")
Back to Journals » Journal of Inflammation Research » Volume 17
Dynamic Changes and Clinical Significance of Plasma Galectin-3 in Patients with Acute Ischemic Stroke Undergoing Endovascular Therapy
Authors Yao M , Liang D, Zeng X, Xie X, Gao J, Huang L
Received 17 December 2023
Accepted for publication 12 February 2024
Published 1 March 2024 Volume 2024:17 Pages 1377—1387
DOI https://doi.org/10.2147/JIR.S455401
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Subashchandrabose Chinnathambi
Mingzheng Yao,1 Dan Liang,2 Xiuli Zeng,1 Xiaomei Xie,1 Jiali Gao,1 Li’an Huang1
1Department of Neurology, The First Affiliated Hospital, Jinan University, Guangzhou, People’s Republic of China; 2Department of Neurology, The Sixth Affiliated Hospital, School of Medicine, South China University of Technology, Foshan, People’s Republic of China
Correspondence: Li’an Huang, Department of Neurology, The First Affiliated Hospital, Jinan University, Guangzhou, People’s Republic of China, Email [email protected]
Purpose: Galectin-3 is a key regulator of microglial proliferation and activation and may have dual and time-dependent effects on ischemic stroke. This study aimed to prospectively investigate the dynamic changes in Galectin-3 levels in patients with acute ischemic stroke receiving endovascular therapy and its clinical significance.
Patients and Methods: A total of 105 patients with acute ischemic stroke who underwent endovascular therapy were prospectively enrolled. Plasma Galectin-3 was quantitatively detected by an enzyme-linked immunosorbent assay before the operation and at 1 day, 3 days and 7 days after the operation. A linear mixed-effect model, Pearson correlation analysis and receiver operating characteristic (ROC) curve analysis were used to evaluate the dynamic changes in the plasma Galectin-3 concentration and its relationship with clinical outcomes.
Results: Increases in plasma Galectin-3 levels at 1 day and 3 days after surgery were associated with early neurological deterioration and death (both P < 0.05). Increased Galectin-3 levels before surgery and at 1 day and 3 days after surgery were associated with poor prognosis (P < 0.05). Pearson correlation analysis revealed that Galectin-3 levels before surgery (r =0.318, P =0.002), at 1 day (r =0.318, P =0.001), 3 days (r =0.429, P < 0.001) and 7 days after surgery (r =0.340, P =0.001) were positively correlated with NIHSS scores. The ROC curve results showed that Galectin-3 concentration had a certain predictive value for death at 1 day (AUC=0.707, P=0.013), 3 days (AUC=0.708, P=0.016) and 7 days after the operation (AUC=0.708, P=0.016), but this predictive value was lower than that of the NIHSS score.
Conclusion: In acute ischemic stroke patients receiving endovascular therapy, an increase in the plasma Galectin-3 levels were associated with death, poor prognosis, and early neurological deterioration. Galectin-3 levels were significantly correlated with the NIHSS score and had a certain predictive value for death.
Plain Language Summary: Galectin-3 is a key regulator of microglial proliferation and activation and may have dual and time-dependent effects on ischemic stroke. However, relevant clinical studies are less at present. In this study, we found that an increase in the plasma Galectin-3 levels had significant values in death, poor prognosis, and early neurological deterioration in acute ischemic stroke patients receiving endovascular therapy at various times.
Keywords: ischemic stroke, Galectin-3, endovascular therapy, inflammation, dynamic change, outcome
Introduction
Since 2015, stroke has become the leading cause of death and disability in China, placing an enormous burden on the country’s health care system and economic development.1 Tissue damage after cerebral ischemia is caused by complex pathophysiological processes such as excitotoxicity, peri-infarction depolarization, inflammation, and apoptosis.2 The number of microglia in the core area of infarction immediately decreases after ischemic stroke, while the number of microglia in the ischemic penumbra increases within a few hours after stroke and peaks at 48–72 hours.3 Galectin-3 is a conserved carbohydrate recognition domain (CRD) that contains approximately 130 amino acids and a variety of bioactivity-binding proteins.4 Galectin-3 is a key regulator of microglial activation and proliferation.5 Both probiotics and adaptive immune responses6 are pleiotropic and contribute to the occurrence and progression of ischemic stroke by influencing inflammatory signaling pathways,7–9 angiogenesis,10–12 neurogenesis,13 and the regulation of apoptotic pathways.10
Galectin-3 tends to cause neurotoxic effects in the acute inflammatory phase of acute ischemic stroke, while it plays a neuroprotective role in the subchronic phase by promoting the polarization of classical proinflammatory M1 microglia into the anti-inflammatory M2 type with healing activity.5,9,14–16 The dual effects of Galectin-3 on the AIS appear to be significantly time dependent. Clinical studies have shown that Galectin-3 at baseline has potential value in the diagnosis and prediction of clinical outcomes in patients with AIS17–20 and is expected to have therapeutic potential as a poststroke immunomodulatory molecule.21 A study involving 3082 patients with AIS showed that high baseline Galectin-3 levels are associated with poor prognosis, poststroke death, and severe disability.17 However, it is unclear whether high Galectin-3 expression in patients with AIS at different time points has different predictive value for clinical outcomes. The objective of this study was to investigate the dynamic changes in plasma Galectin-3 levels in patients with AIS and its relationship with death, poor prognosis and early neurological deterioration.
Materials and Methods
Study Design
This was a prospective observational study. Blood samples from patients with AIS receiving endovascular therapy were collected before the operation and at 1 day, 3 days and 7 days after the operation. Plasma Galectin-3 levels were detected by enzyme-linked immunosorbent assay (ELISA), and clinical data were collected. The dynamic changes in the plasma Galectin-3 concentration and its correlation and predictive value for death, poor prognosis and early neurological deterioration were investigated by using a linear mixed effects model,22,23 Pearson correlation analysis and receiver operating characteristic (ROC) curve analysis. The primary outcome of this study was death within 90 days after endovascular therapy. The causes of death included hemorrhage transformation, malignant brain edema, infarction progression, hernia of brain, neurological function deterioration and so on. The secondary outcomes were poor prognosis at 90 days (mRS score > 2) and early neurological deterioration. This study was approved by the Ethics Committee of the First Affiliated Hospital of Jinan University. All the subjects or authorized subjects signed informed consent, and the study complied with the principles of the Helsinki Declaration.
Patient Selection
A total of 138 inpatients with AIS who underwent endovascular therapy at the Department of Neurology of the First Affiliated Hospital of Jinan University from September 2022 to July 2023 were retrospectively included in this study. Thirty-three patients were excluded; 13 patients had an onset time > 24 h, 8 patients had a preonset mRS score > 2, 3 patients had malignant tumors and other diseases with a low expected survival rate, 2 patients had missing clinical data, 4 patients refused to provide venous blood samples, and 3 patients were lost to follow-up. After strictly following the inclusion and exclusion criteria of this study, a total of 105 patients were ultimately enrolled. The inclusion criteria were as follows: (1) ≥18 years of age, (2) had AIS with intracranial large vessel occlusion confirmed by clinical symptoms and brain imaging, (3) had an onset time < 24 hours, and (4) provided informed consent. The exclusion criteria for patients were as follows: (1) mRS score > 2 points before the onset of the disease; (2) severe immunodeficiency disease, severe hepatic and renal insufficiency, cardiogenic shock, malignant tumor and other expected survival rates < 90 days; (3) recent history of severe active massive bleeding; (4) inability to provide venous blood samples with incomplete clinical data; and (5) refusal of a 90-day postoperative follow-up.
Collection of Baseline Data
The general baseline data included age, sex, previous medical history, time from onset to vascular revascularization, baseline National Institutes of Health Stroke Scale (NIHSS) score, intravenous thrombolysis (yes or no), admission blood glucose, low-density lipoprotein, etc. The etiology of stroke was classified as large-artery atherosclerosis (LAA), cardioembolism (CE), or stroke of undetermined etiology (SUE) according to the Trial of Org 10,172 in Acute Stroke Treatment (TOAST) standard.24 The posterior circulation vessel was recorded as the vertebral basilar artery, and the anterior circulation vessel was recorded as the middle cerebral artery. The above evaluation was performed by a professional neurologist. All patients enrolled in this study underwent successful reperfusion therapy, which was defined as a modified cerebral infarction thrombolysis (mTICI) score of grade 2b/3.25
Detection of Plasma Galectin-3
Peripheral venous blood samples of 2 mL were collected in EDTA tubes before the operation and at 1 day, 3 days and 7 days after the operation. Immediately after collection, the samples were sent to the laboratory for centrifugation (1000 × g, 15 min, 4 °C); 500 μL of the supernatant was placed in an Eppendorf (EP) tube; and the supernatant was stored at −80 °C until the experimental analysis. A human soluble galactoside-binding lectin 3 (Lgals3) ELISA kit (CSB-E11807h, Wuhan Huamei Bioengineering Co., Ltd., China) was used for the quantitative detection of plasma Galectin-3 levels by laboratory technicians who were blinded to the baseline clinical characteristics of the patients. The experimental procedure was carried out in strict accordance with the kit instructions.
Clinical Score
Statistical Analysis
All the statistical analyses and plots were generated with SPSS 22.0 software and GraphPad Prism 9.5 software. Continuous variables are expressed as (x±s) or median interquartile (IQR), and categorical variables are expressed as percentages. Fisher’s exact test or χ²-test was used for qualitative variables. Kolmogorov–Smirnov tests were used to test the normality of the data. Normally distributed quantitative variables were compared between two groups by t tests; otherwise, the Mann–Whitney U-test was used. A linear mixed effects model was used to evaluate the intergroup differences in the plasma Galectin-3 levels among the different subgroups. All patients were selected as subjects, and four time points were used as replicate indicators. The replication covariance type was AR (1), and Galectin-3 was used as the dependent variable. The number of repetitions and group were used as fixed effect factors, and the main effects were compared. Bonferroni correction was used for confidence interval adjustment. Pearson correlation analysis was used to evaluate the correlation between plasma Galectin-3 levels and NIHSS scores at different time points. A receiver operating characteristic (ROC) curve was plotted to analyze the predictive value of the plasma Galectin-3 concentration for death. α =0.05 was used as the test level, and P < 0.05 was considered to indicate statistical significance.
Results
Baseline Characteristics of the Participants in the Primary Outcome Group
In this study, 14 patients died, and 91 survived. Comparison and analysis of the baseline data between the two groups suggested that the age of patients in the nonsurviving group (P =0.006), preoperative NIHSS score (P =0.009), and preoperative thrombolytic therapy (P =0.031) were significantly greater than those in the surviving group (Table 1).
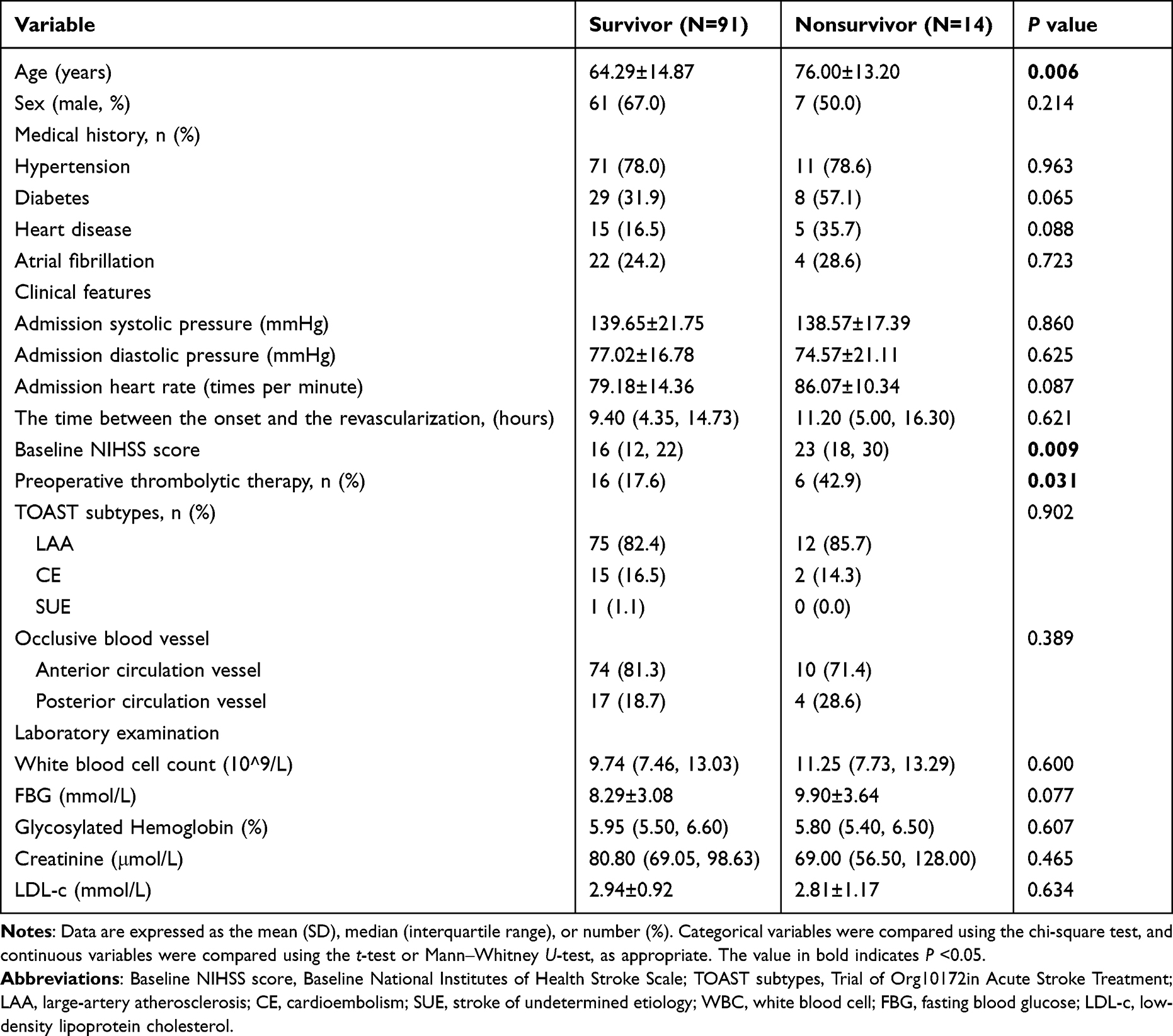 |
Table 1 Baseline Data of the Survivor Group and Nonsurvivor Group |
Plasma Galectin-3 Concentration and NIHSS Scores in All Patients
The NIHSS score of patients showed a continuous downward trend within 7 days after the operation (Figure 1A), suggesting that the neurological recovery of patients after the operation was significantly improved. The plasma Galectin-3 concentration continued to decrease within 3 days after the operation and then increased slightly to 7 days after the operation (Figure 1B). Through Pearson correlation analysis, we further found that Galectin-3 levels were positively correlated with NIHSS scores before the operation (Figure 1C) and 1 day (Figure 1D), 3 days (Figure 1E) and 7 days (Figure 1F) after the operation (P <0.05).
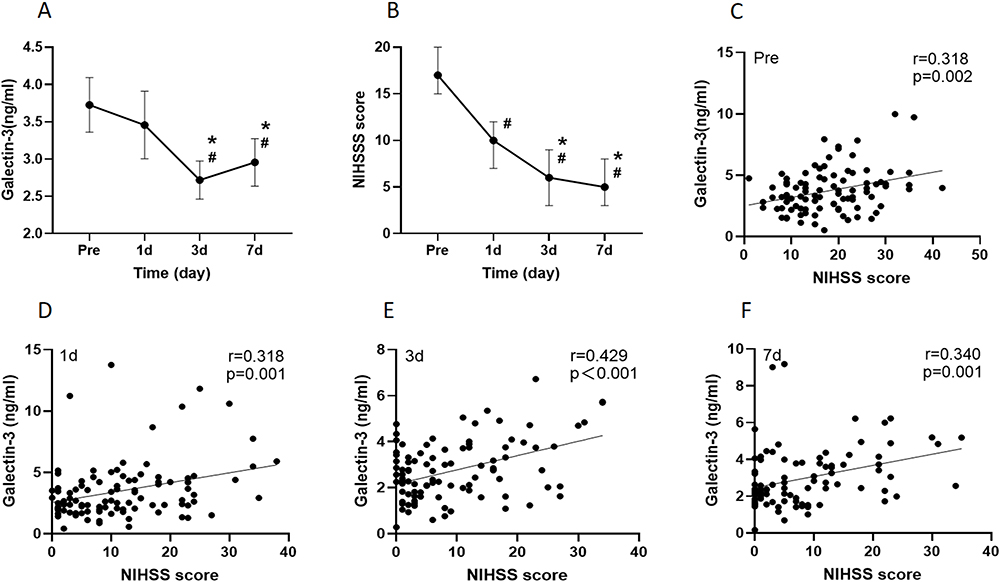 |
Figure 1 The dynamic changes in Galectin-3 and NIHSS scores and the correlation between them. Abbreviations: Pre, preoperation; 1d, 1 day after the operation; 3d, 3 days after the operation; 7d, 7 days after the operation; NIHSS, National Institute of Health Stroke Scale. Notes: The dynamic changes in Galectin-3 levels (A) and NIHSS scores (B) in all patients. The relationship between Galectin-3 levels and NIHSS scores before (C), 1 day (D), 3 days (E), and 7 days (F) was determined by Pearson correlation analysis (all P < 0.05). #Indicates P < 0.05 vs preoperation, *Indicates P < 0.05 vs 1 day from (A and B). |
Plasma Galectin-3 Concentration and NIHSS Score at Death
In this study, 14 patients died, and 91 survived. The plasma Galectin-3 concentration in the death group first increased until the first day after the operation, then decreased at 3 days after the operation, and finally increased slightly until 7 days after the operation, which differed from that in the survival group (Figure 2A). The linear mixed-effect model identified the significant influence of group (P =0.007) on the Galectin-3 levels but did not reveal the time (P =0.570) or the interaction effect between the two (P =0.888), as shown in Table 2. The Galectin-3 levels (Figure 2A) and NIHSS scores (Figure 2B) were greater in the nonsurviving group than in the surviving group before the operation and at 1 day, 3 days and 7 days after the operation. An increase in the Galectin-3 levels at 1 day (P =0.036) and 3 days after the operation (P =0.032) was associated with death.
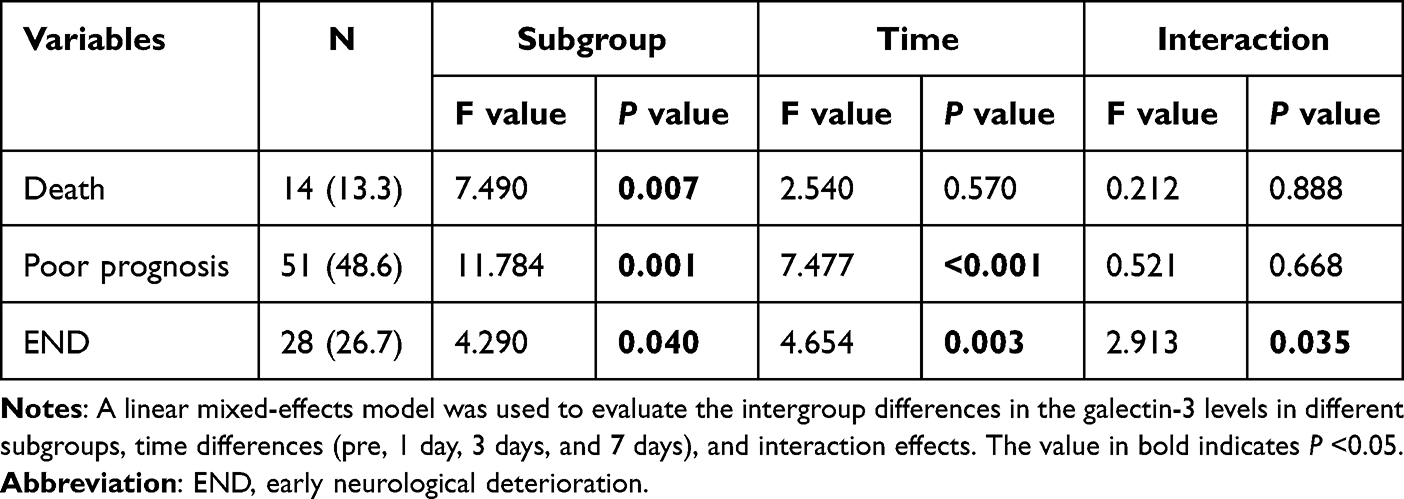 |
Table 2 Subgroup Analysis of the Dynamic Changes in Galectin-3 Levels |
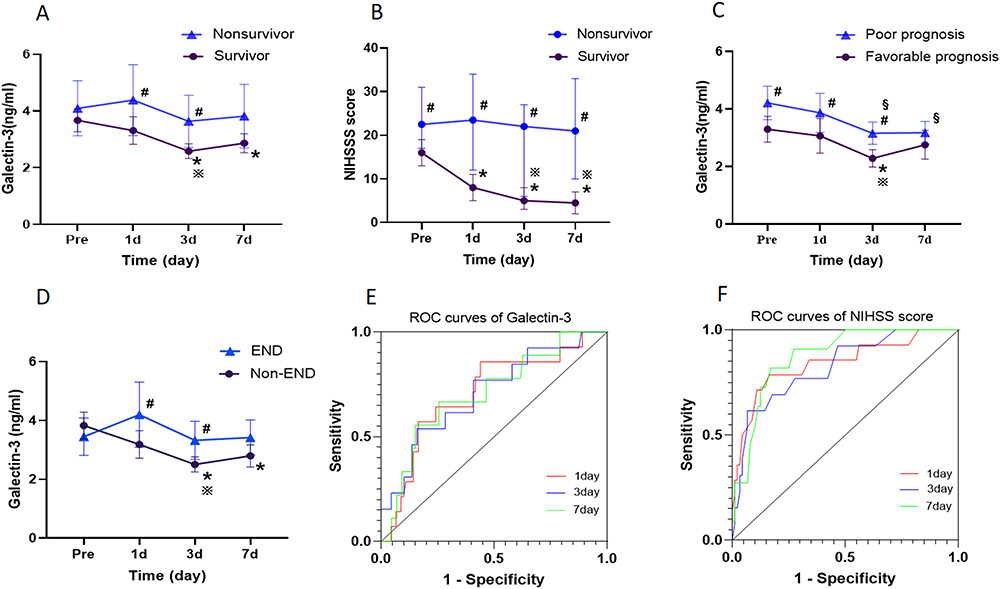 |
Figure 2 Dynamic changes in Galectin-3 levels and NIHSS score and their predictive value for death. Abbreviations: Pre, preoperation; 1d, 1 day after the operation; 3d, 3 days after the operation; 7d, 7 days after the operation; NIHSS, National Institute of Health Stroke Scale; END, early neurological deterioration; Non-END, Nonearly neurological deterioration. Notes: The dynamic changes in the Galectin-3 levels (A) and NIHSS scores (B) between the nonsurvivor group and survivor group. The dynamic changes in the Galectin-3 levels between the poor prognosis group and favorable prognosis group (C) and between the END group and non-END group (D). The predictive value of Galectin-3 (E) and the NIHSS score (F) for death events at 1 day, 3 days, and 7 days was determined using an ROC curve. A linear mixed effects model was used to compare the two groups and compare the different time periods within the groups. #Indicates P < 0.05 vs the survivor group, the favorable group and the non-END group from (A–D); *Indicates P < 0.05 vs pre; ※Indicates P < 0.05 vs 1 day from (A–D). § indicates P < 0.05 vs pre in poor prognosis group (C). |
ROC curve analysis revealed that the Galectin-3 levels at 1 day (AUC=0.707, P=0.013), 3 days (AUC=0.708, P=0.016) and 7 days after surgery (AUC=0.707, P=0.041) were significant predictors of death (Figure 2E and Table 3). The sensitivity and specificity were 0.857 and 0.560, 0.538 and 0.841, and 0.667 and 0.744, respectively. However, the predictive value of the Galectin-3 levels for death was lower than that of the NIHSS scores (Figure 2F).
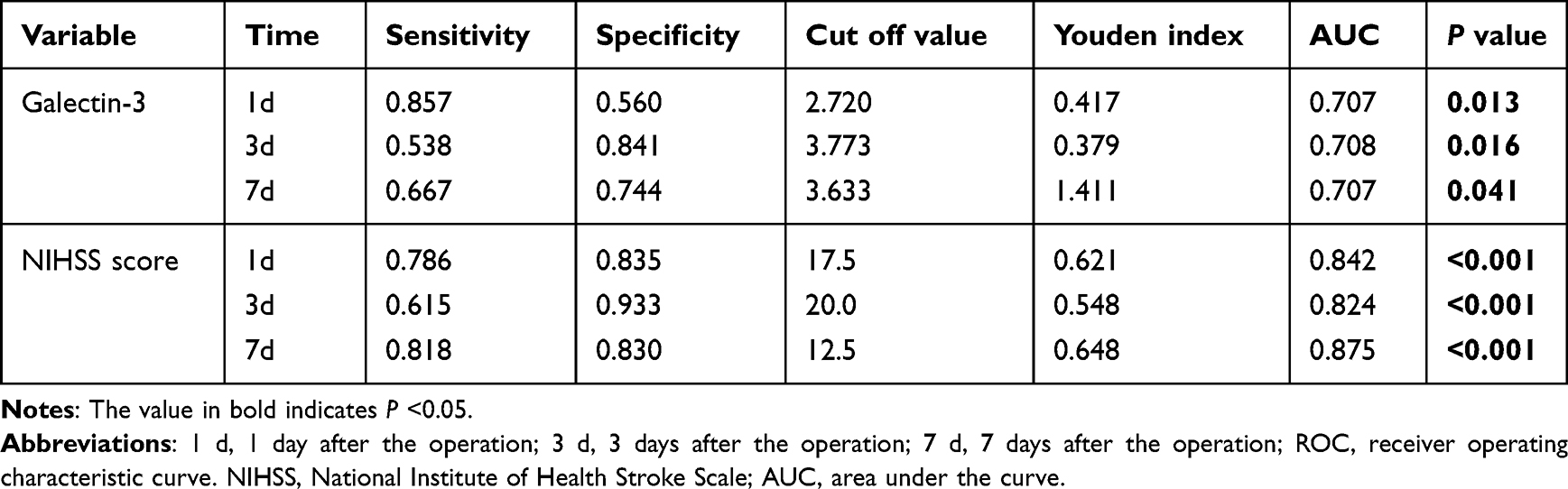 |
Table 3 ROC Curve Analysis of the Ability of Galectin-3 Levels and NIHSS Score to Predict Death |
Plasma Galectin-3 Concentration and 90-Day Prognosis
In this study, there were 51 patients in the poor prognosis group and 54 in the favorable prognosis group. The plasma Galectin-3 levels in the poor prognosis group continued to decrease until 3 days after the operation and then increased slightly to 7 days after the operation, which was similar to that in the poor prognosis group (Figure 2C). The linear mixed-effect model identified the significant effects of group (P =0.001) and time (P < 0.001) on Galectin-3 levels but did not reveal an interaction between the two (p =0.668), as shown in Table 2. An increase in Galectin-3 levels before the operation (P =0.010) and at 1 day (P =0.020) and 3 days after the operation (P =0.008) was associated with poor prognosis.
Plasma Galectin-3 Concentration and END
In this study, there were 28 patients in the END group and 77 in the Non-END group. The plasma Galectin-3 concentration in the END group first increased until the first day after the operation, then decreased until 3 days after the operation, and finally increased slightly until 7 days after the operation, which differed from that in the Non-END group (Figure 2D). The linear mixed-effects model revealed significant effects of group (P =0.040), time (P =0.003) and the interaction of group (P =0.035) on Galectin-3 levels (Table 2). An increase in Glalectin-3 levels at 1 day (P =0.010) and 3 days after the operation (P =0.042) was correlated with END.
Discussion
This study investigated the effects of dynamic changes in plasma Galectin-3 levels on the clinical outcome and END of patients with AIS receiving EVT. The results showed that increases in the plasma Galectin-3 levels in patients with AIS receiving EVT was associated with death, poor prognosis, and early neurological deterioration. There was a significant correlation between Galectin-3 levels and NIHSS scores. The Galectin-3 levels had a certain predictive value for death, but the predictive value was lower than that of the NIHSS score. While limiting the expansion of ischemic brain tissue and reducing infarct size, early reperfusion therapy is also associated with the possibility of “reperfusion injury”,29 such as hemorrhage transformation, brain edema, infarction progression and neurological function deterioration.30 Currently, clinicians’ assessments of patients with AIS are limited by the use of neurological function scales and imaging examinations. In recent years, exploring potential biomarkers of disease has become a research hotspot. However, many biomarkers are often time dependent. Even if biomarkers related to AIS, such as Galectin-3, MMP-9,31 NSE,32 GFAP,33 IncRNA H19,34 and FSAP,35 are identified, larger and more diverse samples are needed for repeated measurements at multiple time points to assess their clinical value.
Previous studies have shown that patients with AIS with a degree of neurological impairment36 and older age37 are at greater risk of poor prognosis, and our findings suggest that these two factors are associated with death in patients with AIS. Although there is no clear conclusion as to whether pre-EVT thrombolytic therapy increases the risk of death in patients with AIS,38–40 our results suggest that a higher risk of death in patients was correlated with receiving thrombolytic therapy, which may be associated with an increased risk of hemorrhagic transformation.41 Zhuang et al20 reported that the Galectin-3 levels were even better than the NIHSS score for predicting ischemic stroke severity. However, our study revealed a significant association between Galectin-3 levels and the NIHSS score, and the predictive value of Galectin-3 for death was lower than that of the NIHSS score. It’s worth noting that the patients with AIS we included all received successful reperfusion therapy. Given that this study did not include a conservative drug therapy group as a control group, further analysis of the impact of reperfusion therapy on the outcome was not possible. Early neurologic deterioration (END) is a common complication in patients with AIS who have undergone reperfusion therapy and is closely associated with adverse clinical outcomes. The potential underlying mechanisms may include symptomatic intracranial hemorrhage (sICH),42 postoperative reocclusion, enlarged infarcts, thromboembolic events, and unknown causation.43 Microglia are the cells that are first activated after stroke and play an important role in the inflammatory microenvironment of stroke; these cells can promote inflammatory effects, neurogenesis and neuronal apoptosis and thus affect the prognosis of stroke.44 In recent years, Galectin-3 has attracted widespread attention as a necessary medium for the proliferation and activation of microglia after cerebral ischemia.
Although inflammation is necessary for neurogenesis during stroke, it can aggravate blood–brain barrier (BBB) injuries in the acute phase, leading to malignant complications such as bleeding transformation and severe cerebral edema29 and the aggravation of brain tissue injuries, ultimately leading to deterioration and adverse clinical outcomes.45 In this study, the changes in the plasma Galectin-3 levels in the END group and the nonsurviving group were almost simultaneous. The Galectin-3 levels first increased until 1 day after the operation, then gradually decreased until 3 days after the operation, and finally increased until 7 days after the operation. However, in a model of cerebral ischemia‒reperfusion injury, Galectin-3 is consistently highly expressed in mice up to 72 h after the injury.5,14 Burguillos et al9 reported that Galectin-3-dependent TLR4 activation may contribute to sustained microglial activation and cause harmful proinflammatory effects. The survival rate of hippocampal neurons in Galectin-3 KO mice increased 24 h after the initial injury compared with that in wild-type mice, which was associated with a decreased inflammatory response. Clinical studies have also shown that high baseline Galectin-3 levels are associated with disease severity, poor prognosis, and death events in patients with AIS,17,20 which is similar to our findings. Galectin-3 levels are low in patients with good neurological recovery and favorable clinical outcomes. We speculate that deterioration of ischemic brain tissue may further activate microglia through high expression of Galectin-3 at an early stage, thereby amplifying adverse proinflammatory effects, neuronal death and the reperfusion injury. To some extent, this may lead to destruction of the BBB, increased permeability, cytotoxic edema, etc., resulting in the risk of adverse events such as malignant cerebral edema,46 bleeding transformation, and early neurological deterioration. Notably, the lack of Galectin-3 in the subchronic phase can affect the level of inflammatory mediators and weaken the activation of microglia, thus aggravating brain injection.15 In this study, the Galectin-3 levels began to rise gradually starting from 3 days until 7 days after the operation. Moreover, Galectin-3 may mediate microglial polarization from the toxic M1 proinflammatory phenotype in the acute phase to the M2 anti-inflammatory phenotype, with healing activity in the subchronic phase.16,47 Maintaining a certain concentration of Galectin-3 from the 3rd to the 7th day after the operation may be conducive to the recovery of neurological function after the operation.
Interestingly, Galectin-3 also promotes angiogenesis and neurogenesis.10,13 Moderate angiogenesis can promote brain tissue remodeling and neural function recovery. Increased angiogenesis is associated with increased survival and BBB stability in stroke patients. However, its benefits are also time dependent. Premature promotion of angiogenesis after stroke (such as via VEGF administration) can lead to increased vascular permeability and an increased risk of hemorrhagic transformation.47 We hypothesized that high Galectin-3 expression in patients with AIS in the acute phase may lead to overactivation and proliferation of microglia and promote the expression of the proinflammatory M1 phenotype. Vascular permeability may also increase during the early excessive angiogenesis process, which is more likely to cause postoperative adverse events such as bleeding transformation and malignant cerebral edema and lead to poor clinical outcomes. However, as an observational study, we did not conduct synchronous monitoring of inflammatory factors or proangiogenic factors. The pathophysiological mechanism of the effect of reperfusion therapy on Galectin-3 levels at different time points could not be further elucidated.
Hansen et al’s48 study showed that Galectin-3 levels at admission were independent predictors of 90-day adverse outcomes, while Galectin-3 levels at 48 h only predicted mortality. Our study revealed that for patients with AIS receiving EVT, higher plasma Galectin-3 levels before and after surgery were associated with poor prognosis. A higher plasma Galectin-3 concentration at multiple points after the operation was associated with death events and had certain predictive value. In this study, dynamic monitoring of plasma Galectin-3 levels was used to identify detection time points with increased sensitivity and specificity. An increase in Galectin-3 levels at 1 day after surgery had a significant warning effect on the risk of END and death and was significantly greater than the effect on preoperative (baseline) Galectin-3 levels. To some extent, these findings improve the clinical value of Galectin-3 in patients with AIS, but larger randomized trials are still needed to confirm these findings.
Finally, we believe that stroke therapy should not be limited to a single anti-inflammatory direction. However, promoting microglia from the classic neurotoxic proinflammatory M1 phenotype to the anti-inflammatory M2 phenotype with neuroprotective effects is still worth exploring, and Galectin-3 may be a worthy target. Modified citrus pectin (MCP), a Galectin-3 inhibitor, activates the NLRP3 inflammasome by inhibiting the TLR4/NF-κB signaling pathway in microglia and plays a neuroprotective role in cerebral ischemia/reperfusion injury.49 However, studies on the use of Galectin-3 inhibitors in patients with AIS are rare. Our study involved dynamic monitoring of Galectin-3 levels in patients with AIS at multiple time points, and this monitoring was combined with an analysis of the patient’s disease changes and clinical outcomes. This study provides a reference for future researchers to explore whether reducing Galectin-3 levels can reduce neurological impairment and ameliorate the adverse clinical outcomes of AIS.
Limitations
First, the sample size of this study was small. Although we adopted the linear mixed effects model to minimize the resulting error, there was still a certain selection bias. Second, all the patients included in this study were successfully treated with reperfusion, and the correlation between plasma Galectin-3 levels and vascular revascularization levels is unclear. Third, this was an observational study. Patients treated with conservative drugs were not included in the control group, and additional simultaneous monitoring of inflammatory factors and proangiogenic factors was not conducted. Ultimately, the pathophysiological mechanism by which reperfusion therapy affects changes in Galectin-3 levels at different time points was not elucidated.
Conclusions
In acute ischemic stroke patients receiving endovascular therapy, an increase in the plasma Galectin-3 levels were associated with death, poor prognosis, and early neurological deterioration. Galectin-3 levels were significantly correlated with the NIHSS score and had a certain predictive value for death. In the future, the sample size could be increased to conduct clinical studies on the simultaneous monitoring of Galectin-3, other inflammatory factors and angiogenic factors, so as to provide more ideas on whether Galectin-3 inhibitors could be an important potential therapeutic target.
Abbreviations
NIHSS score, National Institutes of Health Stroke Scale; TOAST subtypes, Trial of Org10172in Acute Stroke Treatment; LAA, large-artery atherosclerosis; CE, cardioembolism; SUE, stroke of undetermined etiology; WBC, white blood cell; FBG, fasting blood glucose; LDL-c, low-density lipoprotein cholesterol; END, early neurological deterioration; Non-END, Nonearly neurological deterioration; 1 d, 1 day after the operation; 3 d, 3 days after the operation; 7 d, 7 days after the operation; ROC, receiver operating characteristic curve; AUC, area under the curve; AIS, acute ischemic stroke; EVT, endovascular therapy; BBB, blood–brain barrier; MCP, modified citrus pectin.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study that involved human participants was reviewed and approved by the Medical Ethics Committee of the First Affiliated Hospital of Jinan University. The patients/participants provided their written informed consent to participate in this study.
Acknowledgments
We thank all the patients who enrolled in this trial.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by grants from National Nature Science Foundation of China (Grant Number 81971120), Guangdong Natural Science Foundation project - surface project (Grant Number 2022A1515012563), Basic and Applied Basic Research Project jointly funded by Guangzhou Science and Technology Plan Municipal Schools (institutes) (Grant Number 202201020062), National Natural Science Foundation Committee, Youth Science Fund project (Grant Number 82201438).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tu WJ, Wang LD. China stroke surveillance report 2021. Mil Med Res. 2023;10(1):33. doi:10.1186/s40779-023-00463-x
2. Dirnagl U, Iadecola C, Moskowitz MA. Pathobiology of ischaemic stroke: an integrated view. Trends Neurosci. 1999;22(9):391–397. doi:10.1016/S0166-2236(99)01401-0
3. Qiu YM, Zhang CL, Chen AQ, et al. Immune cells in the BBB disruption after acute ischemic stroke: targets for immune therapy? Front Immunol. 2021;12:678744. doi:10.3389/fimmu.2021.678744
4. Liu FT, Rabinovich GA. Galectins as modulators of tumour progression. Nat Rev Cancer. 2005;5(1):29–41. doi:10.1038/nrc1527
5. Lalancette-Hébert M, Swarup V, Beaulieu JM, et al. Galectin-3 is required for resident microglia activation and proliferation in response to ischemic injury. J Neurosci. 2012;32(30):10383–10395. doi:10.1523/JNEUROSCI.1498-12.2012
6. Rabinovich GA, Toscano MA. Turning ‘sweet’ on immunity: galectin-glycan interactions in immune tolerance and inflammation. Nat Rev Immunol. 2009;9(5):338–352. doi:10.1038/nri2536
7. Shin T. The pleiotropic effects of galectin-3 in neuroinflammation: a review. Acta Histochem. 2013;115(5):407–411. doi:10.1016/j.acthis.2012.11.010
8. Srejovic I, Selakovic D, Jovicic N, Jakovljević V, Lukic ML, Rosic G. Galectin-3: roles in neurodevelopment, neuroinflammation, and behavior. Biomolecules. 2020;10(5):798. doi:10.3390/biom10050798
9. Burguillos MA, Svensson M, Schulte T, et al. Microglia-secreted galectin-3 acts as a toll-like receptor 4 ligand and contributes to microglial activation. Cell Rep. 2015;10(9):1626–1638. doi:10.1016/j.celrep.2015.02.012
10. Wesley UV, Sutton IC, Cunningham K, et al. Galectin-3 protects against ischemic stroke by promoting neuro-angiogenesis via apoptosis inhibition and Akt/Caspase regulation. J Cereb Blood Flow Metab. 2021;41(4):857–873. doi:10.1177/0271678X20931137
11. Markowska AI, Liu FT, Panjwani N. Galectin-3 is an important mediator of VEGF- and bFGF-mediated angiogenic response. J Exp Med. 2010;207(9):1981–1993. doi:10.1084/jem.20090121
12. Nangia-Makker P, Honjo Y, Sarvis R, et al. Galectin-3 induces endothelial cell morphogenesis and angiogenesis. Am J Pathol. 2000;156(3):899–909. doi:10.1016/S0002-9440(10)64959-0
13. Yan YP, Lang BT, Vemuganti R, Dempsey RJ. Galectin-3 mediates post-ischemic tissue remodeling. Brain Res. 2009;1288:116–124. doi:10.1016/j.brainres.2009.06.073
14. Lalancette-Hébert M, Gowing G, Simard A, Weng YC, Kriz J. Selective ablation of proliferating microglial cells exacerbates ischemic injury in the brain. J Neurosci. 2007;27(10):2596–2605. doi:10.1523/JNEUROSCI.5360-06.2007
15. Rahimian R, Lively S, Abdelhamid E, et al. Delayed galectin-3-mediated reprogramming of microglia after stroke is protective. Mol Neurobiol. 2019;56(9):6371–6385. doi:10.1007/s12035-019-1527-0
16. Doverhag C, Hedtjärn M, Poirier F, et al. Galectin-3 contributes to neonatal hypoxic-ischemic brain injury. Neurobiol Dis. 2010;38(1):36–46. doi:10.1016/j.nbd.2009.12.024
17. Wang A, Zhong C, Zhu Z, et al. Serum galectin-3 and poor outcomes among patients with acute ischemic stroke. Stroke. 2018;49(1):211–214. doi:10.1161/STROKEAHA.117.019084
18. Dong H, Wang ZH, Zhang N, Liu SD, Zhao JJ, Liu SY. Serum galectin-3 level, not galectin-1, is associated with the clinical feature and outcome in patients with acute ischemic stroke. Oncotarget. 2017;8(65):109752–109761. doi:10.18632/oncotarget.18211
19. Han X, Geng B, Deng F, et al. Galectin-3 is associated with the functional outcome and mortality in stroke patients: a systematic review and meta-analysis. Heliyon. 2023;9:2.
20. Zhuang JJ, Zhou L, Zheng YH, Ding YS. The serum galectin-3 levels are associated with the severity and prognosis of ischemic stroke. Aging. 2021;13(5):7454–7464. doi:10.18632/aging.202610
21. Rahimian R, Béland LC, Kriz J. Galectin-3: mediator of microglia responses in injured brain. Drug Discov Today. 2018;23(2):375–381. doi:10.1016/j.drudis.2017.11.004
22. Liang D, Zeng X, Yao M, et al. Dynamic changes in the glycocalyx and clinical outcomes in patients undergoing endovascular treatments for large vessel occlusion. Front Neurol. 2023;14:1046915. doi:10.3389/fneur.2023.1046915
23. Guo ZN, Guo WT, Liu J, et al. Changes in cerebral autoregulation and blood biomarkers after remote ischemic preconditioning. Neurology. 2019;93(1):e8–e19. doi:10.1212/WNL.0000000000007732
24. Chen PH, Gao S, Wang YJ, Xu AD, Li YS, Wang D. Classifying ischemic stroke, from TOAST to CISS. CNS Neurosci Ther. 2012;18(6):452–456. doi:10.1111/j.1755-5949.2011.00292.x
25. Zaidat OO, Yoo AJ, Khatri P, et al. Recommendations on angiographic revascularization grading standards for acute ischemic stroke: a consensus statement. Stroke. 2013;44(9):2650–2663. doi:10.1161/STROKEAHA.113.001972
26. Jeong HG, Kim BJ, Yang MH, Han MK, Bae HJ. Neuroimaging markers for early neurologic deterioration in single small subcortical infarction. Stroke. 2015;46(3):687–691. doi:10.1161/STROKEAHA.114.007466
27. Zhong W, Yan S, Chen Z, et al. Stroke outcome of early antiplatelet in post-thrombolysis haemorrhagic infarction. J Neurol Neurosurg Psychiatry. 2022;2022:328778.
28. Hao Y, Yang D, Wang H, et al. Predictors for symptomatic intracranial hemorrhage after endovascular treatment of acute ischemic stroke. Stroke. 2017;48(5):1203–1209. doi:10.1161/STROKEAHA.116.016368
29. Molina CA, Alvarez-Sabín J. Recanalization and reperfusion therapies for acute ischemic stroke. Cerebrovasc Dis. 2009;27(1):162–167. doi:10.1159/000200455
30. Xu X, Chen M, Zhu D. Reperfusion and cytoprotective agents are a mutually beneficial pair in ischaemic stroke therapy: an overview of pathophysiology, pharmacological targets and candidate drugs focusing on excitotoxicity and free radical. Stroke Vasc Neurol. 2023;svn–2023–002671. doi:10.1136/svn-2023-002671
31. Ge H, Ma X, Wang J, et al. A potential relationship between MMP-9 rs2250889 and ischemic stroke susceptibility. Front Neurol. 2023;14:1178642. doi:10.3389/fneur.2023.1178642
32. Anand N, Stead LG. Neuron-specific enolase as a marker for acute ischemic stroke: a systematic review. Cerebrovasc Dis. 2005;20(4):213–219. doi:10.1159/000087701
33. Ferrari F, Rossi D, Ricciardi A, et al. Quantification and prospective evaluation of serum NfL and GFAP as blood-derived biomarkers of outcome in acute ischemic stroke patients. J Cereb Blood Flow Metab. 2023;43(9):1601–1611. doi:10.1177/0271678X231172520
34. Rezaei M, Mokhtari MJ, Bayat M, et al. Long non-coding RNA H19 expression and functional polymorphism rs217727 are linked to increased ischemic stroke risk. BMC Neurol. 2021;21(1):54. doi:10.1186/s12883-021-02081-3
35. Tian DS, Qin C, Zhou LQ, et al. FSAP aggravated endothelial dysfunction and neurological deficits in acute ischemic stroke due to large vessel occlusion. Signal Transduct Target Ther. 2022;7(1):6. doi:10.1038/s41392-021-00802-1
36. Bres-Bullrich M, Fridman S, Sposato LA. Relative effect of stroke severity and age on outcomes of mechanical thrombectomy in acute ischemic stroke. Stroke. 2021;52(9):2846–2848. doi:10.1161/STROKEAHA.121.034946
37. Fan J, Li X, Yu X, et al. Global burden, risk factor analysis, and prediction study of ischemic stroke, 1990–2030. Neurology. 2023;101(2):e137–e150. doi:10.1212/WNL.0000000000207387
38. LeCouffe NE, Kappelhof M, Treurniet KM, et al. A randomized trial of intravenous alteplase before endovascular treatment for stroke. N Engl J Med. 2021;385(20):1833–1844. doi:10.1056/NEJMoa2107727
39. Fischer U, Kaesmacher J, S Plattner P, et al. Swift direct: solitaire™ with the intention for thrombectomy plus intravenous t-PA versus direct solitaire™ stent-retriever thrombectomy in acute anterior circulation stroke: methodology of a randomized, controlled, multicentre study. Int J Stroke. 2022;17(6):698–705. doi:10.1177/17474930211048768
40. Mitchell PJ, Yan B, Churilov L, et al. Endovascular thrombectomy versus standard bridging thrombolytic with endovascular thrombectomy within 4·5 h of stroke onset: an open-label, blinded-endpoint, randomised non-inferiority trial. Lancet. 2022;400(10346):116–125. doi:10.1016/S0140-6736(22)00564-5
41. Balami JS, Chen RL, Grunwald IQ, Buchan AM. Neurological complications of acute ischaemic stroke. Lancet Neurol. 2011;10(4):357–371. doi:10.1016/S1474-4422(10)70313-6
42. Bracard S, Ducrocq X, Mas JL, et al. Mechanical thrombectomy after intravenous alteplase versus alteplase alone after stroke (THRACE): a randomised controlled trial. Lancet Neurol. 2016;15(11):1138–1147. doi:10.1016/S1474-4422(16)30177-6
43. Li W, Yuan S, Sui X, et al. Higher serum occludin after successful reperfusion Is associated with early neurological deterioration. CNS Neurosci Ther. 2022;28(7):999–1007. doi:10.1111/cns.13830
44. Ma Y, Wang J, Wang Y, Yang GY. The biphasic function of microglia in ischemic stroke. Prog Neurobiol. 2017;157:247–272. doi:10.1016/j.pneurobio.2016.01.005
45. Álvarez-Sabín J, Maisterra O, Santamarina E, Kase CS. Factors influencing haemorrhagic transformation in ischaemic stroke. Lancet Neurol. 2013;12(7):689–705. doi:10.1016/S1474-4422(13)70055-3
46. Ferro D, Matias M, Neto J, et al. Neutrophil-to-lymphocyte ratio predicts cerebral edema and clinical worsening early after reperfusion therapy in stroke. Stroke. 2021;52(3):859–867. doi:10.1161/STROKEAHA.120.032130
47. Bernardo-Castro S, Sousa JA, Brás A, et al. Pathophysiology of blood-brain barrier permeability throughout the different stages of ischemic stroke and its implication on hemorrhagic transformation and recovery. Front Neurol. 2020;11:594672. doi:10.3389/fneur.2020.594672
48. Hansen C, Sastre C, Wolcott Z, Bevers MB, Kimberly WT. Time-dependent, dynamic prediction of fatty acid-binding protein 4, galectin-3, and soluble ST2 measurement with poor outcome after acute stroke. Int J Stroke. 2021;16(6):660–668. doi:10.1177/1747493020971166
49. Cui Y, Zhang NN, Wang D, Meng WH, Chen HS. Modified citrus pectin alleviates cerebral ischemia/reperfusion injury by inhibiting NLRP3 inflammasome activation via TLR4/NF-ĸB signaling pathway in microglia. J Inflamm Res. 2022;15:3369–3385. doi:10.2147/JIR.S366927
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.