")
Back to Journals » Patient Preference and Adherence » Volume 18
Expert Insight Into the Use of eHealth Interventions to Aid Medication Adherence During COVID-19
Received 30 August 2023
Accepted for publication 13 March 2024
Published 21 March 2024 Volume 2024:18 Pages 721—731
DOI https://doi.org/10.2147/PPA.S437822
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Ahmed Hassan,1 Non Davies2
1School of Medicine, Cardiff University, Cardiff, Wales; 2North Wales Medical School, Bangor University, Bangor, Wales
Correspondence: Ahmed Hassan, North Wales Medical School, Brigantia Building, Penrallt Road, Bangor, Gwynedd, LL57 2AS, Wales, Tel +447459044808, Email [email protected]
Background and Aim: The COVID-19 pandemic has transformed the way healthcare is delivered by the increased utilisation of eHealth tools to deliver remote patient consultations. These eHealth tools served various functions during COVID-19 including monitoring and surveillance of patients. Therefore, assessment of digital health interventions for monitoring medication adherence is crucial to maximise the potential benefits of eHealth. The aim of this study is to understand the perspectives of experts in medication adherence around eHealth interventions used to aid adherence during COVID-19.
Methods: The study was exploratory and utilized a mixed-method approach. Data was gathered from a survey distributed by the International society for Medication Adherence, and from arranging subsequent structured interviews. Purposive sampling was used to collect data from individuals who were rich in knowledge about the field of medication adherence. Template analysis was used to analyse the collected data.
Results: Twenty-one participants responded to the survey and 6 completed the interviews. Results showed that eHealth tools reduced barriers to medication adherence by improving health literacy of patients. The main strengths of eHealth technology used in COVID-19 highlighted by participants were convenience and user empowerment. Moreover, weaknesses and barriers included lack of cooperation between technology providers, lack of awareness of doctors about eHealth and patient’s digital health literacy.
Conclusion and Future Directions: The increased utility of eHealth tools during COVID-19 highlighted their vital role in aiding medication adherence of patients. These technologies have both decreased and increased barriers to medication adherence through numerous ways. Future directions should focus on gaining the perspectives of patients on the use of eHealth interventions and its role in aiding medication adherence.
Keywords: healthcare, telemedicine, digital technology, assessment, perspectives
Introduction
Medication Adherence and Its Impact
Medication adherence is defined by Virjens et al as “the process by which patients take their medications as prescribed”, with the key components of this being initiation, implementation, and discontinuation.1 Lack of medication adherence can have dramatic health consequences on the individual patient and even wider economic loss to the healthcare system and society.2 Failure to adhere to prescribed drug regimens results in wastage of medicines and can lead to poor patient outcomes.3 It is estimated that 30–50% of patients taking medicine for chronic medications discontinue their prescribed medicine, costing England £300 million annually on wasted medicines.4 There are also resultant costs of avoidable illness, hospital admissions, increased number of sick days and decreased productivity which is damaging to the overall economy.4 Overall, worldwide, the non-adherence to medication is approximated to waste $100 billion in preventable medical costs and cause 125,000 preventable deaths per year.5
Digital Health (eHealth) Interventions
Digital healthcare technology can be defined as the healthcare services and health information provided using the internet, computers, mobile devices and information technology to facilitate healthcare delivery and improve quality of life.6 Digital health interventions are categorised by El Benny et al into those that are mobile-based, web-based, telehealth interventions, as well as electronic health records.7 Digital health interventions aiming to support individuals in adhering to their medications often incorporate key elements into their design, such as electronic medication-intake reminders, patient educational material, and patient feedback.8 Other, more novel, digital health interventions aiming to support individuals in adhering to their medications may include the use of artificial intelligence (AI), with AI-based chatbots that are able to provide tailored patient support growing in popularity.9
Numerous studies in the literature highlight the favorable outcomes associated with using digital health interventions to assist patients in adherence to their medication regimens. For instance, a study by Márquez Contreras et al described using the AlerHTA smartphone app to improve participant hypertension control through electronic reminders and educational material.10 Positive results were reported, which included improved adherence to hypertensive medication.10 Similarly, a study by Senoo et al described using the SmartAF app to improve adherence to anticoagulant therapy in elderly participants with atrial fibrillation.11 The app supported participants through electronic reminders and patient engagement, with the study reporting improved adherence to anticoagulant therapy.11
Whilst advantages of using smartphone apps to improve medication adherence include the extensive range of available features and the ability to be implemented in a wide range of settings, limitations might include the exclusion of those who do not own a smartphone, the knowledge and skill of individuals, as well as issues regarding data security.12,13
COVID-19 and eHealth
During the COVID-19 pandemic, patients with chronic conditions became distanced from healthcare due to the unmet clinical demands on healthcare professionals and resources.14,15 In addition, the COVID-19 pandemic has transformed the way that healthcare is delivered by the increased utilisation of eHealth technologies, such as to deliver remote patient consultations.15 Other examples include the use of eHealth technologies during COVID-19, such as apps and virtual reality, to promote physical activity,16,17 or for behaviour management.18
Statement of the Study
The impact of COVID-19 pandemic on medication adherence and the eHealth tools used to tackle this issue warrant further research.19,20 One systematic review aiming to determine the evolution of digital health technologies used in primary care during the COVID-19 pandemic showed that “monitoring and surveillance” was one of the main purposes of using eHealth during this period.21 Hence, assessment of digital health interventions for monitoring medication adherence is crucial to maximise the potential benefits of eHealth.
The aim of this research is to understand the perspectives of experts in medication adherence in relation to assessing eHealth interventions used to improve medication adherence during the COVID-19 pandemic. This will be achieved by analysing a survey distributed by the International Society for Medication Adherence (www.ESPACOMP.eu) to medication adherence experts and arranging subsequent structured interviews, which are the objectives of this research.
The main research questions included i) what are the digital resources available to aid medication adherence during COVID-19? ii) their functionalities, iii) their strengths and weaknesses, iv) how do they increase/decrease barriers to adherence? v) what is the effect of COVID-19 on adherence?
Materials and Methods
Study Design
The study was exploratory and utilized the mixed-method approach to analyze the primary and secondary data.22 The secondary data was collected from a whole survey carried out by the International Society for Medication Adherence (ESPACOMP), and the primary data was collected from interviews with a sub-sample of survey respondents who agreed to attend a follow-up interview. The timing of the mixed-method research components can be described according to simultaneity and dependence.23 The two components of this study had a sequential design, as the survey data were collected before conducting the interviews. In addition, the two components were dependent, as the interview questions depended on the outcome of analysis of the survey data.
Furthermore, there was integration of the survey and interview components through the “methods” and “interpretation and reporting levels” of research.24 In the “methods” level, there was integration through connecting and building approaches.24 The connecting approach meant that the databases of the survey and interview were linked through sampling, as participants for the interview were a sub-sample of respondents from the survey.24 The building approach meant that the data collection of the survey informed the data collection of interviews, with the latter component building on the former.24 In the “interpretation and reporting” level, a narrative contiguous approach was utilised in which the analysed data from the two components were reported in a single report but in different sections.24
Overall, the purpose of mixed-method research approach in this study was complementarity to allow elaboration, enhancement, illustration, and clarification of the survey results with the results from the interviews to examine the research questions.22
Participants
This study employed a purposive sampling technique to collect primary data from individuals who were rich in knowledge about the field of medication adherence. This is widely used in qualitative research to identify and select information-rich subjects for most effective use of limited resources.25
Eligibility for the Participation in the Interview
The study utilized the following criteria for participation in the interview:
- Experience in the field of medication adherence during COVID-19
- To be a member of ESPACOMP
- Answered the survey circulated from ESPACOMP
- Provided consent to be contacted for a follow-up interview
Survey
ESPACOMP administered a survey in September 2021 asking 2400 ESPACOMP members prior to an annual international conference, held on 8–19th of November 2021, about their experience with eHealth technologies available for use during COVID-19. This society is an interprofessional association that aims to understand the reasons for medication non-adherence and to develop interventions supporting medication adherence. The survey included 5 open-ended and 2 closed-ended questions that aimed to assess eHealth interventions used for medication adherence during COVID-19 and to assist in the planning of an interprofessional roundtable at the ESPACOMP conference (Box 1). The questions in this survey assessed the members’ awareness of the available technologies, their effectiveness, and what barriers they might introduce in relation to medication adherence. In addition, the survey invited respondents to provide their contact details for a follow-up structured interview.
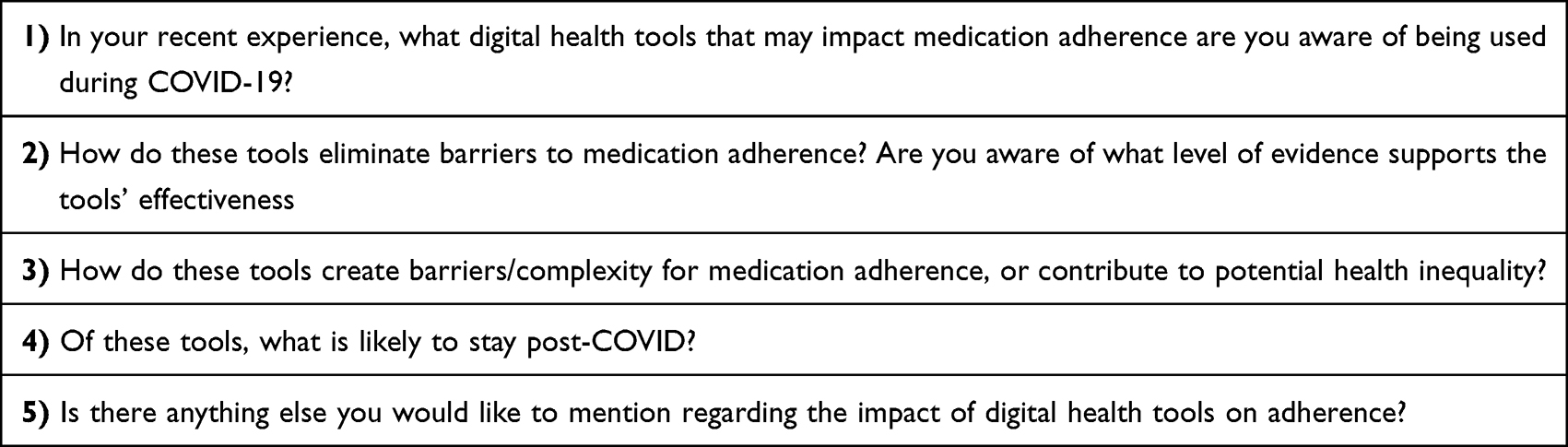 |
Box 1 Survey Sent to ESPACOMP Members to Investigate the eHealth Interventions Used to Aid Medication Adherence During COVID-19 |
Interview
Survey respondents who consented to be re-contacted were invited to a Microsoft Teams meeting with the researcher. Structured interviews included 4 closed- and 6 open-ended questions (Box 2). The closed questions gathered the job title, location, gender and years of experience in the field of medication adherence for the interviewees. The open-ended questions allowed discussions about digital health tools used during COVID-19, the functions available within these technologies, and how COVID-19 may have affected medication adherence based on evidence/anecdote/experience. In addition, a novel topic of medication adherence in the context of COVID-19 non-vaccine treatment was discussed.
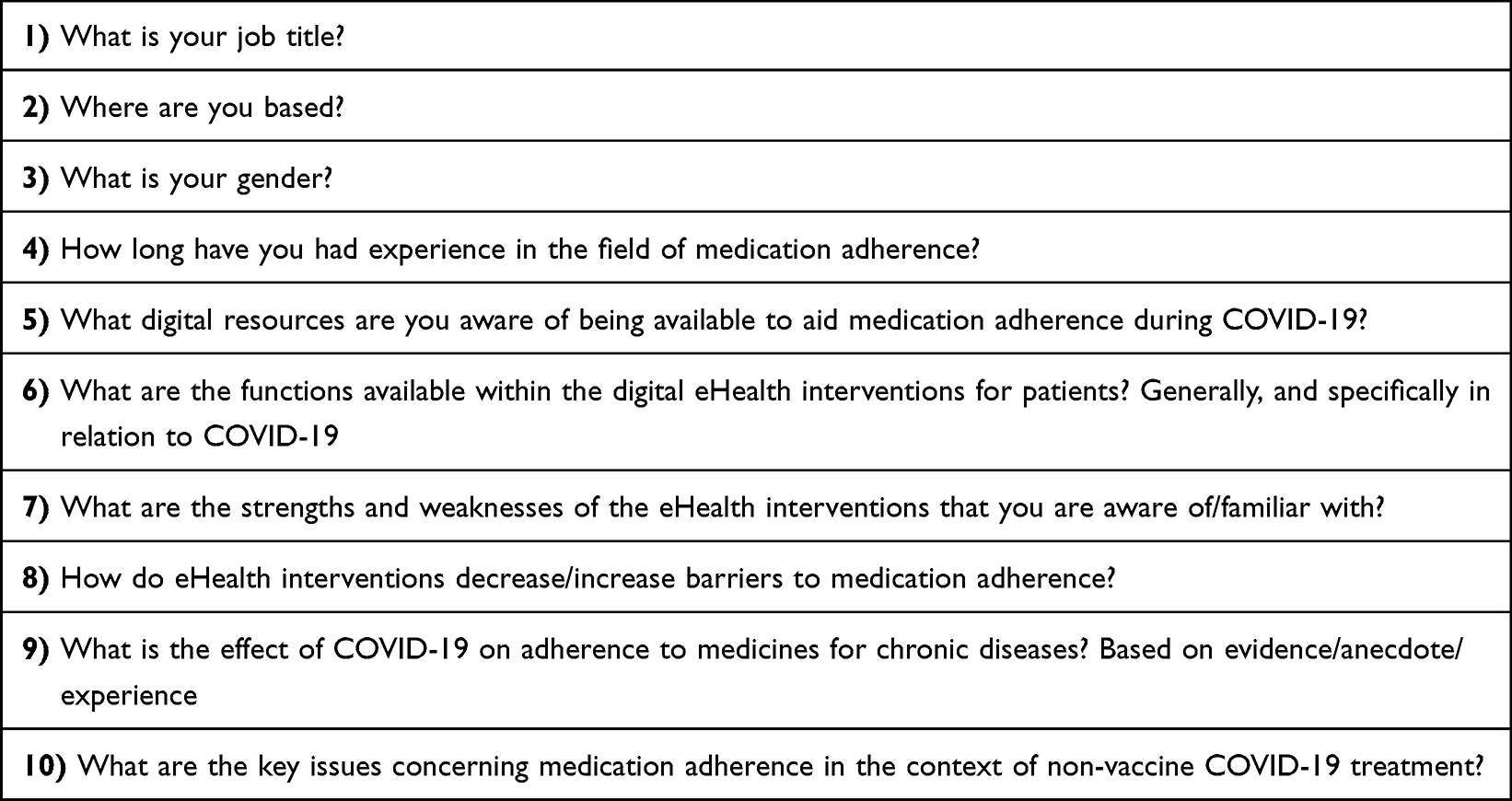 |
Box 2 Layout of the Structured Interview |
Survey and Interview Development
The draft survey was reviewed by two content experts for content assessment and validity, by considering any edits or suggestions. These experts were working and had expertise in the area of medication adherence.
A combination of closed, fixed response and standardised open-ended interview approaches were used in the development of the structured interview questions.26 The questions were developed using an iterative process between the medical student and an expert in the area of medication adherence. A pre-testing of the interview questions was conducted on one key informant in the study area. Following pre-testing, some questions were re-designed, added or removed in the final interview question template. During the interview, the quality of data collected was checked using the member checking method. This involves debriefing the analytical results with participants for agreement.27
Data Analysis
The responses to the survey were thematically analysed using NVivo12 software. The interview audio recordings were transcribed and thematically analysed using template analysis.28 This is a form of thematic analysis which emphasises the use of hierarchical coding in which broader themes derived encompass narrower subthemes. It is based upon a priori themes (themes determined before coding) and offers flexibility by allowing adaptation of themes for the needs of the study.28
In this study, a list of pre-defined themes was gathered from responses of the ESPACOMP survey. The list of themes was subject to further addition, removal or adjustment depending on the themes encountered with the same participants during the interview.28 The recorded audio of the interview was transcribed using NVivo12 software. The audio transcripts were coded; this meant that the themes identified in the transcripts were given a label from the pre-defined themes to index them.28 An initial template was produced after a sub-set of transcripts are coded.28 Once all transcripts were coded, a final template was produced to interpret and write up the findings.28
Consent and Anonymization
Participants were provided with an information sheet and a consent form which were sent 2 weeks before the proposed interview date to allow enough time to make an informed decision. The participants also consented to the publication of anonymized responses. Identifiable information in audio recordings was removed during qualitative analysis.
Ethical Approval
Ethical approval was granted by the School of Medicine Research Ethics Committee of Cardiff University. SREC reference: SMREC 21/92
Results
Survey
Twenty-one people responded to the survey. The themes and sub-themes identified in the survey are summarised in Table 1.
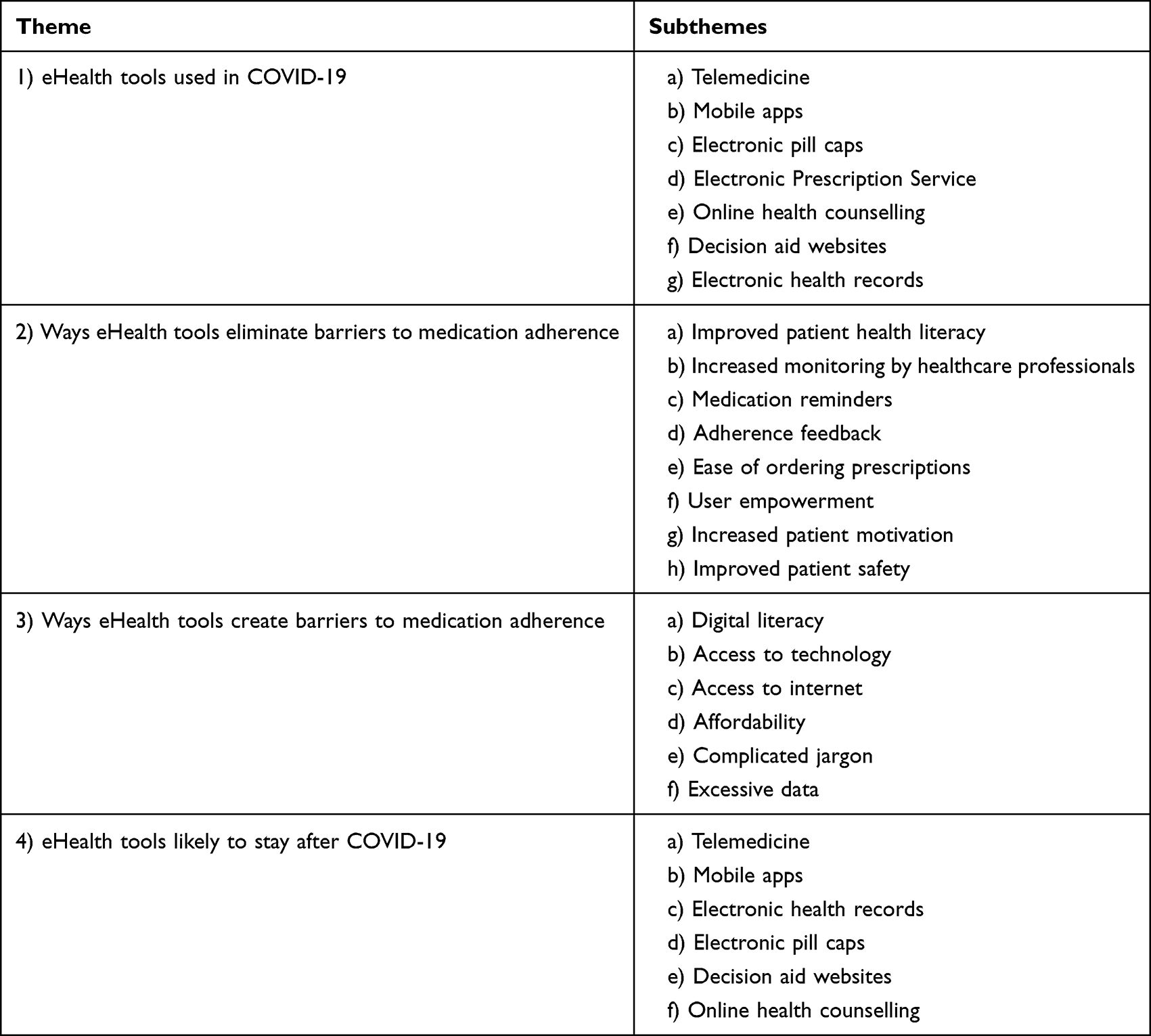 |
Table 1 Assessment of eHealth Interventions Used for Medication Adherence During COVID-19, Gathered from Survey |
eHealth Tools Used During COVID-19 That May Impact Medication Adherence
Respondents were aware of a range of eHealth technologies, covering applications of telemedicine, mobile apps and electronic pill caps (MEMS). Others included electronic prescription service (EPS), online health counselling and decision aid websites (Table 1). Eight out of 21 respondents reported telemedicine as being used during COVID-19. For example, one mentioned in the survey:
We have been using secure teleconsultation platforms since the first confinement when dispensing medicines available in the hospital.
In addition, 7/21 of respondents stated mobile apps and others mentioned electronic health records (EHR), such as EPIC platform. Also, MEMS were used and sometimes linked to EHR to provide medication adherence information, as one stated:
I am not using them, but electronic pill caps can likely also be synched with EHR as part of remote monitoring programs.
Ways eHealth Tools Eliminate Barriers to Medication Adherence, and Their Effectiveness
Respondents believed that eHealth technologies improved medication adherence through a variety of ways including improved patient health literacy, increased monitoring by healthcare professionals, increased patient motivation and easier access to medications. Other ways included ease of ordering prescriptions, providing medication reminders and adherence feedback for patients which may contribute to empowering the user and increase patient motivation (Table 1). One participant commented in the survey on the effectiveness of decision aid website, stating that it was unclear:
I’m aware of the level of the evidence available about decision aids, effectiveness is unclear at this point and more research needs to be done.
Ways eHealth Tools Create Barriers to Medication Adherence
The greatest reported barrier, mentioned by 12, was the digital literacy of patients. Other barriers included access to internet and technology, affordability, complexity and excessive data (Table 1). One respondent summarised the views of many in the survey:
Availability of digital tools is better in richer countries. Richer, higher-educated and younger patients use more often support tools/ digital tools… but sometimes not to other patients e.g. elderly.
eHealth Tools Likely to Stay Post-COVID
EHR, MEMS, online counselling and use of websites were each supported by 1 respondent, while mobile apps and telemedicine were supported by 6 (Table 1).
Interview
Overall, out of the 21 respondents of the survey, 14 provided their contact details to be contacted for a follow-up interview. These fourteen subjects were contacted, and 6 people completed the interview. One person declined the invitation, and others did not respond despite reminders. The sample consisted of 3 females and 3 males, with experience in medication adherence ranging from 2 to 21 years. This included 2 PhD candidates undergoing research in development and validation of medication adherence, a psychologist working as project manager for the digitalization of the electronic records, a pharmacist, an associate professor of medicine, and a CEO of a drug adherence solution company. They were based in Brazil, Colombia, Denmark, Italy, Netherlands and Switzerland. The duration of the interview was between 30 mins and 73 min (mean: 49 min). The data obtained was explored around 6 a priori major themes including (i) eHealth functionalities, (ii) strengths, (iii) weaknesses, (iv) barriers to adherence using eHealth, (v) effect of COVID-19 on adherence, (vi) non-vaccine COVID-19 treatment adherence issues. These were further divided into sub-themes after coding as shown in Table 2.
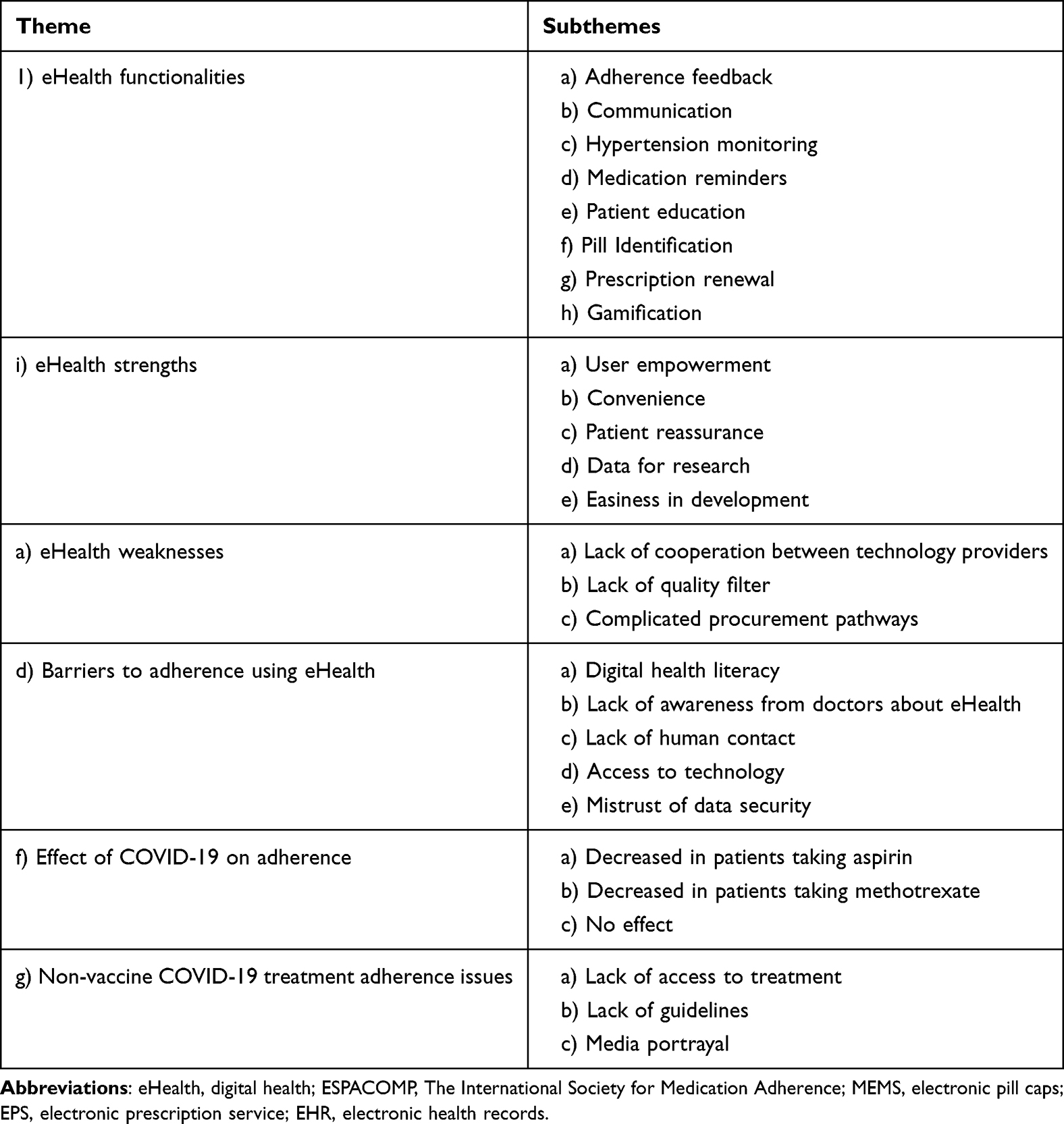 |
Table 2 Assessment of eHealth Interventions Used for Medication Adherence During COVID-19, Gathered from Interviews |
eHealth Functionalities
The reported main functionalities of eHealth included providing adherence feedback, communication between patients and healthcare professionals, hypertension monitoring, medication reminders, patient education, pill identification, prescription renewal and gamification (Table 2).
eHealth Strengths
The strengths discussed by the interviewees were user empowerment, convenience and patient reassurance. The other strengths were more specific for healthcare professionals which included providing data for research, and the relative easiness in development of technology (Table 2). One interviewee mentioned:
It’s in the patients’ hands, so the patient is the one who actually decides and has the all the power and all the information.
eHealth Weaknesses
A main weakness provided by 4/6 interviewees was the lack of cooperation between technology providers. Other weaknesses included the lack of quality filter and complicated procurement pathways (Table 2). One interviewee summarised the view of many:
Each organisation, so each pharmacy, each hospital, each general practitioner will have its own platform or app, or web based… there is a multitude and there’s not a lot of cooperation.
Barriers to Adherence Using eHealth
The main barrier stated by all interviewees is digital health literacy of patients. This was followed by the lack of awareness from doctors about the eHealth tools available, mentioned by 3 subjects. Other barriers stated were lack of human contact, access to technology and mistrust of data security (Table 2). An interviewee mentioned:
They are built for by highly educated people, but the average patient is a low educated person.
Moreover, a psychologist stated:
Human life needs humans. And so, in my opinion, whatever way in this this modern world could be invented to increase patients’ adherence must always be supported by a human being.
Effect of COVID-19 on Adherence
Three participants stated that COVID-19 has caused a lower medication adherence. Reasons included lack of access to medication and lack of attention from healthcare services. One participant stated that adherence was reduced in a specific patient group taking aspirin due to the belief that anti-inflammatory tablets led to worse outcomes in COVID-19 patients. In addition, another interviewee mentioned reduced adherence of methotrexate among patients due to concerns about its effect on COVID-19. Moreover, 1 participant stated that there was no effect in their country Switzerland, and 2 did not know (Table 2).
Non-Vaccine COVID-19 Treatment Adherence Issues
All participants did not know any specific adherence issues relating to this topic. Three participants highlighted other issues not directly related to adherence such as lack of access to such medications and lack of guidelines. One participant emphasised that media portrayal will be of high importance for adherence (Table 2).
Discussion
This study assessed eHealth interventions used during COVID-19 that may impact medication adherence. The results showed that eHealth reduces barriers to medication adherence by enhancing patient education and improving health literacy. However, factors such as digital literacy of patients, lack of awareness from doctors, access to internet and technology create barriers to eHealth and contribute to health inequality.
The interview results have shed more light on the strengths and weaknesses of such eHealth tools. Strengths included user empowerment and convenience for patients as it is easier and faster to get in contact with a healthcare professional through a chat function or video call. The greatest weakness was the lack of cooperation between technology providers which results in duplication of efforts between them. More importantly, this also means that in countries where healthcare is not centralised, the different healthcare providers of the same patient are unable to see patient’s medical information from the different eHealth platforms.
A strength of this study was that a large, international community of experts in medication adherence was approached. Limitations include the small sample size from both the survey and interview participants representing less than 1% of survey recipients, which limits the generalisability of results. In addition, there was no opportunity to test for the reliability of survey questions by calculating the intraclass correlation coefficient.
The barrier to digital health literacy can be regarded as a convergence of digital literacy and health literacy.29 According to systemic review to integrate definitions, health literacy can also be grouped into 4 dimensions including accessing, understanding, appraising and applying health information to decide to maintain and improve health.30 Sorensen et al reported that almost 50% of European population have limited health literacy according to a survey carried out.31 The limited health literacy was more common in groups of social deprivation, low social status, low education and old age.31 More patient education needs to be considered to address the digital and health literacy.
The reported reduction of medication adherence of aspirin during COVID-19 in this study due to concerns among patients is contradictory to the limited literature data on aspirin adherence during COVID-19. One study has found no change in adherence of aspirin in 166 patients with chronic coronary syndromes.32 However, this data was obtained 4 weeks after the French lockdown with a relatively small sample size and does not reflect what happened in other parts of the world. Several studies have shown no association between NSAID use and worse outcomes for COVID-19 patients.33,34 In fact, some studies have shown beneficial effect of aspirin by reducing infection risk and mortality of COVID-19.35
Moreover, in this study, the reported reduced medication adherence of rheumatology patients taking methotrexate due to concerns about its effect on COVID-19 is supported by another research study. This showed 14% of patients with rheumatic disease decreasing or stopping their antimetabolite medication which includes methotrexate.36 Moreover, further studies have highlighted a reduction of medication adherence during COVID-19 across various conditions such as epilepsy and glaucoma.37,38 A systematic review by Olmastroni et al assessed the impact of COVID-19 on medication adherence of many chronic conditions such as inflammatory bowel disease, COPD, osteoporosis, psoriasis and others.39 Overall, they showed that adherence to the chronic therapies were reduced during COVID-19; some examples included biologics, controller inhalers and denosumab injections. Reasons for decreased adherence were difficulty in reaching physicians, fear of infection and unavailability of medications.39 They also showed that for some therapies, where patients were not required to attend the clinic, the use of telemedicine was crucial to ensure continuity of treatment.39 More research on medication adherence during COVID-19 is warranted across other chronic medical conditions.19
Conclusion
Assessing the eHealth technologies used during COVID-19 to aid medication adherence is crucial to improving healthcare accessibility and public health. The survey complemented by the structured interview results highlighted how eHealth decreased or increased barriers to medication adherence during COVID-19. Factors such as improving health literacy decreased the barriers to medication adherence, whereas the main barrier to adherence was the digital literacy of patients followed by the lack of awareness from doctors about eHealth. Moreover, convenience for patients was an attractive feature of using eHealth, but the lack of cooperation between technology providers literacy remained a challenge especially during the difficult times of COVID-19. The reported changes in medication adherence in specific pharmacotherapies including aspirin and methotrexate added further insight to the limited literature available. Overall, this study sheds light on the barriers, strengths and weaknesses of using eHealth to aid medication adherence during COVID-19. It also highlighted the need to increase awareness of eHealth tools among healthcare professionals and improving patient digital health literacy.
The limitations of the study included the relatively small sample size of participants, even though a large international community of experts in medication adherence was approached. Future research should focus on gaining the perspectives of patients on the use of different eHealth interventions and its role in aiding medication adherence.
Acknowledgments
Special thanks to Professor Dyfrig Hughes for supervising this project. Special thanks to ESCPACOMP for providing access to the survey results and allowing follow-up interviews with respondents after obtaining ethical approval.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Vrijens B, De Geest S, Hughes DA, et al. A new taxonomy for describing and defining adherence to medications. Br J Clin Pharmacol. 2012;73(5):691–705. doi:10.1111/j.1365-2125.2012.04167.x
2. Sokol MC, McGuigan KA, Verbrugge RR, Epstein RS. Impact of medication adherence on hospitalization risk and healthcare cost. Med Care. 2005;43(6):521–530. doi:10.1097/01.mlr.0000163641.86870.af
3. Du L, Cheng Z, Zhang Y, Li Y, Mei D. The impact of medication adherence on clinical outcomes of coronary artery disease: a meta-analysis. Eur J Prev Cardiol. 2017;24(9):962–970. doi:10.1177/2047487317695628
4. Trueman P, Lowson K, Blighe A, Meszaros A, Wright D, Glanville J. Evaluation of the Scale, Causes and Costs of Waste Medicines: Final Report. York and London: York Health Economics Consortium and The School of Pharmacy; University of London; 2010.
5. Kleinsinger F. The unmet challenge of medication nonadherence. Perm J. 2018;22(3):18–033. doi:10.7812/tpp/18-033
6. da Fonseca MH, Kovaleski F, Picinin CT, Pedroso B, Rubbo P. E-health practices and technologies: a systematic review from 2014 to 2019. Healthcare. 2021;9(9):1192. doi:10.3390/healthcare9091192
7. El Benny M, Kabakian-Khasholian T, El-Jardali F, Bardus M. Application of the eHealth literacy model in digital health interventions: scoping review. J Med Internet Res. 2021;23(6):e23473. doi:10.2196/23473
8. Chan A, De Simoni A, Wileman V, et al. Digital interventions to improve adherence to maintenance medication in asthma. Cochrane Database Syst Rev. 2022;6(6):Cd013030. doi:10.1002/14651858.CD013030.pub2
9. Aggarwal A, Tam CC, Wu D, Li X, Qiao S. Artificial intelligence-based chatbots for promoting health behavioral changes: systematic review. J Med Internet Res. 2023;25:e40789. doi:10.2196/40789
10. Márquez Contreras E, Márquez Rivero S, Rodríguez García E, et al. Specific hypertension smartphone application to improve medication adherence in hypertension: a cluster-randomized trial. Curr Med Res Opin. 2019;35(1):167–173. doi:10.1080/03007995.2018.1549026
11. Senoo K, Miki T, Ohkura T, et al. A smartphone app to improve oral anticoagulation adherence in patients with atrial fibrillation: prospective observational study. JMIR mHealth Uhealth. 2022;10(1):e30807. doi:10.2196/30807
12. Dayer L, Heldenbrand S, Anderson P, Gubbins PO, Martin BC. Smartphone medication adherence apps: potential benefits to patients and providers. J Am Pharm Assoc. 2013;53(2):172–181. doi:10.1331/JAPhA.2013.12202
13. Giebel GD, Speckemeier C, Abels C, et al. Problems and barriers related to the use of digital health applications: scoping review. J Med Internet Res. 2023;25:e43808. doi:10.2196/43808
14. Chudasama YV, Gillies CL, Zaccardi F, et al. Impact of COVID-19 on routine care for chronic diseases: a global survey of views from healthcare professionals. Diabetes Metab Syndr. 2020;14(5):965–967. doi:10.1016/j.dsx.2020.06.042
15. Mann DM, Chen J, Chunara R, Testa PA, Nov O. COVID-19 transforms health care through telemedicine: evidence from the field. J Am Med Inform Assoc. 2020;27(7):1132–1135. doi:10.1093/jamia/ocaa072
16. Fang P, Shi S, Menhas R, Laar RA, Saeed MM. Demographic characteristics and digital platforms for physical activity among the Chinese residents during the COVID-19 pandemic: a mediating analysis. J Multidiscip Healthc. 2022;15:515–529. doi:10.2147/jmdh.S354984
17. Liu R, Menhas R, Dai J, Saqib ZA, Peng X. Fitness apps, live streaming workout classes, and virtual reality fitness for physical activity during the COVID-19 lockdown: an Empirical Study. Front Public Health. 2022;10:852311. doi:10.3389/fpubh.2022.852311
18. Yang J, Menhas R, Dai J, et al. Virtual Reality Fitness (VRF) for behavior management during the COVID-19 pandemic: a mediation analysis approach. Psychol Res Behav Manag. 2022;15:171–182. doi:10.2147/prbm.S350666
19. Ruksakulpiwat S, Zhou W, Niyomyart A, Wang T, Kudlowitz A. How does the COVID-19 pandemic impact medication adherence of patients with chronic disease?: a systematic review. Chronic Illn. 2022;19(3):17423953221110151. doi:10.1177/17423953221110151
20. Getachew E, Adebeta T, Muzazu SGY, et al. Digital health in the era of COVID-19: reshaping the next generation of healthcare. Front Public Health. 2023;11:942703. doi:10.3389/fpubh.2023.942703
21. Ndayishimiye C, Lopes H, Middleton J. A systematic scoping review of digital health technologies during COVID-19: a new normal in primary health care delivery. Health Technol. 2023;13(2):273–284. doi:10.1007/s12553-023-00725-7
22. Schoonenboom J, Johnson RB. How to construct a mixed methods research design. Kolner Z Soz Sozpsychol. 2017;69(Suppl 2):107–131. doi:10.1007/s11577-017-0454-1
23. Guest G. Describing mixed methods research: an alternative to typologies. J Mixed Methods Res. 2013;7(2):141–151. doi:10.1177/1558689812461179
24. Fetters MD, Curry LA, Creswell JW. Achieving integration in mixed methods designs-principles and practices. Health Serv Res. 2013;48(6 Pt 2):2134–2156. doi:10.1111/1475-6773.12117
25. Palinkas LA, Horwitz SM, Green CA, Wisdom JP, Duan N, Hoagwood K. Purposeful sampling for qualitative data collection and analysis in mixed method implementation research. Adm Policy Ment Health. 2015;42(5):533–544. doi:10.1007/s10488-013-0528-y
26. Patton MQ. Qualitative Research & Evaluation Methods: Integrating Theory and Practice.
27. McGrath C, Palmgren PJ, Liljedahl M. Twelve tips for conducting qualitative research interviews. Med Teach. 2019;41(9):1002–1006. doi:10.1080/0142159x.2018.1497149
28. Brooks J, McCluskey S, Turley E, King N. The utility of template analysis in qualitative psychology research. Qual Res Psychol. 2015;12(2):202–222. doi:10.1080/14780887.2014.955224
29. van Kessel R, Wong BLH, Clemens T, Brand H. Digital health literacy as a super determinant of health: more than simply the sum of its parts. Internet Interv. 2022;27:100500. doi:10.1016/j.invent.2022.100500
30. Sørensen K, Van den Broucke S, Fullam J, et al. Health literacy and public health: a systematic review and integration of definitions and models. BMC Public Health. 2012;12:80. doi:10.1186/1471-2458-12-80
31. Sørensen K, Pelikan JM, Röthlin F, et al. Health literacy in Europe: comparative results of the European health literacy survey (HLS-EU). Eur J Public Health. 2015;25(6):1053–1058. doi:10.1093/eurpub/ckv043
32. Cransac-Miet A, Zeller M, Chagué F, et al. Impact of COVID-19 lockdown on lifestyle adherence in stay-at-home patients with chronic coronary syndromes: towards a time bomb. Int J Cardiol. 2021;323:285–287. doi:10.1016/j.ijcard.2020.08.094
33. Wong AY, MacKenna B, Morton CE, et al. Use of non-steroidal anti-inflammatory drugs and risk of death from COVID-19: an OpenSAFELY cohort analysis based on two cohorts. Ann Rheum Dis. 2021;80(7):943–951. doi:10.1136/annrheumdis-2020-219517
34. Abu Esba LC, Alqahtani RA, Thomas A, Shamas N, Alswaidan L, Mardawi G. Ibuprofen and NSAID use in COVID-19 infected patients is not associated with worse outcomes: a Prospective Cohort Study. Infect Dis Ther. 2021;10(1):253–268. doi:10.1007/s40121-020-00363-w
35. Merzon E, Green I, Vinker S, et al. The use of aspirin for primary prevention of cardiovascular disease is associated with a lower likelihood of COVID-19 infection. Febs j. 2021;288(17):5179–5189. doi:10.1111/febs.15784
36. Rosenbaum JT, Hamilton H, Choi D, Weisman MH, Reveille JD, Winthrop KL. Biologics, spondylitis and COVID-19. Ann Rheum Dis. 2020;79(12):1663–1665. doi:10.1136/annrheumdis-2020-217941
37. Menon S, Sander JW. Effects of the COVID-19 pandemic on medication adherence: in the case of antiseizure medications, A scoping review. Seizure. 2021;93:81–87. doi:10.1016/j.seizure.2021.10.009
38. Subathra GN, Rajendrababu SR, Senthilkumar VA, Mani I, Udayakumar B. Impact of COVID-19 on follow-up and medication adherence in patients with glaucoma in a tertiary eye care centre in south India. Indian J Ophthalmol. 2021;69(5):1264–1270. doi:10.4103/ijo.IJO_164_21
39. Olmastroni E, Galimberti F, Tragni E, Catapano AL, Casula M. Impact of COVID-19 pandemic on adherence to chronic therapies: a systematic review. Int J Environ Res Public Health. 2023;20(5):3825. doi:10.3390/ijerph20053825
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.