")
Back to Journals » Chronic Wound Care Management and Research » Volume 11
Effectiveness of Vibration Therapy for Hard-to-Heal Wounds in Clinical Study: A Scoping Review
Authors Haba D, Itabashi M, Tamai N, Tobe H, Sanada H, Nakagami G
Received 26 May 2023
Accepted for publication 17 January 2024
Published 3 February 2024 Volume 2024:11 Pages 1—12
DOI https://doi.org/10.2147/CWCMR.S423054
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Marco Romanelli
Daijiro Haba,1,2 Mizuho Itabashi,1,3 Nao Tamai,2,4,5 Hiromi Tobe,2,6 Hiromi Sanada,1,2,6 Gojiro Nakagami1,2
1Department of Gerontological Nursing/Wound Care Management, Graduate School of Medicine, The University of Tokyo, Bunkyo-Ku, Tokyo, Japan; 2Global Nursing Research Center, Graduate School of Medicine, The University of Tokyo, Bunkyo-Ku, Tokyo, Japan; 3Department of Gerontological Nursing, Graduate School of Nursing Science, St. Luke’s International University, Chuo-ku, Tokyo, Japan; 4Department of Imaging Nursing Science, Graduate School of Medicine, The University of Tokyo, Bunkyo-Ku, Tokyo, Japan; 5Department of Nursing, Graduate School of Medicine, Yokohama City University, Yokohama, Kanagawa, Japan; 6Ishikawa Prefectural Nursing University, Kahoku, Ishikawa, Japan
Correspondence: Gojiro Nakagami, Department of Gerontological Nursing/Wound Care Management, Graduate School of Medicine, The University of Tokyo, 7-3-1 Hongo, Bunkyo-Ku, Tokyo, 113-0033, Japan, Tel/Fax +81-3-5841-341, Email [email protected]
Abstract: Diminished peripheral blood flow at the wound site remains a key hindrance to effective wound healing. Hard-to-heal wounds are defined as wounds that fail to heal with standard therapy. Vibration therapy may help promote the healing of hard-to-heal wounds such as pressure injuries, diabetic foot ulcers, and venous leg ulcers by improving blood flow. However, evidence supporting its effectiveness on hard-to-heal wounds is inadequate. This scoping review focuses on studying the effectiveness of vibration therapy for healing hard-to-heal wounds by compiling all available research. The following databases were systematically reviewed from 1980 to 2023: MEDLINE, EMBASE, Cochrane Library, Ichu-shi-Web, IEEE, CINAHL, Scopus, Web of Science, and PEDro. The search terms included “wound”, “ulcer”, “hard-to-heal”, “vibration therapy”, and “wound healing”. Two authors independently screened the articles based on inclusion criteria, and the lead author performed data extraction and analysis. A total of 1036 articles were identified, and five articles were eligible to be included in this review. The results suggested that low-frequency and low-intensity vibration therapies helped effectively treat wounds (including pressure injuries, diabetic foot ulcers, and venous leg ulcers) by improving blood flow, relieving pain, reducing exudate, removing necrotic tissue, and increasing the expression of nitric oxide associated with wound healing. This study will inform the treatment choices of clinicians who manage patients with hard-to-heal wounds and researchers who plan to conduct clinical trials using vibration therapy. Further studies on vibration therapy must be performed to gather evidence to support the clinical application of vibration therapy to improve healing time and outcomes in individuals with hard-to-heal wounds.
Keywords: vibration, physical therapy, hard-to-heal wound, chronic wound, wound healing
Introduction
Background
Treatments of hard-to-heal wounds such as pressure injuries (PIs), diabetic foot ulcers (DFUs), and venous leg ulcers (VLUs) poses a significant challenge worldwide,1 especially in aging populations.2,3 These wounds, with a high prevalence (12.8% for PIs globally,4 4–27% among diabetes mellitus (DM) patients worldwide,5 and 2.21 per 1000 individuals for chronic venous leg ulcers)6 contribute to increased healthcare costs and impact patient quality of life and hospitalization length.7,8 Risk factors such as aging, peripheral vascular disease, obesity, and diabetes exacerbate their prevalence and severity.6,9,10
Hard-to-heal wounds, defined by their failure to respond to standard treatments,11 often suffer from delayed healing due to reduced blood flow at the wound site.3,12 Revascularization is general treatment and helps improve peripheral blood circulation;13 however, revascularization surgery is invasive and significantly increases the risk of perioperative complications.14 To address delayed healing, treatments aim to enhance peripheral circulation, leading to the development of various less invasive techniques,15 including negative pressure wound therapy,16 ultrasound,17 electrical stimulation,18 oxygen therapy,19,20 and notably, vibration therapy.21 Vibration therapy, in particular, stands out for its practicality and non-invasive approach, utilizing a vibration stimulus directly at the wound site to promote blood flow, easily applied through devices placed under a mattress or on a vibrating platform.22–25
Vibration therapy may be an effective treatment to facilitate the healing of hard-to-heal wounds by improving peripheral blood circulation, as has been reported in joint and muscle studies.26 Employed for skeletal muscle training and increasingly in clinical settings, whole-body vibration (WBV) therapy has demonstrated numerous benefits25 such as improved muscle strength,27 increased bone mass,28 better skin blood flow,29 and reduced fat and blood glucose levels.30,31 Extensively studied since the 1980s,32 recent research, particularly in animal models, has highlighted its potential in wound healing32–35 Studies have shown that WBV accelerates wound closure, re-epithelialization, and angiogenesis, especially in diabetic hard-to-heal animal models, by reducing tissue hypoxia and promoting tissue regeneration.36–39 Notably, low-frequency and low-intensity WBV have been effective in improving both wound closure and healing quality, making it a promising therapeutic avenue for hard-to-heal wounds.
While vibration therapy’s benefits in animal wound healing studies have been documented, its effectiveness in human clinical cases remains less explored.21 The International Guideline 2019 by EPUAP/NPIAP/PPPIA suggests vibration therapy could offer superior healing outcomes for PIs compared to standard care.40 However, currently, there are no guidelines regulating the use of vibration therapy for DFUs and VLUs. Despite indications of improved healing, its clinical application is limited, possibly due to inadequate clinician familiarity, unclear dosage guidelines, and limited understanding of its healing mechanisms.41 This review addresses this gap by synthesizing available research on vibration therapy in hard-to-heal wounds, aiming to enhance clinical practice and guide future studies.
Study Rationale
There are few studies assessing the effectiveness of vibration therapy in people with hard-to-heal wounds.42 Hard-to-heal wounds are defined as wounds that fail to heal with standard therapy in an orderly and timely manner.11 Our study is centered on evaluating interventions for a variety of wound types commonly associated with hard-to-heal conditions, including PIs, DFUs, VLUs, and arterial leg ulcers (ALU). In defining hard-to-heal wounds, we specifically considered ulcers that had not healed over a long period since their occurrence, regardless of whether such wounds typically respond to standard treatment. We specifically characterized hard-to-heal wounds as ulcers that have not healed for an extended period following their development, irrespective of their usual response to standard treatment.
In this scoping review, we searched for studies with a wide range of study designs that reported the effectiveness of low-frequency vibration in the healing of hard-to-heal wounds. We mapped the available evidence to better understand the effectiveness of vibration therapy for wound healing. Vibration therapy includes various specifications regarding amplitudes and frequencies, which are applied intermittently or continuously through localized vibration or WBV intermittently or continuously.21 The vibration device delivers a frequency measured in hertz (Hz),25 typically ranging from 1 Hz to 100 Hz.42 In this study, ultrasound therapy, which is also a form of mechanical vibrational energy, was excluded because ultrasound therapy involves frequency ranges above 20 kHz.21
Study Objectives
The objectives of this scoping review were to: (a) summarize the available evidence to identify which vibration therapy was effective in terms of healing outcomes of hard-to-heal wounds, as reported in human study, and (b) identify the optimal setting for vibration therapy to promote healing of hard-to-heal wounds.
Scoping Review Question
The following scoping review question was formulated: “What kind of vibration therapy and setting contribute to wound healing in patients with hard-to-heal wounds” “Is there any evidence suggesting that vibration therapy promotes healing of hard-to-heal wounds?”
Material and Methods
Protocol Design
A review protocol was not published. This scoping review was drafted using the scoping review framework of Arksey andO’Malely43 and the JBI framework.44 The Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for scoping reviews (PRISMAScR) Checklist45 were used to prepare this review.
Eligibility Criteria
Papers published between 1980 to 2023 in English and Japanese were included in this review, regardless of the clinical setting, involving participants of all ages with hard-to-heal wounds that had undergone vibration therapy. We excluded papers that reported ultrasound therapy; treatments with high-frequency vibration of kHz and MHz; and if vibration settings were not defined in the paper.25 Conference abstracts, books, letters to the editor, guidelines, protocols, and review articles were also excluded. We investigated the effectiveness of various types of vibration therapy for wounds, focusing on the reduction of wound area and improvement in healing rate or duration. We included original studies and case reports, including (1) randomized controlled trials (RCT), (2) longitudinal studies, (3) cross-sectional studies, (4) case-control studies, excluding animal experiments.
Information Sources
To identify potentially relevant papers, the following bibliographic databases were searched with a date filter of January 1, 1980, to May 31, 2023: MEDLINE (PubMed), Ovid EMBASE, Cochrane Library (Ovid), Ichu-shi-Web, IEEE, EBSCO CINAHL, Scopus, Web of Science, and PEDro. Additional data sources were identified using Semantic Scholar. Search strategies were developed through team discussion. The final search results were exported to Mendeley for better reference management, and duplicates were removed before screening the literature by two researchers.
Search
Search terms and Medical Subject Headings (MeSH) terms related to vibration therapy, wound, and wound healing were used and were combined using the boolean operators “AND” and “NOT”. Our primary search strategy, exemplified by the search conducted in PubMed in May 2023, was as follows:
#1. Wound* OR injur* OR ulcer* OR chronic OR hard-to-heal OR non-healing
#2. Vibrat* OR “vibration therap” OR “whole body vibratio” OR “local vibratio”
#3. Ultraso*
#4. Wound healing [MeSH Terms]
#5. ((#1 AND #2) NOT #3) AND #4
#6. Limit #5 to yr = “1980–2023”
Search results from the digital search process were uploaded to reference management software, and duplicates were removed. It is important to note that multiple search engines were utilized, each with its unique search formula. Due to the extensive number of search strategies employed and their complexity, they have been detailed in the Supplementary Material.
Selection of Sources of Evidence
In the first screening of the title and abstract, the articles that included the terms “vibration therapy”, “whole-body vibration”, “local vibration”, “low-frequency vibration”, or “low-intensity vibration” and neither of “ultraso*” or the terms related to testing such as “vibratory sense examination”, or “vibration test” were selected. The articles that included the terms “wound”, “chronic wound”, “chronic injury”, “chronic ulcer”, “hard-to-heal”, “non-healing”, “pressure ulcer”, “pressure injury”, “diabetic foot ulcer”, “diabetic foot disease” “venous leg ulcer” were selected. In the second full-text screening, original articles lacking wound healing or repair outcomes in patients were excluded.
Data Charting Process
The search results were imported into Rayyan (Qatar Computing Research Institute, Doha, Qatar).46 A data-charting form was developed by two reviewers (D.H. and M.I.) using Rayyan to determine which variables were to be extracted. Two reviewers (D.H. and M.I.) independently charted the data, discussed the results, and continuously updated the data-charting form in an iterative manner. Any disagreements were resolved through discussion between the two reviewers or through further adjudication by a third reviewer.
Data Items
The following information was extracted: 1) article characteristics (e., study authors, year of publication, country); 2) study design/participants/age (eg, target population, the number of participants, age); 3) study subjects/ wound type (eg, details of their condition/ PI, DFU, VLU, or ALU); 4) name of vibration device used/ type of vibration (eg, local vibration and location, WBV); 5) treatment posture or vibration setting (eg, supine position, prone position, standing position); 6) vibration frequency (Hz), vibration intensity (eg, accelerations (g, m/s2), peak-to-peak voltage (Vpp)); 7) vibration protocol (eg, time, duration, wave type, frequency of treatment); 8) control treatment or option, 9) primary outcome for wound healing (eg, wound size, wound closure, duration or ratio of wound healing); 10) secondary outcome associated with wound healing; 11) adverse events; 12) conclusion.
Synthesis of Results
We grouped the studies in the manner in which the vibration device was used in human study. The results are presented in Table 1. The factors related to the vibration setting were summarized for each study, along with the study attributes, study design, wound type, and protocols. We identified a study investigating the effectiveness of wound healing in relation to certain factors and summarized the indicators of the outcomes.
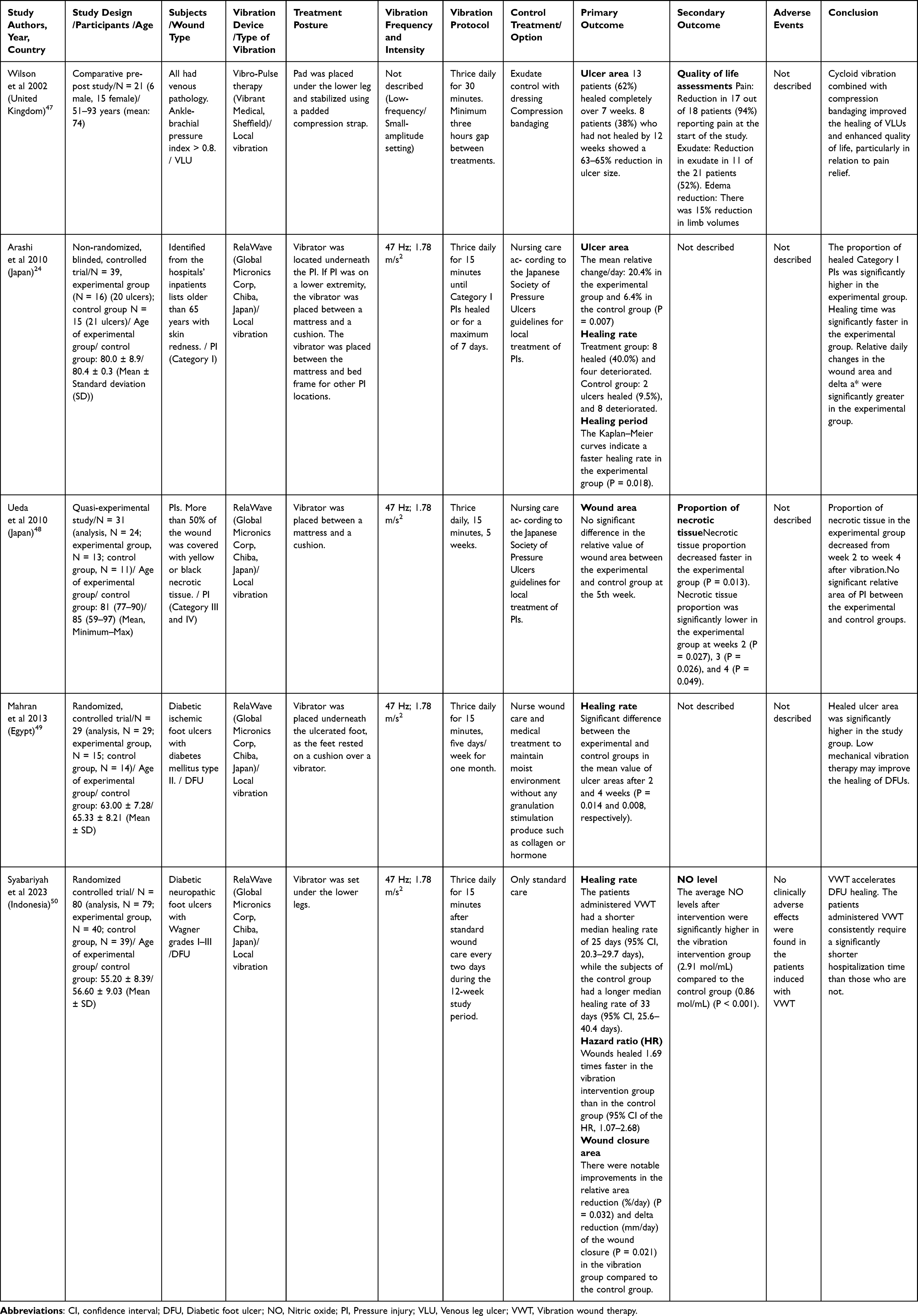 |
Table 1 Summary of Collected Data of Clinical Studies in This Scoping Review |
Results
Selection of Sources of Evidence
The initial search yielded 1,273 studies. After removing the duplicates (n = 238) and including an additional study from other sources (n = 1), 1036 articles remained. After screening the title and the abstract, 1026 papers were excluded. Among the 10 remaining papers, 5 were excluded through full-text screening: one study did not investigate the effects of vibration for wound healing, and four others were ineligible due to wound type and study type. Five articles met the inclusion criteria and were included in this scoping review.24,47–50 The PRISMA flowchart for this review is shown in Figure 1.
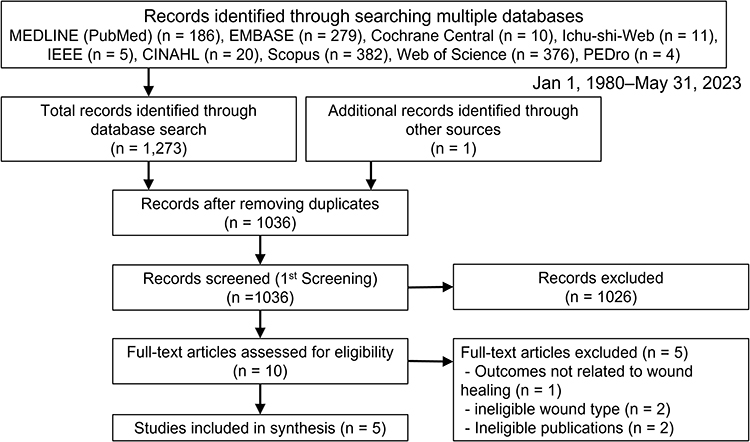 |
Figure 1 Flow chart of this scoping review. A PRISMA flowchart of the current review is shown. Finally, a total of ten articles were included in this scoping review. |
Characteristics of Sources of Evidence
The characteristics of the five included studies are shown in Table 1. These studies included patients with VLUs,47 PIs,24,48 and DFUs.49,50 All study demonstrated that both the intervention group and the control group received the same standard treatment; however, the intervention group additionally underwent vibration therapy. Wilson et al conducted a comparative pre-post study in patients with VLUs. This study used the Vibro-Pulse device (Vibrant Medical, Sheffield), which is used to deliver cycloidal multidirectional vibration therapy.47 In this study, detailed vibrational conditions, including vibration frequency and intensity, were not described. However, the vibration was delivered three times a day for 30 min to patients with a minimum gap of three hours between each therapy session. All 21 patients participated in the study until the end. Thirteen patients (62%) healed completely by 12 weeks; however, the eight patients who had not healed by 12 weeks showed a reduction in ulcer size of 63–65%. Additionally, there was a reduction in pain in 17 out of 18 patients (94%) who reported pain at the start of the study, a reduction in exudate discharge in 11 out of 21 patients (52%), and a 15% reduction in total limb volume. Among these, one case involving a patient with a venous leg ulcer (VLU) that had not healed for 20 years was reported to have healed following the intervention.
In four studies, RelaWave (Global Micronics Corp, Chiba, Japan) was used to deliver local vibration therapy to treat PIs and DFUs.24,48–50 The vibration settings of the RelaWave were the same in all the studies: the frequency and horizontal vibration acceleration were 47 Hz and 1.78 m/s2, respectively. Arashi et al conducted a non-randomized blinded controlled trial in patients with Category I PIs, and vibration was delivered for 15 min three times a day until Category I PIs healed or for a maximum of 7 days. This study demonstrated that the mean relative change in the wound area per day was decreased in the experimental group (20.4%) compared to that of the control group (6.4%); eight ulcers healed (40%) and four ulcers deteriorated in the experimental group. In contrast, two ulcers healed (9.5%) and eight ulcers deteriorated in the control group.24 Additionally, Kaplan–Meier curves indicated a faster healing rate in the experimental group (P = 0.018). Ueda et al conducted a quasi-experimental study using vibration therapy, performed thrice a day for five weeks for category III and IV PIs with necrotic tissue.48 There was no significant difference in the decrease in relative wound area between the experimental and control groups at week five of the study period. However, the proportion of necrotic tissue decreased more rapidly in the experimental group than in the control group at the first week (P = 0.013), second week (P = 0.027), third week (P = 0.026), and fourth week (P = 0.049). Mahran et al conducted an RCT (n = 29) enrolling individuals with DFUs in Egypt, where vibration treatment was applied for 15 min thrice a day, five days per week, for one month.49 This study found a significant difference between the experimental and control groups in the mean value of ulcer healing rate after two and four weeks (P = 0.014 and 0.008), respectively. The authors concluded that low-frequency and low-intensity vibration therapy might improve the healing time of DFUs. Syabariyah et al conducted an RCT (n = 80) including DFUs with diabetic neuropathy in Indonesia. They performed vibration wound therapy for 15 min thrice a day after standard wound care every two days for 12 weeks.50 This study reported that the duration of the wounds was 2.0 ± 1.0 to 4.0 weeks for the control group and 2.0 ± 1.0 to 6.0 weeks for the intervention group, with no significant difference in wound duration between these two groups. The patients in the vibration group (n = 40) had a shorter median healing rate of 25 days (95% confidence interval (CI), 20.3–29.7 days), while the patients in the control group (n = 39) had a longer median healing rate of 33 days (95% CI, 25.6–40.4 days). There was one patient in the control group whose wound was not healed within the designated 12-week study period. This study also calculated the hazard ratio (HR) and found that the wounds healed 1.69 times faster in the vibration group than in the control group (95% CI of the HR, 1.07–2.68). There were notable improvements in the relative area reduction (%/day) and delta reduction (mm/day) of the wound closure in the vibration group compared to the control group (P = 0.032, 0.021, respectively). The author also evaluated the effect of vibration intervention on NO level, which is a factor of vasodilation, prior to and after the intervention. There were no differences in the NO levels between the vibration group and control group before intervention (P = 0.502). However, the two groups had significant differences in NO levels postintervention. The average NO levels after intervention were significantly higher in the vibration intervention group (2.91 mol/mL) compared to the control group (0.86 mol/mL), with a p-value of <0.001. These five human studies indicate that local vibration treatment promotes wound healing in PIs and DFUs in a clinical setting.
Synthesis of results: Effects of Vibration Therapy and Appropriate Vibration Setting for Wound Healing
Four studies reported the same vibration setting, in which the frequency and horizontal vibration acceleration of the present vibrator were 47 Hz and 1.78 m/s2, respectively. The vibration was applied for 15 min three times a day. However, the treatment periods were different for each study ranging from 7 days,24 every two days during the 12 week,50 one month,49 to 5 weeks.48 In three studies, the vibrator was placed between a mattress and a cushion and was positioned underneath the wounds, and all patients lay on the bed. In another study using the same vibrator, the vibrator was set under both lower legs.50 In one study that used cycloidal multidirectional vibration therapy, the vibration setting involved three therapy sessions at the patient’s home, each session of 30 min, with a minimum of three hours rest period between each session.47 The vibration pad was placed under the lower leg and was combined with compression therapy.
Discussion
Summary of Evidence
This scoping review focused on the effects of vibration therapy on wound healing in hard-to-heal wounds and aims to determine the appropriate vibration settings according to human study. To the best of our knowledge, no studies have so far summarized evidence on the effectiveness of vibration therapy on wound healing in hard-to-heal wounds. The final number of articles included in the study was five. In the clinical study, four studies reported a reduction in wound size and improvement in the healing rate. While one study did not indicate a significant difference in the wound area between the vibration and control groups, they reported a reduction in necrotic tissue in the vibration group. Taken together, the evidence from the results suggests that a combination of low-frequency (47 Hz) and low-intensity (1.78 m/s2) vibration with a treatment period of 15–30 minutes thrice daily for 5–7 days a week potentially improved processes involved in wound healing, such as improving blood flow, resulting in wound healing. The results from these ten articles suggested the promising effectiveness of vibration therapy in promoting wound healing, with low-frequency and low-intensity vibration settings being optimal for healing hard-to-heal wounds, including PIs, DFUs, and VLUs.
Implication for Clinical Practice
Vibration therapy presents a promising option for treating hard-to-heal wounds, yet there’s a notable gap between evidence and clinical practice. This scoping review highlights its effectiveness in managing PIs, VLUs, and DFUs. Clinical studies have predominantly used local vibration treatments, acknowledging that patients with hard-to-heal wounds may not be able to use WBV platforms. Research indicates that low-frequency, low-intensity vibration can effectively enhance skin blood flow, crucial for wound healing in both healthy individuals and diabetic patients24,49,51,52 However, it’s important to avoid long-term exposure to high-frequency and high-intensity vibrations to prevent vascular issues like Raynaud’s phenomenon.53 This review provides existing evidence to the clinical practice and may inform future researchers who may plan to conduct clinical trials assessing the effectiveness of vibration therapy.
Mechanisms of Wound Healing by Vibration Therapy
One of the most important treatments to promote hard-to-heal wound healing is to improve blood flow at the wound site. The previous animal studies investigated the mechanisms of wound healing promoted by vibration therapy. They reported that vibration therapy induced regeneration of veins, promoted angiogenesis and blood perfusion, reduced tissue hypoxia, induced re-epithelialization and granular tissue formation, and induced expression of cytokines associated with wound healing.32,34,36,38,54 A previous study reported that low-frequency vibration could accelerate regional blood flow through vasodilation via the production of NO22,23 and wound healing in PIs.24 One study in this review reported that vibration therapy increased NO levels in patients with DFUs.55 However, the outcomes in this review could not explain the discrepancy between the theory and clinical practice, which is that vibration therapy cannot improve peripheral blood flow in DFU patients due to the dysfunction of NO production and severe angiopathy, but low-frequency vibration can promote healing of DFUs.49 Further studies are needed to elucidate the mechanisms underlying the promotion of peripheral blood flow in patients with DFU.
Limitations
This scoping review has some limitations. First, we did not assess the quality of the studies systematically in this scoping review. Furthermore, these studies had small sample sizes, and there was only one paper related to the effects of vibration therapy for VLU, and there was no paper regarding to arterial leg ulcer. These limitations may have affected the evidence.
Conclusion
This scoping review summarized the evidence regarding the effectiveness of vibration therapy for hard-to-heal wounds. Low-frequency and low-intensity local vibration therapy is useful for promoting wound healing based on evidence from human studies. The current optimal settings could be summarized as follows: local vibration at a low frequency within 47 Hz and low-intensity (1.78 m/s2) for less than 30 min, three times a day, and five weeks. The findings from this review may be used by researchers and clinicians planning to conduct clinical trials on vibration therapy to elucidate the mechanisms underlying wound healing to bridge the evidence-practice gap in this area.
Acknowledgments
We would like to express our sincere gratitude to Prof. Carolina D. Weller for her advice and support and Mr. Md. Obaidur Rahman for his help with data search. We acknowledge that this editorial was written with the support of Chat GPT-4 to help synthesize knowledge and improve the clarity of the language.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the JSPS KAKENHI (Grant No. 21J12334 and 21K18287).
Disclosure
Hiromi Sanada, Gojiro Nakagami, and the Global Micronics Corp are co-developers of RelaWave. The authors report no other conflicts of interest in this work.
References
1. Murphy C, Atkin L, Dissemond J, et al. Defying hard-to-heal wounds with an early antibiofilm intervention strategy: ‘wound hygiene’. J Wound Care. 2019;28(12):818–822. doi:10.12968/jowc.2019.28.12.818
2. Alam W, Hasson J, Reed M. Clinical approach to chronic wound management in older adults. J Am Geriatr Soc. 2021;69(8):2327–2334. doi:10.1111/jgs.17177
3. Frykberg RG, Banks J. Challenges in the treatment of chronic wounds. Adv Wound Care. 2015;4(9):560–582. doi:10.1089/wound.2015.0635
4. Li Z, Lin F, Thalib L, Chaboyer W. Global prevalence and incidence of pressure injuries in hospitalised adult patients: a systematic review and meta-analysis. Int J Nurs Stud. 2020;105:103546. doi:10.1016/j.ijnurstu.2020.103546
5. Rosyid FN. Etiology, pathophysiology, diagnosis and management of diabetics’ foot ulcer. Int J Res Med Sci. 2017;5:4206–4213. doi:10.18203/2320-6012.ijrms20174548
6. Martinengo L, Olsson M, Bajpai R, et al. Prevalence of chronic wounds in the general population: systematic review and meta-analysis of observational studies. Ann Epidemiol. 2019;29:8–15. doi:10.1016/j.annepidem.2018.10.005
7. Olsson M, Jarbrink K, Divakar U, et al. The humanistic and economic burden of chronic wounds: a systematic review. Wound Repair Regen. 2019;27(1):114–125. doi:10.1111/wrr.12683
8. Brain D, Tulleners R, Lee X, Cheng Q, Graves N, Pacella R. Cost-effectiveness analysis of an innovative model of care for chronic wounds patients. PLoS One. 2019;14(3):e0212366. doi:10.1371/journal.pone.0212366
9. Jarbrink K, Ni G, Sonnergren H, et al. Prevalence and incidence of chronic wounds and related complications: a protocol for a systematic review. Syst Rev. 2016;5(1):152. doi:10.1186/s13643-016-0329-y
10. Beyene RT, Derryberry SL, Barbul A. The effect of comorbidities on wound healing. Surg Clin North Am. 2020;100(4):695–705. doi:10.1016/j.suc.2020.05.002
11. Azevedo MM, Lisboa C, Cobrado L, Pina-Vaz C, Rodrigues A. Hard-to-heal wounds, biofilm and wound healing: an intricate interrelationship. Br J Nurs. 2020;29(5):S6–S13. doi:10.12968/bjon.2020.29.5.S6
12. Mervis JS, Phillips TJ. Pressure ulcers: prevention and management. J Am Acad Dermatol. 2019;81(4):893–902. doi:10.1016/j.jaad.2018.12.068
13. Hinchliffe RJ, Forsythe RO, Apelqvist J, et al. Guidelines on diagnosis, prognosis, and management of peripheral artery disease in patients with foot ulcers and diabetes (IWGDF 2019 update). Diabetes Metab Res Rev. 2020;36(Suppl 1):e3276. doi:10.1002/dmrr.3276
14. Jd D, Tcf B, Se D, et al. Outcomes after first-time lower extremity revascularization for chronic limb-threatening ischemia between patients with and without diabetes. J Vascular Surg. 2019;67:1159–1169.
15. Hess CL, Howard MA, Attinger CE. A review of mechanical adjuncts in wound healing: hydrotherapy, ultrasound, negative pressure therapy, hyperbaric oxygen, and electrostimulation. Ann Plast Surg. 2003;51(2):210–218. doi:10.1097/01.SAP.0000058513.10033.6B
16. Wynn M, Freeman S. The efficacy of negative pressure wound therapy for diabetic foot ulcers: a systematised review. J Tissue Viability. 2019;28(3):152–160. doi:10.1016/j.jtv.2019.04.001
17. Bekara F, Vitse J, Fluieraru S, et al. New techniques for wound management: a systematic review of their role in the management of chronic wounds. Arch Plast Surg. 2018;45(02):102–110. doi:10.5999/aps.2016.02019
18. Houghton PE. Electrical stimulation therapy to promote healing of chronic wounds: a review of reviews. Chronic Wound Care Manag Res. 2017;4:25–44. doi:10.2147/CWCMR.S101323
19. Eskes A, Vermeulen H, Lucas C, Ubbink DT. Hyperbaric oxygen therapy for treating acute surgical and traumatic wounds. Cochrane Database Syst Rev. 2013;12:CD008059.
20. Frykberg RG, Franks PJ, Edmonds M, et al. A multinational, multicenter, randomized, double-blinded, placebo-controlled trial to evaluate the efficacy of cyclical topical wound oxygen (TWO2) therapy in the treatment of chronic diabetic foot ulcers: the TwO2 study. Diabetes Care. 2020;43(3):616–624. doi:10.2337/dc19-0476
21. Ennis WJ, Lee C, Gellada K, Corbiere TF, Koh TJ. Advanced technologies to improve wound healing: electrical stimulation, vibration therapy, and ultrasound-what is the evidence? Plast Reconstr Surg. 2016;138(3S):94S–104S. doi:10.1097/PRS.0000000000002680
22. Nakagami G, Sanada H, Matsui N, et al. Effect of vibration on skin blood flow in an in vivo microcirculatory model. Biosci Trends. 2007;1(3):161–166.
23. Ichioka S, Yokogawa H, Nakagami G, Sekiya N, Sanada H. In vivo analysis of skin microcirculation and the mole of nitric oxide during vibration. Ostomy Wound Manag. 2011;57:40–47.
24. Arashi M, Sugama J, Sanada H, et al. Vibration therapy accelerates healing of stage I pressure ulcers in older adult patients. Adv Skin Wound Care. 2010;23(7):321–327. doi:10.1097/01.ASW.0000383752.39220.fb
25. Rauch F. Vibration therapy. Dev Med Child Neurol. 2009;51(s4):166–168. doi:10.1111/j.1469-8749.2009.03418.x
26. Carlsöö S. The effect of vibration on the skeleton, joints and muscles. A review of the literature. Appl Ergon. 1982;13(4):251–258. doi:10.1016/0003-6870(82)90064-3
27. Marin PJ, Rhea MR. Effects of vibration training on muscle strength: a meta-analysis. J Strength Cond Res. 2010;24(2):548–556. doi:10.1519/JSC.0b013e3181c09d22
28. Gilsanz V, Wren TA, Sanchez M, Dorey F, Judex S, Rubin C. Low-level, high-frequency mechanical signals enhance musculoskeletal development of young women with low BMD. J Bone Miner Res. 2006;21(9):1464–1474. doi:10.1359/jbmr.060612
29. Johnson PK, Feland JB, Johnson AW, Mack GW, Mitchell UH. Effect of whole body vibration on skin blood flow and nitric oxide production. J Diabetes Sci Technol. 2014;8(4):889–894. doi:10.1177/1932296814536289
30. Omidvar M, Alavinia SM, Craven BC. The effects of whole body vibration therapy on reducing fat mass in the adult general population: a systematic review and meta-analyses. J Musculoskelet Neuronal Interact. 2019;19(4):455–464.
31. Pessoa MF, de Souza HCM, da Silva APV, Clemente RDS, Brandao DC, Dornelas de Andrade A. Dornelas de Andrade A. Acute whole body vibration decreases the glucose levels in elderly diabetic women. Rehabil Res Pract. 2018;2018:3820615. doi:10.1155/2018/3820615
32. Leduc A, Lievens P, Dewald J. The influence of multidirectional vibrations on wound healing and on regeneration of blood- and lymph vessels. Lymphology. 1981;14(4):179–185.
33. Brites-Ferreira A, Taiar R, Cardoso ALBD, et al. Therapeutic approach of whole-body vibration exercise on wound healing in animal models: a systematic review. Int J Environ Res Public Health. 2023;20(6):4925. doi:10.3390/ijerph20064925
34. Sari Y, Sanada H, Minematsu T, et al. Vibration inhibits deterioration in rat deep-tissue injury through HIF1–MMP axis. Wound Repair Regen. 2015;23(3):386–393. doi:10.1111/wrr.12286
35. Wano N, Sanguanrungsirikul S, Keelawat S, Somboonwong J. The effects of whole-body vibration on wound healing in a mouse pressure ulcer model. Heliyon. 2021;7(4):e06893. doi:10.1016/j.heliyon.2021.e06893
36. Weinheimer-Haus EM, Judex S, Ennis WJ, Koh TJ. Low-intensity vibration improves angiogenesis and wound healing in diabetic mice. PLoS One. 2014;9:e91355. doi:10.1371/journal.pone.0091355
37. Yu CO, Leung KS, Jiang JL, Wang TB, Chow SK, Cheung WH. Low-magnitude high-frequency vibration accelerated the foot wound healing of n5-streptozotocin-induced diabetic rats by enhancing glucose transporter 4 and blood microcirculation. Sci Rep. 2017;7:11631. doi:10.1038/s41598-017-11934-2
38. Roberts RE, Bilgen O, Kineman RD, Koh TJ. Parameter-dependency of low-intensity vibration for wound healing in diabetic mice. Front Bioeng Biotechnol. 2021;9:654920. doi:10.3389/fbioe.2021.654920
39. Roberts RE, Cavalcante-Silva J, Del Rio-Moreno M, Bilgen O, Kineman RD, Koh TJ. Liver insulin-like growth factor-1 mediates effects of low-intensity vibration on wound healing in diabetic mice. J Pathol. 2023;260:97–107. doi:10.1002/path.6068
40. European Pressure Ulcer Advisory Panel National Pressure Injury Advisory Panel and Pan Pacific Pressure Injury Alliance. The International Guideline.Emily Haesler. Pressure Ulce. 2019; 2019:1.
41. Reynolds RP, Li Y, Garner A, Norton JN. Vibration in mice: a review of comparative effects and use in translational research. Animal Model Exp Med. 2018;1:116–124. doi:10.1002/ame2.12024
42. Prisby RD, Lafage-Proust MH, Malaval L, Belli A, Vico L. Effects of whole body vibration on the skeleton and other organ systems in man and animal models: what we know and what we need to know. Ageing Res Rev. 2008;7:319–329. doi:10.1016/j.arr.2008.07.004
43. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8:19–32. doi:10.1080/1364557032000119616
44. Aromataris E, Munn Z. JBI reviewer’s manual; 2019.
45. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169:467–473. doi:10.7326/M18-0850
46. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Syst Rev. 2016;5:210. doi:10.1186/s13643-016-0384-4
47. Wilson JM, Arseculeratne YM, Yang Y, Cherry GW. Healing venous ulcers with cycloidal multidirectional vibration therapy. J Wound Care. 2002;11:395–398. doi:10.12968/jowc.2002.11.10.26446
48. Ueda A, Sugama J, Okuwa M, et al. Effects of vibration on the healing of pressure ulcers with necrotic tissue. Jpn J PU. 2010;12:111–117.
49. Mahran HG, Helal OF, El-Fiky AAR. Effect of mechanical vibration therapy on healing of foot ulcer in diabetic polyneuropathy patients. J Am Sci. 2013;9:76–87.
50. Syabariyah S, Nurachmah E, Widjojo BD, et al. The effect of vibration on the acceleration of wound healing of diabetic neuropathic foot ulcer: a prospective experimental study on human patients. Healthcare. 2023;11(2):191. doi:10.3390/healthcare11020191
51. Tzen YT, Weinheimer-Haus EM, Corbiere TF, Koh TJ. Increased skin blood flow during low intensity vibration in human participants: analysis of control mechanisms using short-time Fourier transform. PLoS One. 2018; 13:e0200247.
52. Ren W, Pu F, Luan H, et al. Effects of local vibration with different intermittent durations on skin blood flow responses in diabetic people. Front Bioeng Biotechnol. 2019;7:310. doi:10.3389/fbioe.2019.00310
53. Stoyneva Z. Current pathophysiological views on vibration-induced Raynaud’s phenomenon. Cardiovasc Res. 2003;57:615–624. doi:10.1016/S0008-6363(02)00728-9
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.