")
Back to Journals » Infection and Drug Resistance » Volume 17
Effects of Maternal Health During Pregnancy and Child Immunization on Mother-to-Child Transmission of Hepatitis B Virus: A Multicentre, Large-Sample Study in Southeast China
Authors Huang XX, Lin Q, Li Y, Li L
Received 25 October 2023
Accepted for publication 19 February 2024
Published 13 March 2024 Volume 2024:17 Pages 989—1001
DOI https://doi.org/10.2147/IDR.S443172
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi Ruan
Xin-Xin Huang,1 Quan Lin,2 Yun Li,2 Li Li2
1The Ministry of Health, Fujian Maternity and Child Health Hospital, College of Clinical Medicine for Obstetrics & Gynecology and Pediatrics, Fujian Medical University, Fuzhou, Fujian Province, People’s Republic of China; 2Department of Obstetrics, Fujian Maternity and Child Health Hospital, College of Clinical Medicine for Obstetrics & Gynecology and Pediatrics, Fujian Medical University, Fuzhou, Fujian Province, People’s Republic of China
Correspondence: Li Li, Email [email protected]
Purpose: High hepatitis B infection rates in China are a major public health issue, and mother-to-child transmission (MTCT) is a significant risk factor.
Patients and Methods: This study was conducted with a prospective multicentre design from January 2021 to December 2022 in 245 hospitals providing midwifery services in southeastern China. The participants were pregnant women who were positive for hepatitis B surface antigen (HBs Ag) and their children. The HBs Ag concentration was tested in children aged 8– 12 months. The odds ratio for each risk factor was calculated by logistic regression analysis, and the decision tree model was used.
Results: A total of 5369 children born to hepatitis B-infected mothers between 8 and 12 months of age were enrolled, among whom 81 (1.51%) were positive for HBsAg. The risk factors for hepatitis B infection in 5369 children under one-year-old were a high intrauterine hepatitis B exposure level, a history of hepatitis B immunoglobulin (HBIG) delay beyond 12 hours after birth, and lack of full hepatitis B vaccine (HepB), with risks of 3.356 (1.223~9.209), 5.691 (1.931~16.773), and 5.137 (2.265~11.650), respectively. The discrimination accuracy of the decision tree was 98.5%. The risk factors for hepatitis B infection in 4542 children under one year old with high exposure risk were nonstandard treatment by the mother during pregnancy, HBIG delay beyond 12 hours after birth, and no complete HepB administration, with risks of 2.925 (1.063– 8.047), 5.354 (1.806– 15.871) and 5.147 (2.258– 11.733), respectively. The discrimination accuracy of the decision tree was 98.3%.
Conclusion: To prevent mother-to-child transmission of hepatitis B, it is necessary to standardize the treatment of pregnant women with a high exposure risk of hepatitis B, implement combined vaccination within 12 hours of birth, and standardise the full course of HepB.
Keywords: hepatitis B, prevention of mother-to-child transmission, risk factors, risk of exposure, decision tree
Introduction
Hepatitis B virus (HBV) infection is one of the world’s most serious public health problems. A total of 296 million people are chronically infected with HBV.1 During the perinatal period, HBV is mainly transmitted to infants through the mother’s blood and body fluids.2 Without intervention, 70–90% of infants born to mothers positive for hepatitis B antigen will develop chronic infection.3 The Global Burden of Disease study found that, in contrast to the overall trend of a decreasing burden of other infectious diseases, disability-adjusted life-years (DALYs) due to the long-term sequelae of chronic hepatitis B (CHB) are generally increasing.4
A large proportion of those infected with the HBV are women of childbearing age. In countries with a high incidence of CHB (≥8%), the main routes of transmission are perinatal (>20%) and early childhood infection (>60%).5 In the absence of vaccination, more than 50% of infections occur in childhood and adolescence, and more than 20% are due to perinatal morbidity associated with HBV infection.6,7
Mother-to-child transmission (MTCT) is one of the leading causes of chronic hepatitis B infection and related mortality worldwide.8 MTCT is responsible for 30–50% of HBV transmission in China.2 Therefore, the prevention of MTCT and the elimination of the main transmission route of HBV are essential measures for the eradication of this disease. In 2016, the World Health Organization (WHO) launched the Global Health Sector Strategy on Viral Hepatitis 2016–2021, which focused on eliminating viral hepatitis as a significant public health threat by 2030.9 The prevention of MTCT is one of the five core areas of this strategic plan, aimed at achieving a rate of <0.1% of HBV infection in children under five years of age.9 China is set to play a vital role in achieving the global goal of eradicating hepatitis B by 2030.
Routine vaccination is the most effective way to eliminate hepatitis B in newborns.10 To prevent MTCT of hepatitis B and control the epidemic of hepatitis B, the WHO recommends hepatitis B vaccine (HepB) within 24 hours of birth. China introduced a policy of providing free hepatitis B immunoglobulin (HBIG) to children exposed in utero to the HBV, and used three doses of HepB in the free immunisation programme for all children. According to the national strategy, three doses of the HepB are required for the whole vaccination course, following the 0-1-6 month program, ie, vaccine 1 at birth and vaccines 2 and 3 at one month and six-month intervals. After 18 years of implementation, the program effectively reduced the number of new hepatitis B infections among children nationwide.11 The prevalence of hepatitis B surface antigen (HBs Ag) in children under five was 0.32% in 2014, a 97% decrease from the number of prevaccination years.12 In the present study area, the prevalence of HBV in children under 15 years of age reached a low level (0.5%),13 which indicates the effectiveness of the HepB in reducing the rate of HBV infection.
Despite this great success, more than 50,000 Chinese infants may acquire chronic HBV infection at birth each year.14 Despite adequate HBIG and HepB at birth, 4–10% of neonatal cases after exposure prophylaxis fail.15 A serological study of children born to HBV-infected mothers after three doses of HepB in four provinces in China showed that 91% of infants were anti-HBs positive, suggesting that almost 10% had no evidence of immunity to HBV infection.16 Therefore, vaccination alone is not sufficient for the prevention of infection in children.16 We hypothesized that, in addition to vaccination, the status of HBV infection in children under one year of age was related to maternal pregnancy status.
We conducted this study among pregnant women infected with HBV and babies that were delivered in Fujian Province, Southeast China. We analyzed the pregnancy status of the infants’ mothers and children’s HBs Ag test results. We assessed the incidence of MTCT and associated risks. We report our analysis and recommendations.
Materials and Methods
Study Design
This prospective multicenter study was conducted between January 2021 and December 2022 in 245 healthcare facilities providing midwifery services in southeastern China.
Study Population and Specimen Collection
All pregnant women were tested for HBs Ag, anti-HBS, hepatitis B e antigen (HBe Ag), anti-HBe, and anti-HBc. The detection methods used were enzyme-linked immunosorbent assays. The government fully funded the cost of testing. If conditions permit, pregnant women with positive HBs Ag should be quantitatively tested for HBV DNA. The HBV DNA test uses HBV-specific primers and HBV probes (TAMRA) for real-time qPCR analysis of DNA samples.
Treatment During Pregnancy
For pregnant women with a serum HBV DNA concentration ≥2×105 IU/mL, based on informed consent, antiviral therapy was started at 28 weeks of pregnancy. Pregnant women with an HBV DNA concentration >2×109 IU/mL can be created on antiviral therapy at 24 weeks of gestation. If the HBV DNA test is unavailable or no test result is available, antiviral treatment can be started at 28 weeks of gestation based on the positive outcome of HBe Ag. The therapy was tenofovir disoproxil fumarate (TDF).
Inclusion and Exclusion Criteria
The inclusion criteria were HBs Ag-positive pregnant women and single liveborn individuals who agreed to have their children followed up and were tested for HBs Ag between 8 and 12 months of age. There were no exclusion criteria.
Benefits for Study Participants
With special funding from the Chinese government, all pregnant women are not required to pay for hepatitis B marker testing during pregnancy, and all newborns receive three doses of 0-1-6 HepB free of charge. Infants born to HBV-infected mothers receive HBIG free of charge.
Assessment of Sociodemographic Data
Standardized case registration cards were used to collect self-reported information on age, place of residence, marital status, level of education, occupation, and parity from HBs Ag-positive mothers. Through hospital record review, newborn registration review, and parent-held infant vaccination records, we obtained the child’s date of birth, gender, birth weight, and HBIG and HepB status.
Index Definition
Hepatitis B-Exposed Children
Children born to mothers infected with HBV.
Hepatitis B Exposure Level
If the mother’s HBV DNA concentration was > 2*105 IU/mL, she was considered to have high exposure. If the mother was not tested for HBV DNA during pregnancy, the child whose mother was HBe Ag positive was defined as having high HBV exposure, and the rest were defined as having normal exposure.
Diagnostic Criteria for MTCT of HBV Infection
HBs Ag status was evaluated in infants aged 8–12 months. If the HBs Ag was positive, MTCT was confirmed.
Postbirth and Follow-Up
The children were tested for HBs Ag by contacting their guardians via a mobile phone or home address during the 8–12 months of life. The method was as follows: 3~5 mL of venous blood was extracted and centrifuged at 2000 RPM/min, after which the serum was collected and stored at −80°C. The detection methods used were enzyme-linked immunosorbent assay or chemiluminescence immunoassay.
Statistical Analysis
All the statistical analyses were performed using IBM SPSS Version 27.0 software. Following normality, continuous variables are presented as the mean ± standard deviation or median (interquartile range), and they were compared using a t-test or Wilcoxon rank-sum test. The chi-square test or Fisher’s exact probability method was used to compare counted data. We fitted logistic regression models with children’s HBs Ag level as a binary outcome to calculate odds ratios (ORs) and 95% CIs. The decision tree decision (DT) was selected based on the input element. A value of p ≤ 0.05 was considered to indicate a significant difference.
Sample Size
PASS V.15.0 was used to calculate sample sizes for two-group comparisons. The sample size was calculated according to the proportion of children with high HBV intrauterine exposure in the positive group (with MTCT) and negative group (without MTCT). We adopted an 80% study power, 95% confidence interval (CI), and a 5% alpha error. Therefore, we reached a sample size of no less than 213 children, 71 in the HBs Ag positive group and 142 in the HBs Ag negative group.
Results
The technology roadmap is shown in Figure 1. A total of 5546 HBs Ag-positive pregnant women were enrolled in the study, and 5369 single children with HBs Ag test results were tracked. Among 5369 pregnant women, the mean age was 31.420±4.196 years. A total of 5272 (98.19%) were cohabiting or married. In terms of maximum education level attained, 1542 (28.72%) had completed junior high school or below education, 1574 (29.32%) had completed senior secondary education, and 2253 (41.96%) had completed a bachelor’s or higher education. There were 3106 (57.85%) patients who underwent hepatitis B DNA testing during pregnancy.
 |
Figure 1 Technology roadmap. A total of 5546 HBsAg-positive pregnant women were enrolled in this study. Among them, 140 women with twin or multiple births or stillbirths were excluded, and 37 women were lost to follow-up after delivery. Final inclusion of 5369 pregnant women and their singleton liveborn children. |
Analysis of 5369 HBV-Exposed Children
5369 HBsAg-exposed children aged 8–12 months were enrolled, including 2904 males (54.09%) and 2465 females (45.91%). Eighty-one children (1.51%) were HBs Ag positive, and 5288 (98.49%) were HBs Ag negative. Five children did not receive HBIG due to immediate rescue after birth, and 42 children did not receive the first dose of HepB during hospitalization due to rescue or low birth weight. Ninety-two children did not receive three doses of HepB due to illness or because of the parents’ schedule.
Univariate Analysis
The chi-square or rank-sum test was performed with the HBs Ag test results of children aged 8–12 months as the dependent variable and the series of possible influencing factors as the independent variables. The results showed that high intrauterine exposure to hepatitis B, HBIGand the first dose of HepB delayed until more than 12 hours after birth and no total of three doses of HepB were associated with MTCT of hepatitis B. Mothers who did not receive standard treatment during pregnancy, gender, gestational age at birth, birth weight, or mode of delivery were not significantly associated with MTCT.
Multivariable Logistic Regression
We subsequently performed multivariable logistic regression analysis with the univariate meaningful independent variables. The regression method was used to screen variables (excluding standard p=0.15). A high risk of hepatitis B exposure in utero, delayed HBIG exposure more than 12 hours after birth, and incomplete vaccination with three doses of HepB were risk factors for HBV infection in children younger than one year. Compared with that in children with normal intrauterine exposure, the risk of HBV infection in children with high intrauterine exposure was 3.356 (1.223 to 9.209) times more significant. The risk of HBV infection in children who received the first dose after 12 hours of birth was 5.691 (1.931–16.773) times that of those within 12 hours of birth. The risk of HBV infection in children who were not vaccinated according to the standardized “0-1-6” procedure was 5.137 (2.265–11.650) times greater than that in children vaccinated according to the standardized procedure, as shown in Table 1.
 |
Table 1 Analysis of Hepatitis B Infection Risk in Children Exposed to Hepatitis B |
Decision Tree
The chi-square test was used to compare each independent variable with the target variable, with a group (1= negative, 2= positive) as the dependent variable. The independent variable that showed the most significant difference was chosen as the first level of the tree structure. Each category of the target variable was used as a node in the first level. The chi-square test was then performed on other variables at each node to create subsequent levels of hierarchy and nodes. The panel displays the node hierarchy, with negative nodes (red) and positive nodes (blue) plotted in ascending order of node degree. The highest node degree level is at the top, and nodes at the same horizontal level have the same degree. The decision tree attained an accuracy of 98.5%. Figure 2 illustrates the structure of the decision tree.
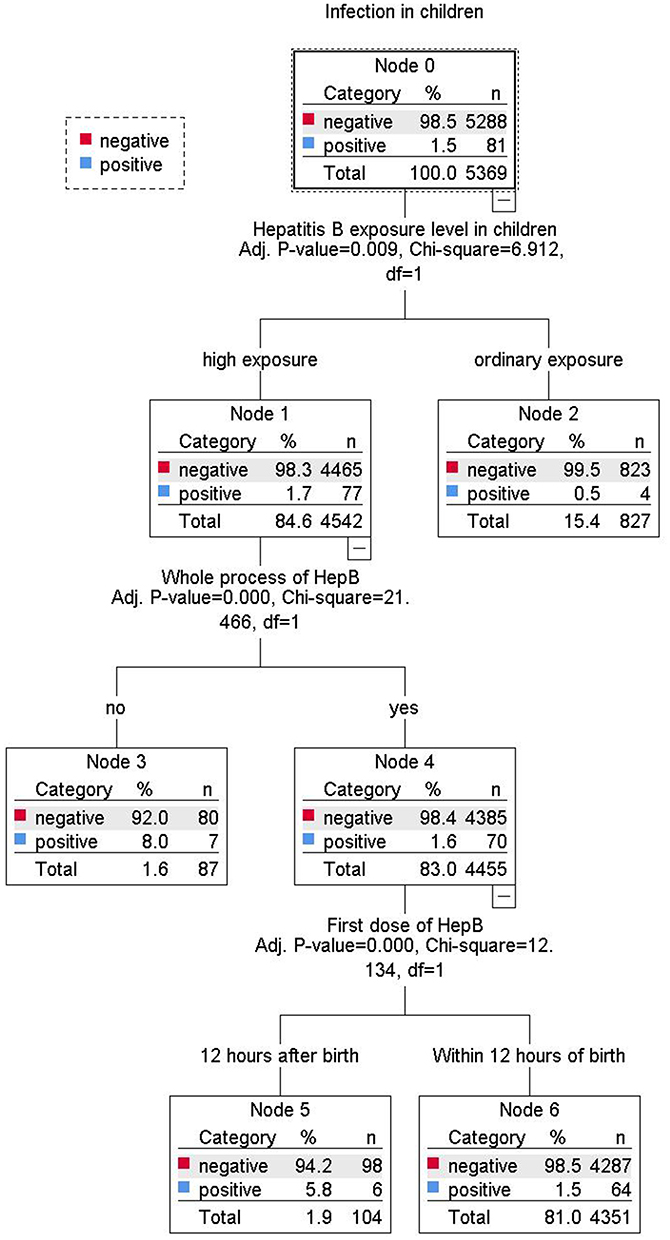 |
Figure 2 Decision tree architectural diagram for 5369 HBV-exposed children. |
Analysis of 4542 Children with High HBV Exposure
Univariate Analysis
With HBs Ag test results in children aged 8–12 months as the dependent variable, a separate analysis of the characteristics of 4542 children with high hepatitis B exposure revealed that the mother did not receive standard treatment during pregnancy, HBIG and the first dose of the HepB were delayed until more than 12 hours after birth, and no complete vaccination of three doses of HepB was associated with MTCT, as shown in Table 2.
 |
Table 2 Analysis of Hepatitis B Infection Risk in Children with High Exposure to Hepatitis B |
Multivariable Logistic Regression
Variables with statistical significance according to univariate analysis were further analyzed via multivariable logistic regression. The regression method was used to screen variables (excluding standard p=0.15). Among the children at high risk of HBV exposure, the risk factors for HBV infection in children were mothers receiving irregular treatment during pregnancy, HBIG delayed until more than 12 hours after birth, and incomplete vaccination with three doses of HepB. The ORs were 2.925 (1.063–8.047), 5.354 (1.806–15.871), and 5.147 (2.258–11.733), respectively, as shown in Table 2.
Decision Tree
The decision tree analysis method was the same as above. The decision tree achieved an accuracy of 98.3%, and the structure of the decision tree is shown in Figure 3.
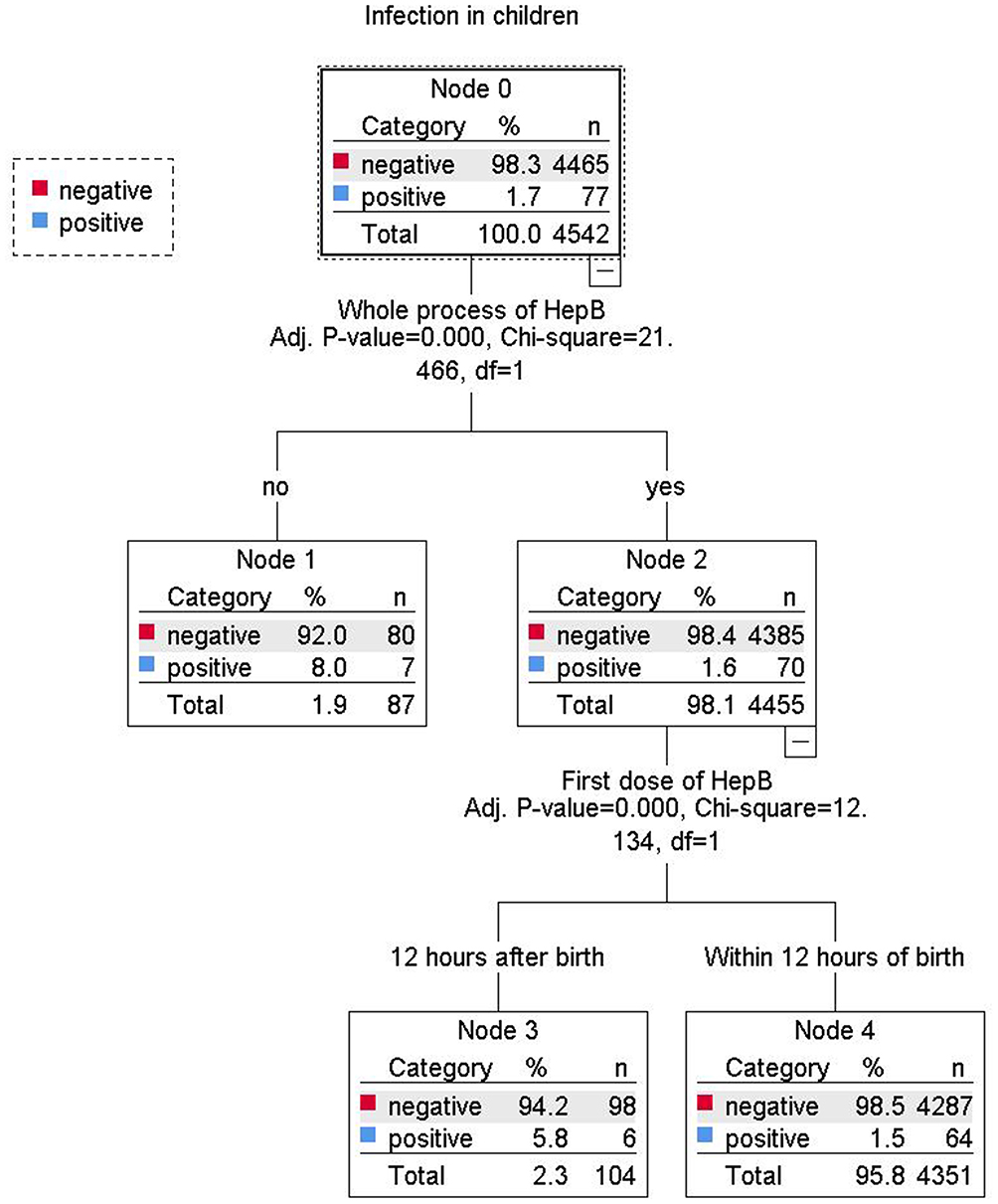 |
Figure 3 Architectural diagram of the decision tree for 4542 children with high HBV exposure. |
Discussion
The transmission routes of HBV mainly include blood, mother-to-child, and sexual contact. The frequency of HBV infection varies worldwide.17 The regions of the world with the highest rates of HBV infection are concentrated in Asia and Africa.18 High prevalence areas were defined as those with an Ag-positive proportion of HBs of at least 8%. Areas of moderate prevalence were limited to those with a positive rate of 5% to 7.99%. Low prevalence areas were defined as those with a positive rate of less than 5%.18,19 HBV infection is a significant health problem in China. Currently, the seroprevalence of HBs Ag in the general population in China is 5–7%.1,20,21 For women of childbearing age, the seroprevalence rate of HBs Ag is 4.87–9.51%.22,23
As the primary route of HBV transmission, MTCT accounts for 40–50% of chronic infections,24 which means that there is also high pressure to prevent MTCT of hepatitis B.
To prevent MTCT, all infants should receive HepB as soon as possible after birth.25 According to the Advisory Committee on Immunization Practices (ACIP), it is recommended that infants born to mothers who test positive for HBs Ag receive the HepB birth dose and HBIG. It protects newborns from infection when administered. A study of hepatitis B exposure in 551 children in China showed that maternal HBs Ag, HBe Ag double-positive, and noncombined birth immunization (HBIG and first dose of HepB) were risk factors for MTCT of HBV.26
Slightly different from the findings in the literature, 99.91% (5364/5369) of the children in this study were vaccinated with HBIG, whereas none of the neonates who were not immunized with HBIG received the first dose of HepB during hospitalization; therefore, we did not analyze the combined immune effects of HepB and HBIG. A prospective observational cohort study was conducted in China to follow up on infants born to HBs Ag-positive mothers at seven months and older. That study revealed that delayed vaccination was independently associated with immunoprophylaxis failure (OR=4.14, 95% CI=1.00–17.18).27 Univariate analysis in this study showed that the rate of HBs Ag positivity at one year was lower in children who received HBIG and the first dose of HepB within 12 hours of birth than in those who received the vaccine after 12 hours. However, in the multivariable logistic regression, the timing of the first dose of the HepB was not entered into the regression equation to account for the synergistic effect of the variables. Based on our study data, it is recommended that obstetricians and neonatologists develop or adjust the timing of the first dose of HepB or HBIG, stockpile sufficient amounts of HepB and HBIG in advance according to the expected date of delivery, regularly train in vaccination for nurses in labor wards and maternity wards, and manage the prognosis to ensure that eligible children are vaccinated on time within 12 hours after birth. It is best given immediately after delivery in the operating room or delivery room. For children referred to the neonatology department for treatment, neonatologists need to assess the condition promptly, reasonably assess contraindications to vaccination, and, if necessary, request a consultation with a public health physician so that neonatal immunization cannot be directly vetoed because of referral to the department for treatment.
The American Society for Maternal-Fetal Medicine (SMFM) considers it essential to complete a three-dose series of HepB for maximum newborn protection and recommends it for all infants regardless of maternal HBV infection status.28 Another study in the study area revealed that among children under 15 years of age, the percentages of patients with positive anti-HBs and anti-HBe antibodies in the whole vaccination group were more significant than those in the nonfull vaccination group.13 We found that failure to follow the whole “0-1-6” HepB schedule was a risk factor for MTCT of hepatitis B, which is consistent with the above findings. The current vaccination rate for hepatitis B among children in China is more than 99%, but a small number of children still do not receive the vaccine regularly. We suggest that in the future, vaccination clinics and hospitals providing routine medical check-ups for children should share data regularly to enhance the health promotion and mobilization of unvaccinated children. We focused on follow-up visits for children with irregular residence ring locations and used big data platforms for timely tracking to ensure timely vaccination. However, in our study, we included only children under 1 year of age who were delivered by HBs Ag-positive mothers and collected HBs Ag results only for children. The WHO and the Western Pacific Region emphasize that postvaccination serological testing (PVST) of infants born to HBs Ag-positive mothers is essential for determining the effectiveness of the prevention of MTCT.28 In the future, additional follow-up studies of the serological data of children at different ages are needed to clarify the protective effect of the entire course of HepB on children with intrauterine hepatitis B exposure. Additionally, depending on the antibody titer, immunization is boosted if necessary.
HBV transmission occurs in 4–10% of immunized persons despite widespread passive and active immunoprophylaxis at birth.15,29 A risk factor for vaccination failure is a high viral load of the mother’s HBV. Previous studies have shown that pregnant women with high levels of HBV DNA have an increased risk of MTCT.30 HBV infection occurs in approximately 8–15% of infants born to hypervolemic mothers.31 Serological tests were also conducted on infants born to HBs Ag-positive mothers in four provinces of China. The results showed that infants born to HBe Ag-positive mothers had a greater risk of being HBsAg-positive than those born to HBe Ag-negative mothers (OR =5.6, 95% CI=2.7–11.5).16 A study conducted in Tanzania revealed that the mothers of children with a high viral load tested positive for HBe Ag with a high degree of sequence similarity, indicating vertical transmission.5 According to the results of the systematic evaluation and meta-analysis, HBe Ag-positive pregnant women have a high failure rate of MTCT interruption.32 Our study also supported the above conclusion that children whose mothers had high DNA levels or were HBe Ag positive were at increased risk of MTCT. However, our study differs from the above mentioned studies in that we preferred to define a maternal DNA level greater than 2*105 IU/mL during pregnancy as high exposure, and only when there was no condition for checking DNA did we use HBe Ag positivity instead. HBV DNA in the serum is a reliable marker of active HBV replication, while HBe Ag indicates active HBV replication.33 The presence of HBeAg during pregnancy increases the risk of vertical transmission of hepatitis B from unvaccinated individuals 31% to 85%.34 The HBV DNA test is not widely available because it is expensive and requires high laboratory expertise.14 A systematic review and meta-analysis in 2021 showed that the implementation rate of HBV-DNA testing was only 36.6% (95% CI, 28.3–45.3%) globally and 31.6% in China.35 In our current study in southeastern China, the detection rate of HBV DNA was 57.85%, higher than in previous reports. However, a significant proportion of infected pregnant women still do not have access to HBV DNA. To prevent MTCT, the use of HBe Ag positivity as an indicator for antiviral therapy in HBV-infected pregnant women should be considered when HBV DNA testing is unavailable.35 It is recommended that pathway management be strengthened in obstetrics in the future and that doctors assess the risk of intrauterine HBV exposure in fetuses immediately after HBs Ag positivity is detected and that in hospitals without the capacity to test for HBV DNA, HBeAg can be used as a substitute. Obstetricians develop pregnancy treatments based on the exposure risk level of the fetus and standardize pregnancy management and treatment modalities for HBs Ag-positive pregnant women with high fetal exposure risk levels.
We did not find an association between treatment during pregnancy and the rate of MTCT of hepatitis B in our analyses of all the samples. Considering that mothers with low HBV DNA levels or HBe Ag negativity during pregnancy are rarely treated and to control for confounding factors, we analyzed data from children with high exposure to hepatitis B separately. The absence of standardized treatment during pregnancy was a risk factor for detecting MTCT of hepatitis B, with a risk of 2.925. Unlike what has been reported, our data reveal the magnitude of the risk of MTCT of hepatitis B in the absence of standardized treatment during pregnancy and delayed or missing childhood immunization. Although the risk of standardized treatment during pregnancy was lower than that of vaccination, these findings confirm the phenomenon observed in our clinical work, whereby children remain infected with HBV after receiving HBIG and three doses of HepB. Thus, treatment during pregnancy for mothers of children at high risk of hepatitis B exposure is an issue that needs to be considered by obstetricians. In a prospective observational study in Egypt, at least a 3-log reduction in maternal viral load at birth was observed in women receiving lamivudine during pregnancy, demonstrating comparable infant protection.36 Previous studies in China have shown that in HBe Ag-positive pregnant women with an HBV viral load >2*105 IU/mL, no transmission was detected in those who received TDF therapy during their third trimester.37 In early pregnancy, before the placenta is formed, HBV can directly infect the fetus. Once the placenta is formed, maternal comorbidities or complications during pregnancy can also compromise the placental barrier and lead to intrauterine HBV infection of the fetus. Intrauterine transmission is a cause of childhood immunization failure that cannot be ignored. Treatment during pregnancy may stop intrauterine HBV infection. Real-world studies have demonstrated that pregnant women at high risk for transmission can be identified, and antiviral therapy can be used with increased efficacy in preventing transmission. TDF is classified as a category B drug and is considered safer than lamivudine for pregnancy.38 Its effectiveness has been confirmed for mothers or infants who were followed up for 24 to 28 weeks.37 Similar results were obtained in our study, which showed that the absence of standardized treatment for mothers during pregnancy increased the risk of MTCT of hepatitis B, as did the lack of full immunization and delayed HBIG. Prevention of MTCT of hepatitis B should be combined with pregnancy care in the future, and HBs antigen, anti-HBS, HBe Ag, and anti-HBc detection should be carried out as soon as possible in early pregnancy. The hepatitis B viral load should be retested at mid-pregnancy, if available, to determine the level of risk of fetal exposure reasonably. For pregnant women at high risk of exposure, a reasonable treatment timing and regimen should be chosen based on the viral load threshold, standard antiviral therapy should be initiated, and multidisciplinary consultation with hepatologists/gastroenterologists should be provided as necessary. If possible, the extent of the reduction in HBV DNA during pregnancy should be periodically reviewed, and the treatment regimen should be adjusted as appropriate.
Decision tree is a predictive method used in machine learning. Based on the decision tree model used in this study, it is possible to predict in advance the probability of HBs Ag positivity in children. In addition, managing high-risk children should be incorporated in conjunction with routine child health care services, the frequency of follow-up visits should increase, and immunization should be strengthened when necessary.
Advantage
This study has several strengths. First, we conducted a multicentre study involving multiple hospitals in China, where hepatitis B has a high incidence. Second, our study focused on the accuracy of the data, which were based on a high-quality database obtained from a prospective study. Information on each mother–infant pair was recorded and verified, reducing the risk of error and bias. Third, we adjusted the data using multivariate logistic regression analysis to ensure reliable estimates. Fourth, we had a sufficiently large sample size to follow up on the detection of HBs Ag in children under one-year-old, providing sufficient evidence for the analysis of the MTCT rate of hepatitis B and its influencing factors.
Limitations
We acknowledge that this study has limitations. We analyzed the serology of hepatitis B-infected pregnant women in the study area during the same period, and the positivity rate of the HBe antigen was 23%. Mothers with high HBV DNA levels or HBe antigen positivity during pregnancy have better compliance with child follow-up and serological testing due to particular concerns about their child’s health. As a result, the proportion of children with high exposure to hepatitis B was more significant than that of children with normal exposure in our recruiting population.
Conclusion
Considering the high incidence of HBV infection among pregnant women in China, pressure is put on the prevention of MTCT. These results provide two valuable pieces of information. Careful surveillance of maternal HBs Ag/HBe Ag/HBV-DNA load status is crucial during pregnancy and the perinatal period. Infected pregnant women should be identified as early as possible, and pregnant women with high-risk levels of exposure should be treated. In childhood, newborns should receive HBIG and the HepB within 12 hours after delivery, and infants within one year of age should receive three doses of HepB on time according to the “0-1-6” program. After three doses of the HepB, routine follow-up testing for hepatitis B markers should be performed to determine the effect of preventing MTCT.
Abbreviations
HBV, hepatitis B virus; HBs Ag, hepatitis B surface antigen; HBe Ag, hepatitis B e antigen; HepB, hepatitis B vaccine; HBIG, hepatitis B immunoglobulin; MTCT, mother-to-child transmission; DT, decision tree.
Data Sharing Statement
The data supporting this study’s findings are available from the corresponding author upon reasonable request.
Ethics Approval
The study was carried out under the ethical principles of the Declaration of Helsinki. The Human Subjects Ethics Committee of Fujian Maternity and Child Health Hospital approved the study. Mothers were informed of the study’s purpose, and written informed consent was obtained before the interviews and blood sample collections. Informed consent was obtained from the children’s legal guardian(s)/parents. All participants’ personal or sensitive information was marked with an alphabetic or numeric code to ensure patient privacy.
Consent to Participate
All participants provided consent for participation.
Funding
No funding was received from the funding agents.
Disclosure
The authors who participated in this study did not have any relationship with the manufacturers of the drugs involved, either in the past or the present, and did not receive funding from the manufacturers to conduct their research.
References
1. Polaris Observatory Collaborators. Global prevalence, treatment, and prevention of hepatitis B virus infection in 2016: a modeling study. Lancet Gastroenterol Hepatol. 2018;3:
2. Liu J, Liang W, Jing W, et al. Countdown to 2030: eliminating hepatitis B disease, China. Bull World Health Organ. 2019;97(3):230–238. doi:10.2471/BLT.18.219469
3. Bleich LM, Swenson ES. Prevention of neonatal hepatitis B virus transmission. J Clin Gastroenterol. 2014;48(9):765–772. doi:10.1097/MCG.0000000000000115
4. Stanaway JD, Flaxman AD, Naghavi M, et al. The global burden of viral hepatitis from 1990 to 2013: findings from the global burden of disease study 2013. Lancet. 2016;388(10049):1081–1088. doi:10.1016/S0140-6736(16)30579-7
5. Geffert K, Maponga TG, Henerico S. Prevalence of chronic HBV infection in pregnant woman attending antenatal care in a tertiary hospital in Mwanza, Tanzania: a cross-sectional study. BMC Infect Dis. 2020;20(1):395. doi:10.1186/s12879-020-05096-2
6. World Health Organization. Documenting the Impact of Hepatitis B immunization: Best Practices for Conducting a Serosurvey. World Health Organization; 2011.
7. World Health Organization. Hepatitis B vaccines. WHO position paper. Wkly Epidemiol Rec. 2009;40(84):405–420.
8. WHO. Prevention of mother--to--child transmission of hepatitis B virus: guidelines on antiviral prophylaxis in pregnancy –- policy brief. Available from: https://www.who.int/publications/i/item/9789240008601.
9. World Health Organization. Global hepatitis sector strategy on viral hepatitis 2016–2021. Geneva: World Health Organization; 2016. Available from: https://www.who.int/hepatitis/strategy2016-2021/portal/en/.
10. Chen DS. Hepatitis B vaccination: the key toward elimination and eradication of hepatitis B. J Hepatol. 2009;50(4):805–816. doi:10.1016/j.jhep.2009.01.002
11. Zheng XQ, Li X, Liu J, et al. Horizontal transmission might be a common route of hepatitis B virus exposure in highly endemic areas. J Med Virol. 2022;94(10):4983–4992. doi:10.1002/jmv.27905
12. Cui F, Shen L, Li L, et al. Prevention of chronic hepatitis B after 3 decades of escalating vaccination policy, China. Emerg Infect Dis. 2017;23(5):765–772. doi:10.3201/eid2305.161477
13. Yang XH, Zhou Y, Zhang HR, et al. Sero-epidemiological survey of hepatitis B in Fujian province from 2019 to 2020. Straits J Prev Med. 2021;27(6):1–4.
14. Cui F, Woodring J, Chan P, Xu F. Considerations of antiviral treatment to interrupt mother-to-child transmission of hepatitis B virus in China. Int J Epidemiol. 2018;47(5):1529–1537. doi:10.1093/ije/dyy077
15. Wang C, Wang C, Jia ZF, et al. Protective effect of an improved immunization practice of mother-to-infant transmission of hepatitis B virus and risk factors associated with immunoprophylaxis failure. Medicine. 2016;95(34):e4390. doi:10.1097/MD.0000000000004390
16. Wang F, Zhang G, Zheng H, et al. Postvaccination serologic testing of infants born to hepatitis B surface antigen positive mothers in 4 provinces of China. Vaccine. 2017;35(33):4229–4235. doi:10.1016/j.vaccine.2017.06.019
17. Schweitzer A, Horj J, Mikolajczyk RT, Krause G, Ott JJ. Estimation of worldwide prevalence of chronic hepatitis B virus infection: a systematic review of data published between 1965 and 2013. Lancet. 2015;386(10003):1546–1555. doi:10.1016/S0140-6736(15)61412-X
18. Ott JJ, Stevens GA, Groeger J, Wiersma ST. Global epidemiology of hepatitis B virus infection: new estimates of age-specific HBsAg seroprevalence and endemicity. Vaccine. 2012;30(12):2212–2219. doi:10.1016/j.vaccine.2011.12.116
19. Shepard CW, Simard EP, Finelli L, Fiore AE, Bell BP. Hepatitis B virus infection: epidemiology and vaccination. Epidemiol Rev. 2006;28:112–125. doi:10.1093/epirev/mxj009
20. Liu J, Zhang S, Wang Q, et al. Seroepidemiology of hepatitis B virus infection in 2 million men aged 21–49 years in rural China: a population-based, cross-sectional study. Lancet Infect Dis. 2016;16:80–86. doi:10.1016/S1473-3099(15)00218-2
21. Wang H, Men P, Xiao Y, et al. Hepatitis B infection in the general population of China: a systematic review and meta-analysis. BMC Infect Dis. 2019;19(1):811. doi:10.1186/s12879-019-4428-y
22. Liu J, Zhang S, Wang Q, et al. Prevalence of HBsAg/HBeAg among 1,936,801 couples preparing for pregnancy in rural China: an observational study. J Viral Hepat. 2017;24:679–686. doi:10.1111/jvh.12693
23. Xin X, Wang Y, Cheng J, et al. Seroepidemiological survey of hepatitis B virus infection among 764,460 women of childbearing age in rural China: a cross-sectional study. J Clin Virol. 2016;81:47–52. doi:10.1016/j.jcv.2016.05.014
24. Lamberth JR, Reddy SC, Pan JJ, et al. Chronic hepatitis B infection in pregnancy. World J Hepatol. 2015;7(9):1233–1237. doi:10.4254/wjh.v7.i9.1233
25. Funk AL, Lu Y, Yoshida K, et al. Efficacy and safety of antiviral pro-phylaxis during pregnancy to prevent mother--to--child transmission of hepatitis B virus: a systematic review and meta--analysis. Lancet Infect Dis. 2021;21(1):70-–84. doi:10.1016/S1473-3099(20)30586-7
26. Huang X, Zhou L, Mu L-H, et al. Efficacy of hepatitis B immunoprophylaxis in children at high risk of hepatitis B and risk factors for mother-to-child transmission of hepatitis B virus. Chin J Contemp Pediatr. 2016;18(5):410–414.
27. Biot B, Laverdure N, Lacaille F, et al. Mother-to-child transmission of hepatitis B virus despite postexposure prophylaxis: a review of the literature and description of 11 observations. Arch Pediatrie. 2017;24(2):135–139.
28. WHO Western Pacific Region. Hepatitis B control through immunization: regional reference guide; 2014.
29. Guo Z, Shi XH, Feng YL, et al. Risk factors of HBV intrauterine transmission among HBsAg-positive pregnant women. J Viral Hepat. 2013:317–321. doi:10.1111/jvh.12032
30. Zhang L, Gui X, Wang B, et al. A study of immunoprophylaxis failure and risk factors of hepatitis B virus mother-to-infant transmission. Eur J Pediatr. 2014;173:1161–1168. doi:10.1007/s00431-014-2305-7
31. Buchanan C, Tran TT. Management of chronic hepatitis B in pregnancy. Clin Liver Dis. 2010;14:495–504. doi:10.1016/j.cld.2010.05.008
32. Boucheron P, Lu Y, Yoshida K, et al. Accuracy of HBeAg to identify pregnant women at risk of transmitting hepatitis B virus to their neonates: a systematic review and meta-analysis. Lancet Infect Dis. 2021;21(1):85–96. doi:10.1016/S1473-3099(20)30593-4
33. Sun W, Zhao S, Ma L, et al. Telbivudine treatment started in early and middle pregnancy completely blocks HBV vertical transmission. BMC Gastroenterol. 2017;17(1):51. doi:10.1186/s12876-017-0608-7
34. Chen HL, Lin LH, Hu FC, et al. Effects of maternal screening and universal immunization to prevent mother-to-infant transmission of HBV. Gastroenterology. 2012;142(4):773–81.e2. doi:10.1053/j.gastro.2011.12.035
35. Liu X, Chen C, Jiang D, et al. Comparison of HBV-DNA and HBeAg as antiviral therapeutic indicators among HBV-infected pregnant women: a systematic review and meta-analysis. Ann Palliat Med. 2021;10(9):9362–9371. doi:10.21037/apm-21-1560
36. Foaud HM, Maklad S, El Din A G, et al. Lamivudine use in pregnant HBsAg-females effectively reduces maternal viremia. Arab J Gastroenterol. 2019;20(1):8–13. doi:10.1016/j.ajg.2019.02.003
37. Ding Y, Cao L, Zhu L, et al. Efficacy and safety of tenofovir alafenamide fumarate for preventing mother to child transmission of hepatitis B virus: a national cohort study. Aliment Pharmacol Ther. 2020;52(8):1377–1386. doi:10.1111/apt.16043
38. Komatsu H, Inui A. Hepatitis B virus infection in children. Expert Rev Anti Infect. 2015;13(4):427–450.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.