")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 20
Excess Mortality in Individuals with Autism Spectrum Disorder: A Population-Based Cohort Study
Authors Huang YH, Wu SI, Lee MJ , Chen YL , Yang YH , Kuo TY, Hung TH, Dewey ME, Stewart R, Chen VCH
Received 29 August 2023
Accepted for publication 29 January 2024
Published 8 February 2024 Volume 2024:20 Pages 247—255
DOI https://doi.org/10.2147/NDT.S437766
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yuping Ning
Yu-Hsin Huang,1,2,* Shu-I Wu,1,2 Min-Jing Lee,3– 5,* Yi-Lung Chen,6,7,* Yao-Hsu Yang,8,9 Ting-Yu Kuo,8 Tai-Hsin Hung,3,4 Michael E Dewey,10 Robert Stewart,11,12 Vincent Chin-Hung Chen3,4
1Department of Medicine, MacKay Medical College, New Taipei City, Taiwan; 2Department of Psychiatry, MacKay Memorial Hospital, Taipei City, Taiwan; 3Department of Psychiatry, Chang Gung Memorial Hospital, Chiayi Branch, Chiayi, Taiwan; 4School of Medicine, Chang Gung University, Taoyuan, Taiwan; 5Department of Psychiatry, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan; 6Department of Healthcare Administration, College of Medical and Health Science, Asia University, Taichung, Taiwan; 7Department of Psychology, College of Medical and Health Science, Asia University, Taichung, Taiwan; 8Health Information and Epidemiology Laboratory, Chang Gung Memorial Hospital, Chiayi Branch, Chiayi, Taiwan; 9Department of Traditional Chinese Medicine, Chang Gung Memorial Hospital, Chiayi Branch, Chiayi, Taiwan; 10Institute of Psychiatry, Psychology and Neuroscience, King’s College London, London, UK; 11Department of Psychological Medicine, Institute of Psychiatry, Psychology and Neuroscience, King’s College London, London, UK; 12South London and Maudsley National Health Services Foundation Trust, London, UK
*These authors contributed equally to this work
Correspondence: Vincent Chin-Hung Chen, Department of Psychiatry, Chang Gung Memorial Hospital, Chiayi Branch, Chiayi, Taiwan, Tel +886-5-3621000 ext2303, Fax +886-5-3622188, Email [email protected]
Purpose: Autism spectrum disorder (ASD) may be associated with increased mortality, but relevant findings have been inconsistent. The modifying effects of gender and intellectual disability on excess mortality in individuals with ASD are underexplored.
Patients and Methods: Using Taiwan’s National Health Insurance Research Database and the National Death Registry, this population-based cohort study selected the data of 75,946 patients with ASD (ASD cohort) and 75,946 age group-, gender-, and income-matched (1:1) patients without ASD (non-ASD cohort). Cox proportional hazards models were used to compare mortality rates between the cohorts, and stratified analyses were used to evaluate the influence of gender and intellectual disability on mortality risk.
Results: The ASD cohort had higher mortality rates for all causes of death than did the non-ASD cohort (adjusted hazard ratio 1.64, 95% confidence interval 1.54– 1.75). Comorbid intellectual disability was associated with an increased risk of mortality, and this association was stronger in female patients than in male patients. Moreover, when focusing on deaths from natural causes, we found a significantly higher odds ratio for mortality in the ASD population with ID compared to those without ID.
Conclusion: ASD is associated with increased mortality, especially among female individuals and those with intellectual disability.
Keywords: mortality, autism, population-based cohort study
Introduction
Autism spectrum disorder (ASD) comprises a set of heterogeneous neurodevelopmental conditions. The worldwide prevalence of ASD is approximately 1% and has steadily increased in the past decades.1 According to data collected by the Autism and Developmental Disabilities Monitoring Network that is funded by the US Centers for Disease Control and Prevention, approximately 1 in 36 children aged 8 years received an ASD diagnosis in 2020.2 ASD is characterized by difficulties in social communication, limited interests, and repetitive behavior, with its onset occurring in early childhood.3 ASD is also associated with long-standing general disadvantages in employment and education and difficulties regarding independent living, which result in lifelong functional impairments.4–6 Individuals with ASD usually have a higher comorbid disease burden and poorer physical or mental health than do those without ASD.7–9
Increasing evidence demonstrates that individuals with ASD have a higher risk of excess mortality than does the general population.10–14 However, a study involving 787,666 students aged 5–24 years in Scotland identified no differences in mortality between participants with ASD and those without ASD.15 A cohort study of Danish young adults reported that co-occurring ASD was not associated with additional mortality risk in individuals with neurological or mental disorders.16 Furthermore, studies investigating mortality associated with ASD have mainly been conducted in Western countries, and studies conducted in Asia are scarce.17
Studies investigating risk factors for excess mortality among individuals with ASD have demonstrated that the female gender, epilepsy, and comorbid medical disorders are associated with relatively high mortality rates.12,18,19 However, studies have reported inconsistent findings regarding the association between intellectual disability (ID) and mortality in ASD. For example, one long-term follow-up study reported no significant association between ID and mortality among individuals with ASD;12 by contrast, two other population-based studies have identified higher mortality rates in individuals with ASD who had ID than in those who did not have ID.14,19 Regarding gender, some studies have reported that the association between mortality and ASD is higher in females than in males.11,12,16,18–20 However, other studies found no difference in gender regarding ASD mortality.14,21 Therefore, we aim to survey these two factors to assess their impact on ASD-related mortality.
Previous studies may not have incorporated the income of the family into their research,11–14,19,22 although some considered it a confounding factor.23 A previous study showed that the mortality rate associated with ASD increased across all income classes.20 Another study found no difference in the income of the family concerning ASD mortality.21 Thus we decided to consider income class as a confounding factor. Individuals with ASD were found to have a high prevalence of comorbidities. In terms of psychiatric comorbidities among individuals with ASD, an umbrella review of systematic reviews and meta-analyses found that the comorbidity rates for depressive disorder ranged from 2.5% to 47.1%, while the comorbidity rates for attention-deficit hyperactivity disorder (ADHD) ranged from 25.7% to 65%.24 Previous studies have shown that individuals with ASD may experience higher mortality than general population due to mental and behavioral issues,19,25 epilepsy,12,18 and other medical conditions.10,11 Thus we decided to consider comorbidity as a confounding factor.
We conducted this population-based study to investigate whether mortality among individuals with ASD would increase after the consideration of potential confounders. We also examined the effects of gender and ID on the risk of mortality among these individuals.
Materials and Methods
Data Source
Taiwan’s National Health Insurance (NHI) program is a mandatory health insurance system that provides universal health-care coverage to the residents of Taiwan. Data from the NHI program are compiled in the National Health Insurance Research Database (NHIRD) for research purposes.26 For this study, we collected data on the following items from the NHIRD: age, gender, income, residential urbanization level, disease diagnoses (based on International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM] and International Classification of Diseases, Tenth Revision, [ICD-10] codes), hospitalizations, outpatient visits, emergency service use, and care receipts. Personal information from the NHIRD is anonymized and deidentified. We complied with the Taiwan National Health Insurance Administrations relevant data protection and privacy regulations.
ASD Cohort and Control Cohort Selection
The ASD cohort comprised patients who had received an NHIRD-recorded diagnosis of ASD (ICD-9-CM code 299 and ICD-10 code F84) on at least two occasions from psychiatrists or pediatricians in outpatient clinics or received such a diagnosis once during hospitalization between 2001 and 2017. The non-ASD cohort comprised patients without recorded ASD who were individually matched to the ASD cohort according to age group (0–5, 6–17, 18–64, and ≥65 years), gender, and low-income status at a 1:1 ratio. Both cohorts were followed-up until death or the end of the study (December 31, 2017).
Covariates
Covariates that were previously reported to be associated with ASD, including low-income status and comorbid physical or psychiatric diseases, were selected as mortality-influencing factors.12,14,18,19,22,25 Low-income status was defined using the Low-Income and Middle-Low-Income Households dataset. Comorbid physical and psychiatric diseases included depression (ICD-9-CM codes 296.2–296.3, 300.4, and 311 and ICD-10 codes F32–F34), ADHD (ICD-9-CM code 314 and ICD-10 code F90), ID (ICD-9-CM codes 317–319 and ICD-10 codes F70–F73, F78, and F79), hypertension (ICD-9-CM codes 401.0, 401.1, 401.9, 402–405, 437.2 and ICD-10 code I10), epilepsy (ICD-9-CM code 345 and ICD-10 code G40), and diabetes mellitus (DM; ICD-9-CM codes 249 and 250 and ICD-10 codes E10–E14).
Outcome
The outcome of interest was mortality. Relevant data on mortality were obtained through linkages to the National Death Registry that is managed by the Office of Statistics, Ministry of Health and Welfare, Taiwan. We further collected the causes of death from the database. The numbers of deaths due to natural causes (ie, illness) and unnatural cause (ie, suicide, accidents, homicides, and unspecified), were recorded.
Statistical Analysis
We used a chi-square test to compare descriptive statistics, namely, age, gender, low-income status, and comorbid diseases, between the ASD and non-ASD cohorts. Moreover, Cox proportional hazards models were used to compare mortality rates between the cohorts. The index date was defined as each patient’s birth date. Results are presented as crude hazard ratios (HRs) and adjusted HRs (aHRs) along with 95% confidence intervals (CIs) for mortality. We calculated aHRs after adjusting for age, gender, sociodemographic characteristics, and comorbidities. All data management and statistical analyses were performed using SAS (version 9.4; SAS Institute, Cary, NC, USA).
Subgroup Analysis
We compared the risk of mortality between the ASD and non-ASD cohorts. To determine whether ID is associated with an increased risk of mortality in individuals with ASD, we conducted a subgroup analysis; we divided the patients with ASD into ID and non-ID subgroups and then compared the risks of mortality between these subgroups and the non-ASD group. Furthermore, the study compared mortality risks between subgroups stratified according to age, gender, ID status, income status, and comorbidities. This study was reviewed and approved by the Research Ethics Committee of China Medical University Hospital (CMUH108-REC1-142).
Results
This study analyzed the data of 75,946 patients with ASD and 75,946 non-ASD matched controls. Table 1 lists the baseline characteristics of the patients, including sex, age group, income status, and comorbid psychiatric and physical illnesses. The cohorts were effectively matched by age group, sex, and income. The ASD cohort had a significantly higher proportion of patients with depression, hypertension, or DM than did the non-ASD cohort. The number of deaths from all causes and natural causes was higher in the ASD cohort than in the non-ASD cohort, but the number of deaths from unnatural causes did not differ between the two groups (Table 1).
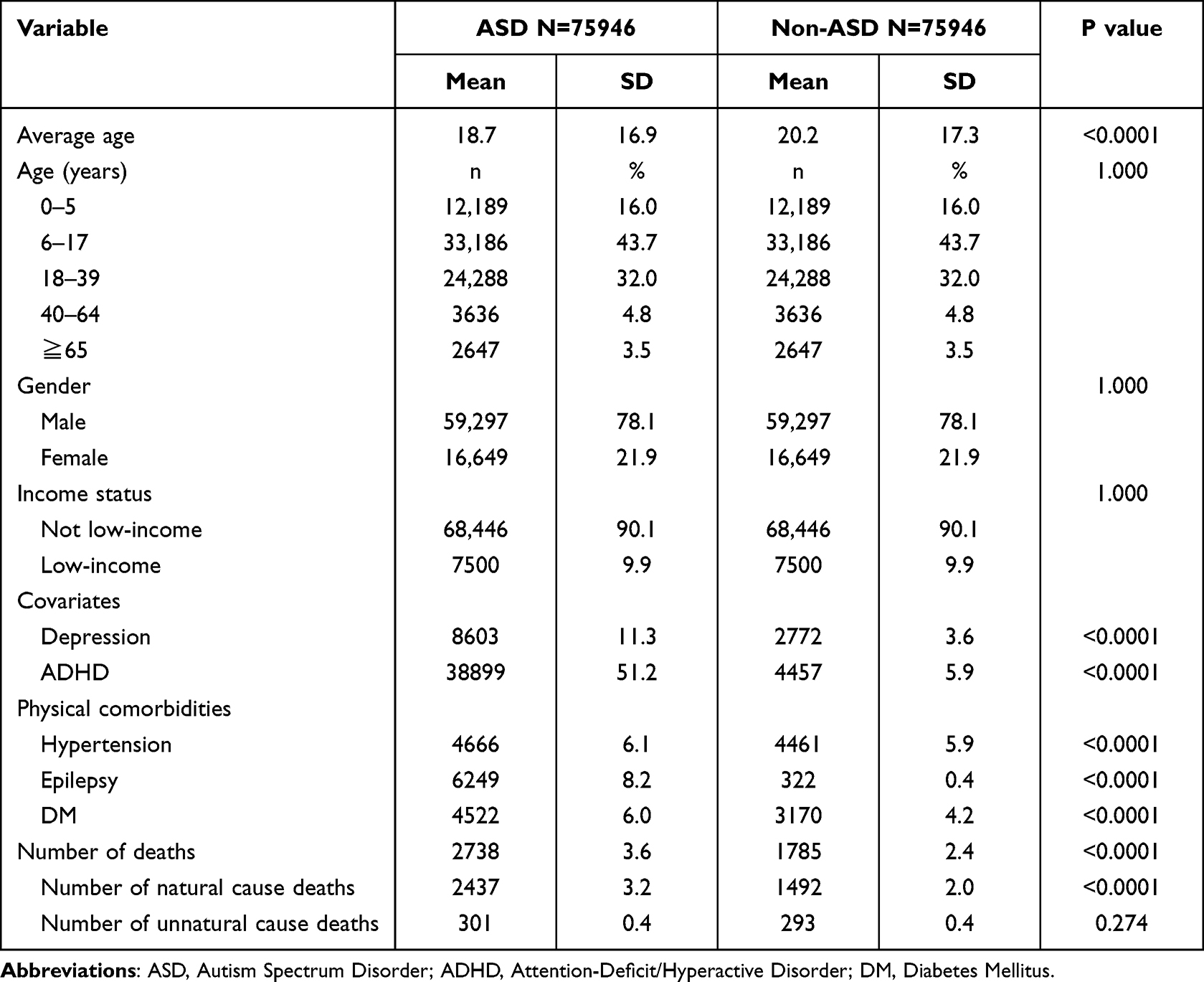 |
Table 1 Basic Characteristics of Autistic Cohort and Non-Autistic Cohort After Matching |
Table 2 presents results obtained from the Cox regression models for the total sample and subgroups. Overall, the ASD cohort had significantly higher mortality than did the control cohort. Regarding the age-based ASD subgroups, patients aged <18 years had lower risks of mortality than did those in the other age subgroups. Moreover, patients aged 40–64 years had significantly higher risks of mortality than did the other age subgroups, followed by patients aged 18–40 years, and those aged ≥65 years. Regarding the sex-based subgroups, we observed more positive HRs in female patients with ASD than in male patients with ASD.
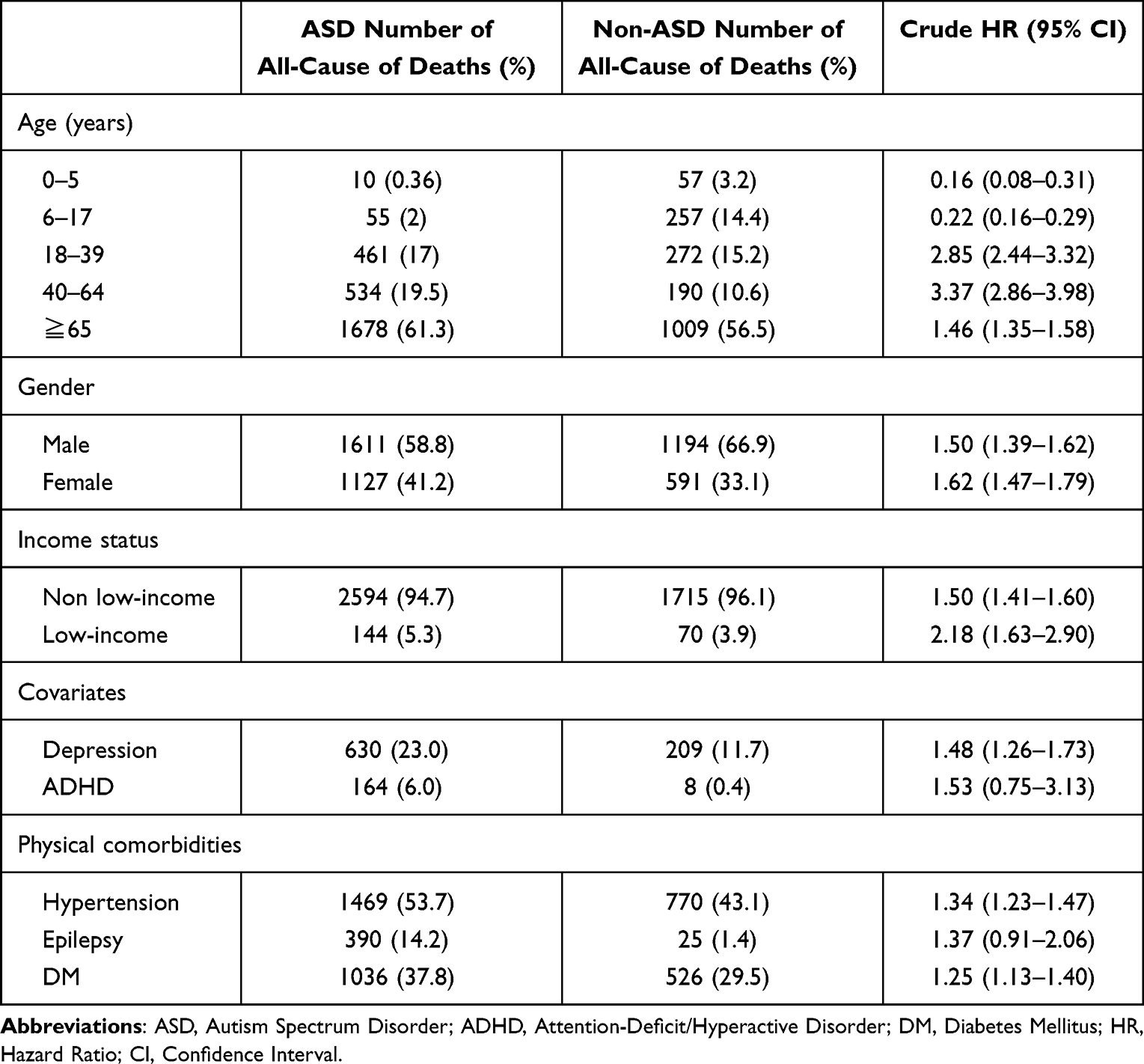 |
Table 2 Comparison of Deaths According to Different Characteristics in the Two Cohorts |
After adjusting for sociodemographic and physical or psychiatric comorbidities, we observed that patients with ASD had significantly higher mortality risks than did those without ASD (aHR 1.64, 95% CI 1.54–1.75; Table 3) when considering deaths from all causes. When compared against the same non-ASD reference, the ID subgroup had a higher relative risk of mortality (aHR 2.87, 95% CI 2.59–3.19) than did the non-ID subgroup (aHR 1.44, 95% CI 1.35–1.54). Considering sex differences, we observed that ASD was associated in higher mortality in both males (aHR 1.65, 95% CI 1.52–1.79) and females (aHR 1.59, 95% CI 1.43–1.76). Among patients with ASD and ID, the risk of mortality was much higher among female patients (aHR 3.85, 95% CI 3.20–4.63) than it was among male patients (aHR 2.48, 95% CI 2.18–2.83).
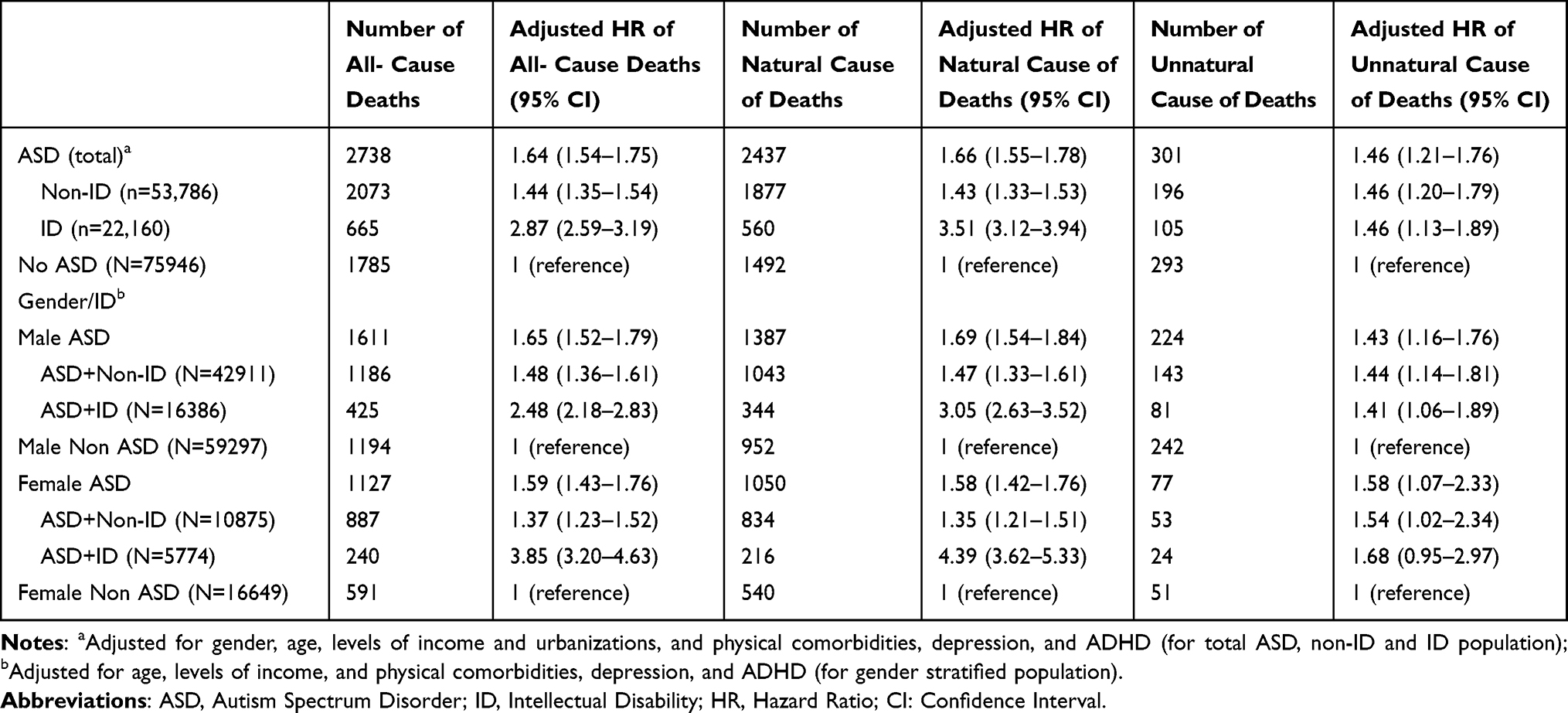 |
Table 3 Comparison of Hazard Ratios of Autism Spectrum Disorder Individuals with Different Gender and Intelligence to Those Without Autism Spectrum Disorder |
When focusing on deaths from natural causes, we found a significantly higher odds ratio for mortality in the ASD population with ID (aHR 3.51, 95% CI 3.12–3.94 for both genders; aHR 3.05, 95% CI 2.63–3.52 for males; aHR 4.39, 95% CI 3.62–5.33 for females; Table 3) compared to the ASD cohort without ID (aHR 1.43, 95% CI 1.33–1.53 for both genders; aHR 1.47, 95% CI 1.33–1.61 for males; aHR 1.35, 95% CI 1.21–1.51 for females). For deaths due to unnatural causes, there was no significant differences in mortality between individuals with ASD with or without intellectual disability. When focusing on females with ASD and ID, there was no higher mortality compared to the general population for deaths due to unnatural causes (aHR 1.68, 95% CI 0.95–2.97).
Discussion
To the best of our knowledge, this study is the first to investigate ASD-associated mortality and its risk profile among Asian patients of all ages. We observed that patients with ASD had a higher risk of mortality for all causes of death than did those without ASD. This risk was greater in the subgroup of patients with ASD and ID, and the excess mortality rate in this subgroup was particularly high among female patients. When focusing on deaths from natural causes, we found a significantly higher odds ratio for mortality in the ASD population with ID compared to those without ID.
Different Mortality Risks Among Different Age Groups
Our findings are consistent with those of a Scottish study involving a sample of pupils.15 Specifically, the Scottish study reported that the rate of mortality in the youngest age group of pupils with ASD was not higher than that in the non-ASD population; the study also reported that the rate of mortality in this age group was significantly lower than that in other ASD age groups. Smith et al cautiously concluded that high-quality care may prevent mortality in some children or adolescents with ASD. Diagnosis itself may be an indicator of higher-quality care. For instance, a study on toddlers found that those diagnosed with ASD at a later age showed more severe ASD symptoms, whereas children diagnosed at a younger age had milder symptoms and were more responsive to intervention.27 Fountain described that children diagnosed at an earlier age were more likely to have parents with higher education level.28 Another population-based cohort study in Taiwan also indicated higher likelihood of being diagnosed with ASD when having higher socioeconomic (SES) status.29 Previous studies showed that parents with higher SES tend to be more attentive and knowledgeable about autism, have greater access to quality healthcare services and exhibit greater parental involvement.30–32 This may lead to superior outcomes than individuals with ASD that did not receive a diagnosis or clinical attention. Besides, those with earlier diagnosis may have more frequent encounters with the healthcare system, which could explain why the younger age group with ASD had lower mortality rates.
Nonetheless, a systemic review identified higher medical comorbidity rates in children and adolescents with ASD than in those without ASD.33 Health-care professionals working with individuals with ASD should be aware of this and should perform routine medical assessments for such individuals. A possible explanation for the lower HRs in younger patients with ASD is that ASD or relevant physical comorbidities are diagnosed at younger ages. Further research on the causes of death in young people with ASD is necessary to improve the overall quality of their care.
The strongest association between ASD and increased mortality was observed in the 40–64-year age group, followed by patients aged 18–40 years. However, a relatively weak association was noted in the ≥65-year age group; this finding may be explained by healthy survivor effects, or it may be due to the weakening of ASD as a risk factor by other inherent risk factors in older age. Our finding of a higher risk of mortality among adults with ASD than among controls is consistent with the results of a previous study, which reported increased odds of inpatient mortality due to a higher prevalence of psychiatric or physical comorbidities in adults with ASD.10 In our data, the higher rates of comorbid depression, hypertension, and DM among individuals with ASD compared to the general population may contribute to higher mortality due to suicide or physical illness in adulthood or during the elder years. Accordingly, physicians must identify and communicate health-care needs to patients with ASD.34 The communication may be difficult for people with autism. In youths or young adults with ASD, those with higher support needs often continue to rely on a caregiver, typically their parents in Taiwan, who helps them communicate with physicians. However, as they reach middle adulthood or old age, their caregiver may become too old to provide assistance, and individuals with ASD may need to be institutionalized. Further studies are needed to examine the health impacts of this transition on individuals with ASD. There are very few studies regarding the healthcare of adults or elderly individuals with ASD in Taiwan. Further studies are warranted.
Impact of ID on ASD Mortality
In our study, ASD was associated with higher mortality regardless of the presence of ID; however, individuals with ASD and ID had higher mortality rates than did those with ASD alone. These findings are consistent with those of previous studies.11,14,19,22 Comorbid ID may affect the quality of self-care and compliance with medical or psychosocial interventions among individuals with ASD. Mouridsen et al observed no differences in mortality between individuals with ASD with and without ID;12 however, their observation may have been influenced by their inclusion criteria (only patients with ASD aged <18 years) or smaller sample sizes. In addition to enabling the provision of appropriate care or education programs, early identification of ASD with IDs may help improve access to care for physical or psychiatric comorbidities and curb adverse multimorbidity trajectories.
Moreover, when focusing on deaths from natural causes, we found a significantly higher odds ratio for mortality in the ASD population with ID compared to those without ID. As mentioned previously, communication to health care workers is particularly challenging for individuals with ASD who also have intellectual disabilities. Natural causes of death were primarily attributed to physical illness. The increased physical comorbidities associated with ASD,10,33 coupled with challenges in adhering to medical treatments and health habits, may contribute to higher mortality rates.
Impact of Sex on ASD Mortality
We observed that among patients with ASD and comorbid ID, the rate of excess mortality was higher among female patients than it was among male patients. This finding is consistent with the findings of Hirvikoski, who used data from a Swedish nationwide database.19 Previous studies have reported that the female sex was associated with increased mortality in individuals with ASD.11–13,18,22,35 A possible explanation for this finding is that female individuals with ASD tended to have concurrent neurological abnormalities and poorer intellectual and adaptive functioning than do male individuals.36 While not universally applicable, female patients with ASD tended to exhibit a higher genetic load or more gene-rich de novo copy number variations.37 Moreover, female patients with ASD tended to be overrepresented among individuals with fragile X syndrome target proteins.38 Therefore, the possible biological etiology underpinning epidemiological findings must be explored.
Strengths and Limitations
This large population-based cohort study has several strengths. First, the nationally representative sample provided substantial interpretability and helped minimize selection bias. Second, diagnoses of ASD and physical illnesses were confirmed by clinicians instead of self-reported assessments. Third, we examined multiple risk factors associated with mortality in patients with or without ASD, considering potential confounding variables. Nevertheless, some limitations require consideration. First, we used insurance administrative data; therefore, diagnoses might have been misclassified, and individuals in the non-ASD cohort may have had undiagnosed ASD (such individuals were likely relatively few). Second, patients with different ASD types and pervasive developmental disorders were grouped together in the ASD cohort without further categorization because of the restrictiveness of ICD diagnoses. Analyzing specific mortality risks for individual diseases may require a larger sample. Accordingly, further comprehensive research is necessary to analyze any correlation between cause-specific mortality and psychotropic drug use.
Conclusion
Our study indicated that patients with ASD had a higher mortality risk than did patients without ASD and that this risk was greater in female patients with comorbid ID. These findings highlight the necessity of appropriately identifying potential underlying psychiatric and physical comorbidities among the most vulnerable patients with ASD and then implementing relevant interventions to reduce excess mortality.
Abbreviations
ASD, Autistic Spectrum Disorder; ID, intellectual disability; NHI, National Health Insurance; NHIRD, National Health Insurance Research Database; ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification; ICD-10, International Classification of Diseases, Tenth Revision; ADHD, attention-deficit hyperactivity disorder; DM, diabetes mellitus; HRs, hazard ratios; aHRs, adjusted HRs; CIs, confidence intervals.
Data Sharing Statement
The NHIRD data used in this study are held by the Taiwan Ministry of Health and Welfare. Data are available by submitting a formal proposal to the Taiwan National Health Insurance Administration. We are not permitted to share the data.
Ethics Statement
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Research Ethics Committee of China Medical University Hospital (CMUH108-REC1-142).
Acknowledgments
The authors are grateful for the support of the Health Information and Epidemiology Laboratory (CLRPG6G0043) of Chang Gung Memorial Hospital, Chiayi, Taiwan. Robert Stewart was partially funded by i) the National Institute for Health Research (NIHR) Maudsley Biomedical Research Centre at the South London and Maudsley National Health Service (NHS) Foundation Trust and King’s College London; ii) the NIHR Applied Research Collaboration South London at King’s College Hospital NHS Foundation Trust; iii) UK Research and Innovation Medical Research Council (MRC) through the Health Data Research Hub DATAMIND (MRC reference: MR/W014386); and iv) the UK Prevention Research Partnership (Violence, Health and Society; MR-VO49879/1), an initiative funded by UK Research and Innovation councils, the Department of Health and Social Care (England), the UK devolved administrations, and leading health research charities.
Disclosure
Robert Stewart declares research support received in the last 3 years from Janssen, GSK, and Takeda; personal fees from Oxford University Press. The other authors report no conflicts of interest in this work.
References
1. Zeidan J, Fombonne E, Scorah J, et al. Global prevalence of autism: a systematic review update. Autism Res. 2022;15(5):778–790. doi:10.1002/aur.2696
2. Prevention CfDCa. Autism spectrum disorder. prevalence and characteristics of autism spectrum disorder among children aged 8 years — autism and developmental disabilities monitoring network, 11 sites, United States, 2020 web site; 2023. Available from: https://www.cdc.gov/mmwr/volumes/72/ss/ss7202a1.htm?s_cid=ss7202a1_w.
3. Lai MC, Lombardo MV, Baron-Cohen S. Autism. Lancet. 2014;383(9920):896–910. doi:10.1016/s0140-6736(13)61539-1
4. Buck TR, Viskochil J, Farley M, et al. Psychiatric comorbidity and medication use in adults with autism spectrum disorder. J Autism Develop Disorders. 2014;44(12):3063–3071. doi:10.1007/s10803-014-2170-2
5. Croen LA, Zerbo O, Qian Y, et al. The health status of adults on the autism spectrum. Autism. 2015;19(7):814–823. doi:10.1177/1362361315577517
6. Henninger NA, Taylor JL. Outcomes in adults with autism spectrum disorders: a historical perspective. Autism. 2013;17(1):103–116. doi:10.1177/1362361312441266
7. Miot S, Akbaraly T, Michelon C, et al. Comorbidity burden in adults with autism spectrum disorders and intellectual disabilities-a report from the EFAAR (frailty assessment in ageing adults with autism spectrum and intellectual disabilities) study. Frontiers in Psychiatry. 2019;10:617. doi:10.3389/fpsyt.2019.00617
8. Vohra R, Madhavan S, Sambamoorthi U. Comorbidity prevalence, healthcare utilization, and expenditures of Medicaid enrolled adults with autism spectrum disorders. Autism. 2017;21(8):995–1009. doi:10.1177/1362361316665222
9. Joshi G, Petty C, Wozniak J, et al. The heavy burden of psychiatric comorbidity in youth with autism spectrum disorders: a large comparative study of a psychiatrically referred population. J Autism Develop Disorders. 2010;40(11):1361–1370. doi:10.1007/s10803-010-0996-9
10. Akobirshoev I, Mitra M, Dembo R, Lauer E. In-hospital mortality among adults with autism spectrum disorder in the United States: a retrospective analysis of US hospital discharge data. Autism. 2019;1362361319855795. doi:10.1177/1362361319855795
11. Bilder D, Botts EL, Smith KR, et al. Excess mortality and causes of death in autism spectrum disorders: a follow up of the 1980s Utah/UCLA autism epidemiologic study. J Autism Develop Disorders. 2013;43(5):1196–1204. doi:10.1007/s10803-012-1664-z
12. Mouridsen SE, Bronnum-Hansen H, Rich B, Isager T. Mortality and causes of death in autism spectrum disorders: an update. Autism. 2008;12(4):403–414. doi:10.1177/1362361308091653
13. Pickett JA, Paculdo DR, Shavelle RM, Strauss DJ. 1998–2002 Update on ”Causes of death in autism”. J Autism Develop Disorders. 2006;36(2):287–288. doi:10.1007/s10803-005-0066-x
14. Hwang YIJ, Srasuebkul P, Foley KR, Arnold S, Trollor JN. Mortality and cause of death of Australians on the autism spectrum. Autism Res. 2019;12(5):806–815. doi:10.1002/aur.2086
15. Smith GS, Fleming M, Kinnear D, et al. Mortality in 787,666 school pupils with and without autism: a cohort study. Autism. 2021;25(1):300–304. doi:10.1177/1362361320944037
16. Schendel DE, Overgaard M, Christensen J, et al. Association of psychiatric and neurologic comorbidity with mortality among persons with autism spectrum disorder in a Danish population. JAMA Pediatr. 2016;170(3):243–250. doi:10.1001/jamapediatrics.2015.3935
17. Catalá-López F, Hutton B, Page MJ, et al. Mortality in persons with autism spectrum disorder or attention-deficit/hyperactivity disorder: a systematic review and meta-analysis. JAMA Pediatr. 2022;176(4):e216401. doi:10.1001/jamapediatrics.2021.6401
18. Gillberg C, Billstedt E, Sundh V, Gillberg IC. Mortality in autism: a prospective longitudinal community-based study. J Autism Develop Disorders. 2010;40(3):352–357. doi:10.1007/s10803-009-0883-4
19. Hirvikoski T, Mittendorfer-Rutz E, Boman M, Larsson H, Lichtenstein P, Bolte S. Premature mortality in autism spectrum disorder. Br J Psychiatry. 2016;208(3):232–238. doi:10.1192/bjp.bp.114.160192
20. Yoo SM, Kim KN, Kang S, Kim HJ, Yun J, Lee JY. Prevalence and premature mortality statistics of autism spectrum disorder among children in Korea: a nationwide population-based birth cohort study. J Korean Med Sci. 2022;37(1):e1. doi:10.3346/jkms.2022.37.e1
21. Smith DaWalt L, Hong J, Greenberg JS, Mailick MR. Mortality in individuals with autism spectrum disorder: predictors over a 20-year period. Autism. 2019;23(7):1732–1739. doi:10.1177/1362361319827412
22. Shavelle RM, Strauss DJ, Pickett J. Causes of death in autism. J Autism Develop Disorders. 2001;31(6):569–576. doi:10.1023/a:1013247011483
23. Kim KN, Yoo SM, Kang S, Kim HJ, Yun J, Lee JY. Mortality of children with autism spectrum disorder using data from a large-scale Korean national cohort. Yonsei Med J. 2021;62(10):943–947. doi:10.3349/ymj.2021.62.10.943
24. Hossain MM, Khan N, Sultana A, et al. Prevalence of comorbid psychiatric disorders among people with autism spectrum disorder: an umbrella review of systematic reviews and meta-analyses. Psychiatry Res. 2020;287:112922. doi:10.1016/j.psychres.2020.112922
25. Chen MH, Pan TL, Lan WH, et al. Risk of suicide attempts among adolescents and young adults with autism spectrum disorder: a nationwide longitudinal follow-up study. J Clini Psych. 2017;78(9):e1174–e1179. doi:10.4088/JCP.16m11100
26. NHIRD. National health insurance research database, Taiwan. Introduction to the National Health Insurance Research Database (NHIRD), Taiwan; 2006. Available from: http://www.nhri.org.tw/nhird/en/index.htm>.
27. Miller LE, Dai YG, Fein DA, Robins DL. Characteristics of toddlers with early versus later diagnosis of autism spectrum disorder. Autism. 2021;25(2):416–428. doi:10.1177/1362361320959507
28. Fountain C, King MD, Bearman PS. Age of diagnosis for autism: individual and community factors across 10 birth cohorts. J Epidemiol Community Health. 2011;65(6):503–510. doi:10.1136/jech.2009.104588
29. Yu T, Lien YJ, Liang FW, Kuo PL. Parental socioeconomic status and autism spectrum disorder in offspring: a population-based cohort study in Taiwan. Am J Epidemiol. 2021;190(5):807–816. doi:10.1093/aje/kwaa241
30. Sun X, Allison C, Auyeung B, Baron-Cohen S, Brayne C. Parental concerns, socioeconomic status, and the risk of autism spectrum conditions in a population-based study. Res Develo Disabil. 2014;35(12):3678–3688. doi:10.1016/j.ridd.2014.07.037
31. Lung FW, Chiang TL, Lin SJ, Shu BC. Urban and education disparity for autism spectrum disorders in Taiwan birth cohort study. J Autism Develop Disorders. 2017;47(3):599–606. doi:10.1007/s10803-016-2980-5
32. Yan T, Hou Y, Liang L. Family socioeconomic status and parental involvement in Chinese parents of children with autism spectrum disorder: a moderated mediation model. Healthcare. 2023;11(9). doi:10.3390/healthcare11091281
33. Muskens JB, Velders FP, Staal WG. Medical comorbidities in children and adolescents with autism spectrum disorders and attention deficit hyperactivity disorders: a systematic review. Eur Child Adolesc Psychiatry. 2017;26(9):1093–1103. doi:10.1007/s00787-017-1020-0
34. Lunsky Y, Klein-Geltink J, Yates E Atlas on the Primary Care of Adults with Developmental Disabilities in Ontario. Toronto: Institute for Clinical Evaluative Sciences and Centre for Addiction and Mental Health; 2013. Available from: https://www.porti-conetwork.ca/documents/38160/99698/Atlas+revised+2014/c2d68a41-ed3d-44dc-8a14-7f30e044c17e.
35. Isager T, Mouridsen SE, Rich B. Mortality and causes of death in pervasive developmental disorders. Autism. 1999;3(1):7–16.
36. Lai MC, Lombardo MV, Auyeung B, Chakrabarti B, Baron-Cohen S. Sex/gender differences and autism: setting the scene for future research. J Am Acad Child Adolesc Psychiatry. 2015;54(1):11–24. doi:10.1016/j.jaac.2014.10.003
37. Sanders SJ, Ercan-Sencicek AG, Hus V, et al. Multiple recurrent de novo CNVs, including duplications of the 7q11.23 Williams syndrome region, are strongly associated with autism. Neuron. 2011;70(5):863–885. doi:10.1016/j.neuron.2011.05.002
38. Pinto D, Delaby E, Merico D, et al. Convergence of genes and cellular pathways dysregulated in autism spectrum disorders. Am J Hum Genet. 2014;94(5):677–694. doi:10.1016/j.ajhg.2014.03.018
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.