")
Back to Journals » Journal of Healthcare Leadership » Volume 15
Evolving Roles and Needs of Psychiatry Chief Residents During the COVID-19 Pandemic and Beyond
Authors Ratnakaran B, Hanafi S, Wobbe H , Howland M
Received 1 March 2023
Accepted for publication 10 June 2023
Published 15 June 2023 Volume 2023:15 Pages 95—101
DOI https://doi.org/10.2147/JHL.S408556
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pavani Rangachari
Badr Ratnakaran,1 Sarah Hanafi,2 Heather Wobbe,3 Molly Howland4
1Department of Psychiatry, Carilion Clinic-Virginia Tech Carilion School of Medicine, Roanoke, VA, USA; 2Department of Psychiatry, McGill University, Montreal, QC, Canada; 3Department of Psychiatry, Summa Health, Akron, OH, USA; 4Department of Psychiatry, Cleveland Clinic, Cleveland, OH, USA
Correspondence: Badr Ratnakaran, Department of Psychiatry, Carilion Clinic-Virginia Tech Carilion School of Medicine, 2017, S Jefferson St, Roanoke, VA, USA, Tel +1 540-855-4648, Fax +1 540 981-7653, Email [email protected]
Abstract: Psychiatry chief residents have diverse leadership roles within psychiatry residency programs. Chief residents have historically been viewed as “middle managers”, and other leadership roles include administrative work, teaching, and advocacy for residents. Chief residents also help in managing the logistics of complex healthcare systems and mediating between many groups with conflicting needs and perspectives. The COVID-19 pandemic has changed the functioning of psychiatry residency programs, and this has also led to the evolution of the roles of the chief residents in psychiatry. During the COVID-19 pandemic, the chief residents had to help with adapting to the changes in teaching and clinical work with residents and faculty. They had to liaison with various healthcare providers in making decisions related to COVID-19 in residency programs. Along with these changes, chief residents also had to advocate for the wellbeing and needs of their fellow residents. This perspective article is written by authors who have served during or after the transition to the COVID-19 pandemic. We discuss our experiences as chief residents as well as evolving roles and wellness needs of chief residents in psychiatry. Based on the administrative, advocacy, academic and middle management roles of chief residents in psychiatry and their wellbeing, we also make recommendations for support and interventions needed for chief residents in the context of the COVID-19 pandemic and beyond.
Keywords: chief residents, psychiatry, COVID-19
Introduction
Psychiatry chief residents have diverse roles within psychiatry residency programs. Though most psychiatry residency programs have one or two chief residents, larger programs may appoint multiple chief residents with predefined roles (eg, clinical administration, education, wellness, and diversity chief residents).1 Residency programs commonly provide role descriptions for chief residents.1 Nevertheless, psychiatry chief resident roles are often ambiguous and malleable to meet the current needs of the resident body, faculty, and health care system.2,3
Despite the diversity of chief resident duties, the literature has highlighted several common features of the position. Chief residents have historically been viewed as “middle managers” or liaisons between residents and faculty, as they identify as both residents and administrators.4–6 Other common features include administrative work (eg, rotation and call scheduling), teaching (eg, during clinical rounds or didactic sessions), and advocacy for resident wellbeing.1–3 They also commonly serve as a liaison for other professions in the hospital system (eg, pharmacists, nurse managers, etc.).4
Chief residents face several challenges, including managing the logistics of complex healthcare systems and mediating between many groups with conflicting needs and perspectives.6 Several papers have outlined interventions such as leadership curricula to assist chief residents in fulfilling their duties.6–11 None to our knowledge have described interventions for the wellness of chief residents.
The COVID-19 pandemic has changed the functioning of psychiatry residency programs. Some studies have explored psychiatry residents’ experience of the pandemic.12,13 Richards et al have commented on the measures taken by psychiatry residency and fellowship program directors to adapt clinical care and teaching to the COVID-19 pandemic.14 These authors highlighted program directors’ role in first promoting residents’ basic needs on Maslow’s hierarchy (eg, supplying personal protective equipment [PPE], ensuring housing and childcare during illness, providing clear information on changing COVID-19 policies), and then focusing on residents’ emotional well-being (eg, starting remote process groups, disseminating mindfulness exercises, hosting virtual game and movie nights).
However, no studies have explored psychiatry chief residents’ evolving roles during the COVID-19 pandemic or lasting changes to their roles as COVID-19 became endemic. As we are in the endemic phase of the COVID-19 pandemic, current chief residents continue many of the practices initiated by their predecessors as described below, including communication between residents, mitigating risks of infection from the virus, adopting new methods of teaching residents, and addressing the emotional and physical well-being of the residents.
The authors are former or current psychiatry chief residents who have served during or after the transition to the COVID-19 pandemic era. The authors met three times from March to May 2022 via videoconferencing platforms and regularly conferred via email to discuss their experiences as chief residents during the pandemic and build consensus about recommendations. Our objectives are to describe chief residents’ evolving roles and wellness needs, as well as recommend supports and interventions for chief residents during the COVID-19 pandemic and beyond.
Role: Administration
The COVID-19 pandemic has presented several administrative challenges for psychiatry chief residents. In our experience, chief residents have been variably involved in decision-making about COVID-19 residency changes (eg, COVID-19 patients on psychiatry units, redeployment to non-psychiatry units, workplace social distancing expectations, etc.). Most COVID-19 policies have been communicated from the hospital or graduate medical education office, though at one author’s program, chief residents had the opportunity to provide input to these stakeholders. Nevertheless, chief residents have been consistently tasked with disseminating, implementing, and enforcing these COVID-19 policies and expectations. As such, chief residents are expected to remain informed about COVID-19 policies, which shift more frequently than policies unrelated to the pandemic. Chief residents must distill this information into concise messages to their residents to prevent information overload.14,15 Many informal communication channels (eg, hallway discussion at didactics) have been unavailable during the pandemic, decreasing opportunities for chief residents and residents to express their opinions about changes. Consequently, chief residents must develop messaging that accounts for decreased processing time, to soften emotional reactions and create space for residents to reflect during virtual meetings. Additionally, chief residents serve as role models and enforcers of COVID-19-related policies.
At some programs, the chief resident assists with organization of and communication surrounding redeployment from psychiatry services to COVID-19 units. At other programs, the graduate medical education office, or the program faculty leadership coordinate redeployment. Half of the authors’ residency programs did not redeploy psychiatry residents. However, at multiple programs, chief residents developed plans for bolstered backup coverage of psychiatry services (eg, additional backup residents/attendings for call/rotations) to cover deployed or ill residents. Finally, chief residents commonly facilitated the transition of residents’ outpatient clinics and inpatient consult-liaison services to telepsychiatry. These COVID-related logistical duties and increased communication needs, as outlined above, have increased chief residents’ work hours and stress.
Recommendations: Administration
As COVID-19 shifts from an emergency to a cyclical challenge, the role of psychiatry chief residents should similarly shift. Redeployment and backup coverage should be anticipated. Psychiatry chief residents are not ideally positioned to take the sole lead in most of these challenges because iterative learning will be lost as chief residents change each year. We recommend that long-term program leaders (eg, the training director or program coordinator) and chief residents share responsibility for these processes, as long-term program leaders are positioned to synthesize “top-down” requirements placed on psychiatry residency programs by the hospital system or the graduate medical education office. Chief residents can learn from long-term leaders how to balance the goals of various stakeholders. Chief residents can also provide “bottom-up” information about the needs and perspectives of psychiatry residents to program leaders and implement program leaders’ plans (eg, assigning residents or developing backup schedules).
Given the increased intensity and frequency of communications during the COVID-19 pandemic, the program leadership should provide formal education to chief residents about communication strategies (eg, professional development courses or leadership curricula). We also recommend maintaining online repositories of dynamic program policies that can easily be updated. We also support the recommendation of Bandstra et al for incoming chief residents to shadow outgoing chief residents, as well as receive supervision and mentorship from program directors and an administrative consultant with no direct relations with the training program given the increase in administrative duties during the COVID-19 pandemic.6 We recommend that program leadership protect an orientation period of approximately 3 months prior to the chief resident’s tenure for shadowing, education about communication strategies, and mentorship with clearly stated competencies from program directors. We recommend that administrative consultants provide education about succeeding in an administrative role as part of an orientation to chief residency year. Mentorship should be incorporated into biweekly mentorship meetings during the chief residents’ tenure.
Role: Resident Support and Advocacy
During the COVID-19 pandemic, chief residents became more directly involved in advocating for resident needs and promoting wellbeing. Residents have been vulnerable to a deterioration in wellbeing during the pandemic as they typically have less agency surrounding their work conditions and fewer material resources to bolster personal resilience.
Chief residents advocate for resident needs in the workplace, including access to personal protective equipment (PPE), vaccination prioritization, access to telehealth technologies, and access to supervision and didactic teaching. Many chief residents provide resident representation at both newly formed and existing organizations within the residency program and hospital administration.
Informal peer support—normally provided during in-person teaching and other events—is more challenging given social distancing during the COVID-19 pandemic. Chief residents have instituted group and individual check-ins with residents to ensure their health and safety, validate their concerns, and acknowledge the unfairness and uncertainty of the situation. Some chiefs had to address incivility as the social cohesion of resident cohorts disintegrated. Many factors may be implicated in this, including social isolation, increased conflict due to differing perspectives in a time of crisis, and centering of individual interests in a time of perceived risk to survival. Attempts to organize virtual community events were limited by inadequate engagement, though one of the authors successfully used alternative virtual venues such as SpatialChat. The authors agree that in-person events better promoted cohesion and chief residents were commonly tasked with organizing in-person events that minimized COVID-19 risks.
Recommendations: Resident Support and Advocacy
Chief residents should promote group cohesion and continue innovating strategies for safe, responsible social connection in future public health crises. Program leaders should provide adequate funding for these social events and assist chief residents to weigh the risks and benefits of social events. Additionally, chief residents can frame the crisis as a common foe, which can mitigate the instinctual prioritization of individual interests and foster the capacity for solidarity and collegiality among residents.12 Sending weekly communiqués reduces residents’ sense of uncertainty. A 2021 pilot study by Chochol et al utilized virtual Balint groups to decrease burnout among child and adolescent psychiatry trainees during the COVID-19 pandemic.16 Each Balint group in this pilot study was comprised of six trainees and one group leader who was already respected within the trainee body. It is possible that the small-group format, as well as the implication of a respected leader, helped mitigate the potential drawbacks of a virtual delivery format and promoted engagement. Chief residents should consider implementing biweekly Balint groups to promote resident wellness. We recommend ensuring resident representation across all organizational levels to increase residents’ sense of agency.14 Finally, we recommend following Maslow’s hierarchy of needs such that physical and safety needs are prioritized ahead of other higher needs.14
Role: Education
Chief residents have encountered teaching challenges during the pandemic. Teaching, supervision, and clinical encounters were adapted to virtual platforms such as Zoom or Microsoft Teams. Chief residents were often the first to become acquainted with these platforms. They assisted residents and faculty unfamiliar with the technology and addressed technological barriers. Some chief residents have helped communicate expectations for virtual learning sessions (eg, proper attire, video use). Managing the transition to virtual platforms and other COVID-19 adaptations such as schedule changes and patient surges can lead to exhaustion and compromise residents’ capacity for education.17 Further, teaching that relies on interaction (eg, case conferences, psychotherapy roleplay) is difficult to recreate virtually.18 Thus, chief residents have used creativity to simulate active learning through digital platforms such as Kahoot and Google documents. Active learning strategies have decreased education disruptions, and remote learning is generally viewed as convenient by both faculty and residents.19 However, adapting teaching sessions to virtual platforms and ensuring access to required technologies have increased chief residents’ workload.
Recommendations: Education
The pandemic has shown that psychiatric education can be delivered by non-traditional teaching methods. Chief residents should poll the resident body about their preferences for in-person versus virtual didactics and implement a hybrid format based on these preferences to balance convenience and connection. They should work with faculty members to modify their didactic curriculum to incorporate changes in teaching methods and suggestions from residents. Program leaders should provide resources for chief residents to understand adult learning theories to engage learners during crises and connect them with psychiatric education experts to build effective virtual educational content.
Role: Middle Managing/Liaison Work
The COVID-19 pandemic has required psychiatry chief residents to strengthen their middle management and liaison skills. Working as a liaison (ie, crossing organizational boundaries to strengthen ties to other organizations) requires a skill set unique from that of middle management (ie, crossing hierarchical boundaries within one organization). For example, a redeployment plan might require liaising with chief residents in other programs, while public health considerations may require communication with external mental and physical health organizations. Chief residents need to balance these competing priorities with resident concerns. For instance, in one author’s program, the state ministry of health mandated the transition to telehealth, but did not provide telehealth accounts or administrative support, necessitating chief residents to advocate for this support. Traditionally, psychiatry chief residents have been concerned with population mental health (eg, preventing and addressing burnout in residents, addressing their region’s mental health needs with the residents in outpatient chief resident roles, etc.). Now, chief residents must also curtail the spread of COVID-19 in their community by minimizing resident exposure to COVID-19 in rotations and didactics, encouraging residents to discuss COVID-19 vaccination with their patients, and balancing public health and resident privacy when notifying residents about staff exposures.
Aspects of chief residents’ middle management work have also evolved. While the decrease in in-person interaction has disrupted rapport-building with residents, the convenience of virtual meetings has facilitated chief residents’ connection with clinical faculty and department leadership as they no longer need to travel to their supervisors’ physical sites to meet. Chief residents did not historically protect the health of their superiors, though during the pandemic, chief residents have had to be mindful of many supervisors’ older age when planning residency events. This role reversal and frequent virtual contact with program leadership have promoted increased identification of psychiatry chief residents with the administration. However, because they may not have similarly frequent virtual contact with all residents, psychiatry chief residents may struggle to develop similar strong connections with other residents.
Recommendations: Middle Managing/Liaison Work
Skills to communicate effectively with various stakeholders in complex situations are not typically taught during residency training (compared to adapting interview styles). Thus, psychiatry chief residents would benefit from didactic education and coaching around interprofessional communication skills needed for liaison work during public health crises. Occupying these boundary-spanning roles may increase chief residents’ psychological distance from their own organization, so these supports should be instituted during a chief resident’s initial transition into their role.20 Additionally, once psychiatry chief residents work outside the psychiatry department, they may encounter inconsistent information and/or pressure to behave in ways that run counter to their own department’s interests.20 Thus, incorporating check-ins about liaison work into regular mentorship meetings with leaders in the psychiatry department will ensure psychiatry chief residents do not view their organization with distrust.
Further, program leadership should provide chief residents with training and coaching in conflict management to shift between their middle manager and liaison roles. This is particularly important during public health crises, when interpersonal conflict is rife, and should be incorporated into chief residents’ orientation. Inherent personality factors may affect an individual’s conflict resolution styles, leading them to select suboptimal approaches for the situation at hand.21 Thus, conflict resolution training should explore how personality factors affect resolution approaches and empower psychiatry chief residents to choose optimal strategies. This will help them work collaboratively across organizational boundaries, which will improve program outcomes.
Wellbeing of Chief Residents
The COVID-19 pandemic has increased stress on chief residents as their roles have grown in complexity and workload. Moral injury can occur when chief residents balance the interests of residents, program leadership, and hospital administration. For instance, chief residents may have to violate their moral principles by risking resident health when assigning residents to care for COVID-positive patients (with inadequate PPE initially). There is a concern that the risk for physician suicide has increased during the COVID-19 pandemic, although no studies have yet established this.22 Due to chief residents’ sense of responsibility for their residents, these unfortunate events can be distressing. Due to confidentiality concerns, chief residents may not be able to share these traumatic experiences with their loved ones. This may compound the effects of social isolation secondary to COVID-19 travel restrictions and distancing policies. During the COVID-19 pandemic, chief residents have had to preferentially use digital technologies for communication and patient care, which may lead to a form of work-related stress called “technostress”.23 These stressors add to usual chief resident challenges such as transitioning to fellowship or employment and studying for board exams.
Recommendations: Wellbeing of Chief Residents
Program leaders should provide a safe space for chief residents to voice their needs, including check-ins both during regular mentorship meetings with program leadership and during weekly meetings with chief residents’ direct supervisors. Adequate weekly protected time of at least one-half working day, free of clinical duties and didactic attendance, during public health crises for chief resident-related administrative tasks should be provided. Program leaders should offer and encourage the use of mental health resources and employee assistance programs during crises. It is also imperative for programs to provide access to training on mindfulness, resilience, and stress management. Finally, residents should attempt to maintain a healthy work–life balance, limit overtime work, and take time off from work when needed.
Relevance to the Endemic COVID-19 Phase and Beyond
We have described how the roles and challenges of psychiatry chief residents have evolved during the COVID-19 pandemic. In our current endemic COVID-19 phase, transient COVID-19 outbreaks persist, and chief residents continue to assist with adapting resident workflow to decrease disruption to patient care and exposure to the COVID-19 virus. Like their predecessors, the current chief residents address the emotional and physical wellbeing of the residents. As such, they continue to need additional support from their residency program.
We have summarized our recommendations to address gaps in the professional development of chief residents in Table 1 during the endemic phase and beyond and for future public health crises specifically in Table 2. Often, chief residents lack formal training, and chief resident supports are variable, representing professional development gaps. We have therefore offered individual- and systems-level recommendations for the roles chief residents should adopt and the support they should receive from program leadership to fulfill these roles. These recommendations have been made based on our experiences as chief residents and our synthesis of literature related to graduate medical education during the COVID-19 pandemic.
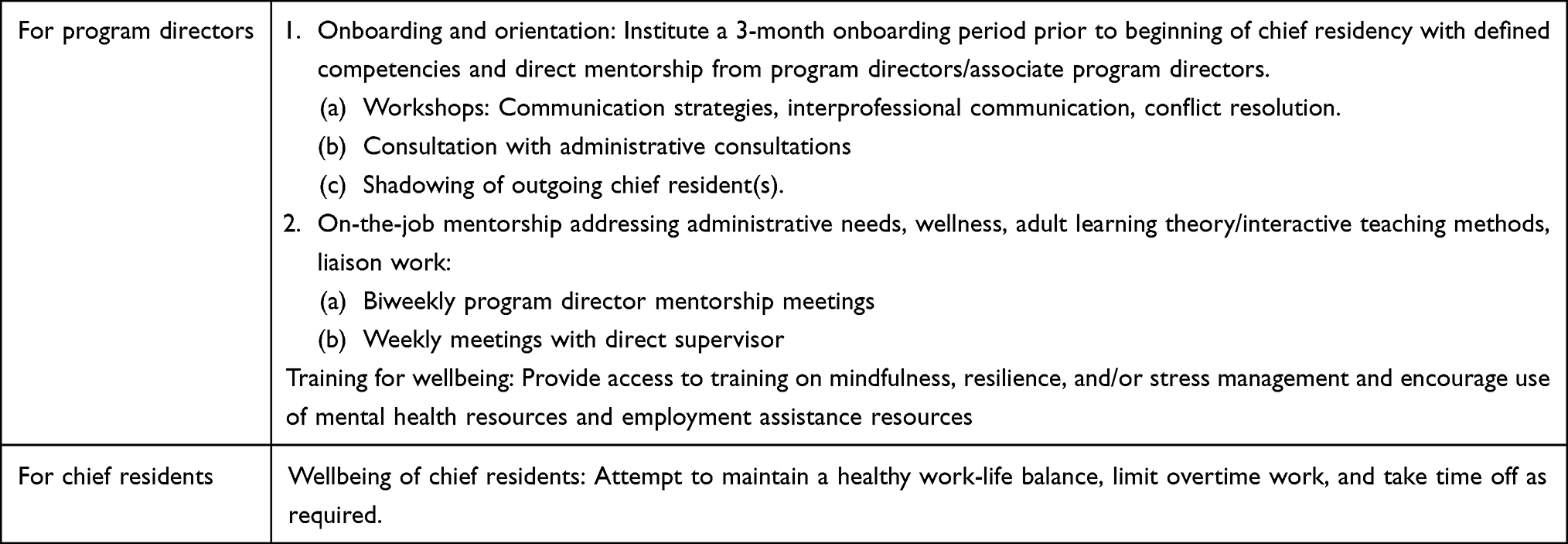 |
Table 1 Recommendations to Address Gaps in Chief Resident Professional Development Exposed by the COVID-19 Pandemic |
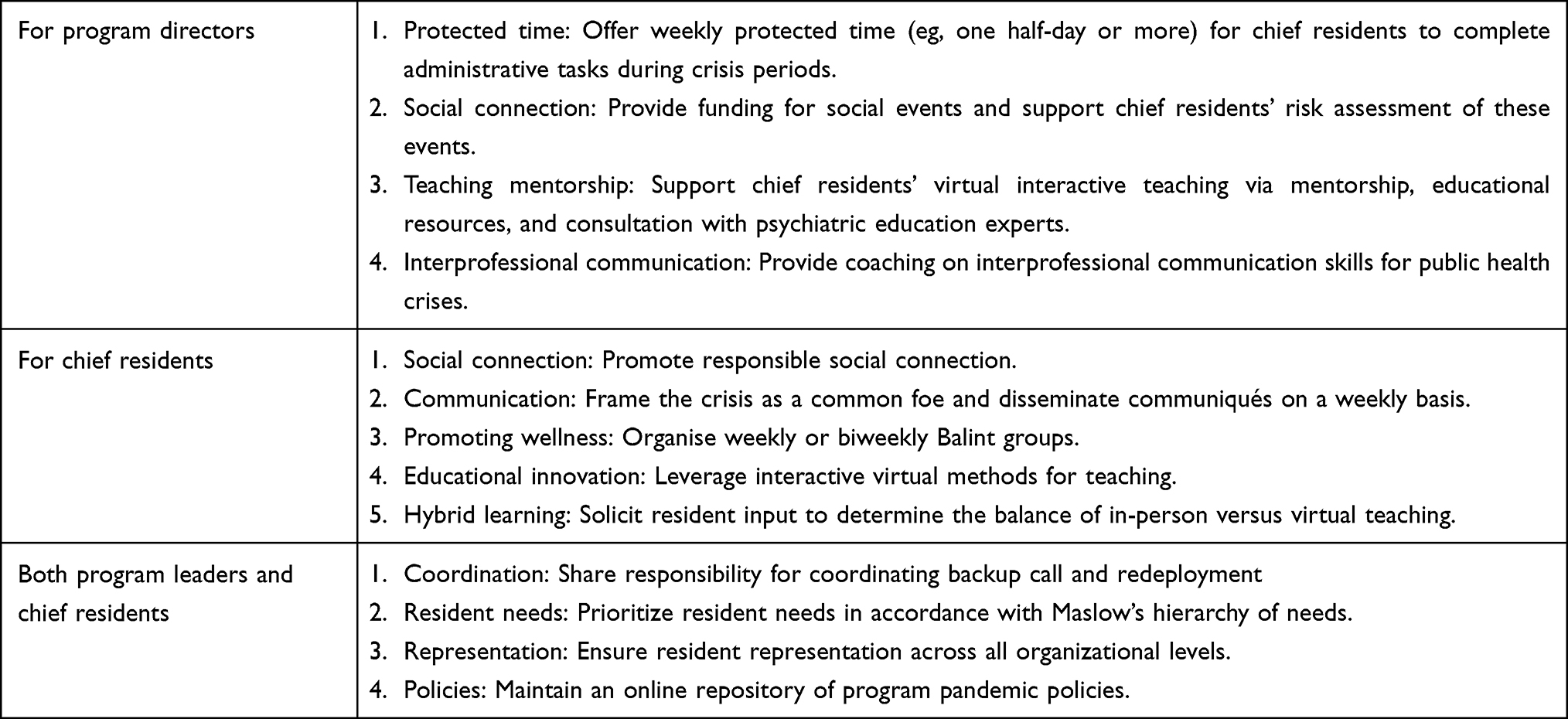 |
Table 2 Recommendations for Future Public Health Crises |
As the COVID-19 endemic becomes less pressing, we recommend that program leadership consider which pandemic adaptations remain useful, including reassessing the indication for practices such as redeployment, backup coverage, and remote socializing while maintaining the option of virtual supervision and didactics, along with creative methods for engaging virtual learners. Further, we recommend that wellness interventions such as frequent check-ins (both between chief residents and program leadership and between chief residents and residents) should be continued in some form post-pandemic given the stressors of residency and chief residency.
Conclusions
Navigating our chief resident responsibilities during the pandemic has helped us balance the needs of our residents and training programs, set realistic goals, and engage our flexibility and creativity in adapting to new teaching methods and technology. Adequate training and support will increase chief residents’ self-efficacy, decrease burnout, and motivate chief residents to pursue future leadership positions in psychiatry.
Disclosure
The authors declare no conflicts of interest.
References
1. Lim RF, Schwartz E, Servis M, Cox PD, Lai A, Hales RE. The chief resident in psychiatry: roles and responsibilities. Acad Psychiatry. 2009;33:56–59. doi:10.1176/appi.ap.33.1.56
2. Grant I, Dorus W, McGlashan T, Perry S, Sherman R. The chief resident in psychiatry. Arch Gen Psychiatry. 1974;30:503–507. doi:10.1001/archpsyc.1974.01760100069011
3. Layde JB, Nicholas P. Chief residencies in psychiatry. Acad Psychiatry. 2007;31:258–260. doi:10.1176/appi.ap.31.4.258
4. Berg DN, Huot SJ. Middle manager role of the chief medical resident: an organizational psychologist’s perspective. J Gen Intern Med. 2007;22:1771–1774. doi:10.1007/s11606-007-0425-8
5. Warner CH, Rachal J, Breitbach J, Higgins M, Warner C, Bobo W. Current perspectives on chief residents in psychiatry. Acad Psychiatry. 2007;31:270–276. doi:10.1176/appi.ap.31.4.270
6. Bandstra BS, Katz M, Huang RW. A curriculum to address issues and challenges of the professional developmental stage of chief residency. Acad Psychiatry. 2013;37:18–22. doi:10.1176/appi.ap.10080123
7. Whitman N. A management skills workshop for chief residents. J Med Educ. 1988;63(6):442–446. doi:10.1097/00001888-198806000-00003
8. McPhillips HA, Frohna JG, Murad MH, et al. Enhancing teamwork between chief residents and residency program directors: description and outcomes of an experiential workshop. J Grad Med Educ. 2011;3:593–597. doi:10.4300/JGME-D-10-00226.1
9. Farver CF, Smalling S, Stoller JK. Developing leadership competencies among medical trainees: five-year experience at the Cleveland clinic with a chief residents’ training course. Australas Psychiatry. 2016;24:499–505. doi:10.1177/1039856216632396
10. Cerrone SA, Adelman P, Akbar S, Yacht AC, Fornari A. Using Objective Structured Teaching Encounters (OSTEs) to prepare chief residents to be emotionally intelligent leaders. Med Educ Online. 2017;22:1320186. doi:10.1080/10872981.2017.1320186
11. Mustafa S, Stoller JK, Bierer SB, Farver CF. Effectiveness of a leadership development course for chief residents: a longitudinal evaluation. J Grad Med Educ. 2020;12:193–202. doi:10.4300/JGME-D-19-00542.1
12. Lim CT, Harris ZB, Caan MP. A psychiatric residency in the era of COVID-19: a bionian perspective. Psychodyn Psychiatry. 2020;48:259–270. doi:10.1521/pdps.2020.48.3.259
13. Shapiro MA. Competence vs. identity, trainees vs. physicians: how COVID-19 has highlighted role confusion in residency training. Acad Psychiatry. 2021;45:545–548. doi:10.1007/s40596-020-01346-2
14. Richards M, DeBonis K. Psychiatric training during a global pandemic: how COVID-19 has affected clinical care, teaching, and trainee well-being. Psychiatr Serv. 2020;71:1300–1302. doi:10.1176/appi.ps.202000277
15. Rakowsky S, Flashner BM, Doolin J, et al. Five questions for residency leadership in the time of COVID-19: reflections of chief medical residents from an internal medicine program. Acad Med. 2020;95:1152–1154. doi:10.1097/ACM.0000000000003419
16. Chochol MD, Pease E, Swintak C, Anand U. Addressing well-being, burnout, and professional fulfillment in child and adolescent psychiatry trainees during the COVID-19 pandemic through implementation of a virtual Balint-like group: a pilot study. Acad Psychiatry. 2021;45:581–586. doi:10.1007/s40596-021-01488-x
17. Schwartz AC, Brenner AM. Psychiatric education and COVID-19: challenges, responses, and future directions. Acad Psychiatry. 2021;45:535–538. doi:10.1007/s40596-021-01530-y
18. Ruble AE, Romanowicz M, Bhatt-Mackin S, Topor D, Murray A. Teaching the fundamentals of remote psychotherapy to psychiatry residents in the COVID-19 pandemic. Acad Psychiatry. 2021;45:629–635. doi:10.1007/s40596-021-01484-1
19. Heldt JP, Agrawal A, Loeb R, Richards MC, Castillo EG, DeBonis K. We’re not sure we like it but we still want more: trainee and faculty perceptions of remote learning during the COVID-19 pandemic. Acad Psychiatry. 2021;45:598–602. doi:10.1007/s40596-021-01403-4
20. Miles RH. Organization boundary roles. In: Cooper CL, Payne R, editors. Current Concerns in Occupational Stress. New York: John Wiley & Sons Inc; 1980:61–96.
21. Antonioni D. Relationship between the big five personality factors and conflict management styles. Int J Conflict Manage. 1998;9:336–355. doi:10.1108/eb022814
22. Kakarala SE, Prigerson HG. Covid-19 and increased risk of physician suicide: a call to detoxify the US medical system. Front Psychiatry. 2022;13:791752. doi:10.3389/fpsyt.2022.791752
23. Ragu-Nathan TS, Tarafdar M, Ragu-Nathan BS, Tu Q. The consequences of technostress for end users in organizations: conceptual development and empirical validation. Inf Syst Res. 2008;19:417–433. doi:10.1287/isre.1070.0165
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.