")
Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 14
Evidence-Based Consensus Recommendations for Skin Care in Healthy, Full-Term Neonates in India
Authors Gupta P , Nagesh K, Garg P, Thomas J, Suryawanshi P, Sethuraman G , Hazarika RD, Verma RJ , Kumar CS, Kumari S, Taneja S, Chavhan V, Thakor P, Pandita A
Received 26 April 2023
Accepted for publication 3 August 2023
Published 25 August 2023 Volume 2023:14 Pages 249—265
DOI https://doi.org/10.2147/PHMT.S414091
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Laurens Holmes, Jr
Piyush Gupta,1,* Karthik Nagesh,2,* Pankaj Garg,3,* Jayakar Thomas,4,* Pradeep Suryawanshi,5,* Giridhar Sethuraman,6,* Rashna Dass Hazarika,7,* Rahul J Verma,8,* C Suresh Kumar,9,* Shantha Kumari,10,* Sunil Taneja,11,* Vaishali Chavhan,12,* Priti Thakor,13,* Ankita Pandita13,*
1Department of Pediatrics, University College of Medical Sciences, New Delhi, India; 2Department of Neonatology, Manipal Hospitals Group (MHEPL), Bangalore, Karnataka, India; 3Department of Neonatology, Sir Ganga Ram Hospital, New Delhi, India; 4Department of Dermatology, The Tamil Nadu Dr. M.G.R. Medical University, Chennai, Tamil Nadu, India; 5Department of Neonatology, BVU Medical College, Pune, Maharashtra, India; 6Department of Neonatology, Chettinad Hospital and Research Institute, Chennai, Tamil Nadu, India; 7Department of Pediatrics & Neonatology, Nemcare Superspecialty Hospital, Guwahati, Assam, India; 8Department of Neonatology & General Pediatrics, Sir H.N Reliance Hospital, Mumbai, Maharashtra, India; 9Department of Pediatrics, Apollo Cradle, Jubilee Hills, Hyderabad, Telangana, India; 10Department of Obstetrics and Gynecology, Yashoda Hospitals, Hyderabad, Telangana, India; 11Sushrut Medical Centre Pvt Ltd, Kanpur, Uttar Pradesh, India; 12Department of Obstetrics and Gynecology, Sahyadri Superspecialty Hospitals, Pune, Maharashtra, India; 13Department of Medical Affairs, JNTL Consumer Health (India) Pvt. Ltd., Mumbai, Maharashtra, India
*These authors contributed equally to this work
Correspondence: Ankita Pandita, JNTL Consumer Health (India) Pvt. Ltd., 501 Arena Space, Behind Majas Bus Depot, off Jogeshwari Vikhroli Link Road, Jogeshwari (E), Mumbai, 400060, India, Tel +91 98735 98808, Fax +91-22 25643410, Email [email protected]; [email protected]
Purpose: Neonatal skin care practices guided by personal experience and preferences might be substantially different across different hospital settings. The aim of this consensus recommendation is to provide clinical practice guidance to healthcare practitioners on evidence-based neonatal skin care practices from delivery-to-discharge, in hospital settings.
Patients and Methods: A Scientific Advisory Board meeting on “Evidence-based Neonatal Skin Care Practices and Protocols” was held in December 2020 with an expert panel comprising neonatologists, pediatricians, obstetricians and gynecologists and pediatric dermatologist. Comprehensive literature search was performed up to 23 March 2021 using PubMed and Google Scholar to retrieve relevant evidence.
Results: Recommendations were developed on critical aspects of skin care in healthy full-term neonates including cleansing at birth, skin-to-skin care, cord care, diaper area care, initial and routine bathing, cleansers and emollients use, and criteria to choose appropriate skin care products. Recommendations include inclusion of skin assessment in routine neonatal care, first bath timing after cardio-respiratory and thermal stabilization, 6– 24 hours after birth; bathing with water alone or adding a mild liquid cleanser could be considered appropriate as it does not impact the developing skin barrier; use of emollients is recommended for neonates with higher risk of development of eczema to maintain and enhance skin barrier function and integrity; and inclusion of skin care advice in neonatal discharge checklist. Importance of rigorous quality control, high-quality clinical trials for assessment of baby products, usage of products that are formulated appropriately for newborns, and full label transparency for baby products were highlighted. The panel identified gaps in literature and discussed the scope for future research.
Conclusion: These recommendations may help to standardize evidence-based skin care for healthy full-term neonates in Indian hospital settings to improve the quality of care that neonates receive in hospital and facilitate improvement in overall neonatal health outcomes.
Keywords: baby products, bathing, cleanser, emollient, hospital setting, neonatal skin care practices
Introduction
The growing trend in institutional deliveries at hospitals or primary health centers, compared to home births in India has extensively improved newborn survival over the past few decades.1,2 Increased facility births have considerably enhanced the opportunity to deliver essential care to every newborn. Accelerated progress for improved neonatal health outcomes and survival requires the strengthening of the quality of care in institutional setups.3 According to the World Health Organization (WHO), neonatal skin care forms an integral part of ‘Essential Newborn Care’.4
The neonatal skin undergoes significant developmental changes during the transition from an aquatic in utero to an aerobic extrauterine environment. Accordingly, the adaptation is facilitated by several vital functions, including thermoregulation, water and electrolyte homeostasis, and protection against trauma, environmental toxins, and infections.5,6 The skin barrier is considered as a multifaceted structure comprising the microbiome, chemical, physical and immune barriers.7 Full-term infants are born with a competent skin barrier; however, continual normal, healthy development during the postnatal period requires specific dermatological care.5 Skin care practices can influence skin integrity, acid mantle, skin microbiome diversity, immunomodulation, and prevention of infection.6,8 The far-reaching effects of skin care practices extend beyond the physical barrier and encompass neurodevelopmental outcomes of the neonate.9
There exists a substantial variability in skin care practices being followed across Indian clinical settings and the majority of the practices employed have been derived from individual experience, rather than evidence-based research. Moreover, in India, several traditional and regional practices are widely followed that may compromise skin function and newborn health.10,11 Thus, there is a need to develop evidence-based consensus recommendations on neonatal skin care by the experts in the field and facilitate their implementation within Indian hospital settings as well as in domestic settings after discharge.
To this end, a Scientific Advisory Board meeting was conducted with the objectives of developing consensus recommendations on evidence-based neonatal skin care practices and designing corresponding protocols; the ultimate aim was to achieve positive health outcomes. These recommendations describe a) the approach to facilitate the adoption of evidence-based skin care practices for full-term healthy neonates within hospital settings, b) provide insights to the healthcare practitioners on the selection and use of appropriate dermatological products for newborns c) areas of limited evidence, with a need and scope for future research. In addition, implementation of the recommendation across institutions might result in new information or data to further support the neonatal skin care practices.
Methods
The Scientific Advisory Board meeting on “Evidence-based Neonatal Skin Care Practices and Protocols” was held on December 12, 2020 on a virtual meeting platform. The expert panel included nationally renowned neonatologists, pediatricians, obstetricians and gynecologists and a pediatric dermatologist. The discussion was focused on current neonatal skin care practices and protocols, the review of existing evidence, the appropriate selection and use of skin care products, the approach to facilitate the adoption of documented protocols within hospitals, identifying gaps in current evidence, and the scope for evidence generation. The meeting involved extensive discussions and inputs regarding specific questions that were developed a priori and communicated beforehand to all panel members; each set of questionnaires was answered by an e-mail. The results were discussed; subsequently, the experts arrived at a consensus based on the available evidence, their collective experiences, and expertise.
The literature search, comprising observational studies, randomized controlled trials, review articles, and meta-analyses in full-term healthy neonates that evaluated the skin care practices was performed using the PubMed and Google Scholar databases on 23 March 2021. The search terms employed were “baby/newborn/neonate/infant”, “skin care”, “dermatology”, “bath/bathing/washing/cleaning”, “WHO”, “guidelines/recommendations”, “umbilical cord care”, “nappy care”, “diaper rash”, “cleanser/baby wash”, “emollient/cream/moisturizer”, “oil”, “massage”, “tactile stimulation”, “multisensory stimulation”, “skin-to-skin care”, “baby products”. The search was restricted to articles in the English language published in February 2021 or prior. However, newer literature, which has relevance to these study recommendations, were also included.
The abstracts and the full text of the studies were screened to find out the relevant article for each section of the manuscript that discussed the outcomes of skin care interventions and practices in full-term healthy neonates. All members participated in the preparation and review of the draft. Following the incorporation of all suggestions, the consensus recommendations were finalized (Table 1).
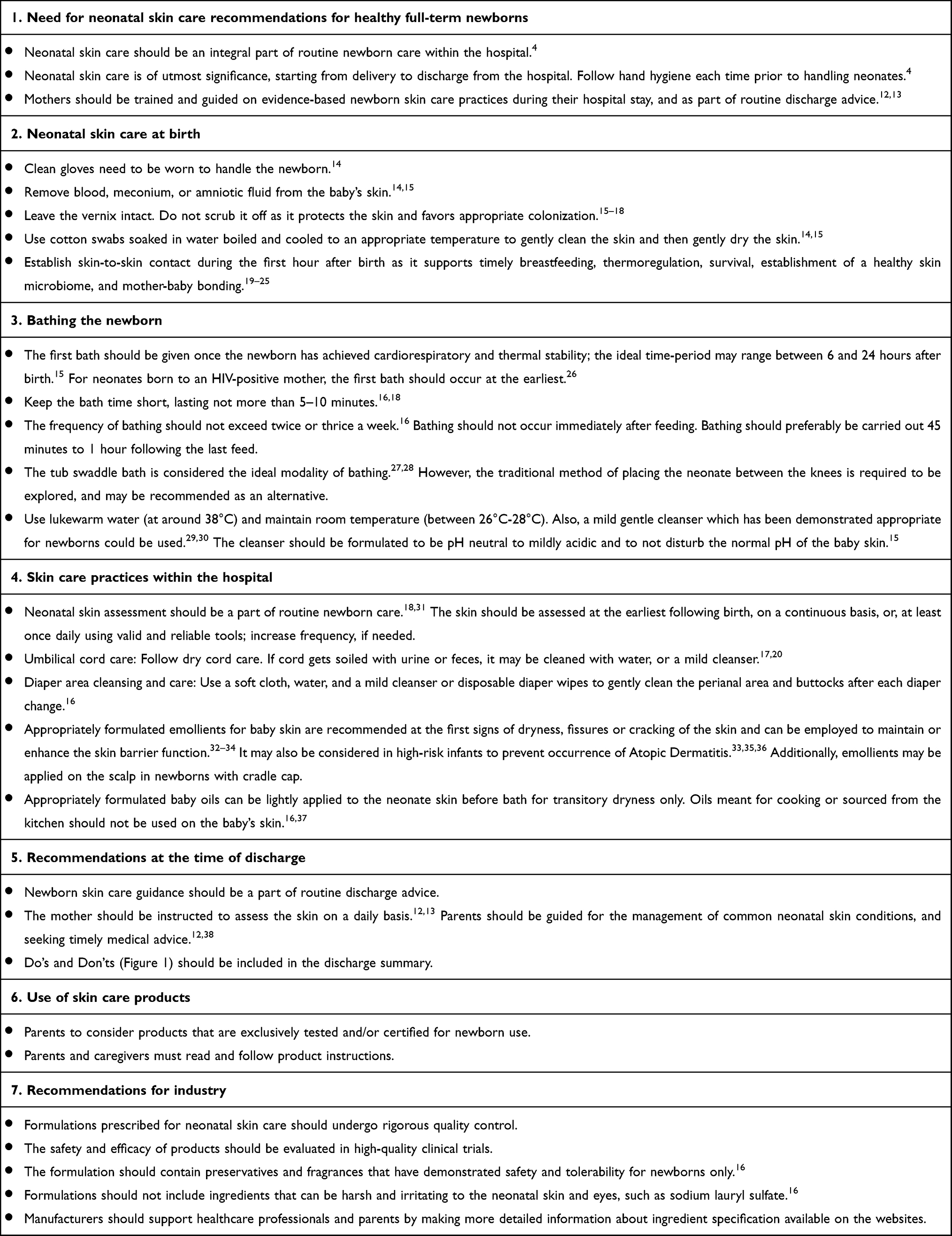 |
Table 1 Summary of Key Consensus Statements |
 |
Figure 1 Do’s and don’ts included in the discharge summary. |
Results
Need for Neonatal Skin Care Recommendations for Healthy Full-Term Newborns
Points of Discussion
Proper care and maintenance of hygiene are essential to improve overall neonatal health and skin integrity.6 Hand hygiene (by hand washing or the use of alcohol-based hand rub) should be ensured before handling the neonate.14 Owing to limited data and the absence of uniform guidelines, skin care practices in healthy full-term newborns are primarily based on experience; physicians, nurses, and other medical staff seek such guidance from non-evidence-based sources.39 The United States-based cohort revealed wide variations in the neonatal skin care practices followed across medical centers and specific populations; these may even be contrary to the best practices documented in the literature.40 The contrary practices include baby’s first bath before cardiorespiratory and thermoregulatory stability is achieved, removal of all vernix after birth, no routine use of emollient, no use of any products in diaper area during diaper change, no use of antiseptics for the umbilical cord, and not following any specific skin care protocol to avoid skin breakdown and infections.40 These disparities highlight the need for data-driven guidelines on standardized and optimized neonatal skin care. All panel members agreed to neonatal skin care should be an integral part of routine newborn care; an unmet need exists for uniform evidence-based neonatal skin care guidelines in hospital settings. Furthermore, the panel emphasized the key barriers to the adoption of evidence-based skin care practices. These include lack of guidelines from centralized bodies, lack of cross-specialty coordination, lack of infrastructure, paucity of trained staff, and the preferential allocation of resources to the more critical aspects of neonatal care.
Neonatal Skin Care at Birth
Points of Discussion
Cleansing the Neonate Soon After Birth
The Ministry of Health and Family Welfare (MoHFW), Govt. of India recommends that gloves and a plastic/rubber apron should be worn while handling the neonate until blood, meconium or amniotic fluid has been removed from the neonate’s skin.14 Blood and meconium should be gently removed from the neonate’s skin using cotton swabs/soft cotton soaked in boiled warm water, followed by drying to avoid infection. Vigorous scrubbing should be avoided.14,15
Vernix Caseosa
The vernix caseosa (vernix) is a protective layer comprising proteins, lipids, and water; it acts as a natural moisturizer and skin cleanser. It protects the fetal skin from the amniotic fluid in utero. Following birth, it helps reduce the trans-epidermal water loss (TEWL) and facilitates acid mantle formation. Additionally, it delivers antioxidant, antimicrobial, and antifungal benefits to the newborn skin.5,41 Considering these benefits of the vernix, the WHO, the Association of Women’s Health, Obstetric and Neonatal Nurses (AWHONN), the European Roundtable meeting on Best Practice Healthy Infant Skin Care, and the recent pediatric skin care guidelines developed by the Indian Academy of Pediatrics (IAP) strongly recommend leaving the residual vernix intact on the neonatal skin in the period following birth.15–18
Skin-to-Skin Care
The WHO, the United Nations International Children’s Emergency Fund (UNICEF), and the pediatric skin care guidelines developed by IAP strongly recommend establishing skin-to-skin contact between all mothers and neonates without complications during the first hour after birth.18–20 This helps prevent hypothermia, stimulates breastfeeding, enhances mother-baby bonding and maternal satisfaction, reduces newborn stress, enables colonization of the neonatal skin with beneficial maternal bacteria, and promotes maturation and functioning of the immune system.19–25
Bathing the Newborn
Points of Discussion
The First Bath ‒ Timing
The first bath is often scheduled around the activities of the mother and newborn, the time and mode of delivery, competing for scheduling priorities (including discharges at, or, before 24 hours), and the availability of primary care nurses to guide the parents; cultural beliefs may also play a part.42–45 Table 2 summarizes various studies comparing the effect of different timings of the first bath on neonatal thermoregulatory status. Studies have demonstrated no significant impact on infant axillary temperatures, when bathing healthy newborns at different time points, from 1 hour up to 9 hours after birth.45–49 However, a study conducted in Uganda demonstrated bathing term newborns at 1 hour of age significantly increases the risk of hypothermia, despite the use of warm water and skin-to-skin care following the bath.50 In contrast, according to a study from Japan, the neonate bath occurring as early as 2 to 5 minutes after birth was reported to be safe; a significantly higher temperature was observed 30 minutes following the bath, compared to the dry care group.51 A large observational study in the Philippines found that early bathing delays thermoregulation and initiation of breastfeeding.52 Another randomized controlled study demonstrated that delaying the first bath to 48 hours postpartum, has a positive effect on preserving the body temperature and the skin moisture level of the neonate.53 A few other studies also suggested that delaying the first bath encourages successful breastfeeding, enhances bonding, and facilitates timely skin-to-skin care.54–57 Globally, variations exist in the timing of the first bath; however, maintaining the neonatal thermoregulation is of primary importance. Therefore, the first bath should be given only after the infant has achieved cardiorespiratory and thermal stability.15,16,58
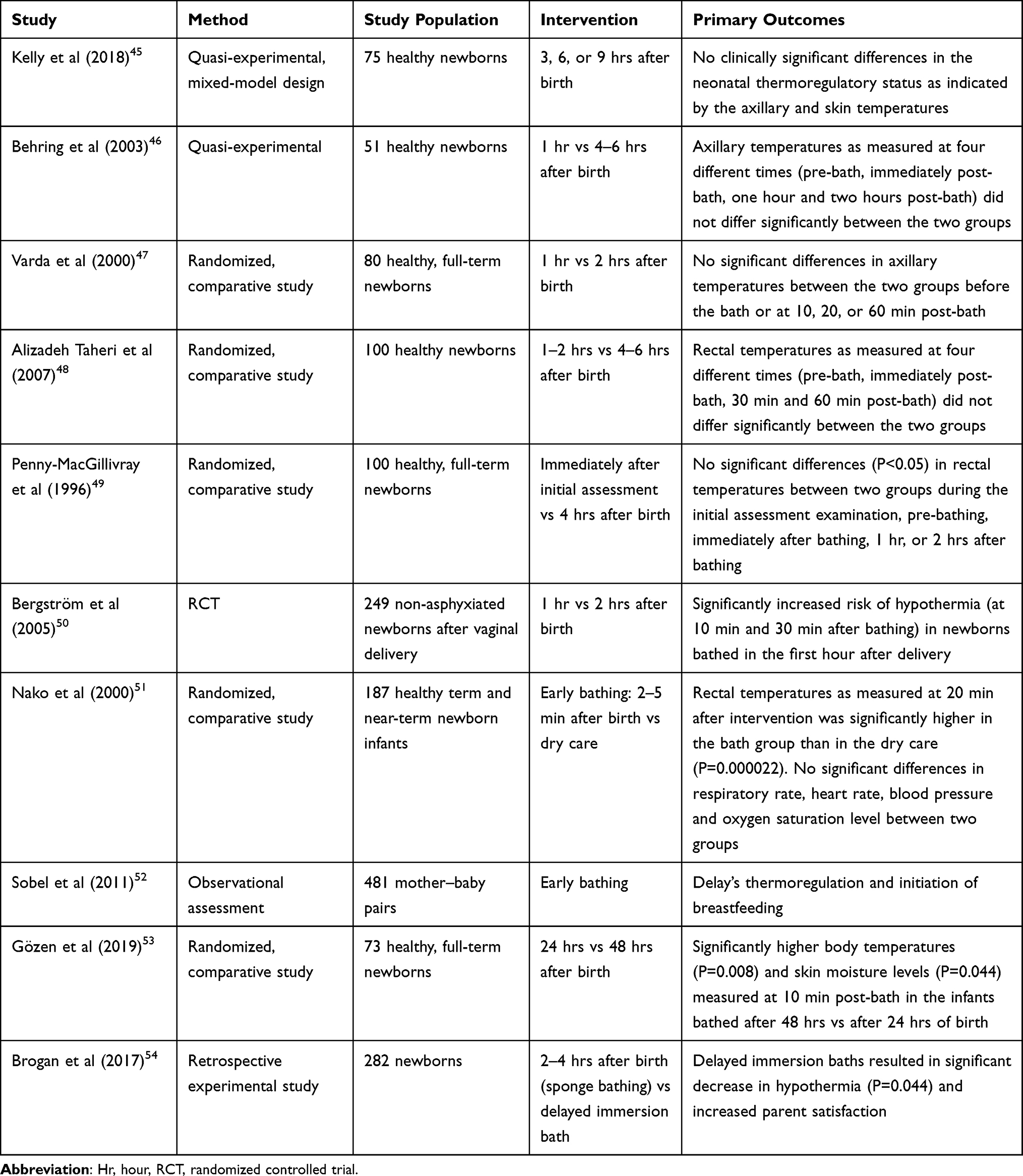 |
Table 2 Studies Comparing the Effect of Different Timings of the First Bath on Neonatal Thermoregulatory Outcome |
The Neonatal Skin Care Evidence-Based Clinical Practice Guideline, developed by the AWHONN, recommends the first bath as occurring between 6 hours and 24 hours after birth.15 For infants born to a human immunodeficiency virus (HIV)-positive mother, the first bath should occur at the earliest, following birth, to prevent the transmission of maternal infection to the newborn.26 The WHO recommends delaying the bath for 24 hours after birth; if cultural reasons do not permit such a delay, wait for a minimum of 6 hours.20 All panel members agreed the first bath in full-term neonates should be given once thermal and cardiorespiratory stability has been achieved (approximately 6 hours after birth), provided the temperatures of the hospital settings and the bath water are carefully monitored.
The First Bath ‒ Frequency and Duration
The European Roundtable Meeting on Best Practice Healthy Infant Skin Care recommends neonatal baths should be conducted at least 2–3 times a week or as frequently as local culture requires.16 The duration of the bath should not last more than 5 minutes; prolonged duration increases the hydration of the skin and reduces the threshold for friction.59,60 The European Roundtable Meeting on Best Practice Healthy Infant Skin Care and the IAP recommend the duration of the infant bath should not exceed 5–10 minutes.16,18
Soaking in water (with or without cleansers) removes natural moisturizing factor (NMF) from the stratum corneum, and results in brittle and dry skin.61 As NMF is low at birth and contributes to the acid mantle, removal of NMF may impact skin pH and colonization of the skin surface with appropriate bacteria in newborns.
Mode of Bathing
Several methods of providing the first bath to newborns are practiced in hospital settings. Sponge bathing is the act of washing using a sponge or a washcloth. It is frequently administered at birth, or within a few hours subsequently.27,43 In tub or immersion bathing, the entire body of the infant (except the head and neck) is placed in warm water (approximately 38°C). This is deep enough to cover the shoulders, being more comfortable for the baby.43 In swaddled immersion bathing, infants are swathed in a soft blanket and gently immersed in a tub of warm water.44 The water covers up to the baby’s shoulders. Each limb is individually unswaddled, washed, rinsed, and reswaddled. The water immersion, combined with the swaddling, has been shown to reduce stress during bathing.
Compared to sponge bathing, newborns who experienced tub (immersion) baths demonstrated reduced temperature variability;27,28 additionally, they cried less and were found to be calmer and more content (Table 3).27 Newborns receiving delayed immersion baths had a significantly higher likelihood of experiencing normothermia compared to a sponge bath shortly after birth.54 Differing opinions exist if the baby should be bathed until the umbilical cord falls off, and the preferred method of bath. Traditionally, sponge bathing is preferred until the cord falls off; tub bathing is favored subsequently. However, studies demonstrated no differences in the rates of umbilical cord healing between the tub and sponge-bathed neonates; additionally, no increase in umbilical cord infections was reported through either of the methods.27,39 This suggests sponge bathing has become incorporated as part of routine newborn care without adequate high-quality evidence. Studies report that swaddled immersion bathing, compared to sponge or tub bathing, effectively maintains body temperature, oxygen saturation levels, and heart rate, and reduces behavioral stress symptoms, such as crying and agitation, improving maternal satisfaction (Table 3).62–67 Thus, swaddling with immersion can be adopted as part of routine newborn care for term infants during the hospital stay.
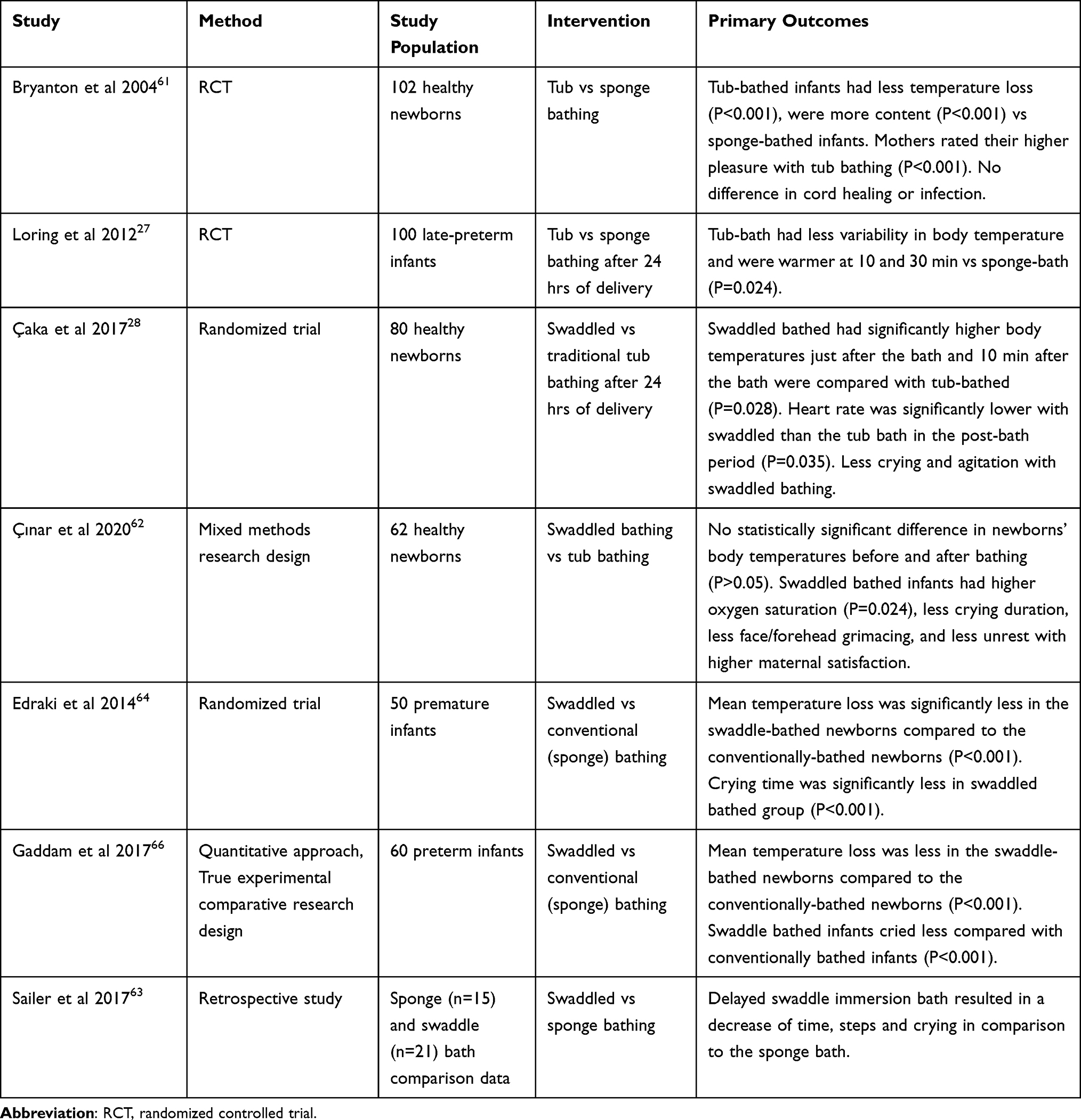 |
Table 3 Studies Comparing Different Bathing Techniques for the First Bath |
All panel members agreed the swaddle immersion method is the ideal technique for bathing healthy term newborns. However, one panelist suggested certain adaptions might be necessary while incorporating the method in Indian hospital settings. These include factors, such as training the staff, time constraint, etc. Another panel member suggested conventional or regional practices like bathing the baby on outstretched legs are required to be explored; this was agreed by all members.
Use of Water Alone vs Mild Cleanser
Randomized studies and systematic literature reviews exhibited clinically equivalent results, upon comparing mild liquid cleansers to water alone for bathing.39,68–70 The exclusive use of water may not be sufficient for the removal of impurities like urine components, fecal enzymes, and fat-soluble surface impurities like fecal remnants.29,30 Having said that, the panel members agreed water alone would be sufficient for newborn bathing unless concerns exist regarding the water quality. Furthermore, a mild cleanser demonstrated appropriate for use on newborns would be recommended for situations requiring bathing of the baby post-massage, or being soiled with dirt, vomitus, feces, etc.
Skin Care Practices Within the Hospital
Points of Discussion
Assessment of the Skin of the Neonate
A comprehensive examination of the newborn skin from head to toe is essential; this includes parameters, such as dryness, scaling, erythema, color, texture, and physiological changes.18,31 Some of the standardized tools including Neonatal Skin Condition Score (NSCS), Neonatal Skin Risk Assessment Scale (NSRAS) and Braden Q scale can be considered for neonatal skin assessment. NSCS ranges from a score of 3 (best condition) to 9 (worst condition), based on dryness, erythema, and skin breakdown (Table 4).31 NSRAS is composed of six subscales (general physical condition, mental state, mobility, activity, nutrition and moisture) and scored 6 to 24 (each subscale is scored 1 point), with a higher score indicative of lower risk. Braden Q scale composed of seven subscales (mobility, activity, sensory perception, moisture, friction/shear, nutrition and tissue perfusion) with scores 1 (least favorable) to 4 (most favorable). Scores <16 implies risk of skin breakdown. NSCS assist nurses or primary caregivers in identifying risk factors for impaired skin integrity, NSRAS considers the physical and developmental requirements of neonatal patients, and Braden Q scale predicts the risk of pressure ulcers.71,72 Visscher M described a skin assessment tool (grading template) that compares the severity of erythema (9-point, 0–4 scale with 0.5 grade increments), dryness (11-point, 0–5 scale with 0.5 grade increments) or rash (7-point, 0–3 scale with 0.5 grade increments) to the normal skin of same person for the rapid measurement of skin condition in NICUs.73 All panel members agreed skin assessment should be included as part of the routine newborn analysis, and NSCS is a suitable tool for the same. Based on the arrived consensus, the NSCS assessment should be performed once neonatal thermal stability has been achieved; the evaluation can be carried out by the pediatrician, nurse, or even potentially the mother with guidance and/or training. The assessment should be undertaken once daily, or, more frequently as clinically indicated, until discharge; new parents should be advised to continue the evaluation at home. Furthermore, panel members insisted the routine checklist for neonatal skin care for the hospital nursing staff should include the NSCS assessment, cleansing, umbilical cord care, diaper area assessment, emollient usage, and identifying risk factors for skin breakdown.
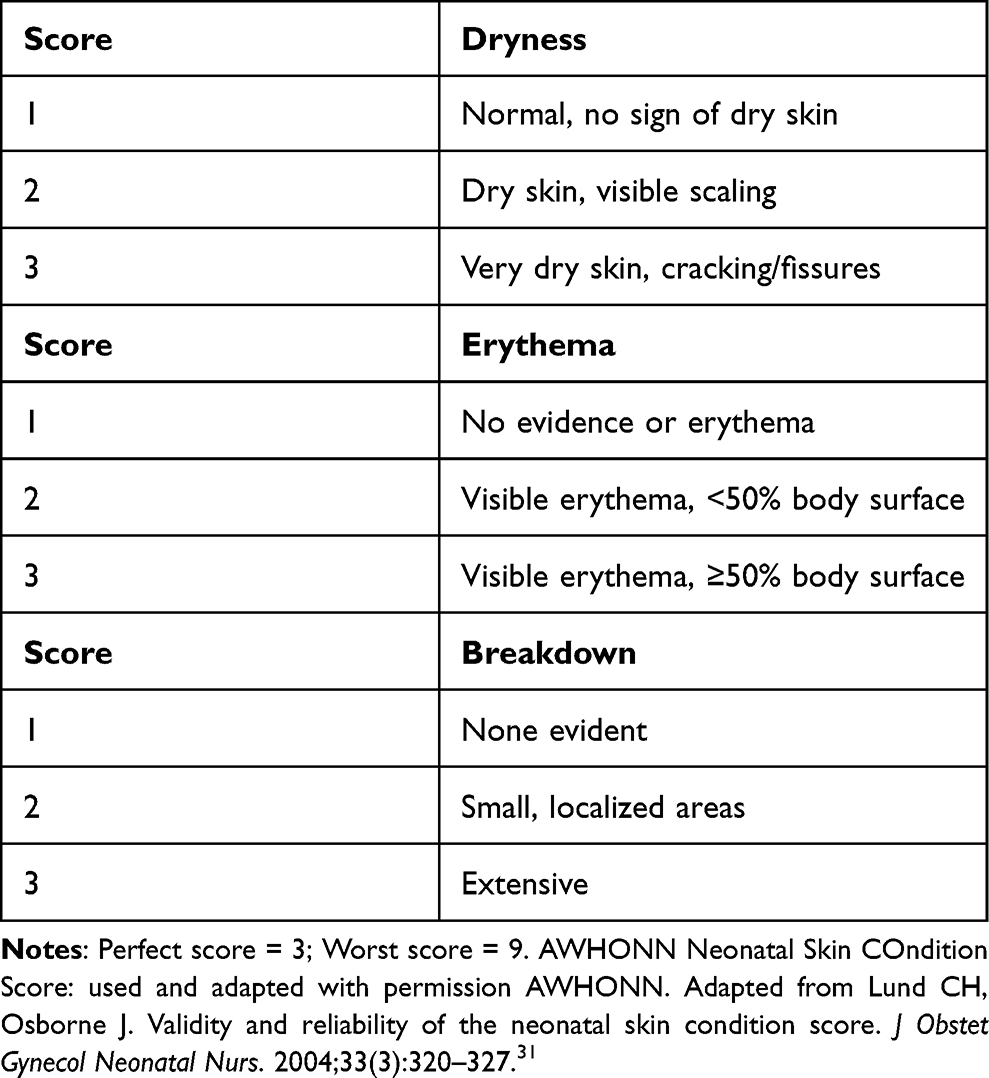 |
Table 4 Neonatal Skin Condition Score (NSCS) |
Umbilical Cord Care
The WHO recommends clean and dry cord care for neonates born in health facilities; hand hygiene is to be followed. If soiled, the cord stump should be washed with water and a mild cleanser and dried thoroughly with a soft, clean cloth. Nothing should be applied to the stump.17,20 However, further research is recommended to evaluate topical antimicrobial treatment for umbilical cord care compared to natural healing.74
Diaper Area Care
Considering the risk of diaper dermatitis, the perianal area should be kept clean and dry; diapers should be changed as often as necessary.15,16 The European Roundtable Meeting on Best Practice Healthy Infant Skin Care recommends diaper wipes should contain buffers to maintain the pH at slightly acidic to neutral. Additionally, the wipes should be free of potential irritants, such as alcohol, and harsh surfactants (eg, sodium lauryl sulfate), and must contain well‐tolerated preservatives and if they contain fragrance, the wipes should be demonstrated non-irritating and well tolerated for use on newborn.16 Drying can be achieved through air‐drying, or gentle patting with a dry towel or a soft cloth to avoid scrubbing that can result in barrier disruption.16 The application of barrier creams containing an appropriate percentage of zinc oxide and petrolatum-based formulations can treat and help prevent diaper dermatitis.75
Emollient Therapy
According to randomized studies, emollient therapy represents a safe and effective approach to reduce TEWL, increase the stratum corneum hydration and was shown in a study to improve the skin microbial richness. In turn, this helps maintain the overall skin barrier integrity.32–34 The role of early use of emollients in prevention of atopic dermatitis (AD) remains inconclusive. While certain literature reported daily application of emollient from birth reduced the occurrence of AD in high-risk patients without increasing risk of food sensitization;33,35,36 the evidence to support this is equivocal with certain studies providing contradictory conclusions as well.9–11 This difference in the results may be attributed to the difference in the study design, study population and the timing of intervention. Hence, further robust interventional clinical trials are required to establish a strong recommendation for the same.
Recommendations at the Time of Discharge
Points of Discussion
Massage Therapy and Multisensory Stimulation
Multiple studies suggest infant massage may display beneficial effects on weight gain, growth, sleep and crying patterns, physiological responses to stress (including reductions in the levels of serum norepinephrine and epinephrine, and urinary cortisol), establishing circadian rhythms through an increase in the secretion of melatonin, decrease in hyperbilirubinemia, and improving mother–baby interaction. Many of these studies have been conducted on preterm infants.76–82 An Indian study conducted on 125 healthy term infants displayed improvement in growth and post-massage sleep.83 A randomized controlled study completed with 191 newborns (94 preterm, 97 term) in a Mumbai-based tertiary care center reported a significant increase in weight gain velocity in term neonates receiving massage with oil compared to the control group.84 In addition, massage using oil has been shown to help lower cortisol levels, reducing stress behavior in babies.18
Massage may be combined with other types of stimulation, such as soothing talk (auditory stimulation), gentle extension and flexion of the limbs (kinesthetic stimulation), etc. The multisensory (auditory, tactile, visual, and vestibular) stimulation has been shown to improve infant growth and reduce stress, as determined by salivary cortisol levels in healthy term newborns.85,86
Discharge Summary
Discharge advice and guidance for new parents are critical in ensuring evidence-based neonatal skin care practices are adhered to at home. Considering the lack of awareness, confusion, and fear among parents regarding the best skin care practices for the newborn, the postpartum nursing staff plays a key role.12,38 Following delivery, the discharge of a healthy term newborn offers an important opportunity to counsel new parents regarding routine neonatal skincare and its significance, with emphasis on evidence-based recommendations.12,38 All panel members agreed that skin care advice should be part of the newborn discharge checklist. Accordingly, mothers or caregivers are required to be educated and trained on certain practices, such as massage, bath time basics, emollient use, hair and scalp care, dry cord care, diaper area care, product advice with respect to standards and characteristics, detection and management of common conditions, warning signs, and follow-up advice.12,13 Additionally, specific practices possibly harming the fragile skin of the newborn should be avoided, such as the application of kajal in the eyes, inserting oil in the ears and nose, the use of abrasives for massage, applying cow dung to the umbilical cord, etc.11,20,87
Use of Skin Care Products
Points of Discussion
All panel members agreed that products used for newborn care should be appropriately formulated and demonstrated to be safe and well tolerated and with special attention paid to the use of dyes, preservatives, fragrances, and new ingredients, whether natural or synthetic. All ingredients in a product should be well characterized and appropriate for newborn use and the full product should be appropriately evaluated and tested.
Further, the panel strongly insisted that products labeled as “herbal”, “green”, “natural” or “organic” should not be accepted blindly. The ingredients in such products may not be defined uniformly by regulatory bodies. The characteristics of an ideal cleanser have been provided in Figure 2.
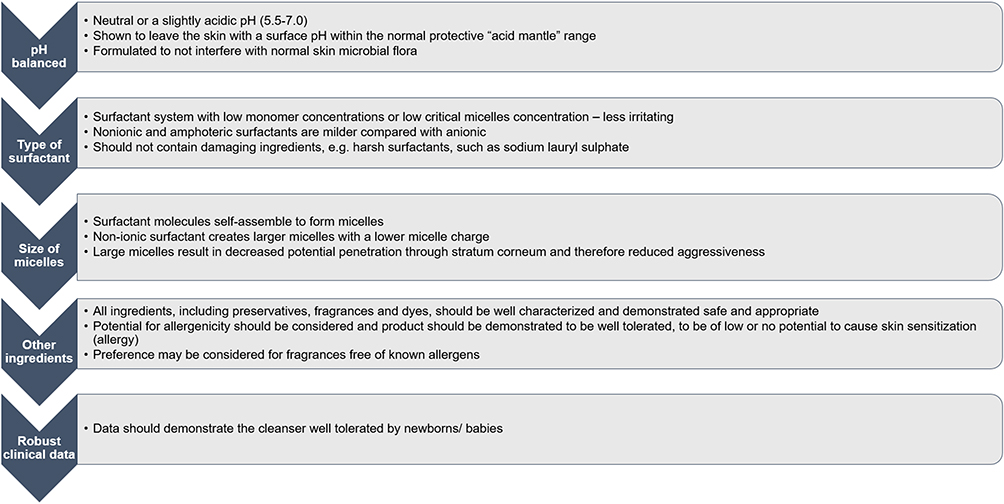 |
Figure 2 Characteristics of an ideal cleanser* for infant skin. Notes: *Water alone would be sufficient for newborn bathing unless concerns exist regarding the water quality. Mild cleansers are required for the removal of urine components, fecal enzymes and fat-soluble surface impurities, such as, fecal remnants. |
Cleanser Formulation
Cleansers can interact with skin in various ways, so mild and gentle cleansing for babies requires multiple considerations. Liquid cleansers having a mildly acidic or neutral pH (range: 5.5–7) are preferred over alkaline agents, which can disrupt the skin surface pH and lipids.18,88 The addition of emollients to liquid cleansers may provide the combined advantage of hydration and protection.88 Additionally, mild baby soaps made from natural oils (typically, the saponification of coconut oil) may be considered for use with evidence of demonstrated safety and tolerability. Fragrance, preservatives, or dyes should be assessed like the other ingredients for their appropriate use and the full product should be demonstrated as safe and well tolerated.
Factors Affecting Cleansers
pH: Gfatter et al studied the pH influence of three cleansing regimens (liquid detergent pH 5.5; compact detergent pH 5.5; alkaline soap bar pH 9.5), comparing each to washing with water alone (control). The alkaline bar displayed the greatest influence on the skin, with a significant increase in the pH and a higher loss of fat. This caused a disruption in the skin acid mantle, compromising the physiological protective function, and changing the resident bacterial flora. Further, the loss of fat affected the hydration of the skin, resulting in dryness.89 Therefore, extra precaution should be taken in selecting the most suitable soaps (liquid or classic), or soapless synthetic detergents (syndets).90 Appropriately formulated cleansers wash effectively while maintaining the skin surface pH; the skin barrier is preserved, conserving the skin microbial diversity.34,70
Type of surfactants: Surfactants act by decreasing the surface tension between water and air, and create lather, allowing emulsification and removal of oils and other fat-soluble impurities from the skin surface. The type of surfactant used in the cleanser determines foaming action and mildness.91 Nonionic and amphoteric surfactants are typically milder compared to anionic components.30,90,92 Surfactants in cleansers can potentially weaken the skin barrier, increase TEWL, and reduce stratum corneum hydration, which in turn can lead to skin dryness, irritation, and redness when the product is not designed considering the critical requirements of mildness and skin compatibility.30,91 The micelle size and shape, nature and concentration of surfactants, and a number of free monomers determine the stratum corneum penetration and the irritation potential of cleansers. Recently introduced hydrophobically modified polymers form larger, more stable structures; these are less likely to penetrate the skin, maintaining the integrity of the barrier.30,92
Size of micelles: Nonionic surfactants result in substantial micelles with a lower micelle charge, and are considered to be mild and safe for neonates.30 Anionic surfactants, such as sodium lauryl sulfate form smaller micelles; these result in skin irritation compared to amphoteric and nonionic surfactants like polyethylene glycol-80 (PEG-80) sorbitan laurate (milder due to micelle stabilization and size).30,90
Gentleness score: Anwar et al proposed a scoring system (5 stars rating for gentleness) to help differentiate the gentleness of cleansing products. This scoring system is based on formulation characteristics (presence of mildness enhancers, absence of allergens and sensitizers, and pH; each equal weightage and contributes 2.5 star out of 5 star) and in vitro assessment (surface penetration through epidermis and contributes 2.5 star out of 5 star).93 The gentleness score can be estimated by checking the formulation and in vitro characteristics described above.
Hardness of water: Hard water generally contains ionized calcium and magnesium divalent cations at concentrations >120 ppm, and could cause irritation to the skin. Certain anionic surfactants like alkyl sulfates present in syndet cleansers may interact with ionized calcium and magnesium divalent cations, leading to surfactant precipitation and thus modifying the composition of the hard water and potentially reducing the available ions to bind to the skin.94 Therefore, baby cleansers composed of these surfactants could be effective to reduce water hardness and can be ideal for baby bath.94
Emollient Formulations
Baby lotions and creams should maintain a mildly acidic to neutral pH and/or be shown to not alter the natural pH of the skin; specific considerations should be taken regarding their ocular and dermal safety.95 Typically, an emollient consists of actives and excipients (emulsifiers, antioxidants, preservatives). The type of active ingredients (emollient, humectant, or occlusive) and how the product is formulated have been shown to determine the impact on skin barrier.96
Oils as emollients: Oils with the lower oleic acid content and the higher linoleic acid content have demonstrated beneficial effects.91 Oleic acid is a skin penetration enhancer that increases TEWL, indicative of barrier disruption. Vegetable oils, such as mustard, soybean, and olive oil (with a higher oleic acid content) display an adverse effect on the maintenance of skin integrity.91 An increased risk of atopic dermatitis and its exacerbation were reported with the use of olive oil.97 Mustard oil is demonstrated to display adverse effects – increased cutaneous water loss, delayed functional maturation of the skin barrier, and an escalated risk for contact dermatitis due to the presence of allyl isothiocyanate.10,91,98 Oils used for cooking and in the kitchen should be avoided as these are chemically heterogeneous, sensitive to oxidation and light, and possess variable biological activity; unpredictable effects may occur upon topical application.16,37 Contrastingly, mineral oils possess emolliency, occlusion and substantivity and thereby maintain the hydration of the stratum corneum.37 The Indian Academy of Pediatrics Guidelines for Pediatric Skin Care highlighted that mineral oil is an effective skincare moisturizer, which has limited penetration, and can be used safely in infants.18 The characteristics of an ideal emollient have been provided in Figure 3.
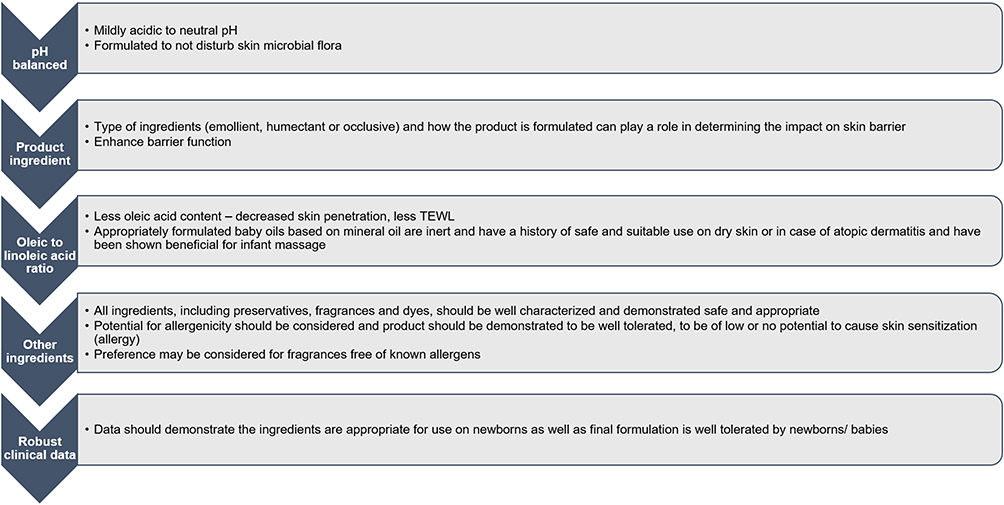 |
Figure 3 Characteristics of an ideal emollient for infants. Notes: TEWL, trans-epidermal water loss. |
Massage Oils
A study conducted by Sankaranarayanan et al displayed oil massage (with coconut oil and mineral oil) resulted in significantly greater weight gain velocity in the term baby group, as compared to the placebo.84 In 2020, an Indian randomized controlled trial validated the efficacy of coconut oil in neonates; enhancement was observed in skin maturity, with a decreased incidence of late-onset sepsis. Thus, hypothermia and apnea were prevented, with enhanced serum vitamin D3 levels and neurodevelopmental outcomes.99 Mustard oil is routinely employed for infant skin massage in the Asian subcontinent; however, its use is not recommended as it slows down the skin barrier recovery, and increases the TEWL.10,100 A recent community study from India did not find any difference in neonatal mortality rate between sunflower seed oil and mustard oil, except in a subgroup of infants weighing ≤1500 g. However, the study highlighted that these results might be due to low adherence to sunflower seed oil application, and further research is needed to establish newborn emollient therapy and its applicability along the continuum of care.101 An abnormal epidermal lipid layering (typical of impaired barrier function), reduced stratum corneum integrity, and an enhanced TEWL following epidermal damage have been observed in neonates treated with olive oil.97 Therefore, the use of olive oil for infant massage and the treatment of dry skin should be discouraged.97
Recommendations for Industry
Points of Discussion
Product Ingredients
All panel members insisted on 100% ingredient transparency for baby products—including fragrances, and all ingredients used in the products should have gone through rigorous evaluation to ensure the safety appropriate for newborn use. Key criteria used to assess baby products are irritancy, pH, ocular safety, and considerations for use of preservatives and fragrance, and potential for skin sensitization (allergenicity). INCIdecoder (https://incidecoder.com/) is an online cosmetics database for consumers to decode the safety and benefits of ingredients present in the product.
Approaches to Facilitate the Adoption of Neonatal Skin Care Protocols Within Hospitals
Standardization of Quality of Care
All panel members regarded the lack of uniform guidelines regarding neonatal skin care from centralized bodies as one of the major barriers to the adoption of evidence-based protocols within hospital settings. Additionally, it was emphasized that such guidelines should be incorporated into clinical practice and the existing structure of the accreditation of the facility.
Creating a Skincare Card
A skincare card may help new mothers follow evidence-based practices at home following discharge. All panel members proposed a need to develop specialized tools and aids, such as educational brochures, multi-vernacular information leaflets, trainings, and visual aids like video links, charts, and pictures to guide new parents and create awareness regarding scientifically documented skin care guidelines.
Evaluating the Outcome and the Impact
The impact of integrating neonatal skin care guidelines as part of routine newborn care can be gauged on the following criteria: Skin barrier integrity parameters (eg, TEWL, stratum corneum hydration, etc.), lower frequency of skin barrier breakdown, reduced skin-related issues during follow-up out-patient department visits, diminished incidence of sepsis or infections, and enhancement in paramedical/nursing staff knowledge (tested using questionnaires).
Literature Gaps and Scope for Future Research
There is a need to develop an appropriate core outcome set for neonatal skin research; these would include benefits over the short-term, as well as, the long-term (hydration, TEWL, skin pH, maternal satisfaction, skin colonization, erythema, etc.). Clear guidelines, with more “real-world” evidence, are needed to address concerns of parents and physicians on skincare practices such as frequency of bathing, type of water being used, hair care, and products being utilized, in particular in the Indian context. There is a need to generate data on traditional care practices that are widely followed across India (eg, the use of turmeric, use of herbal, natural, or organic products). In addition, lack of educational material for new parents, product awareness with respect to standards, characteristics, etc., ideal compositions for cleanser, emollient, or diaper rash cream (eg, zinc oxide content), and effects of the varying quality of water on cleansing were identified among few other areas that warrant further research.
Conclusions
Appropriate neonatal skin care practices support the skin barrier function, as well as, the development and maturation of the newborn skin during the postnatal period. The consensus recommendations may help standardize neonatal skin care in India, facilitating the adoption of evidence-based practices within hospitals. Consequently, a positive impact may be observed on neonatal health outcomes including skin barrier integrity parameters like TEWL and SCH, reduced frequency of skin barrier breakdown along with reduction in skin-related issues during out-patient department visits, and decrease in incidence of sepsis or infections. These recommendations are limited to healthy full-term infants. Future studies are warranted for the populations of preterm neonates and infants born with severe skin diseases.
Abbreviations
AWHONN, Association of Women’s Health, Obstetric and Neonatal Nurses; HIV, Human immunodeficiency virus; IAP, Indian Academy of Pediatrics; MoHFW, Ministry of Health and Family Welfare; NSCS, Neonatal Skin Condition Score; PEG-80, polyethylene glycol-80; TEWL, trans-epidermal water loss; UNICEF, United Nations International Children’s Emergency Fund; WHO, World Health Organization.
Acknowledgments
Akshada Deshpande, PhD and Rabi Panigrahy, PhD, ISMPP provided medical writing assistance, and Sangita Patil, PhD, ISMPP, CMPPTM (all from SIRO Clinpharm Pvt Ltd, India) provided additional editorial support for this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, design, execution, data analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research is funded by JNTL Consumer Health (India) Pvt Ltd. Authors did not receive any financial support from the funder related to this work. The funder did not influence the content of the guideline.
Disclosure
Priti Thakor and Ankita Pandita are employees of JNTL Consumer Health (India) Pvt Ltd. Dr Ankita Pandita reports the advisory board was conducted by JNTL Consumer Health (India) Pvt Ltd. All other authors declare that they have no competing interests.
References
1. Statista Research Department. Number of births by type in India FY 2015-2020; 2021; Available from: https://www.statista.com/statistics/659283/childbirths-by-type-india/.
2. Sankar MJ, Neogi SB, Sharma J, et al. State of newborn health in India. J Perinatol. 2016;36(s3):S3–S8.
3. Bhakoo O. Challenges and opportunities of neonatal care in India. J Pediatrics Assoc India. 2017;6(3):132.
4. World Health Organization. WHO Fact sheets. Newborns: improving survival and well-being; 2020. Available from: https://www.who.int/news-room/fact-sheets/detail/newborns-reducing-mortality.
5. Visscher MO, Adam R, Brink S, Odio M. Newborn infant skin: physiology, development, and care. Clin Dermatol. 2015;33(3):271–280.
6. Darmstadt GL, Dinulos JG. Neonatal skin care. Pediatr Clin North Am. 2000;47(4):757–782.
7. Eyerich S, Eyerich K, Traidl-Hoffmann C, Biedermann T. Cutaneous Barriers and Skin Immunity: differentiating A Connected Network. Trends Immunol. 2018;39(4):315–327.
8. Bouslimani A, da Silva R, Kosciolek T, et al. The impact of skin care products on skin chemistry and microbiome dynamics. BMC Biol. 2019;17(1):47.
9. Chuong CM, Nickoloff BJ, Elias PM, et al. What is the ‘true’ function of skin? Exp Dermatol. 2002;11(2):159–187.
10. Darmstadt GL, Mao-Qiang M, Chi E, et al. Impact of topical oils on the skin barrier: possible implications for neonatal health in developing countries. Acta Paediatr. 2002;91(5):546–554. doi:10.1111/j.1651-2227.2002.tb03275.x
11. Bangari A, Thapliyal SK, Aggrawal B, Sharma U. Traditional beliefs and practices in newborn care among mothers in a tertiary care centre in Dehradun, Uttarakhand, India. Int J Community Med Public Health. 2019;6(2600):
12. Langan RC. Discharge procedures for healthy newborns. Am Fam Physician. 2006;73(5):849–852.
13. Howard County General Hospital. Taking Baby Home. Howard County General Hospital, John Hopkins Medicine; 2010. Available from: https://www.hopkinsmedicine.org/howard_county_general_hospital/_downloads/takingbabyhome_english.pdf.
14. Ministry of Health and Family Welfare, Government of India. National Guidelines for Infection Prevention and Control in Healthcare Facilities; 2020. Available from: https://www.mohfw.gov.in/pdf//National%20Guidelines%20for%20IPC%20in%20HCF%20-%20final%281%29.pdf.
15. Brandon D, Hill CM, Heimall L, et al. Neonatal Skin Care: evidence-Based Clinical Practice Guideline. In: Obstetric and Neonatal Nurses.
16. Blume-Peytavi U, Lavender T, Jenerowicz D, et al. Recommendations from a European Roundtable Meeting on Best Practice Healthy Infant Skin Care. Pediatr Dermatol. 2016;33(3):311–321.
17. World Health Organization. Pregnancy, childbirth, postpartum and newborn care: a guide for essential practice; 2015. Available from: https://www.who.int/maternal_child_adolescent/documents/imca-essential-practice-guide/en/.
18. Madhu R, Vijayabhaskar C, Anandan V, et al. Indian Academy of Pediatrics Guidelines for Pediatric Skin Care. Indian Pediatr. 2021;58(2):153–161.
19. UNICEF. Skin-to-skin contact; 2020. Available from: https://www.unicef.org.uk/babyfriendly/baby-friendly-resources/implementing-standards-resources/skin-to-skin-contact/.
20. World Health Organization. Recommendations on newborn health: guidelines approved by the WHO Guidelines Review Committee; 2017. Available from: https://apps.who.int/iris/handle/10665/259269.
21. Marin Gabriel MA, Llana Martin I, Lopez Escobar A, Fernandez Villalba E, Romero Blanco I, Touza Pol P. Randomized controlled trial of early skin-to-skin contact: effects on the mother and the newborn. Acta Paediatr. 2010;99(11):1630–1634.
22. Moore ER, Anderson GC, Bergman N, Dowswell T. Early skin-to-skin contact for mothers and their healthy newborn infants. Cochrane Database Syst Rev. 2012;1(5):CD003519.
23. Nimbalkar SM, Patel VK, Patel DV, Nimbalkar AS, Sethi A, Phatak A. Effect of early skin-to-skin contact following normal delivery on incidence of hypothermia in neonates more than 1800 g: randomized control trial. J Perinatol. 2014;34(5):364–368.
24. Prescott SL, Larcombe DL, Logan AC, et al. The skin microbiome: impact of modern environments on skin ecology, barrier integrity, and systemic immune programming. World Allergy Organ J. 2017;10(1):29.
25. Srivastava S, Gupta A, Bhatnagar A, Dutta S. Effect of very early skin to skin contact on success at breastfeeding and preventing early hypothermia in neonates. Indian J Public Health. 2014;58(1):22–26.
26. American Academy of Pediatrics. Committee on Infectious Disease, Red book: 2015 Report of the Committee on Infectious Diseases; 2015. Available from: https://redbook.solutions.aap.org/DocumentLibrary/Red%20Book%202015%201.pdf.
27. Bryanton J, Walsh D, Barrett M, Gaudet D. Tub bathing versus traditional sponge bathing for the newborn. J Obstet Gynecol Neonatal Nurs. 2004;33(6):704–712.
28. Loring C, Gregory K, Gargan B, et al. Tub bathing improves thermoregulation of the late preterm infant. J Obstet Gynecol Neonatal Nurs. 2012;41(2):171–179.
29. Gelmetti C. Skin cleansing in children. J Eur Acad Dermatol Venereol. 2001;15 Suppl 1:12–15.
30. Walters RM, Fevola MJ, LiBrizzi JJ, Martin K. Designing cleansers for the unique needs of baby skin. Cosmetics Toiletries. 2008;123(12):53–60.
31. Lund CH, Osborne J. Validity and reliability of the neonatal skin condition score. J Obstet Gynecol Neonatal Nurs. 2004;33(3):320–327.
32. Garcia Bartels N, Scheufele R, Prosch F, et al. Effect of standardized skin care regimens on neonatal skin barrier function in different body areas. Pediatr Dermatol. 2010;27(1):1–8.
33. Simpson EL, Chalmers JR, Hanifin JM, et al. Emollient enhancement of the skin barrier from birth offers effective atopic dermatitis prevention. J Allergy Clin Immunol. 2014;134(4):818–823.
34. Telofski LS, Capone KA, Friscia D, Nikolovski J. Effects of Emollient Use on the Developing Infant Skin Microbiome. Pediatrics. 2020;146(1_MeetingAbstract):128.
35. Zhong Y, Samuel M, van Bever H, Tham EH. Emollients in infancy to prevent atopic dermatitis: a systematic review and meta‐analysis. Allergy. 2022;77(6):1685–1699.
36. Chaoimh CN, Lad D, Nico C, et al. Early initiation of short‐term emollient use for the prevention of atopic dermatitis in high‐risk infants—The STOP‐AD randomised controlled trial. Allergy. 2022.
37. Rawlings AV, Lombard KJ. A review on the extensive skin benefits of mineral oil. Int J Cosmet Sci. 2012;34(6):511–518.
38. World Health Organization. Essential Newborn Nursing. WHO-CC for Training and Research in Newborn Care, All India Institute of Medical Sciences, New Delhi, India; 2013. Available from: https://www.newbornwhocc.org/essential.html#:~:text=Nurses%20play%20critical%20roles%20in,birth%20weight%20neonate%20in%20Kangaroo.
39. Blume-Peytavi U, Hauser M, Stamatas GN, Pathirana D, Garcia Bartels N. Skin care practices for newborns and infants: review of the clinical evidence for best practices. Pediatr Dermatol. 2012;29(1):1–14.
40. Khalifian S, Golden WC, Cohen BA. Skin care practices in newborn nurseries and mother-baby units in Maryland. J Perinatol. 2017;37(6):615–621.
41. Visscher MO, Narendran V, Pickens WL, et al. Vernix caseosa in neonatal adaptation. J Perinatol. 2005;25(7):440–446.
42. Adejuyigbe EA, Bee MH, Amare Y, et al. ”Why not bathe the baby today?”: a qualitative study of thermal care beliefs and practices in four African sites. BMC Pediatr. 2015;15:156.
43. Lund C. Bathing and Beyond: current Bathing Controversies for Newborn Infants. Adv Neonatal Care. 2016;16:S13–S20.
44. Kuller JM. Update on newborn bathing. Newborn Infant Nurs Rev. 2014;14(4):166–170.
45. Kelly PA, Classen KA, Crandall CG, et al. Effect of Timing of the First Bath on a Healthy Newborn’s Temperature. J Obstet Gynecol Neonatal Nurs. 2018;47(5):608–619.
46. Behring A, Vezeau TM, Fink R. Timing of the newborn first bath: a replication. Neonatal Netw. 2003;22(1):39–46.
47. Varda KE, Behnke RS. The effect of timing of initial bath on newborn’s temperature. J Obstet Gynecol Neonatal Nurs. 2000;29(1):27–32.
48. Alizadeh TP, Fakhraee H, Sotoudeh K. Effect of early bathing on temperature of normal newborn infants. Iranian J Publ Health. 2007;36(2):82–86.
49. Penny-MacGillivray T. A newborn’s first bath: when? J Obstet Gynecol Neonatal Nurs. 1996;25(6):481–487.
50. Bergstrom A, Byaruhanga R, Okong P. The impact of newborn bathing on the prevalence of neonatal hypothermia in Uganda: a randomized, controlled trial. Acta Paediatr. 2005;94(10):1462–1467.
51. Nako Y, Harigaya A, Tomomasa T, et al. Effects of bathing immediately after birth on early neonatal adaptation and morbidity: a prospective randomized comparative study. Pediatr Int. 2000;42(5):517–522.
52. Sobel HL, Silvestre MA, Mantaring JB 3rd, Oliveros YE, Nyunt US. Immediate newborn care practices delay thermoregulation and breastfeeding initiation. Acta Paediatr. 2011;100(8):1127–1133.
53. Gozen D, Caka SY, Besirik SA, Perk Y. First bathing time of newborn infants after birth: a comparative analysis. J Spec Pediatr Nurs. 2019;24(2):e12239.
54. Brogan J, Rapkin G. Implementing Evidence-Based Neonatal Skin Care With Parent-Performed, Delayed Immersion Baths. Nurs Womens Health. 2017;21(6):442–450.
55. Chamberlain J, McCarty S, Sorce J, et al. Impact on delayed newborn bathing on exclusive breastfeeding rates, glucose and temperature stability, and weight loss. J Neonatal Nurs. 2019;25(2):74–77.
56. Preer G, Pisegna JM, Cook JT, Henri AM, Philipp BL. Delaying the bath and in-hospital breastfeeding rates. Breastfeed Med. 2013;8(6):485–490.
57. Crenshaw JT. Healthy Birth Practice #6: keep Mother and Baby Together- It’s Best for Mother, Baby, and Breastfeeding. J Perinat Educ. 2014;23(4):211–217.
58. Colwell A. To Bathe or Not to Bathe: the Neonatal Question. Neonatal Netw. 2015;34(4):216–219.
59. Dhar S. Newborn skin care revisited. Indian J Dermatol. 2007;52(1):1.
60. Sarkar R, Basu S, Agrawal RK, Gupta P. Skin care for the newborn. Indian Pediatr. 2010;47(7):593–598.
61. Gunnarsson M, Mojumdar EH, Topgaard D, Sparr E. Extraction of natural moisturizing factor from the stratum corneum and its implication on skin molecular mobility. J Colloid Interface Sci. 2021;604:480–491.
62. Caka SY, Gozen D. Effects of swaddled and traditional tub bathing methods on crying and physiological responses of newborns. J Spec Pediatr Nurs. 2018;23(1):54.
63. Cinar N, Yalnizoglu Caka S, Uslu Yuvaci H. Effect of newborn bathing training with the swaddled and tub bathing methods given to primiparous pregnant women on the mother’s experience, satisfaction and newborn’s stress during the first bathing of the newborn at home: a mixed method study. Jpn J Nurs Sci. 2020;17(4):e12363.
64. Sailer MSN Splish Splash Swaddle Bath (Delayed Swaddle Immersion Bath).
65. Edraki M, Paran M, Montaseri S, Razavi Nejad M, Montaseri Z. Comparing the effects of swaddled and conventional bathing methods on body temperature and crying duration in premature infants: a randomized clinical trial. J Caring Sci. 2014;3(2):83–91.
66. Fern D, Graves C, L’Huillier M. Swaddled bathing in the newborn intensive care unit. Newborn Infant Nurs Rev. 2002;1(2):3–4.
67. Gaddam S, Nandhini P, R PJ, Kanchana S, Celina D. Relative Effectiveness of Swaddle Bath and Conventional Bath on Level of Thermal Stability and Crying Duration among Preterm Infants at Selected Hospital in North India. ICCR-JNR. 2017;2(1):34–54.
68. Dizon MV, Galzote C, Estanislao R, Mathew N, Sarkar R. Tolerance of baby cleansers in infants: a randomized controlled trial. Indian Pediatr. 2010;47(11):959–963.
69. Lavender T, Bedwell C, Roberts SA, et al. Randomized, controlled trial evaluating a baby wash product on skin barrier function in healthy, term neonates. J Obstet Gynecol Neonatal Nurs. 2013;42(2):203–214.
70. Cooke A, Bedwell C, Campbell M, McGowan L, Ersser SJ, Lavender T. Skin care for healthy babies at term: a systematic review of the evidence. Midwifery. 2018;56:29–43.
71. Lund CH, Osborne JW, Kuller J, Lane AT, Lott JW, Raines DA. Neonatal skin care: clinical outcomes of the AWHONN/NANN evidence-based clinical practice guideline. Association of Women’s Health, Obstetric and Neonatal Nurses and the National Association of Neonatal Nurses J Obstet Gynecol Neonatal Nurs. 2001;30(1):41–51.
72. Dolack M, Huffines B, Stikes R, Hayes P, Logsdon MC. Updated neonatal skin risk assessment scale (NSRAS). Ky Nurse. 2013;61(4):6.
73. Visscher M. A practical method for rapid measurement of skin condition. Newborn Infant Nursing Rev. 2014;14(4):147–152.
74. McConnell TP, Lee CW, Couillard M, Sherrill WW. Trends in umbilical cord care: scientific evidence for practice. Newborn Infant Nurs Rev. 2004;4(4):211–222.
75. Heimall LM, Storey B, Stellar JJ, Davis KF. Beginning at the bottom: evidence-based care of diaper dermatitis. MCN Am J Matern Child Nurs. 2012;37(1):10–16.
76. Ferber SG, Laudon M, Kuint J, Weller A, Zisapel N. Massage therapy by mothers enhances the adjustment of circadian rhythms to the nocturnal period in full-term infants. J Dev Behav Pediatr. 2002;23(6):410–415.
77. Field T. Massage therapy research review. Complement Ther Clin Pract. 2016;24:19–31.
78. Garg BD, Kabra NS, Balasubramanian H. Role of massage therapy on reduction of neonatal hyperbilirubinemia in term and preterm neonates: a review of clinical trials. J Matern Fetal Neonatal Med. 2019;32(2):301–309.
79. Juneau AL, Aita M, Heon M. Review and Critical Analysis of Massage Studies for Term and Preterm Infants. Neonatal Netw. 2015;34(3):165–177.
80. Lee HK. The effects of infant massage on weight, height, and mother-infant interaction. Taehan Kanho Hakhoe Chi. 2006;36(8):1331–1339.
81. Underdown A, Barlow J, Chung V, Stewart-Brown S. Massage intervention for promoting mental and physical health in infants aged under six months. Cochrane Database Syst Rev. 2006;1(4):CD005038.
82. Underdown A, Barlow J, Stewart‐Brown S. Tactile stimulation in physically healthy infants: results of a systematic review. J Reproductive Infant Psychol. 2010;28(1):11–29.
83. Agarwal KN, Gupta A, Pushkarna R, Bhargava SK, Faridi MM, Prabhu MK. Effects of massage & use of oil on growth, blood flow & sleep pattern in infants. Indian J Med Res. 2000;112:212–217.
84. Sankaranarayanan K, Mondkar JA, Chauhan MM, Mascarenhas BM, Mainkar AR, Salvi RY. Oil massage in neonates: an open randomized controlled study of coconut versus mineral oil. Indian Pediatr. 2005;42(9):877–884.
85. White-Traut RC, Rankin KM, Yoder JC, et al. Influence of H-HOPE intervention for premature infants on growth, feeding progression and length of stay during initial hospitalization. J Perinatol. 2015;35(8):636–641.
86. White-Traut RC, Schwertz D, McFarlin B, Kogan J. Salivary cortisol and behavioral state responses of healthy newborn infants to tactile-only and multisensory interventions. J Obstet Gynecol Neonatal Nurs. 2009;38(1):22–34.
87. Tiffany-Castiglioni E, Barhoumi R, Mouneimne Y. Kohl and surma eye cosmetics as significant sources of lead (Pb) exposure. J Local Global Health Sci. 2012;2012(1):1.
88. Blume-Peytavi U, Cork MJ, Faergemann J, Szczapa J, Vanaclocha F, Gelmetti C. Bathing and cleansing in newborns from day 1 to first year of life: recommendations from a European round table meeting. J Eur Acad Dermatol Venereol. 2009;23(7):751–759.
89. Gfatter R, Hackl P, Braun F. Effects of soap and detergents on skin surface pH, stratum corneum hydration and fat content in infants. Dermatology. 1997;195(3):258–262.
90. Ananthapadmanabhan KP, Moore DJ, Subramanyan K, Misra M, Meyer F. Cleansing without compromise: the impact of cleansers on the skin barrier and the technology of mild cleansing. Dermatol Ther. 2004;17 Suppl 1:16–25.
91. Kuller JM. Infant Skin Care Products: what Are the Issues? Adv Neonatal Care. 2016;16:S3–S12.
92. Walters RM, Mao G, Gunn ET, Hornby S. Cleansing formulations that respect skin barrier integrity. Dermatol Res Pract. 2012;2012:495917.
93. Anwar SS, Kerriou H, Pragatheeswaran AM, et al. 18684 A scoring method to assess the gentleness of cleansers. J Am Acad Dermatol. 2020;83(6):AB104.
94. Walters RM, Anim-Danso E, Amato SM, et al. Hard water softening effect of a baby cleanser. Clin Cosmet Investig Dermatol. 2016;9:339–345.
95. Siri SD, Jain V. Infant’s skin and care needs with special consideration to formulation additives. Asian J Pharm Clin Res. 2018;11(12):75–81.
96. Purnamawati S, Indrastuti N, Danarti R, Saefudin T. The Role of Moisturizers in Addressing Various Kinds of Dermatitis: a Review. Clin Med Res. 2017;15(3–4):75–87.
97. Danby SG, AlEnezi T, Sultan A, et al. Effect of olive and sunflower seed oil on the adult skin barrier: implications for neonatal skin care. Pediatr Dermatol. 2013;30(1):42–50.
98. Dhar S, Banerjee R, Malakar R. Oil massage in babies: Indian perspectives. Indian J Paediatr Dermatol. 2013;14(1):1.
99. Konar MC, Islam K, Roy A, Ghosh T. Effect of Virgin Coconut Oil Application on the Skin of Preterm Newborns: a Randomized Controlled Trial. J Trop Pediatr. 2020;66(2):129–135. doi:10.1093/tropej/fmz041
100. Ahmed AS, Saha SK, Chowdhury MA, et al. Acceptability of massage with skin barrier-enhancing emollients in young neonates in Bangladesh. J Health Popul Nutr. 2007;25(2):236–240.
101. Kumar A, Mishra S, Singh S, et al. Effect of sunflower seed oil emollient therapy on newborn infant survival in Uttar Pradesh, India: a community-based, cluster randomized, open-label controlled trial. PLoS Med. 2021;18(9):e1003680.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.