")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 20
Effect of Surgical Masks and N95 Respirators on Anxiety
Authors Zhang Y, Yang Q , Ma Q, Wu Y, Wang Y, Chen C, Yao Y , Feng Z, Yuan X, Shi S , Zhang K
Received 31 October 2023
Accepted for publication 17 February 2024
Published 8 March 2024 Volume 2024:20 Pages 551—559
DOI https://doi.org/10.2147/NDT.S447428
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yuping Ning
Yan Zhang,1,* Qiongyao Yang,2– 4,* Qianru Ma,5,* Yuanxiong Wu,5,* Yue Wang,2– 4 Chuanchuan Chen,2– 4 Yitan Yao,2– 4 Ziqiao Feng,2,3 Xiaoping Yuan,2,3 Shengya Shi,2,3 Kai Zhang2,3
1Department of Pneumology, Second People’s Hospital of Anhui Province, Hefei, People’s Republic of China; 2Department of Psychiatry, Chaohu Hospital of Anhui Medical University, Hefei, People’s Republic of China; 3Anhui Psychiatric Center, Anhui Medical University, Hefei, People’s Republic of China; 4School of Mental Health and Psychological Sciences, Anhui Medical University, Hefei, People’s Republic of China; 5Department of Psychiatry, Third People’s Hospital of Fuyang, Fuyang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Kai Zhang, Department of Psychiatry, Chaohu Hospital of Anhui Medical University, Hefei, 238000, People’s Republic of China, Tel/Fax +86-551-82324114, Email [email protected]
Purpose: Masks are designed to reduce the spread of airborne pathogens, such as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), although wearing a mask has some adverse effects. The primary objective of this study was to explore the effects of surgical masks and N95 respirators on patients diagnosed with anxiety.
Methods: Subjects diagnosed with first-episode anxiety disorders were recruited from outpatient departments between February and July, 2023. A self-administered questionnaire was administered at baseline and at follow-up. The questionnaire addressed demographic information, Hamilton Anxiety Rating Scale (HAM-A), Hamilton Depression Rating Scale (HAM-D) and Insomnia Severity Index (ISI). Subjects were divided into three groups (n=30 each): control (no mask); surgical mask; and N95 respirator. The Kruskal–Wallis test and repeated measures analysis of variance were used to examine associations between face mask use and emotion.
Results: Ninety subjects completed the study, of whom 51 (56.67%) were male and 39 (43.33%) were female. Time and group effects were observed in HAM-A score among the 3 groups. After 4 weeks, mean (± SD) HAM-A score decreased from 32.63± 13.37 to 28.07± 9.33 in the control group, increased from 33.67± 12.47 to 36.80± 10.32 in the surgical mask group, and from 32.33± 14.73 to 41.13± 8.29 in the N95 respirator group, with no sex differences among the 3 groups. HAM-A score was significantly higher in the mask groups than that in the control group at follow-up. Only N95 respirator group exhibited significant time effects on HAM-D and ISI scores, with a decreasing trend in HAM-D score and an opposite trend in ISI score.
Conclusion: Prolonged mask use may exacerbate anxiety, especially among those wearing N95 respirator masks. In a post-pandemic environment, governments should improve public health beliefs regarding coronavirus disease 2019 and promote the safety of face mask use, thus reducing the physiological and psychological effects of improper mask use.
Keywords: anxiety, COVID-19, health beliefs, mask, N95
Introduction
The coronavirus disease 2019 (COVID-19) pandemic has increased the global prevalence and burden of mental disorders.1 Increases in the prevalence of stress, depression, anxiety, and sleep disorders have been reported during the COVID-19 pandemic.1,2 On May 5, 2023, the World Health Organization declared COVID-19 a global health emergency.3 Nevertheless, the situation remains uncertain and dynamic. Many countries have enforced compulsory face mask regulations during the COVID-19 outbreak, and a study found that policy stringency was positively associated with face mask use.4 According to Google Trends data, online searches for masks is, in large part, positively correlated with the government response stringency index but not new COVID-19 cases per million population.5 Currently, countries have reduced their response to the pandemic; however, in April 2023, the Chinese Center for Disease Control and Prevention issued a new version of mask wearing guidelines.6 During the pandemic, the mask mandate further reduced the severity of the situation.
The main modes of transmission for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) include droplets, contact, airborne and fomites.7,8 In addition to vaccination and nucleic acid testing, non-pharmaceutical interventions, such as face masks, eye protection, physical distancing, and hand hygiene, are recommended preventive measures for COVID-19.9 Wearing masks is an effective measure commonly used by the public to prevent the spread of airborne pathogens, such as SARS-CoV-2,9,10 and the most commonly used masks include cloth face masks, surgical masks, and (K)N95 respirator masks.5,11
Medical masks, frequently referred to as “surgical masks”, are designed to prevent the transmission of microorganisms from the wearer to the patient.12 Filtering facepiece respirators (also termed N95s), certified by the National Institute for Occupational Safety and Health (NIOSH) and cleared by the Food and Drug Administration (FDA), can filter at least 95% of airborne particles.13 In contrast, the N95 respirator mask is a higher-level protection mask and is designed to fit tightly, conforming to the wearer’s facial contours.9 Laboratory studies have shown that N95 respirator masks exhibit a better blocking effect on infectious viruses than the typical surgical mask.14 Results comparing the clinical effectiveness of these two types of masks, however, have been inconsistent. Some findings suggest that respirator-type masks may be more effective than surgical masks in preventing infection,10 while others have found that surgical masks and respirators did not differ in infection risk, which may be related to the fact that respirator use may lead to more adverse events.9,12 For example, adjusting a respirator-type mask due to facial discomfort may compromise the seal and increase the risk for infection.
Mask-related adverse effects include headache, shortness of breath, impaired cardiopulmonary exercise capacity, acne, pruritus, earlobe discomfort, vocal fatigue, and discomfort from ocular irritation.9,15–18 In addition, face masks that reduce the speed and ability to recognize facial expressions reflecting emotion(s) may lead to misunderstanding and confusion in communication,19,20 which in turn increases tension and anxiety. Compared with surgical masks, N95 respirator masks significantly increase the rates of headache, respiratory distress, feelings of discomfort, and psychological influence.15,21 One study found that wearing N95 or half-face respirator masks continuously for 3 h/day may produce anxiety in clinical situations.22 A scoping review reported that surgical mask or respirator use may increase anxiety, depression, and psychological distress in both the wearers and those who interact with them.23
Most of the scientific literature has focused on the effect of the COVID-19 pandemic on mood, not on masks. Earlier studies have evaluated the physiological impact(s) of mask use, but limited research has addressed psychological impact(s), and most have examined healthcare workers. The main objective of the present study, therefore, was to profile and compare the effects of surgical masks, N95 respirator masks, and no masks among subjects diagnosed with anxiety.
Materials and Methods
Study Participants and Data Collection
Subjects were recruited from the outpatient departments of multiple hospitals between February and July 2023. Surgical and N95 masks were selected as the intervention tools because they are the two most widely used medical masks. Subjects in the surgical mask and N95 respirator groups agreed to wear a surgical mask or N95 for 4 h/day when they go out or at work. All subjects were not informed in advance that wearing a mask might affect anxiety. A self-administered questionnaire was administered at baseline and at follow-up (two-week and four-week). A flow-diagram illustrating the study is shown in Figure 1. The questionnaire included questions addressing age, sex, height, weight, educational level, marital status, medical history, and scale assessments. The scales were assessed by two psychiatrists who had received uniform training using a fixed guideline to ensure consistency of scale assessment.
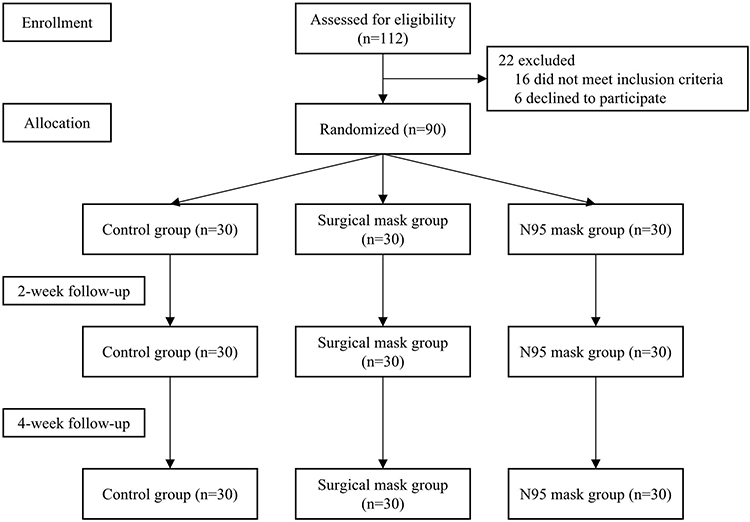 |
Figure 1 Study flowchart. |
Inclusion and Exclusion Criteria
The diagnostic criteria for anxiety disorders in the International Classification of Diseases, 10th Revision (ICD-10), subjects 18–60 years of age, first episode, junior high school education or above, and Hamilton Anxiety Rating Scale (HAM-A) score > 14. Subjects who fulfilled ICD-10 diagnostic criteria for other psychiatric disorders including schizophrenia, bipolar disorder, alcohol dependence, substance abuse, and organic mental disorders were excluded. In addition, pregnant women, those with diabetes, hypertension, heart disease, acute and chronic respiratory disease, a history of mental disorder(s), or those with frequent changes in the type of masks were also excluded.
Instruments
HAM-A
The HAM-A is an extensively used instrument to assess the severity of anxiety symptoms.24 It consists of 14 items with clinical interview measures of somatic and psychological anxiety symptoms rated on a 5-point Likert scale (scored 0 to 4). The total score ranges from 0 to 56, with higher scores indicating more anxiety symptoms. The internal consistency of the questionnaire was 0.87.
Hamilton Depression Rating Scale
The Hamilton Depression Rating Scale (HAM-D) is a standardized scale used to measure the severity of depressive symptoms.25 The scale contains 17 variables that are measured on either five-point or three-point scales. The total score ranges from 0 to 68, with higher scores indicating more depressive symptoms. In the study sample, the total Cronbach’s alpha coefficient for the HAM-D was 0.89.
Insomnia Severity Index
The Insomnia Severity Index (ISI) is a self-reported psychometric questionnaire designed to assess insomnia severity of insomnia.26 It consists of 7 items rated on a 5-point Likert scale. The total score ranges from 0 to 28, with higher scores indicating greater severity of insomnia. A score of 15 to 21 is defined as clinical insomnia (moderate severity). The internal consistency of the ISI was 0.74.
Ethics Approval and Consent
The study design was approved by the Ethics Review Committee of Chaohu Hospital of Anhui Medical University (AnHui, China, KYXM-202301-004), in accordance with the Declaration of Helsinki. The study was registered on the Chinese Clinical Trial Registry (ChiCTR) website (<www.chictr.org.cn>; ID: ChiCTR2300068020). All subjects provided informed consent and could withdraw from the trial at any time.
Statistical Analysis
Quantitative variables regarding subject characteristics are expressed as mean and standard deviation (SD) and percentages for categorical variables. The Kruskal–Wallis test and repeated measures analysis of variance (ie “ANOVA”) were used to examine the associations between face mask use and emotion. Data were plotted using Prism version 9 (GraphPad Inc., San Diego, CA, USA). All statistical analyses were performed using SPSS version 27 (IBM Corporation, Armonk, NY, USA), and differences with a two-tailed P < 0.05 were considered to be statistically significant.
Results
Demographic characteristics of the study population are summarized in Table 1. Ninety participants completed the study: 51 (56.67%) were male and 39 (43.33%) were female. The participants were allocated at a ratio of 1:1:1 to 3 groups (n=30 each): control (no mask); surgical mask; and N95 respirator mask. Subjects ranged in age from 19 to 59 years, with a mean age of 40.64 years. There were no statistically significant differences in demographic characteristics among the 3 groups at baseline.
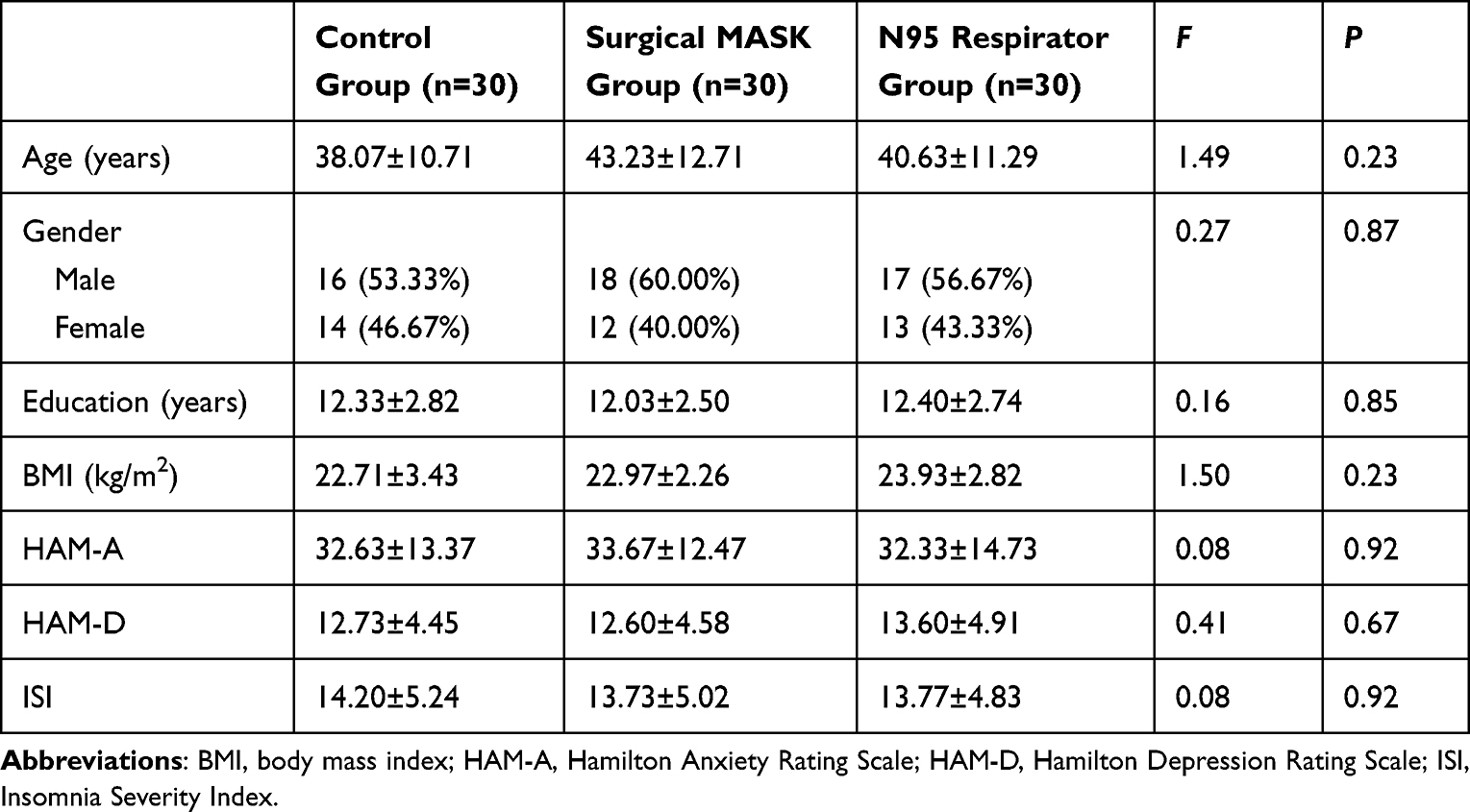 |
Table 1 Demographic Features of All Participants |
The relationship between mask use and emotion is illustrated in Figure 2. As shown in Figure 2A, time and group affected HAM-A scores. There was no significant difference in the HAM-A scores among the 3 groups at baseline. At the four-week follow-up, mean HAM-A score decreased from 32.63±13.37 to 28.07±9.33 (p<0.001, η2=0.150) in the control group, increased from 33.67±12.47 to 36.80±10.32 (p=0.071, η2=0.060) in the surgical mask group, and from 32.33±14.73 to 41.13±8.29 (p<0.001, η2=0.284) in the N95 respirator group. HAM-A score was significantly higher in the mask groups than in the control group at both the two-week (p=0.012, η2=0.070) and four-week (p<0.001, η2=0.232) follow ups. Results of analysis revealed that anxiety levels in the N95 respirator group increased significantly (p<0.001, η2=0.284). The effects of mask type on depression and sleep are shown in Figures 2B and C, respectively. Only the N95 respirator had significant time effects on HAM-D and ISI scores, with a decreasing trend for HAM-D score (p<0.001, η2=0.155) and the opposite for ISI score (p<0.001, η2=0.244).
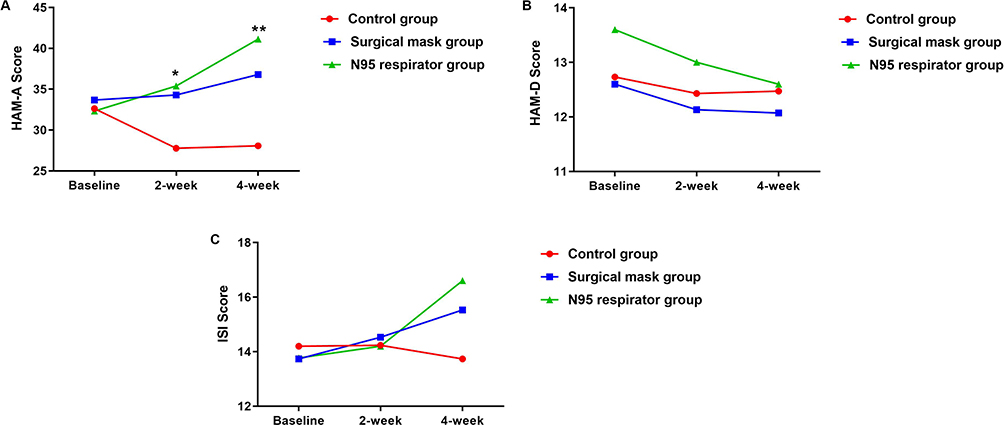 |
Figure 2 The relationship between mask use and emotion. Mean T scores in HAM-A, HAM-D, ISI are shown, respectively. (A) HAM-A, (B) HAM-D, (C) ISI. Comparison between three groups, *p<0.05, **p<0.01. Abbreviations: HAM-A, Hamilton Anxiety Rating Scale; HAM-D, Hamilton Depression Rating Scale; ISI, Insomnia Severity Index. |
The effect of mask use on HAM-A scores for the two sexes is shown in Figure 3. Among males, a time effect was observed in the N95 respirator group. It demonstrated a rising trend for anxiety level (p=0.004, η2=0.206), and the score was significantly higher than that in the control group at follow-up. Among females, the HAM-A score of the control group was lower at the two-week follow-up than at baseline. It increased in the surgical mask group at follow-up, although the difference was not significant, while it was significantly higher in the N95 respirator group than that in the control group at the four-week follow-up.
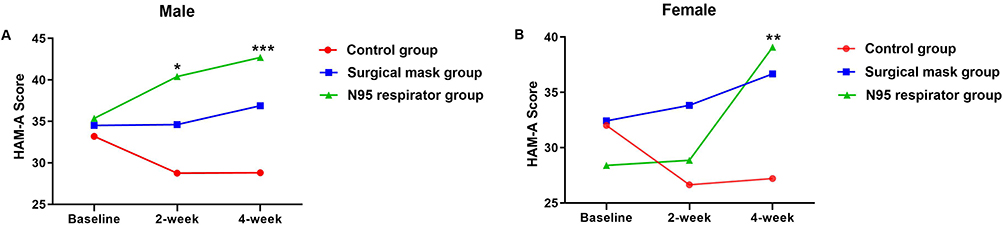 |
Figure 3 The effect of mask use on HAM-A scores for the two sexes among the three groups. (A) Male, (B) Female. Comparison between three groups, *p<0.05, **p<0.01, ***p<0.001. Abbreviations: HAM-A, Hamilton Anxiety Rating Scale. |
Discussion
The present study investigated the effects of long-duration mask use (>4 h daily) on anxiety, depression, and sleep quality, and yielded two key findings. First, wearing surgical masks and N95 respirators was significantly associated with anxiety compared with not wearing a mask, whereas no significant differences were observed for depression or sleep. Second, the N95 respirator had a more severe effect on anxiety than the surgical mask.
Previous studies have found a strong association between sex and COVID-19-related anxiety, with females being more anxious than males.27–29 Females are more sensitive to health issues than males, and previous evidence has suggested that females perceive a higher threat and fear of COVID-19 than males, and are more likely to be affected by the social and economic consequences of the pandemic.30,31 A study investigating mask preferences found that females were more likely to prefer surgical masks, whereas males preferred cloth masks.11 In South Korea, 82.9% of subjects responded that they would be anxious without wearing a mask,32 the proportion of no anxiety about not wearing a mask was higher among males, and the reasons for anxiety included the risk for droplet transmission of COVID-19, negative public opinion, and the habit of wearing a mask. A total of 41.4% of freelancers reported that they would not wear a mask immediately after the end of the COVID-19 pandemic. Conceivably, individuals with anxiety are more likely to wear masks because they have a strong desire to rid themselves of infection and/or prevent reinfection. The current study did not find a sex-based difference in the effect of mask use on anxiety, possibly because the subjects were patients diagnosed with anxiety.
A study investigating the psychological influence of wearing different masks for 8 h/day among healthcare workers found no emotional symptoms in the surgical mask group, while there was 1 case of anxiety and 3 cases of depression in the N95 mask group, although these psychological effects were short-term.33 The work performance of mask wearers was poorer than that of those without masks, and high-anxiety individuals were more affected by mask wearing than low-anxiety individuals.34 Unexpectedly, a possible explanation for the failure of nitrous oxide to produce an analgesic effect in some patients is that masks increase the level of anxiety in children.35 Nevertheless, the relationship between anxiety and masks remains unclear. An exploratory review revealed that mask-wearing may be perceived by individuals with high social anxiety as reducing anxiety, but actually impairs social performance while increasing anxiety.36 Individuals experiencing anxiety often seek to restore their feelings of control using various coping strategies. Some researchers have found that anxiety about COVID-19 was positively associated with the propensity to wear a mask during the pandemic and that the degree of mask wearing mediated the relationship between anxiety and restored feelings of control.37
Health beliefs about COVID-19 were related to face mask use. Individuals with better knowledge of the disease pandemic and higher perceived self-efficacy to wear masks properly were less likely to report depressive symptoms,38 while older individuals who reused facemasks more clearly exhibited depressive symptoms.39 Personal protective equipment (PPE), including masks, gloves, goggles, face shields, and gowns, is used to reduce exposure to health and safety hazards.23 A cross-sectional survey found that anxiety and depression symptoms were lower among respondents in whom PPE needs were being met.40 A plausible reason why our study did not find a significant effect of wearing a mask on depression is that the government’s active propagation of knowledge regarding epidemic prevention and control, continuously optimized mask guidelines and ensured consistent face mask supply, thereby improving individuals’ COVID-19 health literacy.
The present study suggests that prolonged use of masks increases anxiety, which may be explained by several potential reasons. The first is a classical conditioning response in which masks have been associated with the pandemic. Face masks can reduce the spread of respiratory diseases, and people were asked to wear masks in public places during the COVID-19 outbreak. Masks provide protection while their presence increase anxiety because of the pairing of masks with an emergency. Next, improper mask wearing practice is associated with the increased risk of anxiety.41,42 As the participants were not hospitalized patients, we unable to ensure that the mask groups were wearing masks correctly. Lastly, N95 respirators may show more pronounced side effects than surgical masks.9 Physio-metabolic side effects of face-mask wearing, such as hypoxia, may exacerbate anxiety.43
Anxiety and insomnia are mutual risk factors.44 Individuals with anxiety often experience sleep disturbances, and insufficient sleep can further exacerbate anxiety.45 However, the exact mechanisms that underlie sleep and anxiety remain unclear. In this study, after wearing the N95 respirator for 4 weeks, patients with anxiety reached the level of clinical insomnia, which is consistent with previous research demonstrating that N95 respirators could reduce sleep quality.43 Whether wearing an N95 respirator further increases insomnia by increasing the severity of anxiety or directly is unclear and requires further research.
Accumulating evidence has shown that SARS-CoV-2 infection can lead to long-term sequelae affecting multiple organ systems; this condition is commonly referred to as “long COVID”.46,47 More specifically, these symptoms included headache(s), fatigue, dyspnea, palpitations, skin rash, muscle pain, anxiety, depression, and sleeplessness. Currently, there are no clear guidelines directing the safe use of masks among individuals with emotional disorders. The survey found that more than one-half of respondents used social media as the main source of information on COVID-1948 and information searches on social media were positively correlated with mask use. Findings of the present study can be used to analyze mask use in anxious patients, improve the public’s COVID-19-related health beliefs, and adjust mask-wearing recommendations. For example, in concerted efforts by the media, governments may disseminate important information on the effectiveness of face masks and promote the safety of face mask use, thereby reducing the risk for physiological and psychological effects caused by improper mask use.
The present study had some limitations. First, no measures were taken to control the time of the subjects wearing a mask per day because they were recruited from outpatient clinics, although we obtained written consent. Rigorous research design is needed in the future, such as the use of time management software contributing to the understanding of the true duration of mask wear. Previous studies investigating the effects of masks on emotion(s) have focused on healthcare workers; therefore, investigation of outpatients is meaningful. Second, we did not investigate whether participants were aware that prolonged mask use was associated with mood. If participants believed the mask would make them more anxious, it could have led to a nocebo effect. The follow-up study intends to recruit patients with anxiety and randomly divide them into control group and experimental group. Both groups will wear the same type of mask and for the same amount of time, the duration of mask wearing will be standardized and recorded but the experimental group will be told that prolonged use of the mask may aggravate anxiety, to verify the presence of an anti-placebo effect. Third, this study only analyzed the effects of masks on anxiety, and we acknowledge that other predisposing factors, such as stress, personality traits, occupation, climate, and behavioral factors, may also exacerbate anxiety. In addition, participants came from different regions with different epidemic risks, which could also have an impact on anxiety. Further research is needed into the reasons why masks increase anxiety. Finally, the small sample size was a limitation of the present study; as such, more research based on larger samples should be conducted to understand the impact of masks on emotions.
Conclusions
This study showed that compared with not wearing a mask, surgical and N95 respirator masks exacerbated anxiety, especially the N95 respirator. Masks are an effective tool for mitigating the spread of respiratory viruses. In a post-pandemic environment, individuals are encouraged to use appropriate types of masks to ensure comfort and safety, rather than avoiding mask or respirator use. Further research is needed to determine why mask use is associated with greater anxiety, which would be beneficial for governments taking action to promote the safety of face mask use, and thus reduce the risk for physiological and psychological effects caused by the improper use of masks.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent
This study was approved by the ethical review board of Chaohu Hospital of Anhui Medical University (AnHui, China, KYXM-202301-004), which conformed to the principles embodied in the Declaration of Helsinki. Informed consent was obtained from participants involved in the study.
Acknowledgments
The authors thank the Chaohu Hospital of Anhui Medical University.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by grants from the China International Medical Exchange Foundation (Z-2018-35-2002), the Anhui Province Outstanding Young Talents Support Program (gxyqZD2022022), the University Natural Science Research Key Project of Anhui Provincial Department of Education (2023AH050647), and the Research Fund of Anhui Medical University (2020xkj051). The funders had no role in the study design, data collection, and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Santomauro DF, Mantilla Herrera AM, Shadid J. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet. 2021;398(10312):1700–1712. doi:10.1016/S0140-6736(21)02143-7
2. Pappa S, Ntella V, Giannakas T, Giannakoulis VG, Papoutsi E, Katsaounou P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: a systematic review and meta-analysis. Brain Behav Immun. 2020;88:901–907. doi:10.1016/j.bbi.2020.05.026
3. Nations U. WHO chief declares end to COVID-19 as a global health emergency; 2023. Available from: https://news.un.org/en/story/2023/05/1136367.
4. Wismans A, van der Zwan P, Wennberg K, et al. Face mask use during the COVID-19 pandemic: how risk perception, experience with COVID-19, and attitude towards government interact with country-wide policy stringency. BMC Public Health. 2022;22(1):1622. doi:10.1186/s12889-022-13632-9
5. Yeung AWK, Parvanov ED, Horbanczuk JO, et al. Public interest in different types of masks and its relationship with pandemic and policy measures during the COVID-19 pandemic: a study using Google Trends data. Front Public Health. 2023;11:1010674. doi:10.3389/fpubh.2023.1010674
6. Chinese Center for Disease Control and Prevention. Notice on issuing guidelines for the wearing of masks by the public to prevent the infection of the novel coronavirus; 2023. Available from: https://www.gov.cn/lianbo/2023-04/12/content_5751073.htm.
7. Sommerstein R, Fux CA, Vuichard-Gysin D, et al. Risk of SARS-CoV-2 transmission by aerosols, the rational use of masks, and protection of healthcare workers from COVID-19. Antimicrob Resist Infect Control. 2020;9(1):100. doi:10.1186/s13756-020-00763-0
8. Ahmad MDF, Wahab S, Ali Ahmad F, et al. A novel perspective approach to explore pros and cons of face mask in prevention the spread of SARS-CoV-2 and other pathogens. Saudi Pharm J. 2021;29(2):121–133. doi:10.1016/j.jsps.2020.12.014
9. Kunstler B, Newton S, Hill H, et al. P2/N95 respirators & surgical masks to prevent SARS-CoV-2 infection: effectiveness & adverse effects. Infect Dis Health. 2022;27(2):81–95. doi:10.1016/j.idh.2022.01.001
10. Chu DK, Akl EA, Duda S, et al. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: a systematic review and meta-analysis. Lancet. 2020;395(10242):1973–1987. doi:10.1016/S0140-6736(20)31142-9
11. Mouliou DS, Pantazopoulos I, Gourgoulianis KI. Medical/surgical, cloth and FFP/(K)N95 Masks: unmasking preference, SARS-CoV-2 transmissibility and respiratory side effects. J Pers Med. 2022;12(3):325. doi:10.3390/jpm12030325
12. Radonovich LJ, Simberkoff MS, Bessesen MT, et al. N95 respirators vs medical masks for preventing influenza among health care personnel: a randomized clinical trial. JAMA. 2019;322(9):824–833. doi:10.1001/jama.2019.11645
13. Bradford Smith P, Agostini G, Mitchell JC. A scoping review of surgical masks and N95 filtering facepiece respirators: learning from the past to guide the future of dentistry. Saf Sci. 2020;131:104920. doi:10.1016/j.ssci.2020.104920
14. Noti JD, Lindsley WG, Blachere FM, et al. Detection of infectious influenza virus in cough aerosols generated in a simulated patient examination room. Clin Infect Dis. 2012;54(11):1569–1577. doi:10.1093/cid/cis237
15. Fikenzer S, Uhe T, Lavall D, et al. Effects of surgical and FFP2/N95 face masks on cardiopulmonary exercise capacity. Clin Res Cardiol. 2020;109(12):1522–1530. doi:10.1007/s00392-020-01704-y
16. Ribeiro VV, Dassie-Leite AP, Pereira EC, Santos ADN, Martins P, Irineu RA. Effect of wearing a face mask on vocal self-perception during a pandemic. J Voice. 2022;36(6):878 e871–878 e877. doi:10.1016/j.jvoice.2020.09.006
17. Chaiyabutr CST, Pruksaeakanan C, Thumrongtharadol J, Boonchai W, Boonchai W. Adverse skin reactions following different types of mask usage during the COVID-19 pandemic. J Eur Acad Dermatol Venereol. 2021;35(3):e173–e176. doi:10.1111/jdv.17039
18. Burgos-Blasco B, Arriola-Villalobos P, Fernandez-Vigo JI, et al. Face mask use and effects on the ocular surface health: a comprehensive review. Ocul Surf. 2023;27:56–66. doi:10.1016/j.jtos.2022.12.006
19. Williams WC, Haque E, Mai B, Venkatraman V. Face masks influence emotion judgments of facial expressions: a drift-diffusion model. Sci Rep. 2023;13(1):8842. doi:10.1038/s41598-023-35381-4
20. Rinck M, Primbs MA, Verpaalen IAM, Bijlstra G. Face masks impair facial emotion recognition and induce specific emotion confusions. Cogn Res Princ Implic. 2022;7(1):83. doi:10.1186/s41235-022-00430-5
21. Ipek S, Yurttutan S, Gullu UU, Dalkiran T, Acipayam C, Doganer A. Is N95 face mask linked to dizziness and headache? Int Arch Occup Environ Health. 2021;94(7):1627–1636. doi:10.1007/s00420-021-01665-3
22. Cohen ER, Pena S, Misztal C, et al. N95 vs half-face respirator wear in surgical trainees: physiologic and psychological effects of prolonged use. OTO Open. 2021;5(4):2473974X211065437. doi:10.1177/2473974X211065437
23. Leung R, Cook MM, Capra MF, Johnstone KR. The contribution of respiratory and hearing protection use to psychological distress in the workplace: a scoping review. Int Arch Occup Environ Health. 2022;95(8):1647–1659. doi:10.1007/s00420-022-01863-7
24. Hamilton M. The assessment of anxiety states by rating. Br J Med Psychol. 1959;32(1):50–55. doi:10.1111/j.2044-8341.1959.tb00467.x
25. Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. 1960;23(1):56–62. doi:10.1136/jnnp.23.1.56
26. Bastien CH, Vallières A, Morin CM. Validation of the insomnia severity index as an outcome measure for insomnia research. Sleep Med. 2001;2(4):297–307. doi:10.1016/S1389-9457(00)00065-4
27. Metin A, Erbicer ES, Sen S, Cetinkaya A. Gender and COVID-19 related fear and anxiety: a meta-analysis. J Affect Disord. 2022;310:384–395. doi:10.1016/j.jad.2022.05.036
28. Santabarbara J, Lasheras I, Lipnicki DM, et al. Prevalence of anxiety in the COVID-19 pandemic: an updated meta-analysis of community-based studies. Prog Neuropsychopharmacol Biol Psychiatry. 2021;109:110207. doi:10.1016/j.pnpbp.2020.110207
29. Pashazadeh Kan F, Raoofi S, Rafiei S, et al. A systematic review of the prevalence of anxiety among the general population during the COVID-19 pandemic. J Affect Disord. 2021;293:391–398. doi:10.1016/j.jad.2021.06.073
30. Rodriguez-Rey R, Garrido-Hernansaiz H, Collado S. Psychological impact and associated factors during the initial stage of the coronavirus (COVID-19) pandemic among the general population in Spain. Front Psychol. 2020;11:1540. doi:10.3389/fpsyg.2020.01540
31. Nino M, Harris C, Drawve G, Fitzpatrick KM. Race and ethnicity, gender, and age on perceived threats and fear of COVID-19: evidence from two national data sources. SSM Popul Health. 2021;13:100717. doi:10.1016/j.ssmph.2020.100717
32. Kwon M, Yang W. Mask-wearing behaviors after two years of wearing masks due to COVID-19 in Korea: a cross-sectional study. Int J Environ Res Public Health. 2022;19(22):14940.
33. Su CY, Peng CY, Liu HL, Yeh IJ, Lee CW. Comparison of effects of N95 respirators and surgical masks to physiological and psychological health among healthcare workers: a randomized controlled trial. Int J Environ Res Public Health. 2021;18(24):13308. doi:10.3390/ijerph182413308
34. Johnson AT, Dooly CR, Blanchard CA, Brown EY. Influence of anxiety level on work performance with and without a respirator mask. Am Ind Hyg Assoc J. 1995;56(9):858–865. doi:10.1080/15428119591016485
35. Kanagasundaram SALL, Cavalletto BP, Keneally JP, Cooper MG, Cooper MG. Efficacy and safety of nitrous oxide in alleviating pain and anxiety during painful procedures. Arch Dis Child. 2001;84(6):492–495. doi:10.1136/adc.84.6.492
36. Saint SA, Moscovitch DA. Effects of mask-wearing on social anxiety: an exploratory review. Anxiety Stress Coping. 2021;34(5):487–502. doi:10.1080/10615806.2021.1929936
37. Schneider AB, Leonard B. From anxiety to control: mask-wearing, perceived marketplace influence, and emotional well-being during the COVID-19 pandemic. J Consum Aff. 2022;56(1):97–119. doi:10.1111/joca.12412
38. Bressington DT, Cheung TCC, Lam SC, et al. Association between depression, health beliefs, and face mask use during the COVID-19 pandemic. Front Psychiatry. 2020;11:571179. doi:10.3389/fpsyt.2020.571179
39. Kwan RYC, Lee PH, Cheung DSK, Lam SC. Face mask wearing behaviors, depressive symptoms, and health beliefs among older people during the COVID-19 pandemic. Front Med. 2021;8:590936. doi:10.3389/fmed.2021.590936
40. Smith PM, Oudyk J, Potter G, Mustard C. The association between the perceived adequacy of workplace infection control procedures and personal protective equipment with mental health symptoms: a cross-sectional survey of Canadian health-care workers during the COVID-19 pandemic: l’association entre le caractere adequat percu des procedures de controle des infections au travail et de l’equipement de protection personnel pour les symptomes de sante mentale. Un sondage transversal des travailleurs de la sante canadiens durant la pandemie COVID-19. Can J Psychiatry. 2021;66(1):17–24. doi:10.1177/0706743720961729
41. Xu Q, Mao Z, Wei D, et al. Association between mask wearing and anxiety symptoms during the outbreak of COVID 19: a large survey among 386,432 junior and senior high school students in China. J Psychosom Res. 2022;153:110709. doi:10.1016/j.jpsychores.2021.110709
42. Li Q, Tarimo CS, Miao Y, Zeng X, Wu C, Wu J. Effects of mask wearing on anxiety of teachers affected by COVID-19: a large cross-sectional study in China. J Affect Disord. 2021;281:574–580. doi:10.1016/j.jad.2020.11.113
43. Varman A, Nithiya DR, Meghna C, et al. Influence of N95 mask-related hypoxemia on headache, stress, anxiety, and quality of sleep during COVID-19 patient care among frontline health care professionals. J Assoc Physicians India. 2023;71(3):11–12. doi:10.5005/japi-11001-0176
44. Glidewell RN, McPherson Botts E, Orr WC. Insomnia and anxiety: diagnostic and management implications of complex Interactions. Sleep Med Clin. 2015;10(1):93–99. doi:10.1016/j.jsmc.2014.11.008
45. Chellappa SL, Aeschbach D. Sleep and anxiety: from mechanisms to interventions. Sleep Med Rev. 2022;61:101583. doi:10.1016/j.smrv.2021.101583
46. Crook H, Raza S, Nowell J, Young M, Edison P. Long covid-mechanisms, risk factors, and management. BMJ. 2021;374:n1648. doi:10.1136/bmj.n1648
47. Schou TM, Joca S, Wegener G, Bay-Richter C. Psychiatric and neuropsychiatric sequelae of COVID-19 - A systematic review. Brain Behav Immun. 2021;97:328–348. doi:10.1016/j.bbi.2021.07.018
48. Iyamu I, Apantaku G, Yesufu Z, et al. Is social media, as a main source of information on COVID-19, associated with perceived effectiveness of face mask use? Findings from six sub-saharan African countries. Glob Health Promot. 2022;29(3):86–96. doi:10.1177/17579759211065489
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.