")
Back to Journals » Journal of Asthma and Allergy » Volume 16
Factors Involved in Decision-Making Dilemmas Faced by Parents of Children with Severe Asthma in PICU During the Development of Discharge Care Plans: A Phenomenological Study
Authors Fan G, Yi M , Qiu X, Zhao J
Received 2 September 2023
Accepted for publication 14 December 2023
Published 27 December 2023 Volume 2023:16 Pages 1349—1359
DOI https://doi.org/10.2147/JAA.S438318
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amrita Dosanjh
Guimei Fan,1 Mo Yi,2 Xiangmin Qiu,1 Jinfang Zhao1
1Shandong Provincial Hospital Affiliated to Shandong First Medical University, Jinan, Shandong, People’s Republic of China; 2School of Nursing, Peking University, Beijing, People’s Republic of China
Correspondence: Jinfang Zhao, Shandong Provincial Hospital Affiliated to Shandong First Medical University, #324 Jingwuweiqi Road, Huaiyin District, Jinan City, Shandong Province, 250021, People’s Republic of China, Email [email protected]
Purpose: This study aims to explore the complicated decision-making dilemma and challenges confronted by parents of children suffering from severe asthma within the Pediatric Intensive Care Unit (PICU) when participating in the development of their children’s discharge care plans.
Patients and Methods: Employing a phenomenological methodology, a purposive sampling was performed to engage with 17 parents who participated in in-depth and semi-structured interviews between October 2022 and February 2023. The transcripts of these interviews were transcribed into textual data, which was then subjected to Colaizzi’s seven-step analysis for meticulous coding and comprehensive thematic elucidation.
Results: The comprehensive analysis of the factors involved in the intricate decision-making dilemmas faced by parents of children with severe asthma during the process of crafting discharge care plans in the PICU revealed five themes and eight sub-themes: 1) Complexity of asthma-related information; 2) Insufficient provision of comprehensive decision-making support; 3) Encountering negative emotions and wavering confidence; 4) Navigating realistic constraints impacting both parents and HCPs; 5) Balancing the advantages and disadvantages of various plans.
Conclusion: Parents of children with severe asthma in the PICU encounter intricate and multifaceted decision-making dilemmas while engaging in the formulation of discharge care plans. These complexities significantly dampen their decision-making enthusiasm and introduce potential risks to the children’s prognosis and recovery. In the future, it is imperative to leverage the guidance provided by healthcare professionals (HCPs) in the decision-making process, develop tailored decision support tools specifically designed for the formulation of discharge care plans for children with severe asthma in the PICU.
Keywords: severe asthma, parents, discharge care plan, decision-making dilemma, phenomenological study
Introduction
Asthma is the most prevalent chronic respiratory disease in childhood. It has been reported that there are approximately 150 million children with asthma globally, and the prevalence continues to rise each year.1 It is a variable disease with different phenotypes, implying that children with asthma may experience and manifest a range of symptom severities.2 Severe asthma accounts for about 5% of all pediatric asthma cases, yet despite optimization of inhalation therapy, allergen avoidance, comorbidity treatment, they still contribute significantly to the incidence, mortality, resource utilization, and medical costs associated with asthma.3,4 Against the backdrop of the past COVID-19 pandemic, managing severe asthma has added complexity and resource pressures, potentially limiting lung function assessment, use of inhaled corticosteroids, and clinic time.
Severe asthma is characterized by its incurability, high treatment costs, and prolonged disease and caregiving characteristics.5 As primary caregivers and decision agents for children with asthma, parents are repeatedly exposed to the stress of caring for their children, often experiencing high levels of caregiving burden and psychological pressure.6 The disease-specificity of asthma and the weakness of social support systems place parents facing numerous challenges in caregiving, including inadequate knowledge and caregiving skills, directly diminishing the quality of care and symptom control for their children, while amplifying caregiver mental stress, thereby giving rise to a range of psychological, social, and physical health issues.7,8
Guidelines from the US National Heart, Lung, and Blood Institute (NHLBI) provide multiple recommendations for proper childhood asthma management, aimed at minimizing asthma exacerbations. These guidelines encompass medication therapy, reducing environmental triggers, assessing and monitoring asthma control, and patient education.9 The guidelines also stress the importance of educating parents of children as primary caregivers and core decision-makers on how to effectively collaborate with HCPs for the formulation of appropriate asthma management plans for children. However, research has found that these guideline recommendations are not consistently followed, with fewer than half of families receiving any training related to their child’s asthma recovery plan.10,11 Therefore, gaining a deeper understanding of how decision-making occurs between HCPs and parents during the process of pediatric asthma plan formulation, especially for parents of children experiencing acute attacks and severe asthma, is crucial.
Decision dilemmas refer to situations where individuals are confronted with choices involving varying degrees of risk, potential regret, or challenges to one’s values, and in the face of uncertainty about the outcome of the choice, often lead to decision procrastination.12 Previous research has indicated that, influenced by a multitude of factors, parents experience high levels of decision conflict during the process of making clinical decisions related to their children.13 This leads to instances of post-decision regret and decreased decision implementation enthusiasm after the decision is made, thereby affecting compliance with discharge care plans, introducing a great deal of uncertainty to the prognosis and recovery of children with asthma.14,15 Therefore, the collaborative development of precise individualized discharge care plans by nursing personnel and parents is of paramount importance.
Based on this, the purpose of this study is to employ a phenomenological method to deeply comprehend the decision-making dilemmas and experiences of parents of children with severe asthma in PICU who are involved in the formulation of discharge care plans. It aims to dissect their underlying needs in the decision-making process, providing clinical evidence for the future development of decision support tools related to discharge care plans for parents of children with severe asthma in PICU.
Methods
Study Design and Setting
A qualitative phenomenological research design was chosen for this study to gain insights into the experiences and perceptions of parents with children suffering from asthma in the PICU, particularly as they navigate decision-making dilemmas related to their child’s discharge plan. This study was conducted in accordance with the Declaration of Helsinki and adheres to the Consolidated Criteria for Reporting Qualitative Research (COREQ) criteria for reporting qualitative research.16
Study Participants
This study was conducted from October 2022 to February 2023 in a public general hospital in Shandong Province, China. Purposive sampling was employed to select parents of children with severe asthma as participants for interviews. The inclusion criteria for the participants were as follows: 1) Their children met the diagnostic criteria for bronchial asthma and were admitted to the PICU. 2) the children did not experience severe complications, including respiratory failure, pneumothorax, hypoxemia during hospitalization. 3) The children had a discharge plan within the following 3 days. 4) The parents were the primary caregivers of the children and had no history of mental or psychological disorders. 5) The parents have experience of decision-making of their children’s discharge care plans within 1 month.
Exclusion criteria included: 1) Participants who withdrew from the study for various reasons. 2) Participants with other severe physical illnesses. 3) Participants’ age under 20 years old. Informed consent was obtained from all participants prior to their involvement in the study. Participants were informed as part of the consent process that any information used in publications would be unidentifiable. The sample size was determined based on data saturation, where no new themes emerged from the information provided by participants.
Development of Interview Outlines
Based on the research objectives, preliminary interview outlines were formulated through literature review, group discussions, and expert consultations. Initial interviews were conducted with four parents of children with severe asthma to refine the outlines based on practical interview experiences and participant feedback. The final interview outline consisted of the following topics: 1) What concerns did you have before engaging in decision-making with HCPs? 2) What knowledge or qualities do you think are necessary when jointly formulating discharge care plans with HCPs? 3) How did you feel when discussing discharge care plans with HCPs? Were there any aspects that made you uncomfortable? 4) Do you believe you need decision support during the decision-making process? And what support or assistance do you require? 5) what aspects of collaborative discharge care plan formulation with HCPs need improvement in the future?
Data Collection
Researchers established rapport with parents from the child’s admission by familiarizing them with the ward, engaging in communication, and introducing nursing plans. The researchers also participated in case discussions to understand changes in the child’s condition and dynamic treatment program. Interviews were conducted in a quiet meeting room within the department. Before commencing interviews, the researchers introduced the study’s purpose, content, process, and the necessity of result verification to the participants. Recording was only initiated after obtaining consent, with the assurance that recordings and transcribed data would be used exclusively for the study, maintaining strict confidentiality of participant privacy. Anonymization was achieved through systematic coding. Various interviewing techniques were implemented, including probing, repetition, clarification, summarization, and reflection, to comprehensively elucidate participants’ experiences, and perceptions regarding decision-making dilemmas in the formulation of discharge care plans. Thorough interview notes were meticulously recorded, capturing non-verbal cues such as body language and facial expressions. Each interview session extended for an average duration of 30 to 45 minutes. Subsequent to the interviews, contact information was exchanged to facilitate additional validation of the obtained results.
Data Analysis
Participants were assigned identifiers in the order of their interviews. Audio recordings were transcribed into textual data within 24 hours after each interview. The Colaizzi’s 7-step analysis method was employed for data analysis:17 1) Thoroughly reading all materials. 2) Extracting significant statements. 3) Condensing and abstracting meaningful information. 4) Grouping common themes or characteristics. 5) Writing detailed and comprehensive descriptions. 6) Formulating the essential nature of the phenomenon. 7) Validating the findings with participants. Two researchers meticulously analyzed and coded the audio recordings and textual data. Common themes were categorized into main and subthemes, cross-referenced against original data. In cases of divergent theme extraction, the research team engaged in internal discussion and deliberation to finalize the themes, ensuring accuracy, scientific rigor, and reliability.
Results
General Information of Study Participants
A total of 17 parents of patients were ultimately selected for interviews in this study, including 5 fathers and 12 mothers. The average age of the participants was (30 ± 2.87) years. The participants primarily had educational backgrounds of college associate degree or higher (55.56%). The majority of participants reported the yearly actual household income between 80,001~100,000 RMB yuan. Further details regarding the general information of the study participants are provided in Table 1.
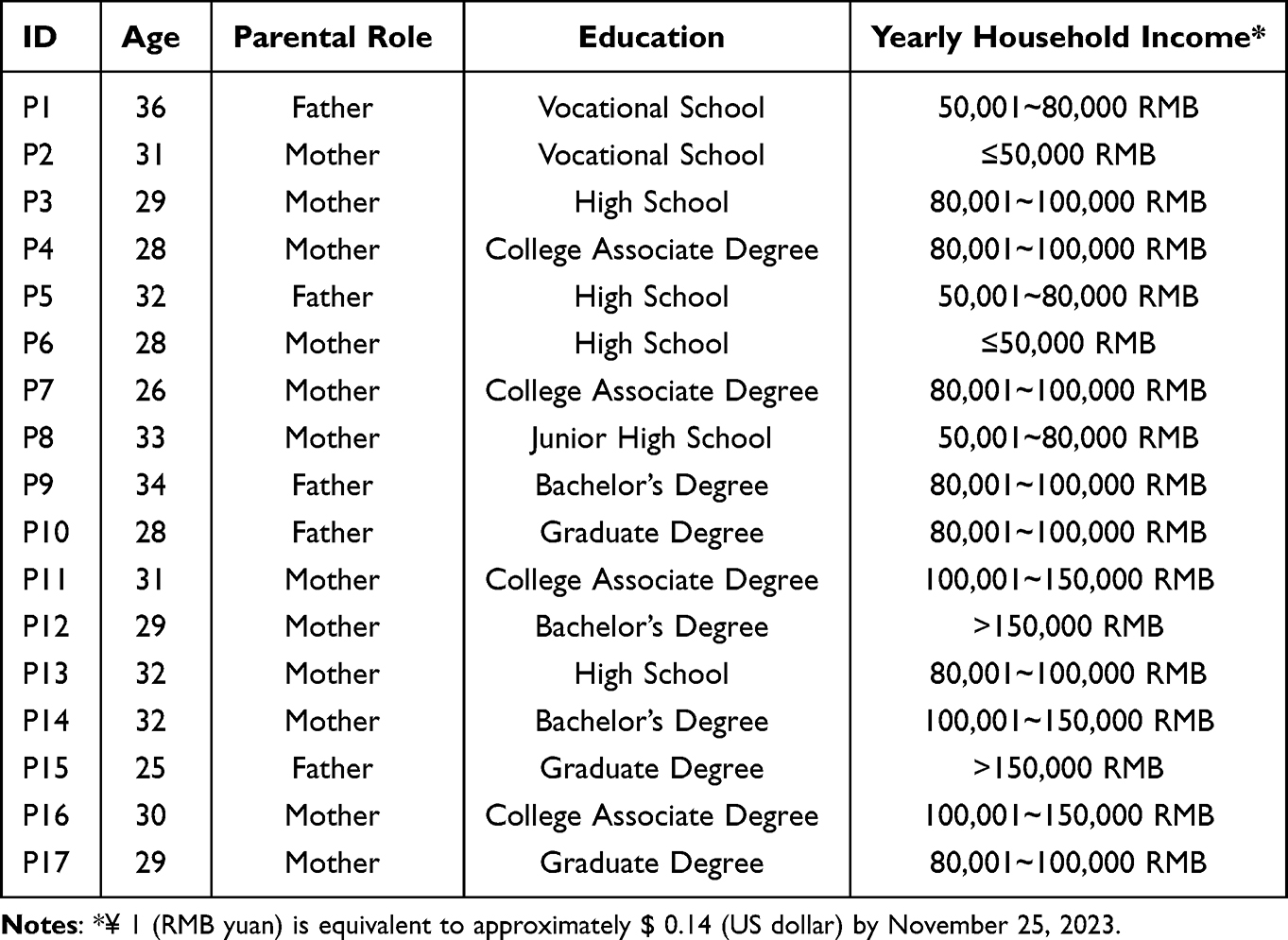 |
Table 1 The Demographics Information of the Participants (n = 17) |
Theme 1: Complexity of Asthma-Related Information
Difficulty in Effectively Discerning Information
In the age of information explosion, diverse sources provide information about asthma, with the internet being a primary resource for parents of children with severe asthma. However, due to the proliferation of asthma-related content on online platforms, most participants faced challenges in accurately evaluating the reliability of such information.
I mainly search for information on search engines and spend time contemplating it. It seems like there’s no better alternative!——P3
These days, experts on platforms like TikTok introduce asthma care methods, but I’ve noticed significant disparities in opinions among different experts. I’m uncertain whom to trust! (Awkward smile) ——P7
A few participants expressed greater confidence in peers’ asthma-related coping experiences and advice from family members compared to online sources. However, they acknowledged the difficulty in determining the credibility of such information.
One time, a colleague’s child was admitted to the ICU due to severe asthma exacerbation. I asked her (referring to the colleague) many questions, and those insights came in handy while devising the discharge plan! (With delight) ——P14
Limited Grasp of Asthma Knowledge
Factors like educational background, occupation, and life experiences led to varying levels of asthma knowledge among participants. Those with lower educational levels, diverse professions, and limited experience struggled to grasp the significance of consistent usage of asthma medications. This lack of comprehension diminished their motivation to actively participate in the formulation of discharge care plans.
To be honest, my education level isn’t high, and I have limited understanding of asthma causes and mechanisms. The more I talk about it, the more I get confused, really! It’s not because of your explanations. ——P2
During discussions about the child’s daily medication dosage with the HCPs, I didn’t comprehend the distinctions in inhalation techniques. It exceeded my understanding. ——P9
My mother (child’s grandmother) has been caring for the child for many years; she’s knowledgeable in this domain. I really want to invite her to assist us in developing the discharge plan! ——P17
Theme 2: Insufficient Provision of Comprehensive Support
Lack of Professional Support from HCPs
Asymmetrical information constitutes a notable impediment for decision-makers. Despite the pivotal role parents played in decision-making processes, a substantial number of participants expressed a pronounced necessity to actively contribute to the formulation of discharge care plans. Nevertheless, they confronted a dearth of requisite, specialized decision-making support, relegating them to a passive role in the decision-making process.
When the HCPs discussed the post-discharge care plan with us, explaining how to use the nebulizer, oxygen device, and other equipment, we often didn’t fully grasp it. ——P11
The HCPs merely mentioned that our child should pay attention to diet and allergens after returning home. We were somewhat perplexed about how to execute it. ——P17
Several participants believed that enhanced care-related decisions necessitate appropriate tools or methods. Gaining support from HCPs emerged as crucial in addressing decision-making challenges.
I believe there should be at least an asthma management manual or software, or perhaps some pre-training for us. This way, we could understand how to observe changes in our child’s condition instead of just receiving verbal instructions (regarding the plan). ——P4
Absence of Emotional Support from Family
Family members play a crucial role in providing essential emotional support during the decision-making process, particularly when parents are confronted with the dual pressures of negative emotions and the health condition of their child. The presence of warmth and encouragement from family members has the potential to significantly enhance parental confidence. Notably, mothers, as compared to fathers, often demonstrated a more pronounced inclination to express their inner feelings. Insufficient attention to addressing emotional support may lead to the emergence of decision-making dilemmas.
During the time my child was hospitalized, my husband was away on a business trip, and I couldn’t focus on the child. It made me feel defeated, and following the nurse’s instructions for the plan felt burdensome. ——P1
My partner (the child’s mother) had trouble sleeping the night before our child was meant to be discharged. I offered a lot of encouraging words to her, and the next day, when I saw her discussing the discharge plan with the nurse, her confidence had significantly increased. ——P10
Theme 3: Encountering Negative Emotions and Wavering Parental Confidence
Parents of children with severe asthma in the PICU experienced three primary psychological patterns: self-blame and distress, contemplative rumination, and active coping. Some participants experienced negative emotions during their child’s hospitalization, such as anxiety, worry, and even depression, which directly impacted their involvement in the formulation of the discharge care plan.
I regret not taking better care of my child and making them suffer. I feel like an inadequate mother, which makes me anxious about making decisions for the child. ——P6
Certain participants held the perspective that the illness experience of their child serve as a notable stressor, exerting a detrimental impact on their parental confidence and prompting them to refrain from implementing care measures that could potentially induce discomfort in the child.
I’ve lost confidence in taking care of my child in the future, making them endure long-term asthma treatment and suffering. ——P7
Seeing my child in distress makes me feel distressed as well. During discussions about the care plan with the nurse, the thought of my child struggling to breathe during an acute attack made my heart ache. ——P13
Theme 4: Navigating Realistic Constraints Impacting Both Parents and HCPs
Limited Time Resources for Clinical Decision-Making
The limitation of temporal resources for collaborative decision-making with HCPs surfaced as a significant concern among participants. HCPs, engrossed in their customary clinical responsibilities, encountered challenges in dedicating substantial time to thorough discussions with parents concerning the rationale and enduring consequences of the discharge care plan. This constraint resulted in parents feeling constrained in their ability to effectively articulate their autonomous perspectives during the decision-making process.
In the ward, HCPs are always in a hurry to prompt us to complete discharge procedures. We understand that they are busy, but this does indeed make us feel passive. ——P1
The HCPs didn’t provide us with detailed follow-up timings and instructions on using the nebulizer effectively; it all felt quite rushed. ——P8
I feel like when I’m making decisions with the HCPs, I can’t say too much; saying too much feels like I’m wasting their time, so we end up feeling somewhat helpless. ——P10
Limitations Arising from the Specific Situation
The children’s family situation also contributes to decision-making dilemmas. Some participants noted that for children of preschool and school age, attending school during the day made it challenging for parents to promptly implement agreed-upon care measures. This led to reliance on teachers for assistance, but this approach did not always yield satisfactory results.
The HCP’s program is authoritative, but quite challenging to implement. For example, scientific exercise and regular medication habits; he (meaning the child) goes to school during the day, so taking medication and breathing exercises during the school day is not feasible, right? --P3
In addition, household income and structure play a role. Regular asthma control medications and pulmonary function exercises, as well as nebulized inhalation therapy as necessary, place a financial burden on low-income families, affecting the long-term quality of discharge care plans. Children cared for primarily by grandparents also face differences in generational perspectives, which create uncertainty in decision-making.
I have elderly family members with medical issues who need financial support. The medications recommended by the HCPs in the discharge plan aren’t inexpensive, and using them long-term would place significant pressure on us. ——P6
We receive a stipend for household expenses while working during the day, and the child is primarily cared for by the elderly. The child’s physical activity, sleep, and diet are areas we don’t have the capacity to manage, so when I’m making decisions, I bring these factors into consideration. ——P8
Theme 5: Balancing the Advantages and Disadvantages of Various Plans
Dilemma Between Restricting and Normalizing Physical Activity
Regular and moderate-intensity exercise can improve ventilation dysfunction caused by narrowed airways and alleviate asthma symptoms. This perspective is widely accepted among HCPs. However, some participants believed that exercise could trigger various discomforts and even impact the child’s learning and daily routines, potentially exacerbating asthma symptoms. Some parents even actively restricted their child’s physical activity due to excessive concerns about acute asthma attacks.
HCPs encourage children to engage in regular physical education classes and maintain a certain level of physical activity after discharge. However, I’m not at ease with this; I’m afraid that another attack might occur. ——P5
My child was admitted to the ICU; this indicates severe symptoms. Can the child engage in physical activity after discharge? I’m having a hard time accepting that. ——P9
The encouragement for children to exercise from doctors makes me hesitant. I felt conflicted when participating in the decision-making process. ——P12
Contradictions Between Different Treatment Plan Choices
Children with severe asthma are typically recommended multiple treatment plans. Post-discharge treatment options for asthma children include asthma medication, inhalation therapy, or oxygen therapy. Parents of these children need to weigh the pros and cons of different options, taking into account their effects, potential risks, and side effects. Additionally, when choosing medication-based treatment, there are different administration methods: oral, intravenous infusion, and inhalation spray. Balancing the contradictions between various treatment plans presents a substantial challenge for parents.
The HCPs explained that one characteristic of asthma is that the child might start wheezing with even mild activity, and they recommended home oxygen therapy. However, oxygen therapy is quite cumbersome and costly, so I’m somewhat uncertain. ——P2
I’m more inclined to have my child use the inhalation spray independently during daily life since I don’t want others to know about the child’s asthma. But I’ve heard that the efficacy of the spray might not be as good as oral medication? ——P9
Consequently, during collaborative development of the discharge care plan with HCPs, some parents experienced psychological conflicts and decision-making apprehension, leading to wavering confidence in their choices, making it difficult to select from different care plans.
My child would rather endure injections than take medication orally, but injections require a hospital visit every time. So, I find it challenging to make a decision (scratches head). ——P10
Discussion
Having a fundamental understanding of the disease and decision-making knowledge is a prerequisite for participating in clinical decision-making between parents and HCPs. This study reveals significant disparities in asthma treatment and care knowledge among parents of children with severe asthma in the PICU. Simultaneously, non-authoritative sources of information fail to meet their information needs when formulating discharge care plan decisions. These factors should not be underestimated as they contribute to the decision-making dilemmas faced by parents.18,19 Previous research has shown that effective HCPs-patient communication plays an essential facilitating role in the clinical decision-making, enhancing the mutual trust, which is a crucial prerequisite for improving decision-making efficiency.20 Turner’s research findings reveal a positive correlation between parent’ willingness to participate in asthma-related decisions and their ability to better cope with acute asthma attacks. A higher level of parental expression of information is associated with an improved family response to acute asthma symptoms. However, up to 47% of families face the risk of reduced communication and have not made a final decision regarding the management plan for childhood asthma.21 Fiks et al conducted a trial to assess the impact of the MyAsthma online decision aid platform on the experiment group.22 This platform not only provides decision support and clarifies family values but also dynamically tracks asthma treatment program and goals, as well as children’s asthma symptoms and outcomes. The results indicated that the MyAsthma platform can facilitate the implementation of shared decision-making, improve decision efficiency, and enhance disease awareness among parents of pediatric asthma patients.
In addition, research has found that individual factors related to decision-making dilemmas, such as educational background and professional expertise, can impede the enthusiasm of parents to participate jointly in the development of discharge care plans, thus limiting the improvement of decision-making ability. Therefore, this suggests that HCPs should accurately assess the disease basic knowledge and decision perception ability of parents of children with asthma at the initial stage of decision-making. They should encourage parents who are involving in the decision-making process for the first time to express their own preferences and provide precise information support through various channels. For parents with inferior education and younger age, more attention should be given, and decision-making training ought to be conducted using simple and understandable language.23,24 Additionally, using physical props and video simulations can deepen their understanding of key points in the pediatric patient’s discharge care plan, thereby avoiding situations where decision-making dilemmas or unmet decision needs arise.25 The results of this study also indicate that the lack of multidimensional support is a significant reason for decision-making dilemmas faced by parents. This finding is in line with the research conducted by Coyne et al, which suggests that support provided by HCPs and family members, in their distinct roles, equally influences the ultimate quality of decisions.26 Compared to the parents of pediatric patients, HCPs play an authoritative role in the development of asthma-related discharge plans, offering parents strong professional decision aids to alleviate their decision-related anxiety.27 Meanwhile, family members have potential to provide emotional psychological support to decision-makers. Research indicates that hospitalization of a child is a psychological test of parenting confidence for most parents.28 Parents of hospitalized children with low confidence are prone to experiencing negative emotions such as guilt, anxiety, a sense of disease uncertainty, and helplessness. It has been demonstrated that these negative emotions are dangerous factors leading to decision-makers falling into decision dilemmas.29,30
Mudd investigated a strong correlation between the decision quality of parents of children with asthma presenting at the emergency department, their level of home management, and their communication with HCPs.29,30 Therefore, the positive psychological state of parents has a significant impact on the prognostic outcomes of the child. Based on this, HCPs should enhance training on key postoperative care skills during routine health education processes, or stimulate parents of pediatric patients to engage in self-improvement practices and seek professional support through empowerment education, addressing their decision support needs.31 Furthermore, coping strategies for negative emotions need be approached from the perspective of the potential benefits and gains in caring for the child, assisting parents in recognizing the advantages and rewards of caring for the child, promoting positive psychological adaptation, and alleviating their negative emotions, thereby enabling them to participate in the process of shared decision-making in a more positive manner.32,33
While the majority of parents recognize the necessity of participating in post-discharge care plans for their child’s prognosis and recovery, this study reveals that certain practical factors force parents to passively follow HCPs’ recommendations during the decision-making process, to some extent limiting the effectiveness of shared decision-making. A qualitative study, from the perspective of HCPs, elucidates that a shortage of time resources is a common challenge in global clinical practice when it comes to facilitating shared decision-making.34 In light of this, scholars unanimously agree that intervening with decision aids for patients can significantly reduce the total time required for decision-making and enhance program efficiency.35 Furthermore, healthcare managers should pay more attention to the heavy daily workload of HCPs, appropriately reducing the clinical workload of those who assume leadership in decision-making tasks, further harnessing the proactive capabilities of HCPs. Some studies also indicate that differences in family-specific circumstances and caregiving experiences affect the quality of health-related decisions for the child, such as family conflicts, economic conditions, and living arrangements.36,37 Therefore, HCPs may consider organizing family meetings to reconcile differences in childcare opinions among different generations within the family and recommend cost-effective care supplies based on a thorough assessment of the family’s economic situation, thus minimizing the impact behind the decision-making dilemmas faced by parents of children with severe asthma.38 Additionally, the research finds that parents are well aware of the benefits of home-based asthma management for their child’s long-term health outcome after discharge. However, they often struggle with how to balance restricted activities and regular activities, as well as the choice between different ongoing asthma treatment programs, leading to decision-making dilemmas.39 In a large cross-sectional survey, Gandhi’s group investigated 160 pairs of children with asthma and their parents, demonstrating that self-efficacy in medical interactions and parental satisfaction with shared decision-making indirectly influence children’s asthma control and asthma-specific quality of life.40 Therefore, interdisciplinary involvement in the development and follow-up of post-discharge care plans for children represents a novel approach to effectively alleviate the confusion and conflicting emotions experienced by parents and enhance their satisfaction with healthcare. Simultaneously, HCPs should take a proactive leadership role, establishing a multidisciplinary continuity care team with specialized nursing at its core, and including physicians, asthma specialist nurses, physical therapists, and respiratory therapists.41 This team can provide precise and effective professional decision guidance to parents, ultimately improving parental compliance with decision recommendations.
Limitations
We also recognize some limitations. Given that our qualitative study was conducted exclusively from the perspective of parents of children with asthma, the experiences and perceptions of other stakeholders, such as children and HCPs, remain unclear and necessitate further research. Moreover, it is essential to consider that this study was carried out in China, a context where clinical decision-making outcomes and quality may be influenced by various domestic policies, healthcare systems, and cultural factors. Therefore, caution should be exercised when extrapolating the study results to populations of various ethnic or cultural backgrounds. Furthermore, the primary aim of our study was to explore the personal experiences of parents in the decision-making process concerning severe childhood asthma. It is conceivable that these findings may not be directly applicable to the development of discharge plans for children with milder asthma. Consequently, future studies could benefit from including a comparison group of children with mild and moderate asthma to provide a more comprehensive understanding of the decision-making dynamics across the spectrum of asthma severity.
Conclusion
This study employed semi-structured in-depth interviews with parents of children with severe asthma in the PICU to analyze the dilemmas they face during the decision-making process of discharge care plans. Five main themes emerged from the analysis, highlighting the complexity of disease-related information, the lack of comprehensive decision support, negative emotions and inadequate parenting confidence, realistic limitations for both caregivers and patients, and the dilemma of balancing pros and cons among different options. The study results suggest that HCPs should encourage active participation of parents in the formulation of discharge care plans, accurately assess parents’ decision-making capabilities and information-seeking attitudes, provide tailored decision support based on their specific family circumstances, facilitate information sharing between caregivers and parents, and promote the high-quality implementation and development of shared decision-making in pediatric nursing practice.
Data Sharing Statement
The data analyzed during our study are not publicly available due to an agreement with the participants on the confidentiality of the data, but are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Our study was approved by the Ethics Committee of the Shandong Provincial Hospital. Informed consent was obtained from all participants. All research activities were conducted in accordance with hospital’s guidelines and requirements.
Acknowledgments
We are grateful to the interviewed parents who participated in the study and healthcare professionals in related hospitals who facilitated and supported this study greatly.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Licari A, Brambilla I, Marseglia A, De Filippo M, Paganelli V, Marseglia GL. Difficult vs. severe asthma: definition and limits of asthma control in the pediatric population. Front Pediatr. 2018;6:170. doi:10.3389/fped.2018.00170
2. Pijnenburg MW, Fleming L. Advances in understanding and reducing the burden of severe asthma in children. Lancet Respir Med. 2020;8(10):1032–1044. doi:10.1016/S2213-2600(20)30399-4
3. Versiani NPDQ, Goncalves AC, Cruz AA, De lima BFLL. Lung function in severe pediatric asthma: a longitudinal study in children and adolescents in Brazil. Clin Transl Allergy. 2017;7:48. doi:10.1186/s13601-017-0183-6
4. Ross KR, Gupta R, DeBoer MD, et al. Severe asthma during childhood and adolescence: a longitudinal study. J Allergy Clin Immunol. 2020;145(1):140–146. doi:10.1016/j.jaci.2019.09.030
5. Larenas-Linnemann D, Nieto A, Palomares O, Pitrez PM, Cukier G. Moving toward consensus on diagnosis and management of severe asthma in children. Curr Med Res Opin. 2018;34(3):447–458. doi:10.1080/03007995.2017.1400961
6. Licari A, Ciprandi R, Marseglia G, Ciprandi G. Anxiety and depression in adolescents with severe asthma and in their parents: preliminary results after 1 year of treatment. Behav Sci. 2019;9(7). doi:10.3390/bs9070078
7. Heuckendorff S, Johansen MN, Overgaard C, Johnsen SP, Kelly Y, Fonager K. Parental mental health, socioeconomic position and the risk of asthma in children-a nationwide Danish register study. Eur J Public Health. 2022;32(1):14–20. doi:10.1093/eurpub/ckab205
8. Rastogi D, Gupta S, Kapoor R. Comparison of asthma knowledge, management, and psychological burden among parents of asthmatic children from rural and urban neighborhoods in India. J Asthma. 2009;46(9):911–915. doi:10.3109/02770900903191323
9. Levy BD, Noel PJ, Freemer MM, et al. Future research directions in asthma. An NHLBI working group report. Am J Respir Crit Care Med. 2015;192(11):1366–1372. doi:10.1164/rccm.201505-0963WS
10. Cazzola M, Matera MG, Rogliani P, Calzetta L, Ora J. Step-up and step-down approaches in the treatment of asthma. Expert Rev Respir Med. 2021;15(9):1159–1168. doi:10.1080/17476348.2021.1935245
11. Reddy AP, Gupta MR. Management of asthma: the current US and European guidelines. Adv Exp Med Biol. 2014;795:81–103.
12. Marangos-Frost S, Wells D. Psychiatric nurses’ thoughts and feelings about restraint use: a decision dilemma. J Adv Nurs. 2000;31(2):362–369. doi:10.1046/j.1365-2648.2000.01290.x
13. Klok T, Lubbers S, Kaptein AA, Brand PL. Every parent tells a story: why non-adherence may persist in children receiving guideline-based comprehensive asthma care. J Asthma. 2014;51(1):106–112. doi:10.3109/02770903.2013.841191
14. Srour-Alphonse P, Cvetkovski B, Azzi E, et al. Understanding the influences behind parents’ asthma decision-making: a qualitative exploration of the asthma network of parents with children with asthma. Pulm Ther. 2021;7(1):151–170. doi:10.1007/s41030-021-00145-w
15. Miller VA. Parent-child collaborative decision making for the management of chronic illness: a qualitative analysis. Fam Syst Health. 2009;27(3):249–266. doi:10.1037/a0017308
16. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
17. Edward KL, Welch T. The extension of Colaizzi’s method of phenomenological enquiry. Contemp Nurse. 2011;39(2):163–171. doi:10.5172/conu.2011.163
18. Brody JL, Annett RD, Scherer DG, Turner C, Dalen J. Enrolling adolescents in asthma research: adolescent, parent, and physician influence in the decision-making process. J Asthma. 2009;46(5):492–497. doi:10.1080/02770900902866768
19. Jonas D, Scanlon C, Bogetz JF. Parental decision-making for children with medical complexity: an integrated literature review. J Pain Symptom Manage. 2022;63(1):e111–e123. doi:10.1016/j.jpainsymman.2021.07.029
20. Becker TD, Lin HC, Miller VA. A pilot study of observed physician-parent-child communication and child satisfaction in a gastroenterology clinic. Patient Prefer Adherence. 2018;12:1327–1335. doi:10.2147/PPA.S171620
21. Turner EM, Koskela-Staples N, Voorhees S, McQuaid EL, Fedele DA. Health-related decision-making in early adolescents with poorly controlled asthma. Clin Pract Pediatr Psychol. 2021;9(1):24–34.
22. Fiks AG, Mayne SL, Karavite DJ, et al. Parent-reported outcomes of a shared decision-making portal in asthma: a practice-based RCT. Pediatrics. 2015;135(4):e965–e973. doi:10.1542/peds.2014-3167
23. Kornblit A, Cain A, Bauman LJ, Brown NM, Reznik M. Parental perspectives of barriers to physical activity in urban schoolchildren with asthma. Acad Pediatr. 2018;18(3):310–316. doi:10.1016/j.acap.2017.12.011
24. Heyduck K, Bengel J, Farin-Glattacker E, Glattacker M. Adolescent and parental perceptions about asthma and asthma management: a dyadic qualitative analysis. Child Care Health Dev. 2015;41(6):1227–1237. doi:10.1111/cch.12277
25. Bokhour BG, Cohn ES, Cortes DE, et al. Patterns of concordance and non-concordance with clinician recommendations and parents’ explanatory models in children with asthma. Patient Educ Couns. 2008;70(3):376–385. doi:10.1016/j.pec.2007.11.007
26. Coyne I, Amory A, Kiernan G, Gibson F. Children’s participation in shared decision-making: children, adolescents, parents and healthcare professionals’ perspectives and experiences. Eur J Oncol Nurs. 2014;18(3):273–280. doi:10.1016/j.ejon.2014.01.006
27. Gutierrez SJ, Fagnano M, Wiesenthal E, Koehler AD, Halterman JS. Discrepancies between medical record data and parent reported use of preventive asthma medications. J Asthma. 2014;51(4):446–450. doi:10.3109/02770903.2013.878351
28. Harrington KF, Haven KM, Bailey WC, Gerald LB. Provider perceptions of parent health literacy and effect on asthma treatment recommendations and instructions. Pediatr Allergy Immunol Pulmonol. 2013;26(2):69–75. doi:10.1089/ped.2013.0237
29. Feudtner C, Schall T, Hill D. Parental personal sense of duty as a foundation of pediatric medical decision-making. Pediatrics. 2018;142(Suppl 3):S133–S141. doi:10.1542/peds.2018-0516C
30. Yoos HL, Kitzman H, Henderson C, et al. The impact of the parental illness representation on disease management in childhood asthma. Nurs Res. 2007;56(3):167–174. doi:10.1097/01.NNR.0000270023.44618.a7
31. Finnvold JE. In their own words: early childhood asthma and parents’ experiences of the diagnostic process. Scand J Caring Sci. 2010;24(2):299–306. doi:10.1111/j.1471-6712.2009.00720.x
32. Lakhanpaul M, Culley L, Robertson N, et al. A qualitative study to identify parents’ perceptions of and barriers to asthma management in children from South Asian and White British families. BMC Pulm Med. 2017;17(1):126. doi:10.1186/s12890-017-0464-9
33. Goddard B, Hutton A, Guilhermino M, McDonald VM. Parents’ decision making during their child’s asthma attack: qualitative systematic review. J Asthma Allergy. 2022;15:1021–1033. doi:10.2147/JAA.S341434
34. Morawska A, Gregory C, Burgess S. Parental beliefs about behaviour problems of their asthmatic children and interventions to support parenting. J Child Health Care. 2012;16(1):75–90.
35. Law GC, Jones CJ, Bulbul A, Smith HE. ”At a loss of what to do”: a qualitative analysis of parents’ online discussion forums about their administration of asthma inhalers to their young children. J Asthma. 2020;57(8):914–923. doi:10.1080/02770903.2019.1615941
36. Srour-Alphonse P, Cvetkovski B, Rand CS, et al. It takes a village - asthma networks utilized by parents when managing childhood asthma medications. J Asthma. 2020;57(3):306–318. doi:10.1080/02770903.2019.1568456
37. Butler AM, Weller B, Titus C. Relationships of shared decision making with parental perceptions of child mental health functioning and care. Adm Policy Ment Health. 2015;42(6):767–774. doi:10.1007/s10488-014-0612-y
38. Yin HS, Dreyer BP, Vivar KL, MacFarland S, van Schaick L, Mendelsohn AL. Perceived barriers to care and attitudes towards shared decision-making among low socioeconomic status parents: role of health literacy. Acad Pediatr. 2012;12(2):117–124. doi:10.1016/j.acap.2012.01.001
39. Silva N, Crespo C, Carona C, Bullinger M, Canavarro MC. Why the (dis)agreement? Family context and child-parent perspectives on health-related quality of life and psychological problems in paediatric asthma. Child Care Health Dev. 2015;41(1):112–121. doi:10.1111/cch.12147
40. Gandhi PK, Kenzik KM, Thompson LA, et al. Exploring factors influencing asthma control and asthma-specific health-related quality of life among children. Respir Res. 2013;14(1):26. doi:10.1186/1465-9921-14-26
41. Cook J, Beresford F, Fainardi V, et al. Managing the pediatric patient with refractory asthma: a multidisciplinary approach. J Asthma Allergy. 2017;10:123–130. doi:10.2147/JAA.S129159
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.