")
Back to Journals » International Journal of Women's Health » Volume 16
Efficacy of Dan’e Fukang Soft Extract in Moderate Ovarian Hyperstimulation Syndrome for Concurrent Treatment of Blood and Fluid Guided by the “Triple Prevention” Principle
Authors Chen YH, Zhang XL, Li ZY, Wang XP, Wang J, Zhang ZP, Zhu PF, Wu XQ
Received 24 August 2023
Accepted for publication 25 February 2024
Published 6 March 2024 Volume 2024:16 Pages 385—394
DOI https://doi.org/10.2147/IJWH.S436965
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Yan-Hua Chen,1 Xue-Luo Zhang,1 Zhong-Yun Li,2 Xian-Ping Wang,1 Jun Wang,3 Zhi-Ping Zhang,1 Peng-Fei Zhu,1 Xue-Qing Wu1
1Reproductive Medicine Center, Shanxi Maternal and Child Health Care Hospital, Taiyuan, People’s Republic of China; 2Rectum Branch, Shanxi Provincial Hospital of Traditional Chinese Medicine, Taiyuan, People’s Republic of China; 3The Sixth Hospital of Shanxi Medical University (General Hospital of Tisco), Taiyuan, People’s Republic of China
Correspondence: Xue-Qing Wu, Reproductive Medicine Center, Shanxi Maternal and Child Health Care Hospital, No. 13, Xinmin Middle Street, Xinghualing District, Taiyuan, Shanxi Province, 030013, People’s Republic of China, Tel +86 351-3360725, Email [email protected]
Objective: This study aimed to evaluate the therapeutic efficacy and safety of Dan’e Fukang soft extracts in moderate ovarian hyperstimulation syndrome (OHSS) for the simultaneous treatment of blood and fluid, guided by the traditional Chinese medicine principle of “triple prevention”.
Methods: This study conducted a retrospective analysis of clinical data from outpatients who underwent in vitro fertilization (IVF)/intracytoplasmic sperm injection embryo transfer (ICSI-ET). A total of 2245 cases were included and divided into a treatment group (1002 cases) and a control group (1243 cases). Patients in the treatment group were administered Dan’e Fukang soft extracts orally in addition to conventional Western medicine. Comparative assessments were made between the two groups on pelvic ascites volume, maximum ovary diameter, dysmenorrhea incidence post-oocyte retrieval, and safety indicators.
Results: There were no statistically significant differences between the treatment group and the control group in terms of general characteristics or the levels of follicle-stimulating hormone (FSH), luteotropic hormone (LH), estradiol (E2), or progesterone (P) at the time of gonadotropin (Gn) initiation. The groups did not differ significantly when we compared the levels of LH, E2, or P on the day of human chorionic gonadotropin (hCG) injection and during ovarian hyperstimulation protocols (P > 0.05 for all indicators). The differences in the volume of pelvic ascites, the maximum ovarian diameter, and the incidence of dysmenorrhea after oocyte retrieval were statistically significant between the treatment group and the control group (P < 0.05 in both). There were no instances of adverse reactions in either group.
Conclusion: Based on the traditional Chinese medicine principle of “triple prevention”, the use of Dan’e Fukang soft extracts for the simultaneous treatment of blood and fluid in moderate OHSS significantly improved the absorption of pelvic ascites, promoted ovarian recovery, and reduced the incidence of dysmenorrhea after oocyte retrieval.
Keywords: Dan’e Fukang soft extracts, guiding principle of triple prevention, in vitro fertilization embryo transfer/intracytoplasmic sperm injection embryo transfer, ovarian hyperstimulation syndrome, simultaneous treatment of blood and fluid
Introduction
Ovarian hyperstimulation syndrome (OHSS) is one of the main complications of artificial reproductive technology (ART) with in vitro fertilization embryo transfer (IVF-ET).1 In clinic, based on the patient’s past medical history, clinical manifestations, and additional examinations, OHSS is classified as mild, moderate, or severe. Previous epidemiological investigations have estimated the incidence of moderate and severe OHSS in patients receiving ART with IVF-ET at 3–6% and 0.1–2%, respectively, which leads to negative impact on the daily activities and work lives of patients to varying degrees.
The pathogenesis and mechanism of OHSS is very complex. Previous studies have shown that an elevated transient receptor potential melastatin 2 (TRPM2) activity has been found in rat’s OHSS-developed ovaries,2 suggesting the important contributions of ion channels on the pathogenesis of OHSS. Besides, the increased secretions of some cytokines or mediators (eg including vascular endothelial growth factor [VEGF], platelet-derived growth [PDGF], insulin-like growth factor‐1 [IGF‐1]) also been demonstrated to occupy an important role in increased capillary permeability as well as the fluid accumulation in the third space, which may be responsible for the inflammatory response associated with follicular maturation, ovulation, corpus luteum function and embryo implantation.3,4
Several strategies have been suggested to prevent or relieve the progression of OHSS according to the results obtained from clinical practice and experimental findings, for example, cycle cancellation, antagonist protocol, withholding gonadotropin administrations and stopping injecting human chorionic gonadotropin (hCG) until hCG drops to a safe level as well as embryos freezing. However, none of these strategies mentioned above are fully effective in preventing OHSS, except for cycle cancellation.5–7 With the development of the related study on treating OHSS, although some alternative strategies have been progressively demonstrated to be associated with the reduction of the intensity of OHSS, there are very limited study data on these strategies up to now.8–12 Therefore, it was urgent to find new and effective strategies for preventing or treating OHSS.
Clinical practices have revealed that traditional Chinese medicine (TCM) has shown advantages in alleviating the symptoms of OHSS. The guiding principle of “triple prevention” in TCM is beneficial in minimizing this negative impact, ie, “prevention before the onset of illness, prevention of deterioration after the onset of illness, [and] prevention of relapse after recovery” are necessary to actively safeguard the health of patients with OHSS.13
TCM is being used more frequently on a daily basis as a result of an increased understanding of TCM and its positive effects in terms of an improved quality of life. Dialectical treatment is provided based on the “triple prevention” principle to reduce the incidence of moderate OHSS in patients undergoing ART with IVF-ET. Dan’e Fukang soft extracts are used in the treatment of moderate OHSS from the perspective of “activating blood circulation and removing blood stasis, soothing [the] liver, acting as a diuretic, regulating menstruation, and relieving pain” in TCM. This can improve microcirculation and counteract inflammation, as well as offer sedation and analgesia to achieve the “simultaneous treatment of blood and fluid”; ie, in clinical practice, when patients develop ascites, it is necessary to promote blood circulation and remove blood stasis, soothe the liver with diuretics, and treat the disease from the perspective of blood.
In the present study, we summarized and retrospectively analyzed the data of patients undergoing ART in the Reproductive Medicine Center of the Shanxi Provincial Maternal and Child Health Hospital, China. We examined the therapeutic efficacy of using Dan’e Fukang soft extracts in the treatment of moderate OHSS along with the latest evidence-based statistical data on OHSS. Our aim was to provide a new clinical treatment plan guided by the TCM principles of “triple prevention” and “simultaneous treatment of blood and fluid”.
Clinical Information
General Information
We collected the data of outpatients who underwent ART with IVF-ET at the Reproductive Medicine Center of Shanxi Provincial Maternal and Child Health Hospital, China, between January 2021 and April 2022. For the present study, we obtained 10 to 20 oocytes from patients who had moderate OHSS after the procedure. After excluding the cases with canceled oocyte retrievals and incomplete data, we screened 2245 cases with complete data for a retrospective analysis (Figure 1). Among them, 1002 cases were assigned to the Dan’e Fukang soft extract treatment group, and the remaining 1243 cases without TCM administration were included in the control group.
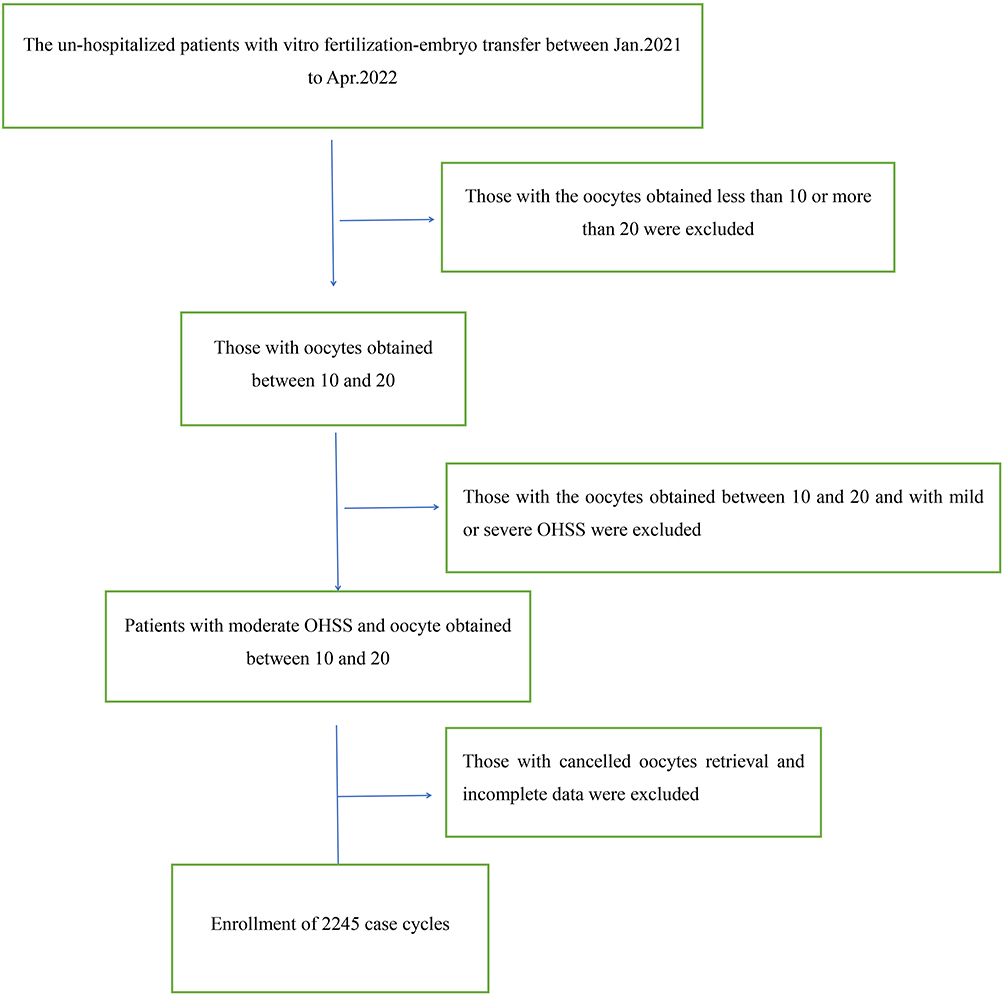 |
Figure 1 Flowchart of the case screening process. |
Methods
Study Design
Following oocyte retrieval, patients in the treatment group took one sachet (15 g/sachet) of Dan’e Fukang soft extracts (Yunnan Shengke Pharmaceutical Co., Ltd., State Drug Administration Z20025253), twice a day orally. The extracts were continued until the patient’s subsequent menstrual period. The patients in the control group received conventional therapy.
Conventional Western medicine treatments were given in both groups (ie, 10 mg of oral dydrogesterone in the morning and 10 mg in the evening, 5 mg of letrozole, 5 mg of bromocriptine anal suppository, and 100 mg of aspirin enteric-coated tablets, taken orally). The patients were instructed to record their daily food intake and output, waist circumference, weight, and other information, and these were reviewed with the supervising physician. The patients were also instructed to follow a high-protein diet and refrain from strenuous activities.
Therapeutic Protocols for in vitro Fertilization Embryo Transfer/Intracytoplasmic Sperm Injection Embryo Transfer
We used the following controlled OHSS protocol of gonadotropin (Gn)-releasing hormone agonist/antagonist/Gn/human chorionic Gn (GnRH-a/GnRH-A/Gn/HCG) protocols:
The long protocol: During the first week of the Gn initiation cycle, 0.1 mg of triptorelin acetate injection (Changchun GenSci Pharmaceutical Co., Ltd.; 0.1 mg/vial; State Drug Administration H20044922) was administered intramuscularly for 14 days. On day 2 of the Gn cycle or 14 days after the injection of treprostinil acetate, based on the levels of the basal sex hormone and follicle size, we calculated the dose of urinary follicle-stimulating hormone (uFSH) for intramuscular injection (Lizhu Group, Lizhu Pharmaceutical Factory; State Drug Administration H20052130).
In all patients, when most of the bilateral dominant follicles were ≥18 mm in diameter, an injection of human chorionic gonadotropin (hCG) (6000 IU) (Lizhu Group, Lizhu Pharmaceutical Factory; 2000 IU/vial; State Drug Administration: 44020673) was administered intramuscularly at night. Around 36–40 hours after the hCG injection, bilateral ovarian oocyte aspiration guided by vaginal ultrasound was conducted. Routine laboratory insemination and culture were performed. The fertilized oocytes were cultured in vitro for three days. Two embryos were selected for intrauterine embryo transfer, and luteal-phase support was initiated. A positive serum β-hCG test on day 10 after transplantation was considered a biochemical pregnancy. Clinical pregnancy was diagnosed on day 27 after transplantation based on the presence of a fetal sac, fetal bud reflection, and a fetal heart detected using a vaginal ultrasound examination.
The short protocol: An injection of 0.1 mg of treprostinil acetate was administered subcutaneously on day 2 of the Gn cycle and continued until the day of the hCG injection. During the same time as the treprostinum acetate injection on day 2 of the Gn cycle, the dose of intramuscular uFSH was calculated based on the levels of basal sex hormone and follicle size. The same monitoring methods were used as with the long protocol. Around 36–40 hours after the nocturnal injection of hCG, bilateral ovarian oocyte aspiration guided by a vaginal ultrasound was done.
The extra-long protocol: On days 2–4 of the menstrual cycle, an injection of 3.75 mg of leuprorelin acetate microspheres (sustained release for injection) (Beijing Boente Pharmaceutical Co., Ltd.; 3.75 mg/vial; State Drug Administration H20093809) was administered. Then, 28 days later, based on the levels of basal sex hormone and the size of the follicles, the dose of intramuscular uFSH was determined. The monitoring methods were the same as those used in the long protocol. Around 36–40 hours after the nocturnal injection of hCG, bilateral ovarian oocyte aspiration guided by a vaginal ultrasound was conducted.
The GnRH-a protocol: On days 2–3 of the menstrual cycle, the dose of uFSH for intramuscular injection was determined according to the levels of basal sex hormone and follicle size. When the maximum follicle diameter was ≥14 mm, an injection of ganirelix acetate (N.V. Organon, registration number: H20160574) was administered (0.25–0.5 mg/d) up to and including the day of the hCG injection. The monitoring methods were the same as those used in the long protocol. Around 36–40 hours after the nocturnal injection of HCG, bilateral ovarian oocyte aspiration guided by a vaginal ultrasound was conducted.
The simple Gn protocol: On days 2–3 of the menstrual cycle, the dose of uFSH for intramuscular injection was determined according to the levels of basal sex hormone and the size of the follicles. When the maximum follicle diameter was ≥14 mm, the levels of sex hormones were monitored. In the event of no elevation in luteotropic hormone (LH), the original protocol was followed until the follicles reached maturity. Around 36–40 hours after the nocturnal hCG injection, bilateral ovarian oocyte aspiration guided by a vaginal ultrasound was conducted. The monitoring methods were the same as those used in the long protocol.
The microstimulation protocol: On days 2–3 of the menstrual cycle, oral clomiphene (50–100 mg/d) and uFSH (150 IU/5 d) (Lizhu Group Lizhu Pharmaceutical Factory; State Drug Administration H10940097) were administered based on the levels of basal sex hormones and follicle size. Follicle monitoring by B-ultrasonography was initiated on day 8 of the menstrual cycle. If the follicle diameter was >10 mm, the dosage of human menopausal gonadotropin (HMG) was not increased. If the follicle diameter was <10 mm, the HMG dosage was increased by 75 IU/d. The monitoring methods were the same as those used in the long protocol. Around 36–40 hours after the nocturnal injection of hCG, bilateral ovarian oocyte aspiration guided by a vaginal ultrasound was conducted.
Clinical Data
We collected the following details from the patients enrolled in the study: age, body mass index (BMI), duration of infertility (years), infertility factors, type of infertility, total Gn dosage, initial Gn dosage, duration of Gn administration (days); the levels of FSH, LH, estradiol (E2), and progesterone (P) on the day of Gn initiation, and the levels of LH, E2, and P on the trigger day with hCG injection.
The ovarian hyperstimulation protocols included the long protocol, the short protocol, the extra-long protocol, the GnRH-a protocol, the simple Gn protocol, and the microstimulation protocol.
Diagnosis and Grading of OHSS
The obstetrics and gynecology department was selected for referrals for the diagnosis and grading of OHSS after considering all the clinical criteria for the diagnosis and grading as well as the testing techniques available in the department.14 As per the clinical manifestations and relevant laboratory findings, OHSS was classified into the following four grades: mild, moderate, severe, and critical.
In mild OHSS, patients had enlarged ovaries along with abdominal distension, abdominal discomfort, additional nausea, and vomiting. However, the ovaries were ≤5 cm in diameter, and the blood E2 level was ≥1500 pg/mL. Based on the manifestations in mild OHSS, patients with moderate OHSS had pleural effusion with ovarian diameters of 5 cm to ≤12 cm. Patients with severe OHSS presented with pleural effusion, ascites, and ovarian diameters ≥12 cm, or they were combined with renal impairment, a hematocrit (Hct) level ≥45%, a white blood cell (WBC) count ≥15 × 109/L, or thrombosis in some cases. Patients with critical OHSS had co-existing acute respiratory distress, with Hct ≥55%, WBC ≥25 × 109/L, and severe renal dysfunction, with a creatinine clearance of <50 mL/min.
In the present study, we included and grouped only patients with moderate OHSS; patients with severe OHSS were excluded.
Observation Indicators
We observed the maximum ovarian diameter, the volume of pelvic ascites after oocyte retrieval and during menstruation, and the incidence of dysmenorrhea after oocyte retrieval in both groups.
Statistical Analysis
We used SPSS 20.0 (SPSS Software, Chicago, IL, USA) software for the statistical analysis. Measurement data that did not satisfy a normal distribution were expressed as median (P25, P75), and the Kruskal–Wallis test was used for analysis of variance for multiple-group comparison. Countable data were expressed as the number of cases (rates), and a chi-squared test was used for intergroup comparisons. A rank-sum test was used for the comparison of rank variables. A P value of <0.05 was considered statistically significant.
Results
Comparison of General Characteristics Between the Two Groups of Patients
The treatment and control groups did not differ significantly in terms of age, BMI, duration of infertility (years), infertility factors, types of infertility, total Gn dosage, initial Gn dosage, duration of Gn administration (days); levels of FSH, LH, E2, and P on the day of Gn initiation; levels of LH, E2, and P on the day of hCG injection, and ovarian hyperstimulation protocols (P > 0.05 for all indicators), as shown in Table 1.
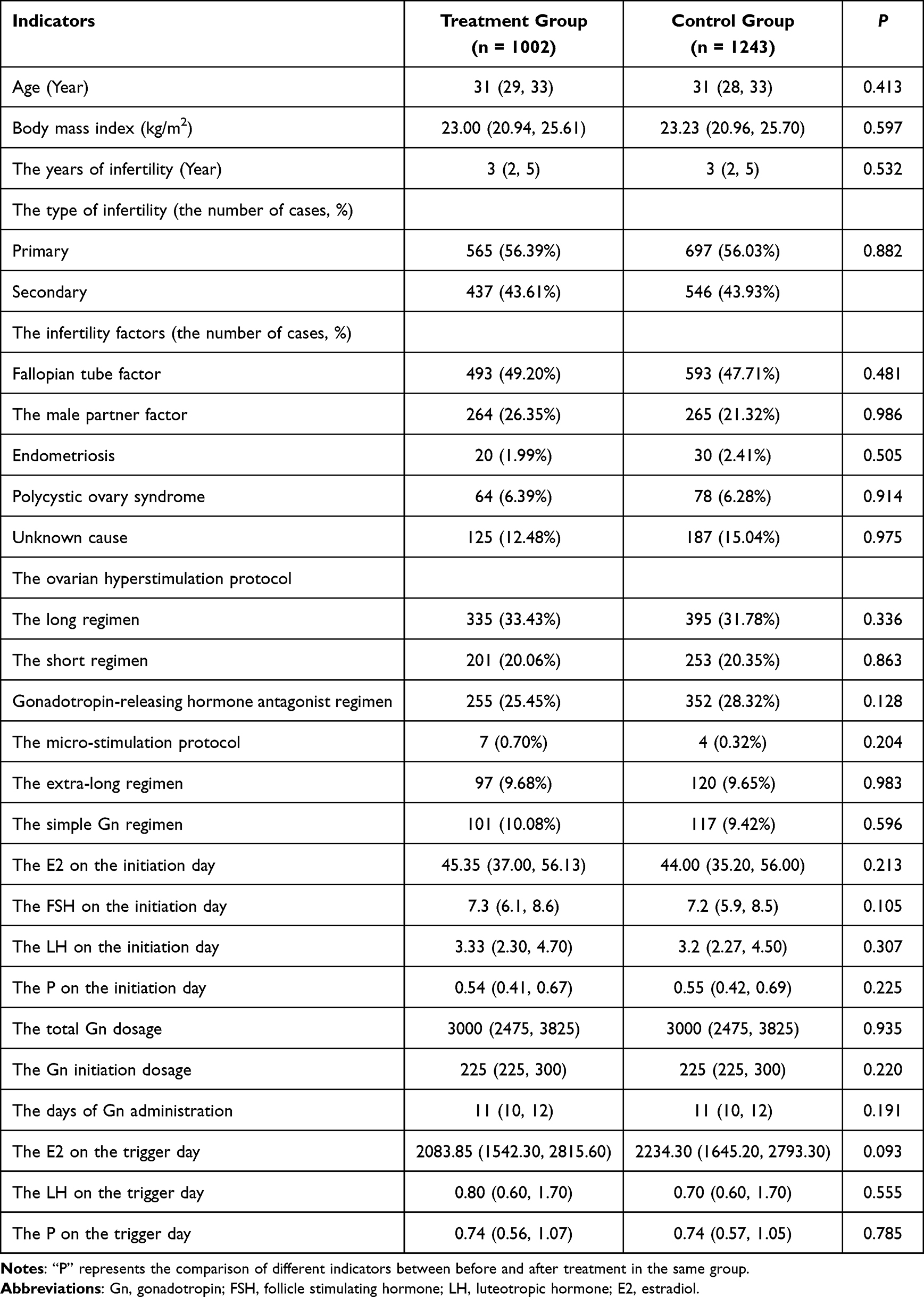 |
Table 1 Comparison of the General Characteristics Between the Two Groups of Patients |
Comparison of the Indicators Pre- and Post-Treatment in Both Groups of Patients
Pre-treatment, the differences in the volume of pelvic ascites and the maximum ovarian diameter were not statistically significant between the treatment group and the control group (P > 0.05 for both indicators). However, post-treatment, we found statistically significant differences between the treatment group and the control group in the volume of pelvic ascites and the maximum ovarian diameter (P < 0.05 for both indicators). The therapeutic efficacy was better in the treatment group. After oocyte retrieval, the incidence of dysmenorrhea in the treatment group and the control group was 20.36% (204/1002 cases) and 30.57% (380/1243 cases), respectively, and this difference was statistically significant between the groups (P < 0.05). The details are presented in Table 2.
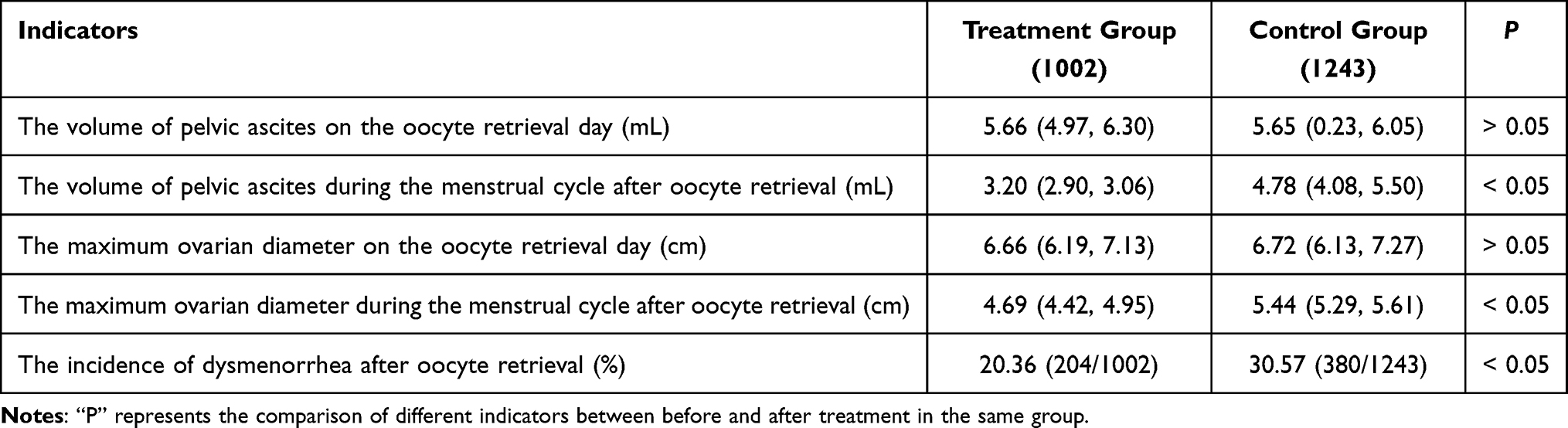 |
Table 2 Comparison of the Indicators Before and After Treatment in the Two Groups of Patients |
Safety Evaluation
During the study, neither group of patients had abnormal liver or renal function, and there were no occurrences of adverse reactions.
Discussion
In this study, Dan’e Fukang soft extracts have performed beneficial effects on improved absorption of pelvic ascites, promoted ovarian recovery, and reduced the incidence of dysmenorrhea after oocyte retrieval of patients with OHSS, demonstrating the treating efficacy of Dan’e Fukang soft extracts on OHSS.
A patented traditional Chinese medicine, Dan’e Fukang soft extracts are composed of several medicinal ingredients such as Salviae Miltiorrhizae Radix et Rhizoma (Danshen), Notoginseng Radix et Rhizoma (Sanqi), Paeoniae Radix Rubra (Chishao), and Curcumae Rhizoma (Ezhu). The effects of these ingredients include soothing the liver and regulating the circulation of Qi, softening and resolving hard mass, promoting blood circulation and removing blood stasis, regulating menstruation, and relieving pain.15 The efficacy of Dan’e Fukang soft extracts has been widely studied. For example, Zhu et al demonstrated that Dan’e Fukang soft extracts could effectively treat endometriosis and relieve depression and anxiety in patients as compared with danazol.16 Another meta-analysis showed that Dan’e Fukang soft extracts had comparable efficacy and a better safety profile than conventional Western medicine, further highlighting the advantages of this preparation in soothing the liver and regulating the circulation of Qi, promoting blood circulation and removing blood stasis, regulating menstruation, and relieving pain.
The kidney-tonifying herbs such as Salviae Miltiorrhizae Radix et Rhizoma (Danshen) in Dan’e Fukang soft extracts have been found to enhance the phagocytic ability of natural killer (NK) cells. Further, traditional Chinese herbs with effects of activating blood circulation and removing blood stasis (such as Paeoniae Radix Rubra) that also regulate fluid circulation have been shown to be involved in increasing the numbers of leukocytes and promoting the transformation of T cells.17
A previous study has shown the action of Dan’e Fukang soft extracts on regulating the body’s immune function, mainly manifesting as softening and shrinking ectopic masses, regulating menstruation, and relieving pain.18 Besides, Dan’e Fukang soft extracts do not affect female endocrine function; on the other hand, it was shown to increase the conception rate in some patients. Adverse emotions such as depression and anxiety in patients with endometriosis could be relieved by the use of Dan’e Fukang soft extracts due to its effects on soothing the liver and regulating the circulation of Qi.19 For instance, Zhi et al found that the quality of life of patients with endometriosis improved after using Dan’e Fukang soft extracts, mainly manifesting as better health status, independence, and improved somatic and psychological function.20
Patients suffering from OHSS often exhibit signs of hepatic Qi stagnation, such as abdominal distension and gastrointestinal reactions. Results of laboratory investigations showed increased systemic capillary permeability21 in patients, resulting in the extravasation of intravascular fluid, increased intravascular blood concentration, and extravasation into the extravascular space. These findings suggest that the diagnosis of OHSS conforms to the stasis and blood stagnation explanation. Therefore, directly using Dan’e Fukang soft extracts for OHSS can provide excellent results in clinical practice.
More significantly, OHSS is a self-limiting disease. “Prevention before the onset of illness, prevention of deterioration after the onset of illness, [and] prevention of relapse after recovery” can significantly improve the clinical symptoms of OHSS with early intervention. However, if early care is not provided, the development of moderate to severe OHSS could be associated with a long duration of treatment and substantial medical costs. Therefore, early intervention should be the focus of prevention and treatment efforts in OHSS, and high-risk individuals should be closely monitored. This is consistent with the “triple prevention” principle of “prevention before the onset of disease” in TCM. Our findings in the present study demonstrate the advantage of dialectical thinking in TCM with regard to the timely treatment of OHSS with Dan’e Fukang soft extracts.22
The “Synopsis of Prescriptions of the Golden Chamber, concomitant treatment of water vapor disease according to both symptoms and pulse” states that blood stasis might result in edema. The “Blood Syndrome Theory” notes that those with blood loss may often have edema, and blood stasis can recruit fluid and also lead to edema. Therefore, it is both a blood disease and an edema. Multiple medical theories explain how a variety of causes can induce increased capillary permeability, which further results in a series of syndromes such as enlarged ovaries, pleural effusion, and ascites. From the TCM perspective, it is hypothesized that “blood disorder causes retained water” and the pathogenesis is Yin essence depletion, blood-phase disharmony, choroid obstruction, and fluid retention. Therefore, blood-fluid concomitant treatment can achieve the effects of hemostasis, promote urination, and calm the fetus.23
The pathogenesis of OHSS involves increased capillary permeability and the extravasation of intravascular fluid due to exogenous factors during ovarian hyperstimulation. From a TCM perspective, the etiology of OHSS is a loss of harmony of the collaterals, and the imbalance of blood and Yin results in bleeding. A large amount of plasma leaks into the interstitial space, further reducing blood volume and aggravating the deficiency of both Yin and blood. Yin deficiency and blood heat, together with the decoction of fluid due to the prolongation of disease, lead to stasis, which affects the blood flowing out of the vessels. The extravasation of blood into the abdomen, chest, and other areas results in effusion and induces disease.
The stasis of blood and effusion are the causes of each other, blocking the flow of Qi. If the flow of Qi is blocked in the middle and upper abdomen, this causes the abdomen to become distended. If the Qi flow is disrupted, clarity and turbidity become imbalanced, as do the transportation and transformation functions of the spleen, resulting in nausea and poor appetite. The internal stagnation of effusion from blood extravasation results in a malfunction of bladder gasification, manifesting as urinary discomfort. In addition to ascites, abdominal distension or discomfort, nausea, vomiting, and fluctuating urine output are the main clinical symptoms in OHSS.
On the one hand, the cause and effect of OHSS are interconnected, and the internal aggregation of effusion is caused by the slow flow of blood and Qi in vessels and meridians as well as the increased permeability of blood vessels. The pathology of Qifen disease is the cause and root of OHSS, while the pathology of water disease is the result and symptom of OHSS. On the other hand, effusion accumulating in the interstitial space affects blood flow and further aggravates bleeding and stasis; ie, blood stasis and effusion exacerbate each other, thereby increasing the severity of OHSS. Therefore, the essence of the pathological mechanism in OHSS is the loss of blood harmony, which manifests as blood stasis, bleeding, and deficiencies in both Yin and blood. The loss of blood harmony leads to stagnation and effusion, while the link between blood stasis and effusion can deregulate the flow of Qi, resulting in a series of clinical syndromes.24–27
In the present study, our results showed that Dan’e Fukang soft extracts had beneficial effects in terms of decreasing the volume of pelvic ascites and increasing the maximum ovarian diameter, suggesting that this preparation could promote blood circulation, remove blood stasis, soothe the liver, and act as a diuretic. Besides, we found an evident drop in the incidence of dysmenorrhea in the patients who were treated with Dan’e Fukang soft extracts, indicating that this formula was effective in regulating menstruation and relieving pain. The administration of Dan’e Fukang soft extracts for the treatment of moderate OHSS improved vascular microcirculation while exerting anti-inflammatory and sedative effects, thus fully realizing the TCM principle of “triple prevention”, that is, “prevention before the onset of illness, prevention of deterioration after the onset of illness, [and] prevention of relapse after recovery”.
In particular, the following aspects may have contributed to the possible mechanisms of Dan’e Fukang soft extracts on OHSS: (1) suppressing vascular endothelial growth factor (VEGF);28,29 (2) regulating the mediators, eg, interleukin-2 (IL-2), interleukin-6 (IL-6), interleukin-8 (IL-8), prostaglandins, elements of the ovarian renin-angiotensin system, and histamine;30,31 (3) having a non-specific analgesic effect by improving pelvic blood circulation and stimulating the release of endorphins; (4) exerting its effect on treating dysmenorrhea by inhibiting cyclooxygenase and thus decreasing the production of prostaglandins. We will continue investigating the mechanisms of action of Dan’e Fukang soft extracts on OHSS in future experiments.
Besides, the fundamental nature of “blood and fluid” in patients with OHSS might be the same. Therefore, the “simultaneous treatment of blood and fluid” was effective in curing the fundamental cause and stopping intravascular bleeding, preventing blood extravasation, and preventing OHSS via the pharmacological effect of hemostasis. Simultaneously, it could regulate Qi and activate blood, disperse blood stasis, and remove dampness (urine); the accumulated effusion was flushed out by urination, thus curing the disease.
Some limitations also existed in present study, mainly included that the potential action mechanisms as well as the biochemical parameters to demonstrate the promising clinical indications of Dan’e Fukang soft extracts for treating OHSS have not been further explored owing to the limited time, which would be carried out in the further work.
Conclusion
In the present study, we found superior therapeutic efficacy in patients in the treatment group who received Dan’e Fukang soft extracts when compared with the control group in terms of ovarian recovery, ascites absorption, and incidence of dysmenorrhea. These results indicate the benefits of using Dan’e Fukang soft extracts to relieve the clinical symptoms of OHSS and improve ultrasonographic indicators. Dan’e Fukang soft extracts had a favorable interventional effect on the outcome in these patients. Further analysis of laboratory data is needed to corroborate these promising clinical indications of Dan’e Fukang soft extracts for treating OHSS.
Abbreviation
IVF-ET, In Vitro Fertilization-Embryo Transfer; ICSI-ET, Intracytoplasmic Sperm Injection-Embryo Transfer; COH, Controlled ovarian hyperstimulation; OHSS Ovarian hyperstimulation syndrome; GnRH-a, Gonadotropin-releasing hormone agonists; GnRH-A, Gonadotropin-releasing hormone antagonists; Gn, gonadotropins; HCG, Human Chorionic Gonadotropin; E2, Estradiol; LH, Luteotropic Hormone; P, Progesterone; FSH, Follicle Stimulating Hormone; WBC, White blood cell; β-HCG, β-Human Chorionic Gonadotropin.
Ethics Approval and Consent to Participate
This study was conducted with approval from the Ethics Committee of Shanxi Maternal and Child Health Care Hospital (IRB-KY-2020-008). This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from all participants.
Funding
This study was funded by the Youth Project of Shanxi Provincial Department of Health (201301038) and Scientific Research Project of Shanxi Administration of Traditional Chinese Medicine (2020ZYYC053).
Disclosure
The authors declare that they have no conflicts of interests.
References
1. Schirmer DA, Kulkarni AD, Zhang Y, et al. Ovarian hyperstimulation syndrome after assisted reproductive technologies: trends, predictors, and pregnancy outcomes. Fertil Steril. 2020;114(3):567–578. doi:10.1016/j.fertnstert.2020.04.004
2. Şanlı C, Atilgan R, Kuloğlu T, et al. Transient receptor potential melastatin 2 ion channel activity in ovarian hyperstimulation syndrome physiopathology. Turk J Med Sci. 2021;51(2):787–795. doi:10.3906/sag-2005-297
3. Rizk B, Aboulghar M, Smitz J, Ron-El R. The role of vascular endothelial growth factor and interleukins in the pathogenesis of severe ovarian hyperstimulation syndrome. Human Reproduction Update. 1997;3(3):255–266. doi:10.1093/humupd/3.3.255
4. Pala Ş, Atilgan R, Ozkan ZS, et al. Effect of varying doses of tamoxifen on ovarian histopathology, serum VEGF, and endothelin 1 levels in ovarian hyperstimulation syndrome: an experimental study. Drug Des Devel Ther. 2015;9:1761–176
5. Kumar P, Sait SF, Sharma A, Kumar M. Ovarian hyperstimulation syndrome. J Hum Reprod Sci. 2011;4(2):70–75. doi:10.4103/0974-1208.86080
6. Tang H, Hunter T, Hu Y, Zhai SD, Sheng X, Hart RJ. Cabergoline for preventing ovarian hyperstimulation syndrome. Cochrane Database Syst Rev. 2012;15:CD008605.
7. Şanlı C, Atılgan R, Kuloğlu T, et al. The investigation of cholinergic receptor muscarinic 1 activity in the rat ovary with induced ovarian hyperstimulation. Turk J Obstet Gynecol. 2023;20(1):53–58. doi:10.4274/tjod.galenos.2023.75336
8. Tso LO, Costello MF, Albuquerque LE, Andriolo RB, Macedo CR. Metformin treatment before and during IVF or ICSI in women with polycystic ovary syndrome. Cochrane Database Syst Rev. 2014;CD006105. doi:10.1002/14651858.CD006105.pub3
9. Jacob SL, Brewer C, Tang T, Picton HM, Barth JH, Balen AH. A short course of metformin does not reduce OHSS in a GnRH antagonist cycle for women with PCOS undergoing IVF: a randomised placebo-controlled trial. Hum Reprod. 2016;31:2756–2764. doi:10.1093/humrep/dew268
10. Boothroyd C, Karia S, Andreadis N, Rombauts L, Johnson N, Chapman M. Consensus statement on prevention and detection of ovarian hyperstimulation syndrome. Aust N Z J Obstet Gynaecol. 2015;55(6):523–534. doi:10.1111/ajo.12406
11. Pfeifer S, Butts S, Dumesic D; Practice Committee of the American Society for Reproductive Medicine. Prevention and treatment of moderate and severe ovarian hyperstimulation syndrome: a guideline. Fertil Sterility. 2016;106(7):1634–1647. doi:10.1016/j.fertnstert.2016.08.048
12. Atilgan R, Pala Ş, Yavuzkır Ş, et al. What is the impact of short- and long-term supplementation of either cabergoline or clarithromycin on resolving rat ovarian hyperstimulation syndrome (OHSS) model? J Obstet Gynaecol. 2019;39(5):687–694. doi:10.1080/01443615.2018.1563774
13. Delvigne A, Rozenberg S. Epidemiology and prevention of ovarian hyperstimulation syndrome (OHSS): a review. Hum Reprod Update. 2002;8(6):559–577. doi:10.1093/humupd/8.6.559
14. Xie X, Gou W. Gynecology and Obstetrics [M].
15. KODAMAN PH. Current strategies for endometriosis management. Obstet Gynecol Clin North Am. 2015;42(1):87–101. doi:10.1016/j.ogc.2014.10.005
16. Zhu J, Zhong LY. Application of Dan’e Fukang soft extracts in the clinical treatment of endometriosis. Jilin J Chin Med. 2016;36(07):700–702.
17. Zhang ST. Clinical observation of danazol combined with reverse addition method in the treatment of endometriosis. Hebei Med J. 2013;35(15):2304–2305.
18. Zhang CE, Li JY. Observation on the therapeutic effect of Danshen Fukan decoction on endometriosis. Shi Zhen Guo Yi Guo Yao. 2008;19(6):1478–1479.
19. Kim JJ, Kurita T, Bulun SE. Progesterone action in endometrial cancer, endometriosis, uterine fibroids, and breast cancer. Endocr Rev. 2013;34(1):130–162. doi:10.1210/er.2012-1043
20. Zhi W. A qualitative study of the perception of experience during the treatment period in patients with endometriosis. J Qilu Nurs. 2015;21(14):10–12.
21. He M, Zhou Y, Liu F. Systematic review on the efficacy and safety of Danfukang soft extracts in the treatment of endometriosis. Chin J Hospital Pharm. 2012;32(07):528–534.
22. Yao L, Xie L, Gong Z, et al. Clinical study on prevention of ovarian hyperstimulation syndrome with wenyang lishuihuoxue prescription. Chin J Mod Drug App. 2020;14(11):198–200.
23. Deng LW, Mu L. Discussing the application of blood and water treatment strategy in ovarian hyperstimulation syndrome from the perspective of ”blood disorder causes retained water”. New Chin Med. 2014;46(04):8–10.
24. Teng Y. Analysis of ovarian hyperstimulation syndrome from traditional Chinese medicine perspective. J Jiangxi Tradit Chin Med. 2010;41(3):8–10.
25. Xu XH, Chen YC, Xu YL, et al. Garcinone E blocks autophagy through lysosomal functional destruction in ovarian cancer cells. World J Tradit Chin Med. 2021;7:209–216.
26. Hu YX, Zhang ZQ, Zhou QJ, Liao JY, Chai XL. Mechanism exploration of the classical traditional Chinese medicine formula huoluo xiaoling pill in clinical treatment and the traditional Chinese medicine theory “treating different diseases with the same method”: a network pharmacology study and molecular docking verification. World J Tradit Chin Med. 2022;8:131–140.
27. Liang X. Research progress of traditional Chinese medicine in the treatment of threatened abortion. J Tradit Chin Med. 2012;27(12):1663–1665.
28. Ismet H, Elif K, Gokay O, et al. Oxytocin and cabergoline alleviate ovarian hyperstimulation syndrome (OHSS) by suppressing vascular endothelial growth factor (VEGF) in an experimental model. Arch Gynecol Obstet. 2021;303(4):1099–1108. doi:10.1007/s00404-020-05855-1
29. Raoul O, Olga DS, Daniel L, et al. Interleukin-2 and SOCS-1 proteins involvement in the pathophysiology of severe ovarian hyperstimulation syndrome--a preliminary proof of concept. J Ovarian Res. 2014;7:106. doi:10.1186/s13048-014-0106-2
30. Sergio RS, Raul G, Carlos S, et al. Targeting the vascular endothelial growth factor system to prevent ovarian hyperstimulation syndrome. Hum Reprod Update. 2008;14(4):321–333. doi:10.1093/humupd/dmn008
31. Scott MN. Prevention and management of ovarian hyperstimulation syndrome. Thromb Res. 2017;151 Suppl 1:S61–S64. doi:10.1016/S0049-3848(17)30070-1
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.