")
Back to Journals » Journal of Asthma and Allergy » Volume 16
Dupilumab Treatment Efficacy and Impact on Clinical Scores, Serum Biomarkers, and Itch in Adult Patients with Atopic Dermatitis: A Retrospective Analysis
Authors Rossi M, Bettolini L , Artelli GL, Fraghì A, Tomasi C, Calzavara-Pinton P
Received 1 September 2023
Accepted for publication 25 October 2023
Published 9 November 2023 Volume 2023:16 Pages 1233—1240
DOI https://doi.org/10.2147/JAA.S433515
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Luis Garcia-Marcos
Mariateresa Rossi,* Luca Bettolini,* Grazia Linda Artelli, Alessandro Fraghì, Cesare Tomasi, Piergiacomo Calzavara-Pinton
Dermatology Department, University of Brescia, ASST Spedali Civili di Brescia, Brescia, Italy
*These authors contributed equally to this work
Correspondence: Luca Bettolini, Department of Dermatology, Spedali Civili, University of Brescia, Brescia, Italy, Tel +39 030 3995301, Fax +39 030 399505, Email [email protected]
Purpose: Dupilumab, a fully human monoclonal antibody that inhibits the signaling pathways of interleukin (IL)-4 and IL-13, has demonstrated remarkable efficacy in the treatment of atopic dermatitis (AD). Dupilumab has been reported to attenuate itch and reduce several serum markers, including blood lactate dehydrogenase (LDH), blood eosinophil count, and serum total immunoglobulin E (IgE).
Patients and Methods: The present study investigated retrospectively changes in clinical scores and serum biomarker from 175 adults with moderate-to-severe AD treated with dupilumab. Clinical manifestations were assessed using eczema area and severity index (EASI) and visual analogue scale (VAS) for itch at baseline and subsequently at 16-week intervals up to a duration of 48 weeks. Total IgE, LDH and blood eosinophil count were also collected.
Results: The dupilumab treatment significantly improved EASI and VAS scores and decreased serum levels of IgE, LDH, and total eosinophil count. The EASI scores were positively correlated with VAS for itch at all recorded time points, whereas serum biomarkers did not exhibit a strong correlation with EASI scores.
Conclusion: These findings highlight the close relationship between the extent and severity of eczema and the intensity of itch experienced by patients and suggest that factors beyond the measured serum biomarkers play a significant role in the clinical manifestations of AD, emphasizing the complex nature of the disease.
Keywords: atopic dermatitis, dupilumab, itch, immunoglobulin E, eosinophils, lactate dehydrogenase
Introduction
Atopic dermatitis (AD) is a common inflammatory skin condition with varying prevalence across different age groups. In Europe and the US, it is estimated to affect between 1% and 3% of adults.1 AD is characterized by persistent itching and recurring eczematous lesions of varying severity.2
Numerous disease severity scales have been developed, such as the Scoring of Atopic Dermatitis (SCORAD) index, the Eczema Area and Severity Index (EASI), and the Patient-Oriented Eczema Measure (POEM). These scales, along with patient quality-of-life measurement tools and the visual analog scales (VAS) of itch and quality of sleeping, have been validated for use in clinical trials and practice.3 However, the correlation between AD severity scores and certain biomarkers, such as serum levels of lactate dehydrogenase (LDH), thymus and activation-regulated chemokine/ Chemokine (C-C motif) ligand (CCL)17 [(TARC)/CCL17], interleukin (IL)-16, eosinophil cationic protein (ECP), and the number of circulating eosinophils,4 is still being debated.5,6
Elevated serum total immunoglobulin E (IgE) levels are observed in approximately 60–80% of AD patients,7,8 and there is a significant correlation between higher levels of IgE and acute exacerbations in these patients.5–7 However, some individuals with severe AD may have normal IgE levels.9 Moreover, elevated IgE levels are also seen in several non-atopic conditions, such as parasitic infections, primary immunodeficiencies, and hyper-IgE syndromes.10
Numerous topical and systemic treatment options are available for AD, and the choice is driven by several factors eg the disease severity, the patient’s age, atopy-related and unrelated comorbidities, the response to previous treatments, and the patient’s ability to comply with the treatment regimen.11–13
Dupilumab is a fully human monoclonal antibody that has been approved for treating patients with moderate-to-severe atopic dermatitis. It blocks the α subunit of the IL-4 receptor, which prevents the signaling cascade of IL-4 and IL-13. This blockade ultimately leads to a reduction in the Th2 immune response. Several randomized comparative trials in both adults and children have demonstrated the efficacy of dupilumab in treating moderate-to-severe AD.13,14
Dupilumab has been shown to reduce total IgE, LDH, and TARC/CCL17 levels. However, it remains to be elucidated whether the changes in these laboratory parameters are predictive markers for the clinical response.
The present study aims to investigate the correlation between the clinical response to dupilumab, as measured by the EASI score, with the VAS of itch, and changes in selected laboratory parameters, including serum levels of total IgE and LDH, as well as blood count of eosinophils.
Materials and Methods
Data on adults ≥18 years diagnosed with AD and treated with dupilumab between February 2019 and May 2021 were collected retrospectively. The study included patients treated at the dermatology department’s outpatient clinic at the University Hospital of Brescia, a tertiary referral center for AD in Northern Italy. Patients treated for 48 weeks and followed up at 16-week intervals were consecutively included in the study. Patients with a diagnosis of AD made by an expert dermatologist who were candidates for systemic therapy (documented history of cyclosporine A (CyA), and either inadequate response to CyA, or intolerance and/or unacceptable toxicity to CyA, or CyA-naïve and not eligible for CyA due to medical contraindications) and who had moderate-to-severe disease (EASI score ≥24), were included in the study. According to the guidelines set forth by the Italian Medical Agency, these treatment criteria are used to determine the appropriateness of prescribing dupilumab to eligible patients.15
The study collected demographic and clinical data, including age, gender, family history of AD, clinical phenotype of AD, atopic comorbidities and previous treatments. In accordance with the Good Clinical Practice guidelines, the severity of the disease was assessed using the EASI score at baseline and during every follow-up visit, as well as the VAS for pruritus, as the average level of itch experienced by patients in the previous 24 hours on a scale ranging from 0 to 10. In addition, blood tests, including a complete blood count with differential, LDH level, and total IgE level, were repeated. All the data were retrieved retrospectively from the patients’ medical charts.
Patients with incomplete clinical or laboratory data were excluded from the study (n=27).
Follow-up visits took place after 16 (T1), 32 (T2), and 48 (T3) weeks of treatment.
All patients received a loading dose of 600 mg of dupilumab, followed by subcutaneous injections of 300 mg of dupilumab every two weeks. Patients were advised to apply emollient creams regularly and generously to their entire body skin. Oral antihistamines were allowed at night if patients experienced severe pruritus and sleep disturbance that were not tolerable. Topical corticosteroids (Cs) and calcineurin inhibitors were used only for the treatment of acute flares in limited body areas for short periods of time during the treatment cycle.
The encoded and anonymous database was formatted using Microsoft-Excel® software and subsequently imported from IBM-SPSS TM ver. 27.1. The normality of the distributions was assessed using the Kolmogorov–Smirnov test. Continuous variables were presented as means ±SD (in case of a normal distribution), or medians and min/max (in case of a skewed distribution); correlations among variables by the Spearman’s rank correlation test. The Wilcoxon rank-sum test was used to evaluate significant differences at various time points for trend analysis. A two-sided α level of 0.05 was used for all tests.
The study received approval from the Brescia ethics committee (DAREG-BS01 protocol number 4707), and all participants provided written informed consent. It was carried out in strict adherence to the principles outlined in the Declaration of Helsinki, ensuring the participants’ data confidentiality and their absolute right to withdraw from the study at any point.
Results
One hundred and seventy-five patients (98 males, 77 females) were included in the study.
Patients’ baseline characteristics are reported in detail in Table 1. In particular, the mean value of age was 44.7 years. The vast majority of patients (n=159) showed a prevalent clinical phenotype of “classic” atopic dermatitis characterized by generalized eczema. The remaining patients had clinical manifestations of prurigo-like AD.13 Out of 175 patients, 80 (47.5%) reported atopic comorbidities, including asthma, rhinitis, conjunctivitis and/or food allergy. 42.9% of the patients had a family history of AD. At baseline, the median EASI score was 26.0 (range: 24–49.0), and the median VAS of itch intensity was 8 (range: 0–10). Regarding laboratory values at baseline, the median of LDH level, IgE level, and blood eosinophil count were 201 mU/mL (range: 121–497), 744 kU/L (range: 1.4–22,085) and 0.35 x 103/μL (range: 0–2.3), respectively.
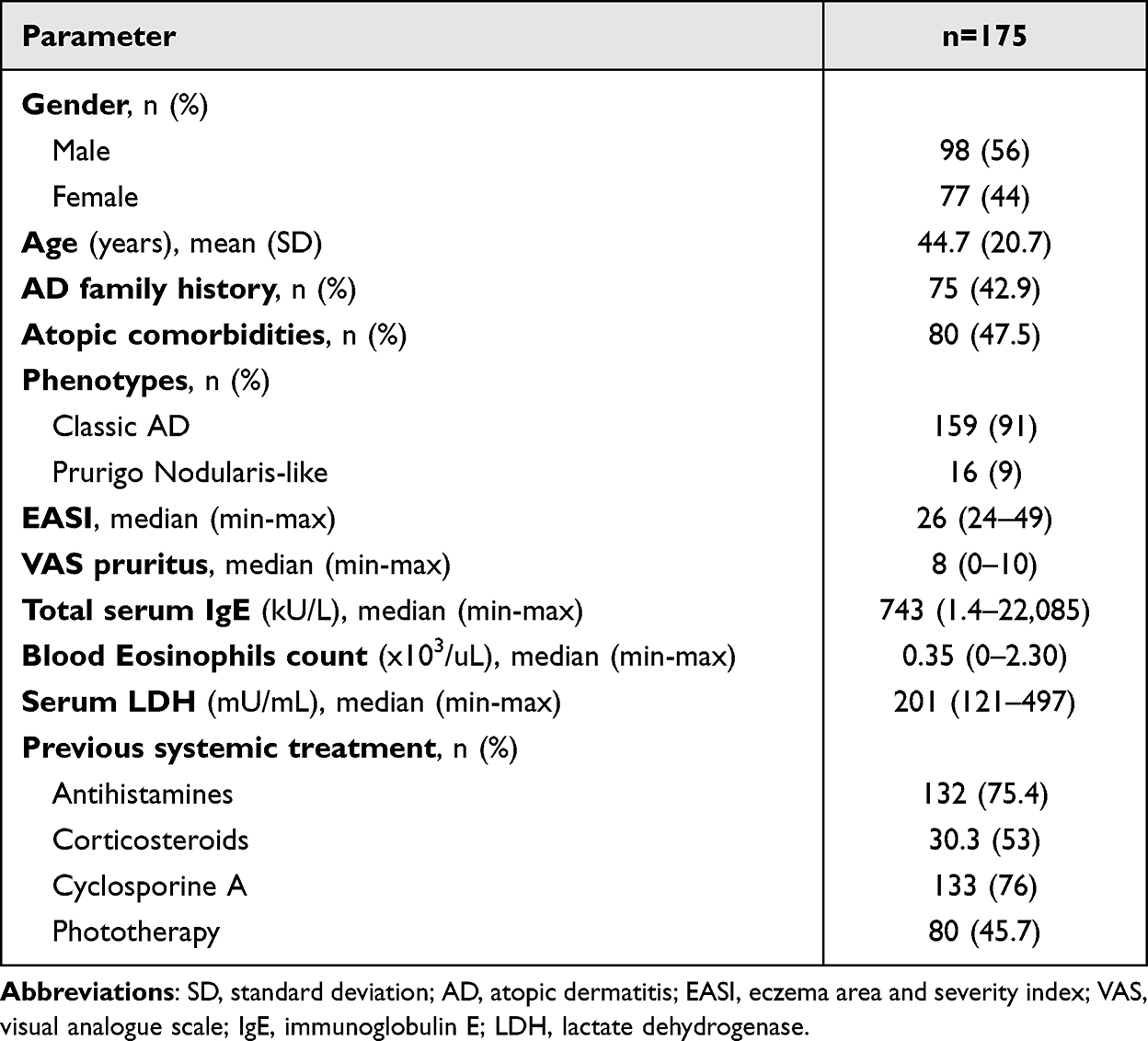 |
Table 1 Baseline Demographics and Disease Characteristics |
Regarding previous systemic treatments, 132 (75.4%) were treated with oral antihistamines, prescribed mainly by general practitioners, 53 (30.3%) with oral Cs, 133 (76%) with CyA, and 80 (45.7%) with phototherapy.
The study retrieved information about the usage of topical therapy by examining the patients’ medical charts. Of the participants, 45 (25.7%) reported intermittent use of topical steroids or calcineurin inhibitors (tacrolimus) during the follow-up period.
Variation of Clinical and Laboratory Parameters
Results are shown in Table 2. The median (range) EASI values and median (range) VAS for itch intensity values exhibited a statistically significant reduction at all time points compared to T0. In terms of laboratory parameters, total IgE exhibited a significant decrease after 16 weeks of therapy (T1), with further subsequent reduction during the entire observational period (statistically significant differences at all timepoints compared to baseline). Only a slight decrease in median values of eosinophils at T1 and T2 compared to T0, with a significant reduction seen after 48 weeks of therapy, was observed.
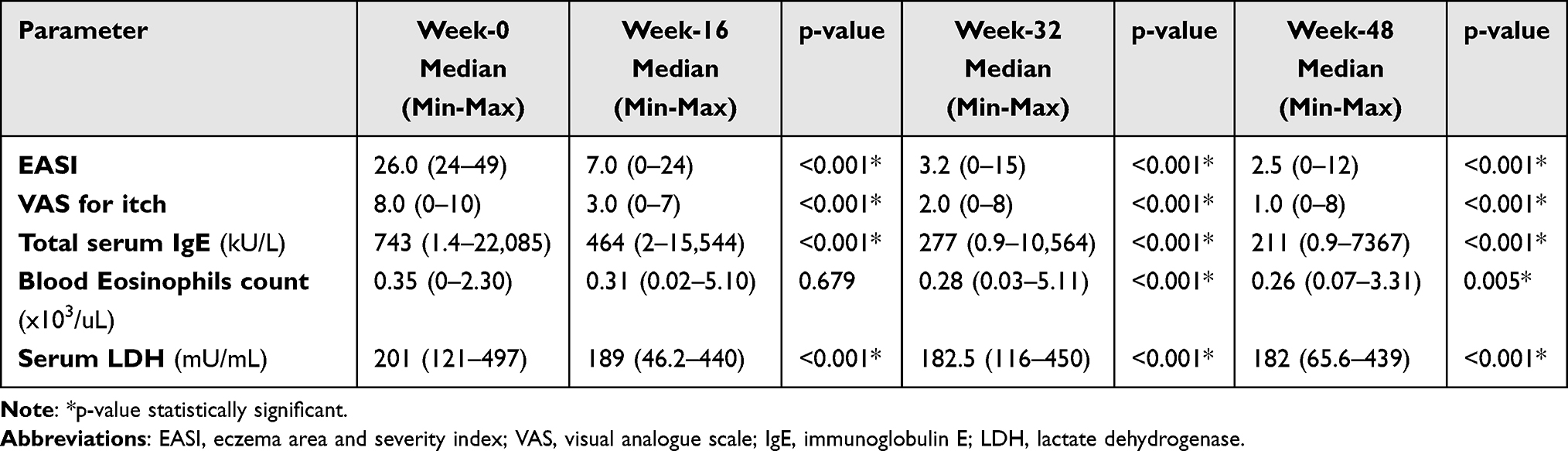 |
Table 2 Statistical Analysis in the Variation of the Outcome Measures Compared to Baseline |
LDH levels showed high variability at baseline, with a progressive reduction observed at all time points compared to T0.
Correlation Analysis Between EASI and the Other Parameters
We subsequently investigated whether patients’ laboratory parameters and pruritus might be linked to the baseline EASI and influence the enhancement of EASI scores due to dupilumab treatment at weeks 16, 32, or 48. Spearman’s rank correlation was calculated to assess the association between the EASI score and VAS for itching, serum LDH and IgE levels, and blood eosinophil count. The results are presented in Table 3.
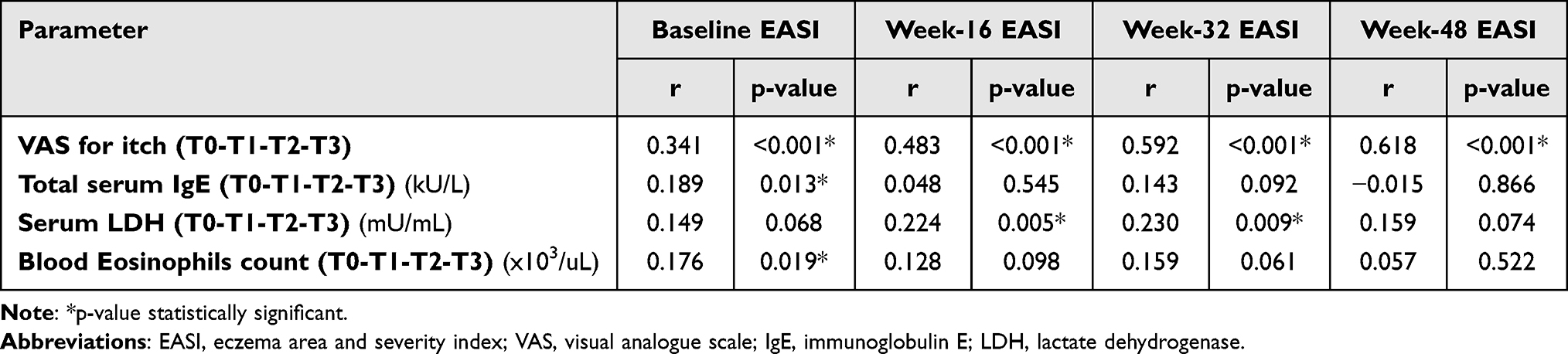 |
Table 3 Correlation Analysis Between EASI and the Other Parameters |
In terms of the EASI score and VAS for itching, there was a positive correlation in terms of reduction at each examination (pT0, pT1, pT2, and pT3 ≤0.001), indicating a moderate to strong association (rT0=0.341, rT1=0.483, rT2=0.592, and rT3=0.613). Additionally, we observed a positive correlation between EASI and LDH at weeks 16 and 32 (pT2=0.005 and pT3=0.009) but with weak correlation coefficients (rT2=0.224 and rT3=0.230).
Concerning serum total IgE levels and blood eosinophil count, we observed a very weak correlation with the EASI score at week 0 (r=0.189 and r=0.176, respectively). However, there was no correlation observed at weeks 16, 32, and 48.
Discussion
In the present study, we enrolled 175 adult patients with severe atopic dermatitis (EASI ≥24) who initiated dupilumab between February 2019 and May 2021. We conducted a data collection retrospectively over an extended observation period of 48 weeks, and we only included patients whose medical charts contained complete data.
Dupilumab demonstrated high efficacy rates, as evidenced by a significant reduction in EASI scores at all time points (16, 32, and 48 weeks) compared to baseline values. Moreover, there was a significant reduction in pruritus, as measured by VAS, after the first 16 weeks of therapy, which was sustained over time.
In terms of laboratory parameters, a significant reduction in total IgE values was observed after the first 16 weeks, with further decreases seen at 32 and 48 weeks. Blood eosinophil count showed only a slight reduction in median values at T1 (with a transient increase seen in 74 of the 175 patients), and a significant decrease was observed only after 48 weeks of therapy compared to baseline.
Correlation analysis revealed a positive association between the reduction in EASI and VAS for itching at all time points. In contrast, a weak correlation was observed between LDH and EASI only at weeks 16 and 32. Total IgE and eosinophil count did not reach a level of statistical significance.
Our study aimed to analyze the variations in clinical and laboratory parameters in a large population of adult atopic patients and explore the potential correlations between these variables at different time points. In 74 out of 175 patients, we observed a transient but non-significant increase in blood eosinophil count from week 0 to weeks 16 and 32, while a significant reduction was only observed after 48 weeks of therapy. Wechsler et al recently reported a similar transient increase in mean eosinophil counts followed by a decline starting at week 24 in patients with asthma, chronic rhinosinusitis with nasal polyposis, and AD who were treated with dupilumab compared to placebo. However, they noted that these transient increases in eosinophil counts did not impact the efficacy of dupilumab and were rarely of clinical significance.14
Another study has shown that administration of dupilumab resulted in a worsening of eosinophil counts, with the increase being associated with baseline levels as well as with other atopic comorbidities (asthma, allergic rhinitis, and food allergy).16
The relatively low number of patients (80/175) with atopic comorbidities in our study may explain the relatively low baseline values of eosinophils (median 0.35 (0–2.30)) and the non-significant increase after the first 16 weeks of therapy compared to baseline. The mechanisms behind dupilumab-induced hypereosinophilia are still unknown. It has been hypothesized that dupilumab could inhibit the migration of eosinophils into tissues by blocking IL-4 and IL-13-mediated production of eotaxins and vascular cell adhesion molecules, but not eosinophil production in the bone marrow.14
In addition, we did not find a correlation between EASI and eosinophil transitions at any time point during the study period.
Regarding serum LDH levels, we observed a significant reduction at week 16, 32, and 48 compared to baseline. LDH is an enzyme that catalyzes the conversion of pyruvate to lactate, and it is released in the bloodstream during tissue damage in all tissue cells, including the skin. Therefore, it is commonly used as a marker for malignancies, cardiac and blood diseases.17
Previous studies have demonstrated that higher serum levels of LDH are associated with more severe AD.18 Additionally, a study conducted in Japan with 54 adult patients who were treated with dupilumab revealed that higher baseline LDH levels were associated with a poorer response to therapy in the long term.4
Additionally, Kogawa et al investigated the correlation between LDH levels and other laboratory parameters such as IgE, TARC levels, and eosinophil count in patients with AD. They observed a positive association between serum LDH and the other biomarkers, but they did not directly compare LDH levels with the severity of AD.19
Our study observed a positive but weak correlation between the EASI and LDH at weeks 16 and 32.
IgE levels are another critical parameter that has been extensively investigated in patients with atopic dermatitis. It has been reported that approximately 80% of patients with AD have high levels of serum IgE.20
Our study is consistent with this data, as 78.4% of patients in our study had high IgE levels at baseline. Different studies have investigated the relationship between IgE levels and AD severity, with contrasting results. For instance, Stone et al did not find a significant association between IgE levels and the severity of atopic disease in a population of 28 patients.21
One study conducted on a large population of pediatric AD patients (n=345) investigated the correlation between the severity of eczema (defined by SCORAD score) and serum IgE levels and found a positive correlation.22 However, a commentary by Joishy et al questioned the statistical methods used to demonstrate this association.23
In a recent review, Renert-Yuval et al found that although total serum IgE levels are often elevated in AD, particularly in extrinsic AD, these levels were not consistently correlated with disease severity or were only weakly correlated. Additionally, in studies investigating the use of dupilumab in AD, patient responses were not affected by their baseline IgE levels. Therefore, the authors concluded that IgE might be a bystander in the pathogenesis of AD rather than a treatment target.24
Askin et al conducted a study on 14 patients diagnosed with moderate-to-severe atopic dermatitis who were treated with dupilumab. They found no correlation between the reduction of SCORAD and the serum total IgE values after 12 weeks of dupilumab treatment.25
Mizuno et al26 conducted a study on 60 patients with AD treated with dupilumab. They observed that the change in EASI scores was strongly associated with serum lactate dehydrogenase (LDH) levels. In contrast, the transitions in serum IgE and eosinophil count were weakly and moderately related to the EASI score, respectively.
Our study yielded similar results, as we found that clinical response (measured by EASI and VAS itch reduction) did not correlate with the reduction of total IgE and eosinophil levels. The use of biomarkers in medicine is evolving, providing a better understanding of pathogenesis, and increasing treatment efficacy and safety. This enables more precise clinical care.
A recent paper by Renert-Yuval et al reaffirms the importance of biomarkers as potential instruments in the toolbox of precision medicine in AD. The authors review the process of biomarker development and validation, as well as the opinions of AD experts on the use of biomarkers. They also discuss the different types of biomarkers, including those that may improve AD diagnosis, reflect disease severity, predict AD development or concomitant atopic diseases, or forecast therapeutic response. According to their findings, CCL17/TARC is the chemokine with the most robust evidence-based support to become a potential AD biomarker, both at baseline and following therapy.27
Recently, the Janus kinase (JAK)1 inhibitor upadacitinib and the antiJAK1/2 baricitinib, have been approved for treating moderate to severe atopic dermatitis in patient aged 12 years and 15 years and older, respectively. Additionally, several authors have investigated the presence of predictors that indicate improvement with JAK inhibitors treatment.
Hagino et al28 discovered that in 65 patients, the percentage decrease in the eosinophil-to-lymphocyte ratio (ELR) exhibited a significant correlation with reductions in both the EASI and Peak Pruritus Numerical Rating Scale (PP-NRS) scores during weeks 4, 12, and 24 of upadacitinib treatment. This finding suggests that ELR can be used as a potential predictive indicator of the effectiveness of upadacitinib. Nevertheless, in a study with 31 patients, Hagino et al29 found that only the total eosinophils count was a predictive factor for response to upadacitinib at week 4.
Regarding baricitinib, at week 4, Hagino et al30 demonstrated that there was no significant correlation between the percentage reductions in laboratory parameters (such as IgE, TARC, LDH, and total eosinophils count) and the observed declines in clinical indexes. However, by week 12, a positive correlation was observed between these laboratory parameters and the decrease in EASI.
These findings suggest that laboratory parameters may not consistently reflect the therapeutic effects of Jak inhibitors, similar to what has been discussed with dupilumab.
Although our study included a substantial number of patients, it has some limitations that need to be acknowledged. Firstly, due to the retrospective nature of the study, the conclusions may not be robust. Secondly, we were unable to test CCL17/TARC since it is not available in our laboratories. However, CCL17/TARC is considered the best biomarker for evaluating AD severity and response to therapy. Despite this, our findings show that other biomarkers, such as LDH and total IgE levels, which are usually considered “predictive” of dupilumab response, may not be as significant in assessing therapy efficacy. Furthermore, we only measured disease activity by using the EASI and VAS pruritus scales. There are different severity scales used to evaluate various aspects of AD. For instance, SCORAD assesses pruritus, sleep disturbance, and xerosis, all of which impact patients’ quality of life.31 Nevertheless, both EASI and SCORAD are validated measures for AD, and EASI is a commonly used assessment tool in clinical studies to evaluate the response to therapy.
In addition to biomarkers, we observed a notable correlation between changes in EASI scores and VAS pruritus ratings. Pruritus is a fundamental characteristic of AD, and a diagnosis of active AD cannot be established without a history of itching. The VAS is a useful tool for quantifying pruritus in various dermatological conditions.32,33
Due to its high impact on the quality of life, many patients with AD evaluate the severity of their condition based on the intensity of pruritus rather than the appearance of lesions. In a recent paper, Legat et al34 reaffirmed that AD is still diagnosed by examining clinical signs and symptoms, such as pruritus, eczematous skin lesions, and its chronic or relapsing course. Pruritus is usually the primary symptom experienced by affected patients and, regardless of AD severity, is the most burdensome symptom overall. It negatively affects patients’ quality of life who frequently complain about sleep disturbances due to itch.
Given these premises, we can affirm that pruritus, in addition to biomarkers, could be a valuable tool for evaluating the efficacy of therapy. Although it is a “subjective” parameter, it has been demonstrated to correlate well with the burden and activity of the disease.
Conclusion
The use of dupilumab as a treatment was well-tolerated and showed rapid and sustained effectiveness in reducing eczema, pruritus, and tested blood parameters. From weeks 16 to 48, there was a consistent decrease in EASI, VAS for itching, IgE, and LDH. Moreover, there was a significant decline in the blood eosinophil count, which started at week 32.
The study results demonstrate that dupilumab is capable of inducing a clinically significant improvement in most of patients in terms of EASI and itch reduction, and that these two parameters are closely related. VAS for itching is a subjective parameter that may act as an indicator for improving clinical signs by treating of AD with dupilumab. Despite the progressive decrease in the EASI score and the blood parameters over time, only LDH displayed a positive but weak correlation at weeks 16 and 32. This finding suggests that the improvement in clinical manifestations, as measured by EASI, may not be solely attributed to changes in the measured blood parameters, emphasizing the complex nature of the disease.
Acknowledgments
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Nutten S. Atopic dermatitis: global epidemiology and risk factors. Ann Nutr Metab. 2015;66(Suppl. 1):8–16. doi:10.1159/000370220
2. Eichenfield LF, Tom WL, Chamlin SL, et al. Guidelines of care for the management of atopic dermatitis: part 1: diagnosis and assessment of atopic dermatitis. J Am Acad Dermatol. 2014;70(2):338. doi:10.1016/j.jaad.2013.10.010
3. Chopra R, Silverberg JI. Assessing the severity of atopic dermatitis in clinical trials and practice. Clin Dermatol. 2018;36(5):606–615. doi:10.1016/j.clindermatol.2018.05.012
4. Kato A, Kamata M, Ito M, et al. Higher baseline serum lactate dehydrogenase level is associated with poor effectiveness of dupilumab in the long term in patients with atopic dermatitis. J Dermatol. 2020;47(9):1013–1019. doi:10.1111/1346-8138.15464
5. Wu KG, Li TH, Chen CJ, Cheng HI, Wang TY. Correlations of serum interleukin-16, total ige, eosinophil cationic protein and total eosinophil counts with disease activity in children with atopic dermatitis. Int J Immunopathol Pharmacol. 2011;24(1):15–23. doi:10.1177/039463201102400103
6. Dhar S, Malakar R, Chattopadhyay S, Dhar S, Banerjee R, Ghosh A. Correlation of the severity of atopic dermatitis with absolute eosinophil counts in peripheral blood and serum ige levels. Indian J Dermatol Venereol Leprol. 2005;71(4):246–249. doi:10.4103/0378-6323.16615
7. Avena-Woods C. Overview of atopic dermatitis. Am J Manag Care. 2017;23(8 Suppl):S115–S123.
8. Gelmetti C, Girolomoni G, Patrizi A. Critical review of guidelines and practical recommendations for the management of patients with atopic dermatitis. Dermatite Atopica 2016–2017 SIDeMaST; 2016. Available from: www.aidro.org.
9. Wollenberg A, Thomsen SF, Lacour JP, Jaumont X, Lazarewicz S. Targeting immunoglobulin E in atopic dermatitis: a review of the existing evidence. World Allergy Organ J. 2021;14(3):100519. doi:10.1016/j.waojou.2021.100519
10. Mogensen TH. Primary immunodeficiencies with elevated ige. Int Rev Immunol. 2016;35(1):39–56. doi:10.3109/08830185.2015.1027820
11. Wollenberg A, Blauvelt A, Guttman-Yassky E, et al. Tralokinumab for moderate-to-severe atopic dermatitis: results from two 52-week, randomized, double-blind, multicentre, placebo-controlled Phase III trials (ECZTRA 1 and ECZTRA 2). Br J Dermatol. 2021;184(3):437–449. doi:10.1111/bjd.19574
12. Deleuran M, Thaçi D, Beck LA, et al. Dupilumab shows long-term safety and efficacy in patients with moderate to severe atopic dermatitis enrolled in a Phase 3 open-label extension study. J Am Acad Dermatol. 2020;82(2):377–388. doi:10.1016/j.jaad.2019.07.074
13. Silvestre Salvador JF, Romero-Pérez D, Encabo-Durán B. Atopic dermatitis in adults: a diagnostic challenge. J Investig Allergol Clin Immunol. 2017;27(2):78–88. doi:10.18176/jiaci.0138
14. Wechsler ME, Klion AD, Paggiaro P, et al. Effect of dupilumab on blood eosinophil counts in patients with asthma, chronic rhinosinusitis with nasal polyps, atopic dermatitis, or eosinophilic esophagitis. J Allergy Clin Immunol Pract. 2022;10(10):2695–2709. doi:10.1016/j.jaip.2022.05.019
15. Italian Medical Agency (AIFA, Agenzia Italiana Farmaco). Dupilumab: assessment of innovativeness. WWW document; 2020. Available from: https://www.aifa.gov.it/documents/20142/1308577/97_Dupixent_14869_scheda_innovativita_GRADE.pdf.
16. de Bruin-Weller M, Thaçi D, Smith CH, et al. Dupilumab with concomitant topical corticosteroid treatment in adults with atopic dermatitis with an inadequate response or intolerance to ciclosporin A or when this treatment is medically inadvisable: a placebo-controlled, randomized phase III clinical trial (LIBERTY AD CAFÉ). Br J Dermatol. 2018;178(5):1083–1101. doi:10.1111/bjd.16156
17. Forkasiewicz A, Dorociak M, Stach K, Szelachowski P, Tabola R, Augoff K. The usefulness of lactate dehydrogenase measurements in current oncological practice. Cell Mol Biol Lett. 2020;25(1). doi:10.1186/s11658-020-00228-7
18. Thijs J, Krastev T, Weidinger S, et al. Biomarkers for atopic dermatitis: a systematic review and meta-analysis. Curr Opin Allergy Clin Immunol. 2015;15(5):453–460. doi:10.1097/ACI.0000000000000198
19. Kogawa K, Minakawa S, Matsuzaki Y, et al. Correlation between lactate dehydrogenase and other laboratory data in patients with atopic dermatitis. J Cutan Immunol Allergy. 2022;5(4):133–135. doi:10.1002/cia2.12225
20. Holm JG, Agner T, Clausen ML, Thomsen SF. Determinants of disease severity among patients with atopic dermatitis: association with components of the atopic march. Arch Dermatol Res. 2019;311(3):173–182. doi:10.1007/s00403-019-01895-z
21. Stone SP. Atopic dermatitis and ige. relationship between changes in ige levels and severity of disease. Arch Dermatol. 1976;112(9):1254–1255. doi:10.1001/archderm.1976.01630330024005
22. Laske N, Niggemann B. Does the severity of atopic dermatitis correlate with serum IgE levels? Pediatr Allergy Immunol. 2004;15(1):86–88. doi:10.1046/j.0905-6157.2003.00106.x
23. Joishy M, Alfaham M, Tuthill D. Does the severity of atopic dermatitis correlate with serum IgE levels? Pediatr Allergy Immunol. 2005;16(3):283. doi:10.1111/j.1399-3038.2005.00212.x
24. Renert-Yuval Y, Del Duca E, Pavel AB, et al. The molecular features of normal and atopic dermatitis skin in infants, children, adolescents, and adults. J Allergy Clin Immunol. 2021;148(1):148–163. doi:10.1016/j.jaci.2021.01.001
25. Askin O, Yucesoy SN, Serdaroglu S. The evaluation of dupilumab treatment response in atopic dermatitis patients. North Clin Istanbul. 2020;8:2.
26. Mizuno M, Horiguchi G, Teramukai S, et al. Association study of transition of laboratory marker levels and transition of disease activity of atopic dermatitis patients treated with dupilumab. Australas J Dermatol. 2021;62(4):e504–e509. doi:10.1111/ajd.13719
27. Renert-Yuval Y, Thyssen JP, Bissonnette R, et al. Biomarkers in atopic dermatitis-A review on behalf of the international eczema council. J Allergy Clin Immunol. 2021;147(4):1174–1190.e1. doi:10.1016/j.jaci.2021.01.013
28. Hagino T, Saeki H, Fujimoto E, Kanda N. The eosinophil-to-lymphocyte ratio acts as an indicator for improvement of clinical signs and itch by upadacitinib treatment in atopic dermatitis. J Clin Med. 2023;12(6):2201. doi:10.3390/jcm12062201
29. Hagino T, Saeki H, Kanda N. The efficacy and safety of upadacitinib treatment for moderate to severe atopic dermatitis in real-world practice in Japan. J Dermatol. 2022;49(11):1158–1167. doi:10.1111/1346-8138.16549
30. Hagino T, Saeki H, Fujimoto E, Kanda N. Efficacy and safety of baricitinib treatment for moderate to severe atopic dermatitis in real-world practice in Japan. J Dermatol. 2023;50(7):869–879. doi:10.1111/1346-8138.16763
31. Stalder JF, Taïeb A, Atherton DJ, et al. Severity scoring of atopic dermatitis: the scorad index. consensus report of the European task force on atopic dermatitis. Dermatology. 1993;186(1):23–31.
32. Ständer S, Steinhoff M. Pathophysiology of pruritus in atopic dermatitis: an overview. Exp Dermatol. 2002;11(1):12–24. doi:10.1034/j.1600-0625.2002.110102.x
33. Reich A, Riepe C, Anastasiadou Z, et al. Itch assessment with visual analogue scale and numerical rating scale: determination of minimal clinically important difference in chronic itch. Acta Derm Venereol. 2016;96(7):978–980. doi:10.2340/00015555-2433
34. Legat FJ. Itch in atopic dermatitis - what is new? Front Med . 2021;8:644760. doi:10.3389/fmed.2021.644760
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.