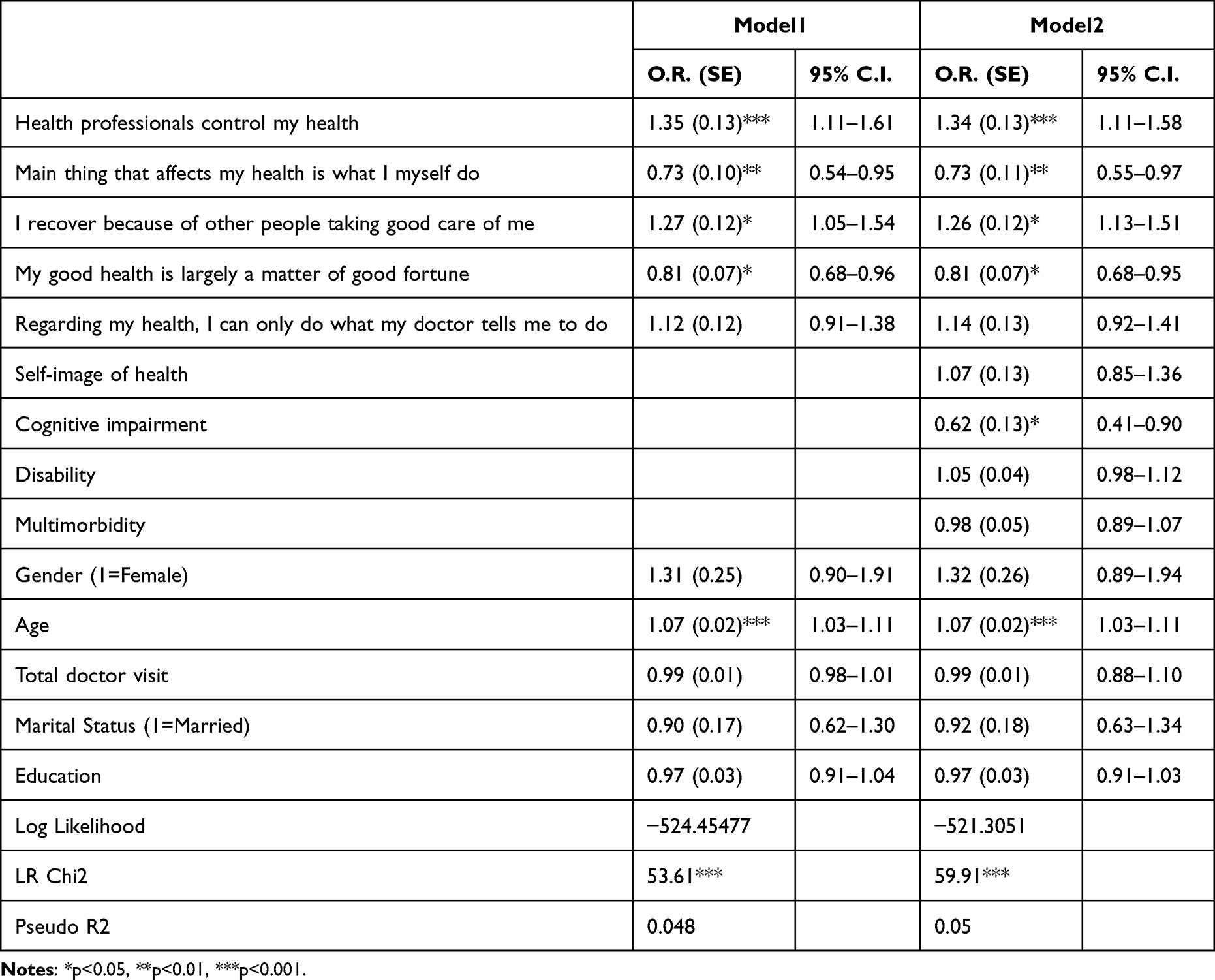 |
Table 2 Ordinal Regression Model Estimates Representing the Influence of Multidimensional Locus of Control |
Older adults who think more strongly that they recover from illness because of other people taking good care of them had significantly higher odds (OR=1.27, p<0.05) of reporting more adherence to physician or care providers recommendations.
Older adults who more strongly believe that the main factor that affects health is what they do themselves had lower odds of adherence to physician’s recommendations (OR=0.73, p<0.01). This relationship remained the same in model 2 even after adjusting for cognitive health, disability, multimorbidity, self-image of health, and other covariates. Further analysis showed that those who said that they “strongly agree” and “agree” that the main thing that affects their health is what they do themselves were relatively healthy and had lower mean chronic conditions (3.15 and 3.52 respectively) compared to those who disagreed (3.79) or strongly disagreed (4.05).
Likewise, older adults who more strongly believed that health is largely a matter of good fortune, had lower odds of adherence to physician’s or care provider’s recommendations (OR=0.81, p<0.05). This relationship remained the same even after entering other health status and functional limitation variables and adjusting for other covariates in model 2.
For respondents with cognitive impairment, the odds of adherence to physician’s or care provider’s recommendation always versus the combined frequently and less frequently was 0.62 (p<0.05) times lower than for older adults who did not have cognitive impairment. Disability, however, was a not a significant predictor of adherence to physician’s or care giver’s recommendations. Age was also positively associated with higher adherence. For every one-year increase in age, the odds of adhering to physician’s or care providers recommendations always and frequently versus less frequently was 1.07 (p<0.001) times greater. Marital status, gender, and education were not significant predictors of the level of adherence to physician’s or health care provider’s recommendations.
Discussion
Our findings provide evidence of the significance of health-related locus of control beliefs on older adult’s adherence to physician’s or health care provider’s recommendations. However, we found that not all health-related beliefs predicted adherence. Our finding shows that older adults who believe that health care professionals control their health had higher adherence to those recommendations compared to those who believed so less. Patient trust in physicians has been shown to have positive effects on adherence37,38 and this shows the possible link between the belief that health care providers control health and patient trust in them. This also indicates that people who believe that health professionals control their health also value the significance of such recommendations. Additionally, our finding shows that older adults who believe that health is a matter of good fortune had lower adherence. Patients’ beliefs about the influence of good fortune on their health reflect an unexpected reliance to external influences. Older adults who had internal locus of control of health beliefs had lower adherence to the recommendations of the physician’s or care provider. Respondents who agreed or strongly agreed that the main thing that affects their health is what they do themselves had lower number of chronic conditions and healthier than those who disagreed or strongly disagreed. However, no difference in hospital visit was observed among them, indicating that this relationship between internal locus of control and adherence was not a function of their encounter with physician in the past year. This finding contradicts previous studies about patient adherence to medication and internal locus of control variables.39,40 However, these prior studies were based on relatively younger samples than our study.
Our study found that older adults who had any cognitive impairment were likely to report low adherence. However, multiple chronic conditions were not a significant predictor of adherence. Our findings about cognitive impairment are consistent with previous studies in this area.12,28 For older adults with cognitive impairment regimen complexity and recall issues can cause low adherence.
Our analysis did not find any association between self-rated health and adherence to physician recommendations. This finding contradicts some previous studies conducted among older adults.41 Our study also found a positive association between age and adherence to recommendations. This finding is consistent with prior studies about medication adherence among older adults.10,42 This could indicate higher adherence as people age. However, we suggest caution in interpreting this finding only as an age effect, as alternatively, this could indicate a cohort difference, given the cross-sectional data used in this study.
We did not find any difference in adherence to recommendations by gender and marital status. No association between marital status and adherence could be due to health behaviors which are not practiced without being reminded by partners. This would be possible if one was married or living with partner. However, this non-association may mean that older adults make these decisions about adherence to recommendations based on their own beliefs about medication as found in previous studies.42–45
We suggest that our findings should be viewed in the context of diminished continuity of care and reduced trust between patients and doctors. Indeed, it has been argued that diminished trust in doctors in the era of managed care is likely to impact adherence to medical recommendations.46 Accordingly, adherence can be viewed as a relational construct that transcends patient attitudes and characteristics. Our study findings point to the value of considering patient’s locus of control beliefs for understanding their adherence to physician’s recommendations. Discussions between patients and physicians about patient’s health beliefs could prove beneficial.
There are several limitations of this study. Our study was conducted in the context of independent living older adults who preferred to relocate to retirement communities. It may not be generalized to older adults in other contexts. It is possible that more physically impaired older adults would exhibit different pattern of adherence to physician’s recommendations. Our sample is comprised of relatively healthy older adults who were Whites. Thus, the study findings may not reflect the adherence to physician’s recommendations among other racial/ethnic groups. Our dependent variable was self-reported by the respondents and therefore can differ from the actual practices of older adults. Self-reported assessment of adherence to physician’s or health care providers’ recommendations can undercount non-adherences due to memory or recall issues or misunderstood recommendations or schedules. For adherence regarding medication use, using administrative datasets for prescription drug use can provide useful insights. However, single measure of dependent variable (eg, medication use) may not be able to capture all dimensions of the adherence to recommendations. In the paper, we used cross-sectional data, since the adherence questions were asked in only one wave. A longitudinal design would better show the relationship between the outcome and predictors.
Conclusion
Our study has valuable theoretical, policy, and clinical implications. Our findings underscore the need to reflect on the different dimensions of patient adherence as well as the need to consider health-related locus of control in understanding patient adherence among older adults. This study also provides evidence of the significance of the health care-related beliefs held by older adults as well as some physical and cognitive conditions which can have significant implications on patient adherence to physicians’ or care provider’s recommendations.
The concept of adherence to recommendations by physicians or health care providers is not very well defined in gerontological literature. We believe that future studies should aim to provide a clear understanding of the different aspects of the recommendations and should go beyond adherence to medication use. Future research could benefit from focusing on older adult’s locus of control beliefs in relationship to adherence to health care recommendations. Our study provides evidence for influence of select health-related locus of control beliefs and cognitive impairment on adherence to physicians’ or providers’ recommendations. Our findings underscore the policy and clinical significance of these health-related beliefs held by older adults.
Acknowledgment
We would like to thank our colleagues Polina Ermoshkina, MA and Tirth Raj Bhatta, PhD for their constructive feedback.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Conn VS, Hafdahl AR, Cooper PS, Ruppar TM, Mehr DR, Russell CL. Interventions to improve medication adherence among older adults: meta-analysis of adherence outcomes among randomized controlled trials. Gerontologist. 2009;49(4):447–462. doi:10.1093/geront/gnp037
2. DiMatteo MR, Giordani PJ, Lepper HS, Croghan TW. Patient adherence and medical treatment outcomes a meta-analysis. Med Care. 2002;40(9):794–811. doi:10.1097/00005650-200209000-00009
3. Horwitz RI, Horwitz SM. Adherence to treatment and health outcomes. Archiv Int Med. 1993;153(16):1863–1868. doi:10.1001/archinte.1993.00410160017001
4. Vik SA, Maxwell CJ, Hogan DB. Measurement, correlates, and health outcomes of medication adherence among seniors. Ann Pharmacother. 2004;38(2):303–312. doi:10.1345/aph.1D252
5. Chew SM, Lee JH, Lim SF, Liew MJ, Xu Y, Towle RM. Prevalence and predictors of medication non‐adherence among older community‐dwelling people with chronic disease in Singapore. Journal of Advanced Nursing. 2021;77(10):4069–4080. doi:10.1111/jan.14913
6. Botelho RJ, Dudrak R. Home assessment of adherence to long-term medication in the elderly. J Fam Pract. 1992;35(1):61–65.
7. van Eijken M, Tsang S, Wensing M, de Smet PA, Grol RP. Interventions to improve medication compliance in older patients living in the community: a systematic review of the literature. Drugs Aging. 2003;20(3):229–240. doi:10.2165/00002512-200320030-00006
8. Chung GC, Marottoli RA, Cooney LM, Rhee TG. Cost‐related medication nonadherence among older adults: findings from a nationally representative sample. J Am Geriatr Soc. 2019;67(12):2463–2473. doi:10.1111/jgs.16141
9. Yap AF, Thirumoorthy T, Kwan YH. Medication adherence in the elderly. J Clin Gerontol Geriatrics. 2016;7(2):64–67. doi:10.1016/j.jcgg.2015.05.001
10. Cheen MHH, Tan YZ, Oh LF, Wee HL, Thumboo J. Prevalence of and factors associated with primary medication non‐adherence in chronic disease: a systematic review and meta‐analysis. Int J Clin Pract. 2019;73(6):e13350. doi:10.1111/ijcp.13350
11. Zhang NJ, Terry A, McHorney CA. Impact of health literacy on medication adherence: a systematic review and meta-analysis. Ann Pharmacother. 2014;48(6):741–751. doi:10.1177/1060028014526562
12. Hayes TL, Larimer N, Adami A, Kaye JA. Medication adherence in healthy elders: small cognitive changes make a big difference. J Aging Health. 2009;21(4):567–580. doi:10.1177/0898264309332836
13. Beach MC, Keruly J, Moore RD. Is the quality of the patient-provider relationship associated with better adherence and health outcomes for patients with HIV? J Gen Intern Med. 2006;21(6):661–665. doi:10.1111/j.1525-1497.2006.00399.x
14. Ward LM, Thomas J. Patient perception of physicians and medication adherence among older adults with hypertension. J Aging Health. 2020;32(1–2):95–105. doi:10.1177/0898264318806390
15. Grant RW, Devita NG, Singer DE, Meigs JB. Polypharmacy and medication adherence in patients with type 2 diabetes. Diabetes Care. 2003;26(5):1408–1412. doi:10.2337/diacare.26.5.1408
16. Gellad WF, Grenard JL, Marcum ZA. A systematic review of barriers to medication adherence in the elderly: looking beyond cost and regimen complexity. Am J Geriatric Pharmacother. 2011;9(1):11–23. doi:10.1016/j.amjopharm.2011.02.004
17. Shtompel N, Whiteman K, Ruggiano N. Negative feelings and help seeking among older adults with chronic conditions. J Gerontol Soc Work. 2014;57(8):810–824. doi:10.1080/01634372.2014.898008
18. Ng TW, Sorensen KL, Eby LT. Locus of control at work: a meta‐analysis. J Organizational Behav. 2006;27(8):1057–1087. doi:10.1002/job.416
19. Koulayev S, Simeonova E, Skipper N. Can physicians affect patient adherence with medication? Health Econom. 2017;26(6):779–794. doi:10.1002/hec.3357
20. De Jesus M, Xiao C. Predicting health care utilization among Latinos: health locus of control beliefs or access factors? Health Educ Behav. 2014;41(4):423–430. doi:10.1177/1090198114529130
21. Kesavayuth D, Poyago-Theotoky J, Zikos V, Zikos V. Locus of control, health and healthcare utilization. Econ Modell. 2020;86:227–238. doi:10.1016/j.econmod.2019.06.014
22. Strudler Wallston B, Wallston KA. Locus of control and health: a review of the literature. Health Educat Monograph. 1978;6(1):107–117. doi:10.1177/109019817800600102
23. Chipperfield JG, Greenslade L. Perceived control as a buffer in the use of health care services. J Gerontol B. 1999;54:3.
24. Hong TB, Oddone EZ, Dudley TK, Bosworth HB. Medication barriers and anti-hypertensive medication adherence: the moderating role of locus of control. Psychol Health Med. 2006;11(1):20–28. doi:10.1080/14786430500228580
25. Vermeire E, Hearnshaw H, Van Royen P, Denekens J. Patient adherence to treatment: three decades of research. A comprehensive review. J Clin Pharm Ther. 2001;26(5):331–342. doi:10.1046/j.1365-2710.2001.00363.x
26. Henninger DE, Whitson HE, Cohen HJ, Ariely D. Higher medical morbidity burden is associated with external locus of control. J Am Geriatr Soc. 2012;60(4):751–755. doi:10.1111/j.1532-5415.2012.03904.x
27. Hulka BS, Cassel JC, Kupper LL, Burdette JA. Communication, compliance, and concordance between physicians and patients with prescribed medications. Am J Public Health. 1976;66(9):847–853. doi:10.2105/AJPH.66.9.847
28. Abada S, Clark LE, Sinha AK, et al. Medication regimen complexity and low adherence in older community-dwelling adults with substantiated self-neglect. J Appl Gerontol. 2019;38(6):866–883. doi:10.1177/0733464817714565
29. Stilley CS, Bender CM, Dunbar-Jacob J, Sereika S, Ryan CM. The impact of cognitive function on medication management: three studies. Health Psychol. 2010;29(1):50. doi:10.1037/a0016940
30. Kahana E, Lawrence RH, Kahana B, et al. Long-term impact of preventive proactivity on quality of life of the old-old. Psychosomatic Med. 2002;64(3):382–394. doi:10.1097/00006842-200205000-00003
31. Kahana E, Kelley-Moore J, Kahana B. Proactive aging: a longitudinal study of stress, resources, agency, and well-being in late life. Aging Ment Health. 2012;16(4):438–451. doi:10.1080/13607863.2011.644519
32. Lee JE, Kahana B, Kahana E. Social support and cognitive functioning as resources for elderly persons with chronic arthritis pain. Aging Ment Health. 2016;20(4):370–379. doi:10.1080/13607863.2015.1013920
33. Pfeiffer E. A short portable mental status questionnaire for the assessment of organic brain deficit in elderly patients. J Am Geriatr Soc. 1975;23(10):433–441. doi:10.1111/j.1532-5415.1975.tb00927.x
34. Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. 1969;9(3_Part_1):179–186. doi:10.1093/geront/9.3_Part_1.179
35. Graf C. The Lawton instrumental activities of daily living (IADL) scale. Medsurg Nurs. 2009;18(5):315–316.
36. Wallston KA, Strudler Wallston B, DeVellis R. Development of the multidimensional health locus of control (MHLC) scales. Health Educat Monograph. 1978;6(1):160–170. doi:10.1177/109019817800600107
37. Stavropoulou C. Non-adherence to medication and doctor–patient relationship: evidence from a European survey. Patient Educ Couns. 2011;83(1):7–13. doi:10.1016/j.pec.2010.04.039
38. Thom DH, Kravitz RL, Bell RA, Krupat E, Azari R. Patient trust in the physician: relationship to patient requests. Fam Pract. 2002;19(5):476–483. doi:10.1093/fampra/19.5.476
39. Omeje O, Nebo C. The influence of locus control on adherence to treatment regimen among hypertensive patients. Patient Preference Adherence. 2011;5:141–148. doi:10.2147/PPA.S15098
40. Morowatisharifabad MA, Mahmoodabad SSM, Baghianimoghadam MH, Tonekaboni NR. Relationships between locus of control and adherence to diabetes regimen in a sample of Iranians. Int J Diabetes Dev Countries. 2010;30(1):27. doi:10.4103/0973-3930.60009
41. Rodgers JE, Beyhaghi H, Sueta CA, et al. Predictors of medication adherence in the elderly: the role of mental health. Med Care Res Rev. 2018;75(6):746–761. doi:10.1177/1077558717696992
42. Fernandez-Lazaro CI, García-González JM, Adams DP, et al. Adherence to treatment and related factors among patients with chronic conditions in primary care: a cross-sectional study. BMC Fam Pract. 2019;20(1):1–12. doi:10.1186/s12875-019-1019-3
43. Park HY, Seo SA, Yoo H, Lee K. Medication adherence and beliefs about medication in elderly patients living alone with chronic diseases. Patient Prefer Adher. 2018;Volume 12:175–181. doi:10.2147/PPA.S151263
44. Ge L, Heng BH, Yap CW. Understanding reasons and determinants of medication non-adherence in community-dwelling adults: a cross-sectional study comparing young and older age groups. BMC Health Serv Res. 2023;23(1):905. doi:10.1186/s12913-023-09904-8
45. Widyakusuma NN, Suryawati S, Wiedyaningsih C. What do seniors believe about medication adherence? A qualitative study among seniors with chronic conditions in Yogyakarta, Indonesia. Patient Preference Adherence. 2023;Volume 17:1381–1392. doi:10.2147/PPA.S412981
46. Thom DH, Hall MA, Pawlson LG. Measuring patients’ trust in physicians when assessing quality of care. Health Affairs. 2004;23(4):124–132. doi:10.1377/hlthaff.23.4.124
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.