")
Back to Journals » Journal of Healthcare Leadership » Volume 15
Ethical Leadership in LTC: From Caregivers’ Customer Orientation to Senior’s Satisfaction and Well-Being
Received 18 July 2023
Accepted for publication 13 October 2023
Published 2 November 2023 Volume 2023:15 Pages 297—311
DOI https://doi.org/10.2147/JHL.S426602
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pavani Rangachari
Miriam Etges,1 Arnaldo Coelho2
1Project Department, International Iberoamerican University, Campeche, México; 2CeBER – Faculty of Economics, University of Coimbra, Coimbra, Portugal
Correspondence: Miriam Etges, Project Department, International Iberoamerican University, Rua Pastor Hildebrand, 81, Santa Cruz do Sul/RS - CEP, 96.810-084, Brasil, Tel +55 51 984079747, Email [email protected]
Background: In response to the growth of the world’s senior population, an investigation of ethical leadership on LTCs is needed, in particular in the impact it may have on customer orientation and on seniors’ well-being.
Objective: We propose a model to identify the relationship between ethical leadership in LTCs and caregivers’ customer orientation, and its influence on satisfaction with the service, satisfaction with life, and the quality of the interaction between caregivers and seniors.
Sampling: We present a matched sample of 277 caregivers and 277 elderly Brazilians, workers and seniors’ in LTCs in Brazil. The minimum sample size was 222, determined using G-Power software version 3.1.9.2, based on the desired statistical power parameters and the number of predictors. Two structured questionnaires were developed, one for caregivers and the other for the elderly. 69 LTCs were contacted and 29 participated in the survey (10 nonprofit, 34.48%). Data were treated statistically using SEM modelling.
Results: We identified a positive influence of ethical leadership on caregivers’ attitudes, favoring their orientation towards the seniors’. A positive relationship between customer-oriented caregivers and customer satisfaction, life satisfaction, and the quality of the senior’s interaction. A customer-oriented caregiver exerts a mediating effect between ethical leadership and the seniors’ related outcomes, making ethical leadership beneficial to seniors and their family members.
Conclusion: Ethical leadership favors successful management of LTCs, increasing customer orientation, and provides clues to establish a better causality and a chain of effects between leadership and senior-related outcomes. Therefore, LTCs may be the appropriate outlet for the role of ethics in leadership.
Practical Implications: This study provides managers with an understanding of the effects of ethical leadership in the context of LTCs, for both caregivers and seniors. The powerful effects of ethical leadership can be a stimulus to increase the role of ethics in LTCs, improving the quality of care, the well-being of the seniors, and, therefore, the human and financial performance of these institutions.
Keywords: ethical leadership, seniors, formal caregiver, patient, customer orientation
Introduction
According to the Aging World Population 2019, there were 703 million people aged 65 and over in 2019, changing patterns of longevity, death, and illness.1,2 Knowing where people live and where they may die is essential for the education and training of caregivers to ensure a workforce that provides good care, allowing older people to live better.1 According to Spasova, Baeten, and Vanhecke (2018) the European LTC service faces challenges in the quality of care, access and adequate provision and financial sustainability, among others. In Brazil, there are more than 2000 nonprofit organizations that provide specific care for the elderly.3 LTCs are fundamental for the care of the elderly, but in Brazil the lack of data on the sector points to the invisibility of both these units and their residents.4 It is vital to have a living environment where the senior can count on the necessary support to compensate for the physical and social changes that accompany aging.5 Older people want to live in a safe environment, receive good care, and exercise personal control and autonomy. Therefore, caregivers must find the right balance between the needs of the senior and the needs of the organization,6 providing the senior with an excellent experience and quality of life through a human relationship where there is affection, and sensitivity.5 The healthcare environment is challenging and needs leaders who promote technical and professional training but also work to improve staff satisfaction and morale.7
Caregiver satisfaction and positive results in the relationship with the senior are often related to leadership.8 Healthcare professionals are interested in leaders who can lead in positive and encouraging ways,9 reducing burnout and promoting happiness in healthcare work.10 Leadership can be associated with customer orientation,11,12 encouraging a focus on patients and clients, and establishing an excellent service climate and quality of care service.
Organizations are working, for the first time in history, with four different generations at the same time (Silent Generation, Baby Boomer Generation, Generation X, and Generation Y),13 and servant and ethical leadership aligns with interdisciplinary collaboration,7 fostering teamwork and addressing the needs of residents while respecting the cultural aspects of the team and seniors and their families.8,13–15
Ethical leadership has been offering ethical and effective guidance, prioritizing moral and ethical codes, and providing occupational satisfaction to employees and employees’ willingness to make extra efforts.16 The attitudes of ethical leaders can adapt to the demands of the caregiver profession, especially on the nursing side, for the benefit of the senior, families, and organizations17.
Leadership in the health service has been studied in different ways. The quality side of leadership quality,14 where its influence may be direct and indirect, improving working and care conditions, therefore generating job satisfaction and staff retention.8 Transformational leadership9,13 promotes staff retention and job satisfaction in nursing services. In seniors LTC,18,19 this leadership style is essential to increase senior safety, facilitates the balance between resources and work demands, as well as the balance between effort and reward in the work of caregivers, and creates a solid safety culture in the health services. A leader with proper normative conduct becomes an ethical leader,20 creating circumstances where doing the right thing is expected and valued.21
Specchia et al show a significant correlation between leadership style and job satisfaction in health services, affecting the professionals, performance, improving the work environment, and the seniors’ well-being. Good leaders need to signal the behaviors they want to see replicated by their followers,10 leading by example rather than words.13 Competent leaders, who promote happiness in the organization, and prevent burnout, can strongly impact seniors’ satisfaction, safety and quality of life, and the productivity and financial efficiency of LTCs.10
The relationship between leadership and customer orientation is known.11 However, according to Liaw et al, how ethical leadership can contribute to improving ethical standards, customer-oriented behaviors, and seniors’ satisfaction is a relationship that has received little attention in the existing literature.11 The literature presents us with how leaders perceive their ethical role,22 the importance of leadership in increasing the quality of care,9 ethical behavior focused on the elderly for organizational success,21 there are still gaps to be investigated. Although there are empirical studies on the positive impact of ethical leadership on the health service quality16 for seniors’, families, and organizations,17 the study of ethical leadership and its influence on caregivers orientation towards the seniors’ and the impacts of the caregiver/old aged relationship on this senior’s life quality is an issue that needs to be investigated.14 The caregiver/senior interaction requires emotional balance, control, and overcoming from the professional, often in the face of the senior’s aggressiveness and imminent death.5 The effects of ethical leadership on the results desired by the client, which are expected to be quite indirect, still need links or tools that help to transfer these effects because, according to Ko et al, studies on ethical leadership are a fragmented field.23 The relationship between ethical business practices and customer orientation have to be unpacked and further research is needed to help avoid misconducts24 and provide a better experience to customers. Therefore, this leadership style deserves further investigation in the hospitality and healthcare sectors where ethical issues and deviant behaviours may have special impacts on customers and their families.25 In fact, some recent major disruptive events like the covid outbreak increased the risks in logistics and labour,26 while the old-age dependency ratio almost doubled in the last 50 years and tend to increase.27
Our study aims to analyze the relationship between ethical leadership and customer orientation and the consequent influence on seniors´ satisfaction, quality of interaction with the caregiver, and satisfaction with life through the actions of the client-oriented caregiver, based on the perceptions of the old-aged. Additionally, this investigation innovates by exploring the influence of ethical leadership on the customes’ desired outcomes, like satisfaction with life, care, and the quality of the senior’s interaction with the caregiver, using the mediating effect of customer orientation (CO). To do so, we collected data from paired caregivers and the senior to establish this chain of effects.
The methodology used in this investigation is based on applying a structured questionnaire to 277 caregivers and 277 senior residents of 29 LTCs in the Rio Grande do Sul/Brazil, and the hypotheses testing was performed using structural equation modeling. This article is organized as follows: foundations for the research and hypotheses development, then the description of the research method, followed by the presentation and discussion of the results. Finally, we conclude with practical implications for leadership in LTC, with directions for future research.
Literature Review and Hypotheses Development
Ethical Leadership
In recent years, ethical leadership has become popular in leadership and business.28 Especially in nursing leadership, those who are self-aware, recognize their strengths and weaknesses, and exhibit humility while interacting calmly with colleagues, patients, and families through eye contact help others “feel cared for”.29–31 Ethical leaders treat their employees fairly,32 promoting social exchange behaviors among employees, fostering virtuous attitudes of civic behavior, and assisting in personal and collective solutions for the organization and the community, aiming for the common good.10,31,33
According to Gandolfi and Stone (2018), despite numerous pieces of research on leadership styles, there is still a deficiency in examining the leadership “style”. Buchanan (2013) believes that leadership has evolved since the 1980s from a “command and control” concept to an “empower-and-track” approach until the 2000s and a “connect and nurture” approach in the present.34 Lewin, Lippitt, and White (1939) categorized and introduced leadership styles from the autocratic, democratic, and laissez-faire frameworks, enabling the emergence of future styles based on leader/follower relationships.34 Although there are many definitions of ethical leadership, the most cited is that of Brown, Trevino & Harrison (2005), who define ethical leadership as the demonstration of proper conduct through personal actions and interpersonal relationships and promotes such conduct to followers through two-way communication, reinforcement and decision making.23 The same authors understood ethical leadership as an emerging concept to compare it with an approach related to transformation, authenticity, and spirituality.23 Ethical leadership demonstrates proper conduct through personal actions and relationships and promotes that conduct in followers through two-way communication, reinforcement, and decision.23 According to Treviño & Brown (2000), we can find two main components in an ethical leader: a moral person and a moral manager. A moral person is characterized by individual traits such as honesty, integrity, reliability, fairness, and selfless motivation, who cares about and supports their employees, cares about the overall society, and behaves as an exceptional role model. The moral manager proactively influences employees’ values, beliefs, and thoughts around an ethical message, playing an essential role in shaping employee behavior.35,36 The moral manager can influence followers through the model intention of ethical behavior, establishing responsibilities, and linking the ethical behavior of employees to the organizational performance management system.37 Ethical leaders guide desirable and undesirable conduct through transactional forms of leadership, reinforcing employees’ expected behaviors through a reward system.37 It is from the leader’s attitude, influencing their followers through actions, that followers develop work engagement, commitment, and citizenship behaviors, thus enhancing the organization’s success.30,38
The behaviors raised by leader-follower relationships in change-oriented or task-oriented leadership styles are decisive.13 The leader can promote good conditions and job satisfaction for the caregivers, leading them to put the best dedication on the care of the old-aged, therefore achieving the organizational result of high-quality care for the seniors and their satisfaction and delight.18 According to Rooke & Torbet (2005), leaders interpret their environment, which influences their reactions in different situations, demanding a high degree of self-knowledge and emotional intelligence from the leader in the context inside and outside the organization.34 The ethical executive leader must find ways to guide the organization in ethics, values, and principles that will guide the actions of all employees.35
The Social Learning Theory developed by Bandura (1977) shows how people learn norms and behaviors from credible and attractive others.20 When people learn through behavior, when managers behave in a fair, honest, trustworthy, and caring way, a positive cycle is created where this behavior is perpetuated in the work climate.39 Ethical leaders contribute to greater satisfaction in the lives of their followers, as they are perceived as their supporters, creating a climate of trust and two-way communication, and promoting a positive work experience.40 Competition among LTCs has increased due to longevity,13 requiring ethical and strong leaders who understand that values and morality are shaped by education, professional guidance, society, and the organizational context where ethics occur.22 In this way, ethical leaders tend to encourage individual and collective citizenship behaviors, developing collective solutions for the common good of the community41 and retaining talent within the organization.9 Yang’s (2014) study positively associates ethical leadership with followers’ well-being and life satisfaction, mediated by job satisfaction. It is vital that the practice of ethical leadership on the leader himself, pointed out in the study by Inceoglu et al, that by complying with and enforcing workplace regulations, leaders experience greater happiness and life satisfaction.40 Table 1 shows the main interactions of ethical leadership with the employees’ and customer-related outcomes.
 |
Table 1 Interactions of Ethical Leadership with the Employees’ and Customer-Related Outcomes |
Ethical leadership in LTC becomes challenging due to the dual focus on quality: quality of care provided and perceived quality of life.9 Ethical leadership practices at LTC may help increase the caregiver team engagement and empowerment,42 which contributes to the functional improvement and autonomy of the senior, increasing their satisfaction and quality of life.43 Ethical leadership has a positive and direct impact on the ethical climate and ethical behavior of employees and customer satisfaction, as it is customer-oriented.12,41 Leaders capable of good relationship management and with social skills will find satisfaction in their work and enable their subordinates to feel the same, positively impacting the elderly and family members with a sense of care, generating happiness.29,32
Customer Orientation
Customer orientation (CO) is defined as meeting the customers’ interests, needs, and expectations and delivering services tailored to the employees’ behavior.44 Ifie (2014) and Narver and Slater (1990) approach CO as the organization putting the interests of customers first, and Zablah et al conceptualize a customer-oriented employee in two ways: as a set of behaviors aimed at customer satisfaction or as a psychological variable that motivates employees to satisfy the needs of their customers.12 According to Genzi et al, customer orientation is an essential and positive predictor of service worker development, directly related to customer repurchase interest.45 CO is widely used in marketing practice, whose concept says that an organization identifies the needs of a target market and adapts to satisfy its needs better than its competition, providing a positive buying experience and generating customer satisfaction, therefore achieving the company´s objectives.44 Recently, studies are approaching more broadly from the theory of Stakeholders, which proposes that creation and value be a collaborative effort in relationships that ideally benefits the business in question and all stakeholders.46
In healthcare organizations (patients/seniors are customers), CO is defined as the ability to provide care to adapt its service to reflect the reality of seniors, providing quality of life, satisfaction, and well-being, thus improving the effectiveness of the service. When the CO focuses on the senior, on how they care for internal clients (employees), who care for external clients (seniors), the leadership role is the main driver of health service excellence. While there are empirical studies that examine the relationship between different forms of leadership and CO, there is little research on the role of ethical leadership in CO.12 The study by Walumbwa et al shows that when employees perceive that leadership acts in their best interests, is fair and respectful, they tend to reciprocate by improving their performance in performing tasks.12 A study by Kumar (2017) shows that a change in leadership can affect service usage decisions, namely based on CO, which can result in better or worse customer service and high or low service quality, and more or less senior satisfaction.11 Shaller (2007) points out that the most critical factor for improving health care is the commitment and engagement of senior leadership and the way it promotes CO. According to social learning theory, employees learn through behavior20 and replicate based on the example and signals they receive from their supervisors. Once the relationship between internal customers (employees) has high quality, the relationship with external customers (seniors) will improve, increasing the quality of health services.11 Therefore, according to Lindblom (2015), employees’ perception of ethical leadership is closely related to the employee’s CO. Therefore, the following hypothesis is proposed:
H1: There is a positive relationship between ethical leadership and customer orientation.
Customer Satisfaction
Oliver’s (2010) studies define Customer Satisfaction (CS) as the post-consumption consumer’s judgment about whether the good or service provided a pleasurable level of general satisfaction related to its use.47 Regarding CS in the service sector, Grönroos (1984) states that perceived quality is an evaluation procedure where the customer compares their expectations with what is observed in the service15 and may be close to the concept of satisfaction. Therefore, Pekkaya et al CS measures perceived service quality and customer expectations.48 Research developed by Frambach et al points out that CO is valuable in maintaining harmonious relationships and positive expectations between customers and employees,45 thus influencing customer loyalty.49 Job satisfaction is positively impacted by ethical leadership and the ethical climate that these leaders cultivate in the workplace,17 enhancing employees’ personal development and their feelings of affective well-being.50 According to the study by Zhang et al, this influence can be extended to the WOM, which, according to the author, can be one of the most persuasive elements of customer behavior.51
In LTCs, formal caregivers establish intimate bonds with the senior, and their work is both emotional and objective, resulting in positive and negative aspects for both the caregiver and the senior.5 Therefore, OC can provide additional satisfaction based on attention and a good relationship between caregivers and seniors.52 Authors show that senior satisfaction involves evaluating courtesy, respect, kindness, and individualized attention received from professionals and can lead to positive WOM.52,53 The satisfaction of the seniors is significant because the caregiver provides information and respect and makes them participate in decision-making regarding their care and treatment.52 Thus, in an LTC where social and family ties can be broken, the caregiver/senior relationship may undergo a process of replacing old social roles with new ones: the care provided by a CO caregiver tends to favor the quality of aging and life, health, with positive and significant impacts on quality of life and well-being.6 Even in the face of stress and suffering, the professional caregiver can feel pleasure and reward in helping the other, providing senior satisfaction from the CO behavior.54 Therefore, the following hypothesis is proposed:
H2: There is a positive relationship between Customer Orientation and Customer Satisfaction.
Interaction Quality
Frambach et al consider CO in service companies to be valuable as it leads to a more harmonious relationship between workers and customers, maintaining high customer expectations.45 Thus, according to Gronroos (1982, 1984), based on the way the service is provided, customers tend to evaluate the quality of interaction (IQ).55 Bitner (1990) shows that the behaviors and attitudes of service workers greatly influence the customer’s perception of service quality.56 Regarding customer satisfaction (CS), Gerrard and Cunningham (2001) emphasize that the role of the service professional is very important, an approach supported by Jamel and Nasser (2002), stating that the IQ between customer and employee directly influences the CS, being the quality of this relationship is an antecedent of CS.57 A study by Gaur et al shows that the critical point to leverage CS is IQ based on politeness, sympathy, sensitivity, and empathy. IQ leads seniors to be well informed about their health conditions and treatment, reducing uncertainty about their health and increasing CS levels.57
Guided by their leadership, CO caregivers are more likely to help and understand the senior, trying to help them get better healthcare.11 Gaur et al point out that seniors informed about their conditions and treatment alternatives through polite communication with employees may present a lower level of vulnerability about their conditions, which can mean high consumer loyalty.55 Mutual IQ is a desirable outcome of ongoing care that a CO caregiver can turn into solid and meaningful bonds, improving the well-being of the senior.58 Therefore, the following hypothesis is proposed:
H3: There is a positive relationship between employees’ customer orientation and interaction quality.
Life Satisfaction
For Johnson (1978), life satisfaction (LS) is a cognitive assessment of life as a whole, where judgments are based on subjective criteria and not necessarily reflecting external conditions.54 Diener (1984) conceptualized LS as the cognitive assessment of life.59 Emotionally, everyday life consists of ups and downs and influences CS with life60 remains in doubt. Studies by Borg, Halberg and Blomkvist (2006), Bozkurt & Ylmaz (2016) and Jung, Muntaner and Choi (2010) point out that for the senior there is a relationship between functional capacity and LS, followed by studies by Bangerter, Heid, Abbott and Van Haitsma (2017) and Sherwin & Winsby (2010) who relate autonomy to LS.43 The family/life satisfaction domain approach contributes more to overall LS in older adults than, for example, satisfaction with standard of living and health.61 Therefore, CO caregivers should be more likely to create a family climate for the senior and foster close relationships between staff and seniors.5 CO caregivers develop perceptions of the pace of life of the senior, meeting their needs, expectations, and interests, strengthening bonds.5 CO caregivers can provide highly personalized and CS quality services and develop patient-centered care for senior safety.11 Being cared for and nourished can reinforce the process of feeling healthy, favoring the quality of life and LS of the senior.6 Therefore, the following hypothesis is proposed:
H4: Customer orientation is positively related to senior life satisfaction.
Mediation
The influence of ethical leadership (EL) on senior-related outcomes can be pretty indirect9 since leadership plays a fundamental role in providing efficient care for the senior, based in particular on the excellence of the professional care and the human climate and harmonious and healthy environment.7 The impacts of EL on CO are known,12,58,62 even if these effects are not sufficiently explored.12,21 The different effects of leadership on service quality, customer outcomes, and organizational goals lack understanding.7 According to Specchia (2021), there is a correlation between the leadership style and the caregivers’ job satisfaction, influencing the team’s performance.7 It was proposed to investigate the impacts of CO orientation on CS, interaction quality, and LS since caregivers are guided by EL, encouraging effort and quality of care on the team.17 Therefore, EL can have an indirect effect on CS, IQ, and EL through the mediating effects of CO since ethical leadership can contribute to the satisfaction of its subordinates, providing a positive work experience, bringing improvement of their efforts in customer relationships.40 Therefore, the following hypotheses are proposed: H5a: CO mediates the relationship between ethical leadership and senior satisfaction. H5b: CO mediates the relationship between ethical leadership and the quality of the senior’s interaction. H5c: CO mediates the relationship between ethical leadership and the life satisfaction of the senior.
Method
Caregivers are subordinate to leadership that will affect them positively (or not), improve the senior’s quality of care, and decrease healthcare costs by reducing staff turnover,9 affecting caregivers and the senior in many ways. Hence, this study examines how leadership style influences the caregiver and, consequently, the senior, directly and indirectly. The conceptual research model and the suggested relationships between the study variables are shown in Figure 1.
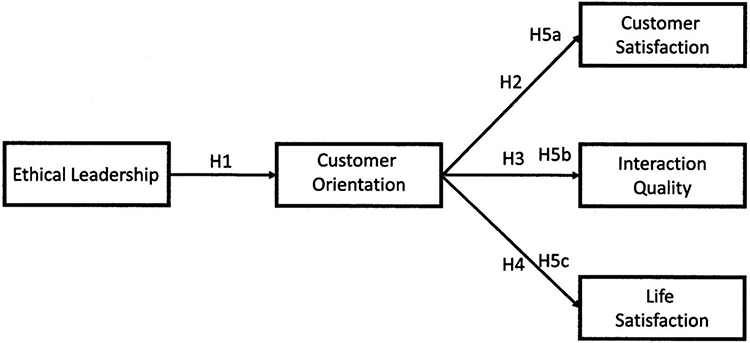 |
Figure 1 Conceptual research model and the suggested relationships between the study variables. |
Sampling
We present a matched sample of 277 caregivers and 277 elderly Brazilians, workers and seniors’ in LTCs in Brazil. The minimum sample size was 222, determined using G-Power software version 3.1.9.2, based on the desired statistical power parameters and the number of predictors. This sample size was significant for the effect size f2 (0.15), alpha=0.05, and confidence interval of 0.95.63,64 In fact, the final sample had more respondents caregivers, than seniors, and it was possible to retain one respondent per caregiver, and eliminated the others. Therefore, to each caregiver corresponds only one senior.
Two structured questionnaires were developed, one for caregivers and the other for the elderly. 69 LTCs were contacted and 29 participated in the survey (10 nonprofit, 34.48%). Information was collected from caregivers and seniors assigned to them. The caregiver’s response was associated by him to the closed envelope with the response of his senior or seniors when more than one responded. Anonymity was guaranteed for both caregivers and seniors. Most caregivers interviewed are female (88.6%), aged between 18 and 34 years (44.6%), technicians/caregivers (62%), and work from 01 to 03 years (61%). Most of the senior sample is female (71.8%), aged between 70 and 90 years (69.9%), and length of residence at the LTC from 1 to 3 years (72.8%). LTC residents are mostly women because men’s longevity is clearly lower (see Table 2).
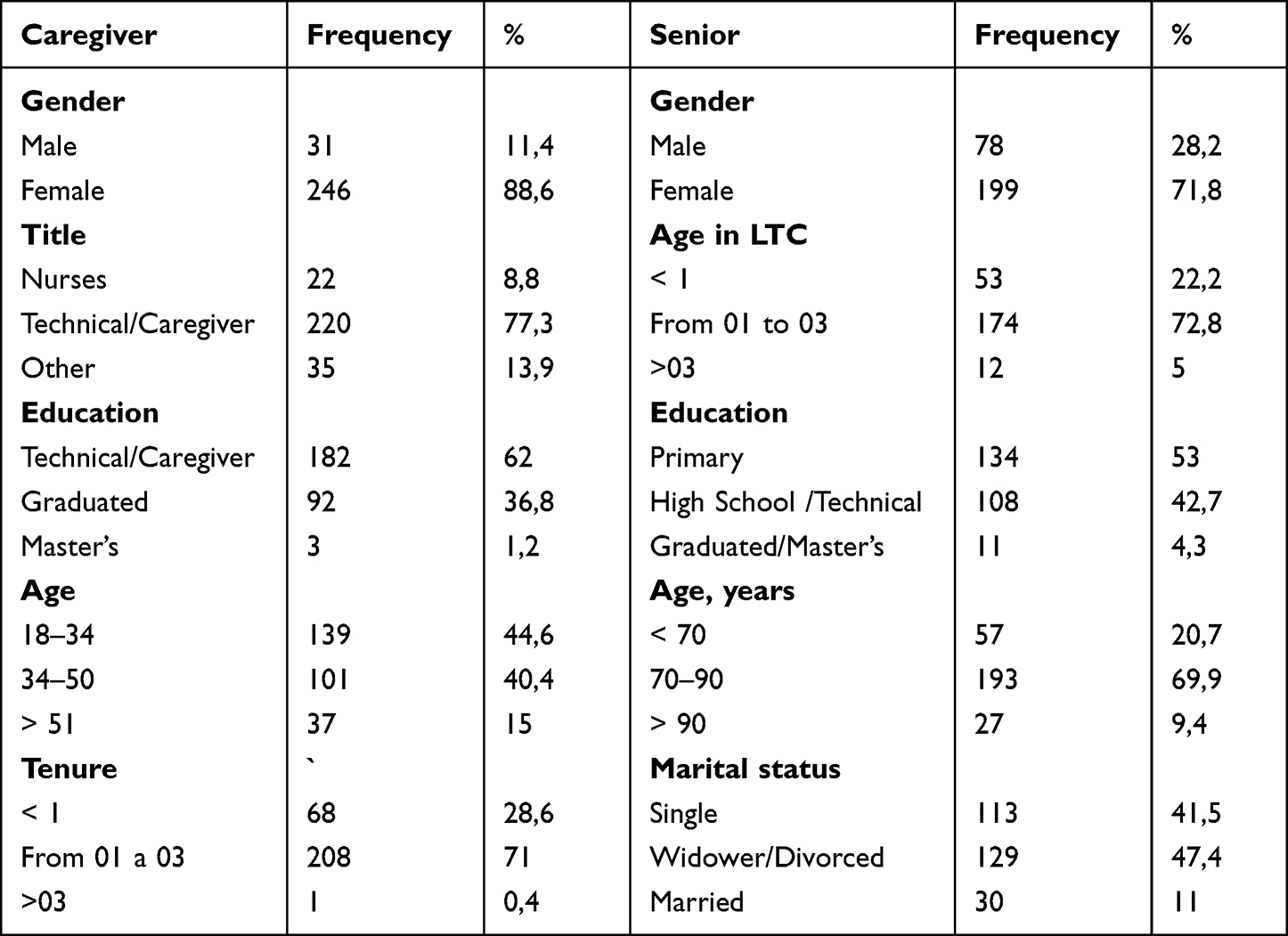 |
Table 2 Sample of Caregivers and Seniors |
Measurement Scales
The variables used were measured based on previously tested scales, translated into Portuguese by means of back-translation, and measured on a 7-point Likert scale, ranging from 1=strongly disagree to 7=strongly agree. A pre-test was carried out to ensure the readability and understanding of the instrument. Metrics can be found in Table 3, identifying the metric source and standardized regression weights. Ethical leadership was measured based on the revised scale from Khan and Javed (2018), based on the ethical leadership scale from Brown et al (2005). This revision allowed a more comprehensive approach of the 2 proposed dimensions of ethical leadership: moral manager; and moral person.37,65,66 Descriptive statistics, correlations, and EFA were performed using IBM SPSS (version 28). CFA and SEM data were performed using IBM SPSS AMOS (version 28).
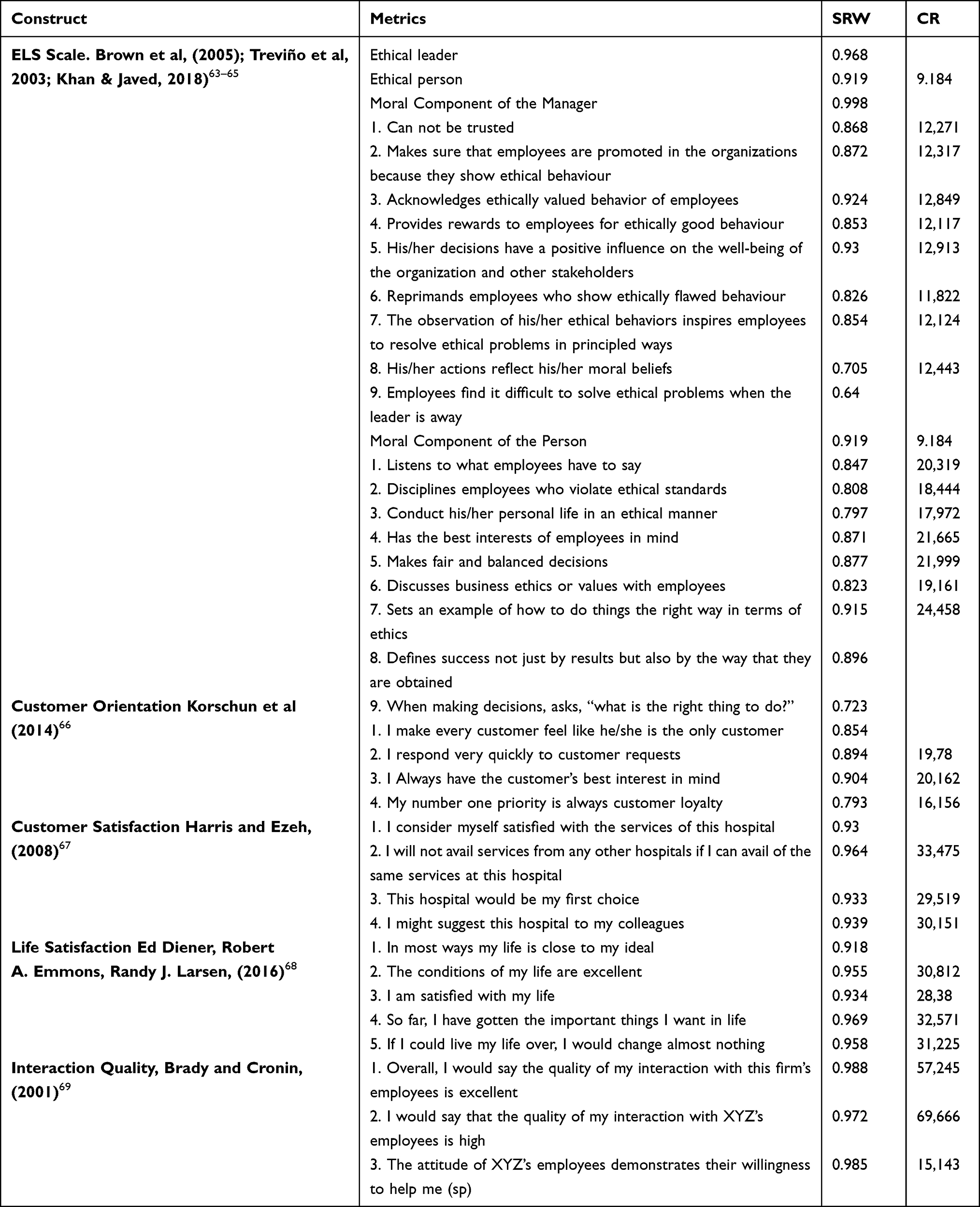 |
Table 3 Metric Source and Standardized Regression Weights |
Measurement Model and Validity
Confirmatory factor analysis was performed to measure the psychometric properties of the scales and the fit of the measurement model using AMOS 28. The model shows a good fit (IFI=0.963 TLI=0.959; CFI=0.963; RMSEA=0.056; X2/df= 1.819). Composite reliability (CR) and extracted mean variance were calculated. All scales presented values above 0.7 in the CR and above 0.5 in the AVE, according to the recommendations.70 Discriminant validity is supported because all correlations between the constructs are less than one, and the square correlations calculated for each pair of constructs are always smaller than the variance extracted for the corresponding constructs,71 thus confirming the discriminant validity (see Table 4).
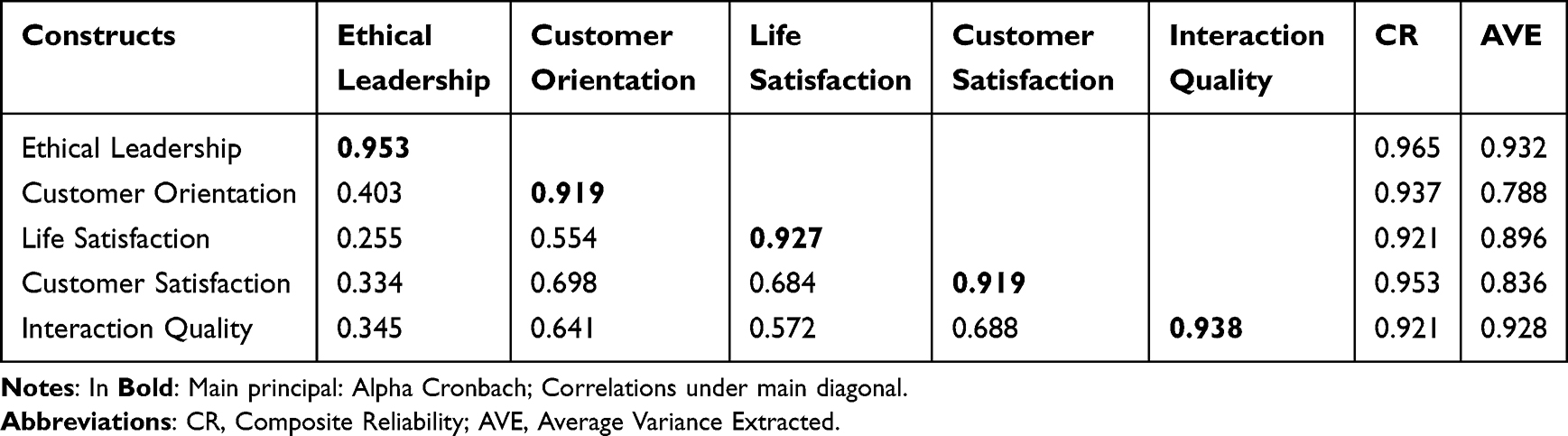 |
Table 4 Confirmatory of Discriminant Validity |
Findings and Discussion
Finally, we calculated the structural model using IBM SPSS AMOS (version 28) to test the proposed hypotheses. We found a good fit in the structural model (IFI=0.962 TLI=0.959; CFI=0.962; RMSEA=0.057; X2/df=1.8147). The regression results are shown in Table 5. All hypotheses are statistically significant. We also tested the first-order effects of each of the two dimensions, ethical person and ethical manager, on customer orientation, which can be seen, in Table 5.
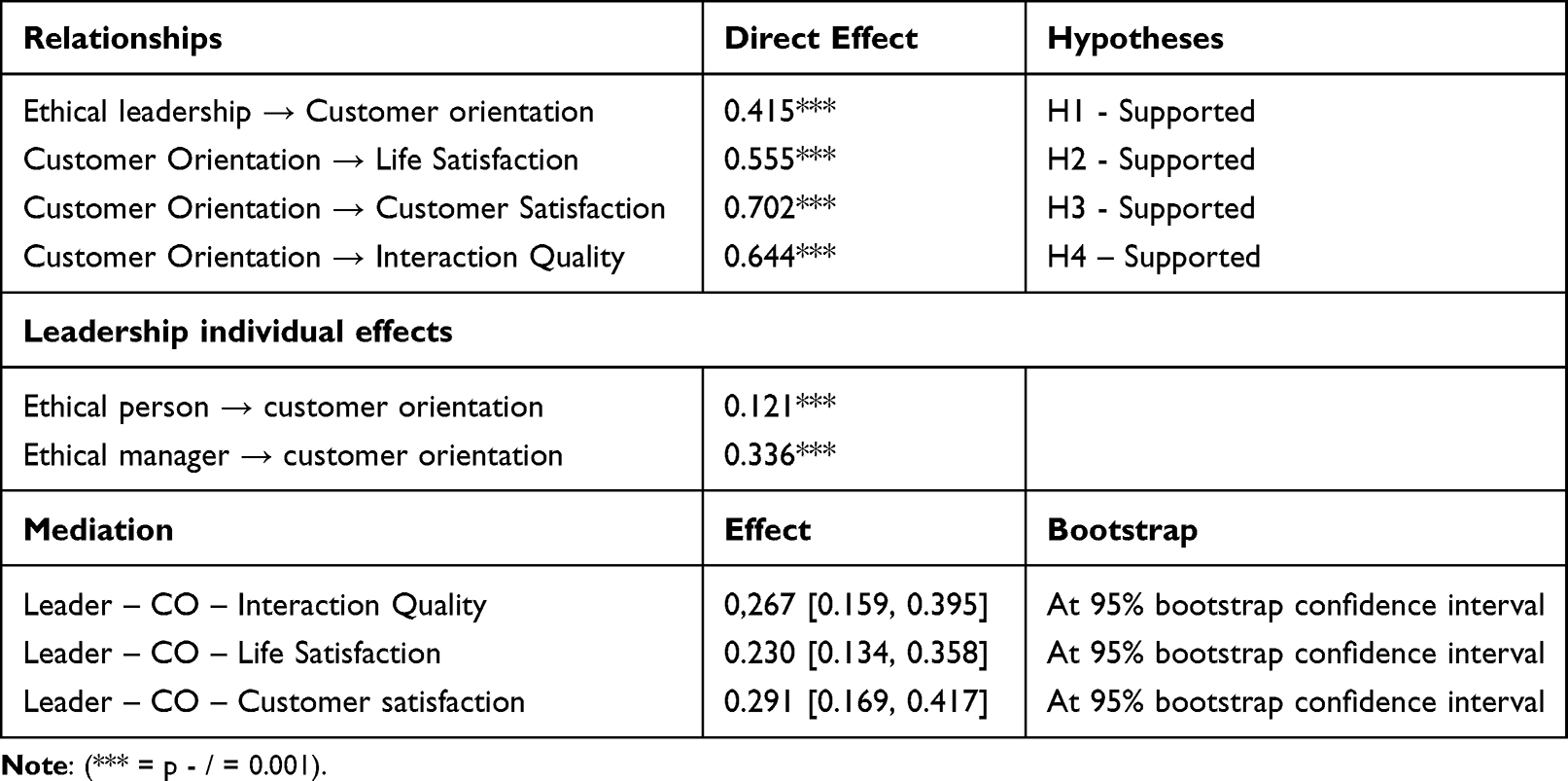 |
Table 5 Confirmatory of Discriminant Validity of Ethical Person and Ethical Manager on Customer Orientation |
Discussion
This research focuses on identifying of the ethical leadership style perceived in health care, namely in LTC, its impacts on caregivers’ CO, and the effects it may have on senior residents, namely on their satisfaction with care, with caregivers, and with their life. The results revealed a positive interaction between EL and CO, a positive interaction of the caregiver with the seniors’, and their satisfaction with care and life. According to H1, there is a positive relationship between EL and CO in an LTC environment (r=0.415, p=***). A study by Enghiad, Venturato, and Ewashen (2021) showed that nursing leadership affects staff satisfaction and senior outcomes. Interacting with the team is the key to good leadership.9 Gountas & Gountas (2016) point out that leaders can promote CO, improve employee satisfaction and encourage service quality.11 According to Shaller (2007), the most critical factors for improving health care are leadership commitment and engagement.11 McDermott, Kidney, and Flood (2013) caregivers recognize the effectiveness of leadership when the leader is able to inspire and prioritize needs, producing a sense of calm and security in caregivers.34 Ethical leaders who develop moral sensitivity create an ethical attitude and response in caregivers to provide ethical care and services to the senior.21 The combination of an ethical person with an ethical manager produces an example, guidance, stimulation, and a climate that promotes the engagement and willingness of caregivers to orient themselves towards the client and overcome their tasks, providing care, attention, and affection to the people who are vulnerable and lacking autonomy.35 Our results support the proposed idea that EL in an LTC can help build relationships and a sense of community, especially when these aspects fill in the lack of facilities, working conditions, and quality of life.14 Overall, ethical leadership plays a crucial role in shaping the customer orientation of caregivers in senior residences.7,18 It fosters a culture of respect, empathy, and resident-centred care, ultimately leading to improved resident satisfaction, caregiver morale, and the overall reputation of the senior residence.16,31,32,62
H2 is also positively supported, as the CO positively influences life satisfaction (r=0.555; p=***). According to Cho, Martin & Poon (2015), LS is a critical indicator of the quality of care for the senior in LTC.60 The literature shows that the behavior of service workers affects the quality of service provided to the customer.62 The senior perceive the quality of service through the caregiver’s behavior,62 based on the quality of care, personal relationships, achieved autonomy, and even affection.72 According to Ciccone et al, the quality of health, self-management, and life satisfaction stems from a “partnership” between caregivers and the senior.72 Living with other people and recognizing local references allows the construction of family spaces for the senior.73 By demonstrating a positive relationship between CO and LS, it is possible to affirm that caregivers committed to their seniors’ and the quality of their work positively contribute to the satisfaction with care and with the life of the senior. The CO caregiver guarantees the possibility of coexistence for the senior, integrating them into everyday life in a dignified and humane way.5 Therefore, caregivers’ customer orientation can significantly influence seniors’ life satisfaction in senior residences. When caregivers prioritize individualized care, emotional support, respect, and a sense of security, seniors are more likely to lead fulfilling and satisfying lives in their residential settings.5,74 This, in turn, can have a positive impact on their overall well-being and quality of life.19,75
H3 supports a positive relationship between CO and customer satisfaction (r=0.702; p=***). According to Oliver (2010), SC has to do with the general level of pleasure that the senior person has for the service.47 LTCs whose caregivers are COs tend to better understand the needs and desires of the senior, causing caregivers to provide higher quality and closer service, which is perceived by the senior.62 The search for a higher CO also tends to produce greater caregiver satisfaction, reducing turnover,9 and stabilizing the relationships between caregivers and the senior, taking advantage of the bonds with the senior that tend to be reinforced.5 CO and CS often go hand in hand.15 However, this relationship is expected to be stronger in LTC services due to the importance of combining the quality of the service with the humanization of the environment and the bond.5 The results of our study strongly support the positive relationship between CO and CS in LTC, where CO caregivers can anticipate the needs and expectations of the senior and put all their efforts into satisfying them.52 Customer-oriented caregivers take the time to understand each senior’s unique needs, preferences, and routines.21 They provide individualized care plans that cater to these specific requirements, leading to greater satisfaction among seniors who receive personalized attention.75
CO is positively related to the IQ between caregivers and the senior, supporting H4 (r=0.644; p=***). The study by Gronroos (1982, 1984) shows that customers’ perception of the service quality and their satisfaction is highly related to the IQ of the staff, especially the caregivers.55 The service delivery is highly centered on the relationships and bonding they develop with the staff, during the encounters with the caregiver, but also in their daily life and the informal meetings and contacts they maintain with the LTC team.76 According to Bitner, Booms & Tetreault (1990), evaluating IQs has three main aspects: behavior, actions, and caregivers’ abilities to provide care/attention and solve possible failures.56 According to Gaur et al, the quality of the interaction has critical elements such as politeness, sympathy, sensitivity, warmth, and empathy.77 Therefore, these basic IQ features are clearly stimulated in an environment where CO prevails.11 See Table 5. Therefore, caregivers’ customer orientation plays a crucial role in shaping the quality of the relationship between seniors and caregivers in senior residences.30,55 A customer-oriented approach fosters trust, respect, open communication, and a sense of empowerment within the relationship, ultimately leading to a more positive and satisfying caregiving experience for seniors.72
Mediation
Satisfied customer-oriented caregivers are more likely to provide good care.12,55 It is essential to mention that the positive results found in this study show the importance of EL in LTC. Good leaders tend to have good followers and satisfied and happy old-aged.10 In healthcare services, especially in LTCs, the emotional bonds created between caregivers and the seniors result from the positive relationships between leaders and followers, namely, caregivers.34 Strong relationships between leadership and caregivers improve care, build good relationships and communication, and improve working conditions and high-level care.14 When there is a positive connection with the leader, caregivers feel empowered to offer excellent care to the senior, generating greater satisfaction, better bonding, and IQ, and finally, LS, supporting H5.9 EL in LTCs is directly and indirectly essential, fostering good working and care conditions.14 So, the quality of the interaction perceived by the senior during care provision impacts the perception of the quality of care, supporting the H5b hypothesis.56,76 Ethical leaders, both as persons and managers, exerting their influence based on proximity, ethics, and example,13 that produce CO caregivers will lead indirectly to better customer-related outcomes: better senior interactions,12 an overall feeling of satisfaction with service, and a humanized environment where senior experience a better life quality.6 Seniors tend to feel satisfied with their lives when they perceive that courteous, friendly, kind, respectful, receptive, individualized, and warm treatment helps to overcome the lack of family and reinforces their autonomy.52
Contributions
The growth of the senior population in the world1 has led to the development of institutions and places offering care to this part of the population, the LTCs. These institutions proliferated on a large scale to the point of being called the Care industry, according to Soares (2012), being the quintessence of work in the social services sector.5 In LTCs, some formal caregivers are the closest people who provide care to the senior,6 with a prevalence of women who do not always have adequate training to perform the function.77 The prevalence of women in care78 can lead to health impairments in these caregivers, such as burnout.79 In this scenario, we developed our study showing a positive relationship between EL and senior-related outcomes in LTCs. This investigation presents four main contributions: 1) We establish the chain of effects between EL and customer-related outcomes. We achieved the results of this chain based on the collection of paired information from caregivers and seniors. Bourgeault (2021) says there is a lack of empirical data on leadership discernment in LTC. Our investigation minimizes this lack of investigation, explicitly addressing the ethical leadership style in LTC. 2) When we investigated the role of the CO caregiver in LTC, it was possible to detect the importance of this caregiver when interacting positively with the senior, offering them presence, security, affection, life, and even humanity. By promoting solid affective bonds with the senior, this professional allows intimacy, security, increased autonomy, the meaning of life, well-being, and happiness.75 3) It is possible to say that CO caregivers are mediators of the EL - senior’s satisfaction and well-being linkage since the effects of leadership on customer-related outcomes might be rather indirect.18 Ethical leaders understand well the importance of ethics, values, and example for a positive caregiver/senior interaction to assure successful care.80 4) Investigating the role of EL in healthcare services, especially in LTC, whether directly or indirectly, is even more critical since seniors´ satisfaction and happiness, as well as families’ security, confidence, and tranquillity, are involved.
Therefore, our results, combining information from caregivers and seniors, showed exactly this virtuous chain of effects between EL and the quality of the services provided, expressed in the customer-related outcomes tested: CS with service and life and good relationship quality with the staff. Providing better-working attitudes and conditions and EL, directly or indirectly, contributes to the improvement of care conditions and care results.14 Ethical leaders care about their followers, promoting an environment that provides well-being and a sense of accomplishment when caregivers transcend their obligations and tasks. CO lets the caregiver get to know the older person, identifying their capacity for action, assessing their conditions, and helping them in the needed activities.81 This attitude allows the seniors to feel alive and decide about their autonomy, providing satisfaction with their life.
Managerial Contributions
EL is particularly relevant in LTCs, providing the development of a supportive environment for both caregivers and seniors. Ethical leaders care about their followers, understanding that the work performed is part of their emotional experiences and how they relate to the world, influencing the caregiver’s life and health, balancing the caregiver’s mind and body, and stimulating their CO.81 Bourgeault (2021) mentions the inconsistency of information to discern leadership in LTC, whether it acts only as supervision or if it plays a management role. Our investigation of the EL style showed that the development of a CO might, directly or indirectly, influence the services provided.80 Ethical leaders understand that caregivers’ daily cooperation to care for the seniors will improve relationships with them and their families and increase the organization’s performance.81 Although care difficulties often result from a lack of technical resources, knowledge, and social support, ethical leaders can overcome these difficulties by training their teams and putting the seniors at the center of the equation.75 The positive results of our investigation of the seniors show the importance of the affective bonds between caregivers and the senior. Therefore, the option for ethical leaders or the deepening of the ethical characteristics of the leaders has proved to be the right way to have customer-oriented caregivers. Additionally, through customer orientation, the services provided may improve and excel, bringing additional senior satisfaction, better bonding with caregivers, and improved well-being. As CO, job satisfaction, and team retention are linked,9 ethical leaders tend to promote respect as they set an example for their followers for competence, effective decision-making, compassion, and trust.9
Non-profit organizations are increasingly important for the economic and social development of countries, as they create proximity to citizens, being, in the vast majority, service providers in the care of the elderly.82,83 These organizations intervene in situations where the government service is unable to adequately cover them, while at the same time acting in advocacy and working in partnership to improve services.84 They have the competence to involve the community, volunteers and family members for social support of their activity.82 Allied to this, non-profit organizations, by prioritizing ethical leadership in their staff, tend to obtain many gains because ethical leadership establishes trust, promotes a culture of integrity in the organization and makes its decisions guided by, which generates in the caregiver customer-oriented attitude.12,22,36 Ethical leaders are accountable and transparent.22 In elderly care, non-profit organizations tend to develop patient-centered,22 they value the quality of their care by developing active care for the elderly9 combined with care with empathy, dignity and respect, which promotes the emotional and physical well-being of the elderly.11
In the health area, positions are replaceable, but people are not. So, retaining positive professionals makes all the difference in the quality of care, senior satisfaction, and business success, giving EL a central role in LTC success.
Limitations and Future Research
Our investigation shows causal relationships between variables in LTC in Brazil. Specifically, the role of EL on the caregiver´s CO and, therefore, on the senior´s satisfaction and well-being. However, we use cross-sectional data, which might not be ideal for establishing a clear causality. Longitudinal data suits these goals better. At the same time, data collection had to privilege old-aged who were in physical and intellectual conditions to answer our questionnaire. Because cultural aspects are determinant in this kind of care, even religious issues, this investigation should be replicated in other countries, considering the effects of culture and religion. The positive influence of EL on customer-related outcomes in LTCs seems to be rather indirect through the caregivers’ behavior. Therefore, it would be interesting to deepen the investigation using other variables such as emotional intelligence, caregivers’ spiritual well-being, commitment, and turnover. These variables may reveal more information to improve leadership effectiveness, senior satisfaction, and well-being in LTCs.
Information Statement
The study was approved by the Ethics Committee of the International Ibero-American University. Participants’ consent was obtained in writing, as well as consent from the organization to conduct the research. The guidelines outlined in the Helsinki Declaration were followed.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bone AE, B. G, Etkind SE, et al. What is the impact of population ageing on the future provision of end-of-life care? Population-based projections of place of death. Palliat Med. 2018;32(2):329–336. doi:10.1177/0269216317734435
2. United Nations. Ageing, older persons and the agenda for sustainable development. World Population Ageing 2019, United Nations: Department of Economic And Social Affairs: Population Division; 2021.
3. BRASIL, Ministério da Mulher, da Família e dos Direitos Humanos, 2020.
4. Lacerda TTB, Neves APM, Buarque GLA, et al. Geospatial panorama of long-term care facilities in Brazil: a portrait of territorial inequalities. Geriatr Gerontol Aging. 2021;15. doi:10.53886/gga.e0210060
5. Mizan MD. O Cuidador do Idoso em ILPI: Uma Relação Humana e Delicada. São Paulo: Portal Edições; 2019.
6. Santos CC, Salmazo da Silva H, Gutierrez BA. Os cuidados de longa duração e a percepção de idosos institucionalizados sobre velhice, velhice bem-sucedida e qualildade da atenção. Revi Kairós-Gerontologia. 2017;20(3):151–178. doi:10.23925/2176-901X.2017v20i3p151-178
7. Specchia ML, Cozzolino MR, Di Pilla A, Galletti C, Ricciardi W, Damiani G. Leadership styles and nurses’ job satisfaction. results of a systematic review. Int J Environ Res Public Health. 2021;18(4):1552. doi:10.3390/ijerph18041552
8. Enghiad P, Venturato L, Ewashen C. Exploring clinical leadership in long‐term care: an integrative literature review. J Nurs Manag. 2021;30(1):90–103. doi:10.1111/jonm.13470
9. Robbins B, Davidhizar R. Transformational leadership in health care today. Health Care Manag. 2020;39(3):117–121. doi:10.1097/HCM.0000000000000296
10. Harolds JA. Quality and safety in healthcare, part LV leadership to prevent burnout and increase joy. Clin Nucl Med. 2020;45(2):123–124. doi:10.1097/RLU.0000000000002714
11. Bruno A, Dell’Aversana G, Zunino A. Customer orientation and leadership in the health service sector: the role of workplace social support. Front Psychol. 2017;8:1920. doi:10.3389/fpsyg.2017.01920
12. Kia N, Halvorsen B, Bartram T. Ethical leadership and employee in-role performance: the mediating roles of organisational identification, customer orientation, service climate, and ethical climate. Person Rev. 2019;48(7):1716–1733. doi:10.1108/PR-12-2018-0514
13. Sahne BS, Sar S. Leadership and healthcare services. A Alv Contem Leader Chall. 2017;233–250. doi:10.5772/65288
14. Bourgeaultl IL, Daly T, Aubrecht C, Armstrong P, Armstrong H, Braedley S. Leadership for quality in long-term care. Healthc Manage Forum. 2022;35(1):5–10. doi:10.1177/08404704211040747
15. Fatima T, Malik SA, Shabbir A. Hospital healthcare service quality, patient satisfaction and loyalty: an investigation in context of private healthcare systems. Int J Qual Reliabil Manage. 2018;35(6):1195–1214. doi:10.1108/IJQRM-02-2017-0031
16. Aloustani S, Atashzadeh-Shoorideh F, Zagheri-Tafreshi M, Nasiri M, Barkhordari-Sharifabad M, Skerrett V. Association between ethical leadership, ethical climate and organizational citizenship behavior from nurses’ perspective: a descriptive correlational study. BMC Nurs. 2020;19(1):1–8. doi:10.1186/s12912-020-0408-1
17. Özden D, Arslan GG, Ertugrul B, Karakaya S. The effect of nurses’ ethical leadership and ethical climate perceptions on job satisfaction. Nurs Ethics. 2019;26(4):1211–1225. doi:10.1177/0969733017736924
18. Keisu BI, Öhman A, Enberg B. Employee effort – reward balance and first‐level manager transformational leadership within elderly care. Scand J Caring Sci. 2018;32(1):407–416. doi:10.1111/scs.12475
19. Seljemo C, Viksveen P, Ree E. The role of transformational leadership, job demands and job resources for patient safety culture in Norwegian nursing homes: a cross-sectional study. BMC Health Serv Res. 2020;20(1):1–8. doi:10.1186/s12913-020-05671-y
20. Byun G, Karau SJ, Dai Y, Lee S. A three-level examination of the cascading effects of ethical leadership on employee outcomes: a moderate mediation analysis. J Bus Res. 2018;88:44–53. doi:10.1016/j.jbusres.2018.03.004
21. Zhang N, Li M, Gong Z, Xu D. Effects of ethical leadership on nurses’ service behaviors. Nurs Ethics. 2019;26(6):1861–1872. doi:10.1177/0969733018787220
22. Devik SA, Munkeby H, Finnanger M, Moe A. Nurse Managers’ perspectives on working with everyday ethics in long-term-care. Nurs Ethics. 2020;27(8):1669–1680. doi:10.1177/0969733020935958
23. Cullen JG. Moral recovery and ethical leadership. J Bus Ethics. 2022;3(3):485–497. doi:10.1007/s10551-020-04658-3
24. Halvorsen B, Bartram T, Kia N, Cavanagh J. Meeting customer needs through ethical leadership and training: examining Australian bank employees. Asia Pac J Hum Resour. 2023;61(1):79–100. doi:10.1111/1744-7941.12329
25. Hoang G, Yang M, Luu TT. Ethical leadership in tourism and hospitality management: a systematic literature review and research agenda. Int J Hosp Manag. 2023;114:103563. doi:10.1016/j.ijhm.2023.103563
26. Tortorella GL, Fogliatto FS, Saurin TA, Tonetto LM, McFarlane D. Contributions of Healthcare 4.0 digital applications to the resilience of healthcare organizations during the COVID-19 outbreak. Technovation. 2022;111:102379. doi:10.1016/j.technovation.2021.102379
27. Cho D, Lee KW. Population aging and fiscal sustainability: nonlinear evidence from Europe. J Int Money Finance. 2022;126:102665. doi:10.1016/j.jimonfin.2022.102665
28. Ko C, Ma J, Bartnik R, Haney MH, Kang M. Ethical leadership: an integrative review and future research Agenda. Ethics Behav. 2018;28(2):104–132. doi:10.1080/10508422.2017.1318069
29. White DE, Grason S. The importance of emotional intelligence in nursing care. J Comp Nurs Res Care. 2019;4(2):152. doi:10.33790/jcnrc1100152
30. Sfantou DF, Lalio-tis A, Patelarou AE, Sifaki-Pistolla D, Matalliotakis M, Patelarou E. Importance of leadership style towards quality of care measures in healthcare settings: a systematic review. Healthcare. 2017;5(4):73. doi:10.3390/healthcare5040073
31. Zaghini F, Fiorini J, Piredda M, Fida R, Sili A. The relationship between nurse managers’ leadership style and patients’ perception of the quality of the care provided by nurses: cross sectional survey. Int J Nurs Stud. 2020;101:103446. doi:10.1016/j.ijnurstu.2019.103446
32. Sarwar H, Ishaqb MI, Aminb A, Ahmed R. Ethical leadership, work engagement, employees’ well-being, and performance: a cross-cultural comparison. J Sustaina Tour. 2020;28(12):2008–2026. doi:10.1080/09669582.2020.1788039
33. Ruiz-Palomino P, Morales-Sánchez R, Martínez-Cañas R. Corporate sustainability, ethics and employee satisfaction. Sustainability. 2021;13:11964. doi:10.3390/su132111964
34. Gandolfi F, Stone S.Leadership, leadership styles, and servant leadership. J Manag Res. 2018;18(4):261–269.
35. Treviño LK, Hartman LP, Brown M. Moral person and moral manager: how executives develop a reputation for ethical leadership. Calif Manage Rev. 2000;42(4):128–142. doi:10.2307/41166057
36. Franczukowska AA, Krczal E, Knapp C, Baumgartner M. Examining ethical leadership in health care organizations and its impacts on employee work attitudes: an empirical analysis from Austria. Leader Health Serv. 2021;34(3):229–247. doi:10.1108/LHS-06-2020-0034
37. Khan SR, Javed U.Revision of ethical leadership scale. J Res Refle Educ. 2018;12(2):121–135.
38. Linuesa-Langreo J, Ruiz-Palomino P, Elche D. Servant leadership, empowerment climate, and group creativity: a case study in the hospitality industry. Ramon Llull J Appl Ethics. 2016;7:9–36.
39. Neubert MJ, Carlson DS, Kacmar KM, Roberts JA, Chonko LB. The virtuous influence of ethical leadership behavior: evidence from the field. J Bus Ethics. 2009;90(2):157–170. doi:10.1007/s10551-009-0037-9
40. Nassif AG, Hackett RD, Wang G. Ethical, virtuous, and charismatic leadership: an examination of differential relationships with follower and leader outcomes. J Bus Ethics. 2021;172(3):581–603. doi:10.1007/s10551-020-04491-8
41. Ruiz-Palomino P, Linuesa-Langreo J, Elche D. Team-level servant leadership and team performance: the mediating roles of organizational citizenship behaviour and internal social capital. Busin Ethics Env Resp. 2023;32(S2):127–144.
42. Berridge C, Lima J, Schwartz M, Bishop C, Miller SC. Leadership, staff empowerment, and the retention of nursing assistants: findings from a survey of U.S. Nursing homes. J Am Med Dir Assoc. 2020;21(9):1254–1259.e2. doi:10.1016/j.jamda.2020.01.109
43. Liu LH, Kao CC, Ying JC. Functional capacity and life satisfaction in older adult residents living in long-term care facilities: the mediator of autonomy. J Res Nurs. 2020;28(4):e102. doi:10.1097/JNR.0000000000000362
44. Saxe R, Weitz BA. The SOCO scale: a measure of the customer orientation of salespeople. J Mar Res. 1982;19(3):343–351. doi:10.1177/002224378201900307
45. Tseng LM. How customer orientation leads to customer satisfaction: mediating mechanism of service workers’ etiquette and creativity. Int J Bank Mark. 2019;37(1):210–225. doi:10.1108/IJBM-10-2017-0222
46. Freudenreich B, Lüdeke-Freund F, Schaltegger S. A stakeholder theory perspective on business models: value creation for sustainability. J Busin Ethics. 2020;166(1):3–18. doi:10.1007/s10551-019-04112-z
47. Otto AS, Szymanski DM, Varadarajan R. Customer satisfaction and firm performance: insights from over a quarter century of empirical research. J Aca Mar sci. 2020;48(3):543–564. doi:10.1007/s11747-019-00657-7
48. Zaid AA, Arqawi SM, Mwais RM, Shobaki MJ, Abu-Naser SS. The impact of total quality management and perceived service quality on patient satisfaction and behavior intention in Palestinian healthcare organizations. Technol Report Kansai Un. 2020;62(03):13.
49. Connelly BL, Certo ST, Ireland RD, Reutzel CR. Signaling theory: a review and assessment. J Manage. 2011;37(1):39–67. doi:10.1177/0149206310388419
50. Jiménez-Estévez P, Yáñez-Araque B, Ruiz-Palomino P, Gutiérrez-Broncano S. Personal growth or servant leader: what do hotel employees need most to be affectively well amidst the turbulent COVID-19 times? Technol Forecast Soc Change. 2022;190. doi:10.1016/j.techfore.2023.122410
51. Zhang L, Li D, Cao C, Huang S. The influence of greenwashing perception on green purchasing intentions: the mediating role of green word-of-mouth and moderating role of green concern. J Clean Prod. 2018;187:740–750. doi:10.1016/j.jclepro.2018.03.201
52. Ng JH, Luk BH. Patient satisfaction: concept analysis in the healthcare context. Patient Educ Couns. 2019;102(4):790–796. doi:10.1016/j.pec.2018.11.013
53. Sun X, Foscht T, Eisingerich AB. Does educating customers create positive word of mouth? J Retail Consu Serv. 2021;62:102638. doi:10.1016/j.jretconser.2021.102638
54. Margolis S, Schwitzgebel E, Ozer DJ, Lyubomirsky S. A new measure of life satisfaction: the riverside life satisfaction scale. J Pers Assess. 2019;101(6):621–630. doi:10.1080/00223891.2018.1464457
55. Eneizan B, Taamneh M, Enaizan O, Almaaitah MF, Ngah AH, Alsakarneh A. Human resources practices and job satisfaction on customer satisfaction: the mediating role of quality of customer interaction in online call center. Int J Data Netw Sci. 2021;11–18. doi:10.5267/j.ijdns.2020.12.001
56. Brady MK, Cronin JJ. Customer orientation: Effects on customer service perceptions and outcome behaviors. J Serv Res. 2001;3(3):241–251. doi:10.1177/109467050133005
57. Joon Choi B, Sik Kim H. The impact of outcome quality, interaction quality, and peer‐to‐peer quality on customer satisfaction with a hospital service. Manag Serv Qual. 2013;23(3):188–204. doi:10.1108/09604521311312228
58. Feng T, Wang D, Lawton A, Luo BN. Customer orientation and firm performance: the joint moderating effects of ethical leadership and competitive intensity. J Bus Res. 2019;100:111–121. doi:10.1016/j.jbusres.2019.03.021
59. Pavot W, Diener E. The satisfaction with life scale and the emerging construct of life satisfaction. J Posit Psychol. 2008;3(2):137–152. doi:10.1080/17439760701756946
60. Willroth EC, John OP, Biesanz JC, Mauss IB. Understanding short-term variability in life satisfaction: the Individual Differences in Evaluating Life Satisfaction (IDELS) model. J Pers Soc Psychol. 2020;119(1):229–248. doi:10.1037/pspp0000261
61. Nakamura JS, Delaney SW, Diener E, VanderWeele TJ, Kim ES. Are all domains of life satisfaction equal? Differential associations with health and well-being in older adults. Qual Life Res. 2022;31(4):1043–1056. doi:10.1007/s11136-021-02977-0
62. Li WP, Pomegbe WWK, Dogbe CSK, Novixoxo JD. Employees’ customer orientation and customer satisfaction in the public utility sector: the mediating role of service quality. Afr J Econ Manag Stud. 2019;10(4):408–423. doi:10.1108/AJEMS-10-2018-0314
63. Cohen J. Statistical Power Analysis for the Behavioral Sciences.
64. Hair JF, Gabriel ML, Patel VK. Modelagem de Equações Estruturais Baseada em Covariância (CB-SEM) com o AMOS: orientações sobre a sua aplicação como uma Ferramenta de Pesquisa de Marketing. Rev Brasileira de Market. 2014;13(2):44–55. doi:10.5585/remark.v13i2.2718
65. Treviño LK, Brown M, Hartman LP. A qualitative investigation of perceived executive ethical leadership: perceptions from inside and outside the executive suite. Hum Relat. 2003;56(1):5–37. doi:10.1177/0018726703056001448
66. Brown ME, Treviño LK, Harrison DA. Ethical leadership: a social learning perspective for construct development and testing. Organ Behav Hum Decis Process. 2005;97(2):117–134. doi:10.1016/j.obhdp.2005.03.002
67. Korschun D, Swain SD, Swain SD. Corporate social responsibility, customer orientation, and the job performance of frontline employees. J Mark. 2014;78(3):20–37. doi:10.1509/jm.11.0245
68. Harris LC, Ezeh C. Servicescape and loyalty intentions: as empirical investigation. Eur J Mark. 2008;42(3/4):390–422. doi:10.1108/03090560810852995
69. Diener ED, Emmons RA, Larsen RJ, Griffin S. The satisfaction with life scale. J Pers Assess. 1985;49(1):71–75. doi:10.1207/s15327752jpa4901_13
70. Hair JF, Black WC, Babin BJ, Anderson RE. Multivariate Data Analysis.
71. Shiu E, Pervan SJ, Bove LL, Beatty SE. Reflections on discriminant validity: reexamining the Bove et al. (2009) findings. J Bus Res. 2011;64(5):497–500. doi:10.1016/j.busres.2010.04.004
72. Park SS, Sok SR. Relation modeling of factors influencing life satisfaction and adaptation of Korean older adults in long-term care facilities. Int J Environ Res Public Health. 2020;17(1):317. doi:10.3390/ijerph17010317
73. de Oliveira LF. O pertencimento e o lugar: um estudo acerca das representações sociais de cuidadores de idosos de uma Instituição de Longa Permanência de um município no interior de Minas Gerais. Geografia em Questão. 2019;12(1):75–102. doi:10.48075/geoq.v12i1.19937
74. Gerridzen IJ, Hertogh CMPM, Joling KJ, et al. Caregivers perspectives on good care for nursing home residents with Korsakoff syndrome. Nurs Ethics. 2021;28(3):358–371. doi:10.1177/0969733020921507
75. Justo AM, Peterle TS. Quem cuida dos idosos: narrativas de cuidadores formais em ILPI. Estudos Interdisciplinares sobre o Envelhecimento. 2020;25(3). doi:10.22456/2316-2171.102868
76. Choi BJ. The impact of outcome quality, interaction quality, and peer‐to‐peer quality on customer satisfaction with a hospital service. Manag Serv Qual. 2013. doi:10.1108/09604521311312228
77. Ghandour A, Padovani RD, Batistoni SS. Habilidades de resolução de problemas e indicadores de bem-estar emocional em profissionais de enfermagem que atuam em Instituições de Longa Permanência para Idosos. Revista Kairós Gerontologia. 2014;17(2):239–255. doi:10.23925/2176-901X.2014v17i2p239-255
78. Martins G, Corrêa L, Caparrol AJ, Santos PT, Brugnera LM, Gratão AC. Sociodemographic and health characteristics of formal and informal caregivers of elderly people with alzheimer’s disease. Esc Anna Nery. 2019;2(2):e20180327. doi:10.1590/2177-9465-ean-2018-0327
79. Tanaka K, Iso N, Sagari A, et al. Burnout of long-term care facility employees: relationship with employees’ expressed emotion toward patients. Int J Gerontol. 2015;9(3):161–165. doi:10.1016/j.ijge.2015.04.001
80. Passos YN, Khoury HT. Atitude de cuidadoras formais de idosas institucionalizadas sobre a velhice: efeito de uma investigação educativa. Revi Kairós-Gerontologia. 2019;22(3):277–299. doi:10.23925/2176-901X.2019v22i3p277-2982
81. de Abreu Pestana DM. Notas psicanalíticas sobre o cuidar além do curar: observações para cuidadores formais. Revista Sol Nascente. 2022;79–110. doi:10.13140/RG.2.2.23787.62245
82. Alves A, Carvalho A, Ferreira MR. How social performance indicators and leadership contribute to the development of non-profits – an approach to long-term care homes. Int J Environ Workplace Employ. 2021;6(3):205–219. doi:10.1504/IJEWE.2021.119687
83. Blomkvist R, Winblad U. Why no nonprofits? State, market, and the strive for universalism in Swedish elder care. Nonprofit Volunt Sect Q. 2019;1–19. doi:10.1177/0899764018819870
84. Raeymaechers P, Puyvelde SV. Nonprofit advocacy coalitions in times of COVID-19: brokerage, crowdfunding, and advocacy roles. Nonprofit Volunt Sect Q. 2021;50(6):1304–1317. doi:10.1177/0899764021991675
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.