")
Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 15
Endodontic Orthograde Retreatments: Challenges and Solutions
Authors Zanza A, Reda R , Testarelli L
Received 3 May 2023
Accepted for publication 5 October 2023
Published 24 October 2023 Volume 2023:15 Pages 245—265
DOI https://doi.org/10.2147/CCIDE.S397835
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Alessio Zanza, Rodolfo Reda, Luca Testarelli
Department of Oral and Maxillo-Facial Sciences, Sapienza University of Rome, Rome, Italy
Correspondence: Rodolfo Reda, Department of Oral and Maxillo-Facial Sciences, Sapienza University of Rome, Via Caserta 06, Rome, 00161, Italy, Email [email protected]
Abstract: Endodontic orthograde retreatments are considered one of the possible treatment options in case of post-treatment diseases considering the promising results present in the literature. Despite this, a plethora of articles have been published on this topic, and drawing conclusions could be challenging. For this reason, this review aims to summarize the crucial points on each aspect of non-surgical endodontic retreatments, discussing and comparing the current protocols, techniques, materials, and indications. Taking into consideration data from the literature, in terms of diagnosis, CBCT should be considered the first choice, since it can thoroughly affect the diagnosis and treatment plan. Regarding the procedural phases, some conclusions can be drawn: when present, coronal restoration materials such as crowns, partial prostheses, post, and core should be removed; the use of magnification devices, ultrasonic instruments, and an in-depth interpretation of radiographic images with both 2D and 3D images are strongly recommended during the orifice location; additional protocols such as irrigants activation, ultrasonic cleaning, and rotary or reciprocating instrumentation of treated canals are strongly recommended for filling materials removal and to achieve a high-quality chemo-mechanical disinfection; perforations should be treated as soon as possible, and the material of choice to treat them is the MTA or other calcium-silicate-based repair materials; the presence of ledges does not intrinsically reduce the success rate of RCRts if properly managed; in case of instrument fragments, their removal should be considered as the first treatment option, however many variables should be considered to select the proper technique or consider the option of bypassing.
Keywords: endodontic retreatment, endodontic retreatment outcome, diagnosis, ledge, perforation, instrument fragment removal, missed anatomy, filling material removal
Introduction
Despite the high success rate of primary orthograde endodontic treatments, post-treatment diseases are common.1 As stated by Ricucci, the primary and post-treatment periapical lesions are always associated with intraradicular and/or extraradicular bacteria.2 In case of persistent pathosis after root canal treatment, endodontic retreatment is strongly recommended and should be considered the first treatment option.3 According to the Glossary of Endodontic Terms by the American Association of Endodontists, a non-surgical root canal retreatment procedure is defined as a procedure to remove root canal filling materials from the tooth, followed by cleaning, shaping, and obturating the canals.
This review of the literature aims to describe the state of the art of non-surgical orthograde retreatments in terms of outcome, diagnosis, and clinical procedures, highlighting the most significant points on the theme, as well as providing a possible direction for future scientific and clinical research.
Outcome Assessment for Root Canal Treatments and Decision-Making Process for Root Canal Retreatments
Treatment outcome assessment in Endodontics has been a source of debate since the second half of the XX century. This mainly arises from the complexity of the periapical healing process that, as thoroughly demonstrated, usually takes up 1 year but could require a longer period, even 4 or 10 years.4–6 The healing process duration depends on several factors, and one above all is undoubtedly the host’s immune response and systemic health status.6 Regarding this, as described by Segura-Egea et al, the repair of periapical tissues is favored by the association of the reduction in bacterial load of root canals and the host’s immune response, taking into consideration that the individual’s systemic conditions, such as diabetes, bowel chronic diseases, cardiovascular diseases and infective diseases like HIV, can interfere in this process, determining the delay or the impairment of the healing process.7 Despite the interindividual differences during the endodontic disease resolutions, the European Society of Endodontology proposed guidelines for the assessment of the outcome of root canal treatments (RCTs), defining the terms “success” and “failure” in Endodontics. First of all, the primary orthograde endodontic treatment should be assessed at least after 1 year, and a favorable outcome is indicated when these findings are accomplished: absence of pain, swelling, and other symptoms, no sinus tract, no loss of function, and radiological evidence of a normal periodontal ligament space around the root.8 On the other hand, an unfavorable outcome should be assessed when one of the following findings is present: the presence of signs and symptoms of an infection; a radiologically visible lesion has appeared subsequently to treatment or a pre-existing lesion has increased in size; a lesion has remained the same size or has only diminished in size during the 4-year assessment period; signs of continuing root resorption are present.8 All conditions in which the lesion has remained the same size or has reduced its volume after 1 year, the outcome is assessed as uncertain and a further follow-up period is required up to 4 years.8 Nevertheless, the above-mentioned terminology is focused on the treatment rather than the disease/healing status and the patient, and this point has been thoroughly debated and argued by researchers.9–11 According to this, the American Association of Endodontists (AAE) proposed a patient-centered terminology for the assessment of endodontic outcomes focused on the healing/disease status, dividing the endodontic cases into “healed/functional”, “healing” and “non-healed”. The healed tooth is defined as a functional, asymptomatic tooth with no or minimal radiographic periradicular pathosis that is serving its intended purpose in the dentition. On the contrary, a non-healed tooth is defined as a nonfunctional, symptomatic tooth with or without radiographic periradicular pathosis. Between these two opposite conditions, it has been described as an intermediate and ongoing situation that considers the healing process duration, according to the interindividual differences as discussed before: the “healing” tooth. This status is described as a tooth with periradicular pathosis, which is asymptomatic and functional, or a tooth with or without radiographic periradicular pathosis, which is symptomatic but whose intended function is not altered (AAE (2005) Approved definitions of the endodontic outcome. Chicago, IL: American Association of Endodontists Communique, XXIX, 3.).9 Moreover, the AAE terminology focuses the attention on the concept of the functional tooth, trying to solve the never-ending debate on limitations of the periapical healing assessment that is actually based on the surrogate measures of both radiographic and clinical criteria. As thoroughly described by Friedman & Mor, the “functional” category comprises teeth with clinical normalcy without regard to radiographic (periapical) status.10 The aim of the introduction of the “functional state” was to limit the retreatment or extraction procedures on asymptomatic teeth, continuing monitoring as long as they remain asymptomatic.9 This point is crucial in determining the decision-making process in asymptomatic teeth with a chronic stable periapical disease, resulting in a more conservative approach. The above-mentioned concept is based on the fact that in most cases, the persistent lesions remain asymptomatic even when a slight radiographical change occurs over long periods, with a low risk of painful exacerbation.12,13
In addition to the periapical status and symptomatology, another factor must be taken into consideration during the decision-making process in secondary endodontics: the quality of the coronal sealing and post-endodontic rehabilitation. As demonstrated by several articles, those factors have a major impact on the probability of periapical healing, and a tooth characterized by a “satisfactory” post-endodontic restoration exhibits a three-fold better periapical healing rate than a tooth with “unsatisfactory” post-endodontic restoration.14–17 However, clarifying what “satisfactory” and “unsatisfactory” mean in terms of coronal restoration is necessary to have an in-depth understanding and interpretation of the decision-making process of secondary endodontic treatments. “Satisfactory” restorations have been defined as restorations in which none of these points is found: evidence of marginal discrepancy or leakage; evidence of marginal discoloration; evidence of recurrent caries; evidence of exposure of canal root filling materials; and history of restoration decementation.5,6,16,18–20
In light of the above, the Authors propose a decision-making process that aims to indicate when retreatment of previously endodontically treated teeth should be suggested, taking into account the most relevant factors affecting the treatment plan determination: quality of previous endodontic treatment, presence of signs and symptoms, presence of periapical radiolucency, quality of coronal and post-endodontic restoration, the elapsed time from primary endodontic treatment and need of prosthodontics intervention involving the tooth (Figure 1). Moreover, the previous indications should be interpreted with a broad point of view considering the general contra-indications for root canal treatments and the indications for surgical endodontics, summarized in Table 1.8
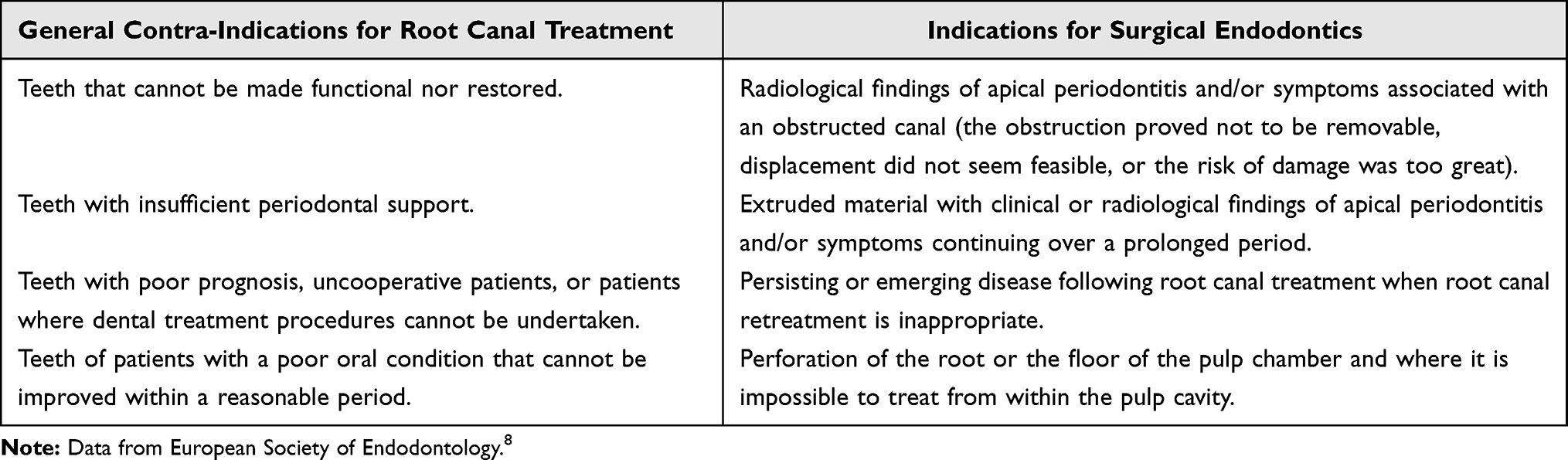 |
Table 1 List of General Contra-Indications for Root Canal Treatment and Indication for Surgical Endodontics According to the Consensus Report of the European Society of Endodontology. |
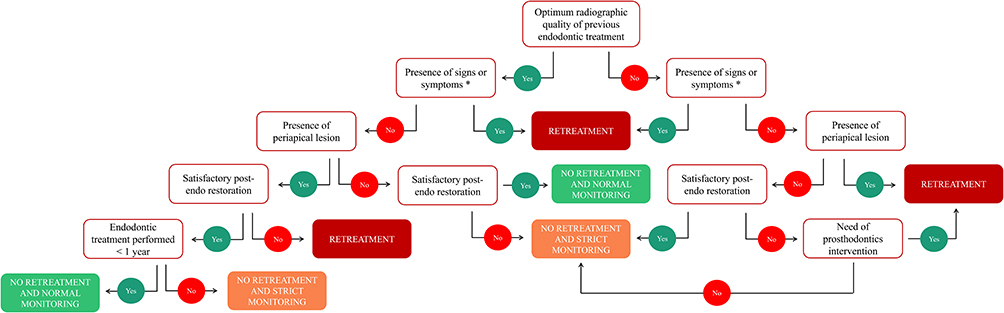 |
Figure 1 Schematic representation of the decision-making process for root canal retreatment. Note: *Presence of signs or symptoms strictly related to endodontic causes. |
General Factors Affecting the Outcome of Root Canal Retreatments
The results of non-surgical retreatments in endodontics strictly depend on several factors, among which the assessment criteria for the success rate and healing of periapical tissues are crucial. The most common surrogate measures for the outcome evaluation of root canal retreatments (RCRts) are bidimensional radiography, thanks to its high specificity, and the evaluation of clinical signs and symptoms.14,21,22 In a recent scoping review, it has been reported that clinical and radiographic evaluations, as outcome measurement tools, were performed in 73% (n = 259) and 88% (n = 311) of the studies evaluated (n = 354).23 Nevertheless, three-dimensional imaging is more sensitive to detect periapical lesions than bidimensional radiography. As demonstrated by Aminoshariae et al, Cone-Beam Computed Tomography (CBCT) has doubled the chance of detecting periapical lesions than bidimensional periapical radiography in endodontic outcome studies.24 However, due to higher ionizing radiation exposure, possible higher levels of scatter and noise, and higher costs, the use of CBCT as an assessment tool for the outcome of RCRts is not justified.25,26 To date, three-dimensional evaluation was used for only a small number of studies, either in combination with bidimensional evaluation. Azarpazhooh et al reported that CBCT was used in combination with periapical radiographs in only 20 studies (6%) and as a stand-alone radiographic outcome measurement tool in 6 studies (2%).23 The most widespread bidimensional radiographic index for the assessment of RCRts outcome is the Periapical Index score (PAI score) proposed by Orstavik et al in 1986.27 Although the PAI score is originally composed of five categories, it has usually been used as a dichotomic score: PAI 1 and 2 (“success” or “healthy”) versus PAI 3, 4 and 5 (“failure” or “diseased”).22,28–30 Following this scoring system, some authors investigated the RCRts outcome by using both strict and lenient criteria.14,31 Usually, the treatment outcome determined by using stricter criteria has been categorized as “successful”, “uncertain”, and “failure.” Successful treatments are those in which at the follow-up the PAI score is 1 or 2, while failure treatments are those in which the PAI score is 4 or 5 or has a worse value than the initial condition. Uncertain treatments, otherwise, include the cases in which the PAI score has moved from an initial score of 4 or 5 to a better score, indicating that the healing process is ongoing, despite the short observation times that have not allowed complete healing.31 When lenient criteria are used, both “successful” and “uncertain” teeth are considered as a positive outcome, and thus, the success rate is higher. Ng et al in a systematic review of the literature published in 2008 evidenced a pooled weighted success rate ranging from 76.7% (strict criteria) to 77.2% (lenient criteria), but the raw data showed different results, with ranges from 62% to 90% based on strict criteria and 28% to 93% based on lenient criteria.14 Another systematic review by Torabinejad et al, published in 2009, showed comparable results, with a success rate for RCRts of 70.9% at 2–4 years.32 Moreover, a more recent (2017) systematic review by Chercoles-Ruiz et al showed slightly different success rates, ranging from 84.1% to 88.6% after 4 to 10 years for RCRts, with the majority of studies analyzed not specifying the assessment criteria.33
In conclusion, considering the wide heterogeneity among studies in terms of assessment measurement tools, follow-up period, the definition of success, failure, healed, healing, etc., missing information, and misreporting of data, defining the actual positive outcome rate is impossible.23 For this reason, strict, standardized, repeatable, and complete methodologies should be promoted, defining easy-to-use reporting guidelines.
Despite this, there have been several attempts to define the factors able to affect the outcome of primary and secondary root canal treatments,5,6,14,15,34 the last of which has been recently (2023) published by Gulabivala et al.16 According to the authors, the factors able to influence the outcome of RCRts are identical to those able to affect primary endodontic treatments, except for peculiar factors related to unresolved biological problems, alteration of the original root canal system morphology, removal of any obstructing restorative materials and iatrogenic errors introduced by the primary treatment attempt.16 Regarding those specific factors, an in-depth discussion is performed below in each specific paragraph.
From a general point of view, the factors that may affect the outcome of primary and secondary non-surgical root canal treatments can be divided into three groups:
- Pre-operative factors: in which are listed all patient and tooth factors such as sex, age, systemic health, tooth anatomy and position, pre-operative pulpal and periapical status, tooth integrity, and operator’s qualification.
- Intra-operative factors: in which are listed all factors related to the endodontic procedures from the access cavity to the root canal filling, considering devices and tools used by the endodontist.
- Post-operative restorative factors: in which are listed all factors related to post-endodontic rehabilitation such as the remaining tooth structure and its integrity, type of post-endodontic restoration and its material, the timing of permanent restoration, marginal adaptation, and occlusal dynamics.
Since the discussion of each factor and its relationship to the endodontic outcome is not the main scope of this review, the authors merely summarized them in Table 2, highlighting the positive, negative, uncertain, or absent relationship with the endodontic outcome. Among all, as described by Gorni and Gagliani, canal and apical morphology alterations should be considered the most affecting factor in the endodontic outcome. In those situations in which the initial anatomy was altered by the primary orthograde treatment, the success percentage of RCRts at 2 years was halved (from 80–90% to 40–50%), independently from the tooth type.35
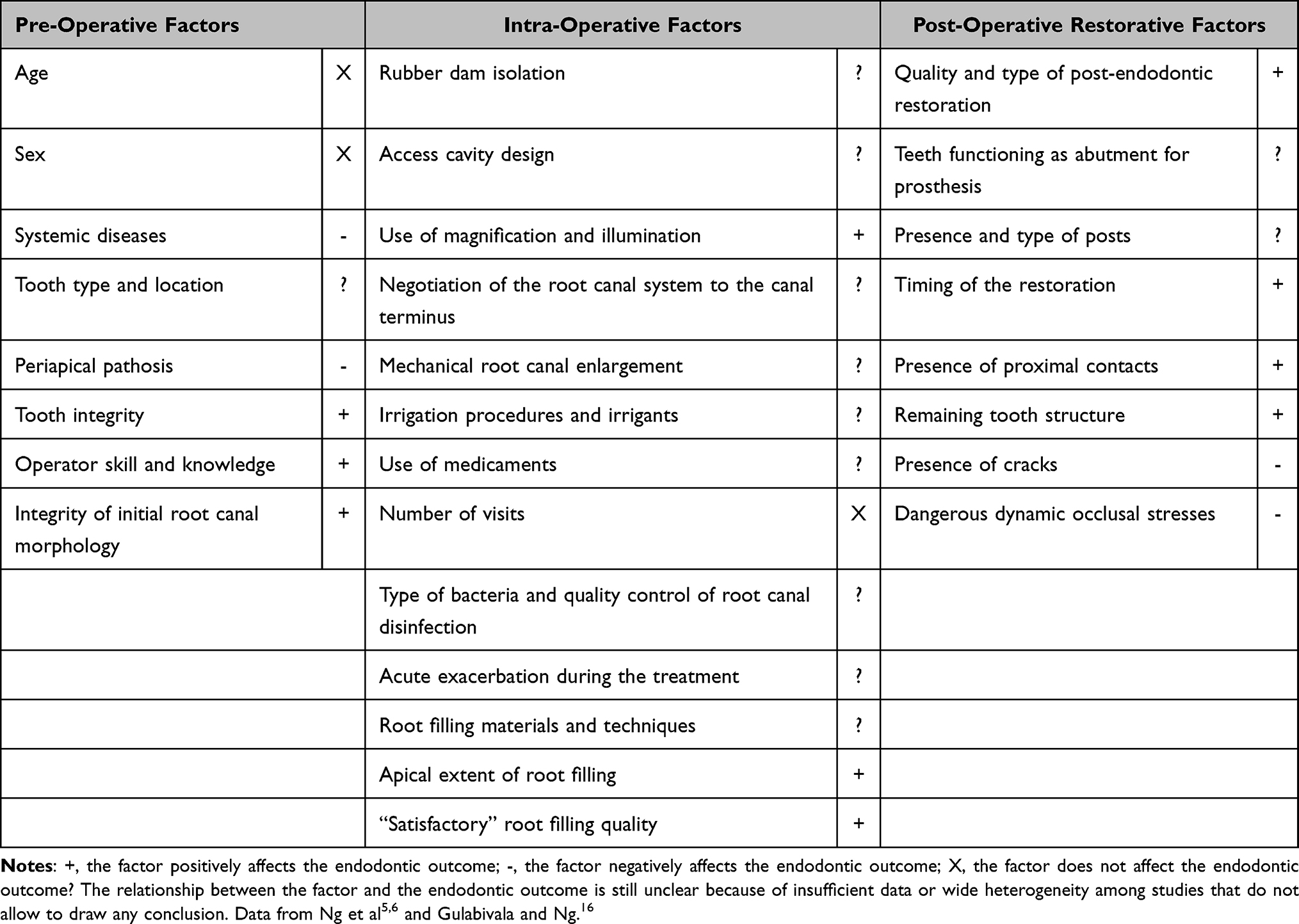 |
Table 2 Summary Table of All Investigated Factors Affecting the Endodontic Outcome Divided According to the Operative Phase., |
As shown in the above-mentioned table, most of the factors, especially in the intra-operative group, have a doubt influence on the treatment outcome. As stated by Ng et al and by Gulabivala et al, this is mainly due to the lack of data and the wide heterogeneity among studies that do not allow to draw clear conclusions in terms of periapical healing and tooth survival.5,6,15,16,34 Based on this, further clinical research with a high-quality control of bias and confounding factors is needed in order to guarantee an in-depth understanding of the topic.
Diagnosis
The diagnosis process in secondary root canal treatments follows a strict process of data collection and it is mainly divided into medical and dental history recording, clinical examination (extra-oral and intra-oral), and radiographic examination.8 Once common clinical diagnostic tests such as observation of both hard and soft tissues, palpation, percussion, periodontal examination, occlusal analysis, caries diagnosis, and testing for possible cracked or fractured teeth have been performed, a radiographic examination should be conducted. There are two levels of radiologic examination: the traditional two-dimensional (2D) radiography, represented by intraoral (bite-wing, periapical, etc.) and panoramic radiographs, and the three-dimensional (3D) radiography, represented by CBCT imaging. The main limitation of 2D imaging undoubtedly arises from the compression of a three-dimensional object in a 2D image, resulting in a superimposition of anatomical structures that could hide relevant elements useful for the diagnostic process.36 However, despite the greater anatomical information provided, 3D imaging subjects patients to higher doses of ionizing radiation. Nevertheless, the results of this diagnostic process directly influence treatment planning, clinical decisions, and thus, the outcome of RCRts, therefore, the selection of the proper imaging examination mode is crucial.37,38 Bhatt et al recently (2021) investigated the impact of CBCT on clinical decision-making and initial diagnosis in comparison to conventional radiographs regarding endodontic treatments, concluding that the additional information obtained from CBCT images resulted in the modification of the initial diagnoses, and, thus, the treatment plans, respectively, in 59 of 96 RCRts cases (61%) and in 64 of 96 RCRts cases (66%).39 Another similar study by Ee et al drew a similar conclusion, stating that the implementation of the radiographic examination with CBCT scans led to treatment plan modifications in approximately 62% of the cases.38
As reviewed by Venskutonis et al, 3D imaging is a valid tool in the management of endodontic cases.36 First of all, thanks to the three orthogonal planes visualization of the anatomy without superimposition of anatomical structures, CBCT guarantees a detailed assessment of the root canal system, providing useful information regarding missed anatomy of previous endodontic treatments, root canal configuration, and morphology, presence of confluences, interpretation of curvatures in a 3-dimensional view, and unusual anatomy such as dens in dente, dilacerated teeth, and so on.36 Moreover, it has been demonstrated that the CBCT is able to evidence periapical radiolucency more sensitively than bidimensional radiographs, with an increment of 50–70%.36,40 Additionally, the accuracy of CBCT in root fracture diagnosis has been investigated and compared to periapical radiographs. Results are conflicting since some studies have evidenced that CBCT is more accurate than periapical radiographs in detecting root fractures, whilst other studies have found opposite results or no statistically significant differences.41–44 Despite this, it is clear that the diagnostic quality of CBCT scans is thoroughly influenced by several technical factors such as field of view (FOV), region of interest (ROI), voxel size, tube current (milliamperage (mA)), exposure time, and kilovoltage. Moreover, the presence of high-density materials, if not properly managed with a determined acquisition setting, could generate the formation of beam-hardening artifacts that jeopardize the quality and accuracy of CBCT imaging, particularly during the diagnosis of root fractures.45 In light of the above, de Lima et al with a systematic review of the literature stated that smaller voxels (respectively, 0.08 mm and 0.1 mm voxels) and FOV sizes seem to provide more accurate vertical root fracture detection values when using CBCT.46 Moreover, use of the metal artifact reduction (MAR) tool has been suggested to increase as much as possible the diagnostic accuracy in the detection of vertical root fracture; however, a recent systematic review (2021) concluded that better results in terms of root fracture detection were found when the MAR software was deactivated, although a low level of evidence and high heterogeneity was observed.47
Two other clinical scenarios in which CBCT is able to provide a more accurate, sensitive, and specific diagnosis are external and internal resorptions and perforations. CBCT imaging is able to determine the spatial orientation of the defects, giving clinicians the exact size and position of the lesion and providing crucial information for treatment planning and prognosis.36
In conclusion, taking into consideration the scientific data, CBCT could be considered the first choice for endodontic retreatment planning, since it provides crucial information that could thoroughly affect the diagnosis. Obviously, the indiscriminate prescription of CBCT is strongly discouraged, and low-dose acquisitions are recommended. The emitted ionizing radiations should be maintained as low as possible, selecting the proper FOV, voxel size, and ROI, coherently with the anatomical area under investigation. Readers are strongly encouraged to consider the guidelines stipulated by scientific societies.25,26
Clinical Procedures
This section will discuss all intra-operative phases of root canal retreatments from the initial coronal disassembling to the obturation of the root canal system, describing the challenges and consequent solutions proposed in the literature.
Coronal Disassembly
The initial operative step during secondary root canal treatment aims to remove any manufacts or materials placed in the post-space and/or coronally to the endodontium. The majority of the teeth that require RCRts have been previously restored with dental prostheses and sometimes posts. For this reason, in order to obtain optimum access to the root canal system, it is strongly recommended to remove all restorative materials from the pulp chamber and crown to promote the localization of root canal orifices. Despite this, sometimes clinicians are required to not completely remove coronal restoration so as not to compromise the whole prosthodontics rehabilitation. In those cases, access to the endodontium is performed through restorative material, but the clinician must be sure that the existing post-endodontic restoration is functional, well-fitting without any leakage or secondary decay, and esthetically pleasing, taking into consideration the increased difficulties in the following step of RCRts (Figure 2). If the above-mentioned requirements are not accomplished, the removal of the restorative materials is strongly suggested to preserve the long-term outcome of RCRts.
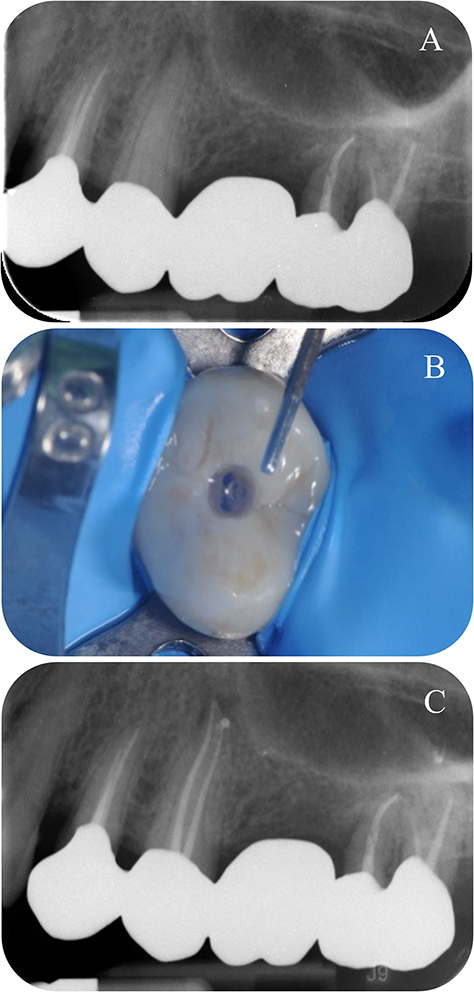 |
Figure 2 Clinical example in which the root canal treatment was performed without coronal disassembling. Notes: (A) pre-operative periapical radiograph showing periapical radiolucency affecting the upper left second premolar. (B) Conservative access cavity performed through a metal-free crown. (C) Post-operative periapical radiograph. |
One of the most challenging aspects during coronal disassembling is the posts removal. They can be cataloged according to their morphology into parallel and tapered, or accordingly to their material and retention mechanism into metallic or non-metallic (fiber post) and active or non-active. The removal of active/screwed posts is performed by removing the core material around the post without damaging it and by ultrasonically mobilizing it with circumferential CCW motion of the ultrasonic tip, taking care of cooling the substrates to avoid periodontal damage due to heat.48,49 In the case of prefabricated or cast cemented posts associated with a composite or metal core, the procedures are similar to those described above. When a composite core is present, it should be carefully removed with a bur without damaging the post, then the latter is removed by vibration with dedicated ultrasonic tips and water coolant, in order to promote cement/bond failure (Figure 3).
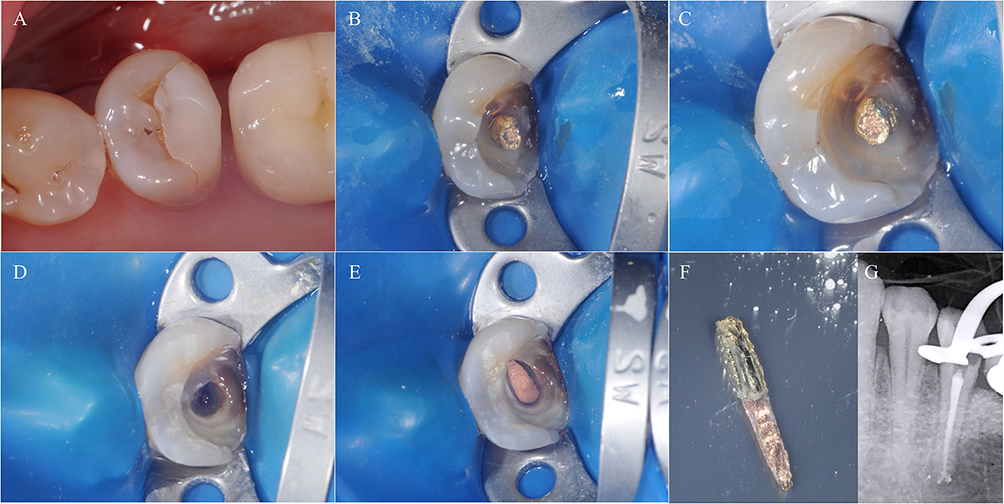 |
Figure 3 Clinical example of prefabricated metal post removal associated with a composite core. Notes: (A) Initial intraoral situation of left lower second premolar, in which a marginal leakage of post-endodontic composite restoration is evidenced. (B) Removal of composite core and isolation of the metal post. (C) Higher magnification of image B. (D) Endodontic system after the metal post removal, a composite remnant can be noted on the buccal aspect of the canal orifice. (E) Obturation of the root canal system. (F) The removed metal post. (G) Post-operative radiograph showing the obturation of the root canal system before post-endodontic restoration. |
However, fiber posts are usually disintegrated with burs, dedicated drills, or ultrasonic tips, since their removal is prevented by the adhesive materials used for their cementation inside canals. During the disintegration phases, maintaining the tip centered in the fiber post is crucial in order to prevent perforation and excessive removal of sound dentin. To facilitate those procedures, the creation of a pilot hole in the center of the post is strongly recommended as well as the use of magnification with an adequate source of light (Figures 4–5).
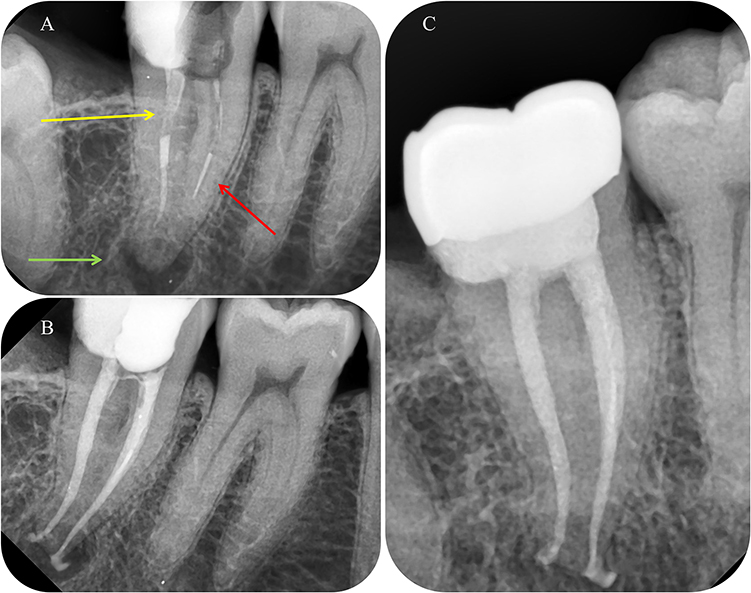 |
Figure 4 Clinical example of RCRt with several problems: fiber post in the distal root (yellow arrow), instrument fragment in the mesio-buccal canal (red arrow), apical part of the endodontic system non-instrumented and obturated, chronic periapical lesion (green arrow). Notes: (A) Pre-operative periapical radiograph. (B) Post-endodontic periapical radiograph after fiber post removal and instrument fragment bypassing. (C) 1-year follow-up showing the healing of the periapical tissues. |
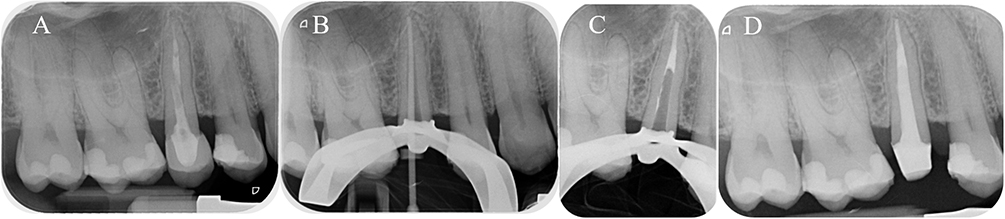 |
Figure 5 Clinical example of RCRt with fiber post removal. Notes: (A) Pre-operative periapical radiograph showing the presence of a fiber post and a not satisfactory root canal filling. (B) intra-operative radiograph showing radiographic working length confirmation. (C) Intra-operative radiograph after the warm vertical obturation. (D) Post-operative periapical radiograph after fiber post insertion and build-up. |
Although ultrasonic vibration and degradation is the most common method for posts removal as stated by Castrisos and Abbott, several methods have been proposed over the years such as the Eggler post-removal kit, Masserann kit, Auto Abdicator system, Gonon and Ruddle post-removal systems, and DT Post Removal Kit.50,51 Moreover, some authors proposed innovative techniques for post removal by using a static guide in order to reduce as much as possible the iatrogenic error and sound dentine removal.52,53
In addition to the possible iatrogenic errors during posts removal and the above-mentioned possibility of heating the periodontal ligament, if a cooling action is not performed, three other drawbacks should be considered during posts removal: tooth volume changes, residual material left in the canal, and dentinal microcrack formation. Depending on the posts removal technique selected, data in the literature showed mean volumes of residual material left in the canal between 1.1 ± 6.8 and 3.3 ± 4.0 mm3, with the lowest values associated with ultrasonic disintegration of posts.54,55 This is because ultrasonic tips are more tapered and, thus, less conservative than burs present in the posts removal kits, resulting in a higher removal of sound dentine. Haupt et al in a laboratory study using Micro-CT found that ultrasonic degradation and carbide drill or round bur degradation resulted in dentinal microcracks formation after post removal, independently from the amount of dentin removed.51 Nevertheless, Abbott and Aydemir et al stated that posts removal should be considered a predictable and safe procedure if appropriate techniques and devices are used, with a low rate of tooth fracture.56,57
In conclusion, in RCRts where a post is present, considering the high percentage of successful post removal and the correlated low risk of root fracture, non-surgical orthograde retreatments should be preferred to surgical retreatments. Despite this, further research is needed to indicate which posts removal technique is superior in terms of sound dentine removal, required time, predictability, dentinal microcracks formation, and root fracture.
Orifice Location and Missed Anatomy
The etiopathogenesis of endodontic infections is bacterial; thus, the removal of bacteria and their byproducts from the root canal system through adequate chemo-mechanical disinfection is crucial for a long-term successful outcome.2,58 As stated by Ricucci, persistent intraradicular bacteria should be considered as the primary cause of post-treatment diseases and the reason why RCRts are required.2 For the above-mentioned reasons, missed anatomy is one of the most common causes of primary endodontic treatment failures.59,60 Mashyakhy et al found that the frequency of apical periodontitis in root canal-treated teeth with missed canals was about 90%, whilst Baruwa et al found a frequency of 82.6% and Costa et al 98%.61–63 Therefore, one of the aims of RCRts is to find and treat the missed anatomy. According to data in the literature, the missed canals involve mainly the first maxillary molars, especially the mesio-buccal 2 (MB2) canal (Figure 6), followed by the first mandibular molars, especially the second canal in the distal roots.60,64,65 Moreover, an additional mesial canal, the middle mesial canal, in lower molars is frequently found with a percentage ranging from 0.26% to 53.8%.66–68 Martins et al reported that the overall prevalence of a second canal in the lower central and lateral incisors and canines was 20.4%, 25.3%, and 5.9%, respectively, with the actual percentage strictly related to the population ethnicity as described by Dhuldhoya et al (Figure 7)69,70 Other two scenarios that should be taken into consideration are the prevalence of accessory canals in upper and lower premolars and C-shaped canals in lower molars. According to this, Karobari et al in a recently published systematic review found a prevalence of accessory canals in lower premolars ranging from about 2% to 60%, accordingly to the population ethnicity, while Martins et al observed a prevalence of C-shaped configuration of 0.3% (0.1–0.6%) for mandibular first molars, and 12% (10.3–13.7%) for mandibular second molars.71–73
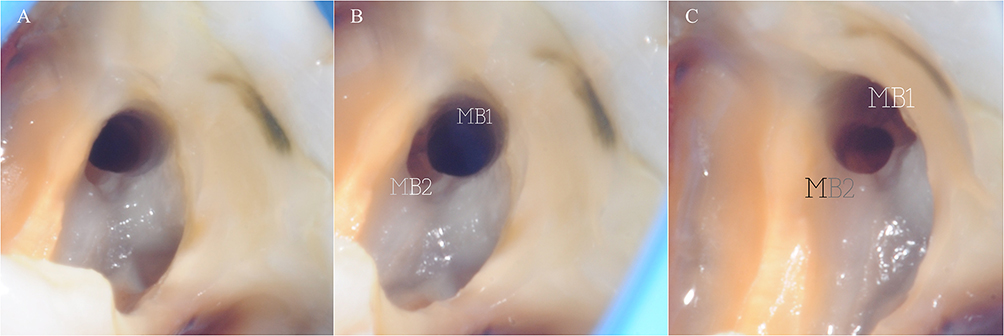 |
Figure 6 Intra-operative photos showing a particular anatomy of the mesio-buccal system of an upper first molar with different angulations. Notes: The mesio-buccal 1 (MB1) and mesio-buccal 2 (MB2) canals start from the same orifice and a few millimeters below, the MB2 diverges from the MB1 in a mesio-palatal direction. (A) MB2 location before orifice opening. (B) MB2 location after orifice opening. (C) Different angulations showing the MB2 orifice. |
 |
Figure 7 RCRt case of a central lower incisor characterized by three different orifices and three canals with a single port of exit. Notes: (A) Pre-operative CBCT image showing the missed anatomy and a periapical chronic lesion. (B) intraoral photo of the access cavity showing three different orifices. (C) CBCT scan after 2 years of follow-up showing the healing of the periapical lesion. |
According to this anatomical variability in the root canal morphologies and configurations, several suggestions have been raised by authors to properly detect and treat accessory canals. First of all, a correct visualization of the root canal anatomy is fundamental, and to gain this at least two different periapical radiographs with different angulations should be performed. However, even this approach, as mentioned before, does not allow a full understanding of the three-dimensional anatomy, so CBCT is suggested.26 Moreover, high magnification devices such as loops and operative microscopes increase visibility, enhancing the identification process of accessory canals.74 In addition to magnification devices, several articles described the importance of ultrasonic tips, resulting in an increased quality of operative procedures during RCTs and RCRts.75
In conclusion, due to the high variability of root canal anatomy according to each ethnicity, further research with international sample populations is needed to assess the actual probability of the presence of accessory anatomy. However, from a clinical point of view, the use of magnification devices, ultrasonic instruments, and an in-depth interpretation of radiographic images with both 2D and 3D images are strongly recommended.
Removal of Previous Root Filling Materials
Removal of previous root filling materials from the root canal system is a crucial step to guarantee adequate chemo-mechanical disinfection and obturation and solve the cause of primary endodontic treatment failure.76 Gutta-percha is undoubtedly the most used filling material in combination with sealers or cements of variable chemical composition, and it is used with several obturation techniques that could be mostly divided into “cold” and “hot” techniques. The latter provides a three-dimensional condensation/compaction of gutta-percha in the root canal system, resulting in a challenging removal when RCRts are required. For this reason, several solvents have been proposed to soften the obturation materials, such as chloroform, eucalyptus oil, xylene/xylol, methyl chloroform, tetrahydrofuran, methylene chloride, halothane or rectified turpentine.77 However, some concerns have been raised regarding their cytotoxicity and the amount of filling material remnants in root canals. Horvath et al demonstrated that the use of solvent in RCRts resulted in more gutta-percha and sealer remnants on root canal walls and inside dentinal tubules that could potentially compromise the following chemo-mechanical disinfection and obturation procedures, jeopardizing the RCRts outcome.78 However, the literature is still lacking on this topic; thus, further research is strongly needed. Besides the chemical dissolution of root filling materials, mechanical removal is still the most widespread technique.76 Several instruments have been proposed for this aim, both manual and engine-driven NiTi instruments. Due to the enhanced mechanical and metallurgical properties of NiTi instruments in comparison to stainless-steel manual files, the removal of previous root filling materials is more effective, and efficient, and requires less operative time, resulting in fewer remnants in the root canal system.76,77 Despite this, the main risks of using NiTi instrument for the removal of filling materials are the instrument fracture and iatrogenic errors such as ledge, stripping, false channel formation, and perforation, especially with the retreatment instrument with an active tip. Two other additional techniques have been proposed for root filling materials removal, the ultrasonic devices and lasers.76 The first one can be used during the initial phases of filling materials removal to soften the gutta-percha by frictional heating, facilitating its removal. However, it is a useful tool to disrupt hard filling materials such as MTA and hydraulic sealer or to remove gutta-percha and sealer remnants from the canal walls, since the traditional techniques are not able to fully remove them.79–81 Er:YAG laser irradiation has been proposed as a root filling materials removal technique, but with contradictory results. Tachinami et al found out positive results in laser removal of filling materials, whilst Gorduysus et al demonstrated that Er:YAG laser beam is not so efficient when compared to ultrasonic devices and, moreover, found out thermal side effects and burning damages on the root canal dentinal walls.82,83 Also, regarding this topic, further clinical and ex-vivo studies are needed to have an in-depth understanding on the theme.
In addition to the main filling material removal techniques, some supplementary protocols have been proposed to enhance the cleaning and disinfection processes, such as sonic agitation, passive ultrasonic or laser activation, multisonic activation and additional root canal nstrumentationwith XP endo or Self-Adjusting file.77 Baumeier et al concluded that additional cleaning protocols enabled removing a greater amount of root canal filling materials without any statistically significant difference between passive ultrasonic irrigation, sonic agitation, and XP-endo Finisher R instrumentation.84 Several articles found consistent results, concluding that additional protocols are strongly recommended for filling materials removal.85–87 Nevertheless, the actual influence of these procedures on the RCRts outcome and which additional protocol results in a better cleaning is still unclear; therefore, further clinical research is needed.
Perforation
Root perforation can be due to both pathological and iatrogenic causes and it has been defined as a condition in which there is communication between the root canal system and the outer surface of the roots. Pathological perforations are a result of resorptive processes and caries, whilst iatrogenic perforations arise from complications during or after root canal treatment.88 The diagnostic process consists of a multistep procedure that comprises clinical examination (bleeding from the perforation and pain), use of an apex locator that in case of perforation shows values as if the file is beyond the apical foramina, periodontal examination since it can affect the prognosis, and radiographic examination (both 2D and 3D imaging).89–92
The prognosis of perforation repair is strictly related to several factors: early diagnosis; location; and crestal root perforation are more susceptible to epithelium migration that worsens the prognosis; nature of the perforation; material used for the repair; chosen treatment; periodontal conditions; operator experience and available devices such as an operating microscope.93–95 Since the introduction of MTA and hydraulic root repair materials as the materials of choice for perforation repair, the size of the perforation is no longer considered a factor able to affect the treatment outcome.88,92,94 Over the years, several perforation repair materials have been proposed such as amalgam, zinc oxide-eugenol sealer, calcium hydroxide, glass ionomer cement, composite resin, and SuperEBA (Keystone Industries), but none of them have shown performances comparable to the MTA ones. The properties that make the MTA the eligible material for perforation repair can be attributed to its ability in guaranteeing a favorable environment that provides the re-establishment of the physiological tissue architecture while maintaining the endodontium and periodontium separation.96,97 In the last decade, a new generation of bioactive endodontic cement has been introduced and of which the MTA is the predecessor. Despite the first promising results, long-term data are still scarce and further research is needed.88
Nevertheless, alternative materials for perforation repair in some specific situations have been described in the literature. According to this, MTA has some limitations such as the prolonged setting time up to 3h with the risk of being washed out, especially in the cases where there is a communication between the perforation site and oral environment. For this reason, some authors proposed alternative materials such as other bioactive endodontic cements, resin-bonded glass-ionomers, or composites.88 Moreover, another limitation of MTA is linked to its potential to cause tooth discoloration, compromising the aesthetic result of treatments especially in the anterior zone. In order to overcome this limitation, other bioactive endodontic cements should be taken into consideration and in case of perforations above the crestal bone, the application of dedicated adhesive materials can guarantee an adequate seal, aesthetic, and fast setting time.88
The clinical management of perforations strongly depends on their location and accessibility. Based on this, two different approaches are evidenced: non-surgical and surgical.88 However, since the surgical approach is out of the scope of this review, it will be no longer addressed, and the attention will be focused on the clinical procedure of non-surgical management of perforations. As mentioned before, the clinical approach is different according to the location of the perforation. The perforations located on the crown, furcation, or pulp floor are managed by isolating the involved tooth and debriding the defect. However, if the perforation does not bleed, and the instrumentation, irrigation, and obturation of the root canal system can be performed without any complication, the clinician should fill the root canals and then treat the perforation. The debridement procedure of the defect is strongly related to the lapse of time between the repair and the moment at which the perforation has been made. Old and chronic perforations have greater chances to enclose infected and granulomatous tissues, which must be removed before inserting the repair material. This goal is achieved by the use of ultrasonic tips, burs, and manual excavators. Despite this, once the lesion has been removed, there is the possibility of profuse bleeding, with difficult hemostasis, which is essential to avoid an early washout of the repair material.98 In case of challenging hemostasis, the use of epinephrine pellets, collagen, calcium sulphate, or calcium hydroxide is strongly recommended rather than nonspecific intravascular clotting agents such as ferric sulphate, because they can damage the alveolar bone.88,99 Once the infected tissues have been removed and hemostasis obtained, the underlying bone defect size should be evaluated. In the case of wide and deep defects, the positioning of matrixes as a barrier is suggested to avoid extrusion of the material beyond the external tooth surface. The application of MTA or other repair materials is performed with dedicated devices (eg, MAP–Micro Apical Placement System, Produits Dentaires SA; Dovgan MTA Carrier, G. Hartzell & Son) or pluggers, and slightly compacted with sterile paper point. After the MTA placement, a wet cotton pellet is placed over the MTA to allow its setting and a temporary restoration is performed. The new generation of root repair materials requires a few tens of minutes to complete the setting; therefore, intermediate medication is not required, and a definitive restoration could be performed, increasing the strength of the endodontically treated teeth. On the other hand, middle root perforations are more difficult to treat because of the reduced visibility. The procedural steps include the control of the bleeding, the placement of a space maintainer inside the root canal to maintain the apical patency without obstructing the canal with the repair material, the positioning of the repair material, and the definitive obturation of the root canal system. In those cases, one of the major difficulties is to decide if to treat the perforation before the root canal obturation or vice versa. Since there are no scientific data on this point, the decision is left to the clinicians, to their expertise, and the specific case.
Ledges
A ledge is defined as an iatrogenic irregularity created in the root canal that could comprise the access of instruments and irrigants apically to it, decreasing the chemo-mechanical disinfection of the root canal system.100 As stated by several authors, ledging of root canals reduces the success rate of endodontic treatments and it can be considered as one of the causes of RCRts requirement.100–102 Ledge formation can be caused by several factors: incorrect access cavity; misinterpretation of endodontic anatomy, especially in case of curvatures (in this case the ledge is located in the opposite direction to the three-dimensional canal curvature);103 incorrect working length (WL) determination; incorrect use of stainless-steel manual files, which have an active tip (ie use of no pre-bent instrument in severe curvatures or excessive inward force with a file of high diameter); incorrect use of rotary or reciprocating instruments; the attempt of negotiation of the calcified canal; the attempt of removal of separated instruments; incorrect post-space preparation.100 The recognition of a ledge can be performed both clinically and radiographically. From a clinical point of view, the endodontic instrument is no longer able to reach the WL because it impacts the ledge. The clinicians in this case feel that the instrument is hitting a solid wall. Radiographically, a ledge can be recognized by taking one or two periapical radiographs with different angulations with an endodontic instrument inserted at the point of non-progression. If the file deviates from the canal axis, it means that there is a ledge.
Accordingly, one of the crucial steps during RCRts is the ledge bypassing to achieve patency at the canal terminus.6 In the literature, several techniques have been proposed to manage ledges with both manual and rotary/reciprocating instruments. First of all, the pre-enlargement of the canal portion coronal to the ledge is strongly recommended to remove any coronal interferences that could alter the tactile sensation during the ledge bypassing. After that, a small K-file (#6, 8, or #10) should be pre-curved and carefully moved inside the canal until the ledge is reached. At this point, the K-file is progressively and circumferentially rotated with slight up and down movements of 0.5 mm until the clinician feels the apical progression of the file. Without removing the K-file, taking an intra-operative radiograph is suggested to verify the right progression of the file. Without removing the K-file coronally to the ledge, a circumferential filing should be performed in order to reduce the ledge. These phases should be repeated by increasing the tip diameter of the K-file until there is an easy progression to the WL.104 Those procedural steps could be performed using nickel–titanium (NiTi) instruments instead of stainless-steel manual files. The main advantage of NiTi instruments consists of their increased taper and the possibility to rotate them at higher speeds, resulting in more effective management.105 Despite this, not all NiTi instruments can be used for this purpose because of their metallurgical properties. The conditio sine qua non for their use is the martensitic crystallographic phase at the intracanal temperature, which allows them to be pre-bendable.106 Once the small NiTi instrument is pre-curved, the ledge is bypassed by manually inserting the NiTi rotary instrument and then rotated with an endodontic motor with up and down movements of 1mm of amplitude apically to the ledge.105 Nevertheless, there are some alternatives to the above-mentioned techniques. Ünlü et al compared the effectiveness of a recently introduced NiTi instrument characterized by a bent tip with K-file in bypassing ledges, concluding that Fanta AF™ Ledge Correction instruments had higher performances in terms of centering ability, shaping ability and effectiveness.105 Another tip is to induce martensitic crystallographic transformation of austenitic instruments by cooling their tip with the conventional cold pulp testing spry, so as to be pre-bendable and use them as described above. However, there are no articles in the literature describing this technique.
In conclusion, the presence of ledges does not intrinsically reduce the success rate of RCRts if properly managed, not affecting the overall prognosis. Despite this, further research is required to assess the safest and most effective, in terms of intraoperative time, centering ability, shaping ability, and canal transportation.
Instrument Fragments
The main causes of intracanal separation of NiTi rotary and reciprocating instruments are cyclic fatigue and the excessive torsional load or the combination of the two mentioned factors.106–109 Despite the presence of an instrument fragment in the root canal system is not intrinsically a factor able to affect the outcome of endodontic treatments, if not properly managed, it can jeopardize chemo-mechanical disinfection and obturation procedures, compromising the eradication of vital and/or infected tissues.110,111 According to the literature, the incidence of intracanal separation ranges from approximately 0.2% to 25%, with a decreasing trend over the years probably due to innovations in terms of design, metallurgy, and kinematics.112–117 Moreover, considering the root canal thirds and the prevalence of instrument separation, the highest percentage has been found in the apical third (52.5%–71.43%), followed by the middle third (27.5%–28.57%) and coronal third (0%–12.5%).114,118
In the management of an instrument fragment, there are two treatment options: bypass or retrieve it, not considering the possibility of cleaning/shaping and filling the root canal to the level of the fragment.119 As stated by Madarati et al, fragment removal should be considered the goal standard in the management of instrument fragments.119 However, the risks/benefits of this procedure should be carefully analyzed, considering the preservation of the tooth integrity. Sometimes, fragment removal could cause excessive and detrimental dentinal removal, compromising the tooth’s mechanical resistance. In these situations, bypassing the fragment can be taken into consideration to guarantee optimal chemo-mechanical disinfection and obturation of the root canal system.120 Despite this, even bypassing procedures have some limitations and risks such as ledge formation, false channel formation, perforation, secondary separation of instruments, pushing the fragment apically, and complete fragment extrusion.119 Neverthelessto date, no clinical studies have been comparing the success rate of these two treatment options for the management of instrument fragments.
Several studies have been conducted to investigate the factors affecting instrument retrieval. Terauchi et al have synthesized them in:
- Clinician’s armamentarium (operating microscope, ultrasonic tips, and knowledge of instrument retrieval protocols).120,121
- Tooth type: instrument retrieval from the root canal system of posterior teeth is more challenging than anterior teeth due to the more complex anatomy in terms of curvature, confluence, reduced visibility, and limited mouth opening, resulting in a lower success rate.120
- Types of instrument fractures: considering the crystallographic phase of NiTi instruments, the retrieval of austenitic instrument fragments is more difficult than the retrieval of martensitic or stainless-steel fragments, because the austenite tends to straighten out on the outer curvature wall, resulting in a longer time for creating the adequate space around the instrument fragment for its retrieval and a higher dentinal removal.122,123
- Length and size of the fractured instrument: longer fragments require more retrieval times. Fu et al stated that for each 1-mm increase in the fragment length, the retrieval time approximately increases by 80s.121 Moreover, the fragment size also positively affects the preparation time for loosening the fractured instruments, with a higher amount of dentinal removal.124
- Location of the fractured instrument: the more the fragment is apical to the curvature, the more the success rate decreases.
- Root canal curvature: the retrieval success rate is positively and negatively affected by the canal radius and curvature degrees, respectively, due to increased visibility and accessibility.124
- Operator fatigue and experience: expert clinicians predictably remove fractured instruments in less operative time, with greater preservation of dentine and fewer iatrogenic accidents.125
The retrieval techniques can be divided into three main groups: mechanical, chemical, and surgical retrieval. Since the literature is clear regarding the most effective and predictable techniques, chemical and surgical retrieval methods will no longer be discussed.119 Mechanical protocols for fragment removal strictly depend on the canal anatomy at the point of fracture, since it thoroughly influences the visibility and accessibility of the fragment. However, as mentioned before, also the instrument fragment characteristics such as length and size should be considered to select the proper technique. Generally, all techniques comprise two phases: the first one (preparation phase) aims to loosen the fragment by creating a wider coronal space with rotary or ultrasonic instruments, while the second one (retrieval phase) consists of the retrieval process with a dedicated device or ultrasonic tips (Table 3). In literature, different retrieval techniques have been described.
- Instrument retrieval with ultrasonics:
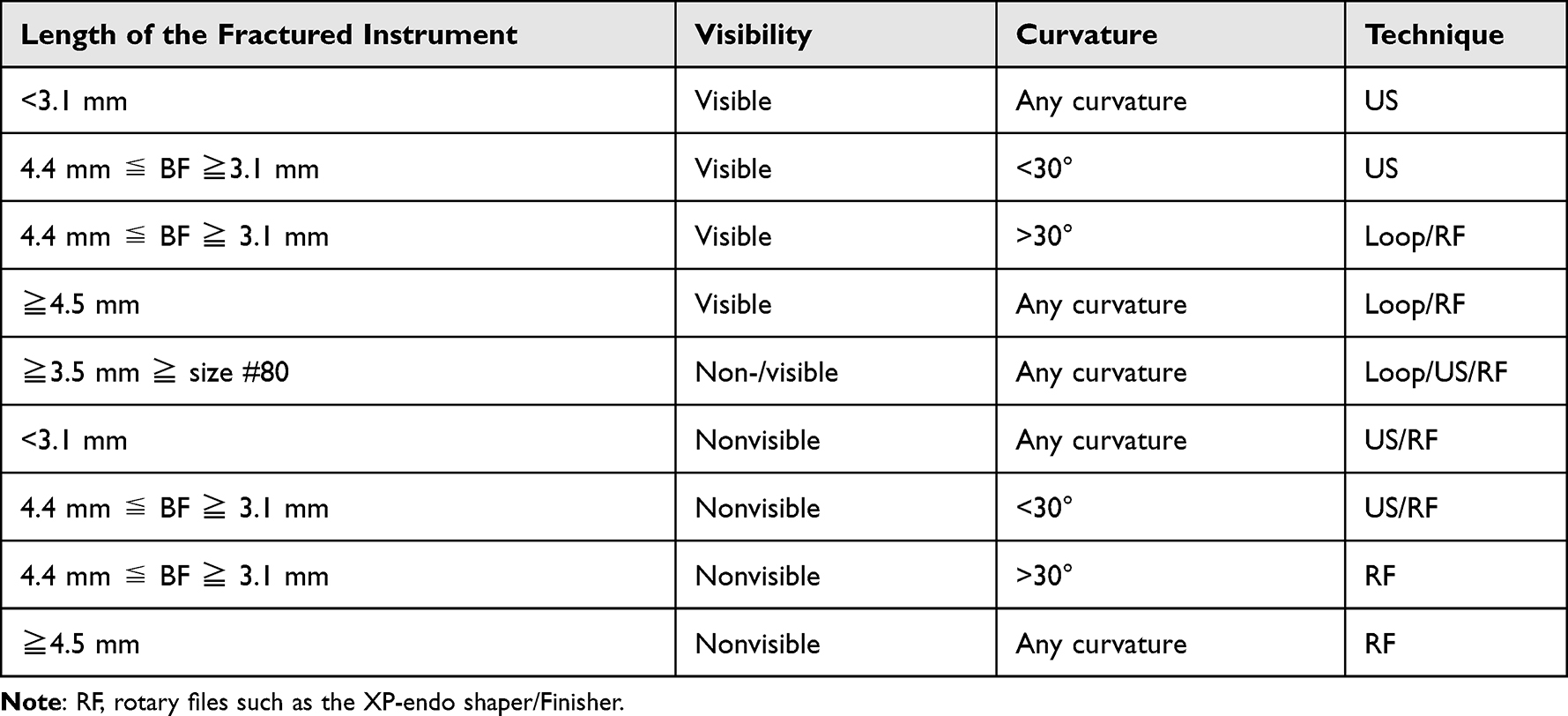 |
Table 3 Summary of Recommended Instrument Retrieval Techniques Accordingly to the Fragment Length. (US) Ultrasonics |
Once the preparation phase has been completed and the top of the instrument is completely disengaged, the canal should be dried with dedicated devices in order to facilitate the fragment loosening thanks to the blown air. After that, the retrieval procedure could be performed in a wet environment depending on the canal curvature. Some authors suggested soybean oil or EDTA in case of >30° or <30° of curvature, respectively.117 Once the canal and the access cavity space are completely filled with liquid, the ultrasonic tip should be positioned in the inner part of the curvature in direct contact with the most accessible apical part of the fragment and activated at a power 10–20% higher than the one set for the preparation phase. According to Terauchi et al, with short up-and-down strokes being performed on the inner curve, the fragment is usually removable in 10s.124
- Instrument retrieval with loop system:
Unlike other retrieval techniques, the loop system one should be performed in dry conditions since each step requires clear visibility. First of all, the preparation phase should guarantee a peripheral space >0.4 mm in terms of diameter, and >0.7 mm in terms of depth. Once the vertical and horizontal spaces have been prepared, the preparation can be checked by the insertion of a #40 plugger. After that, the loop should be inserted with an angle of 45° into the canal and then placed over the fractured instrument and tightened around it. Once the fragment is secured, the loop should be retrieved by moving it in several directions.117
- Instrument retrieval with XP-Endo Finisher (FKG Dentaire):
This technique is based on the particular morphology of the XP-Endo Finisher, characterized by a spoon shape once it is exposed to intracanal temperature following transformation to the austenitic phase.126 Rotating it in a high-speed clockwise direction, it is able to remove a loosened fragment from a wider canal by braiding it and creating a swirling fluid flow in the coronal direction, especially in cases in which the fractured instrument is extruded beyond the apex.117
Medicaments and Irrigation Technique
Medicament and irrigation technique in endodontic retreatments are two of the most controversial topics in the field. The use and efficacy of medicament and the number of appointments to perform root canal retreatments are still controversial and the lack of evidence suggests the need for further research. For example, Yoldas et al evaluated the post-operative pain in orthograde retreatment cases completed in a single visit or two visits with the use of intracanal medication with calcium hydroxide (Ca(OH)2). The authors found that the two-visit retreatment with intracanal medication with Ca(OH)2 was more effective in reducing postoperative pain, also decreasing the number of flare-ups in all retreatment cases.127 However, other authors stated that the use of intracanal medicaments does not influence the occurrence of postoperative pain and that the two-visit retreatment could compromise the mechanical strength of the endodontically treated tooth if the temporary filling is not properly managed, without any potential benefits.128–130
Regarding irrigation techniques and protocols during orthograde retreatments, the literature does not evidence any difference from procedures and materials suggested for orthograde treatments. The most common irrigants are represented by EDTA and NaOCl, respectively, at 17% and 3–6%. However, some authors investigated the effectiveness of chlorhexidine gluconate (CHX) as a final irrigant in treatment and retreatment cases. One of the main points raised in favor of CHX is its substantivity that should endure a prolonged effect in terms of antimicrobial activity, preventing bacterial recolonization.131 Despite this, it was demonstrated that CHX substantivity in root canal system has been investigated under rather unrealistic conditions, undermining the clinical significance of those studies.132 In conclusion, the use of CHX is not supported by scientific evidence, and further studies are required to clarify this point.133
Moreover, several studies suggest the use of agitation or activation devices to increase the effectiveness of intracanal irrigation such as sonic agitation, ultrasonic activation, laser activation, and multisonic activation. Although in vitro, laboratory, and ex vivo studies have shown promising results in terms of increased antimicrobial activity and diffusion of irrigants, the number of randomized clinical trials on this topic is still scarce and actual evidence on their clinical significance is dubious. Despite this, since endodontic diseases are based on bacterial infection, any procedure that could increase the antimicrobial activity of irrigants without causing adverse effects is strongly recommended.133 However, based on the available data and clinical experience, freshly NaOCl and EDTA delivered by a syringe and needle and ultrasonically activated in several cycles (20 s each for 1 min for each irrigant) during the final rinse, remain the keystone of root canal irrigation protocols.133
Conclusion
Non-surgical endodontic retreatment should be considered the first treatment option in most cases of endodontic post-treatment diseases. The success rate is high and comparable to other surgical treatments; however, the diagnostic process is crucial to assess the outcome affecting factors that could compromise the therapy. In the literature, several techniques have been described for each situation (ledge, perforation, instrument fragment management, etc.) and they all represent valid treatment options. Obviously, with the development of innovative techniques and materials, the success rate will exponentially increase. Researchers are asked to focus their attention on long-term clinical trials to assess and compare different techniques and/or materials.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Meirinhos J, Martins JNR, Pereira B, et al. Prevalence of apical periodontitis and its association with previous root canal treatment, root canal filling length and type of coronal restoration – a cross-sectional study. Int Endod J. 2020;53(4):573–584. doi:10.1111/iej.13256
2. Ricucci D, Siqueira JF Jr, Bate AL, Pitt Ford TR. Histologic investigation of root canal-treated teeth with apical periodontitis: a retrospective study from twenty-four patients. J Endod. 2009;35(4):493–502. doi:10.1016/j.joen.2008.12.014
3. Sayed ME, Jurado CA, Tsujimoto A, Garcia-Cortes JO. Clinical decision-making regarding endodontic therapy vs extraction and implant-assisted replacement: a systematic review and meta-analysis. Gen Dent. 2021;69(1):52–57.
4. Azim AA, Griggs JA, Huang GT. The Tennessee study: factors affecting treatment outcome and healing time following nonsurgical root canal treatment. Int Endod J. 2016;49(1):6–16. doi:10.1111/iej.12429
5. Ng YL, Mann V, Gulabivala K. A prospective study of the factors affecting outcomes of non-surgical root canal treatment: part 2: tooth survival. Int Endod J. 2011;44(7):610–625. doi:10.1111/j.1365-2591.2011.01873.x
6. Ng YL, Mann V, Gulabivala K. A prospective study of the factors affecting outcomes of nonsurgical root canal treatment: part 1: periapical health. Int Endod J. 2011;44(7):583–609. doi:10.1111/j.1365-2591.2011.01872.x
7. Segura-Egea JJ, Cabanillas-Balsera D, Martín-González J, Cintra LTA. Impact of systemic health on treatment outcomes in endodontics. Int Endod J. 2023;56(S2):219–235. doi:10.1111/iej.13789
8. Endodontology ESo. Quality guidelines for endodontic treatment: consensus report of the European Society of Endodontology. Int Endod J. 2006;39(12):921–930. doi:10.1111/j.1365-2591.2006.01180.x
9. Messer HH, Yu VS. Terminology of endodontic outcomes. Int Endod J. 2013;46(3):289–291. doi:10.1111/iej.12014
10. Friedman S, Mor C. The success of endodontic therapy--healing and functionality. J Calif Dent Assoc. 2004;32(6):493–503.
11. Bystrom A, Happonen RP, Sjogren U, Sundqvist G. Healing of periapical lesions of pulpless teeth after endodontic treatment with controlled asepsis. Endod Dent Traumatol. 1987;3(2):58–63. doi:10.1111/j.1600-9657.1987.tb00543.x
12. Van Nieuwenhuysen JP, Aouar M, D’Hoore W. Retreatment or radiographic monitoring in endodontics. Int Endod J. 1994;27(2):75–81. doi:10.1111/j.1365-2591.1994.tb00234.x
13. Yu VS, Messer HH, Yee R, Shen L. Incidence and impact of painful exacerbations in a cohort with post-treatment persistent endodontic lesions. J Endod. 2012;38(1):41–46. doi:10.1016/j.joen.2011.10.006
14. Ng YL, Mann V, Gulabivala K. Outcome of secondary root canal treatment: a systematic review of the literature. Int Endod J. 2008;41(12):1026–1046. doi:10.1111/j.1365-2591.2008.01484.x
15. Ng YL, Mann V, Rahbaran S, Lewsey J, Gulabivala K. Outcome of primary root canal treatment: systematic review of the literature -- Part 2. Influence of clinical factors. Int Endod J. 2008;41(1):6–31. doi:10.1111/j.1365-2591.2007.01323.x
16. Gulabivala K, Ng YL. Factors that affect the outcomes of root canal treatment and retreatment-A reframing of the principles. Int Endod J. 2023;56(Suppl 2):82–115. doi:10.1111/iej.13897
17. Mannocci F, Bitter K, Sauro S, Ferrari P, Austin R, Bhuva B. Present status and future directions: the restoration of root filled teeth. Int Endod J. 2022;55 Suppl 4(Suppl 4):1059–1084. doi:10.1111/iej.13796
18. Hoskinson SE, Ng YL, Hoskinson AE, Moles DR, Gulabivala K. A retrospective comparison of outcome of root canal treatment using two different protocols. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002;93(6):705–715. doi:10.1067/moe.2001.122822
19. Ricucci D, Russo J, Rutberg M, Burleson JA, Spångberg LS. A prospective cohort study of endodontic treatments of 1369 root canals: results after 5 years. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;112(6):825–842. doi:10.1016/j.tripleo.2011.08.003
20. López-Valverde I, Vignoletti F, Vignoletti G, Martin C, Sanz M. Long-term tooth survival and success following primary root canal treatment: a 5- to 37-year retrospective observation. Clin Oral Investig. 2023. doi:10.1007/s00784-023-04938-y
21. Huumonen S, Ørstavik D. Radiological aspects of apical periodontitis. Endodontic Topics. 2002;1(1):3–25. doi:10.1034/j.1601-1546.2002.10102.x
22. Kirkevang LL, Ørstavik D, Wenzel A, Vaeth M. Prognostic value of the full-scale Periapical Index. Int Endod J. 2015;48(11):1051–1058. doi:10.1111/iej.12402
23. Azarpazhooh A, Sgro A, Cardoso E, et al. A Scoping Review of 4 Decades of Outcomes in Nonsurgical Root Canal Treatment, Nonsurgical Retreatment, and Apexification Studies-Part 2: outcome Measures. J Endod. 2022;48(1):29–39. doi:10.1016/j.joen.2021.09.019
24. Aminoshariae A, Kulild JC, Syed A. Cone-beam Computed Tomography Compared with Intraoral Radiographic Lesions in Endodontic Outcome Studies: a Systematic Review. J Endod. 2018;44(11):1626–1631. doi:10.1016/j.joen.2018.08.006
25. Fayad MI. AAE and AAOMR Joint Position Statement: use of Cone Beam Computed Tomography in Endodontics 2015 Update. Oral Surg Oral Med Oral Pathol Oral Radiol. 2015;120(4):508–512. doi:10.1016/j.oooo.2015.07.033
26. Patel S, Brown J, Semper M, Abella F, Mannocci F. European Society of Endodontology position statement: use of cone beam computed tomography in Endodontics: European Society of Endodontology (ESE) developed by. Int Endod J. 2019;52(12):1675–1678. doi:10.1111/iej.13187
27. Orstavik D, Kerekes K, Eriksen HM. The periapical index: a scoring system for radiographic assessment of apical periodontitis. Endod Dent Traumatol. 1986;2(1):20–34. doi:10.1111/j.1600-9657.1986.tb00119.x
28. Marending M, Peters OA, Zehnder M. Factors affecting the outcome of orthograde root canal therapy in a general dentistry hospital practice. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;99(1):119–124. doi:10.1016/j.tripleo.2004.06.065
29. Kirkevang LL, Vaeth M, Wenzel A. Ten-year follow-up observations of periapical and endodontic status in a Danish population. Int Endod J. 2012;45(9):829–839. doi:10.1111/j.1365-2591.2012.02040.x
30. Jordal K, Valen A, Örstavik D. Periapical status of root-filled teeth in Norwegian children and adolescents. Acta Odontol Scand. 2014;72(8):801–805. doi:10.3109/00016357.2014.913193
31. Stueland H, Ørstavik D, Handal T. Treatment outcome of surgical and non-surgical endodontic retreatment of teeth with apical periodontitis. Int Endod J. 2023. doi:10.1111/iej.13914
32. Torabinejad M, Corr R, Handysides R, Shabahang S. Outcomes of nonsurgical retreatment and endodontic surgery: a systematic review. J Endod. 2009;35(7):930–937. doi:10.1016/j.joen.2009.04.023
33. Chércoles-Ruiz A, Sánchez-Torres A, Gay-Escoda C. Endodontics, Endodontic Retreatment, and Apical Surgery Versus Tooth Extraction and Implant Placement: a Systematic Review. J Endod. 2017;43(5):679–686. doi:10.1016/j.joen.2017.01.004
34. Ng YL, Mann V, Rahbaran S, Lewsey J, Gulabivala K. Outcome of primary root canal treatment: systematic review of the literature - part 1. Effects of study characteristics on probability of success. Int Endod J. 2007;40(12):921–939. doi:10.1111/j.1365-2591.2007.01322.x
35. Gorni FG, Gagliani MM. The outcome of endodontic retreatment: a 2-yr follow-up. J Endod. 2004;30(1):1–4. doi:10.1097/00004770-200401000-00001
36. Venskutonis T, Plotino G, Juodzbalys G, Mickevičienė L. The importance of cone-beam computed tomography in the management of endodontic problems: a review of the literature. J Endod. 2014;40(12):1895–1901. doi:10.1016/j.joen.2014.05.009
37. Liang YH, Li G, Wesselink PR, Wu MK. Endodontic outcome predictors identified with periapical radiographs and cone-beam computed tomography scans. J Endod. 2011;37(3):326–331. doi:10.1016/j.joen.2010.11.032
38. Ee J, Fayad MI, Johnson BR. Comparison of endodontic diagnosis and treatment planning decisions using cone-beam volumetric tomography versus periapical radiography. J Endod. 2014;40(7):910–916. doi:10.1016/j.joen.2014.03.002
39. Bhatt M, Coil J, Chehroudi B, Esteves A, Aleksejuniene J, MacDonald D. Clinical decision-making and importance of the AAE/AAOMR position statement for CBCT examination in endodontic cases. Int Endod J. 2021;54(1):26–37. doi:10.1111/iej.13397
40. Patel S, Dawood A, Ford TP, Whaites E. The potential applications of cone beam computed tomography in the management of endodontic problems. Int Endod J. 2007;40(10):818–830. doi:10.1111/j.1365-2591.2007.01299.x
41. Ozer SY. Detection of vertical root fractures of different thicknesses in endodontically enlarged teeth by cone beam computed tomography versus digital radiography. J Endod. 2010;36(7):1245–1249. doi:10.1016/j.joen.2010.03.021
42. Varshosaz M, Tavakoli MA, Mostafavi M, Baghban AA. Comparison of conventional radiography with cone beam computed tomography for detection of vertical root fractures: an in vitro study. J Oral Sci. 2010;52(4):593–597. doi:10.2334/josnusd.52.593
43. Junqueira RB, Verner FS, Campos CN, Devito KL, Do Carmo AM. Detection of vertical root fractures in the presence of intracanal metallic post: a comparison between periapical radiography and cone-beam computed tomography. J Endod. 2013;39(12):1620–1624. doi:10.1016/j.joen.2013.08.031
44. Brady E, Mannocci F, Brown J, Wilson R, Patel S. A comparison of cone beam computed tomography and periapical radiography for the detection of vertical root fractures in nonendodontically treated teeth. Int Endod J. 2014;47(8):735–746. doi:10.1111/iej.12209
45. Khedmat S, Rouhi N, Drage N, Shokouhinejad N, Nekoofar MH. Evaluation of three imaging techniques for the detection of vertical root fractures in the absence and presence of gutta-percha root fillings. Int Endod J. 2012;45(11):1004–1009. doi:10.1111/j.1365-2591.2012.02062.x
46. de Lima KL, Silva LR, de Paiva Prado TB, Silva MAG, de Freitas Silva BS, Yamamoto-Silva FP. Influence of the technical parameters of CBCT image acquisition on vertical root fracture diagnosis: a systematic review and meta-analysis. Clin Oral Investig. 2023;27(2):433–474. doi:10.1007/s00784-022-04797-z
47. Fontenele RC, Machado AH, de Oliveira Reis L, Freitas DQ. Influence of metal artefact reduction tool on the detection of vertical root fractures involving teeth with intracanal materials in cone beam computed tomography images: a systematic review and meta-analysis. Int Endod J. 2021;54(10):1769–1781. doi:10.1111/iej.13569
48. Gluskin AH, Ruddle CJ, Zinman EJ. Thermal injury through intraradicular heat transfer using ultrasonic devices: precautions and practical preventive strategies. J Am Dent Assoc. 2005;136(9):1286–1293. doi:10.14219/jada.archive.2005.0346
49. Satterthwaite JD, Stokes AN, Frankel NT. Potential for temperature change during application of ultrasonic vibration to intra-radicular posts. Eur J Prosthodont Restor Dent. 2003;11(2):51–56.
50. Castrisos T, Abbott PV. A survey of methods used for post removal in specialist endodontic practice. Int Endod J. 2002;35(2):172–180. doi:10.1046/j.1365-2591.2002.00466.x
51. Haupt F, Riggers I, Konietschke F, Rödig T. Effectiveness of different fiber post removal techniques and their influence on dentinal microcrack formation. Clin Oral Investig. 2022;26(4):3679–3685. doi:10.1007/s00784-021-04338-0
52. Schwindling FS, Tasaka A, Hilgenfeld T, Rammelsberg P, Zenthöfer A. Three-dimensional-guided removal and preparation of dental root posts-concept and feasibility. J Prosthodont Res. 2020;64(1):104–108. doi:10.1016/j.jpor.2019.04.005
53. Perez C, Sayeh A, Etienne O, et al. Microguided endodontics: accuracy evaluation for access through intraroot fibre-post. Aust Endod J. 2021;47(3):592–598. doi:10.1111/aej.12524
54. Arukaslan G, Aydemir S. Comparison of the efficacies of two different fiber post-removal systems: a micro-computed tomography study. Microsc Res Tech. 2019;82(4):394–401. doi:10.1002/jemt.23180
55. Haupt F, Pfitzner J, Hülsmann M. A comparative in vitro study of different techniques for removal of fibre posts from root canals. Aust Endod J. 2018;44(3):245–250. doi:10.1111/aej.12230
56. Abbott PV. Incidence of root fractures and methods used for post removal. Int Endod J. 2002;35(1):63–67. doi:10.1046/j.1365-2591.2002.00457.x
57. Aydemir S, Arukaslan G, Sarıdağ S, Kaya-Büyükbayram I, Ylıdıran Y. Comparing Fracture Resistance and the Time Required for Two Different Fiber Post Removal Systems. J Prosthodont. 2018;27(8):771–774. doi:10.1111/jopr.12575
58. Ricucci D, Siqueira JF Jr. Biofilms and apical periodontitis: study of prevalence and association with clinical and histopathologic findings. J Endod. 2010;36(8):1277–1288. doi:10.1016/j.joen.2010.04.007
59. Nair PN. On the causes of persistent apical periodontitis: a review. Int Endod J. 2006;39(4):249–281. doi:10.1111/j.1365-2591.2006.01099.x
60. Witherspoon DE, Small JC, Regan JD. Missed canal systems are the most likely basis for endodontic retreatment of molars. Tex Dent J. 2013;130(2):127–139.
61. Baruwa AO, Martins JNR, Meirinhos J, et al. The Influence of Missed Canals on the Prevalence of Periapical Lesions in Endodontically Treated Teeth: a Cross-sectional Study. J Endod. 2020;46(1):34–39.e1. doi:10.1016/j.joen.2019.10.007
62. Costa F, Pacheco-Yanes J, Siqueira JF Jr, et al. Association between missed canals and apical periodontitis. Int Endod J. 2019;52(4):400–406. doi:10.1111/iej.13022
63. Mashyakhy M, Hadi FA, Alhazmi HA, et al. Prevalence of Missed Canals and Their Association with Apical Periodontitis in Posterior Endodontically Treated Teeth: a CBCT Study. Int J Dent. 2021;2021:9962429. doi:10.1155/2021/9962429
64. Peña-Bengoa F, Cáceres C, Niklander SE, Meléndez P. Association between second mesiobuccal missed canals and apical periodontitis in maxillary molars of a Chilean subpopulation. J Clin Exp Dent. 2023;15(3):e173–e176. doi:10.4317/jced.60156
65. Colakoglu G, Kaya Buyukbayram I, Elcin MA, Garip Berker Y, Ercalik Yalcinkaya S. Association between second mesiobuccal canal and apical periodontitis in retrospective cone-beam computed tomographic images. Aust Endod J. 2023;49(1):20–26. doi:10.1111/aej.12672
66. Kuzekanani M, Walsh LJ, Amiri M. Prevalence and Distribution of the Middle Mesial Canal in Mandibular First Molar Teeth of the Kerman Population: a CBCT Study. Int J Dent. 2020;2020:8851984. doi:10.1155/2020/8851984
67. Pomeranz HH, Eidelman DL, Goldberg MG. Treatment considerations of the middle mesial canal of mandibular first and second molars. J Endod. 1981;7(12):565–568. doi:10.1016/s0099-2399(81)80216-6
68. Versiani MA, Ordinola-Zapata R, Keleş A, et al. Middle mesial canals in mandibular first molars: a micro-CT study in different populations. Arch Oral Biol. 2016;61:130–137. doi:10.1016/j.archoralbio.2015.10.020
69. Dhuldhoya DN, Singh S, Podar RS, Ramachandran N, Jain R, Bhanushali N. Root canal anatomy of human permanent mandibular incisors and mandibular canines: a systematic review. J Conserv Dent. 2022;25(3):226–240. doi:10.4103/jcd.jcd_40_22
70. Martins JNR, Marques D, Leal Silva EJN, Caramês J, Mata A, Versiani MA. Influence of Demographic Factors on the Prevalence of a Second Root Canal in Mandibular Anterior Teeth - A Systematic Review and Meta-Analysis of Cross-Sectional Studies Using Cone Beam Computed Tomography. Arch Oral Biol. 2020;116:104749. doi:10.1016/j.archoralbio.2020.104749
71. Karobari MI, Assiry AA, Lin GSS, et al. Roots and Root Canals Characterization of Permanent Mandibular Premolars Analyzed Using the Cone Beam and Micro Computed Tomography-A Systematic Review and Metanalysis. J Clin Med. 2023;12(6):657.
72. Martins JNR, Marques D, Silva E, Caramês J, Mata A, Versiani MA. Prevalence of C-shaped canal morphology using cone beam computed tomography - a systematic review with meta-analysis. Int Endod J. 2019;52(11):1556–1572. doi:10.1111/iej.13169
73. Reda R, Zanza A, Bhandi S, Biase A, Testarelli L, Miccoli G. Surgical-anatomical evaluation of mandibular premolars by CBCT among the Italian population. Dent Med Probl. 2022;59(2):209–216. doi:10.17219/dmp/143546
74. Carr GB, Murgel CA. The use of the operating microscope in endodontics. Dent Clin North Am. 2010;54(2):191–214. doi:10.1016/j.cden.2010.01.002
75. Plotino G, Pameijer CH, Grande NM, Somma F. Ultrasonics in endodontics: a review of the literature. J Endod. 2007;33(2):81–95. doi:10.1016/j.joen.2006.10.008
76. Duncan HF, Chong BS. Removal of root filling materials. Endodontic Topics. 2008;19(1):33–57. doi:10.1111/j.1601-1546.2011.00257.x
77. Ajina MA, Shah PK, Chong BS. Critical analysis of research methods and experimental models to study removal of root filling materials. Int Endod J. 2022;55(Suppl 1):119–152. doi:10.1111/iej.13650
78. Horvath SD, Altenburger MJ, Naumann M, Wolkewitz M, Schirrmeister JF. Cleanliness of dentinal tubules following gutta-percha removal with and without solvents: a scanning electron microscopic study. Int Endod J. 2009;42(11):1032–1038. doi:10.1111/j.1365-2591.2009.01616.x
79. Boutsioukis C, Noula G, Lambrianidis T. Ex vivo study of the efficiency of two techniques for the removal of mineral trioxide aggregate used as a root canal filling material. J Endod. 2008;34(10):1239–1242. doi:10.1016/j.joen.2008.07.018
80. Hess D, Solomon E, Spears R, He J. Retreatability of a bioceramic root canal sealing material. J Endod. 2011;37(11):1547–1549. doi:10.1016/j.joen.2011.08.016
81. Pirani C, Iacono F, Chersoni S, et al. The effect of ultrasonic removal of various root-end filling materials. Int Endod J. 2009;42(11):1015–1025. doi:10.1111/j.1365-2591.2009.01612.x
82. Tachinami H, Katsuumi I. Removal of root canal filling materials using Er:YAG laser irradiation. Dent Mater J. 2010;29(3):246–252. doi:10.4012/dmj.2008-079
83. Gorduysus MO, Al-Rubai H, Salman B, Al Saady D, Al-Dagistani H, Muftuoglu S. Using erbium-doped yttrium aluminum garnet laser irradiation in different energy output levels versus ultrasonic in removal of root canal filling materials in endodontic retreatment. Eur J Dent. 2017;11(3):281–286. doi:10.4103/ejd.ejd_111_17
84. Baumeier NC, Húngaro Duarte MA, Vivan RR, Lemos AC, Machado R, da Silva Neto UX. Passive ultrasonic irrigation, EndoActivator system and XP-endo Finisher R as additional cleaning techniques to remove residual filling materials from flattened root canals. J Conserv Dent. 2022;25(4):385–391. doi:10.4103/jcd.jcd_117_22
85. Matoso FB, Quintana RM, Jardine AP, et al. XP Endo Finisher-R and PUI as supplementary methods to remove root filling materials from curved canals. Braz Oral Res. 2022;36:e053. doi:10.1590/1807-3107bor-2022.vol36.0053
86. De-Deus G, Belladonna FG, Zuolo AS, et al. XP-endo Finisher R instrument optimizes the removal of root filling remnants in oval-shaped canals. Int Endod J. 2019;52(6):899–907. doi:10.1111/iej.13077
87. Uzunoglu-özyürek E, Küçükkaya Eren S, Karahan S. Contribution of XP-Endo files to the root canal filling removal: a systematic review and meta-analysis of in vitro studies. Aust Endod J. 2021;47(3):703–714. doi:10.1111/aej.12503
88. Clauder T. Present status and future directions - Managing perforations. Int Endod J. 2022;55(Suppl 4):872–891. doi:10.1111/iej.13748
89. Bryan EB, Woollard G, Mitchell WC. Nonsurgical repair of furcal perforations: a literature review. Gen Dent. 1999;47(3):274–8; quiz 279–80.
90. D’Assunção FL, Sousa JC, Felinto KC, et al. Accuracy and repeatability of 3 apex locators in locating root canal perforations: an ex vivo study. J Endod. 2014;40(8):1241–1244. doi:10.1016/j.joen.2014.02.004
91. Patel S, Durack C, Abella F, Shemesh H, Roig M, Lemberg K. Cone beam computed tomography in Endodontics - a review. Int Endod J. 2015;48(1):3–15. doi:10.1111/iej.12270
92. Krupp C, Bargholz C, Brüsehaber M, Hülsmann M. Treatment outcome after repair of root perforations with mineral trioxide aggregate: a retrospective evaluation of 90 teeth. J Endod. 2013;39(11):1364–1368. doi:10.1016/j.joen.2013.06.030
93. Fuss Z, Trope M. Root perforations: classification and treatment choices based on prognostic factors. Endod Dent Traumatol. 1996;12(6):255–264. doi:10.1111/j.1600-9657.1996.tb00524.x
94. Gorni FG, Andreano A, Ambrogi F, Brambilla E, Gagliani M. Patient and Clinical Characteristics Associated with Primary Healing of Iatrogenic Perforations after Root Canal Treatment: results of a Long-term Italian Study. J Endod. 2016;42(2):211–215. doi:10.1016/j.joen.2015.11.006
95. Siew K, Lee AH, Cheung GS. Treatment Outcome of Repaired Root Perforation: a Systematic Review and Meta-analysis. J Endod. 2015;41(11):1795–1804. doi:10.1016/j.joen.2015.07.007
96. Lee YL, Lee BS, Lin FH, Yun Lin A, Lan WH, Lin CP. Effects of physiological environments on the hydration behavior of mineral trioxide aggregate. Biomaterials. 2004;25(5):787–793. doi:10.1016/s0142-9612(03)00591-x
97. Holland R, Bisco Ferreira L, de Souza V, Otoboni Filho JA, Murata SS, Dezan E Jr. Reaction of the lateral periodontium of dogs’ teeth to contaminated and noncontaminated perforations filled with mineral trioxide aggregate. J Endod. 2007;33(10):1192–1197. doi:10.1016/j.joen.2007.07.013
98. Arens DE, Torabinejad M. Repair of furcal perforations with mineral trioxide aggregate: two case reports. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1996;82(1):84–88. doi:10.1016/s1079-2104(96)80382-9
99. Lemon RR, Steele PJ, Jeansonne BG. Ferric sulfate hemostasis: effect on osseous wound healing. Left in situ for maximum exposure. J Endod. 1993;19(4):170–173. doi:10.1016/s0099-2399(06)80681-3
100. Lambrianidis T. Ledging and blockage of root canals during canal preparation: causes, recognition, prevention, management, and outcomes. Endodontic Topics. 2006;15(1):56–74. doi:10.1111/j.1601-1546.2009.00235.x
101. Schäfer E, Bürklein S. Impact of nickel-titanium instrumentation of the root canal on clinical outcomes: a focused review. Odontology. 2012;100(2):130–136. doi:10.1007/s10266-012-0066-1
102. Bergenholtz G, Lekholm U, Milthon R, Heden G, Odesjö B, Engström B. Retreatment of endodontic fillings. Scand J Dent Res. 1979;87(3):217–224. doi:10.1111/j.1600-0722.1979.tb00675.x
103. Berutti E, Alovisi M, Moccia E, et al. Micro-computed tomographic evaluation of endodontic ledge position in relation to canal curvatures. BMC Oral Health. 2022;22(1):482. doi:10.1186/s12903-022-02531-5
104. Bhuva B, Ikram O. Complications in Endodontics. Prim Dent J. 2020;9(4):52–58. doi:10.1177/2050168420963306
105. Ünlü O, Güneç HG, Haznedaroğlu F. Investigation of the efficacy of different Ni-Ti systems on acrylic blocks for correcting ledge formation. BMC Oral Health. 2023;23(1):174. doi:10.1186/s12903-023-02865-8
106. Zanza A, D’Angelo M, Reda R, Gambarini G, Testarelli L, Di Nardo D. An Update on Nickel-Titanium Rotary Instruments in Endodontics: mechanical Characteristics, Testing and Future Perspective—An Overview. Bioengineering. 2021;8(12):789.
107. Seracchiani M, Reda R, Zanza A, D’Angelo M, Russo P, Luca T. Mechanical Performance and Metallurgical Characteristics of 5 Different Single-file Reciprocating Instruments: a Comparative In Vitro and Laboratory Study. J Endod. 2022;48(8):1073–1080. doi:10.1016/j.joen.2022.05.009
108. Zanza A, Russo P, Reda R, et al. Mechanical and Metallurgical Evaluation of 3 Different Nickel-Titanium Rotary Instruments: an In Vitro and In Laboratory Study. Bioengineering. 2022;9(5). doi:10.3390/bioengineering9050221
109. Zanza A, Russo P, Di Matteo P, et al. Mechanical properties and metallurgical features of two similar endodontic rotary instruments with different heat treatments (FireWire™ and Gold). Sci Prog. 2022;105(2):368504221103763. doi:10.1177/00368504221103763
110. Panitvisai P, Parunnit P, Sathorn C, Messer HH. Impact of a retained instrument on treatment outcome: a systematic review and meta-analysis. J Endod. 2010;36(5):775–780. doi:10.1016/j.joen.2009.12.029
111. Spili P, Parashos P, Messer HH. The impact of instrument fracture on outcome of endodontic treatment. J Endod. 2005;31(12):845–850. doi:10.1097/01.don.0000164127.62864.7c
112. Alapati SB, Brantley WA, Svec TA, Powers JM, Nusstein JM, Daehn GS. SEM observations of nickel-titanium rotary endodontic instruments that fractured during clinical Use. J Endod. 2005;31(1):40–43. doi:10.1097/01.don.0000132301.87637.4a
113. Bueno CSP, Oliveira DP, Pelegrine RA, Fontana CE, Rocha DGP, Bueno C. Fracture Incidence of WaveOne and Reciproc Files during Root Canal Preparation of up to 3 Posterior Teeth: a Prospective Clinical Study. J Endod. 2017;43(5):705–708. doi:10.1016/j.joen.2016.12.024
114. Ruivo LM, Rios MA, Villela AM, et al. Fracture incidence of Reciproc instruments during root canal retreatment performed by postgraduate students: a cross-sectional retrospective clinical study. Restor Dent Endod. 2021;46(4):e49. doi:10.5395/rde.2021.46.e49
115. Caballero-Flores H, Nabeshima CK, Binotto E, Machado MEL. Fracture incidence of instruments from a single-file reciprocating system by students in an endodontic graduate programme: a cross-sectional retrospective study. Int Endod J. 2019;52(1):13–18. doi:10.1111/iej.12982
116. Iqbal MK, Kohli MR, Kim JS. A retrospective clinical study of incidence of root canal instrument separation in an endodontics graduate program: a PennEndo database study. J Endod. 2006;32(11):1048–1052. doi:10.1016/j.joen.2006.03.001
117. Terauchi Y, Ali WT, Abielhassan MM. Present status and future directions: removal of fractured instruments. Int Endod J. 2022. doi:10.1111/iej.13743
118. Tzanetakis GN, Kontakiotis EG, Maurikou DV, Marzelou MP. Prevalence and management of instrument fracture in the postgraduate endodontic program at the Dental School of Athens: a five-year retrospective clinical study. J Endod. 2008;34(6):675–678. doi:10.1016/j.joen.2008.02.039
119. Madarati AA, Hunter MJ, Dummer PM. Management of intracanal separated instruments. J Endod. 2013;39(5):569–581. doi:10.1016/j.joen.2012.12.033
120. Nevares G, Cunha RS, Zuolo ML, Bueno CE. Success rates for removing or bypassing fractured instruments: a prospective clinical study. J Endod. 2012;38(4):442–444. doi:10.1016/j.joen.2011.12.009
121. Fu M, Zhang Z, Hou B. Removal of broken files from root canals by using ultrasonic techniques combined with dental microscope: a retrospective analysis of treatment outcome. J Endod. 2011;37(5):619–622. doi:10.1016/j.joen.2011.02.016
122. Cheung GSP. Instrument fracture: mechanisms, removal of fragments, and clinical outcomes. Endodontic Topics. 2007;16(1):1–26. doi:10.1111/j.1601-1546.2009.00239.x
123. Zanza A, Seracchiani M, Reda R, Miccoli G, Testarelli L, Di Nardo D. Metallurgical Tests in Endodontics: a Narrative Review. Bioengineering. 2022;9(1). doi:10.3390/bioengineering9010030
124. Terauchi Y, Sexton C, Bakland LK, Bogen G. Factors Affecting the Removal Time of Separated Instruments. J Endod. 2021;47(8):1245–1252. doi:10.1016/j.joen.2021.05.003
125. Suter B, Lussi A, Sequeira P. Probability of removing fractured instruments from root canals. Int Endod J. 2005;38(2):112–123. doi:10.1111/j.1365-2591.2004.00916.x
126. Leoni GB, Versiani MA, Silva-Sousa YT, Bruniera JF, Pécora JD, Sousa-Neto MD. Ex vivo evaluation of four final irrigation protocols on the removal of hard-tissue debris from the mesial root canal system of mandibular first molars. Int Endod J. 2017;50(4):398–406. doi:10.1111/iej.12630
127. Yoldas O, Topuz A, Isçi AS, Oztunc H. Postoperative pain after endodontic retreatment: single- versus two-visit treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004;98(4):483–487. doi:10.1016/j.tripleo.2004.03.009
128. Sathorn C, Parashos P, Messer H. The prevalence of postoperative pain and flare-up in single- and multiple-visit endodontic treatment: a systematic review. Int Endod J. 2008;41(2):91–99. doi:10.1111/j.1365-2591.2007.01316.x
129. Patel S, Bhuva B, Bose R. Present status and future directions: vertical root fractures in root filled teeth. Int Endod J. 2022. doi:10.1111/iej.13737
130. Ordinola-Zapata R, Noblett WC, Perez-Ron A, Ye Z, Vera J. Present status and future directions of intracanal medicaments. Int Endod J. 2022;55 Suppl 3(Suppl 3):613–636. doi:10.1111/iej.13731
131. Rosenthal S, Spångberg L, Safavi K. Chlorhexidine substantivity in root canal dentin. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004;98(4):488–492. doi:10.1016/j.tripleo.2003.07.005
132. Boutsioukis C, Arias-Moliz MT, Chávez de Paz LE. A critical analysis of research methods and experimental models to study irrigants and irrigation systems. Int Endod J. 2022;55 Suppl 2(Suppl 2):295–329. doi:10.1111/iej.13710
133. Boutsioukis C, Arias-Moliz MT. Present status and future directions - irrigants and irrigation methods. Int Endod J. 2022;55(Suppl 3):588–612. doi:10.1111/iej.13739
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.