")
Back to Journals » Risk Management and Healthcare Policy » Volume 17
External Vs Internal e-Referrals: Results from a Nationwide Epidemiological Study Utilizing Secondary Collected Data
Authors Aljerian NA, Alharbi AA , Alghamdi HA , Binhotan MS, AlOmar RS , Alsultan AK, Arafat MS, Aldhabib A, Alabdulaali MK
Received 17 December 2023
Accepted for publication 23 March 2024
Published 28 March 2024 Volume 2024:17 Pages 739—751
DOI https://doi.org/10.2147/RMHP.S453042
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Haiyan Qu
Nawfal A Aljerian,1,2 Abdullah A Alharbi,3 Hani A Alghamdi,4 Meshary S Binhotan,5,6 Reem S AlOmar,7 Ali K Alsultan,1 Mohammed S Arafat,1 Abdulrahman Aldhabib,1 Mohammed K Alabdulaali1
1Medical Referrals Centre, Ministry of Health, Riyadh, Kingdom of Saudi Arabia; 2Emergency Medicine Department, King Saud Bin Abdulaziz University for Health Sciences, Riyadh, Kingdom of Saudi Arabia; 3Family and Community Medicine Department, Jazan University, Jazan, Kingdom of Saudi Arabia; 4Department of Family and Community Medicine, King Saud University, Riyadh, Kingdom of Saudi Arabia; 5Emergency Medical Services Department, King Saud Bin Abdulaziz University for Health Sciences, Riyadh, Kingdom of Saudi Arabia; 6King Abdullah International Medical Research Centre, Riyadh, Kingdom of Saudi Arabia; 7Department of Family and Community Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Kingdom of Saudi Arabia
Correspondence: Hani A Alghamdi, Department of Family and Community Medicine, College of Medicine, King Saud University, P.O Box 12372, Riyadh, 7065, Kingdom of Saudi Arabia, Tel +966507022266, Email [email protected]
Background: E-referral systems, streamlining patient access to specialists, have gained global recognition yet lacked a comparative study between internal and external referrals in Saudi Arabia (KSA).
Methods: This retrospective study utilized secondary data from the Saudi Medical Appointments and Referrals Centre system. The data covers 2020 and 2021, including socio-demographic data, referral characteristics, and specialties. Logistic regression analysis was used to assess factors associated with external referrals.
Results: Out of 645,425 e-referrals from more than 300 hospitals, 19.87% were external. The northern region led with 48.65%. Males were 55%, and those aged 25– 64 were 56.68% of referrals. Outpatient clinic referrals comprised 47%, while 61% of referrals were due to a lack of specialty services. Several significant determinants are associated with higher rates of external referral with (p-value < 0.001) and a 95% Confidence interval. Younger individuals under 25 exhibit higher referral rates than those aged 25– 64. Geographically, compared to the central region, in descending order, there were increasing trends of external referral in the northern, western, and southern regions, respectively (OR = 19.26, OR = 4.48, OR 3.63). External referrals for outpatient departments (OPD) and dialysis services were higher than for routine admissions (OR = 1.38, OR = 1.26). The rate of external referrals due to the lack of available equipment was more predominant than other causes. Furthermore, in descending order, external referrals for organ transplantation and oncology are more frequent than for medical specialties, respectively (OR = 9.39, OR = 4.50).
Conclusion: The study reveals trends in e-referrals within the KSA, noting regional differences, demographic factors, and types of specialties regarding external referrals, benefiting the New Model of Care for the 2030 Vision. Findings suggest expanding virtual consultations to reduce external referrals. Strengthening primary care and preventive medicine could also decrease future referrals. Future studies should assess resource distribution, including infrastructure and workforce, to further inform healthcare strategy.
Keywords: e-referrals, health policy, epidemiology, public health
Background
Referrals form a large part of both inpatient and outpatient services. Timely access to specialized facilities and personnel is necessary to achieve optimal patient care.1 The traditional paper-based referrals have been shown to cause delayed treatment due to potentially missing information as well as inconvenience to patients. Literature shows that the use of e-referral systems forces the standardization of information and communication as part of the referral process, hence improving waiting times and efficiency.2 Given these reported benefits, it is naturally expected that more countries are adopting e-referral systems such as Canada, Norway, England, and Denmark.3–6
In the Kingdom of Saudi Arabia (KSA), the Saudi Medical Appointments and Referrals Centre (SMARC), formerly known as Ehalati, operates and manages e-referrals across the country.7 The SMARC system manages both internal and external referrals. Internal referrals represent any referral of patients from one health institution to another within the same administrative area, whereas external referrals represent the referral of patients to healthcare institutions outside of that referring administrative area. Although internal referrals are preferred, they are sometimes insufficient to meet patients’ healthcare needs due to the variability of healthcare services between areas. Referrals involved within the SMARC system include those for inpatient as well as outpatient services, ie, where beds are required.8 Variations in healthcare services and resources, including hospitals, physicians and equipment, between regions within a country are well documented and known worldwide.9,10 Thus, to meet the aim of the referral concept, which is to move a patient from a place that has insufficient resources such as equipment and specialized healthcare providers to another facility, external referrals are also available within the SMARC e-referral system.7,11
External referrals are likely to be more complicated to manage and costly than standard internal referrals. The Ministry of Health (MoH) in the KSA provides flight tickets and daily living expenses to patients and their fellows when they are referred externally.12 Also, in some cases according to patients’ conditions, external referrals may include transferring patients using ground or air ambulance services, which consequently increases both complexity and cost. However, external referrals are essential to ensure high-quality care for all people across the country. Nevertheless, it is difficult to draw conclusions between internal and external referrals, due to the lack of studies in the literature.
The concept of internal vs external referrals between regions, defined in this study, is not investigated yet in the literature. The published studies had used other definitions of internal vs external referrals, according to the purpose of each conducted study. For example, Merlo et al13 defined external referrals as any referral outside the healthcare center where the study was conducted while Porter et al14 defined it as any referral outside the investigated specialty (eg, family medicine) in their study. Other definitions were also noted.15,16 This creates a knowledge gap in the literature concerning the internal vs external referrals between regions on a national level.
To our knowledge, no study has yet investigated the differences between internal and external referrals using similar nationwide secondary collected data. Exploring and understanding the pattern of internal and external referrals as well as identified factors associated with external referrals can provide insight on the structural and functional capacities within and between regions and subsequently inform public health policy.
Methods
Study Design and Setting
A retrospective analytical study is used to analyze secondary data acquired from the SMARC e-referral system of the KSA which covers 300 hospitals. This system which began formal national operations through a unified referral system in 2019 covers all 13 administrative areas of the country. Any referral whether internal, ie within the administrative area itself or external, ie across the border of a specific administrative area, will have been registered within the system. The current study encompasses data for both 2020 and 2021.
Ethical Considerations
The study compiles with the ethical principles of the World Medical Association Declaration of Helsinki.17 The MoH central institutional review board and the Imam Abdulrahman Bin Faisal University’s institutional review board have both approved the study (IRB log No: 23–77 E and IRB-2023-01-305). The data did not include any personally identifying information, and the data was secured and used only for the purposes of this research.
Study Variables
The data included demographic variables of patients such as age, sex and nationality, as well as referral characteristics which included the date of the visit which facilitated the extraction of the seasons of referrals, the region of the visit according to the five business units (BUs),18 bed types that have been requested during the referral, the type of the referral itself, the reasons for referrals, the specialties for which the referral is requested and finally, whether the referral is internal or external.
Data Analysis
The main dependent variable in this study was internal vs external referrals. They are defined as whether an e-referral has been requested to another hospital within any of the administrative areas or outside an administrative area. Descriptive statistics were given through frequencies and percentages. Cross tabulations were performed, and p-values were computed by means of a series of chi-squared tests. A binary logistic regression analysis was performed to obtain Odds Ratios (ORs) and their related 95% Confidence Intervals (CIs). The level of significance was set at 0.05, and the Stata Statistical Software version 16 was used for all analyses.19
Results
Sociodemographic Characteristics According to Internal Vs External Referral Requests
As shown in Table 1, the data included 645,428 referral requests. Of those, 80.13% were internal and 19.87% were external. Of the total population, adults aged between 25 and less than 65 years old had the highest number of requests, followed by the geriatric population (56.68% and 13.44% respectively). Among the external requests across all age groups, infants were observed to be the highest (24.91%), followed by children aged between 1 and <14 years of age (21.90%). With regard to sex, even though males had more requests than females in total (55.42%), females were higher in terms of external referrals when compared to males (21.40% and 19.12% respectively). Saudis also had higher requests compared to non-Saudis and were also higher in external requests (84.89% and 21.25% respectively). The number of both total, internal, and external requests increased during 2021 compared to 2020. Finally, and with regards to the five business units, the Western BU had the highest share of all referral requests, and the Eastern BU had the lowest. However, the Northern BU was the highest in terms of external referrals reaching 48.65%.
 |
Table 1 Sociodemographic Characteristics of Patients According to Internal Vs External Requests Across the Kingdom of Saudi Arabia |
Referral Characteristics According to Internal Vs External Referral Requests
Table 2 presents the results of referral characteristics. The results show that mostly referrals were for outpatient departments (OPDs), hence no beds were required for those specific referrals in 47.05% of all referrals. These were followed by regular ward beds in 36.15% of referrals, and the least requested bed type was burning beds (0.09%). For external referrals, OPDs were also the most common followed by pediatric intensive care (PICU) beds and cardiac care unit (CCU) beds (25.37%, 19.90% and 19.26%, respectively). Also, for referral request types, 47.25% consisted of referrals for routine OPD. This was also the most common for external referral requests (25.41%), and this was followed by patients for dialysis (20.18%) although there were only 114 dialysis patients in total. With regard to the reasons for referral, unavailable specialty was the most commonly reported reason in 61.58% of all referrals. However, specifically for external referrals, unavailability of a machine was the most commonly reported reason in 26.20% compared to all other reasons.
 |
Table 2 Patient Characteristics According to Internal Vs External Requests Across the Kingdom of Saudi Arabia |
Distribution of Medical/Surgical Specialties Requested for Referrals
Table 3 presents the distribution of medical and surgical specialties requested for referrals according to internal vs external referrals. Surgery was the leading specialty constituting 26.06% of all referrals followed by medicine and cardiac surgery (22.26–9.69% respectively). With respect to external requests, organ transplantation was the most common reaching 58.96% compared to other specialties, followed by oncology and medical rehabilitation (41.60–34.88%). The least common specialty with external referrals was psychiatry (8.38%).
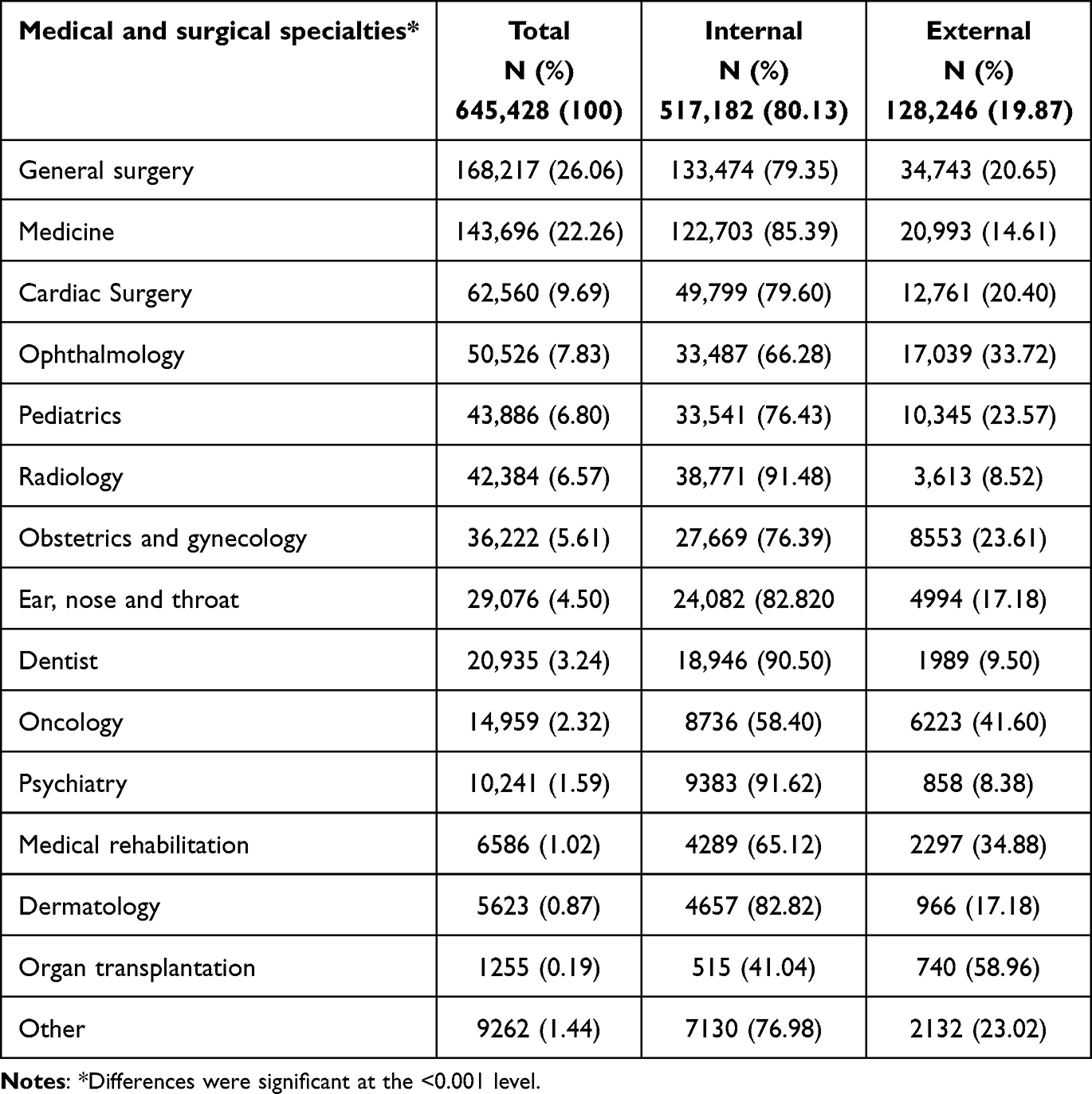 |
Table 3 Distribution of Specialties According to Internal Vs External Referrals Across the Kingdom of Saudi Arabia |
Multivariable Analysis of Factors Associated with External Referrals
Table 4 shows the ORs and 95% CI from the multivariable logistic regression analysis of factors associated with external referrals. Firstly, it was observed that infants aged less than 1 year had 21% increased likelihood of receiving external referrals when compared with adults (95% CI = 1.17–1.25), whereas the elderly had a 9% decreased likelihood (95% CI = 0.89 −0.93). With respect to the types of referrals and when compared to routine admissions, an increased likelihood was observed for both routine OPD referrals (OR = 1.38, 95% CI = 1.35–1.42) and dialysis patients, however for dialysis it was not significant. Also, for both lifesaving and ER referral types, a decreased likelihood for external referral was observed (OR = 0.91, 95% CI = 0.88–0.95 and OR = 0.82, 95% CI = 0.80–0.84 respectively). Compared to the unavailability of machines as the reason for referral, all other reasons had a decreased likelihood for external referrals; however, social reasons were observed to have the lowest decreased likelihood where the OR was 0.26 (95% CI = 0.21–0.88). Examining the ORs for external referrals by the different specialties, organ transplantation, and oncology had the highest likelihood (OR = 9.39, 95% CI = 8.13–10.83 and OR = 4.50, 95% CI = 4.31–4.71), whereas radiology had the lowest likelihood (OR = 0.39).
 |
Table 4 Adjusted Binary Logistic Regression Analyses for Characteristics Associated with External Referrals |
Discussion
This study is the first of its kind to explore the differences between internal and external referrals at the national level in the KSA utilizing secondary routinely collected data. Furthermore, no study has yet investigated the distribution of external and internal referrals between secondary and tertiary care, an area our research has sought to address. The analyses presented here have been successfully able to highlight potentially problematic areas and inform on health policy issues. Results shed light on areas that need further exploration and assessment to justify the discrepancy in referral characteristics between these regions.
E-referral systems, which integrate part of the referral process via information technology, have undergone various evaluations globally. A recent study examining the patterns and trends of e-referral request acceptances contrasting with the SMARC system in the KSA revealed that the predominant patient demographic consists of middle-aged Saudi males, primarily located in the Western regions. This trend is largely attributed to the absence of specialized physicians or medical specialties in local facilities.8 In Australia, the US Veterans Administration, and the UK, these systems have been tested, utilized, and assessed, revealing challenges related to coordination, policy, standardization, and mixed outcomes on referral content quality.20–22 Denmark reports extensive use of e-referrals by general practitioners, leading to substantial cost savings, while Norway highlights the importance of collaboration among clinicians for effective e-referral implementation.23,24
The study found that the majority of referrals were internal. This indicates an overall good quality of healthcare services offered in the KSA. While this is largely true, several discrepancies were observed. For example, infants had the highest percentage of external referrals compared to other age categories. Also, referral by bed type exhibited a slightly higher percentage for pediatric intensive care units (PICU) and neonatal intensive care units (NICU) which indicates a need for specialized care for this age group that may not be available in specific administrative areas. Infant services may be undervalued due to the lower density of the population at this age compared to other age groups, especially adults aged between 25 < 65 years and the potentially higher need for services among these relatively older people. In the KSA, the adult population surpasses the number of children, leading to a health system primarily directed towards adults.25 Also, the high prevalence of chronic conditions among adults necessitates substantial health resources.26,27 On the other hand, the lower incidence of critical conditions in children is reflected in the higher odds of external referrals among this vulnerable age group for specialized care, compared to adults who receive comprehensive services that are more distributed across regions. This population density resource distribution reflects the demographic and epidemiological realities of the Saudi healthcare landscape. This is similar in the US, where most critical care beds are designated for adults, while only 6% are for pediatrics, highlighting a pronounced shortage in pediatric critical care and trained personnel and emphasizing the disparity in resource distribution between adult and pediatric critical care services.28 Additionally, international studies have indicated that, due to the scarcity of PICU resources, it is imperative to refer only patients who truly require this service to regional PICUs.29–32
We also found that female patients were referred to external medical facilities more than males. Worldwide, an estimated 287,000 women die annually due to maternal causes. The majority of these maternal deaths are a direct result of obstetric causes. Obstetric complications often arise during or shortly after delivery and can quickly become life-threatening.33 Referral to more advanced medical facilities for maternity-related conditions may be mainly due to complications that require life-saving interventions.34 This is also evident by the high external referral requests for obstetrics and gynecology found in this study, even though no statistically significant association was found for sex.
The sociodemographic findings also show more external referrals to Saudis compared to non-Saudis. However, statistics reveal that non-Saudis are fewer than Saudi nationals and are primarily located in the capital which offers the best specialized services, and subsequently, less demand for external referrals is needed.35 In addition, SMARC, under the Saudi MoH, predominantly manages public hospitals that serve citizens who do not require insurance. Meanwhile, non-Saudi workers are provided with private insurance and tend to be treated in private hospitals,36 which utilizes a different referral system. This results in a higher rate of referrals within the public sector for Saudis. Nonetheless, non-Saudis also benefit from quality healthcare, regardless of the type of hospital.
Although the Western BU was the highest in terms of total referrals, a closer look at the pattern of referrals showed a significant proportion of internal referrals in the Central BU, while the highest proportion of external referrals was in the Northern BU. According to the 2021 edition of the statistical yearbook issued by the MoH, the number of both governmental and private hospitals in the last five years in the Central BU was 111 with a total number of beds equal to 20,515. Whereas the total number of hospitals and beds in the Northern BU was only 46 and 6650, respectively.37 This regional disparity with lower resources in the Northern BU is consistent with previous studies that examined the variation in the quality of care between the five BUs.18,38,39 Albeit the confined focus in those studies were COVID-19 patients, they did examine the quality of care from different angles at a national level and have all arrived at the conclusion that the infrastructure and allocated resources in the Northern BU are of concern. This also explains the higher percentage of external referrals in the Northern BU compared to other BUs.
Around half of all referrals had originated from outpatient departments (OPDs), and only around a quarter of those OPD referrals were externally referred. In OPDs, there are often fewer complex cases that can be managed internally and referred easily to other neighboring hospitals. This is also complemented with the finding that routine referrals were the most common also reaching around half of all referral types. Whereas referrals for CCU and PICU were slightly higher than other categories among the external referrals which could reflect deficiency in providing these services for the patients. We also found that only a small proportion of referrals were categorized as lifesaving and only 12.18% being external, indicating the overall good quality of healthcare services when dealing with life-threatening cases.
With regard to the reason of referral, the most common reason for external referrals was a lack of healthcare equipment. This issue is not unique to the KSA, as The United States Food and Drug Administration regularly publishes shortage list of equipment required for a variety of clinical specialties.40 This shortage has the ability to impact the process of diagnosing a disease as well as patient management and subsequently patients’ outcomes.41 The data indicate the need for this equipment to avoid the cost of external referrals, which may not always be possible due to issues surrounding training and maintenance.42
Unavailable specialty and physician were ranked as the second and third most common reasons for external referrals. This issue may have a detrimental effect on the delivery of timely and much needed healthcare services.43,44 Unfortunately, research predicts that these shortages may become worse within the next decade as the demand for physicians outweighs the supply.45 This is likely due to the changes in population dynamics, including the growing number of people.46 In fact, in a very recent study which had examined referrals for emergency cases alone, it was observed that the most common reason for those referrals was also the unavailability of a subspecialized department followed by the availability of a physician.8 Although the use of telemedicine and the Saudi experience with the Seha Virtual Hospital may compensate for the shortages in some areas, they may not always be applicable.47–49 Therefore, local initiatives to compensate the shortages in specialties and physicians are recommended.
In recent years, the demand for organ transplants has increased dramatically worldwide and in the KSA as well.50 Our data clearly demonstrate that organ transplantation is the highest specialty that refers patients externally to major cities where organ transplant centers are located.51 Several challenging factors make it difficult to develop such centers in all areas of the country. These include complex medical and ethical regulations imposed by the WHO governing the medical practice of organ transplantation as well as the complexity of the multi-step process of these procedures which requires a team of highly qualified professionals, financial barriers, lack of support staff and its major economic burden on the healthcare system.52,53 Organ transplant was followed by oncology. In the KSA, and as per the MoH’s statistical yearbook of 2021, the MoH oversees only four centers, two of which are within the boundaries of the Central BU.37 Furthermore, the main center for supervising and regulating organ donations known as the Saudi Centre for Organ Transplantation participates in a network of organ sharing with other Gulf countries, hence increases the possibility of external referrals.54 However, access to oncology remains inadequate worldwide. Similar to the KSA, the United Kingdom applies centralized care to oncology patients which subsequently requires external referrals.55 Treatment for cancerous patients is among the most expensive and challenging due to a lack of financial and human resources.56 These realities may explain the need for external referrals to areas equipped with advanced medical facilities and personnel.
The current findings have several health policy implications. Firstly, we strongly recommend hastening the implementation of the unified electronic medical records across all areas of the KSA. The primary objective is to centralize the registration of comprehensive medical information, by increasing convenient healthcare for service users and providers through eliminating unnecessary travel for stable cases, for example, patients that require follow-up. This will allow patients to perform any necessary investigation at the nearest hospital rather than travel externally. It will also allow healthcare providers to be informed of the health status of patients. Secondly, we believe that virtual clinics are an incredible tool that would help keep external and internal referrals at a minimum, thereby reducing costs and easing accessibility to patients. Thirdly, focusing on an advanced primary healthcare system especially with preventive medicine will contribute to a coherent and well-rounded healthcare system. For example, ensuring periodic examination of the patient, early detection of diseases, and reducing disease complications will most probably decrease pressures on hospitals. Finally, enabling interaction and communication among diverse stakeholders, such as the MoH, other governmental organizations, and private medical agencies, through regular meetings is essential to facilitating integration, cooperation, and communication throughout the referral system. A proactive stance strengthens the referral system and effectively addresses existing challenges to ensure all parties are well-informed regarding current and updated protocols and guidelines. By creating a collaborative environment and facilitating knowledge sharing, medical organizations will achieve efficiency and effective referral processes, improving healthcare delivery and thus patient outcomes.
This study is the first to utilize nationally and routinely collected data to explore the predictors of external referrals in the KSA. Nevertheless, there are limitations to consider in this study. First, the retrospective design restricts our ability to establish reliable relationships and draw conclusions. Second, our study lacked detailed information on several crucial factors, including the availability of human and non-human resources in each region. Finally, we are limited to data collected by the SMARC e-referral system.
We propose several approaches to future research to address these limitations and advance the field forward. Firstly, prospective or longitudinal studies could be designed to confirm the predictors identified and explore their causal relationships with external referral rates among regions in the KSA. Secondly, qualitative research exploring healthcare providers’ perspectives could reveal additional predictors not captured by the SMARC e-referral system. Lastly, further research could provide a more comprehensive understanding of the referral process by expanding the dataset and integrating additional variables such as socioeconomic status, resource distribution among regions, patient preferences, and detailed clinical outcomes.
Conclusions
This study is the first to provide the pattern of internal and external e-referrals across the KSA and to identify potential factors predicting external referrals. Patients aged between 25 < 65 had the highest referral requests, indicating higher needs of care for this group of patients. Most referral requests were internal, which are suggestive of prevalent high-quality care within the administrative areas and BUs. Infants and younger patients, requests originating from the Northern region followed by the Western and Southern regions, unavailability of machines, referrals for organ transplantation followed by oncology and surgical specialties, were all factors predicting external referrals, highlighting resource allocation concerns. The expansion of virtual clinics, focusing on preventive strategies as well as future research focusing on service provision, referral services, and resource availability across all levels of healthcare is recommended in order to aid in the implementation of the New Model of Care under the new 2030 Vision of the KSA.
Abbreviations
KSA, Kingdom of Saudi Arabia; SMARC, Saudi Medical Appointments and Referrals Centre; MoH, Ministry of Health; BU, Business unit; OR, Odds Ratio; CI, Confidence interval; PICU, Pediatric intensive care units; NICU, Neonatal intensive care units.
Data Sharing Statement
The datasets used and analyzed during the current study are available for request from the SMARC system.
Acknowledgments
The authors would like to thank all personnel involved in maintaining the SMARC database.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research is non-funded.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Azamar-Alonso A, Costa AP, Huebner L-A, Tarride J-E. Electronic referral systems in health care: a scoping review. Clinicoecon Outcomes Res. 2019;325–333. doi:10.2147/CEOR.S195597
2. Bichel A, Erfle S, Wiebe V, Axelrod D, Conly J. Improving patient access to medical services: preventing the patient from being lost in translation. Healthc Q. 2009;13:61–68. doi:10.12927/hcq.2009.21100
3. Heimly V. Electronic referrals in healthcare: a review. Med Inf Unit Health Europ. 2009;327–331.
4. Liddy C, Hogel M, Blazkho V, Keely E. The current state of electronic consultation and electronic referral systems in Canada: an environmental scan. Global Telehealth. 2015;75–83.
5. Protti D, Johansen I. Further lessons from Denmark about computer systems in physician offices. Electronic Healthcare. 2003;2(2):36–43.
6. Heimly V. Electronic referrals in the health sector in Norway, challenges on the road from standard to high volume use. 2010 International Symposium on Collaborative Technologies and Systems. IEEE; 2010.
7. Alnassar A, Aljerian N, Alhosaini A, et al. Trends of referrals throughout the kingdom, a retrospective analysis of the Saudi medical appointments and referrals centre registry, Saudi Arabia. Int j Innov Res Med Sci. 2022;7(11):563–578. doi:10.23958/ijirms/vol07-i11/1517
8. Aljerian N, Alharbi A, Alharbi IVAA. Assessing medical emergency e-referral request acceptance patterns and trends: a comprehensive analysis of secondary data from the kingdom of Saudi Arabia. Cureus. 2024;16(2). doi:10.7759/cureus.53511
9. Co-operation OfE, Development. Geographic Variations in Health Care: What Do We Know and What Can Be Done to Improve Health System Performance? OECD Publishing; 2014.
10. Corallo AN, Croxford R, Goodman DC, Bryan EL, Srivastava D, Stukel TA. A systematic review of medical practice variation in OECD countries. Health Policy. 2014;114(1):5–14. doi:10.1016/j.healthpol.2013.08.002
11. WHO. Management of health facilities: referral systems. World Health Organization. 2014.
12. Ministry of Health. MOH manifests patient’s referral mechanism; 2013Available from: https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/news-2013-11-11-002.aspx. (
13. Merlo A, Khoury A, Shah M, et al. Temporal trends in internal vs. external referrals for TAVR in a large academic center: patients characteristics and outcomes. J Interv Cardiol. 2022;2022:1–6. doi:10.1155/2022/6074368
14. Porter M, Malaty J, Michaudet C, Blanc P, Shuster JJ, Carek PJ. Outpatient referral rates in family medicine. Am J Account Care. 2018;6(1):25–28.
15. Safi M, Clay-Williams R, Thude BR, Vaisman J, Brandt F. Today’s referral is tomorrow’s repeat patient: referrals to and between medical outpatient clinics in a hospital. BMC Health Serv Res. 2022;22(1):254. doi:10.1186/s12913-022-07633-y
16. Wright JR, Madhusudhan DK, Lawrence DC, et al. Costs of specialist referrals from employer-sponsored integrated health care clinics are lower than those from community providers. J Gen Intern Med. 2022;37(15):3861–3868. doi:10.1007/s11606-022-07724-w
17. Hurst SA. World medical association declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
18. Alharbi AA, Alqassim AY, Alharbi AA, et al. Variations in length of stay of inpatients with COVID-19: a nationwide test of the new model of care under vision 2030 in Saudi Arabia. Saudi J Biol Sci. 2021;28(11):6631–6638. doi:10.1016/j.sjbs.2021.07.040
19. StataCorp. Stata Statistical Software: Release 16. College Station, TX: StataCorp LLC; 2019.
20. Nicholson C, Jackson CL, Wright B, et al. Online referral and OPD booking from the GP desktop. Aust Health Rev. 2006;30(3):397–404. doi:10.1071/AH060397
21. Hysong SJ, Esquivel A, Sittig DF, et al. Towards successful coordination of electronic health record based-referrals: a qualitative analysis. Implement Sci. 2011;6(1):1–12. doi:10.1186/1748-5908-6-84
22. Shaw LJ, de Berker DA. Strengths and weaknesses of electronic referral: comparison of data content and clinical value of electronic and paper referrals in dermatology. Br J Gen Pract. 2007;57(536):223–224.
23. Cannaby S, Westcott D, Pedersen CD, Voss H, Wanscher CE. The cost benefit of electronic patient referrals in Denmark: summary report. Stud Health Technol Inform. 2004;100:238–245.
24. Heimly V. Collaboration across organizational boarders, the referral case. In: Information Technology in Health Care: Socio-Technical Approaches. IOS Press; 2010:p106–11.
25. Saudi Census. Population in broad age groups; 2022Available from: https://portal.saudicensus.sa/portal/public/1/15/100646?type=TABLE.
26. Alzahrani MS, Alharthi YS, Aljamal JK, Alarfaj AA, Vennu V, Noweir MD. National and regional rates of chronic diseases and all-cause mortality in Saudi Arabia-analysis of the 2018 household health survey data. Int J Environ Res Public Health. 2023;20(7):5254. doi:10.3390/ijerph20075254
27. Hazazi A, Wilson A. Noncommunicable diseases and health system responses in Saudi Arabia: focus on policies and strategies. A qualitative study. Health Res Policy Sys. 2022;20(1):63. doi:10.1186/s12961-022-00872-9
28. King MA, Matos RI, Hamele MT, et al. PICU in the MICU: how adult ICUs can support pediatric care in public health emergencies. Chest. 2022;161(5):1297–1305. doi:10.1016/j.chest.2021.12.648
29. Kanter RK. Regional variation in child mortality at hospitals lacking a pediatric intensive care unit. Crit Care Med. 2002;30(1):94–99. doi:10.1097/00003246-200201000-00015
30. White JR, Pollack MM. Easy access to pediatric intensive care unit care: an urban legend? Crit Care Med. 2002;30(1):256–257. doi:10.1097/00003246-200201000-00044
31. Goh AY, Mok Q. Centralization of paediatric intensive care: are critically ill children appropriately referred to a regional centre? Intensive Care Med. 2001;27:730–735. doi:10.1007/s001340000820
32. Frankel LR, Hsu BS, Yeh TS, et al. Criteria for critical care infants and children: PICU admission, discharge, and triage practice statement and levels of care guidance. Pediatr Crit Care Med. 2019;20(9):847–887. doi:10.1097/PCC.0000000000001963
33. Singh S, Doyle P, Campbell OM, Mathew M, Murthy G, Ho Y-S. Referrals between public sector health institutions for women with obstetric high risk, complications, or emergencies in India–A systematic review. PLoS One. 2016;11(8):e0159793. doi:10.1371/journal.pone.0159793
34. Ameyaw EK, Njue C, Tran NT, Dawson A. Quality and women’s satisfaction with maternal referral practices in sub-Saharan African low and lower-middle income countries: a systematic review. BMC Pregnancy Childbirth. 2020;20:1–16. doi:10.1186/s12884-020-03339-3
35. Saudi Census. Population by Nationality. 2022 [Available from: https://portal.saudicensus.sa/portal/public/1/15/100643?type=TABLE.
36. Walston S, Al-Harbi Y, Al-Omar B. The changing face of healthcare in Saudi Arabia. Ann Saudi Med. 2008;28(4):243–250. doi:10.5144/0256-4947.2008.243
37. Ministry of Health KoSA. Statistical Yearbook 2021 [Available from: https://www.moh.gov.sa/en/Ministry/Statistics/book/Pages/default.aspx.
38. Alharbi AA, Alqassim AY, Muaddi MA, Alghamdi SS. Regional differences in COVID-19 mortality rates in the Kingdom of Saudi Arabia: a simulation of the new model of care. Cureus. 2021;13(12).
39. Alharbi AA, Alqassim AY, Muaddi MA, et al. Regional differences in COVID-19 mortality rates in the kingdom of Saudi Arabia: a simulation of the new model of care. Cureus. 2021;13(12).
40. U.S Food & Drug Administration. Medical device shortages list; 2023[updated 07/14/2023. Available from: https://www.fda.gov/medical-devices/medical-device-supply-chain-and-shortages/medical-device-shortages-list#shortage.
41. Chaudhary P, Kaul P. Factors affecting utilization of medical diagnostic equipment: a study at a tertiary healthcare setup of Chandigarh. chrismed J Health Res. 2015;2(4).
42. Organization WH. Medical Equipment Maintenance Programme Overview; 2011.
43. Weissman C, Avidan A, Tandeter H, Zisk Rony RY. Unpopular medical specialties: exploring the concept that “the customer knows best”. BMC Med Educ. 2023;23(1):1–9. doi:10.1186/s12909-023-04241-0
44. Zhang X, Lin D, Pforsich H, Lin VW. Physician workforce in the United States of America: forecasting nationwide shortages. Human Resources for Health. 2020;18(1):1–9. doi:10.1186/s12960-020-0448-3
45. Health UDo, Services H. State-Level Projections of Supply and Demand for Primary Care Practitioners: 2013-2025. Rockville, MD: National Center for Health Workforce Analysis; 2016.
46. Oslock WM, Satiani B, Way DP, et al. A contemporary reassessment of the US surgical workforce through 2050 predicts continued shortages and increased productivity demands. Am J Surg. 2022;223(1):28–35. doi:10.1016/j.amjsurg.2021.07.033
47. Barbosa W, Zhou K, Waddell E, Myers T, Dorsey ER. Improving access to care: telemedicine across medical domains. Ann Rev Public Health. 2021;42:463–481. doi:10.1146/annurev-publhealth-090519-093711
48. Haleem A, Javaid M, Singh RP, Suman R. Telemedicine for healthcare: capabilities, features, barriers, and applications. Sens Int. 2021;2:100117. doi:10.1016/j.sintl.2021.100117
49. Ministry of Health. Seha Virtual Hospital 2023 [updated 24/07/2023. Available from: https://www.moh.gov.sa/en/Ministry/Projects/Pages/Seha-Virtual-Hospital.aspx.
50. Platt JL, Cascalho M. New and old technologies for organ replacement. Curr Opin Organ Tran. 2013;18(2):179. doi:10.1097/MOT.0b013e32835f0887
51. Al Sebayel M, Abaalkhail F, Al Abbad S, et al. Liver transplantation in the kingdom of Saudi Arabia. Liver Transpl. 2017;23(10):1312–1317. doi:10.1002/lt.24803
52. Bogomazova I. On the Implementation of the WHO guiding principles on human cell, tissue and organ transplantation. Medicne pravo. 2022;1(29):9–18. doi:10.25040/medicallaw2022.01.009
53. David W As the need for organ transplants grows, the number of transplant physicians dwindles; 2019[Available from: https://www.statnews.com/2019/10/17/transplant-physicians-number-dwindling/.
54. AlSulaiman NS, Alassaf MA, Boumarah DN, Almubireek AM, Alkaltham GK, Menezes RG. Organ transplantation in Arabian Gulf countries: ethical and legal practice and beyond. Forensic Sci Med Pathol. 2021;17(4):670–678. doi:10.1007/s12024-021-00398-6
55. Woo YL, Kyrgiou M, Bryant A, Everett T, Dickinson HO. Centralisation of services for gynaecological cancers—a Cochrane systematic review. Gynecologic Oncol. 2012;126(2):286–290. doi:10.1016/j.ygyno.2012.04.012
56. Keating NL, Jhatakia S, Brooks GA, et al. Association of participation in the oncology care model with medicare payments, utilization, care delivery, and quality outcomes. JAMA. 2021;326(18):1829–1839. doi:10.1001/jama.2021.17642
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.