")
Back to Journals » Journal of Healthcare Leadership » Volume 15
Evaluating the Methodological Approaches of Cross-Cultural Adaptation of the Bedside Handover Attitudes and Behaviours Questionnaire into Portuguese
Authors Cruchinho P , Teixeira G , Lucas P , Gaspar F
Received 20 May 2023
Accepted for publication 26 July 2023
Published 1 September 2023 Volume 2023:15 Pages 193—208
DOI https://doi.org/10.2147/JHL.S422122
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pavani Rangachari
Paulo Cruchinho, Gisela Teixeira, Pedro Lucas, Filomena Gaspar
Nursing Research, Innovation and Development Centre (CIDNUR) of Lisbon, Nursing School of Lisbon, Lisboa, 1600-190, Portugal
Correspondence: Paulo Cruchinho, Nursing School of Lisbon, Avenida Prof. Egas Moniz, Lisboa, 1600-190, Portugal, Tel +351 217913400, Email [email protected]
Abstract: Nurse managers need culturally adapted assessment instruments to support the implementation of change to Nursing Bedside Handover (NBH) in healthcare institutions. This study aimed to cross-culturally adapt the Bedside Handover Attitudes and Behaviours (BHAB) questionnaire to the Portuguese context and evaluate the methodological approaches used for this purpose. To guide this study, we followed a guideline for cross-cultural translation and adaptation measurement instruments in healthcare. The results of the content validity testing suggested that the BHAB questionnaire is a valid instrument for use in the Portuguese context. To obtain these results we showed 1) using of a new methodological approach, the dual focus, to resolve the divergences and ambiguities in the translators’ committee and the multi-professional committee; 2) the lack of a conceptual definition of the construct of the instrument as a requirement to retain items with I-CVI < 0.70 after validity relevance pretesting and 3) the cognitive debriefing and relevance pretesting as methodological approaches which can be used alone or together to reinforce the evaluation of cultural relevance of the items. We concluded there is a need for guidelines to support the decision-making process of healthcare researchers with comprehensive information about the different methodological approaches they can follow.
Keywords: patient handoff, nursing, questionnaire, translation, validity, methodological study
Introduction
Nursing Bedside Handover (NBH) is one of the most common and effective communication practices among healthcare professionals, particularly nurses.1 Its implementation is classified as an intervention that allows promoting patients’ participation in the delivery of nursing care.2 It is associated with a concern with Patient Safety,3 and it has been documented its significant effect in the reduction of some adverse events, such as medication errors, falls and pressure ulcers.4 It also has a positive impact on patients’ hospitalization experience, because they perceive that nurses know their situation and their progress,5,6 as well as their expectations and their care plans.7–9 Although most studies report positive effects in the involvement of patients during handover,5,10,11 some studies revealed contradictory results regarding the effect of sharing decision-making between nurses and patients,12,13 as well as nurses’ resistance behaviors arising from the high number of situations in which NBH could not be performed.14 Nurses’ resistance to change is defined as a behavior aimed at preventing or interrupting a given change.15 Therefore, the relevance of the involvement of Nurse Managers (NMs) in the leadership and management of the organizational change from conventional handover to NBH has been affirmed in the nursing scientific literature.16–21
The participation of NMs in the successful management of this change can be achieved with a diversity of strategies. Givens et al,7 reported a Quality Improvement Project (QIP) in a neuro geriatric inpatient psychiatric unit, which increased nurses’ satisfaction from 5.7 to 8.3 from: 1) conducting meetings with the nursing team; 2) sharing scientific evidence produced in similar clinical settings; 3) using a feedback board for nurses to write their perceptions about the change in the nursing station; 4) promoting an open discussion of the pros and cons of the change; 5) use of three nurses with a professional experience of more than 15 years to act as facilitating agents together with NMs in anticipating barriers and challenges, and identifying the changes to be made; 6) encouraging nurses at the door of the wards to perform NBH and 7) monitoring of satisfaction with the duration of the handover. Wollenhaup et al,22 also reported that a QIP in a postpartum unit generated a 40.34% increase in nurses’ satisfaction with the performance of NBH at a private moment among nurses and another one with the parturient. The implementation of two separate moments was intended to avoid discussion and exposure of sensitive information and used: 1) two nurse facilitators trained by NMs to support and guide the team; 2) an educational program on the benefits of involving the parturient and families in the handover process; 3) the use of a structured format as a template for the NBH; 4) a guideline of the handover content fixed on computers for nurses to use for handover and 5) fortnightly follow-up meetings to obtain feedback on implementation and to provide team support.
To refine the process of NBH implementation, NMs need to use assessment instruments (scales, tests, tools, questionnaires, and surveys).23 Using assessment instruments allows to adjust the strategies for implementing change in the organizational contexts of healthcare institutions.24,25 There are few assessment instruments with available psychometric information addressing NBH.26 Recently, Tobiano et al,27 developed an instrument to measure patients perceptions of their participation in the NBH. Slade et al,28 also, reported the development of the Nursing Bedside Attitudes and Behaviours (BHAB) questionnaire to assess nurses’ attitudes and behaviors towards the mandatory implementation of NBH. Furthermore, in Portugal, there are no known studies that have culturally adapted this questionnaire to the Portuguese context, nor that aim to develop an assessment instrument to monitor nurses’ practices during NBH. The BHAB questionnaire is the only available evaluation instrument targeting nurses. Adopting this questionnaire in the Portuguese healthcare organizations is important because the National Plan for Patients Safety (NPPS) 2021–2026 established the development and implementation of safe communication devices between healthcare professionals as an priority action for Portugal.29
Translating and adapting assessment instruments from one cultural context to another requires following a process, which is not limited to their translation.30 This process intends, mainly, to obtain an instrument equivalent to the original for the cultural context in which it is intended to be used.31 Typically, it involves phases of translation, synthesis of translations, back-translation, harmonization of translations, pre-testing and evaluation of the final structure.32 The latter comprises the assessment of psychometric properties and it tests the outcome of the cross-cultural adaptation process.33 Overall, these phases include a variety of methodological strategies, such as using bilingual and bicultural translators,34 performing blind translations,35 using team approaches to decide on the adequacy of the translation,36 on which population and monolingual subjects may participate,35 using dual focus procedures,37 panel of experts,31 focus groups,38 and cognitive debriefing interviews to assess the clarity and relevance of items,32 and content validity assessment procedures.
The use of different methodological approaches improves the quality of the measurement instrument obtained.39 This occurs because the use of different methodological approaches allows different types of equivalence to be achieved.40 Herdman et al,41 classified the equivalence of measurement instruments into five categories: 1) conceptual equivalence; 2) item equivalence; 3) semantic equivalence; 4) operational equivalence and 5) measurement equivalence. Conceptual equivalence checks which domains are important for the concept in the “target culture” and their interrelationship.41 Item equivalence critically analyses the items covered by the domains of the concept.41 Semantic equivalence ensures that the translations of the items correspond semantically to the items in the original version.41 Operational equivalence seeks to ensure that the measurement methods used are appropriate in the target culture.41 Measurement equivalence verifies the outcome of the process in terms of the behaviors of the instrument.41 Without careful description of the methodological approaches used and the equivalences obtained, it is impossible to draw conclusions about the instruments that are proposed,42,43 without assessing the absence of cross-cultural biases.44 These biases can result from problems of: 1) conceptual equivalence; 2) item equivalence; and 3) operational equivalence.44
As NBH is a nursing practice that is by nature variable due to nurses’ resistance45,46 and whose concept is not yet mature,47 there is a need to provide comprehensive information on the process of cross-cultural adaptation of assessment instruments to be used. Consequently, we established as objectives of this study: a) to cross-culturally adapt the BHAB questionnaire,28 to the Portuguese context and b) evaluate the methodological approaches used for this purpose. The existence of an instrument culturally adapted to the Portuguese context, will allow the development of experimental studies involving the NBH as a phenomenon of study.
Methods
Study Design
This methodological study was part of a larger study with a cross-sectional exploratory research design which analyzed the psychometric characteristics of the BHAB questionnaire,28 in the Portuguese population. Although there is no recognized nomenclature,48,49 methodological studies have been defined as studies aiming the development, testing, and evaluation of research instruments.50 They are used to develop the reliability and validity of assessment instruments that measure constructs used as variables in research.51 Methodological studies allow to identify knowledge gaps with reference to methodological approaches and strategies for improving research practices.48 This methodological study was based on Sousa and Rojjasnarirat’s guideline.31 We chose this guideline because it is the most recent in the healthcare field.
Ethical Considerations
This study was conducted in a Portuguese healthcare organization with experience in implementing the NBH for more than five years. The study was approved by the Ethics Committee and followed the international guidelines of the ICN Code of Ethics for Nurses.52 It also followed the ethical principles established by the World Medical Association, particularly on the participants’ right to refuse to take part in the study or to leave without being adversely affected.53 All participants gave their written and voluntary consent to participate.
Questionnaire Description
The BHAB questionnaire,28 is a 32-item self-administered questionnaire that was developed in Australia to assess nurses’ attitudes and abilities to perform the NBH in a mandatory manner. The questionnaire is composed of a set of nurses’ actions that characterize the NBH, divided into two subscales. The attitudes subscale has 18 items that assess nurses’ level of agreement to implement a set of actions during handovers. The subscale of behaviors comprises 14 items that assess nurses’ ability to perform the same actions. All items have a six-point Likert-type response format (1. “strongly disagree” to 6. “strongly agree”) devoid of a neutral point, but with a “not applicable” point. The questionnaire also contains a third section to collect nurses’ personal data, namely: a) length of professional experience as a nurse; b) length of professional experience in the hospital; 3) highest academic qualification; 4) gender; 5) age; 6) job category; 7) clinical supervision activity and 8) unit or service in which they work. To date, no study has reported the dimensionality of the BHAB questionnaire. Authors and publisher’ permissions were requested to use this questionnaire.
Translation and Cross-Cultural Adaptation
The BHAB questionnaire,28 was translated from English to Portuguese by two independent and bilingual translators, with Portuguese language as the mother tongue. One of the translators was familiar with the NBH, while the other did not meet this requirement and had no clinical profile. The two versions of the questionnaire in translated to Portuguese were subsequently compared with each other and with the original questionnaire by a third bilingual translator not familiar with the NBH. This translator identified the ambiguities and discrepancies existing in both translations and developed a unified translation proposal for discussion in a Translators’ Committee, which brought together the two previous translators. The committee consensualized a single version of the questionnaire in Portuguese, which was subsequently translated into English. This translation was independently performed by two bilingual native English translators, neither of them familiar with the NBH and with no clinical profile. In order to identify the ambiguities and discrepancies in the translations and propose a single translation of the questionnaire into Portuguese, an expert in the area of linguistics compared the two English versions with the two Portuguese versions and the original version. The translation proposal developed by this expert was presented and discussed in a Multiprofessional Committee composed of the translators who produced the translation to Portuguese and English, a nurse with current experience in performing the NBH, and a monolingual nurse unfamiliar with the NBH, whose mother tongue was the Portuguese. Despite being optional in Sousa and Rojjanasrirat guideline,31 a monolingual element was included because monolingual elements detect foreign constructions more easily than bilinguals.37 The two nurses had no access to either the original questionnaire or any of its translations. In this committee, a consensus was reached on an adapted version of the BHAB questionnaire,28 for use in the Portuguese population. The Translation, Translators’ Committee, Back Translation, and Multiprofessional Committee included the record of the doubts and decisions made regarding the respective versions of the questionnaire.
To facilitate consensus in the Translators Committee and the Multiprofessional Committee, the dual focus technique was used, which consists of an iterative process of attention and discussion on the wording of the items in the two languages of the instrument with inputs from those familiar with the construct of the instrument. In the Multiprofessional Committee this input was obtained from the target population and monolingual nurses.37 The aim of the dual focus is the consensus of all translators on the semantic and conceptual equivalence of the assessment instrument.37 The role of the members familiar with the construct of the instrument is to ask questions about the different meanings of the words and to discuss more precise wordings.37 In both Translators Committee and Multiprofessional Committee all divergences and discrepancies found in the items were presented for discussion. In both meetings, a member of the research team (P.C.) moderated the discussion, asking the translators to agree on the wording with the best semantic equivalence for each item. Subsequently, members familiar with the construct were asked if they had any questions or any wording suggestions that would be more suitable for the NBH construct. Dual focus may involve replacing items or parts of items with more appropriate ones in the target language in order to mitigate the difficulty of adapting certain content from the source culture.54
Content Validity Testing
We tested the Content Validity of the adapted version of the BHAB questionnaire,28 in a Portuguese hospital institution. The content validity test included a pretest to assess items’ clarity and a pretest to assess their relevance. To assess the clarity of the items, we recruited a sample of 24 nurses from all units and services that use the NBH (in inpatient units of pediatrics, medicine, surgery, obstetrics, general emergency department, intensive care unit, and labor and delivery unit). We included all units and services that perform NBH because healthcare organizations comprise several specific subcultures.55 Sample size was determined based on the desired level of expertise and on the range of knowledge representation of the panel,56 given the number of services included in the study. For this, the head nurses of each unit or service were asked to suggest three nurses to participate. Each nurse answered an electronic questionnaire accessed through a hyperlink with the items of the adapted version of the BHAB questionnaire,28 and with a dichotomous response format (“is clear” and “is not clear”). For items marked as “not clear”, nurses were asked to reword the respective items in order to improve their clarity. The second pretest consisted of an Expert Panel composed of NMs from units and services using the NBH. Only NMs were included due to their role in managing the change to the NBH.11,57,58 A total of nine NM participated in this Expert Panel, who individually assessed the relevance of each of the BHAB questionnaire’s items,28 with a 4-point Likert-type response format (1. “not at all relevant”, 2. “somewhat relevant”, 3. “quite relevant” and 4. “highly relevant”). The number of experts was determined based on the desired level of expertise and the range of knowledge representation of the panel,56 given the number of services included in the study. For the Expert Panel, one NM of each service or unit was recruited. Subsequently, the NMs were asked to qualitatively assess the relevance of the total questionnaire. In both the first and second pretests, the questionnaire was distributed by hyperlink by a nurse collaborating in the institution hosting the study. The anonymity of the answers of the nurses who took part of the two pretests was guaranteed prior the access to the online questionnaire. All experts in the two pretests were recruited through a non-probability convenience sampling method. To determine the number of experts, the criteria of the desired level of expertise and the range of knowledge representation of the panel were followed,56 as an alternative minimum and maximum number of participants defined in the guideline by Sousa and Rojjanasrirat,31 since it is a questionnaire that aims to assess the practices of nurses in various subcultures. The two pretests were both conducted in May 2021.
Data Analysis
Content Validity is a psychometric characteristic that analyses the degree to which an assessment instrument reflects the domain of interest and the conceptual definition of the construct of the assessment instrument.59 In the adapted version of the BHAB questionnaire,28 Content Validity was determined by calculating the Content Validity Index (CVI) from the participants’ answers in the two pretests. The CVI constitutes a method of quantifying the degree of agreement between participants who evaluated the content of the assessment instrument.60 To determine the CVI, we first calculated the CVI of each item (I-CVI) and then the average of all the items (S-CVI) comprising the BHAB questionnaire.28 These two methods were also used by the authors of the original questionnaire to assess the content validity.28 The I-CVI was calculated based on the quotient between the sum of all participants’ responses and the number of participants.61 To calculate the average of all items, we used two approaches: 1) the average of the CVI indices (S-CVI/Ave), and 2) the universal agreement index (S-CVI/UA). For the determination of the S-CVI/Ave we used the following formula: S-CVI/Ave = (sum I-CVI scores)/(number of items).61 The S-CVI/UA was obtained from the following formula: S-CVI/UA = (sum of UA scores)/(number of items).61 In this study, we used both approaches to increase confidence in the content validity of the BHAB questionnaire.28 Because CVI and UA are suitable for dichotomous-type responses, in the relevance pretest the responses were recoded as 0 (for responses 1 and 2) and 1 (for relevance responses 3 and 4).61 To calculate the S-CVI/UA the responses were further recoded into 0 in situations where there was not 100% agreement between the participants and into 1 when there was 100% agreement. As reference values, we adopted the minimum value of 0.50 for the I-CVI,60 0.80 for the S-CVI/UA and 0.90 for the S-CVI/Ave.62 An assessment instrument has excellent content validity when it simultaneously has adequate I-CVI and S-CVI values.62,63 Items with I-CVI values less than 0.79 are considered as “candidates to be revised” (if I-CVI between 0.78 and 0.71), or “candidates to be eliminated” (if I-CVI less than 0.70), or mandatorily eliminated (if I-CVI less than 0.50).60 The original authors of the BHAB questionnaire reported I-CVI>0.78 on all items and S-CVI>0.90 on each of the subscales.28
Results
The process of cross-cultural adaptation of the BHAB questionnaire,28 followed the guideline of Sousa and Rojjanasrirat.31 To produce an adapted version of the BHAB questionnaire,28 which was equivalent to the original version, the existence of ambiguities and discrepancies after the translation and back translation of the instrument were investigated. In the translation of the BHAB questionnaire,28 into Portuguese, 11 semantic ambiguities and six discrepancies in the translation of the items were identified. In relation to the response format, no ambiguities and discrepancies were found. Most discrepancies involved specific NBH terms, such as “handover”, “incoming nurses” and “treatment plan”. Semantic ambiguities resulted from the diversity of meanings in the translation of English words and phrases, such as the verb “react to”, which in Portuguese can mean respond or react. All ambiguities and discrepancies resulting from the translation were resolved by discussion and consensus in the Translators’ Committee using the dual focus technique (Table 1). The contributions of the translator familiar to the NBH were crucial to solve the discrepancies, while the ambiguities had more contributions from the translator with no clinical profile. In the back translation of the questionnaire into English, 10 semantic discrepancies and three ambiguities were identified, two of which were conceptual. The conceptual ambiguities were identified in item a6 “outgoing nurses should ask incoming nurses for clarification and confirmation of information discussed” and c4 “as an outgoing nurse, I introduce myself and each member of the incoming team”. The conceptual ambiguity of item a6 was related to the concept of Safe Communication characterized by a clarification and validation of the accuracy of the interpretations made,64 and in relation to which, only outgoing nurses could clarify the information discussed in the handover. The item c4 had two possible meanings: a) the nurses who are leaving the shift introduce themselves to the incoming team or b) introduce the patient to the incoming team. The conceptual ambiguity of this item involved the concept Nursing Transfer of Accountability at the Bedside,65 and the concept Patient Involvement during NBH.66,67 These two ambiguities were clarified by email with one of the authors of the original questionnaire (J.P.). Relating to the item c4 it was clarified that the behavior assessed in this item indicates the presentation of the patient by the outgoing nurse to each incoming team member. All semantic discrepancies and ambiguities were resolved in the Multiprofessional Committee by discussion and consensus using the dual focus technique (Table 2). The target population nurse and the monolingual nurse both had an active role in the construction of the final wordings of the BHAB questionnaire items. For a comprehensive analysis of all versions produced in each stage of the cross-cultural adaptation process for the 32 items of the BHAB questionnaire,28 see Table S1.
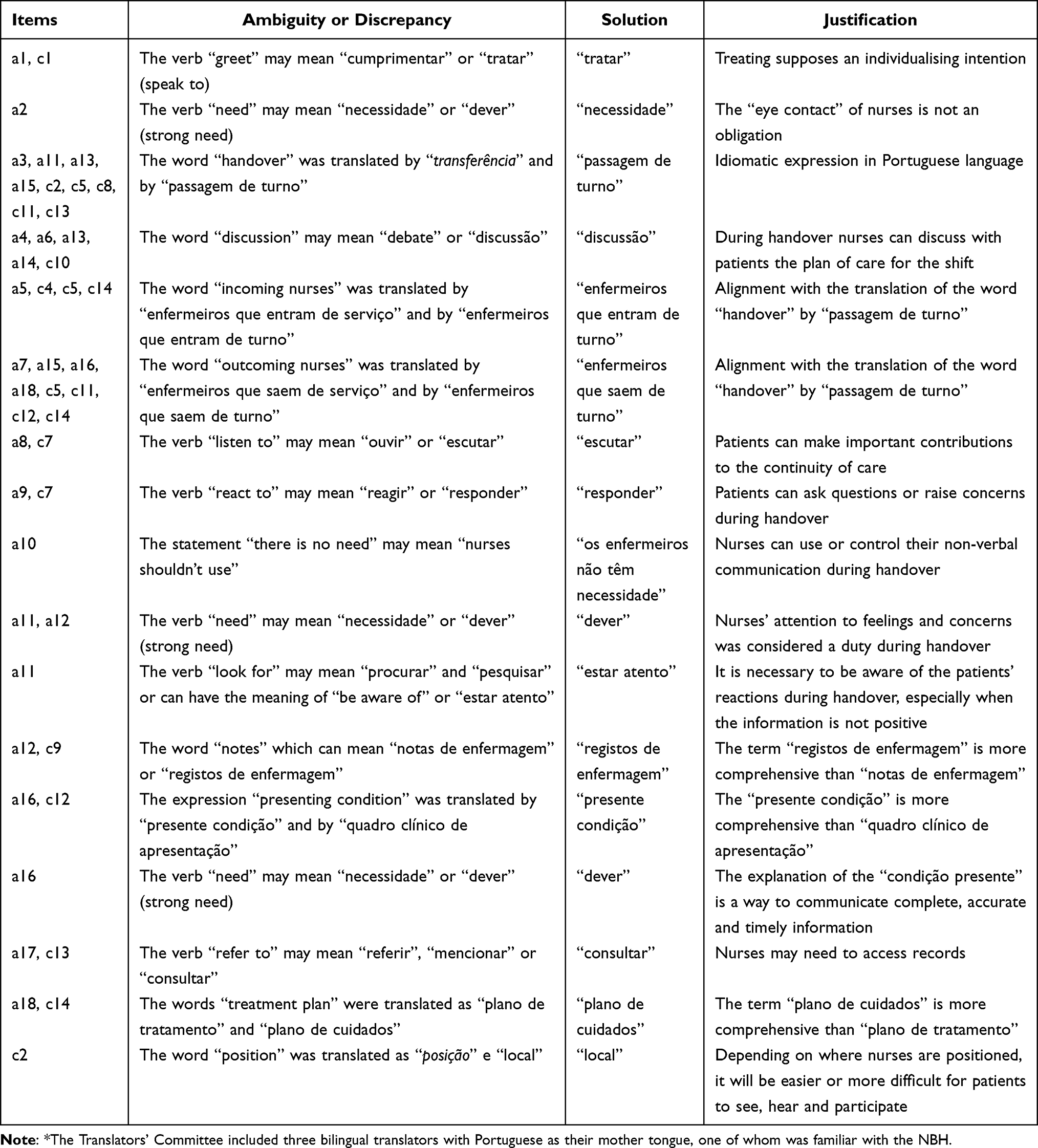 |
Table 1 Solutions Adopted by the Translators’ Committee* for the Ambiguities and Discrepancies Found in the Translations of the BHAB Questionnaire |
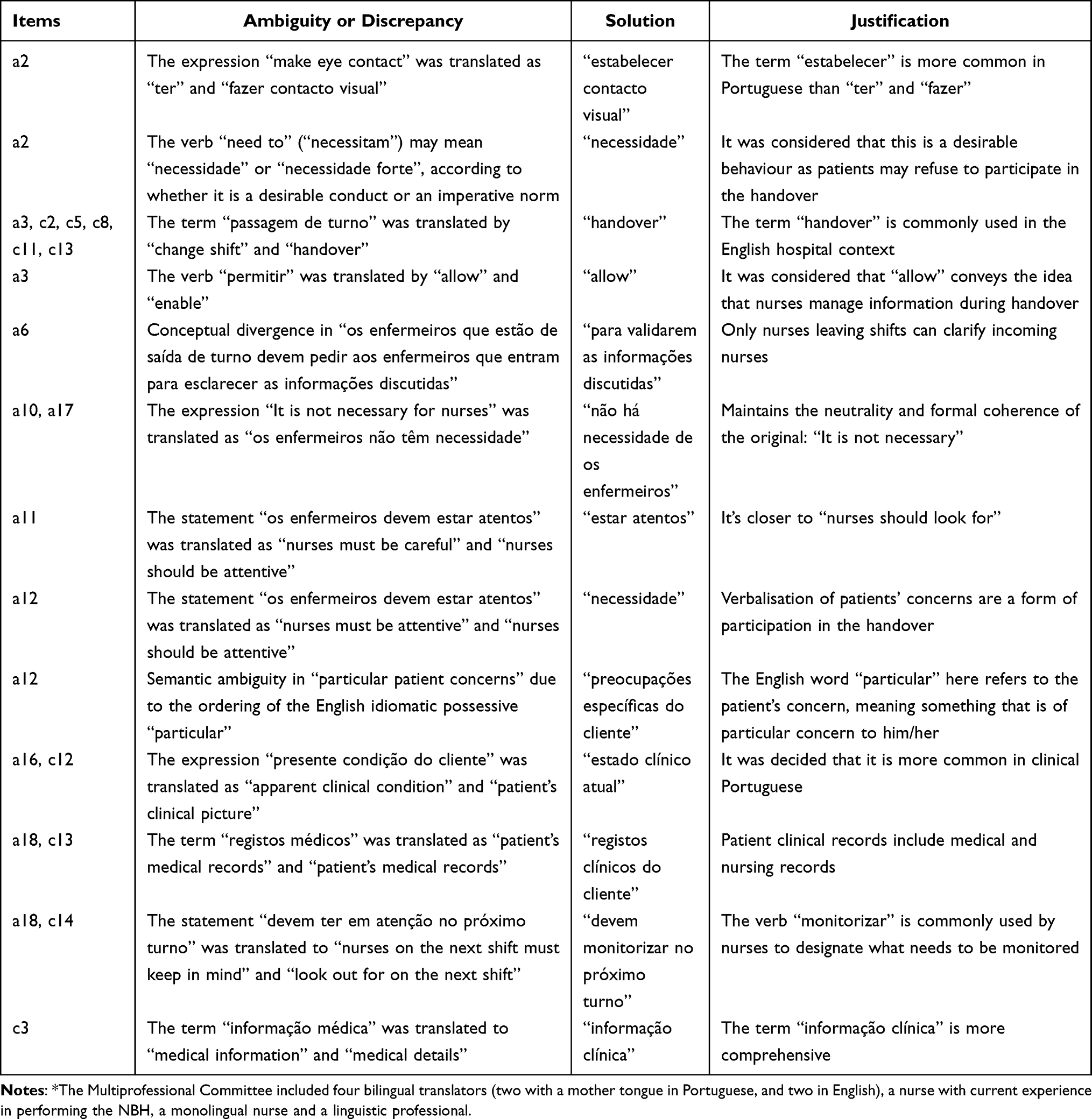 |
Table 2 Solutions Adopted by the Multiprofessional Committee* to the Ambiguities and Discrepancies Found in the Back-Translations of the BHAB Questionnaire |
When testing the content validity, it was followed the current good practice of describing the process, the participants’ personal data, and the results found.62 Regarding the process, the performance of a Cognitive Debriefing in the clarity pretest was not planned because it was not clear in the guideline followed the advantages of its use.31 The need for the Cognitive Debriefing subsequently arose with a number of responses that were only comments rather than suggested improved wording for the not clear items. As the guideline advocates a sample size of 10–40 participants to conduct the clarity pretest,31 we chose to perform the content validity testing via an electronic questionnaire. The anonymity of the questionnaire prevented us from exploring participants’ comments through a Cognitive Debriefing. This consists of an interview conducted individually with a set of participants after they have responded to the assessment tool.32,68 It is a qualitative approach,69 that allows researchers to assess: 1) the meaning; 2) understanding, and 3) cultural relevance of each item of the adapted instrument.70 The assessment of cultural relevance comprises the identification of erroneous assumptions concerning the target population on which the instrument is to be used.71 Because it involves a sample size of 10–40 subjects,31 it can be a time-consuming pretest.72 Regarding the number and qualifications of the participants, they were considered adequate. The personal data of the participants can be seen in Table S2.
In the clarity pretest all items presented I-CVI values≥0.93 and were considered clear (100%). There were only four items with some disagreement among the participants, namely: a13 “é aceitável usar exemplos pessoais ou humor na discussão da passagem de turno”, a16 “é necessário que os enfermeiros que estão de saída de turno expliquem o estado clínico atual do cliente”, a18 “é necessário que os enfermeiros que saem de turno, expliquem o plano de cuidados e o que os enfermeiros que entram, devem monitorizar no turno”, and c14 “como enfermeiro que está de saída de turno, sou explícito em relação ao plano de cuidados e ao que os enfermeiros devem monitorizar” (all with values of I-CVI=0.96). Wording suggestions were obtained for these items, which were analyzed by two nurses collaborating in the study, who were NMs in the institution where the study was carried out, and who decided not to modify any item. Some of the suggestions made by the participants were comments, which did not include drafting proposals, such as “it is necessary them to listen but not during handover, in my opinion”, “depending on the situation, it may be necessary to use non-verbal communication” and “in my opinion, it is not the right time, for the patient to contribute”.
Regarding the items’ relevance, the I-CVI ranged between 0.56 and 1.00, of which 29 had an I-CVI>0.78. It was achieved a I-CVI<0,70 in three items, namely: a13 “é aceitável usar exemplos pessoais ou humor na discussão da passagem de turno” (I.CVI=0.56); a15 “os enfermeiros que estão de saída de turno devem iniciar a passagem de turno identificando o cliente, o seu médico e a razão pela qual está no hospital” (I-CVI=0.67), and c11 “como enfermeiro que está de saída, início a passagem de turno identificando o cliente, o seu médico e a razão pela qual está no hospital” (I-CVI=0.67). Apart from the previous items, most were considered relevant (91%). For the total questionnaire, adequate content validity indices were obtained in both pretests (S-CVI/Ave>0.90 and S-CVI/UA>0.80). As the NBH concept is not a mature concept,47 all items with I-CVI<0.70 were the subject of discussion between the research team and two of the study nurses who were NM at the institution where the study was conducted. It was decided to retain these items as they measure nurses’ attitudes and behaviors that are seen as important and are often undervalued during the performance of the NBH and consequently require high need for improvement.
Discussion
This study aimed: a) to cross-culturally adapt the BHAB questionnaire,28 to the Portuguese context and b) evaluate the methodological approaches used for this purpose.
Cross-Cultural Adaptation of BHAB Questionnaire
The cross-cultural adaptation of assessment instruments is a complex and iterative process,73 aiming to identify differences between the “source culture” and the “target culture”,32 requiring a rigorous assessment of divergences and ambiguities in all steps.31 These divergences and ambiguities may be of semantic and conceptual nature,30 and translate the dimensions of analysis of the equivalence between the versions of the assessment instruments.41 In this study, we found a higher number of semantic divergences than ambiguities after back translation. This may be explained by the use of a blind back translation, in which the translators had no contact with the original assessment instrument.35 Contrarily, after translation, the number of semantic ambiguities observed was higher than the number of divergences. The variety of options that translators have when translating a word or expression from one language to another may be one explanation.36 After back translation, two conceptual ambiguities were also identified. The back translation of assessment instruments amplifies wording with conceptual errors.74 The identified ambiguities and divergences were eliminated through a Translators’ Committee and a Multiprofessional Committee. These approaches increase semantic and conceptual equivalence between the original and adapted versions of the assessment instruments.36 Two conceptual ambiguities were clarified by one of the authors of the original assessment instrument. Contact with the authors of the original instruments is recommended to increase conceptual equivalence and avoid cross-cultural biases.31 The clarification obtained was essential due to: 1) the lack of knowledge about the dimensionality of the assessment instrument,47 and 2) the fact that the NBH is not yet a mature concept with clearly defined attributes.47 When the literature does not provide enough details about an assessment instrument, it is useful to contact the authors to clarify the doubts that arise during the cross-cultural adaptation process.75
Some contingent factors affected the use of some methodological approaches outlined in Sousa and Rojjanasrirat’s guideline.31 Due to the unavailability of resources, none of the translators who performed the back translation of the BHAB questionnaire,28 were familiar with the NBH. To address this difficulty, we recruited a nurse from the host hospital institution to include a Multiprofessional Committee. For this committee, the guideline of Sousa and Rojjanasrirat,31 establishes only the inclusion of a healthcare professional without specifying any other requirement that characterizes him/her. With respect to the translators who translated and back translated the instrument, the guideline specifies that one of the translators at each stage should be familiar with the health terminology and the construct of the assessment instrument. The contributions of this nurse were, in most situations of the Multiprofessional Committee, decisive in achieving consensus among the translators. According to Bornman et al,35 subjects from the target population to whom the assessment tool will be applied should participate in the Multiprofessional Committee so that decisions are not exclusively made based on linguistic equivalence. The inputs of the members of the target population in the Multiprofessional Committee ensure conceptual equivalence between the original and the adapted versions of the assessment instruments.76
We used a technique that is not established by Sousa and Rojjanasrirat’s guideline,31 and that allows resolving the divergences and ambiguities found in the Translators’ Committee and the Multiprofessional Committee. This is a decision procedure regarding the items’ translation and takes into account both semantic equivalence and conceptual equivalence, called dual focus.37,77 Its use may be important in nursing studies due to the use of terminology which is specific to nurses’ professional culture in assessment instruments and with which translators may not be familiar. Dual focus was instrumental, in this study, in translating and adapting into Portuguese the terms “handover” (a3, a11, a13, a15, c2, c5, c8, c13), “incoming nurses” (a5, a18, c5, c14), “patient progress” (a5), “outgoing nurses” (a6, a15, a16, a18, c4, c5, c11, c12, c14), “notes” (a12, c9), “presenting condition” (a16, c12), “patient´s medical notes” (a17, c13), “treatment plan” (a18, c14) and “medical information” (c3, c13). It was also important to translate and adapt “Bedside Handover” from the title of the questionnaire, which is an idiomatic expression. Idiomatic expressions are combinations of words, which have a specific cultural meaning different from their literal meaning,78 and which are not easy to translate into another language.79 Therefore, they tend to be either borrowed from or adapted to the “target language”.80 One of the strategies that may be used in the cross-cultural adaptation of idioms is the identification of comparable idioms in the “target language”.81 In Portugal, the expressions “passar o turno” and “passar ocorrências” are used to define the transmission of information between nurses between their working shifts. The consensus obtained for the international term ‘Bedside Handover’ was also based on the expressions “enfermeiro de cabeceira” and “cabeceira do cliente”, which are also used in other cultures to refer to the proximity of nurses to patients. Based on this, Nursing Bedside Handover was adapted as the “Passagem de Turno à Cabeceira do Cliente”.
Using the dual focus allowed to adopt a centring approach during the cross-cultural adaptation process, which is not sufficiently explained in Sousa and Rojjanasrirat’s guideline.31 This methodological approach considers the adapted version to be as important as the original version of the assessment instrument in order to allow for the replacement of complete and/or the parts of items, ensuring the content validity.76,82 To promote the use of dual focus in the Multiprofessional Committee, we streamlined the discussion on the translation of the items in the following sequence: 1) opinions of the translators one by one (semantic equivalence); 2) opinions of the member acquainted with the NBH (conceptual equivalence) and 3) consensus reached by the committee (semantic and conceptual equivalence). In the Translators’ Committee, the sequence was similar. Dual focus can lead to the complete or partial replacement of parts of items by others more appropriate to the “target culture”.83–88 However, none of the items in the BHAB questionnaire,28 had a complete replacement in this study. All methodological approaches used in the cross-cultural adaptation of the BHAB questionnaire,28 were rigorously followed. Although, some of them are not included in the Sousa and Rojjanasrirat’s guideline,31 we evaluated them as adequate to obtain a conceptual equivalence between the original and adapted questionnaire.
Analysis of the Content Validity of the Adapted Version
In the assessment of the Content Validity of the adapted version of the BHAB questionnaire,28 we described the process, the participants’ personal data, and the results obtained.62 In the relevance pretest, I-CVI values considered as “candidates to be eliminated”,60 were observed in items a13, a15, and c11 (I-CVI<0.70). These items characterize the NBH with the possibility of: 1) the use of self-disclosure and humor (a13) and 2) of the introduction of the handover of each patient with the identification of the patient and his/her doctor, and the reason for hospital admission (a15 and c11). The experts’ low agreement regarding item a13 may be explained by the fear that self-disclosure may question the limits of the nurse-patient relationship.89 Self-disclosure is a communication technique that can be verbal and non-verbal, intentional or not revealing something personal to nurses.90 Its use by nurses can be useful if it is carefully applied.91 When it is used appropriately, it is recognized as a characteristic of effective communication.92 Contrarily, the absence or excess of self-disclosure by nurses constitutes characteristics of ineffective communication.92 Personal information disclosed may relate to: 1) close family members; 2) activities and interests; 3) life experiences, and 4) personal opinions.93 The purpose of using self-disclosure is to support patients’ experience rather than belittle or devalue it,94 through a therapeutic bond with nurses.89 Its use in nursing is reported, for example, in obstetrics,95 cardiology,96 and oncology units.97 Regarding humor, the low agreement of the experts may be justified by the fear of negative reactions from patients or even the loss of mutual respect.98 Humor also aims to improve nurse-patient relationship,99 and communication.100 It is used by nurses, for example, in oncology,101 paediatric,102 and nursing homes.103
In turn, the experts’ low agreement in items a15 and c11 may be explained by the consultation of nurses’ electronic documentation as a source of information during the NBH.104–106 In the hospital institution that hosted this study, consulting the electronic documentation is performed during the NBH through a laptop computer, which is mobilized through the wards. Consequently, the nurses’ access through the electronic documentation systems to information about the patient’s identity, the doctor, and the reason he/she is in the hospital may make it irrelevant to repeat it during the NBH. In a study conducted by Johnson et al, who developed an electronic documentation system to be accessed during NBH, only included bed information, patient identification, and the reason for hospital admission.107 The possibility of consulting the electronic documentation during the NBH allows the documented information not to be repeated verbally and allow nurses to focus the NBH on updating and discussing the plan of care.108 The identification of the patient’s physician is much less reported information during handovers than the patient’s name and the reason for admission.109 Furthermore, the I-CVI values of items a15 and c11 can also be explained by the possibility of breach of confidentiality of patient information due to the presence of other patients and family members during the NBH, namely regarding medical diagnosis information,110 and regarding sensitive information about test results.111
Items with I-CVI<0.70,60 items a13, a15, and c11 were not eliminated after the pretest of relevance. Two factors that hindered the decision to eliminate these items were 1) the lack of a conceptual definition of the NBH describing its attributes,47 and 2) the unfamiliarity of the dimensionality of the BHAB questionnaire.47 One conceptual definition we found resulted from a conceptual analysis of the concept of handover in nursing, which did not include the NBH.112 The absence of a conceptual definition of the construct to be assessed by the assessment instrument makes it difficult to interpret the results and perform useful critical analyses of the instrument on its conceptual basis.113 According to Morse and Carter,114 a well-defined concept should include its main delimited attributes and specified preconditions and outcomes. As a result of the absence of a conceptual definition for the NBH and the dimensionality of the BHAB questionnaire,28 the researchers were unable to envision whether the deletion of the mentioned items could threaten the conceptual equivalence between the adapted and original versions of the BHAB questionnaire.28 When two versions of an assessment instrument are partially equivalent in the construct being measured by two different cultures, construct bias is said to exist.115 Haynes et al argue that the content validity procedures, as well as the content validity indices obtained, should be treated as categories of construct validity of the assessment instruments and should be reported systematically and in the same detail as other elements of construct validation.116 Achieving I-CVI values of less than 0.70, the researchers inferred that the content validity assessment of the adapted BHAB questionnaire,28 requires a rigorous refinement process of the construct domain using a larger sample size and statistical methods to know its internal structure. Recent studies recommending a flexible,58,117,118 and adaptive119 implementation of the NBH rather than a mandatory implementation support the need for refinement of the domain of the NBH construct.
Strong conceptualization of the construct is a fundamental requirement for obtaining acceptable I-CVIs.63,120,121 This element plays a key role in assessing content validity because it provides information about the conceptual and operational definition of the construct and what the instrument measures.122 In addition, experts need to be carefully selected,120 and have a beforehand conceptual and operational definition of the instrument’s construct.123 The operational definition identifies either empirical referents or indicators of the construct that can be observed and measured, while the theoretical definition defines a construct in relation to other constructs.124 In the pre-test of relevance, the experts were the NM of each of the services in which the NBH was implemented. Therefore, the researchers considered the experts qualified for the relevance assessment of the items, but they did not hold any conceptual or operational definition of the NBH construct. This requirement was not considered by the researchers because it was not specified in the guideline by Sousa and Rojjasnarirat,31 followed in this study. Nevertheless, the poor conceptualization of the NBH construct identified as a gap in the field of research on NBH implementation,67 would prevent the researchers from ensuring that this requirement was met in the pre-test of relevance. As a result, the researchers considered the methodological approach of reviewing the items with NMs from the target population to be an acceptable approach given the current state of conceptualization of the NBH construct.
Retaining items with an I-CVI<0.70, met the standards which suggest that only I-CVI values below 0.50 are unacceptable, and is in line with the variable nature of the NBH,1 and with the purpose of the BHAB questionnaire to assess the implementation of the NBH in hospital institutions.28 Some studies have found that the NBH is performed differently than drawn,46 and that it is not always performed or only involves introduction to the patient and the nurse starting the shift.125 This variability has been reported in relation to individual nurses’ practices, in relation to the duration of the NBH, the method used, the location of performance and the information passed on and shared with patients.126 In some studies, inconsistencies in the implementation of NBH by both nurses and patients have been reported.125,127 Malfait et al,19 in a study, which aimed to determine the existence of differences in compliance in the application of a structured NBH protocol in 12 different services, found a unilateral decision by nurses not to perform NBH in almost 30% of the cases observed. They also found that in 1/3 of the cases where NBH was performed, nurses did not actively involve patients. This was interpreted as an indicator of nurses’ resistance.14 Resistance to the use of NBH had already been identified in previous studies for two reasons: 1) NBH causing outgoing nurses to leave their shift later and causing incoming nurses to be late in their work,128,129 and 2) the possibility of breaching the confidentiality of patient information.129 Consequently, ensuring consistent implementation of NBH is a major challenge for NMs.58
This methodological approach to values of I-CVI<0.70 was not specified in the Sousa and Rojjanasrirat’s guideline,31 but was considered as adequate for the NBH implementation field of study.
Limitations and Recommendations
The present study has some limitations. Firstly, the similarity of the items relating to attitudes and behaviors may have introduced a possible habituation bias in the responses of the pre-test participants. This type of bias is generated by the possibility that subjects respond equally to very similar questions.130 Secondly, the use of electronic questionnaire in the clarity pretest preventing us from exploring the comments made by the participants to some of the items to evaluate their cultural relevance for the target population. This evaluation was carried out in the relevance pretest. Thirdly, we did not evaluate the factorial structure of the Portuguese-adapted version. As a line of future work, we intend to continue to refine the content validity of the BHAB questionnaire,28 during the psychometric validation of the instrument. Lastly, it is imperative to keep in mind that there are cultural and linguistic differences between the European Portuguese and the Portuguese spoken in the Portuguese Language Countries and this adaptation was made into European Portuguese. Portuguese is the sixth most widely spoken language in the world.131 It is the official language of Portugal, Brazil, Angola, Mozambique, Guinea-Bissau, São Tomé and Príncipe, Cape Verde and East Timor,131 which together form the Community of Portuguese Language Countries.132 We recommend the cross-cultural adaptation and validation of BHAB questionnaire in Portuguese-speaking countries. The future development of multicentric projects in Portuguese-speaking countries is only possible if there are assessment instruments culturally adapted to the contexts of these countries.
Conclusions
We conclude that given the state-of-the-art regarding the conceptualization of the NBH construct, the BHAB questionnaire is a valid content assessment instrument. Furthermore, this study showed, to improve the semantic and conceptual equivalence between the original and adapted versions of assessment instruments, researchers can make decisions that differ from the guidelines established. In other words, the use of a guideline guiding the process of translation and cross-cultural adaptation does not mean that researchers do not add or replace methodological approaches considered by others more suitable for the study in progress. This depends on the comprehensiveness and depth of the researcher’s knowledge of methodological approaches to cross-cultural adaptation. Researchers’ methodological knowledge is essential to enhance decision-making and understanding about the purposes, procedures, techniques, and criteria to be used, whether or not they are included in the guidelines.
In particular, this study showed that the use of conceptual and operational definitions of the construct to be measured by the instrument is a key requirement to avoid cross-cultural biases and to ensure conceptual equivalence during the cross-cultural adaptation process. To achieve this equivalence, it also showed the relevance of the dual focus technique during the Translators Committee and the Multiprofessional Committee, as well as the inclusion of a monolingual element in this latter. In addition, it showed the importance of complementing the Cognitive Debriefing with the clarity pretest to explore the item wording suggestions. Regarding the definition of the number of experts in the pretests, an alternative criterion of the minimum and maximum number of participants, based on the desired level of expertise and the range of knowledge representation of the panel,56 was also shown to be more suitable for assessment instruments intended to evaluate the practices of professionals in various subcultures. Finally, it was also shown that the elimination of items with I-CVI< 0.70 may not be a mandatory criterion in relation to instrument constructs with a weak conceptualization and where instruments aim to monitor practices susceptible to variability. This study shows novice researchers that the use of methodological approaches to cross-culturally adapt assessment instruments must be carefully selected from the construct of the instrument whose equivalence one wants to obtain. Guidelines with comprehensive information about the different methodological approaches are needed to support decision-making process of healthcare researchers, especially novice researchers.
Data Sharing Statement
All data analyzed during this study were included in this published article and its additional files.
Ethics Approval and Informed Consent
Ethical approval was obtained from the Ethics Committee from the Hospital de Cascais Dr. José de Almeida [Approval No 5/CE from 03/31/2021]. Before being included in the study, all participants received written and oral information and signed an informed consent form.
Acknowledgments
The authors wish to thank the Director of Nursing Dulce Gonçalves for supporting this research project from the first moment. We also thank Nurses Sónia Ganilho, José Friães, Vera Frasquilho, Filipe Pires, Rosário Costa, Carla Veigas, Sandra Letras, Carmen Gaudêncio and, Rita Carneiro for collecting the data. Additionally, the authors thank Cláudia Bacatum, Paulo Pereira, Richard Sidway, Rhian Atkin, Margarida Martins, Patrícia Silva, Laura Viegas, Carmen Gaudêncio, Rita Carneiro, and Jack Pun for their important contribution of knowledge and collaboration in the translation and transcultural adaptation process of the questionnaire BHAB. Finally, we thank every anonymous nurse who participated in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This paper was supported by the Nursing Research, Innovation, and Development Centre of Lisbon, (CIDNUR), Lisbon, Portugal [06/2023].
Disclosure
The authors declare that there is no conflict of interest regarding the publication of this paper.
References
1. Mardis T, Mardis M, Davis J, et al. Bedside shift-to-shift handoffs. J Nurs Care Qual. 2016;31(1):54–60. doi:10.1097/NCQ.0000000000000142
2. Goodridge D, McDonald M, New L, et al. Building patient capacity to participate in care during hospitalisation: a scoping review. BMJ Open. 2019;9(7):e026551. doi:10.1136/bmjopen-2018-026551
3. Jeffs L, Cardoso R, Beswick S, et al. Enablers and barriers to implementing bedside reporting: insights from nurses. Nurs Leadersh. 2013;26(3):39–52. doi:10.12927/cjnl.2013.23551
4. Bradley SM, Mott S. Handover: faster and safer? Aust J Adv Nurs. 2014;30(1):23–32.
5. Lupieri G, Creatti C, Palese A. Cardio-thoracic surgical patients’ experience on bedside nursing handovers: findings from a qualitative study. Intensive Crit Care Nurs. 2016;35:28–37. doi:10.1016/j.iccn.2015.12.001
6. McMurray A, Chaboyer W, Wallis M, Johnson J, Gehrke T. Patients’ perspectives of bedside nursing handover. Collegian. 2011;18(1):19–26. doi:10.1016/j.colegn.2010.04.004
7. Givens SE, Skully C, Bromley G. Psychiatric Inpatient Bedside Handoff: implementation of a Quality Improvement Project and Nurses’ Responses. J Psychosoc Nurs Ment Health Serv. 2016;54(7):33–37. doi:10.3928/02793695-20160616-06
8. Lu S, Kerr D, Mckinlay L. Bedside nursing handover: patients’ opinions. Int J Nurs Pract. 2014;20(5):451–459. doi:10.1111/ijn.12158
9. Olasoji M, Plummer V, Reed F, et al. Views of mental health consumers about being involved in nursing handover on acute inpatient units. Int J Ment Health Nurs. 2018;27(2):747–755. doi:10.1111/inm.12361
10. Jeffs L, Beswick S, Acott A, et al. Patients’ views on bedside nursing handover: creating a space to connect. J Nurs Care Qual. 2014;29(2):149–154. doi:10.1097/NCQ.0000000000000035
11. Mellawani YK, Nuraini T. Caring behavior of nurses is linked to the implementation of bedside handover between shifts. Enfermería Clínica. 2019;29:439–444. doi:10.1016/j.enfcli.2019.06.007
12. Köberich S. Nursing bed-side handover does not influence cardiac or vascular surgery patients involvement in decision-making about nursing care-an evaluation three months after implementation. Int J Caring Sci. 2014;7(3):823–833.
13. Kullberg A, Sharp L, Johansson H, Brandberg Y, Bergenmar M. Improved patient satisfaction 2 years after introducing person‐centred handover in an oncological inpatient care setting. J Clin Nurs. 2019;28(17–18):3262–3270. doi:10.1111/jocn.14903
14. Malfait S, Eeckloo K, Van Biesen W, Deryckere M, Lust E, Van Hecke A. Compliance with a structured bedside handover protocol: an observational, multicentred study. Int J Nurs Stud. 2018;84(8):12–18. doi:10.1016/j.ijnurstu.2018.04.011
15. DuBose BM, Mayo AM. Resistance to change: a concept analysis. Nurs Forum. 2020;55(4):631–636. doi:10.1111/nuf.12479
16. White-Trevino K, Dearmon V. Transitioning nurse handoff to the bedside: engaging staff and patients. Nurs Adm Q. 2018;42(3):261–268. doi:10.1097/NAQ.0000000000000298
17. Small A, Gist D, Souza D, Dalton J, Magny-Normilus C, David D. Using Kotter’s change model for implementing bedside handoff. J Nurs Care Qual. 2016;31(4):304–309. doi:10.1097/NCQ.0000000000000212
18. Mullen A, Harman K, Flanagan K, O’Brien B, Isobel S. Involving mental health consumers in nursing handover: a qualitative study of nursing views of the practice and its implementation. Int J Ment Health Nurs. 2020;1157–1167. doi:10.1111/inm.12756
19. Malfait S, Van Hecke A, Van Biesen W, Eeckloo K. Do bedside handovers reduce handover duration? An observational study with implications for evidence-based practice. Worldviews Evidence-Based Nurs. 2018;15(6):432–439. doi:10.1111/wvn.12330
20. Malfait S, Eeckloo K, Van Biesen W, Van Hecke A. Barriers and facilitators for the use of nursing bedside handovers: implications for evidence‐based practice. Worldviews Evidence-Based Nurs. 2019;16(4):289–298. doi:10.1111/wvn.12386
21. Burston S, Chaboyer W, Gillespie B, Carroll R. The effect of a transforming care initiative on patient outcomes in acute surgical units: a time series study. J Adv Nurs. 2015;71(2):417–429. doi:10.1111/jan.12508
22. Wollenhaup CA, Stevenson EL, Thompson J, Gordon HA, Nunn G. Implementation of a modified bedside handoff for a postpartum unit. J Nurs Adm. 2017;47(6):320–326. doi:10.1097/NNA.0000000000000487
23. Agency for Healthcare Research and Quality. Guide to Patient and Family Engagement in Hospital Quality and Safety. Agency Healthcare Res Quality. 2017:67.
24. Elkins KR, Nguyen CM, Kim DS, Meyers H, Cheung M, Huang SS. Successful strategies for high participation in three regional healthcare surveys: an observational study. BMC Med Res Methodol. 2011;11(1):176. doi:10.1186/1471-2288-11-176
25. Morgenthaler TI, Lovely JK, Cima RR, et al. Using a framework for spread of best practices to implement successful venous thromboembolism prophylaxis throughout a large hospital system. Am J Med Qual. 2012;27(1):30–38. doi:10.1177/1062860611411518
26. O’Connell B, Macdonald K, Kelly C. Nursing handover: it’s time for a change. Contemp Nurse. 2008;30(1):2–11. doi:10.5172/conu.673.30.1.2
27. Tobiano G, Marshall AP, Gardiner T, Jenkinson K, Shapiro M, Ireland M. Development and psychometric testing of the patient participation in bedside handover survey. Heal Expect. 2022;25(5):2492–2502. doi:10.1111/hex.13569
28. Slade D, Murray KA, Pun JKH, Eggins S. Nurses’ perceptions of mandatory bedside clinical handovers: an Australian hospital study. J Nurs Manag. 2019;27(1):161–171. doi:10.1111/jonm.12661
29. da Saúde M. Despacho n 9390/2021. Diário da república. 2021;187:96–103.
30. Beaton D, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine. 2000;25(24):3186–3191. doi:10.1097/00007632-200012150-00014
31. Sousa V, Rojjanasrirat W. Translation, adaptation and validation of instruments or scales for use in cross-cultural health care research: a clear and user-friendly guideline. J Eval Clin Pract. 2011;17(2):268–274. doi:10.1111/j.1365-2753.2010.01434.x
32. Epstein J, Santo RM, Guillemin F. A review of guidelines for cross-cultural adaptation of questionnaires could not bring out a consensus. J Clin Epidemiol. 2015;68(4):435–441. doi:10.1016/j.jclinepi.2014.11.021
33. Sekiguchi T, Hagiwara Y, Ando A, et al. Validation and reliability of a Japanese version of the Shoulder Pain and Disability Index: a cross-sectional study. J Orthop Sci. 2021;26(4):595–598. doi:10.1016/j.jos.2020.06.007
34. Hedrih V. Assessing equivalence of different language version of a test. In: Adapting Psychological Tests and Measurement Instruments for Cross-Cultural Research: Um Introduction. Routledge; 2020:126–127.
35. Bornman J, Sevcik RA, Romski M, Pae HK. Successfully translating language and culture when adapting assessment measures. J Policy Pract Intellect Disabil. 2010;7(2):111–118. doi:10.1111/j.1741-1130.2010.00254.x
36. Coster WJ, Mancini MC. Recommendations for translation and cross-cultural adaptation of instruments for occupational therapy research and practice. Rev Ter Ocup da Univ São Paulo. 2015;26(1):50. doi:10.11606/issn.2238-6149.v26i1p50-57
37. Erkut S. Developing multiple language versons of instruments for intercultural research. In: Ji M, editor. Cross-Cultural Health Translation: Exploring Methodological and Digital Tools. Routledge; 2019:9–10.
38. Amro I, Ghuloum S, Mahfoud Z, et al. Cross-cultural adaptation of the Arabic Positive and Negative Syndrome Scale in schizophrenia: qualitative analysis of a focus group. Transcult Psychiatry. 2019;56(5):973–991. doi:10.1177/1363461519850345
39. Beatty P. Developing measures of health behavior and he alth service utilization. In: Johnson TP, editor. Handbook on Health Survey Methods. Willey; 2015: 186–187. Available from: https://books.google.pt/.
40. Hilton A, Skrutkowski M. Translating Instruments Into Other Languages: development and Testing Processes. Cancer Nurs. 2002;25(1):1–7. doi:10.1097/00002820-200202000-00001
41. Herdman M, Fox-Rushby J, Badia X. A model of equivalence in the cultural adaptation of HRQoL instruments: the universalist approach. Qual Life Res. 1998;7(4):323–335. doi:10.1023/a:1024985930536
42. Borsa JC, Damásio BF, Bandeira DR. Adaptação e validação de instrumentos psicológicos entre culturas: algumas considerações. Paid. 2012;22(53):423–432. doi:10.1590/S0103-863X2012000300014
43. van Widenfelt BM, Treffers PDA, de Beurs E, Siebelink BM, Koudijs E. Translation and cross-cultural adaptation of assessment instruments used in psychological research with children and families. Clin Child Fam Psychol Rev. 2005;8(2):135–147. doi:10.1007/s10567-005-4752-1
44. Waltz CF, Strickland OL, Lenz ER. Other mesurement isues. In: Measurement in Nursing and Health Research.
45. Mardis M, Davis J, Benningfield B, et al. Shift-to-shift handoff effects on patient safety and outcomes. Am J Med Qual. 2017;32(1):34–42. doi:10.1177/1062860615612923
46. Sun L, Liu H, Tan M. Clinical handover at the bedside: an evidence-based quality implementation project. Int J Evid Based Healthc. 2016;14(4):186–187. doi:10.1097/01.XEB.0000511323.73435.9d
47. Cruchinho P Tradução e validação para população portuguesa do Bedside Handover Attitudes and Behaviours Questionnaire; 2022. Available from: https://comum.rcaap.pt/handle/10400.26/41493.
48. Lawson DO, Puljak L, Pieper D, et al. Reporting of methodological studies in health research: a protocol for the development of the methodologIcal Study reporting checklist (MISTIC). BMJ Open. 2020;10(12):1–11. doi:10.1136/bmjopen-2020-040478
49. Mbuagbaw L, Lawson DO, Puljak L, Allison DB, Thabane L. A tutorial on methodological studies: the what, when, how and why. BMC Med Res Methodol. 2020;20(1):1–12. doi:10.1186/s12874-020-01107-7
50. Clamp CGL, Gough S, Land L. Measurement. In: Resources for Nursing Research: An Annotated Bibliography.
51. Grove SK, Burns N, Gray JR. Selecting a quantitative research design. In: The Practice of Nursing Research: Appraisal, Synthesis, and Generation of Evidence. Sth. Elsevier; 2021:309.
52. International Council of Nurses.The ICN Code of Ethics for Nurses. International Council of Nurses; 2021. Available from: https://www.icn.ch/system/files/2021-10/ICN_Code-of-Ethics_EN_Web_0.pdf.
53. World Medical Association. WMA Declaration of Helsinki: ethical principles for medical research involving human subjects; 2018. Available from:https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/.
54. Hedrih V. Test translation. In: Adapting Psychologic Tests and Measurement Instruments for Cross-Cultural Research: Um Introduction. Routledge; 2020:48–98. Available from: https://books.google.pt/.
55. MacPhee M. Strategies and tools for managing change. JONA J Nurs Adm. 2007;37(9):405–413. doi:10.1097/01.NNA.0000285138.34247.5b
56. Grant JS, Davis LL. Selection and use of content experts for instrument development. Res Nurs Health. 1997;20(3):269–274. doi:10.1002/(sici)1098-240x(199706)20:3<269::aid-nur9>3.0.co;2-g
57. Scheidenhelm S, Reitz OE. Hardwiring bedside shift report. JONA J Nurs Adm. 2017;47(3):147–153. doi:10.1097/NNA.0000000000000457
58. Gregory S, Tan D, Tilrico M, Edwardson N, Gamm L. Bedside shift reports: what does the evidence say? J Nurs Adm. 2014;44(10):541–545. doi:10.1097/NNA.0000000000000115
59. Arafat S, Chowdhury H, Qusar M, Hafez M. Cross cultural adaptation and psychometric validation of research instruments: a methodological review. J Behav Heal. 2016;5(3):129. doi:10.5455/jbh.20160615121755
60. Polit DF, Beck CT, Owen SV. Is the CVI an acceptable indicator of content validity? Appraisal and recommendations. Res Nurs Health. 2007;30(4):459–467. doi:10.1002/nur.20199
61. Yusoff MSB. ABC of content validation and content validity index calculation. Educ Med J. 2019;11(2):49–54. doi:10.21315/eimj2019.11.2.6
62. Shi J, Mo X, Sun Z. Content validity index in scale development. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2012;37(2):152–155. doi:10.3969/j.issn.1672-7347.2012.02.007
63. Polit DF, Beck CT. The content validity index: are you sure you know what’s being reported? Critique and recommendations. Res Nurs Health. 2006;29(5):489–497. doi:10.1002/nur.20147
64. Schuster PM, Nykolyn L. Communication and patient safety: understanding the connection. In: Communication for Nurses: How to Prevent Harmful Events and Promote Patient Safety. F.A. Davis Company; 2010:3–10. Available from: https://books.google.pt/.
65. Miller KB, Hamza A, Metersky K, Gaffney DM. Nursing transfer of accountability at the bedside: partnering with patients to pilot a new initiative in Ontario community hospitals. Patient Exp J. 2018;5(1):90–96. doi:10.35680/2372-0247.1163
66. Oxelmark L, Whitty JA, Ulin K, Chaboyer W, Oliveira Gonçalves AS, Ringdal M. Patients prefer clinical handover at the bedside; nurses do not: evidence from a discrete choice experiment. Int J Nurs Stud. 2020;105:103444. doi:10.1016/j.ijnurstu.2019.103444
67. Kidd L. Promoting patient involvement through person-centred handovers in nursing. Evid Based Nurs. 2019;22(3):74. doi:10.1136/ebnurs-2018-102982
68. Willis G. Pretesting of health survey questionnaires: cognitive interviewing, usability testing, and behavior coding. In: Johnson TP, editor. Handbook on Health Survey Methods. Willey; 2015:221.
69. Wild D, Grove A, Martin M, et al. Principles of good practice for the translation and cultural adaptation process for patient-reported outcomes (PRO) measures: report of the ISPOR task force for translation and cultural adaptation. Value Heal. 2005;8(2):94–104. doi:10.1111/j.1524-4733.2005.04054.x
70. Webster KA, Peipert JD, Lent LF, Bredle J, Cella D. Translations/Universal translation approach. In: Kassianos AP, editor. Handbook of Quality of Life in Cancer. Spinger Publishing; 2022:84.
71. Issel LM. Sampling designs and data sources for effect evaluations. In: Health Program Planning and Evaluation: A Practical Systematic Approach for Community Health.
72. Holyk GG. Question testing methods. In: Encyclopedia of Survey Research Methods. Vol. II. Sage; 2008:658–659.
73. Korabik K, van Rhijn T. Best practices in scale translation and establisment mesurement equivalence. In: Shockey KM, Shen W, Johnson RC, editors. The Cambridge Handbook of the Global Work–Family Interface. Cambridge University Press; 2018:212–229.
74. Beaton D, Bombardier C, Guillemin F, Ferraz MB. Recommendations for the cross-cultural adaptation of the DASH & QuickDASH outcome measure. Inst Work Heal. 2007;45.
75. Luepker RV, Evans A, McKeigue P, Reddy KS. Conduction the research. In: Cardiovascular Survey Methods.
76. Guillemin F, Bombardier C, Beaton D. Cross-cultural adaptation of health-related quality of life measures: literature review and proposed guidelines. J Clin Epidemiol. 1993;46(12):1417–1432. doi:10.1016/0895-4356(93)90142-N
77. Erkut S, Alarcón O, Coll CG, Tropp LR, García HAV. The dual-focus approach to creating bilingual measures. J Cross Cult Psychol. 1999;30(2):206–218. doi:10.1177/0022022199030002004
78. St. Amant K. A new web for the new millennium. In: Lipson C, Day M, editors. Technical Communication and the World Wide Web. Lawrence Erlbaum Associates Publishers; 2005:148.
79. Silverblatt A, Zlobin N. Production elements. In: International Communications: A Media Literacy Approach. Routledge; 2015:108. Available from: https://books.google.pt/.
80. Mattielo E. The influence of English slang on Intalian. In: Coleman J, editor. Global English Slang Methodologies and Perspectives. Routledge; 2014:150.
81. Drasgow F, Probst TM. The psicometrics of adaptation: evaluating measurement equivalance across languages and cultures. In: Hambletom RK, Merenda PF, Spielberg CD, editors. Adapting Educational and Psychological Tests for Cross-Cultural Assessment. Lawrence Erlbaum Associates Publishers; 2005:361.
82. Peña ED. Lost in translation: methodological considerations in cross-cultural research. Child Dev. 2007;78(4):1255–1264. doi:10.1111/j.1467-8624.2007.01064.x
83. Coll-Risco I, Camiletti-Moirón D, Acosta-Manzano P, Aparicio VA. Translation and cross-cultural adaptation of the Pregnancy Physical Activity Questionnaire (PPAQ) into Spanish. J Matern Neonatal Med. 2019;32(23):3954–3961. doi:10.1080/14767058.2018.1479849
84. Grundström H, Rauden A, Olovsson M. Cross-cultural adaptation of the Swedish version of Endometriosis Health Profile-30. J Obstet Gynaecol. 2020;40(7):969–973. doi:10.1080/01443615.2019.1676215
85. Marcondes FB, de Vasconcelos RA, Marchetto A, de Andrade ALL, Filho AZ, Etchebehere M. Translation and cross-cultural adaptation of the Rowe score for Portuguese. Acta Ortop Bras. 2012;20(6):346–350. doi:10.1590/S1413-78522012000600007
86. Muquith MA, Islam MN, Haq SA, Ten Klooster PM, Rasker JJ, Yunus MB. Cross-cultural adaptation and validation of a Bengali version of the modified fibromyalgia impact questionnaire. BMC Musculoskelet Disord. 2012;13(1):1. doi:10.1186/1471-2474-13-157
87. Nepal GM, Shrestha A, Acharya R. Translation and cross-cultural adaptation of the Nepali version of the Rowland universal dementia assessment scale (RUDAS). J Patient-Reported Outcomes. 2019;3(1). doi:10.1186/s41687-019-0132-3
88. Polesello GC, Godoy GF, De Castro Trindade CA, De Queiroz MC, Honda E, Ono NK. Translation and cross-cultural adaptation of the modified Hip outcome tool (mhot) into Portuguese. Acta Ortop Bras. 2012;20(2):88–92. doi:10.1590/S1413-78522012000200006
89. Warrender D. Self-disclosure: the invaluable grey area. Br J Ment Heal Nurs. 2020;9(1):9–15. doi:10.12968/bjmh.2019.0010
90. Sully P, Dallas J. Appendix 1 – glossary. In: Nicol M, editor. Essential Communication Skills for Nursing & Midwifery.
91. Miller E, Webb L. Active listening and atending: communication skills and the healthcare environment. In: Webb L, editor. Nursing: Communication Skills in Practice.
92. Blake T, Blake T. Improving therapeutic communication in nursing through simulation exercise. Teach Learn Nurs. 2019;14(4):260–264. doi:10.1016/j.teln.2019.06.003
93. Unhjem JV, Vatne S, Hem MH. Transforming nurse-patient relationships-A qualitative study of nurse self-disclosure in mental health care. J Clin Nurs. 2018;27(5–6):e798–e807. doi:10.1111/jocn.14191
94. Sully P, Dallas J. Introduction. In: Nicol M, editor. Essential Communication Skills for Nursing & Midwifery.
95. Racine JL, Gillespie K, Hartke K, Wautlet C, Antony KM. Barriers to self-disclosing level of maternal care: what are Wisconsin hospitals worried about? WMJ. 2021;120(1):45–50.
96. Zhang W, Zhang H. Effects of comprehensive nursing intervention based on self-disclosure on improving alexithymia in elder patients with coronary heart disease. BMC Nurs. 2022;21(1):216. doi:10.1186/s12912-022-01006-w
97. Zhao H, Li X, Zhou C, Wu Y, Li W, Chen L. Psychological distress among Chinese patients with breast cancer undergoing chemotherapy: concordance between patient and family caregiver reports. J Adv Nurs. 2022;78(3):750–764. doi:10.1111/jan.15004
98. Ghaffari F, Dehghan-Nayeri N, Shali M. Nurses’ experiences of humour in clinical settings. Med J Islam Repub Iran. 2015;29:182.
99. Tanay MA, Wiseman T, Roberts J, Ream E. A time to weep and a time to laugh: humour in the nurse–patient relationship in an adult cancer setting. Support Care Cancer. 2014;22(5):1295–1301. doi:10.1007/s00520-013-2084-0
100. Sousa LMM, Marques-Vieira CMA, Antunes AV. Humor intervention in the nurse-patient interaction. Rev Bras Enferm. 2019;72(4):1078–1085. doi:10.1590/0034-7167-2018-0609
101. Rose SL, Spencer RJ, Rausch MM. The use of humor in patients with recurrent ovarian cancer. Int J Gynecol Cancer. 2013;23(4):775–779. doi:10.1097/IGC.0b013e31828addd5
102. Sim IO. Humor intervention program for children with chronic diseases. Appl Nurs Res. 2015;28(4):404–412. doi:10.1016/j.apnr.2015.09.001
103. Chenoweth L, Low L-F, Goodenough B, et al. Potential benefits to staff from humor therapy with nursing home residents. J Gerontol Nurs. 2014;40(2):47–52. doi:10.3928/00989134-20130930-01
104. Campbell D, Dontje K. Implementing bedside handoff in the emergency department: a practice improvement project. J Emerg Nurs. 2019;45(2):149–154. doi:10.1016/j.jen.2018.09.007
105. Elgin KW, Poston RD. Optimizing registered nurse bedside shift report: innovative application of simulation methods. J Nurses Prof Dev. 2019;35(2):E6–E14. doi:10.1097/NND.0000000000000526
106. Wong X, Tung YJ, Peck SY, Goh ML. Clinical nursing handovers for continuity of safe patient care in adult surgical wards: a best practice implementation project. JBI Database Syst Rev Implement Reports. 2019;17(5):1003–1015. doi:10.11124/JBISRIR-2017-004024
107. Johnson M, Jefferies D, Nicholls D. Developing a minimum data set for electronic nursing handover. J Clin Nurs. 2012;21(3–4):331–343. doi:10.1111/j.1365-2702.2011.03891.x
108. Nelson BA, Massey R. Implementing an electronic change-of-shift report using transforming care at the bedside processes and methods. J Nurs Adm. 2010;40(4):162–168. doi:10.1097/NNA.0b013e3181d40dfc
109. Johnson M, Sanchez P, Suominen H, et al. Comparing nursing handover and documentation: forming one set of patient information. Int Nurs Rev. 2014;61(1):73–81. doi:10.1111/inr.12072
110. Tobiano G, Whitty JA, Bucknall T, Chaboyer W. Nurses’ perceived barriers to bedside handover and their implication for clinical practice. Worldviews Evidence-Based Nurs. 2017;14(5):343–349. doi:10.1111/wvn.12241
111. Streeter AR, Harrington NG. Nurse handoff communication. Semin Oncol Nurs. 2017;33(5):536–543. doi:10.1016/j.soncn.2017.10.002
112. Kim EJ, Seomun G. Handover in Nursing: a Concept Analysis. Res Theory Nurs Pract. 2020;34(4):297–320. doi:10.1891/RTNP-D-19-00089
113. Delgado-Rico E, Carrectero-Dios H, Ruch W. Content validity evidences in test development: an applied perspective. Int J Clin Heal Psychol. 2012;12(3):449–459.
114. Morse JM, Carter B. The essence of enduring and expressions of suffering: the reformulation of self. Sch Inq Nurs Pract. 1996;10(1):43–60.
115. Riccio CA, Yoon H, McCormick AS. Neuropsychological test selection with clients who are Asian. In: In: Davis JM, D´Amato RC, editors. Neuropsychology of Asians and Asian-Americans: Practical and Theoretical Considerations. Spinger Publishing; 2014:153.
116. Haynes SN, Richard DCS, Kubany ES. Content validity in psychological assessment: a functional approach to concepts and methods. Psychol Assess. 1995;7(3):238–247. doi:10.1037/1040-3590.7.3.238
117. Schirm V, Banz G, Swartz C, Richmond M. Evaluation of bedside shift report: a research and evidence-based practice initiative. Appl Nurs Res. 2018;40:20–25. doi:10.1016/j.apnr.2017.12.004
118. Buus N, Hoeck B, Hamilton BE. Nurses’ shift reports: a systematic literature search and critical review of qualitative field studies. J Clin Nurs. 2017;26(19–20):2891–2906. doi:10.1111/jocn.13655
119. McCloskey RM, Furlong KE, Hansen L. Patient, family and nurse experiences with patient presence during handovers in acute care hospital settings. JBI Database Syst Rev Implement Reports. 2019;17(5):754–792. doi:10.11124/JBISRIR-2017-003737
120. Davis LL. Instrument review: getting the most from a panel of experts. Appl Nurs Res. 1992;5(4):194–197. doi:10.1016/S0897-1897(05)80008-4
121. Morgan RO, Sail KR, Witte LE. Patient-reported outcomes data. In: Richessen RL, Andrews JE, editors. Clinical Research Informatics.
122. Slocumb EM, Cole FL. A practical approach to content validation. Appl Nurs Res. 1991;4(4):192–195. doi:10.1016/S0897-1897(05)80097-7
123. Almanasreh E, Moles R, Chen TF. Evaluation of methods used for estimating content validity. Res Soc Adm Pharm. 2019;15(2):214–221. doi:10.1016/j.sapharm.2018.03.066
124. Nursing Research Society of India. Theoretical and conceptual frameworks. Nursing Research and Statistics; Pearson; 2013. 88–113.
125. Sand-Jecklin K, Sherman J. A quantitative assessment of patient and nurse outcomes of bedside nursing report implementation. J Clin Nurs. 2014;23(19–20):2854–2863. doi:10.1111/jocn.12575
126. Street M, Eustace P, Livingston PM, Craike MJ, Kent B, Patterson D. Communication at the bedside to enhance patient care: a survey of nurses’ experience and perspective of handover. Int J Nurs Pract. 2011;17(2):133–140. doi:10.1111/j.1440-172X.2011.01918.x
127. Sand-Jecklin K, Sherman J. Incorporating bedside report into nursing handoff: evaluation of change in practice. J Nurs Care Qual. 2013;28(2):186–194. doi:10.1097/NCQ.0b013e31827a4795
128. Evans D, Grunawalt J, McClish D, Wood W, Friese CR. Bedside shift-to-shift nursing report: implementation and outcomes. Medsurg Nurs. 2012;21(5):281–284, 292.
129. Kassean HK, Jagoo ZB. Managing change in the nursing handover from traditional to bedside handover: a case study from Mauritius. BMC Nurs. 2005;4(1):1. doi:10.1186/1472-6955-4-1
130. Parent M. The Gemba. In: The Lean Innovation Cycle: A Multidisciplinary Framework for Designing Value with Lean and Human-Centered Design. Taylor & Francis; 2022:67.
131. Carvalho AM, Lucchesi D. Portuguese in contact. In: Wetzels WL, Costa J, Menuzzi S, editors. The Handbook of Portuguese Linguistics. Wiley-Blackwell; 2016:41.
132. CPLP. CPLP: comunidade dos países de Língua Portuguesa; 2022. Available from:https://www.cplp.org/id-2597.aspx.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.