")
Back to Journals » Patient Preference and Adherence » Volume 18
Factors Related to Treatment Non-Adherence Among Caregivers of Pediatric and Adolescent Growth Hormone Deficiency Patients in Japan
Authors Akazawa M , Sato T , Ebata N , LoPresti M , Nishi R
Received 26 October 2023
Accepted for publication 6 February 2024
Published 8 March 2024 Volume 2024:18 Pages 607—622
DOI https://doi.org/10.2147/PPA.S446649
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Manabu Akazawa,1 Takahiro Sato,2 Nozomi Ebata,2 Michael LoPresti,3 Ryosuke Nishi3
1Department of Public Health and Epidemiology, Meiji Pharmaceutical University, Kiyose, Tokyo, Japan; 2Medical Affairs, Rare Disease, Pfizer Japan Inc, Shibuya-ku, Tokyo, Japan; 3Value & Access, INTAGE Healthcare Inc., Chiyoda-ku, Tokyo, Japan
Correspondence: Takahiro Sato, Pfizer Japan Inc, 3-22-7 Yoyogi, Shibuya-ku, Tokyo, 151-8589, Japan, Tel +81 90-2935-0848, Email [email protected]
Background: About one-third of caregivers of pediatric or adolescent growth hormone deficiency (pGHD) patients in Japan have reported poor treatment adherence. However, few studies have examined factors related to adherence for that group.
Objective: The aim of this study is to consider factors related to poor adherence to daily treatment among caregivers of pGHD patients in Japan.
Methods: A cross-sectional survey was conducted among caregivers of pGHD patients in Japan. Caregivers were asked about demographic and treatment characteristics, health literacy, treatment satisfaction, opinions about treatment, and treatment adherence. Health literacy was assessed using the 14-item health literacy scale (HLS-14). Adherence was assessed using the 8-item Morisky Medication Adherence Scale (MMAS-8). Statistical association with adherence was considered using Chi-square and Student’s t–testing. An exploratory factor analysis (EFA) and K-means cluster analysis was conducted to consider the influence of treatment satisfaction and opinions concerning treatment on adherence.
Results: Responses were collected from 112 caregivers. The caregiver’s age being 30– 39 years old, the primary caregiver being male, the primary caregiver being employed, and low functional health literacy for the caregiver were associated with poor adherence. Patients being pre-elementary school age was also associated with poor adherence. Low satisfaction with drug treatment and/or their device and communication with healthcare professionals (HCPs), and lack of agreement with the importance of treatment management (eg, keeping injection records, getting informed about the disease/therapy, reporting non-adherence, and sticking to an administration schedule), were also associated with poor adherence.
Conclusion: Strategies to improve treatment adherence among caregivers of pGHD patients in Japan should consider the age, gender, and employment status of the caregiver – as well as their functional literacy. Improvement in satisfaction with the drug or device used, better communication with HCPs, and greater awareness of the importance of treatment management, may also lead to better adherence.
Keywords: growth hormone, adherence, determinants, satisfaction, communication, health literacy
Introduction
Growth hormone deficiency (GHD) is said to affect less than 1% of the pediatric population in Japan with about 2000 new GHD patients per year.1–3 While GHD can also affect adults, GHD is typically diagnosed at a young age necessitating the involvement of parents in the management of treatment.4,5 Subcutaneous injections of recombinant human growth hormone (rhGH) have been available in Japan since 1988 and are recommended as treatment for GHD with many parents and patients involved in self-administration of treatment injections.2,5 The importance and benefits of regular treatment with rhGH has been well-documented and lack of adherence to hGH treatment has been shown to be associated with a number of negative outcomes, including poorer clinical outcomes, poorer QOL, and higher treatment costs.5–11
Despite the potential benefit of hGH treatment and the positive relationship between adherence and treatment outcomes, adherence with treatment has been shown to be suboptimal. Adherence to treatment may be defined as the extent that recommendations from healthcare professionals (HCPs) concerning treatment administration are followed including the amount to be administered and the frequency of administrations, for example.12–17 A previous analysis of findings from this study reported that about one-third of caregivers of pediatric and adolescent GHD patients in Japan report poor adherence.18 An online study conducted in 2015 among Japanese persons that reported having been treated for GHD, or that had children that were treated for GHD, also found that nearly two-thirds (64.3%) had missed a treatment in the past.7 The same study showed that about 1 out of 4 caregivers of pGHD patients do not always follow the instructions of the physician concerning administration of treatment. In fact, 20% said that they follow the instructions of their physician only 70–89% of the time, and 3.5% said they follow the instructions of their physician less than 70% of the time overall. Other studies conducted in Japan have reported higher levels of adherence to hGH treatment but were conducted in a clinical trial setting where treatment adherence is expected to be higher.19,20
While previous studies have shown that adherence to GH treatment among pediatric and adolescent patients is poor for many patients in Japan, factors associated with poor adherence among caregivers of pediatric and adolescent GHD patients in Japan is less clear. Previous findings suggest that forgetfulness, going somewhere overnight, refusal/resistance by the patients to undergo treatment, concern about side effects / safety, and being busy with school activities are some more common reasons for skipping treatment.18 Among those, forgetfulness, concern about side effects, and concern about safety have been shown to be associated with poor adherence. Several recent systematic literature reviews were also identified that considered factors related to poor adherence to GH treatment.17,21,22 Together they point to a combination of patient, caregiver, and treatment characteristics that may influence adherence.
Patient and caregiver characteristics that have been shown to influence adherence include the age of the patient and their duration of treatment, the level of education of the caregiver, lack of knowledge and understanding about GHD and its treatment, the degree of forgetfulness of the caregiver, and being away from home.17,21,22 Treatment characteristics that have been shown to influence adherence include administration frequency, the design of their injection device, pain / discomfort associated with treatment, and the quality of their relationship with HCPs.17,21,22 While not explicitly mentioned in previous studies, aspects concerning treatment satisfaction and opinions concerning treatment management are also thought to influence treatment adherence among caregivers of pediatric and adolescent GHD patients in Japan. A closer examination of the factors related to adherence among caregivers in Japan may help inform treatment decisions and approaches to improve adherence.
For this study we examine patient, caregiver, and treatment characteristics associated with adherence among caregivers of pediatric and adolescent GHD patients in Japan. We also consider how health literacy among caregivers, the degree of satisfaction with different aspects of treatment and the opinions of caregivers concerning treatment can affect adherence to daily hGH treatment among caregivers of pGHD patients in Japan.
Methods
Study Design and Participants
A cross-sectional survey was conducted in September 2021 among caregivers of patients being treated for pGHD or for being small for gestational age (SGA), that had been treated with growth hormones for 3 months or more. The study inclusion criteria were those involved in the administration of daily hGH injections for at least the past 3 months or longer to children aged 3–14 years old with GHD or being SGA. All caregivers or their spouse/partner were the primary person administering rhGH to the patient.
A detailed description of the recruitment process for caregivers is included in the initial analysis of treatment adherence described by Akazawa et al 2022.18 Caregivers were recruited from a registered panel of Japanese consumers maintained by INTAGE Inc. (Tokyo, Japan) and a separate consumer panel managed by Rakuten Insight, Inc. For this study, we aimed for a minimum of 100 responses from caregivers based on what was felt to be achievable using an online consumer panel. Data collection was completed between September 9, 2021 to September 16, 2021. An online survey comprising 29 questions was conducted. The survey instrument was developed by the authors after a targeted review of existing literature on factors related to adherence to daily hGH treatment among pediatric and adolescent patients and caregivers. The draft survey instrument was reviewed by medical affairs specialists at Pfizer Japan Inc. (Tokyo, Japan) that specialize in GHD to improve its comprehension. Caregivers were contacted to answer an initial online screening questionnaire. Those meeting the study inclusion criteria were invited to participate in the main online survey.
Survey Content
The online survey was developed by the authors following a targeted literature review of previous studies that considered aspects associated with treatment adherence for GHD patients and their caregivers. In addition to questions concerning treatment adherence, the survey included various questions on the background of the caregiver respondents, the primary caregiver, and the patients that they care for. Caregivers were asked about their age, gender, the number of children under the age of 18 living at home, the gender of the primary caregiver (ie, the person primarily administering treatment), the employment status of the primary caregiver, the highest educational attainment of the primary caregiver, their annual household income, and their health literacy. Concerning the patients, the survey included questions about their gender and school age (ie, school year). Caregivers were also asked about various aspects concerning treatment for the GHD patient including the kind of facility they primarily visit, the department (specialty) of the physician primarily managing the patient’s treatment, their degree of satisfaction with various aspects of daily hGH treatment and their opinions about treatment. Some of these patient and caregiver characteristics were said to be associated with adherence to daily hGH treatment based on previous studies.6–10,14,15,17
For treatment satisfaction, respondents were asked to describe their satisfaction with various items related to treatment on a 5-point Likert scale, with 1 meaning that they are very dissatisfied and 5 meaning that they are very satisfied with the item. For their opinions concerning treatment, respondents were asked to indicate the degree that they agree or disagree with various statements concerning treatment on a 5-point Likert scale, with 1 meaning that they do not agree with the statement at all and 5 meaning that they agree with it a lot.
Health literacy was assessed using the 14-item health literacy scale (HLS-14). This 14-item scale was developed for Japan and has been used on a large-scale basis via cross-sectional mail and online surveys in Japan in the past.23–25 The HLS-14 consists of 14 items that assess three dimensions of health literacy: functional, communicative, and critical health literacy.26 Functional health literacy refers to the ability to understand and use health information to make informed decisions about health care. Communicative health literacy refers to the ability to communicate effectively with HCPs. Critical health literacy refers to the ability to evaluate health information critically and make informed decisions about health care. The items on the HLS-14 are rated on a 5-point scale, ranging from 1 (not at all) to 5 (very much). The total score on the HLS-14 ranges from 14 to 70, with higher scores indicating higher health literacy.
Adherence to daily hGH treatment was assessed using the 8-item Morisky Medication Adherence Scale (MMAS-8). The MMAS-8 instrument is a structured self-reported measure of medication-taking behavior that has been widely used in various countries for a number of different conditions.27–38 The highest attainable score on the MMAS-8 is eight points and a higher score indicates a higher degree of treatment adherence. A Japanese version of the MMAS-8 is available from the license holder. It has been used outside Japan among GHD and SGA patients and has been used in Japan among non-GHD patients / caregivers.15,27–38
Statistical Analyses
Quantitative data collected were analyzed by INTAGE Healthcare using Microsoft Excel (2016) and statistical analysis was conducted using R statistical software. A descriptive analysis of the data was performed using summary statistics for categorical and continuous data. For categorical data, frequencies and proportions are provided. Missing data was not an issue for this study because the online survey method involved rigorous review and testing of the survey program internally by INTAGE Healthcare and respondents could not continue to the next question without providing a response to each question sequentially presented to them.
For treatment satisfaction items and opinions concerning treatment, the top 2 responses (satisfied / very satisfied and agree / agree a lot) were calculated and frequencies and proportions for the top 2 responses are reported. Moreover, for health literacy mean scores and the standard deviation were calculated for the overall HLS-14 responses and for each sub-domain (functional, communicative, and critical health literacy). Moderate to good treatment adherence among caregivers was defined as a score of 6 to 8 on the MMAS-8 scale. Conversely, those with a score of less than 6 were defined as having poor adherence. This categorization has been used to describe poor, moderate, and good adherence in previous studies that utilized the MMAS-8 instrument.27–32
Chi-square testing was used to assess the significance of the difference between those with poor adherence and those with moderate to good adherence for patient and caregiver characteristics, treatment characteristics, satisfaction with treatment, and opinions concerning treatment. A Student’s t–test was used to consider the significance of the difference between those with moderate to good adherence and those with poor adherence in terms of their health literacy. A p-value of 0.05 or lower was considered to be statistically significant.
Exploratory Factor Analysis and K-Means Clustering Analysis
An exploratory factor analysis (EFA) for satisfaction with treatment-related items and opinions concerning treatment was conducted in order to identify factors that best describe each of those areas. Factor analysis, including EFA, has been used in studies to examine factors that are associated with medication adherence and to consider factors for inclusion in scales that measure adherence.39–42 An EFA can be used to reduce data to a smaller set of summary variables.43 While numerous items related to treatment satisfaction and opinions about treatment were included in the survey questions, not all items may describe overall satisfaction and agreement as clearly. EFA was therefore used to refine the variables to those with the most explanatory value.
Specifically, the EFA was conducted using the following steps. First, the minimum residuals method was used to minimize the residuals of the model. Next, promax rotation was performed. The number of factors was set to three. This was done based on the Kaiser criterion, which states that factors with eigenvalues greater than 1 should be retained. For each factor, items with loadings of 0.5 or more were included. This was done to ensure that the items were loading on the factors in a meaningful way. Items with loadings of less than 0.5 for all factors were deleted in order to remove items that were not loading on any of the factors.
Graham et al and Orso et al reviewed studies related to adherence to daily hGH treatment and Gomez et al proposed a conceptual framework related to barriers to adherence.17,21,22 In addition to patient and caregiver characteristics such as age and education, factors such as satisfaction with treatment, communication with HCPs, and satisfaction with the device were also said to be important aspects. The variables used for the EFA for the present study were selected based on those studies with items related on treatment satisfaction, satisfaction related to communication, devices and medication included as variables.
After conducting an EFA of satisfaction with treatment-related items and opinions concerning treatment, a K-means clustering analysis was conducted for each area. The factor scores obtained from each EFA were used as the variables for the respective K-means clustering analysis. K-means clustering analysis is a type of non-hierarchical clustering that generates clusters by computing the Euclidean distance with K = 4.44 This analysis can be used to group similar data points together and discover underlying patterns. The relationship between adherence and each of satisfaction with treatment-related items and opinions concerning treatment is considered, based on the findings.
Ethical Consideration
This study was conducted in accordance with the Declaration of Helsinki and is consistent with Good Pharmacoepidemiology Practices and the applicable laws and regulations of Japan. This study also adhered to the European Pharmaceutical Market Research Association (EphMRA) Code of Conduct.45 Ethical approval for this study was obtained from the central ethical review committee maintained by the Saga Memorial Hospital based in Saga, Japan on November 2, 2021, prior to starting data collection. Informed consent to participate in the study was obtained from all respondents prior to start of the survey.
Results
Caregiver, Patient, and Treatment Characteristics
Table 1 shows the characteristics of the survey participants by level of treatment adherence based on the MMAS-8 instrument where moderate to good treatment adherence is defined as a score 6 to 8 and poor adherence is defined as a score of less than 6. The survey was completed by 112 caregivers of patients being treated for pGHD or for being SGA that had been treated with growth hormones for 3 months or more. About two-thirds (67.9%) of caregivers reported having moderate to good adherence and about one-third (32.1%) reported poor adherence to rGH treatment based the MMAS-8 instrument. Over half of caregivers (54.5%) were female and most (85.8%) were aged 30 to 49 years old. About 1 out of 5 caregivers (19.6%) indicated that they had only one child under the age of 18 living at home, while most (75.0%) had 2 or more under the age of 18 living at home. About two-thirds (69.6%) reported that the primary caregiver - ie, the primary administrator of rGH treatment for the patient - is female. Most (76.8%) said that the primary caregiver for the patient worked full-time or part-time and most (80.4%) said that the primary caregiver for the patient has at least some post-secondary education. In fact, more than half (55.4%) of the primary caregivers for the patients had at least a 4-year college education. Most caregivers (71.4%) had an annual household income of 5 million JPY or higher and more than one-third (38.4%) had an annual household income of 10 million JPY or higher.
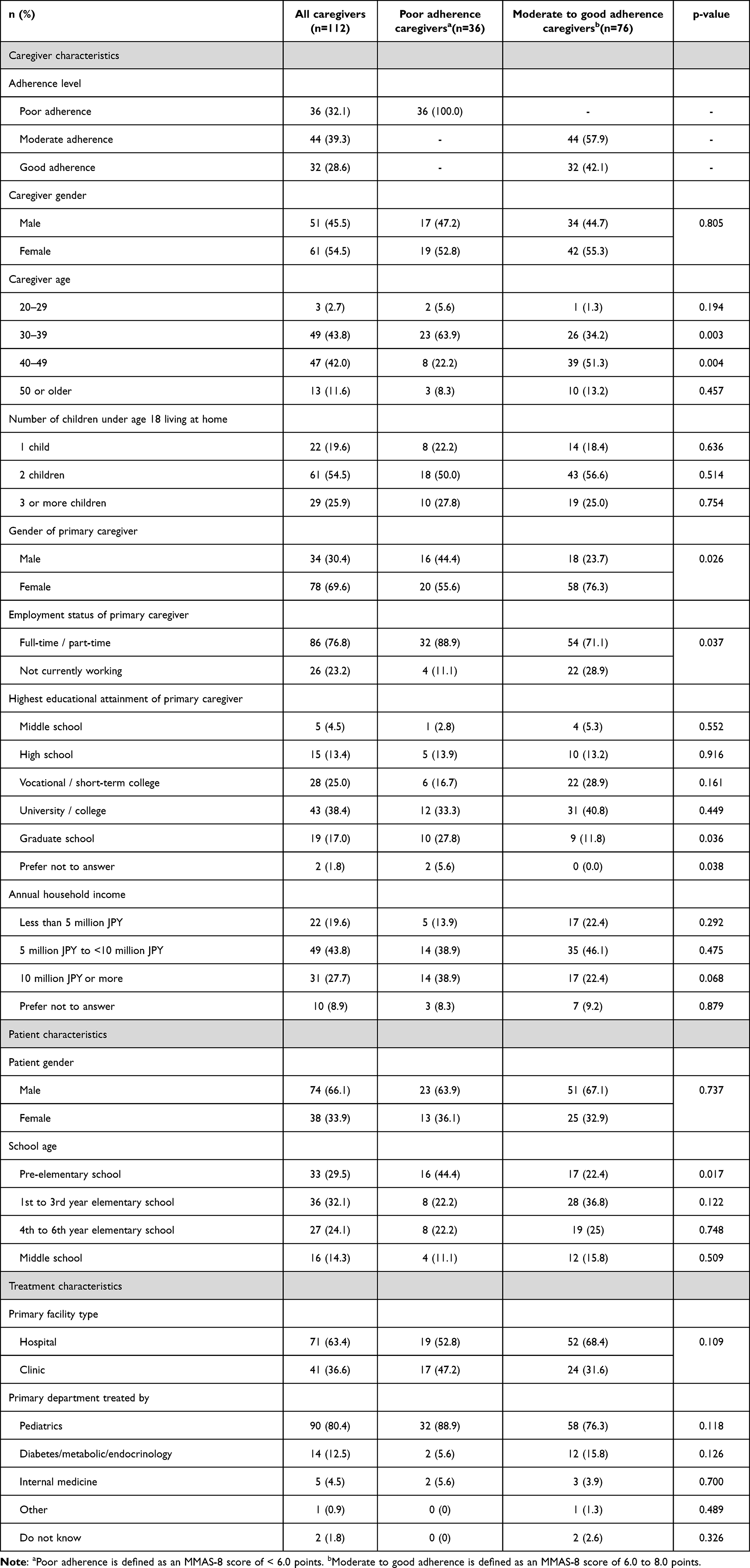 |
Table 1 Treatment Adherence and Caregiver, Patient, and Treatment Characteristics |
In terms of patient characteristics, about two-thirds (66.1%) of the GHD patients cared for were male and more than half (56.2%) were in their 1st to 6th year of elementary school (as opposed to pre-elementary school or middle school). Nearly one-third of GHD patients (29.5%) were pre-elementary school-age patients. In terms of treatment characteristics, about two-thirds of caregivers (63.4%) reported that their child was primarily being treated at a hospital and 80.4% were primarily being treated by a pediatrician.
Health Literacy
Table 2 shows the overall score for health literacy based on the HLS-14 instrument. The average overall healthcare literacy score was 50.1 points with a standard deviation of ±7.3 based on a maximum possible score of 70 points. The average score for functional health literacy was 17.6 points with a standard deviation of ±5.0 based on a maximum possible score of 25 points. The average score for communicative health literacy was 18.8 points with a standard deviation of ±3.5 based on a maximum possible score of 25 points. Lastly, the average score for critical health literacy was 13.7 points with a standard deviation of ±2.8 based on a maximum possible score of 20 points.
 |
Table 2 Treatment Adherence and Health Literacy Among Caregivers Based on HLS-14 |
Satisfaction with Treatment
Table 3 shows the percent of caregivers that selected 4 or 5 on a 5-point Likert scale concerning their satisfaction with different aspects of treatment, with 4 meaning they are “Satisfied” and 5 meaning they are ‘Very satisfied’ with the item. Again, items related to satisfaction with treatment that were included in the present study were selected based on their inclusion in the aforementioned literature reviews which considered factors that may be related to treatment adherence. Caregivers generally reported a high degree of satisfaction with items related to treatment. Satisfaction was highest, on average, for the treatment options available to them (76.8%), communication with physicians (76.8%), their drug treatment used (75.0%), and their device used (74.1%) based on a response of 4 or 5 on a 5-point Likert scale. On the other hand, satisfaction was lowest, on average, for physical and mental burden of the caregiver related to treatment (49.1%), physical and mental burden of the patient related to treatment (53.6%), and treatment safety (60.7%) based on a response of 4 or 5 on a 5-point Likert scale.
 |
Table 3 Treatment Adherence and Satisfaction Concerning Treatment |
Opinions Concerning Treatment
Table 4 shows the percent of caregivers that selected 4 or 5 on a 5-point Likert scale concerning their agreement with statements related to treatment, with 4 meaning they “Agree” with the statement and 5 meaning they “Agree with it a lot”. Again, items related to opinions about treatment that were included in the present study were selected based on their inclusion in the aforementioned literature reviews which considered factors that may be related to treatment adherence. Agreement with statements concerning treatment varied. Agreement was highest, on average, for the notion that caregivers should decide in advance when to give growth hormone injections and adhere to it (59.8%), that caregivers should get informed about the disease/therapy as needed (58.9%), that physicians should take the initiative in providing information about the disease and its treatment (58.9%), that physicians, pharmacists, or nurses should ask caregivers about any problems with the drug/device (injector) used (57.1%), and that caregivers should report non-adherence (missed or unintentional injections) during consultations (55.4%) based on a response of 4 or 5 on a 5-point Likert scale. On the other hand, agreement was lowest, on average, for the notion that intentionally skipping an injection once or twice a month is not a problem (19.6%), that drugs/devices (injectors) should be selected by the caregiver (23.2%), and that missing an injection once or twice a month is not a problem (39.3%) based on a response of 4 or 5 on a 5-point Likert scale.
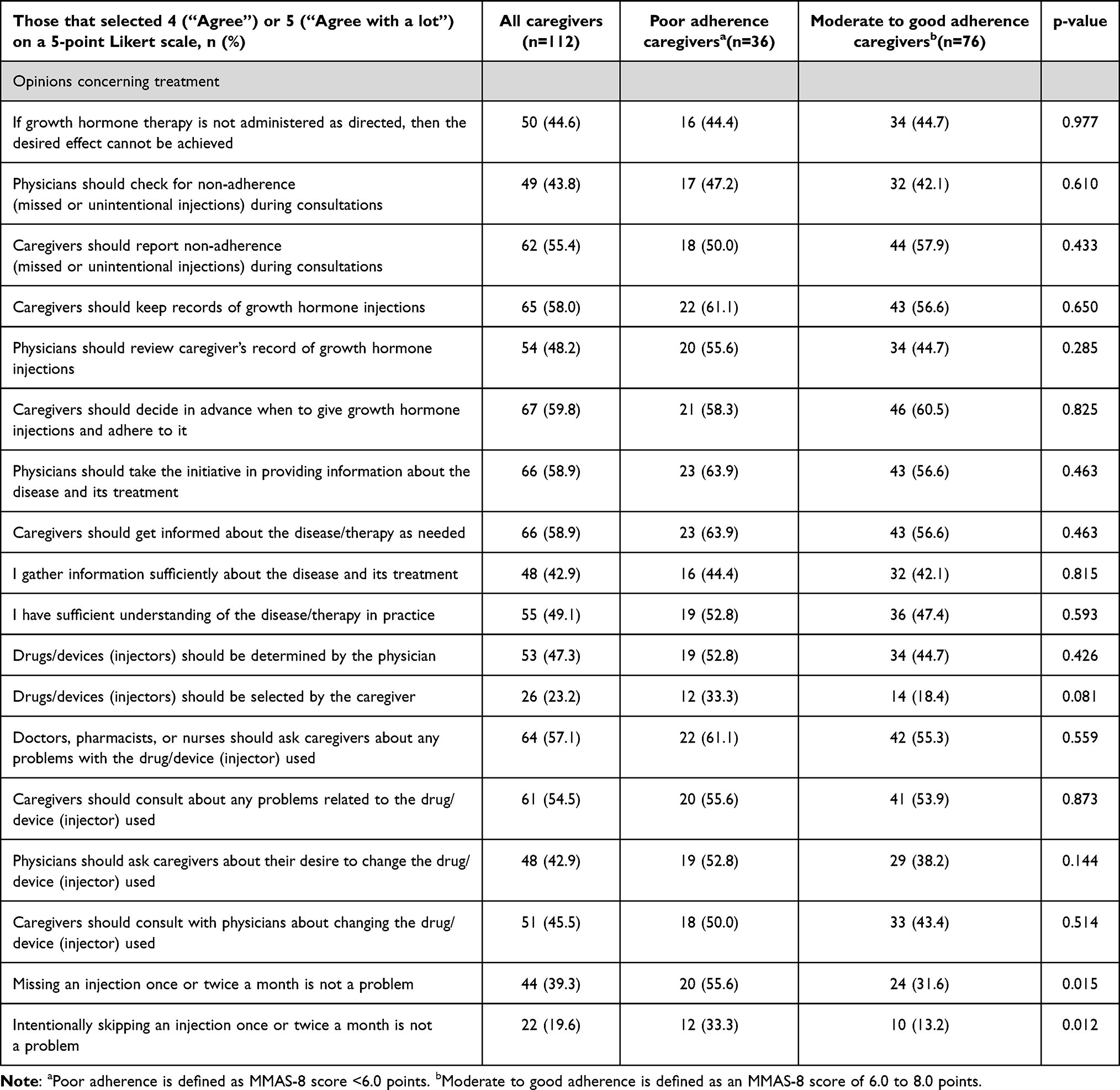 |
Table 4 Treatment Adherence and Opinions Concerning Treatment |
Characteristics of Those with Poor Treatment Adherence
Table 1 also shows the characteristics of caregivers and patients and treatment characteristics for those with poor adherence (n=36, 32.1%) and those with moderate to good adherence (n=76, 67.9%) to daily rGH treatment. Adherence to daily rGH treatment was associated with some caregiver age ranges (30–39 and 40–49 years old), the gender of the primary caregiver, and the employment status of the primary caregiver based on a univariate analysis. Among those with moderate to good adherence, about one-third (34.2%) were aged 30–39 years old, compared to nearly two-thirds (63.9%) of those with poor adherence – suggesting that caregivers with poor adherence are more commonly aged 30–39 years old.
Among caregivers with moderate to good adherence, 76.3% reported that primary caregiver is female, compared to 55.6% of those with poor adherence - suggesting that the primary caregiver being female may be associated with better adherence. Similarly, among caregivers with moderate to good adherence, 28.9% reported that the primary caregiver is not currently working, compared to 11.1% of those with poor adherence - suggesting that not currently working may be associated with better adherence. These differences were both statistically significant. Among caregivers with moderate to good adherence, about 22.4% cared for GHD patients that were pre-elementary school age, compared to 44.4% of those with poor adherence - suggesting that caring for pre-elementary school age children is associated with better adherence. That difference was also statistically significant.
While overall health literacy based on the HLS-14 instrument was not shown to be associated with adherence to daily rGH treatment, responses to the functional health literacy domain questions were shown to be associated with treatment adherence (Table 2). The functional health literacy domain includes questions on the ability to understand and use health information to make informed decisions about health. Specifically, it includes questions such as whether or not they feel confident with reading the Japanese characters in the literature / pamphlets provided by the hospital and/or pharmacy, whether or not they have found that material difficult to read, whether or not it takes them a good deal of time to read that material, or if they have had to have someone read it for them. Among the caregivers interviewed, those with moderate to good adherence reported 18.6 points on average, for the functional health literacy domain compared to only 15.6 points, on average, for those with poor adherence - suggesting that those with better functional literacy have better adherence.
Relationship Between Treatment Satisfaction and Adherence
Among the items considered for treatment satisfaction, none of items included were shown to be associated with adherence based on a univariate analysis. Among those with moderate to good adherence, 81.7% and 78.9% indicated that they are satisfied with the drug treatment used, respectively, compared to only 66.7% for those with poor adherence - suggesting that satisfaction with drug treatment may be associated with better adherence. However, the differences were not statistically significant and therefore, as a whole, these findings suggest that, aside from satisfaction with the drug treatment used, satisfaction with treatment may be a poor predictor of treatment adherence.
To further examine the relationship between satisfaction with treatment and adherence to daily rGH treatment, an EFA of treatment satisfaction items thought to be related to adherence was conducted. The results of that analysis are shown in Table 5. That analysis revealed three categories of factors that best describe overall satisfaction based on the items included: 1) satisfaction with the drug / device used, 2) satisfaction with the degree of physical and mental burden related to treatment, and 3) satisfaction with communication with HCPs. Other items such as satisfaction with treatment efficacy and satisfaction with treatment safety, failed to yield factor loadings above the minimum threshold of 0.5 for any of the factors.
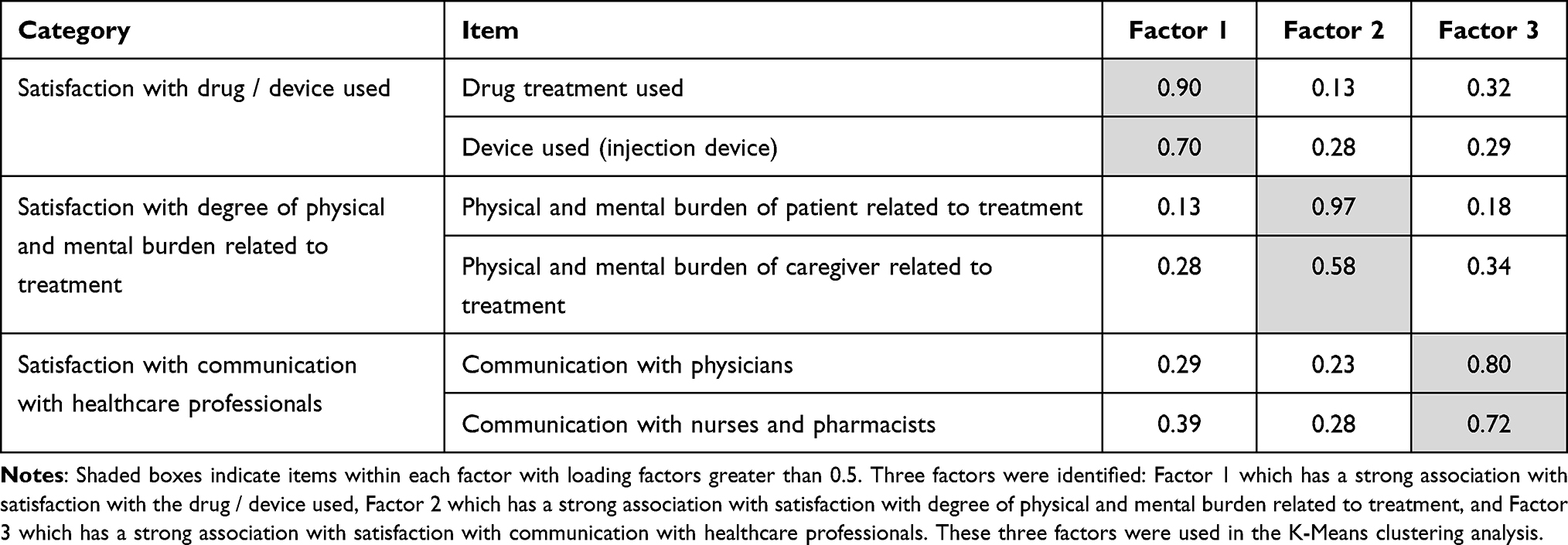 |
Table 5 Exploratory Factor Analysis: Treatment Satisfaction |
The three factors identified were then used as inputs for a K-mean clustering analysis. The results of that analysis are shown in Table 6. Four distinct clusters were identified. Names were assigned to each cluster identified to help understand their tendencies. Cluster 2 (“Satisfied”) had the highest level of adherence with 87.5% of caregivers included in that cluster reporting moderate to good adherence. Caregivers in Cluster 2 (“Satisfied”) showed a higher degree satisfaction with the drug / device used, the physical and mental burden of treatment, and communication with HCPs. Caregivers in Cluster 1 (“Burdened”) had the next highest level of treatment adherence with nearly three-fourths of caregivers (70.4%) in that cluster reporting moderate to good adherence. Caregivers in Cluster 1 (“Burdened”) reported a low degree of satisfaction with the physical and mental burden of treatment, but a moderate satisfaction with the drug/device used and communication with HCPs.
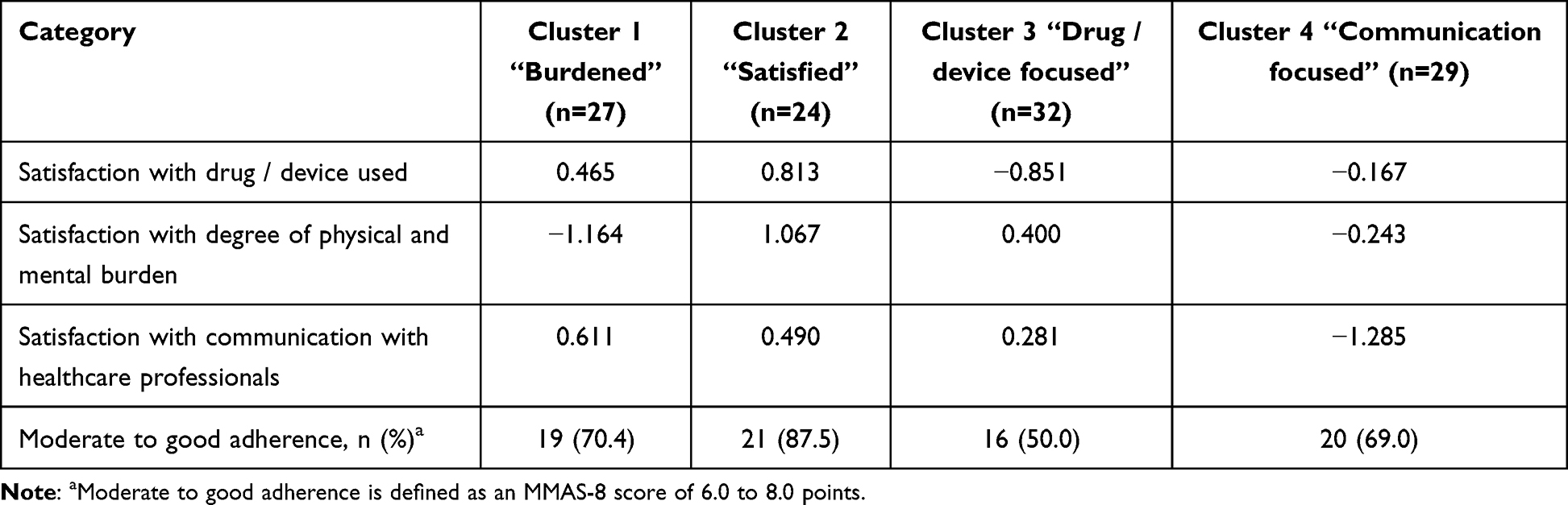 |
Table 6 K-Means Cluster Analysis: Treatment Satisfaction |
Cluster 4 (“Communication focused”) had the next highest level of adherence with 69.0% reporting a moderate to good adherence. Caregivers in Cluster 4 (“Communication focused”) had a low degree of satisfaction with their communication with HCPs. This suggests that communication with HCPs may be important to maintaining and improving adherence. Lastly, caregivers in Cluster 3 (“Drug / device focused”) had the lowest level of adherence with only 50.0% of caregivers in that cluster reporting moderate to poor adherence. Cluster 3 (“Drug / device focused”) reported the lowest degree of satisfaction with the drug / device used. Overall, these findings suggest that satisfaction with the drug / device used may indeed be an important driver for adherence - and to some degree satisfaction with communication with HCPs and satisfaction with degree of physical and mental burden as well.
Relationship Between Opinions Concerning Treatment and Adherence
Among the items considered for opinions concerning treatment, only agreement with the notion that intentionally skipping an injection once or twice a month is not a problem was associated with adherence based on a univariate analysis. Among those with moderate to good adherence, 13.2% indicated that intentionally skipping an injection once or twice a month is not a problem, compared to 33.3% for those with poor adherence. Overall, these findings suggest that, aside from holding more easy-going views on the idea of skipping treatment, opinions about treatment may be a poor predictor of treatment adherence.
To further examine the relationship between opinions about treatment and adherence to daily rGH treatment, an EFA of opinions about treatment thought to be related to adherence was conducted. The results of that analysis are shown in Table 7. That analysis revealed three categories of factors that best summarize opinions concerning treatment: 1) the importance of treatment management, 2) the importance of consultation concerning the drug / device used, and 3) the importance of treatment info gathering and understanding. Other items, such as agreement with the notion that not administering growth hormone therapy as directed can lead to not achieving the desired effect, failed to yield factor loadings above the minimum threshold of 0.5.
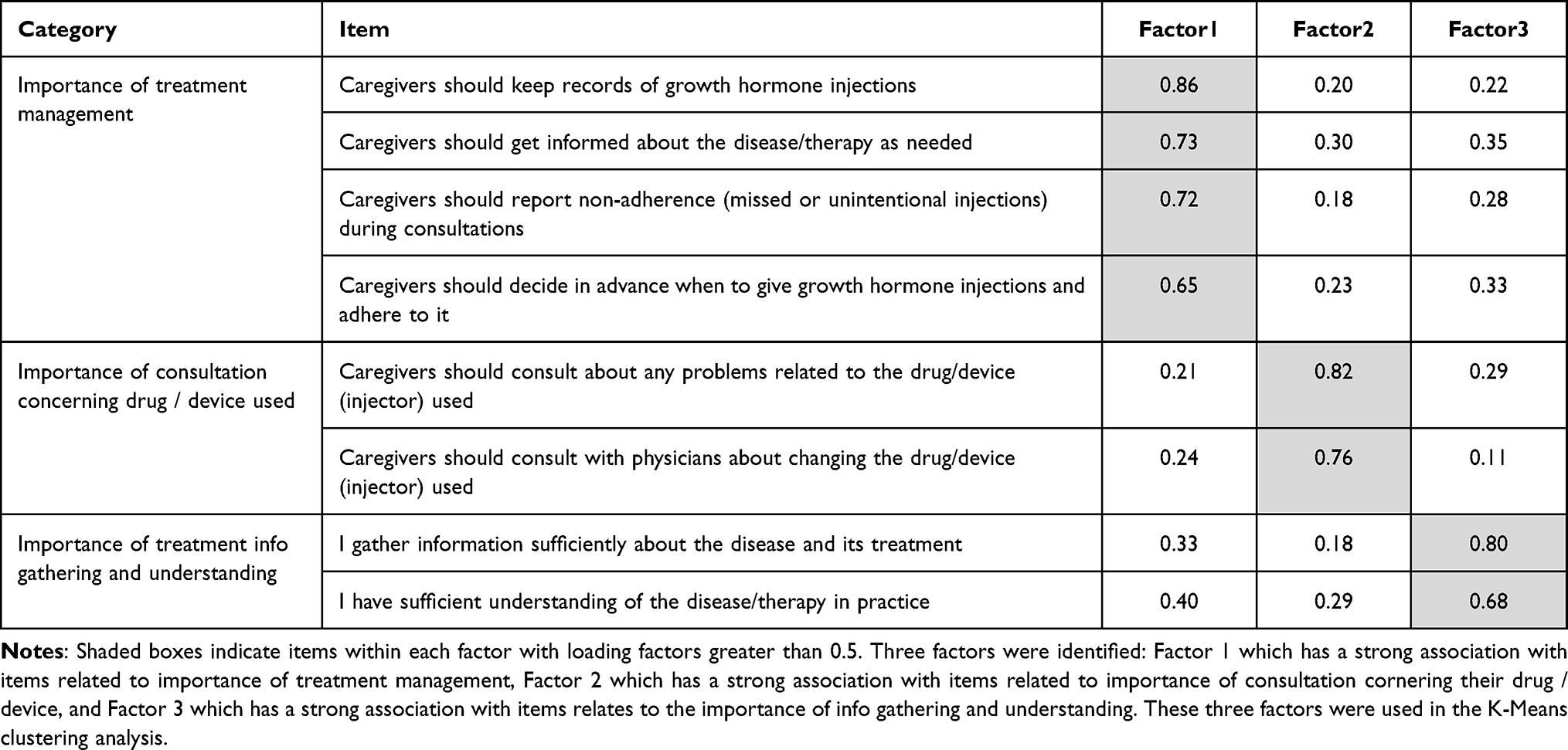 |
Table 7 Exploratory Factor Analysis: Opinions Related to Treatment |
The three factors identified were then used as inputs for a K-mean clustering analysis. The results of that analysis are shown in Table 8. Four distinct clusters were identified. Again, names were assigned to each cluster identified to help understand their tendencies. Caregivers in Cluster 4 (“Uninvolved”) had the highest level of adherence with 73.3% of caregivers in that cluster reporting moderate to good adherence. Caregivers in Cluster 4 (“Uninvolved”) showed a low degree of agreement with all three factor categories, especially the importance of consultation concerning drug / device used. Next, caregivers in Cluster 2 (“Managed”) had the next highest level of adherence with 71.9% caregivers in that cluster reporting moderate to good adherence. Caregivers in Cluster 2 (“Managed”) showed a high degree of agreement with the importance of treatment management, and a moderate degree of disagreement with the importance of consultation concerning the drug / device used.
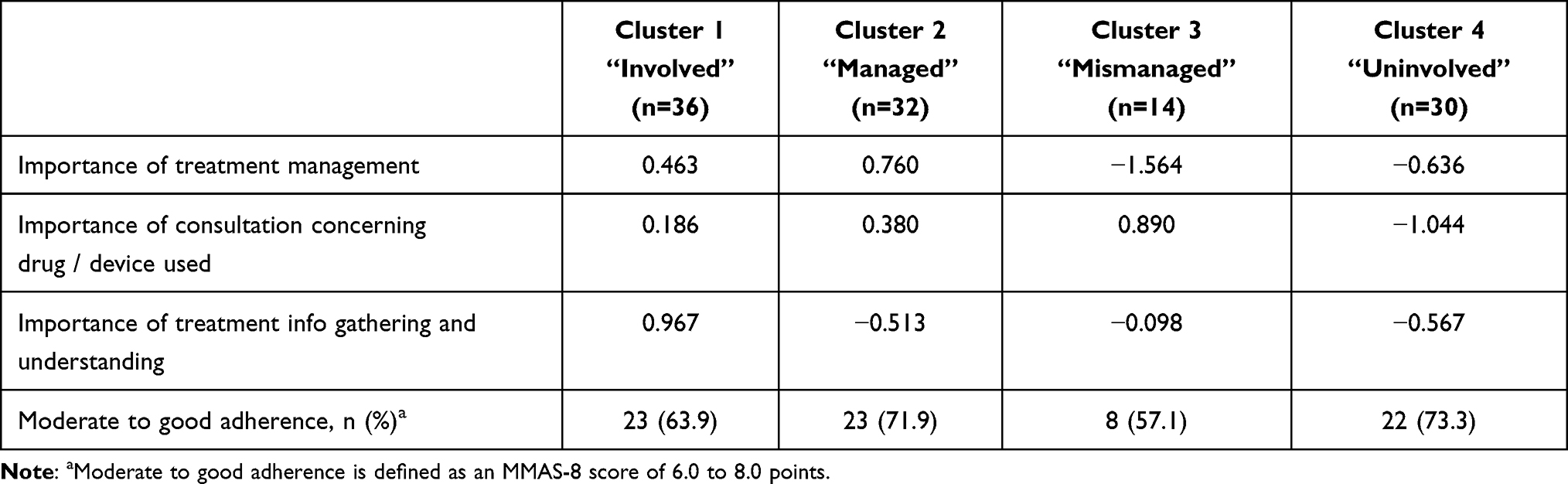 |
Table 8 K-Means Cluster Analysis: Opinions Related to Treatment |
Caregivers in Cluster 1 (“Involved”) had the next highest level of adherence with around two-thirds of caregivers in that cluster (63.9%) reporting moderate to good adherence. Caregiver in Cluster 1 (“Involved”) had a moderate to high degree of agreement with the importance of all three factor categories, especially the importance of treatment info gathering and understanding. Lastly, caregivers in Cluster 3 (“Mismanaged”) had the lowest degree of adherence with only 57.1% of caregivers included in that cluster reporting moderate to good adherence. Caregivers in Cluster 3 (“Mismanaged”) showed a low degree of agreement with the importance of treatment management, and a high degree of agreement with the importance of consultation regarding the drug / device used. This suggests that agreement with the importance of proactively managing treatment such as keeping records of growth hormone injections, getting informed about the disease/therapy as needed, reporting non-adherence (missed or unintentional injections) during consultations, and deciding in advance when to give growth hormone injections and adhering to it; may be important for achieving adherence, and perhaps more importantly, that the lack of emphasis on the importance of such treatment management may lead to poor adherence.
Discussion
Findings from this study suggest that adherence to daily rhGH treatment among caregivers of pGHD patients in Japan is associated with a mix of caregiver and patient characteristics as well as certain aspects related to treatment satisfaction and opinions concerning treatment. First, in terms of the characteristics of caregivers and the patients that they care for, the caregiver’s age, gender, employment status, and functional literacy are important factors. Caregivers with poor adherence are more commonly aged 30–39 compared those with good adherence. Moreover, among those with moderate to good adherence, the primary caregivers are more commonly female and not currently employed. Caregivers with moderate to good adherence tended to have a higher functional health literacy compared to those with poor adherence. The age of the patient is also important. The patients of caregivers with poor adherence were more commonly pre-elementary school age children compared to those with moderate to good adherence. These differences were all statistically significant.
Next, this study has shown that among items related to treatment satisfaction, low satisfaction with drug / device used, and to some extent low satisfaction with communication with HCPs, are associated with poorer adherence. Moreover, among items related to opinions concerning treatment, agreement with the notion that intentionally skipping an injection once or twice a month is not a problem, is associated with poorer adherence based on a univariate analysis. These relationships were, to a large extent, confirmed based on the EFA and K-means cluster analyses.
These findings are to our knowledge, the first to assess how caregiver, patient, and treatment characteristics can influence adherence to daily rhGH treatment among caregivers of pGHD patients in Japan, using statistical analysis. While previous studies for Japan have considered the level of adherence to treatment among caregivers and their preferences concerning treatment, none have examined how caregiver, patient and treatment characteristics are associated with treatment adherence using statistical analysis.5,7,18
Although no previous studies were identified that considered the age of the caregiver, some previous studies have examined barriers to adherence based on the age of the patient.34,46–48 Similar to the present study, a study by Maggio et al 2018 found lower adherence among younger pediatric patients aged 9 or younger in Italy, compared those that aged 10–13 years old. Other studies, however, have shown an inverse association between the age of the patient and treatment adherence with adherence declining over time.48 The association between patient age and treatment adherence may, therefore, be complex with poor adherence in younger and older patient groups and better adherence among those in the middle age groups.
The gender and employment status of the caregiver has also not typically been examined in previous studies that considered barriers to treatment adherence among caregivers of pGHD patients. However, some studies have suggested that a busier injection schedule (eg, 7 injections per week instead of 6 injections or a single injection) may be associated with poor adherence.18,34,49 The combination of a busy injection schedule and a busy lifestyle due to employment may affect adherence. Specifically, to the extent that being employed full-time or part-time can lead to a busier lifestyle, making an injection schedule more difficult to manage, caregivers that are employed may have a more difficult time achieving moderate / good treatment adherence. While the impact of once-weekly injections on treatment adherence among caregivers in Japan is still unclear, caregivers have reported a strong preference for fewer treatment injections.5 Based on this, less frequent treatment injections, such as the recently introduced once-weekly rhGH injection product, may improve adherence for employed persons.47
While no similar studies were found that examined the relationship between health literacy and treatment adherence for pGHD, several previous studies have suggested that lack of treatment understanding is associated with poorer adherence for pGHD treatment.46,50,51 For example, in their survey that included the parents of children with pGHD, Rosenfeld et al 2008 found that misperception about the consequences of missing doses is associated with poorer adherence.50 Moreover, in their survey of patients and caregivers involved in the administration of rhGH treatment for pGHD, Bagnasco et al 2017, showed that adherent patients were more likely to have a parent that had completed a high level of education, and that lack of family education / awareness is related to poorer adherence.51 Other studies have reported cases of low adherence due to poor initial injection instruction and training, but improved adherence as a result of adequate and appropriate instruction during subsequent visits to the clinic.52 While there was no statistical difference in treatment adherence based on educational attainment observed for the present study, functional health literacy is clearly an important factor associated with treatment adherence in Japan.
Some previous studies have also suggested that satisfaction with the drug and device used is related to treatment adherence.50,51 Satisfaction with the drug and device can in turn be driven by the frequency of injections required, the pain associated with injections, the perceived safety of the product, etc.18,50 Japanese caregivers that administer daily rhGH treatment have described a preference for fewer injections and easier dosing time / set up.5 Caregivers have also expressed some concern about the safety of pGHD treatment.18,53,54 Studies have found that 67% of caregivers report concern about the side effects associated with treatment and that concern has been linked to refusal to adhere.53,54 Continual efforts to improve satisfaction with drug and device used are likely to help improve adherence. Moreover, more dialogue between physicians and parents about the safety of treatment may be needed.
Lastly, while no previous study was found that examined the opinions of caregivers concerning treatment and treatment adherence, the present study found that lack of agreement with the importance of treatment management - eg, keeping records of growth hormone injections, getting informed about the disease/therapy as needed, reporting non-adherence (missed or unintentional injections) during consultations, and deciding in advance when to give growth hormone injections and adhering to it - is associated with poorer treatment adherence for caregivers of pGHD patients. While not explicitly related to concern about treatment management, several previous studies have suggested that forgetfulness is associated with poorer adherence.15,18,49 To the extent that forgetfulness concerning treatment administration is associated with lack of agreement with the importance of treatment management, the findings may be related.
Based on the findings from this study, interventions that specifically target those aged 30–39, caregivers that are male, caregivers that are working, and caregivers that are caring for pre-elementary school age children may lead to an overall improvement in treatment. Instructions and communications concerning the administration of rhGH treatment could be designed specifically for those groups. Moreover, interventions geared towards those with lower functional literacy such as visual aids, treatment-management support programs and more incorporation of digital technologies may lead to an improvement in treatment.55,56 Specific drug and device use by caregivers, their level of communication with HCPs and the importance they place on treatment management are clearly important.
It has also been reported that there is a gap in the perceived level of adherence between caregivers of pGHD and physicians.18 While many factors influence treatment adherence and clinical outcomes, the importance of shared decision making (SDM) in shaping these decisions is becoming increasingly clear.57 SDM is an approach where clinicians and patients share the best available evidence when faced with the task of making decisions, and where patients are supported to consider their options to achieve informed preferences. We believe that this concept also could be an intervention tool to optimize adherence. While physicians in Japan tend to see a lot of patients per day, more active communication with caregivers about the importance of treatment management and sharing information about the best treatment option available may lead to an improvement in adherence. For example, the availability of a newly medical treatment option may improve satisfaction with drug treatment and improve treatment management.
Study Limitations
While this study offers as unprecedented review of the factors related to treatment adherence among caregivers of pGHD patients in Japan, it has a number of limitations. Several limitations inherent to the survey method are highlighted in the initial analysis presented.18 However, there are some limitations that are unique to the study analysis. First, while the number of caregivers included is thought to be sufficient to gauge overall adherence, healthcare literacy, treatment satisfaction, etc., findings from the EFA and K-means cluster analyses may be limited due to small sample sizes for the subgroups. A larger study population may have revealed more or stronger associations for adherence. Moreover, this survey was conducted prior to the recent introduction of a once weekly rhGH treatment option in Japan.
Conclusion
Strategies to improve treatment adherence among caregivers of pGHD patients in Japan could target specific groups of caregivers and patients such as caregivers aged 30–39, male caregivers, employed caregivers, and those caring for pre-elementary school age patients. Moreover, efforts to improve the functional health literacy of caregivers and to identify and provide support to those low functional health literacy, may lead to an improvement in treatment adherence. Finally, improvement in satisfaction with the drug and/or device used, communication between patients and HCPs, and education about the importance of proactive treatment management may also lead to an improvement in treatment adherence.
Acknowledgments
We thank Daisuke Shima from Pfizer Japan Inc. for their support with the review of this manuscript and advice concerning the content. The MMAS-8 instrument, content, name, and trademarks are protected by US copyright and trademark laws. Permission for use of the scale and its coding is required. A license agreement is available from Donald E. Morisky, ScD, ScM, MSPH,; [email protected].
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by Pfizer Japan Inc.
Disclosure
MA has received honoraria and manuscript fees from Pfizer, Jansen, GSK, Novartis, Takeda, Shionogi and Astellas. TS and NE are full-time employees of Pfizer Japan Inc. ML and RN are full-time employees of INTAGE Healthcare Inc., which received funding from Pfizer Japan Inc. to conduct the analysis and reporting for this study. The authors report no other conflicts of interest in this work.
References
1. Tanaka T. Growth hormone treatment in Japan: past, present, and future. Pediatr Endocrinol Rev. 2012;10(Suppl 1):89–97.
2. Yokoya S, Tanaka T. The history of growth hormone treatment for GHD in Japan. Pediatr Endocrinol Rev. 2017;14(Suppl 1):201–208. doi:10.17458/per.vol14.2017.yt.historygrowthhormone
3. Ministry of Health, Labor and Welfare. Research on the practical infrastructure for the promotion of measures against chronic specific diseases in children. Policy research project on intractable diseases (policy research project on intractable diseases. study report. ministry of, health, labor and welfare, FY2008-–2010; 2024. Avaiable from: https://www.shouman.jp/research/pdf/23_2830/2830_18.pdf.
4. Lackner L, Jh Q, Witt S. Caregiving burden and special needs of parents in the care of their short-statured children – a qualitative approach. Front Endocrinol. 2023;14:1093983. doi:10.3389/fendo.2023.1093983
5. Tanaka T, Sato T, Yuasa A, et al. Patient preference for growth hormone treatment in Japanese children. Pediatr Int. 2021;63(10):1185–1191. doi:10.1111/ped.14760
6. Graham S, Neo S, Auyeung V, et al. What potentially modifiable factors are associated with treatment nonadherence in pediatric growth hormone deficiency? A quantitative study. Endocr Pract. 2021;27(2):146–151. doi:10.4158/EP-2020-0543
7. Nishinaga H, Kishimoto S, Nishi Y. Survey of growth hormone treatment in clinical practice and patient choice of device. Prog Med. 2015;35:1348–1352.
8. Kapoor R, Burke S, Sparrow S, et al. Monitoring of concordance in growth hormone therapy. Arch Dis Child. 2008;93:147–148. doi:10.1136/adc.2006.114249
9. Cutfield W, Derraik J, Gunn A, et al. Non-compliance with growth hormone treatment in children is common and impairs linear growth. PLoS One. 2011;6:e16223. doi:10.1371/journal.pone.0016223
10. Hartmann K, Ittner J, Müller-Rossberg E, et al. Growth hormone treatment adherence in prepubertal and pubertal children with different growth disorders. Horm Res Paediatr. 2013;80(1):1–5. doi:10.1159/000351800
11. Foo J, Maghnie M, Colao A, et al. Cost-consequence analysis of human recombinant growth hormone (r-hGH) treatment administered via different devices in children with growth hormone deficiency in Italy. Clinicoecon Outcomes Res. 2019;11:525–537. doi:10.2147/CEOR.S195265
12. Horne R. Compliance, adherence, and concordance: implications for asthma treatment. Chest. 2006;130(1):65S–72S. doi:10.1378/chest.130.1_suppl.65S
13. National Institutes for Health and Care Excellence. Medicines Adherence: Involving Patients in Decisions About Prescribed Medicines and Supporting Adherence. London: National Institutes for Health and Care Excellence; 2009.
14. Norgren S. Adherence remains a challenge for patients receiving growth hormone therapy. Pediatr Endocrinol Rev. 2009;6(Suppl 4):545–548.
15. Mohseni S, Heydari Z, Qorbani M, et al. Adherence to growth hormone therapy in children and its potential barriers. J Pediatr Endocrinol Metab. 2018;31(1):13–20. doi:10.1515/jpem-2017-0157
16. Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353(5):487–497. doi:10.1056/NEJMra050100
17. Graham S, Weinman J, Auyeung V. Identifying potentially modifiable factors associated with treatment non-adherence in paediatric growth hormone deficiency: a systematic review. Horm Res Paediatr. 2018;90(4):221–228. doi:10.1159/000493211
18. Manabu A, Daisuke S, Takahiro S, et al. Perception of adherence to daily human growth hormone treatments among pediatric and adolescent patients in japan: a cross-sectional survey of physicians and caregivers. Patient Prefer Adherence. 2022;10(16):3081–3094.
19. Fumio O, Takahashi Y, Tahara S, Ogawa Y, Højby Rasmussen M, Takano K. Similar safety and efficacy in previously treated adults with growth hormone deficiency randomized to once-weekly somapacitan or daily growth hormone. Clin Endocrinol. 2020;93(5):620–628. doi:10.1111/cen.14273
20. Tanaka T, Susumu Y, Hoshino Y, et al. Long-term safety and efficacy of daily recombinant human growth hormone treatment in Japanese short children born small for gestational age: final report from an open and multi-center study. Clin Pediatr Endocrinol. 2018;27(3):145–157. doi:10.1297/cpe.27.145
21. Gomez R, Ahmed SF, Maghnie M, et al. Treatment adherence to injectable treatments in pediatric growth hormone deficiency compared with injectable treatments in other chronic pediatric conditions: a systematic literature Review. Front Endocrinol. 2022;13:795224. doi:10.3389/fendo.2022.795224
22. Orso M, Polistena B, Granato S, et al. Pediatric growth hormone treatment in Italy: a systematic review of epidemiology, quality of life, treatment adherence, and economic impact. PLoS One. 2022;17(2):e0264403. doi:10.1371/journal.pone.0264403
23. Suka M, Yamauchi T, Sugimori H. Relationship between individual characteristics, neighbourhood contexts and help-seeking intentions for mental illness. BMJ Open. 2015;5(8):e008261. doi:10.1136/bmjopen-2015-008261
24. Ishikawa H, Takeuchi T, Yano E. Measuring functional, communicative, and critical health literacy among diabetic patients. Diabetes Care. 2008;31(5):874–879. doi:10.2337/dc07-1932
25. Goto E, Ishikawa H, Okuhara T, Kiuchi T. Relationship of health literacy with utilization of health-care services in a general Japanese population. Preven Med Rep. 2019;14:100811. doi:10.1016/j.pmedr.2019.01.015
26. Suka M, Odajima T, Kasai M, et al. The 14-item health literacy scale for Japanese adults (HLS-14). Environ Health Prev Med. 2013;18(5):407–415. doi:10.1007/s12199-013-0340-z
27. Giavoli C, Profka E, Giancola N, et al. Growth hormone therapy at the time of Covid-19 pandemic: adherence and drug supply issues. Eur J Endocrinol. 2020;183:L13–L15.
28. Tanaka M, Kawakami A, Maeda S, et al. Validity and reliability of the Japanese version of the morisky medication adherence scale-8 in patients with ulcerative colitis. Gastro Nur. 2021;44(1):31–38. doi:10.1097/SGA.0000000000000533
29. Furue M, Takeuchi S, Murota H. Poor adherence to oral and topical medication in 3096 dermatological patients as assessed by the morisky medication adherence scale-8. Br J Dermatol. 2015;172(1):272–275. doi:10.1111/bjd.13377
30. Ichiyama S, Ito M, Funasaka Y. Assessment of medication adherence and treatment satisfaction in Japanese patients with psoriasis of various severities. J Dermatol. 2018;45(6):727–731. doi:10.1111/1346-8138.14225
31. Ikeda N, Kono A. The relationship between health habits, medication adherence, kidney function, and QOL among kidney transplant patients. J Jpn Acad Nurs Sci. 2018;38(1):365–373. doi:10.5630/jans.38.365
32. Miyazaki M, Nakashima A, Nakamura Y, et al. Association between medication adherence and illness perceptions in atrial fibrillation patients treated with direct oral anticoagulants: an observational cross-sectional pilot study. PLoS One. 2018;13(9):e0204814. doi:10.1371/journal.pone.0204814
33. Sultan S, El-Hourani M, Rondeau E, et al. Categorizing factors of adherence to parenteral treatment in growth hormone deficiencies and hemophilia: what should be the targets for future research? Patient Prefer Adherence. 2018;12:2039–2063. doi:10.2147/PPA.S177624
34. Maggio M, Vergara B, Porcelli P, et al. Improvement of treatment adherence with growth hormone by easypod™ device experience of an Italian centre. Ital J Pediatr. 2018;44(1):113–121. doi:10.1186/s13052-018-0548-z
35. Morisky DE, Ang A, Krousel-Wood M, et al. Predictive validity of a medication adherence measure in an outpatient setting. J Clin Hypertens. 2008;10(5):348–354. doi:10.1111/j.1751-7176.2008.07572.x
36. Beriowitz DR, Foy CG, Kazis LE, et al. Impact of intensive bIood pressure therapy on patient- reported outcomes. outcomes results from the SPRINT study (for the SPRINT study research group). N Engl J Med. 2017;377(8):733–744. doi:10.1056/NEJMoa1611179
37. Bress AP, Bellows BK, King J, et al. Cost-effectiveness of intensive versus standard bIood pressure control. N Engl J Med. 2017;377(8):745–755. doi:10.1056/NEJMsa1616035
38. Orimo H, Sato M, Kimur S, et al. Understanding the factors associated with initiation and adherence of osteoporosis medication in Japan: an analysis of patient perceptions. Osteoporos Sarcopenia. 2017;3:174–184. doi:10.1016/j.afos.2017.10.002
39. Levin JB, Aebi ME, Howland M, et al. The relationship between medication attitudes and medication adherence behavior in adults with bipolar disorder. J Nerv Ment Dis. 2020;208(2):87–93. doi:10.1097/NMD.0000000000001083
40. Axelsson M, Cliffordson C, Lunbach B, et al. The function of medication beliefs as mediators between personality traits and adherence behavior in people with asthma. Patient Prefer Adherence. 2013;7:1101–1109. doi:10.2147/PPA.S49725
41. Klinovszky A, Kiss IM, Papp-Zipernovszky O, et al. Associations of different adherences in patients with type 2 diabetes mellitus. Patient Prefer Adherence. 2019;13:395–407. doi:10.2147/PPA.S187080
42. Boateng GO, Neilands TB, Frongillo EA, et al. Best practices for developing and validating scales for health, social, and behavioral research: a primer. Front Public Health. 2018;11(6):149. doi:10.3389/fpubh.2018.00149
43. Columbia University – mailman School of Public Health. Exploratory Factor Analysis. Columbia University; 2023. Available from: https://www.publichealth.columbia.edu/research/population-health-methods/exploratory-factor-analysis.
44. Columbia University – mailman School of Public Health. K-Means Cluster Analysis. Columbia University; 2023. Available from: https://www.publichealth.columbia.edu/research/population-health-methods/k-means-cluster-analysis.
45. Japan marketing research association. ephmra code of conduct (Japanese edition). Japan marketing research association; 2018. Availablre from: https://www.jmra-net.or.jp/LinkClick.aspx?fileticket=L%2F3co0zdIpM%3D&tabid=466.
46. De Pedro S, Murrilo M, Salinas I, et al. Variability in adherence to rhGH treatment: socioeconomic causes and effect on children’s growth. Growth Hormon IGF Res. 2016;26:32–35. doi:10.1016/j.ghir.2015.12.002
47. Arrabal Vela MA, Garcia Gijon CP, Pascual Martin M, et al. Adherence to somatotropin treatment administered with an electronic device. Endocrinol Diabetes Nutr. 2018;65(6):314–318. doi:10.1016/j.endinu.2018.02.003
48. Lass N, Reinehr T. Low treatment adherence in pubertal children treated with thyroxin or growth hormone. Horm Res Paediatr. 2015;84(4):240–247. doi:10.1159/000437305
49. Aydın BK, Aycan Z, Şıklar Z, Berberoğlu M, Öcal G. Çetinkaya S, et al Adherence to growth hormone therapy: results of a multicenter study. Endocr Pract. 2014;20(1):46–51. doi:10.4158/EP13194.OR
50. Rosenfeld RG, Bakker B. Compliance and persistence in pediatric and adult patients receiving growth hormone therapy. Endocr Pract. 2008;14(2):143–154. doi:10.4158/EP.14.2.143
51. Bagnasco F, Di Iorgi N, Roveda A, et al. Prevalence and correlates of adherence in children and adolescents treated with growth hormone: a multicenter Italian study. Endocr Pract. 2017;23(8):929–941. doi:10.4158/EP171786.OR
52. Urakami T. Effectiveness of a smartphone application on medication adherence in children with short stature receiving GH therapy: a multicenter prospective cohort study (GTL-App). Clin Pediatr Endocrinol. 2021;30(2):85–92. doi:10.1297/cpe.30.85
53. Marini MG, Chesi P, Mazzanti L, et al. Stories of experiences of care for growth hormone deficiency: the CRESCERE project. Future Sci OA. 2016;2(1):FSO82. doi:10.4155/fso.15.82
54. Amereller F, Schillbach K, Schopohl J, et al. Adherence, attitudes and beliefs of growth hormone deficient patients – a questionnaire-based cohort study. Exp Clin Endocrinol Diabet. 2019;129(2):112–117. doi:10.1055/a-0956-1919
55. Sudore RL, Schillinger D. Interventions to improve care for patients with limited health literacy. J Clin Outcomes Manag. 2009;16(1):20–29.
56. Graham S, Quirke-McFarlane S, Auyeung V, et al. Interventions designed to improve adherence to growth hormone treatment for pediatric patients and their families: a narrative review. Pharmaceutics. 2022;14(11):2373. doi:10.3390/pharmaceutics14112373
57. Acerini CL, Segal D, Criseno S, et al. Shared decision-making in growth hormone therapy-indications for patient care. Front Endocrinol. 2018;9:1–14. doi:10.3389/fendo.2018.00688
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.