")
Back to Journals » Journal of Inflammation Research » Volume 14
Efficacy and Safety of First-Generation EGFR-TKIs Combined with Chemotherapy for Treatment-Naïve Advanced Non-Small-Cell Lung Cancer Patients Harboring Sensitive EGFR Mutations: A Single-Center, Open-Label, Single-Arm, Phase II Clinical Trial
Authors Lin J, Li M , Chen S, Weng L, He Z
Received 27 March 2021
Accepted for publication 2 June 2021
Published 16 June 2021 Volume 2021:14 Pages 2557—2567
DOI https://doi.org/10.2147/JIR.S313056
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ning Quan
Jinghui Lin, Meifang Li, Shijie Chen, Lihong Weng, Zhiyong He
Department of Thoracic Medical Oncology, Fujian Medical University Cancer Hospital, Fujian Cancer Hospital, Fuzhou City, Fujian Province, 350014, People’s Republic of China
Correspondence: Zhiyong He
Department of Thoracic Medical Oncology, Fujian Medical University Cancer Hospital, Fujian Cancer Hospital, No. 420 Fuma Road, Fuzhou City, Fujian Province, 350014, People’s Republic of China
Email [email protected]
Purpose: This single-center, open-label, single-arm, phase II clinical trial aimed to examine the efficacy and safety of the first-generation EGFR-TKIs combined with chemotherapy among treatment-naïve advanced non-small-cell lung cancer (NSCLC) patients harboring sensitive EGFR mutations.
Materials and Methods: Patients with advanced EGFR-mutant NSCLC were given concurrent gefitinib (250 mg orally daily) and 3-week cycle of carboplatin plus pemetrexed for 4 to 6 cycles, followed by gefitinib maintenance until disease progression or unacceptable toxicity. The primary endpoint was progression-free survival (PFS), and the secondary endpoints were overall survival (OS), objective response rate (ORR), disease control rate (DCR) and safety. This trial was registered at ClinicalTrials.gov (NCT02886195).
Results: Of the 21 patients enrolled in this study, a 76.2% ORR and 100% DCR were observed and a higher ORR was seen in patients with EGFR 21L858R mutations than in those with 19del mutations (P = 0.012). The subjects had a median PFS of 15.0 months and a median OS of 26.0 months, and numerically longer PFS was seen in patients with EGFR 21L858R mutations than in those with 19del mutations (P = 0.281). There were 15 NSCLC patients without cerebral metastases at baseline, with 4 cases developing cerebral metastases during the treatment, and the 6-, 12- and 24-month cumulative incidence rates of the central nervous system metastasis were 6.67%, 13.3% and 26.7%, respectively. There were 17 subjects with progressive diseases tested for EGFR T790M mutations, and 11 cases were positive for T790M mutations. Grade 3 toxicity included neutropenia (9.5%), leukopenia (4.8%), liver dysfunction (9.5%) and diarrhea (4.8%), and no grade 4 adverse events or treatment-related death occurred.
Conclusion: The combination of first-generation EGFR-TKIs and chemotherapy achieves a satisfactory PFS, ORR and DCR and well-tolerated toxicity in advanced NSCLC patients with EGFR mutations, notably in patients with EGFR L858R mutations.
Keywords: non-small-cell lung cancer, EGFR-TKIs, chemotherapy, combination strategy, clinical efficacy, toxicity
Introduction
Mutation of the epidermal growth factor receptor (EGFR) gene is the most common oncogenic driver in advanced non-small-cell lung cancer (NSCLC),1 and the frequency of EGFR mutation is approximately in 50% of Asian NSCLC patients.2 During the past decade, results from multiple Phase III clinical trials have identified the first-generation EGFR-tyrosine kinase inhibitors (EGFR-TKIs), including gefitinib, erlotinib, icotinib as the first-line therapy for patients with EGFR-mutant advanced NSCLC.3–8 Increasing evidences have proved that resistance to first-generation EGFR-TKIs is inevitable in NSCLC.9–11 Although the mechanisms underlying the resistance to first-generation EGFR-TKIs have been extensively investigated in lung cancer, the underlying mechanisms remain to be illustrated.12–14 The combination of first-generation EGFR-TKIs and chemotherapy has therefore been proposed as the first-line strategy to overcome the resistance to EGFR-TKIs in NSCLC.15–17
Previous clinical trials have shown that the treatment strategy of first-generation EGFR-TKIs combined with chemotherapy is effective to delay the resistance to first-generation EGFR-TKIs.18–20 However, there are still many questions that remain to be answered, such as the combination treatment on the development of acquired EGFR T790M mutation-positive clones, the difference between the efficacy of the combination treatment for NSCLC harboring sensitive EGFR mutations of 19del and 21L858R, and the prophylactic effect of the combination therapy for intracranial metastases. To solve these clinical issues, this single-center, open-label, single-arm, prospective phase II clinical trial was therefore designed with aims to examine the efficacy and safety of first-generation EGFR-TKIs combined with chemotherapy for treatment-naïve advanced NSCLC patients harboring sensitive EGFR mutations, so as to provide insights into the optimization of the first-line treatment regimen containing first-generation EGFR-TKIs plus chemotherapy.
Subjects and Methods
Study Subjects
Patients with stage IV NSCLC harboring activating EGFR exon 19 deletion or exon 21 L858R point mutations that met the following criteria were recruited, Eastern Cooperative Oncology Group performance status (ECOG-PS) score of 0 to 2, ages of 20 to 75 years, sufficient organ functions and no previous systemic treatment, and patients with central nervous system (CNS) metastases whose conditions were neurologically stable were also eligible. Those with serious concomitant systemic disorders like interstitial pneumonia or another primary malignancy, or pregnant women were excluded from the trial. This trial has been registered at ClinicalTrials.gov (NCT02886195).
Study Design
This study was a single-center, open-label, single-arm, phase II clinical trial. Patients received concurrent gefitinib (250 mg orally daily) and carboplatin dosed to a target area under the free carboplatin plasma concentration versus time curve (AUC) of 5 × (day 1)/pemetrexed (500 mg/m2, day 1) once every 3-week cycle for 4 to 6 cycles, followed by gefitinib maintenance until disease progression, unacceptable toxicity, or death. Patients with brain metastases at baseline were allowed to receive synchronous whole-brain palliative radiotherapy.
Outcomes Measure
The primary endpoint was progression-free survival (PFS), which was defined as the duration from patient enrolment to disease progression or death from any cause,21 and the secondary endpoints were toxicity, overall survival (OS), which was defined as the duration from patient enrolment to date of death from any cause, and clinical tumor response, including objective response (defined as complete [CR] or partial response [PR]) and disease control (defined as CR, PR, or stable disease [SD]).21
Clinical Assessments
Radiological assessments were performed with CT or magnetic resonance imaging (MRI) at baseline and every 6 weeks until disease progression according to the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1.21 After disease progression, survival data were collected every 12 weeks until death or withdrawal from the trial. Treatment-related toxicity was assessed according to the Common Terminology Criteria for Adverse Events (CTCAE) version 4.0 issued by the National Cancer Institute.22 The highest toxicity grade for each patient in all cycles of chemotherapy was included in the final toxicity analysis.
Detection of EGFR Mutations
All specimens were obtained by biopsy from primary or metastatic tumors. EGFR mutation was detected in biopsy specimens using the amplification refractory mutation system PCR (ARMS-PCR) assay prior to enrollment.23 After disease progression, plasma circulating tumor DNA (ctDNA) analysis for detection of the EGFR T790M mutation was performed using droplet digital PCR (ddPCR) assay.24
Statistics
All statistical analyses were performed using the statistical software SPSS version 22.0 (SPSS, Inc.; Chicago, IL, USA). Fisher’s exact test was employed for inter-group comparisons of objective response rate (ORR) and disease control rate (DCR). The PFS and OS were estimated using the Kaplan-Meier method and compared using the Log rank test. A P-value of <0.05 was considered statistically significant.
Results
Patient Characteristics
A total of 21 advanced, treatment-naïve NSCLC patients harboring sensitive EGFR mutations were enrolled during the period from April 2015 through October 2017, and all cases were pathologically diagnosed with lung adenocarcinoma. The subjects had a median age of 52 years (range, 32 to 70 years), and included 10 men and 11 women. There were 19 patients with an ECOG-PS score of 1 and two cases with a score of 2, and 85.7% were non-smokers. ARMS-PCR assay was done in all subjects, and identified EGFR 19del mutations in 10 cases and 21L858R mutations in 11 cases. 66.7% completed 4 cycles of chemotherapy and 33.3% completed 6 cycles. In addition, there were 15 cases without brain metastases and 6 cases with brain metastases at initial diagnosis, including 3 cases with concurrent whole-brain radiotherapy (Table 1 and Supplementary Table 1). All 21 patients were successfully followed up through the visits to the hospital or telephone, with the final database lock on June 1, 2020. The study subjects had a median follow-up period of 26 months (range, 5 to 62 months), and during the follow-up period, 95.2% of the patients progressed and 76.2% died (Supplementary Table 2).
 |
Table 1 Clinical Responses to First-Generation EGFR-TKIs Combined with Chemotherapy in Advanced NSCLC Patients Harboring EGFR Mutations by Demographic and Clinical Characteristics |
Survival Benefits
Among the 21 participants, there were 16 cases achieving PR and 5 achieving SD, with a 76.2% ORR and 100% DCR observed. Figure 1 shows the best response to the combined treatment of first-generation EGFR-TKIs and chemotherapy. A significantly higher ORR was seen in subjects harboring EGFR 21L858R mutations than in those with EGFR 19del mutations (100% vs 50%, P = 0.012), while no heterogeneity occurred with respect to gender, age, brain metastasis or depth of response (DpR) (P > 0.05) (Table 1).
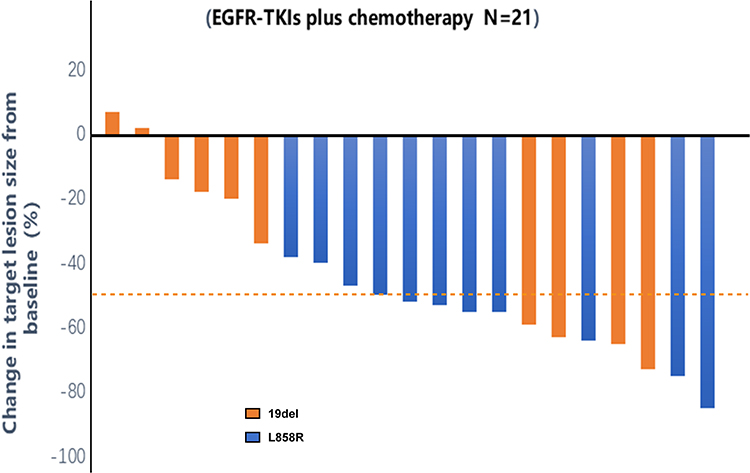 |
Figure 1 Maximum tumor change from baseline by the best overall response, as per Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1, each bar represents the maximum change in the sum of the diameters of the target lesions of an individual patient. |
At the final database lock, 95.2% experienced PFS outcomes and 76.2% had OS outcomes. The median PFS and OS were 15.0 months (95% CI, 10.6‒19.4 months) and 26.0 months (95% CI, 24.5‒27.4 months) (Figure 2A and B), and no heterogeneity was seen across the gender, age, type of EGFR mutations, development of brain metastasis or DpR (P > 0.05) (Table 1). In addition, there were no significant differences in PFS (12.0 vs 15.0 months, P = 0.281) or OS (26.0 vs 25.0 months, P = 0.876) between advanced NSCLC patients harboring EGFR 19del mutations and 21L858R mutations (Figure 2C and D).
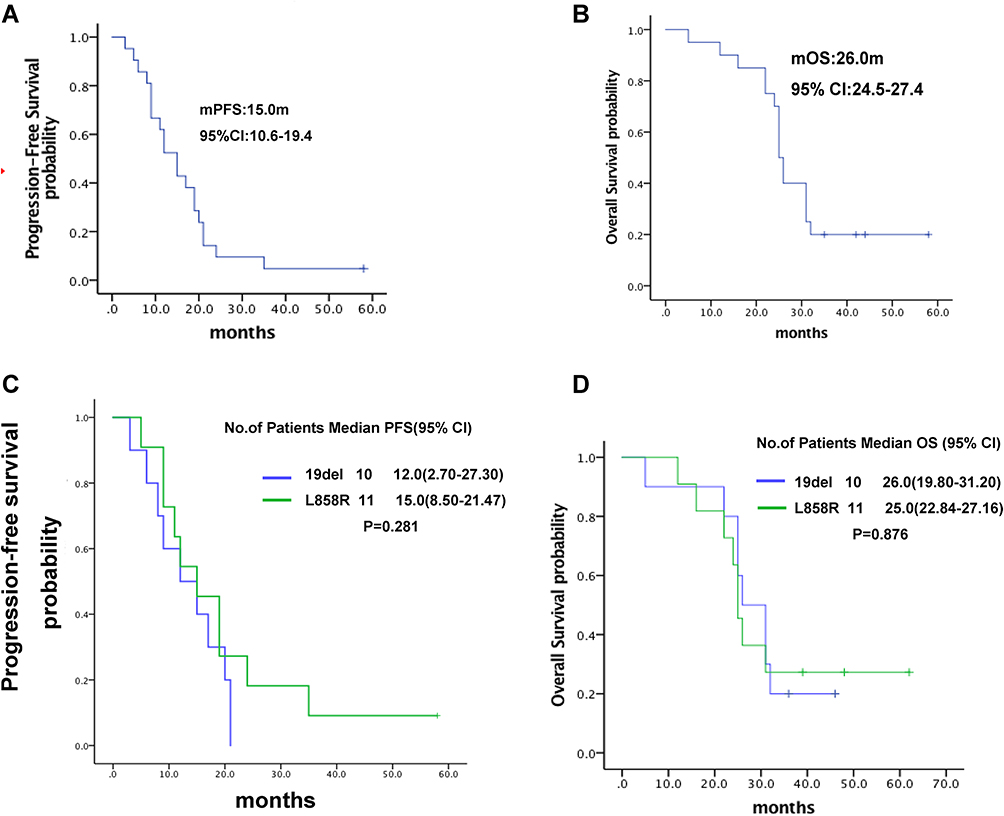 |
Figure 2 Kaplan-Meier estimates of survival. (A) Progression-free survival; (B) overall survival; (C) comparison of progression-free survival between advanced NSCLC patients harboring EGFR 19del and L858R mutations; (D) comparison of overall survival between advanced NSCLC patients harboring EGFR 19del and L858R mutations. |
Efficacy of First-Generation EGFR-TKIs Combined with Chemotherapy for Brain Metastasis
There were 6 cases with brain metastases at baseline. The time to intracranial progression was 19, 19 and 24 months for the 3 cases receiving first-generation EGFR-TKIs plus chemotherapy with concurrent whole-brain radiotherapy, and 9, 15 and 17 months for those receiving first-generation EGFR-TKIs plus chemotherapy. The median PFS and OS were 18.0 and 28.0 months among these 6 cases, respectively.
Among the 15 participants without brain metastasis at baseline, 4 cases (26.7%) developed intracranial metastases and had PFS of 6, 9, 21 and 21 months. The 6-, 12- and 24-month cumulative incidence rates of the CNS metastases were 6.67%, 13.3% and 26.7% and the median PFS and OS were 12.0 and 26.0 months among these 15 cases, respectively.
Efficacy of First-Generation EGFR-TKIs Combined with Chemotherapy Against the Development of Acquired EGFR T790M Mutation-Positive Clones
There were 17 participants that were subject to ddPCR assay for detection of EGFR T790M mutations in the plasma, and 64.7% were tested positive for T790M mutations. We observed no significant difference in the incidence of acquired T790M mutations between advanced NSCLC patients harboring EGFR 19del mutations and 21L858R mutations (75.0% vs 55.6%, P = 0.62). There were 8 participants undergoing the later-line treatment with osimertinib, which resulted in PR in 5 cases, SD in 3 cases, showing a 60% ORR and a 100% DCR, and the PFS was 5.0, 3.0, 4.0, 6.0, 6.0, 9.0, 5.0, and 21.0 months for these 8 cases, with a median PFS of 6.0 months.
Safety
The participants were well tolerant to the combined treatment with first-generation EGFR-TKIs and chemotherapy, and the common adverse reactions included rash (81%), neutropenia (81%), leukopenia (66.7%), liver function damage (52.4%), fatigue (47.6%) and diarrhea (23.8%). Rash and fatigue were all classified as grade 1 and 2. Grade 3 hematological toxicity included neutropenia (9.5%) and leukopenia (4.8%), and grade 3 non-hematological toxicity mainly included liver function damage (9.5%) and diarrhea (4.8%). No grade 4 adverse events occurred, and no treatment-related death was found (Table 2).
 |
Table 2 Toxicities During the Treatment with First-Generation EGFR-TKIs in Combination with Chemotherapy in Advanced NSCLC Patients Harboring EGFR Mutations |
Discussion
Increasing evidences from large-scale clinical trials have shown that first-generation EGFR-TKIs achieve unsatisfactory outcomes for treatment of advanced NSCLC patients harboring sensitive EGFR mutations, resulting in median PFS of 9.2 to 11.3 months and median OS of 26.3 to 38.8 months.25–27 The combination therapy containing EGFR-TKIs has therefore been proposed in order to improve the survival benefits and delay the resistance to EGFR-TKIs in lung cancer,28–30 and the combination of EGFR-TKIs and chemotherapy is a preferred option of choice.31–33 In a Phase 2, multicenter, randomized study conducted in East Asian patients with advanced nonsquamous NSCLC harboring EGFR mutations, the gefitinib-pemetrexed combination was found to improve median PFS (16.2 vs 11.1 months) and OS (43.4 vs 36.8 months) in relative to gefitinib alone.34 Results from the NEJ009 study showed that gefitinib combined with carboplatin plus pemetrexed achieved an increase in PFS (20.9 vs 18.0 months, P = 0.092) and OS (50.9 vs 38.8 months, P = 0.021) as compared to treatment with gefitinib alone in newly diagnosed metastatic NSCLC patients with EGFR mutations.19 However, the effects of combined treatment with first-generation EGFR-TKIs and chemotherapy on the development of EGFR T790M mutation-positive clones, on the efficacy of advanced NSCLC harboring different types of sensitive EGFR mutations, and on intracranial metastases remain unknown until now.
This single-center, open-label, single-arm, prospective phase II clinical trial, initiated since April 2015, aimed to test the efficacy and safety of gefitinib, a first-generation EGFR-TKI, in combination with carboplatin plus pemetrexed as a first-line therapy for advanced NSCLC patients with sensitive EGFR mutations. The combination therapy achieved an overall ORR of 76.2%, DCR of 100%, median PFS of 15.0 months and median OS of 26.0 months among all 21 participants, and no significant differences were seen in PFS or OS in terms of gender, age, type of EGFR mutations, development of brain metastasis or DpR (P > 0.05). During the follow-up to June 1, 2020, no treatment-related death or grade 4 adverse events occurred, and grade 3 hematological toxicity included neutropenia (9.5%) and leukopenia (4.8%), while grade 3 non-hematological toxicity mainly included liver function damage (9.5%) and diarrhea (4.8%). Our data demonstrate that the combined treatment of gefitinib, carboplatin and pemetrexed is safe and well tolerant in advanced NSCLC patients with sensitive EGFR mutations, which is in agreement with the tolerated adverse reactions observed in the NEJ009 study.19
In this phase 2 clinical trial, gefitinib in combination with carboplatin plus pemetrexed was found to achieve comparable PFS in relative to the combined treatment with other first-generation EGFR-TKIs and chemotherapy, and showed superior PFS than treatment with first-generation EGFR-TKIs alone,18–20,31–33 indicating that the combining strategy of first-generation EGFR-TKIs and chemotherapy is effective to postpone the resistance to first-generation EGFR-TKIs. In metastatic NSCLC patients receiving a targeted treatment with an ALK inhibitor or immunotherapy with an anti-PD-1 antibody, a greater DpR was reported to correlate with longer PFS and OS,35 which is similar to the findings from the NEJ009 study.19 In the current study, 57.1% of the participants had a DpR of 50% and greater, and the greater DpR did not lead to PFS or OS benefits. However, our data presented inferior OS to that reported in recent clinical trials.19,34 This may be because the current study is a real-world clinical trial, and the confounding effects of the subsequent therapy may affect the OS; in addition, the small sample size may cause a bias.
Exon 19 deletion and exon 21 L858R point mutations are the two most common subtypes of EGFR mutations in NSCLC.36 It has been reported that NSCLC patients harboring EGFR 19del and 21L858R mutations present diverse biological profiles, clinical features and prognoses,37 and previous studies have demonstrated various responses to first-generation EGFR-TKIs between NSCLC patients harboring EGFR 19del and 21L858R mutations.38–44 Results from a meta-analysis of 22 eligible trials involving 1082 patients showed that advanced NSCLC patients harboring EGFR 19del mutations had longer OS and PFS than those with 21L858R mutations,45 which may be explained partly by the higher proportion of the EGFR T790M mutation in patients with EGFR 19del mutations.46 However, the exact mechanisms responsible for the difference in the responses to EGFR-TKIs between advanced NSCLC patients with EGFR 19del and 21L858R mutations remain to be investigated. Optimizing the treatment regimen to improve better survival benefits is therefore paid much attention among advanced NSCLC patients harboring sensitive EGFR 21L858R mutations,47 and the combination strategy with first-generation EGFR-TKIs and chemotherapy has shown improvements in the therapeutic efficacy in advanced NSCLC patients harboring sensitive EGFR 21L858R mutations.19,20,34 Among chemotherapy-naïve, East Asian patients with advanced nonsquamous NSCLC and activating EGFR 21L858R mutations, the gefitinib-pemetrexed combination achieved superior PFS than gefitinib alone (12.6 vs 10.9 months, HR = 0.58).20 In the current study, gefitinib in combination with carboplatin plus pemetrexed achieved a significantly higher ORR in advanced NSCLC patients harboring EGFR 21L858R mutations than in those with EGFR 19del mutations, and the combination therapy resulted in improvements in PFS (median PFS of 15 months) as compared to previous reports seen in first-generation EGFR-TKIs alone in advanced NSCLC patients with EGFR 21L858R mutations.19,20 Our findings demonstrate that the combining strategy of first-generation EGFR-TKIs and chemotherapy is effective to achieve better PFS benefits in advanced NSCLC patients with EGFR 21L858R mutations. This may be attributed to that the proportion of concurrent mutations is higher in advanced NSCLC patients with EGFR 21L858R mutations than in those with 19del mutations, and the combination strategy may facilitate the removal of EGFR-mutant clones and the delay in the emergence of resistance to EGFR-TKIs.48,49
Although EGFR-TKIs have shown highly active against EGFR-mutant NSCLC, resistance to EGFR-TKIs seems inevitable.9–11 To date, EGFR T790M mutation has been identified as the most common cause of secondary resistance to first-generation EGFR-TKIs.50–52 Previous studies have detected 50% to 60% T790M mutation-positive rates in NSCLC specimens that are resistant to first-generation EGFR-TKIs,48,53 while the plasma T790M mutation positive rate is 23% to 63% in NSCLC patients harboring resistance to first-generation EGFR-TKIs.54,55 Osimertinib, a third-generation EGFR-TKI, is effective to selectively inhibit EGFR T790M mutations and significantly prolong the survival in NSCLC patients with EGFR mutations.56–58 The effects of first-generation EGFR-TKIs combined with chemotherapy on EGFR T790M mutations have not been fully understood until now. In this study, ddPCR assay detected a 64.7% plasma EGFR T790M mutation-positive rate following disease progression in advanced NSCLC patients undergoing gefitinib combined with carboplatin plus pemetrexed, which is greater than previous findings reported in the plasma of NSCLC patients with resistance to first-generation EGFR-TKIs.59–62 This suggests that the combining strategy of first-generation EGFR-TKIs and chemotherapy facilitates the clearance of heterogeneous tumor clones, leading to a higher clonal homogeneity of EGFR T790M-positive and EGFR-TKIs resistant NSCLC. However, further studies recruiting more study subjects are required to validate the findings from this trial, since the small study sample may cause a bias in the present study. In addition, there were 8 EGFR T790M-positive patients undergoing osimertinib therapy in this study, which resulted in a 60% ORR and a 100% DCR, suggesting the reliability of detection of EGFR T790M mutation in peripheral ctDNA by ddPCR assay. We found that osimertinib achieved a median PFS of 6 months in these 8 EGFR T790M mutation-positive patients, which is significantly shorter than that reported in the AURA3 study.63 This may be because the small sample size affects the study results, and the tumor heterogeneity and complicated mechanisms of drug resistance may affect the efficacy of osimertinib treatment in EGFR T790M mutation-positive, advanced NSCLC patients.64–66
Brain metastasis has been identified as a major contributor to treatment failure and death in EGFR-mutant lung adenocarcinoma patients after treatment with first-generation EGFR-TKIs,67 and development of treatments to overcome CNS metastasis of NSCLC has been paid great attention.68,69 Results from a retrospective analysis to compare the efficacy of erlotinib and gefitinib as first-line treatment for CNS metastasis in NSCLC patients with EGFR-sensitizing mutations showed that the 6-, 12- and 18-month cumulative incidence rates of CNS progression were 5.8%, 9.4% and 17% for the gefitinib treatment group.70 In patients with EGFR-mutant advanced NSCLC without baseline CNS metastasis given first- and/or third-generation EGFR-TKIs, the 1-, 2-, and 3-year cumulative incidences of symptomatic CNS metastasis were 3.5%, 7.5%, and 15.3%, respectively.71 Results from the NEJ009 study showed that gefitinib combined with carboplatin plus pemetrexed resulted in survival benefits from PFS and OS benefits relative to gefitinib alone in newly diagnosed metastatic NSCLC patients with EGFR mutations regardless of brain metastasis at baseline; however, the effects of the combination therapy on brain metastasis and the incidence of subsequent brain metastasis were not reported.19 In this study, the 6-, 12- and 24-month cumulative incidence rates of the CNS metastasis were 6.67%, 13.3% and 26.7% in 15 advanced NSCLC patients following treatment with gefitinib combined with carboplatin plus pemetrexed. Our data showed no superiority of the combination strategy of first-generation EGFR-TKIs and chemotherapy in the prevention of CNS metastasis relative to EGFR-TKIs alone in advanced NSCLC patients with EGFR mutations as reported previously. It has been reported that the combination of systemic therapy and whole-brain radiotherapy achieves better benefits in managing the intracranial progression in NSCLC patients with baseline brain metastases.72 Similarly, our findings showed that the time to intracranial progression was 19, 19 and 24 months for participants with concurrent whole-brain radiotherapy.
This study has some limitations. First, this is a single-center, single-arm clinical trial enrolling 21 advanced NSCLC patients with EGFR mutations, and the small sample size may cause a bias. Second, this real-world study started to recruit study subjects in 2015. ARMS-PCR assay was employed to detect EGFR mutations at baseline, which failed to detect baseline concomitant mutations, and next-generation sequencing was not employed to investigate the mechanisms underlying drug resistance after disease progression following treatment with first-generation EGFR-TKIs. Third, further identification of dominant subjects and illustration of the effect of the combination treatment on clonal evolution of NSCLC, notably on EGFR T790M mutation-positive clones, are required during the development of the combination strategy of first-generation EGFR-TKIs and chemotherapy. Further large-scale, multi-center, controlled clinical trials recruiting more subjects to validate the findings from this study seem justified.
Conclusions
In summary, this single-center, open-label, single-arm, phase II clinical trial further confirms that the combination of first-generation EGFR-TKIs and chemotherapy is a well-tolerant first-line treatment to delay EGFR-TKIs resistance among advanced NSCLC patients harboring sensitive EGFR-TKI mutations, and better survival benefits may be achieved in advanced NSCLC patients harboring EGFR L858R mutations.
Data Sharing Statement
All data reported in this study are available upon request by contact with the corresponding author.
Ethical Statement
This study was approved by the Ethical Review Committee of Fujian Provincial Cancer Hospital, and all procedures were performed in accordance with the Declaration of Helsinki, as well as international and national laws, regulations and guidelines. Written informed consent was obtained from all participants following a detailed description of the purpose and potential benefits from the study.
Acknowledgments
We would like to thank all subjects participating in this study, and sincere thanks are also delivered to the three anonymous reviewers for their kind and suggestive comments on the manuscript.
Funding
This study was supported by the grants from Wu Jieping Medical Foundation (grant no. 320.6799.15006), Fujian Provincial Science & Technology Guiding Project (grant no. 2018Y0017), Joint Funds for the Innovation of Science and Technology, Fujian Province (grant no. 2017Y9080), and the Startup Fund for Scientific Research of Fujian Medical University (grant no. 2017XQ1217).
Disclosure
The authors declare no conflicts of interest.
References
1. Harrison PT, Vyse S, Huang PH. Rare epidermal growth factor receptor (EGFR) mutations in non-small cell lung cancer. Semin Cancer Biol. 2020;61:167–179. doi:10.1016/j.semcancer.2019.09.015
2. Midha A, Dearden S, McCormack R. EGFR mutation incidence in non-small-cell lung cancer of adenocarcinoma histology: a systematic review and global map by ethnicity (mutMapII). Am J Cancer Res. 2015;5(9):2892–2911.
3. Fukuoka M, Wu YL, Thongprasert S, et al. Biomarker analyses and final overall survival results from a Phase III, randomized, open-label, first-line study of gefitinib versus carboplatin/paclitaxel in clinically selected patients with advanced non-small-cell lung cancer in Asia (IPASS). J Clin Oncol. 2011;29(21):2866–2874. doi:10.1200/JCO.2010.33.4235
4. Zhou C, Wu YL, Chen G, et al. Final overall survival results from a randomised, phase III study of erlotinib versus chemotherapy as first-line treatment of EGFR mutation-positive advanced non-small-cell lung cancer (OPTIMAL, CTONG-0802). Ann Oncol. 2015;26(9):1877–1883. doi:10.1093/annonc/mdv276
5. Shi YK, Wang L, Han BH, et al. First-line icotinib versus cisplatin/pemetrexed plus pemetrexed maintenance therapy for patients with advanced EGFR mutation-positive lung adenocarcinoma (CONVINCE): a Phase 3, open-label, randomized study. Ann Oncol. 2017;28(10):2443–2450. doi:10.1093/annonc/mdx359
6. Mitsudomi T, Morita S, Yatabe Y, et al. Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): an open label, randomised phase 3 trial. Lancet Oncol. 2010;11(2):121–128. doi:10.1016/S1470-2045(09)70364-X
7. Han JY, Park K, Kim SW, et al. First-SIGNAL: first-line single-agent iressa versus gemcitabine and cisplatin trial in never-smokers with adenocarcinoma of the lung. J Clin Oncol. 2012;30(10):1122–1128. doi:10.1200/JCO.2011.36.8456
8. Inoue A, Kobayashi K, Maemondo M, et al. Updated overall survival results from a randomized phase III trial comparing gefitinib with carboplatin-paclitaxel for chemo-naïve non-small cell lung cancer with sensitive EGFR gene mutations (NEJ002). Ann Oncol. 2013;24(1):54–59. doi:10.1093/annonc/mds214
9. Westover D, Zugazagoitia J, Cho BC, Lovly CM, Paz-Ares L. Mechanisms of acquired resistance to first- and second-generation EGFR tyrosine kinase inhibitors. Ann Oncol. 2018;29(suppl_1):i10–i19. doi:10.1093/annonc/mdx703
10. Ralki M, Maes B, Pat K, Wynants J, Cuppens K. Triple trouble: a case of multiple resistance mechanisms after first generation EGFR-TKI in NSCLC. Case Rep Oncol. 2019;12(2):625–630. doi:10.1159/000502214
11. Otsubo K, Sakai K, Takeshita M, et al. Genetic profiling of non-small cell lung cancer at development of resistance to first- or second-generation EGFR-TKIs by CAPP-Seq analysis of circulating tumor DNA. Oncologist. 2019;24(8):1022–1026. doi:10.1634/theoncologist.2019-0101
12. Karachaliou N, Codony-Servat J, Bracht JWP, et al. Characterising acquired resistance to erlotinib in non-small cell lung cancer patients. Expert Rev Respir Med. 2019;13(10):1019–1028. doi:10.1080/17476348.2019.1656068
13. Kobayashi N, Katakura S, Kamimaki C, et al. Resistance mechanisms of epidermal growth factor receptor tyrosine kinase inhibitors in non-small cell lung cancer patients: a meta-analysis. Thorac Cancer. 2021;12(7):1096–1105. doi:10.1111/1759-7714.13878
14. Nagano T, Tachihara M, Nishimura Y. Mechanism of resistance to epidermal growth factor receptor-tyrosine kinase inhibitors and a potential treatment strategy. Cells. 2018;7(11):212. doi:10.3390/cells7110212
15. Del Re M, Crucitta S, Gianfilippo G, et al. Understanding the mechanisms of resistance in EGFR-positive NSCLC: from tissue to liquid biopsy to guide treatment strategy. Int J Mol Sci. 2019;20(16):3951. doi:10.3390/ijms20163951
16. Gao J, Li HR, Jin C, Jiang JH, Ding JY. Strategies to overcome acquired resistance to EGFR TKI in the treatment of non-small cell lung cancer. Clin Transl Oncol. 2019;21(10):1287–1301. doi:10.1007/s12094-019-02075-1
17. Lim SM, Syn NL, Cho BC, Soo RA. Acquired resistance to EGFR targeted therapy in non-small cell lung cancer: mechanisms and therapeutic strategies. Cancer Treat Rev. 2018;65:1–10. doi:10.1016/j.ctrv.2018.02.006
18. Sugawara S, Oizumi S, Minato K, et al. Randomized phase II study of concurrent versus sequential alternating gefitinib and chemotherapy in previously untreated non-small cell lung cancer with sensitive EGFR mutations: NEJ005/TCOG0902. Ann Oncol. 2015;26(5):888–894. doi:10.1093/annonc/mdv063
19. Hosomi Y, Morita S, Sugawara S, et al.; North-East Japan Study Group. Gefitinib alone versus gefitinib plus chemotherapy for non-small-cell lung cancer with mutated epidermal growth factor receptor: NEJ009 Study. J Clin Oncol. 2020;38(2):115–123. doi:10.1200/JCO.19.01488
20. Cheng Y, Murakami H, Yang PC, et al. Randomized phase II trial of gefitinib with and without pemetrexed as first-line therapy in patients with advanced nonsquamous non-small-cell lung cancer with activating epidermal growth factor receptor mutations. J Clin Oncol. 2016;34(27):3258–3266. doi:10.1200/JCO.2016.66.9218
21. Choi HC, Kim JH, Kim HS, et al. Comparison of the RECIST 1.0 and RECIST 1.1 in non-small cell lung cancer treated with cytotoxic chemotherapy. J Cancer. 2015;6(7):652–657. doi:10.7150/jca.11794
22. Ott PA, Elez E, Hiret S, et al. Pembrolizumab in patients with extensive-stage small-cell lung cancer: results from the phase Ib KEYNOTE-028 Study. J Clin Oncol. 2017;35(34):3823–3829. doi:10.1200/JCO.2017.72.5069
23. Little S. Amplification-refractory mutation system (ARMS) analysis of point mutations. Curr Protoc Hum Genet. 2001. doi:10.1002/0471142905.hg0908s07
24. Li C, He Q, Liang H, et al. Diagnostic accuracy of droplet digital PCR and amplification refractory mutation system PCR for detecting EGFR mutation in cell-free DNA of lung cancer: a meta-analysis. Front Oncol. 2020;10:290. doi:10.3389/fonc.2020.00290
25. Li YX, Yang JY, Xu YF, et al. A meta-analysis of the comparing of the first-generation and next-generation TKIs in the treatment of NSCLC. Math Biosci Eng. 2019;16(5):5687–5696. doi:10.3934/mbe.2019283
26. Pilotto S, Rossi A, Vavalà T, et al. Outcomes of first-generation EGFR-TKIs against non-small-cell lung cancer harboring uncommon EGFR mutations: a post hoc analysis of the BE-POSITIVE study. Clin Lung Cancer. 2018;19(1):93–104. doi:10.1016/j.cllc.2017.05.016
27. Pluzanski A, Krzakowski M, Kowalski D, Dziadziuszko R. Real-world clinical outcomes of first-generation and second-generation epidermal growth factor receptor tyrosine kinase inhibitors in a large cohort of European non-small-cell lung cancer patients. ESMO Open. 2020;5(6):e001011. doi:10.1136/esmoopen-2020-001011
28. Yoneda K, Imanishi N, Ichiki Y, Tanaka F. Treatment of non-small cell lung cancer with EGFR-mutations. J UOEH. 2019;41(2):153–163. doi:10.7888/juoeh.41.153
29. Xu R, Shao H, Zhu J, Ju Q, Shi H. Combination strategies based on epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors for cancer patients: pooled analysis and subgroup analysis of efficacy and safety. Medicine. 2019;98(13):e14135. doi:10.1097/MD.0000000000014135
30. Iwama E, Nakanishi Y, Okamoto I. Combined therapy with epidermal growth factor receptor tyrosine kinase inhibitors for non-small cell lung cancer. Expert Rev Anticancer Ther. 2018;18(3):267–276. doi:10.1080/14737140.2018.1432356
31. Zhang Z, Zeng K, Zhao S, et al. Pemetrexed/carboplatin plus gefitinib as a first-line treatment for EGFR-mutant advanced nonsmall cell lung cancer: a Bayesian network meta-analysis. Ther Adv Med Oncol. 2019;11:1758835919891652. doi:10.1177/1758835919891652
32. Rebuzzi SE, Alfieri R, La Monica S, Minari R, Petronini PG, Tiseo M. Combination of EGFR-TKIs and chemotherapy in advanced EGFR mutated NSCLC: review of the literature and future perspectives. Crit Rev Oncol Hematol. 2020;146:102820. doi:10.1016/j.critrevonc.2019.102820
33. Wang S, Gao A, Liu J, Sun Y. First-line therapy for advanced non-small cell lung cancer with activating EGFR mutation: is combined EGFR-TKIs and chemotherapy a better choice? Cancer Chemother Pharmacol. 2018;81(3):443–453. doi:10.1007/s00280-017-3516-1
34. Yang JC, Cheng Y, Murakami H, et al. A randomized phase 2 study of gefitinib with or without pemetrexed as first-line treatment in nonsquamous NSCLC with EGFR mutation: final overall survival and biomarker analysis. J Thorac Oncol. 2020;15(1):91–100. doi:10.1016/j.jtho.2019.09.008
35. McCoach CE, Blumenthal GM, Zhang L, et al. Exploratory analysis of the association of depth of response and survival in patients with metastatic non-small-cell lung cancer treated with a targeted therapy or immunotherapy. Ann Oncol. 2017;28(11):2707–2714. doi:10.1093/annonc/mdx414
36. da Cunha Santos G, Shepherd FA, Tsao MS. EGFR mutations and lung cancer. Annu Rev Pathol. 2011;6:49–69. doi:10.1146/annurev-pathol-011110-130206
37. Castellanos E, Feld E, Horn L. Driven by mutations: the predictive value of mutation subtype in EGFR-mutated non-small cell lung cancer. J Thorac Oncol. 2017;12(4):612–623. doi:10.1016/j.jtho.2016.12.014
38. Zhou J, Ben S. Comparison of therapeutic effects of EGFR-tyrosine kinase inhibitors on 19Del and L858R mutations in advanced lung adenocarcinoma and effect on cellular immune function. Thorac Cancer. 2018;9(2):228–233. doi:10.1111/1759-7714.12568
39. Zhuo M, Zheng Q, Zhao J, et al. Survival difference between EGFR Del19 and L858R mutant advanced non-small cell lung cancer patients receiving gefitinib: a propensity score matching analysis. Chin J Cancer Res. 2017;29(6):553–560. doi:10.21147/j.issn.1000-9604.2017.06.10
40. Deng W, Lei Y, Liu S, et al. Comparing overall survival between first generation EGFR-TKIs and chemotherapy in lung cancer patients with Del19/L858R. Chin J Cancer Res. 2016;28(3):339–347. doi:10.21147/j.issn.1000-9604.2016.03.08
41. Koyama N, Watanabe Y, Iwai Y, et al. Distinct benefit of overall survival between patients with non-small-cell lung cancer harboring EGFR exon 19 deletion and exon 21 L858R substitution. Chemotherapy. 2017;62(3):151–158. doi:10.1159/000454944
42. Zhang Y, Sheng J, Kang S, et al. Patients with exon 19 deletion were associated with longer progression-free survival compared to those with L858R mutation after first-line EGFR-TKIs for advanced non-small cell lung cancer: a meta-analysis. PLoS One. 2014;9(9):e107161. doi:10.1371/journal.pone.0107161
43. Zhou S, Hu X, Wang Y, et al. Clinicopathologic characteristics and outcome of patients with different EGFR mutations. Asia Pac J Clin Oncol. 2019;15(3):166–171. doi:10.1111/ajco.13072
44. Liu HL, Han G, Peng M, et al. Efficacy of EGFR tyrosine kinase inhibitors in non-small cell lung cancer patients harboring different types of EGFR mutations: a retrospective analysis. J Huazhong Univ Sci Technolog Med Sci. 2017;37(6):864–872. doi:10.1007/s11596-017-1819-4
45. Wang H, Huang J, Yu X, et al. Different efficacy of EGFR tyrosine kinase inhibitors and prognosis in patients with subtypes of EGFR-mutated advanced non-small cell lung cancer: a meta-analysis. J Cancer Res Clin Oncol. 2014;140(11):1901–1909. doi:10.1007/s00432-014-1709-0
46. Ke EE, Zhou Q, Zhang QY, et al. A higher proportion of the EGFR T790M mutation may contribute to the better survival of patients with exon 19 deletions compared with those with L858R. J Thorac Oncol. 2017;12(9):1368–1375. doi:10.1016/j.jtho.2017.05.018
47. Chmielecki J, Foo J, Oxnard GR, et al. Optimization of dosing for EGFR-mutant non-small cell lung cancer with evolutionary cancer modeling. Sci Transl Med. 2011;3(90):90ra59. doi:10.1126/scitranslmed.3002356
48. Yu HA, Arcila ME, Rekhtman N, et al. Analysis of tumor specimens at the time of acquired resistance to EGFR-TKI therapy in 155 patients with EGFR-mutant lung cancers. Clin Cancer Res. 2013;19(8):2240–2247. doi:10.1158/1078-0432.CCR-12-2246
49. Camidge DR, Pao W, Sequist LV. Acquired resistance to TKIs in solid tumours: learning from lung cancer. Nat Rev Clin Oncol. 2014;11(8):473–481. doi:10.1038/nrclinonc.2014.104
50. Huang L, Fu L. Mechanisms of resistance to EGFR tyrosine kinase inhibitors. Acta Pharm Sin B. 2015;5(5):390–401. doi:10.1016/j.apsb.2015.07.001
51. Lu X, Yu L, Zhang Z, Ren X, Smaill JB, Ding K. Targeting EGFRL858R/T790M and EGFRL858R/T790M/C797S resistance mutations in NSCLC: current developments in medicinal chemistry. Med Res Rev. 2018;38(5):1550–1581. doi:10.1002/med.21488
52. Wu SG, Shih JY. Management of acquired resistance to EGFR TKI-targeted therapy in advanced non-small cell lung cancer. Mol Cancer. 2018;17(1):38. doi:10.1186/s12943-018-0777-1
53. Sequist LV, Waltman BA, Dias-Santagata D, et al. Genotypic and histological evolution of lung cancers acquiring resistance to EGFR inhibitors. Sci Transl Med. 2011;3(75):75ra26. doi:10.1126/scitranslmed.3002003
54. Passaro A, Guerini-Rocco E, Pochesci A, et al. Targeting EGFR T790M mutation in NSCLC: from biology to evaluation and treatment. Pharmacol Res. 2017;117:406–415. doi:10.1016/j.phrs.2017.01.003
55. Li H, Wang J, Zhang G, et al. Detection of plasma T790M mutation after the first generation EGFR-TKI resistance of non-small cell lung cancer in the real world. J Thorac Dis. 2020;12(3):550–557. doi:10.21037/jtd.2019.12.122
56. Soria JC, Ohe Y, Vansteenkiste J, et al. FLAURA investigators. Osimertinib in untreated EGFR-mutated advanced non-small-cell lung cancer. N Engl J Med. 2018;378(2):113–125. doi:10.1056/NEJMoa1713137
57. Al-Quteimat OM, Amer AM. A review of osimertinib in NSCLC and pharmacist role in NSCLC patient care. J Oncol Pharm Pract. 2020;26(6):1452–1460. doi:10.1177/1078155220930285
58. Malapelle U, Ricciuti B, Baglivo S, et al. Osimertinib. Recent Results Cancer Res. 2018;211:257–276.
59. Nishikawa S, Kimura H, Koba H, et al. Selective gene amplification to detect the T790M mutation in plasma from patients with advanced non-small cell lung cancer (NSCLC) who have developed epidermal growth factor receptor tyrosine kinase inhibitor (EGFR-TKI) resistance. J Thorac Dis. 2018;10(3):1431–1439. doi:10.21037/jtd.2018.01.144
60. Zhang S, Zhu L, Xia B, et al. Epidermal growth factor receptor (EGFR) T790M mutation identified in plasma indicates failure sites and predicts clinical prognosis in non-small cell lung cancer progression during first-generation tyrosine kinase inhibitor therapy: a prospective observational study. Cancer Commun (Lond). 2018;38(1):28.
61. Chan DLH, Toh GLX, Goh LL. Clinical implementation of plasma EGFR T790M testing using droplet digital PCR in TKI-resistant NSCLC patients. Exp Mol Pathol. 2020;116:104515. doi:10.1016/j.yexmp.2020.104515
62. Xiong L, Cui S, Ding J, et al. Dynamics of EGFR mutations in plasma recapitulates the clinical response to EGFR-TKIs in NSCLC patients. Oncotarget. 2017;8(38):63846–63856. doi:10.18632/oncotarget.19139
63. Mok TS, Wu Y-L, Ahn M-J, et al. AURA3 Investigators. Osimertinib or platinum-pemetrexed in EGFR T790M-positive lung cancer. N Engl J Med. 2017;376(7):629–640.
64. Takeda M, Nakagawa K. First- and second-generation EGFR-TKIs are all replaced to osimertinib in chemo-Naive EGFR mutation-positive non-small cell lung cancer? Int J Mol Sci. 2019;20(1):146. doi:10.3390/ijms20010146
65. Choo JR, Tan CS, Soo RA. Treatment of EGFR T790M-positive non-small cell lung cancer. Target Oncol. 2018;13(2):141–156. doi:10.1007/s11523-018-0554-5
66. Russo A, Franchina T, Ricciardi GRR, et al. Third generation EGFR TKIs in EGFR-mutated NSCLC: where are we now and where are we going. Crit Rev Oncol Hematol. 2017;117:38–47. doi:10.1016/j.critrevonc.2017.07.003
67. Joo JW, Hong MH, Shim HS. Clinical characteristics of T790M-positive lung adenocarcinoma after resistance to epidermal growth factor receptor-tyrosine kinase inhibitors with an emphasis on brain metastasis and survival. Lung Cancer. 2018;121:12–17. doi:10.1016/j.lungcan.2018.04.013
68. Shetty V, Babu S. Management of CNS metastases in patients with EGFR mutation-positive NSCLC. Indian J Cancer. 2019;56(Supplement):S31–S37. doi:10.4103/ijc.IJC_455_19
69. Ahluwalia MS, Becker K, Levy BP. Epidermal growth factor receptor tyrosine kinase inhibitors for central nervous system metastases from non-small cell Lung cancer. Oncologist. 2018;23(10):1199–1209. doi:10.1634/theoncologist.2017-0572
70. Li MX, He H, Ruan ZH, et al. Central nervous system progression in advanced non-small cell lung cancer patients with EGFR mutations in response to first-line treatment with two EGFR-TKIs, gefitinib and erlotinib: a comparative study. BMC Cancer. 2017;17(1):245. doi:10.1186/s12885-017-3165-0
71. Zhou Y, Wang B, Qu J, et al. Survival outcomes and symptomatic central nervous system (CNS) metastasis in EGFR-mutant advanced non-small cell lung cancer without baseline CNS metastasis: osimertinib vs. first-generation EGFR tyrosine kinase inhibitors. Lung Cancer. 2020;150:178–185. doi:10.1016/j.lungcan.2020.10.018
72. He ZY, Li MF, Lin JH, Lin D, Lin RJ. Comparing the efficacy of concurrent EGFR-TKI and whole-brain radiotherapy vs EGFR-TKI alone as a first-line therapy for advanced EGFR-mutated non-small-cell lung cancer with brain metastases: a retrospective cohort study. Cancer Manag Res. 2019;11:2129–2138. doi:10.2147/CMAR.S184922
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.