")
Back to Journals » International Journal of Women's Health » Volume 16
Estradiol Decline Before hCG Administration in COH Has a Negative Effect on IVF Outcomes in Patients Without OC Pretreatment
Authors Zhu Y, Zheng Z, Fan B, Sun Y, Zhai J, Du Y
Received 8 June 2023
Accepted for publication 30 January 2024
Published 6 March 2024 Volume 2024:16 Pages 411—419
DOI https://doi.org/10.2147/IJWH.S423089
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Yinci Zhu,1,2 Zhong Zheng,1,2 Bihong Fan,1,2 Yun Sun,1,2 Junyu Zhai,1,2 Yanzhi Du1,2
1Department of Reproductive Medicine, Ren Ji Hospital, Shanghai Jiao Tong University, School of Medicine, Shanghai, 200135, People’s Republic of China; 2Shanghai Key Laboratory for Assisted Reproduction and Reproductive Genetics, Shanghai, 200135, People’s Republic of China
Correspondence: Junyu Zhai; Yanzhi Du, Department of Reproductive Medicine, Ren Ji Hospital, Shanghai Jiao Tong University, School of Medicine, Shanghai, 200135, People’s Republic of China, Tel +86-21-20284525; +86-21-20284518, Email [email protected]; [email protected]
Purpose: Together with ultrasound measurement of follicle size, serum estradiol (E2) provides guidance for controlled ovarian hyperstimulation (COH). However, during the COH process, some patients experience decreased serum E2 level, especially before human chorionic gonadotropin (hCG) trigger. In order to elucidate the effect of E2 reduction as well as the role of oral contraceptive pretreatment, a retrospective study was performed in our center from 2013 to 2019.
Patients and Methods: In total, 333 patients who experienced an E2 decrease prior to hCG administration were recruited as E2 decline group, while 333 patients with continuously E2 increase during COH were considered as control group. Based on pretreatment strategy, the two groups were further categorized into oral contraceptive (OC) and non-OC sub-groups, and IVF and clinical outcomes were compared between paired groups.
Results: Number of dominant follicles on hCG day and normally fertilized zygotes were significantly decreased in E2 decline group, and the significantly reduced live birth rate in E2 decline group indicated the close relationship between E2 decline and clinical outcomes. To analyse further, we found that in patients without OC pretreatment, the pregnancy rate and live birth rate of E2 decline group (n = 141) were significantly lower than control group (n = 136) (56.3% versus 68.0%, 50.8% versus 63.5%, respectively). However, for patients with OC pretreatment, no difference was detected between two groups, suggesting a potential effect of OC pretreatment on clinical outcomes.
Conclusion: E2 decline prior to hCG-triggering day adversely affects IVF and clinical outcomes in patients without OC pretreatment, especially fertilization rate and live birth rate.
Keywords: estradiol decline, controlled ovarian hyperstimulation, oral contraceptive, in vitro fertilization, fertilization rate, live birth rate
Introduction
Serum estradiol (E2) measurement is recognized as an indispensable parameter for follicle monitoring during controlled ovarian hyperstimulation (COH) in in vitro fertilization (IVF) cycles.1,2 The E2 value of different stages can be indicative for assessment and prognosis of treatment protocols when combined with other index.3,4 Moreover, high level of serum E2 associated with multiple follicle development in high responders may predict high risk for ovarian hyperstimulation syndrome (OHSS).5,6
Prior to the prevalence of GnRH agonist protocols, decreased serum E2 level before the day of human chorionic gonadotropin (hCG) administration was related to suboptimal IVF indexes even clinical outcomes.7 Subsequently, several studies focused on the effects of serum E2 decline in GnRH agonist protocols. A.K. Styer et al reported that decreased E2 level before the day of hCG administration had no impact on pregnancy loss rate or live birth rate of the patients with GnRH-agonist protocol.8 On the other side, S. Fisher et al concluded that in either standard long or flare protocol, spontaneously falling E2 was linked to lower fertilization rate and clinical pregnancy rate compared to controls, whereas no such differences existed in patients with decreased E2 due to deliberate protocol modification.9 Thus, monitoring of E2 level is closely related to drug adjustment during COH. In flare and antagonist protocols, oral contraceptive (OC) is frequently used as a pretreatment strategy before COH. Therefore, we focused on the role of E2 drop before hCG-triggering and its relationship to OC pretreatment. Previous summary and conclusion were based mainly on two protocols and limited sample size, making the conclusion ambiguous. In order to clarify the above issues, we selected patients from a broader scale with different treatment protocols, with or without OC pretreatment. Then, we made comparison between paired groups from a full-scale angle, hoping to provide further insights for clinical treatment.
Materials and Methods
Study Participants
This retrospective study was conducted in Center for Reproductive Medicine, Ren Ji Hospital, School of Medicine, Shanghai Jiao Tong University. Considering the retrospective nature of the study, informed consent forms were waived by the Ethics Committee for Reproductive Medicine of RenJi Hospital. We confirmed that personal private information was confidentially conducted and maintained only for scientific purposes.
Participants underwent IVF and intracytoplasmic sperm injection (ICSI) during their first cycle in our center were reviewed in the period of 2013–2019. All enrolled participants met the following requirements: (1) age ≤40 with a body mass index (BMI)≤28; (2) antral follicle number between 5~10 (both ovaries combined); (3) basal FSH <15 IU/L on the day 2–3 of menstrual cycle. Exclusion criteria included endometriosis, adenomyosis, intrauterine adhesion, uterine malformation, uterus with operation, hyperthyroidism and hypothyroidism, hyperprolactinemia, recurrent spontaneous abortion, recurrent implantation failure and cycle cancellation due to some reasons. In accordance with the above standards, participants who experienced a drop in serum E2 level during COH cycle were enrolled as the test group (n = 333) (Figure 1). At the same time, participants whose E2 level continuously increased until the day of hCG administration during their first cycle were selected as the control group (n = 333) (Figure 1).
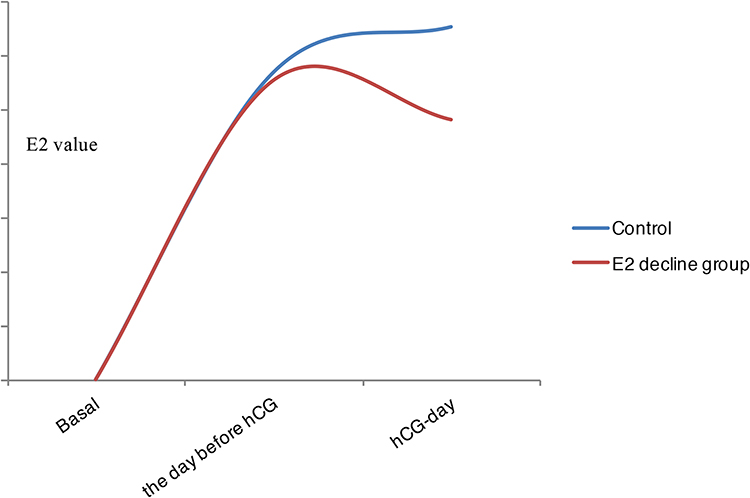 |
Figure 1 Illustration of E2 change during controlled ovarian hyperstimulation in control and E2 decline group. Note: This image describes the different trends of E2 change in our test and control groups during controlled ovarian hyperstimulation. |
Hyper-Stimulation Protocols
Four standard ovarian stimulation protocols include GnRH agonist ultra-short protocol, short protocol, long protocol and GnRH antagonist protocol were used in this study. Based on the application of oral contraceptive (OC) pretreatment before their first cycle, the test and control groups were further categorized into OC and non-OC sub-groups. The proportion of these four protocols was matched between paired groups.
In the GnRH agonist ultra-short protocol, GnRH agonist was administrated on the day 2 or day 3 of the menstrual cycle for 3 days, and gonadotropin (Gn) was given on the day 3 or day 4 of the menstrual cycle until the triggering day. In the GnRH agonist short protocol, GnRH agonist administration starts on the day 2 of the menstrual cycle, and then exogenous Gn was injected on the day 3 until the day of hCG administration. In the GnRH agonist long protocol, the administration of GnRH agonist started on the 21th day of last cycle (mid-luteal phase), and Gn administration starts on the day 3 of the next menstrual cycle until the triggering day. In the GnRH antagonist protocol, Gn was started on the day 2 of the menstrual cycle, and GnRH antagonist was administrated depending on individual’s follicle size and E2 level until the day of hCG administration.
During the COH, blood test and ultrasound follicular monitoring were carried out individually. When the leading follicles developed ≥18mm in diameter, hCG was administrated for oocyte maturation. Oocyte retrieval was guided by transvaginal ultrasonography 33–36hrs after the injection of hCG, and all the follicles with diameters ≥12mm were obtained. Retrieved oocytes were fertilized by conventional insemination or intracytoplasmic sperm injection, based on the semen quality. 16–18hrs after the fertilization, embryos with 2 pronucleus were considered as normal fertilization. Patients who were scheduled to transfer fresh embryos began luteal support on the day after oocyte retrieval, and fresh embryos were transferred at 72hrs after oocyte retrieval. Other patients were scheduled to transfer frozen embryos. The first pregnancy ultrasound was performed at 4 weeks after the embryo transfer, and the occurrence of gestational sacs was considered as clinical pregnancy.
Embryo Evaluation
On the third day after fertilization, embryos development was measured by regularity, the number of blastomeres and embryonic fragmentation, according to standard morphological criteria.10 Embryos with ≥6 cells and <20% fragmentation were defined as high-quality embryos, which were transferred or frozen by vitrification. The other embryos were continuously cultured into the blastocyst stage. On the day 5 or day 6, blastocysts scored as good morphology were frozen on the basis of Gardner et al criteria.11
Data Collection
Demographic information such as age, BMI, basal FSH, and anti-Mullerian hormone (AMH) was collected for each patient. Stimulation parameters like E2, LH, FSH and progesterone value on the day of hCG administration, peak E2 level, total hCG and Gn dosage were also gathered. IVF outcomes were assessed by the number of retrieved oocytes, normally fertilized zygotes and high-quality embryos, retrieved oocyte rate (the ratio of retrieved oocyte number to the number of follicles with ≥14mm in diameter on the triggering day), fertilization rate (for conventional insemination, the ratio is defined as the number of normally fertilized zygotes to the number of retrieved oocytes; for intracytoplasmic sperm injection, the ratio is defined as the number of normally fertilized zygotes to the number of MII oocytes) and high-quality embryo rate (the ratio of high-quality embryo number to the embryo number on day 3). Clinical outcomes were evaluated as implantation rate, pregnancy rate, miscarriage rate and live birth rate accumulated within the first treatment cycle individually. Implantation rate was defined as the ratio of implanted embryo numbers to transferred embryo numbers (fresh and frozen embryos), and pregnancy rate was the ratio of gestational cycle numbers to transferred cycle numbers. Miscarriage rate was the ratio of abortive cycles to the number of gestational cycles, while live birth rate was the ratio of live birth number to transferred cycle numbers.
Considered that the first pregnancy ultrasound was performed at 4 weeks after the embryo transferred, the numbers of implanted embryos and the cycles of clinical pregnancy were calculated as the number of intrauterine gestational sacs on record.
Statistical Analysis
All the data were analyzed using SPSS (Version 20.0). Numeric variables were presented as the mean ± SD, and categorical variables were expressed as numbers and percentages. For continuous variables, statistical analysis was carried out using T-test, and categorical variables were analyzed using Chi-square test, with p <0.05 was considered statistically significant.
Results
General Characteristics Between E2 Decline and Control Groups
In total, no difference was detected in age, proportion of infertility indications, treatment protocols, AMH, hCG dosage and Gn dosage during COH between E2 decline group and control group (p > 0.05). Participants of the E2 decline group have lower BMI (21.0 ± 2.6kg/m2 versus 21.5 ± 2.6kg/m2, p = 0.021) and higher basal FSH level (7.0 ± 2.0IU/L versus 6.7 ± 1.8IU/L, p = 0.041) when compared with control group. Moreover, the peak E2 value, E2, LH and FSH levels on the day of hCG administration in the E2 decline group were all remarkably reduced compared with control group (11,065.1 ± 8292.1pmol/L versus 13,048.9 ± 7883.1pmol/L, 9614.0 ± 7457.3pmol/L versus 13,048.9 ± 7883.1pmol/L, 1.7 ± 1.9IU/L versus 2.8 ± 2.3IU/L, 11.0 ± 3.7IU/L versus 11.6 ± 3.6IU/L, respectively) (p < 0.05) (Table 1).
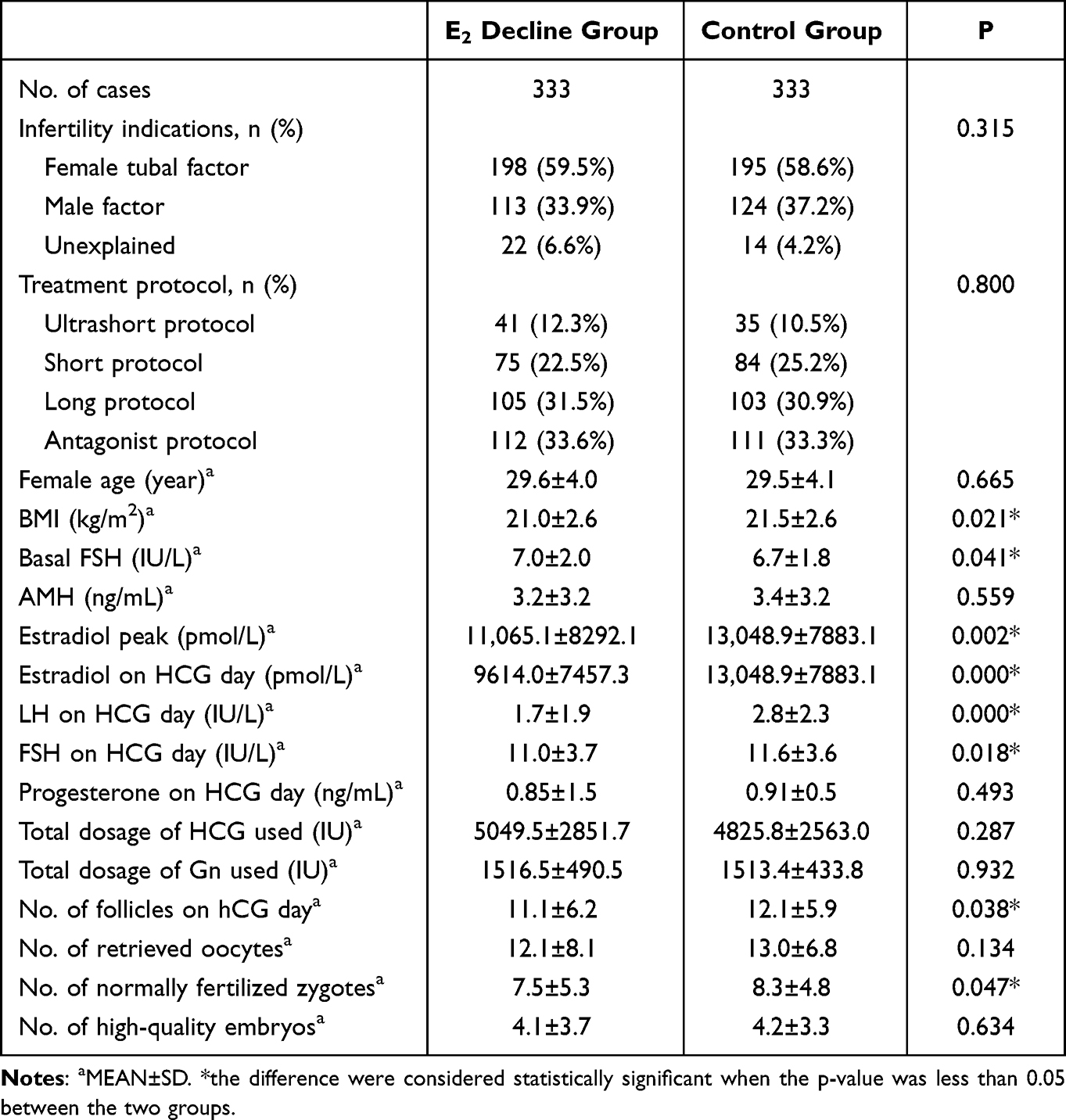 |
Table 1 Demographics and Cycle Parameters of the E2 Decline Group and Control Group |
IVF and Clinical Outcomes Between E2 Decline and Control Group
In regard to IVF outcomes, number of follicles on hCG day and normally fertilized zygote in E2 decline group was significantly decreased versus control group (11.1 ± 6.2 versus 12.1 ± 5.9, p = 0.038 and 7.5 ± 5.3 versus 8.3 ± 4.8, p = 0.047, respectively) without any changes in other IVF outcome parameters (Tables 1 and 2).
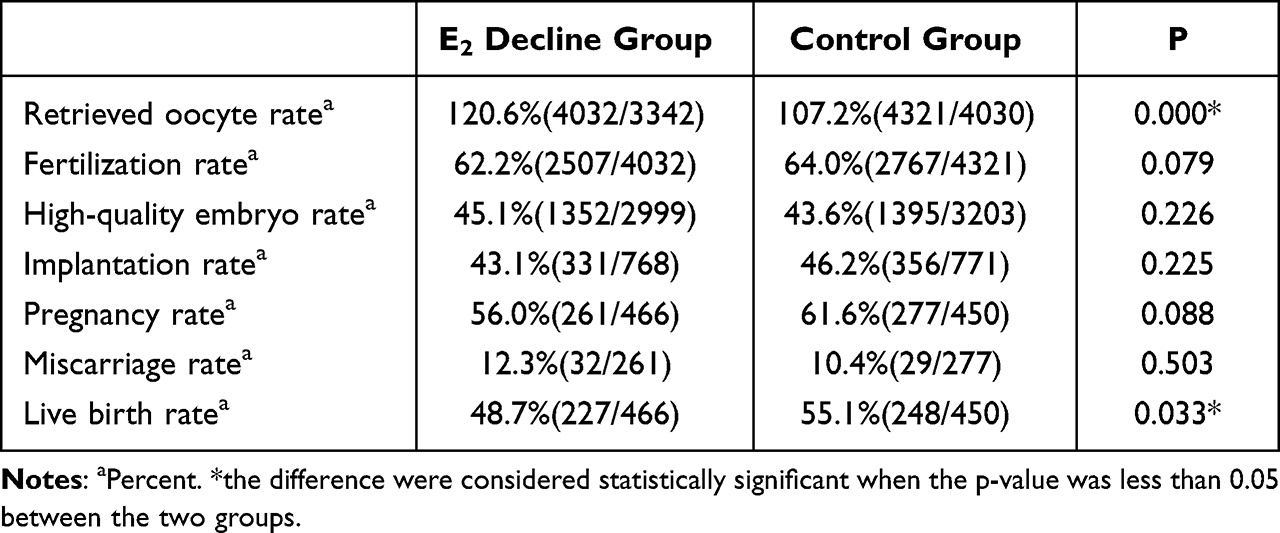 |
Table 2 IVF and Clinical Outcomes of the E2 Decline Group and Control Group |
As for the clinical outcomes, significantly decreased live birth rate in E2 decline group (48.7% versus 55.1%, p = 0.033) indicated an adverse effect of E2 drop on IVF and clinical outcomes. Moreover, the pregnancy rate of the E2 decline group was lower than the control (56.0% vs 61.6%, p = 0.088), although the differences were not statistically significant. In addition, the implantation rate and miscarriage rate were similar between the two groups (43.1% vs 46.2%, p = 0.225 and 12.3% vs 10.4%, p = 0.503, respectively) (Table 2).
The Role of OC Pretreatment on the IVF and Clinical Outcomes of Both E2 Decline and Control Group
Depending on pretreatment strategy before the cycle, we classified the E2 decline group and control group into OC and non-OC subgroups, and made respective comparisons as illustrated in Tables 3 and 4.
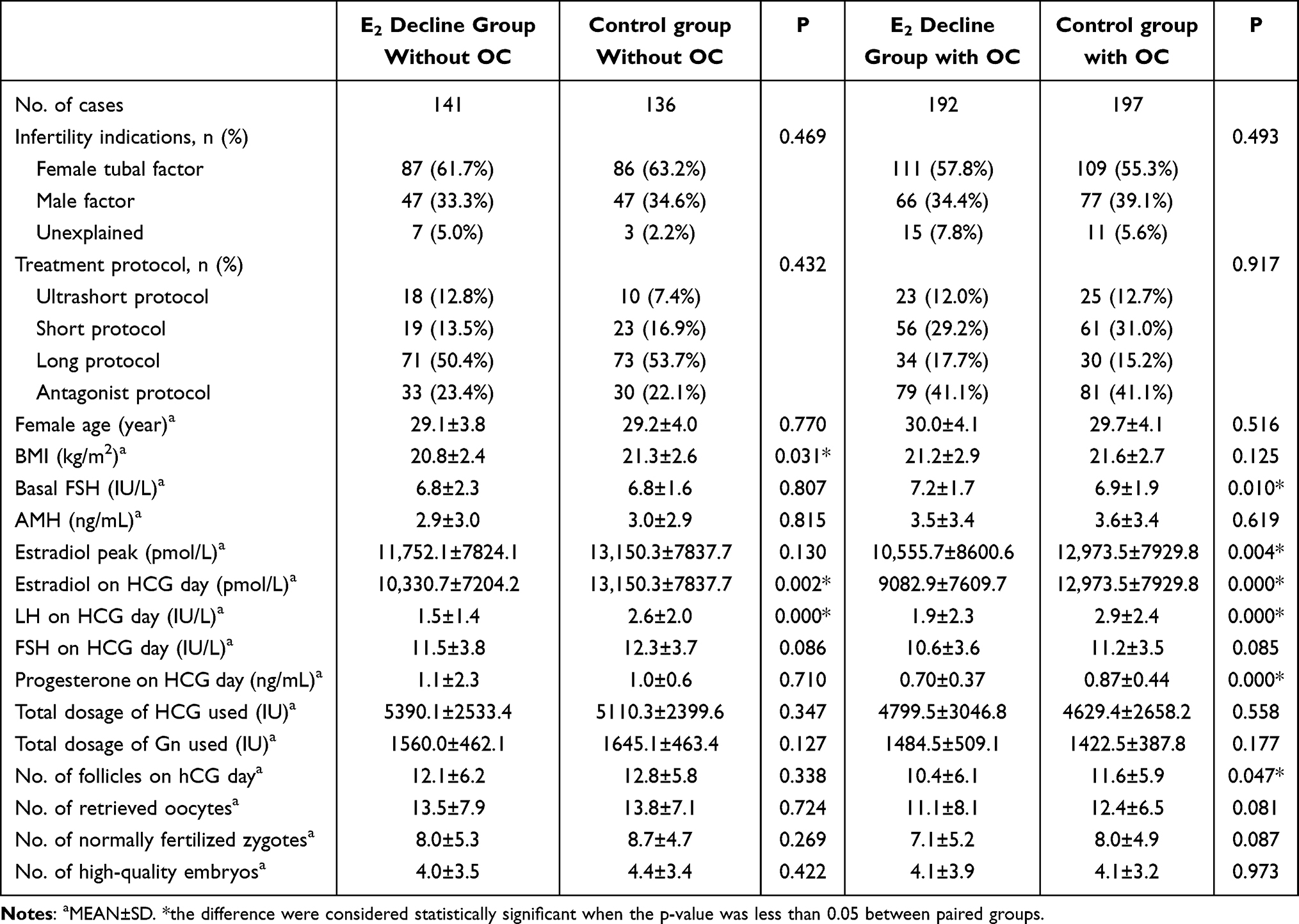 |
Table 3 Demographics and Cycle Parameters of the E2 Decline Group and Control Group Without Pretreatment of Oral Contraceptive (OC) and with Pretreatment of Oral Contraceptive (OC) |
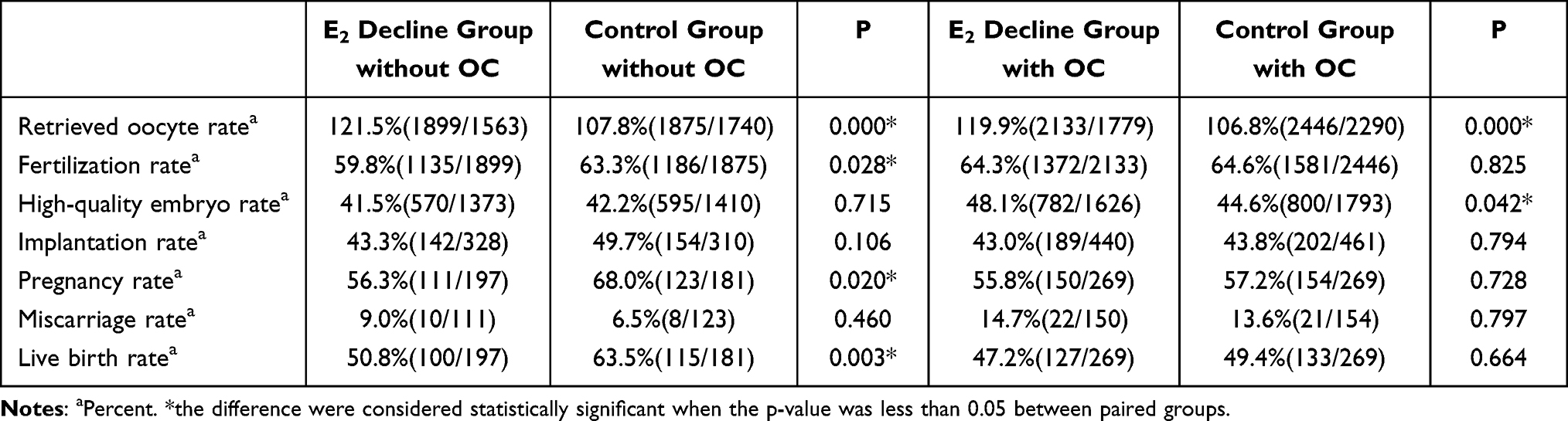 |
Table 4 IVF and Clinical Outcomes of the E2 Decline Group and Control Group Without Pretreatment of Oral Contraceptive (OC) and with Pretreatment of Oral Contraceptive (OC) |
For patients without OC pretreatment, the fertilization rate, pregnancy rate and live birth rate of the E2 decline group were significantly lower than those in the controls (59.8% versus 63.3%, p = 0.028, 56.3% versus 68.0%, p = 0.020 and 50.8% vs 63.5%, p = 0.003, respectively), suggesting the negative prediction role of E2 drop in patients without OC pretreatment (Table 4). Furthermore, a significant reduction in BMI, E2 and LH value on hCG day was detected in the E2 decline group compared with controls (20.8 ± 2.4 versus 21.3 ± 2.6kg/m2, p = 0.031; 10,330.7 ± 7204.2 versus 13,150.3 ± 7837.7pmol/L, p = 0.002; 1.5 ± 1.4 versus 2.6 ± 2.0, p = 0.000, respectively) (Table 3). Others were comparable in infertility indications proportion, treatment protocol application, age, basal FSH, AMH value, hCG and Gn dosage in E2 deline groups versus controls (p > 0.05). However, for participant pretreatment with OC, except for higher retrieved oocyte rate and high-quality embryo rate of E2 deline group, no difference was detected in IVF and clinical outcomes between the E2 decline and control groups (p > 0.05) with comparable infertility indications proportion, treatment protocol application, age, BMI, AMH value and Gn dosage (p > 0.05) (Tables 3 and 4). Netherless, we found lower peak E2 value, E2, LH and progesterone value on hCG day in the E2 decline group pretreatment with OC when compared with the control group pretreatment with OC (10,555.7 ± 8600.6 versus 12,973.5 ± 7929.8pmol/L, p = 0.004; 9082.9 ± 7609.7 versus 12,973.5 ± 7929.8pmol/L, p = 0.000; 1.9 ± 2.3 versus 2.9 ± 2.4, p = 0.000; 0.70 ± 0.37 versus 0.87 ± 0.44, p = 0.000, respectively).
Discussion
Serum hormone measurement and ultrasound follicular monitoring are two integral components for COH treatment in most IVF programs.12,13 In our study, we found that the occurrence of falling E2 before the day of hCG administration could be observed in many protocols, such as flare protocol, long protocol, antagonist protocol. Therefore, we collected participants of these protocols and matched contemporaneous cases to explore the potential influence on IVF/clinical outcomes. We found that E2 decline group had decreased dominant follicles on hCG day and normally fertilized zygotes than the control group and live birth rate were also significantly reduced in the E2 decline group.
In cultured granulosa cells, estrogen enhanced FSH- and LH-induced aromatase activity, cyclic adenosine monophosphate (cAMP) production and progestin biosynthesis, which were related to granulosa cell proliferation, follicle growth and follicular antrum formation.14,15 E2 level in follicular fluid was a direct reflection of aromatase activity in correlation with granulosa cell number and follicular maturity,16,17 hence the occurrence of falling E2 might be due to decreased granulosa cell number or aromatase activity of the developing follicle.9 In addition, previous research demonstrated that estrogens could inhibit granulosa cell apoptosis, whereas androgens increased DNA fragmentation associated with follicular atresia.18 Therefore, the consequence of E2 decline prior to hCG administration maybe associate with compromised oocyte quality. And in our study, the E2 decline group did have lower normally fertilized zygote number and then live birth rate than control group (7.5 ± 5.3 versus 8.3 ± 4.8, p = 0.047; 48.7% versus 55.1%, p = 0.033, respectively), which may imply compromised oocyte quality in E2 decline group.
Oral contraceptive pretreatment before COH is widely used for scheduling cycles.19 Through suppression of endogenous gonadal function, oral contraceptives assist synchronizing antral follicle cohort before gonadotropin administration.20 Consequently, based on pretreatment strategy before their first cycle, we divided the E2 decline group and control group into OC and non-OC sub-groups. We found that patients without OC (E2 decline group without OC combined with control group with OC) had higher implantation rate, pregnancy rate and live birth rate than patients with OC (E2 decline group with OC combined with control group with OC) (Table 4). Several studies demonstrated than OC pretreatment was associated with persistently lower LH concentrations and thinner endometrium, then resulted in lower pregnancy rate and increased miscarriage rate.21–23 Besides, different ratio of stimulation protocol constitution in OC and non-OC groups may attribute to the above discrepancy. Subsequently, results in our study indicated that in participants without OC pretreatment, fertilization rate, pregnancy rate and live birth rate of the E2 decline group were significantly lower than the control (Table 4). During the late luteal phase, antral follicles are exposed to progressively increased FSH levels to guarantee their subsequent growth. Small antral follicles that are sensitive to lower level of FSH develop earlier than others in this period.20 With the gradual exposure of follicles to FSH, size discrepancies may be enhanced during the subsequent cycle. In COH without OC pretreatment, this marked discrepancies may lead to compromised oocyte quality, plus E2 decline associated with decreased oocyte quality; these may imply a potential reason for the significant lower fertilization rate and live birth rate in E2 decline group without OC pretreatment. Of course, due to limitation of sample quantity and retrospective analysis, this speculation needs more supportive evidence. In addition, with the progressive application of artificial intelligence in many fields of medicine,24 we may integrate individualized biological and clinical parameters to predict future performance.
Conclusion
In summary, for participants with normal ovarian reserve, the occurrence of E2 decline before the day of hCG administration during COH without OC pretreatment was linked with decreased fertilization rate, pregnancy rate and live birth rate. In contrast, for participants with OC pretreatment, E2 decline had no impact on IVF and clinical outcomes. Due to the limitations of relatively small sample size and retrospective property, this study inevitably had selection bias. Therefore, a prospective randomized controlled trial (RCT) is needed with large samples from multiple centers to provide support for this conclusion in the future, hoping to provide new insights for individualized treatment.
Abbreviation
AMH, anti-Mullerian hormone; BMI, body mass index; cAMP, cyclic adenosine monophosphate; COH, controlled ovarian hyperstimulation; E2, estradiol; FSH, follicle stimulating hormone; Gn, gonadotropin; GnRH, gonadotropin releasing hormone; hCG, human chorionic gonadotropin; ICSI, intracytoplasmic sperm injection; IVF, in vitro fertilization; LH, luteinizing hormone; OC, oral contraceptive; OHSS, ovarian hyperstimulation syndrome.
Ethics Approval
This retrospective study involving available data was in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The Ethics Committee for Reproductive Medicine of RenJi Hospital approved this study.
Acknowledgments
Thank all the participants who enrolled in this study for great cooperation and the colleagues for professional and technical support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Key Research and Development Program of China under Grant No. 2021YFC2701104 and 2022YFC2703204; National Natural Science Foundation under Grant No. 82171623; Program of Shanghai Academic Research Leader under Grant No. 21XD1401900; Shanghai Commission of Science and Technology under Grant 20DZ2270900; Three-Year Action Plan for Strengthening the Construction of the Public Health System in Shanghai (GWVI-11.1-36); and Shanghai’s Top Priority Research Center Construction Project (2023ZZ02002).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Calhaz-Jorge C, Leal F, Cordeiro I., et al. Pituitary down-regulation in IVF cycles: is it necessary to use strict criteria? J Assist Reprod Genet. 1995;12(9):615–619. doi:10.1007/BF02212585
2. Garnett E, Bruno-Gaston J, Cao J, et al. The importance of estradiol measurement in patients undergoing in vitro fertilization. Clin Chim Acta. 2020;501:60–65. doi:10.1016/j.cca.2019.09.021
3. Lyttle Schumacher BM, Mersereau JE, Steiner AZ. Cycle day, estrogen level, and lead follicle size: analysis of 27,790 in vitro fertilization cycles to determine optimal start criteria for gonadotropin-releasing hormone antagonist. Fertil Steril. 2018;109(4):633–637. doi:10.1016/j.fertnstert.2017.12.021
4. Geng Y, Xun Y, Hu S, et al. GnRH antagonist versus follicular-phase single-dose GnRH agonist protocol in patients of normal ovarian responses during controlled ovarian stimulation. Gynecol Endocrinol. 2019;35(4):309–313. doi:10.1080/09513590.2018.1528221
5. Garcia-Velasco JA, Isaza V, Quea G, et al. Coasting for the prevention of ovarian hyperstimulation syndrome: much ado about nothing? Fertil Steril. Mar. 2006;85(3):547–554.
6. Sun B, Ma Y, Li L, et al. Factors Associated with Ovarian Hyperstimulation Syndrome (OHSS) Severity in Women With Polycystic Ovary Syndrome Undergoing IVF/ICSI. Front Endocrinol. 2020;11:615957. doi:10.3389/fendo.2020.615957
7. Jones HW, Acosta A, Andrews MC, et al. The importance of the follicular phase to success and failure in in vitro fertilization. Fertil Steril. 1983;40(3):317–321. doi:10.1016/S0015-0282(16)47293-6
8. Styer AK, Jackson KV, Hornstein MD, et al. Pregnancy outcomes in in vitro fertilization cycles with serum estradiol drop prior to human chorionic gonadotropin. Int J Gynaecol Obstet. 2005;89(2):133–137. doi:10.1016/j.ijgo.2005.02.005
9. Fisher S, Grin A, Paltoo A, et al. Falling estradiol levels as a result of intentional reduction in gonadotrophin dose are not associated with poor IVF outcomes, whereas spontaneously falling estradiol levels result in low clinical pregnancy rates. Hum Reprod. 2005;20(1):84–88. doi:10.1093/humrep/deh543
10. Fragouli E, Alfarawati S, Spath K, et al. Morphological and cytogenetic assessment of cleavage and blastocyst stage embryos. Mol Hum Reprod. 2014;20(2):117–126. doi:10.1093/molehr/gat073
11. Gardner DK, Lane M, Stevens J, et al. Reprint of: blastocyst score affects implantation and pregnancy outcome: towards a single blastocyst transfer. Fertil Steril. 2019;112(4 Suppl1):e81–e84. doi:10.1016/j.fertnstert.2019.08.077
12. Kwan I, Bhattacharya S, Woolner A. Monitoring of stimulated cycles in assisted reproduction (IVF and ICSI). Cochrane Database Syst Rev. 2021;4(4):CD005289. doi:10.1002/14651858.CD005289.pub4
13. Zhang Y, Xu Y, Wang Y, et al. Comparison of the predictive value of progesterone-related indicators for pregnancy outcomes of women undergoing the short-acting GnRH agonist long protocol: a retrospective study. J Ovarian Res. 2021;14(1):14. doi:10.1186/s13048-021-00768-2
14. Shoham Z, Schachter M, Schachter M. Estrogen biosynthesis--regulation, action, remote effects, and value of monitoring in ovarian stimulation cycles. Fertil Steril. 1996;65(4):687–701. doi:10.1016/S0015-0282(16)58197-7
15. Adashi EY, Hsueh AJ. Estrogens augment the stimulation of ovarian aromatase activity by follicle-stimulating hormone in cultured rat granulosa cells. J Biol Chem. 1982;257(11):6077–6083. doi:10.1016/S0021-9258(20)65107-9
16. McNatty KP, Smith DM, Makris A, et al. The microenvironment of the human antral follicle: interrelationships among the steroid levels in antral fluid, the population of granulosa cells, and the status of the oocyte in vivo and in vitro. J Clin Endocrinol Metab. 1979;49(6):851–860. doi:10.1210/jcem-49-6-851
17. Hillier SG, Reichert LE, Van Hall EV. Control of preovulatory follicular estrogen biosynthesis in the human ovary. J Clin Endocrinol Metab. 1981;52(5):847–856. doi:10.1210/jcem-52-5-847
18. Billig H, Furuta I, Hsueh AJ. Estrogens inhibit and androgens enhance ovarian granulosa cell apoptosis. Endocrinology. 1993;133(5):2204–2212. doi:10.1210/endo.133.5.8404672
19. Xu L, Ding L, Jiang J, et al. Effects of oral contraceptive pretreatment on IVF outcomes in women following a GnRH agonist protocol. Reprod Biomed Online. 2019;39(6):924–930. doi:10.1016/j.rbmo.2019.08.002
20. Nassar J, Tadros T, Adda-Herzog E, et al. Steroid hormone pretreatments in assisted reproductive technology. Fertil Steril. 2016;106(7):1608–1614. doi:10.1016/j.fertnstert.2016.09.013
21. Wei D, Shi Y, Li J, et al. Effect of pretreatment with oral contraceptives and progestins on IVF outcomes in women with polycystic ovary syndrome. Hum Reprod. 2017;32(2):354–361. doi:10.1093/humrep/dew325
22. Kolibianakis EM, Papanikolaou EG, Camus M, et al. Effect of oral contraceptive pill pretreatment on ongoing pregnancy rates in patients stimulated with GnRH antagonists and recombinant FSH for IVF. A randomized controlled trial. Hum Reprod. 2006;21(2):352–357. doi:10.1093/humrep/dei348
23. Meldrum DR, Scott RT, Levy MJ, et al. Oral contraceptive pretreatment in women undergoing controlled ovarian stimulation in ganirelix acetate cycles may, for a subset of patients, be associated with low serum luteinizing hormone levels, reduced ovarian response to gonadotropins, and early pregnancy loss. Fertil Steril. 2009;91(5):1963–1965. doi:10.1016/j.fertnstert.2008.01.007
24. Medenica S, Zivanovic D, Batkoska L, et al. The future is coming: artificial intelligence in the treatment of infertility could improve assisted reproduction outcomes-the value of regulatory frameworks. Diagnostics. 2022;12(12):2979. doi:10.3390/diagnostics12122979
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.