")
Back to Journals » Journal of Asthma and Allergy » Volume 16
Domestic Parasitic Infections in Patients with Asthma and Eosinophilia in Germany – Three Cases with Learnings in the Era of Anti- IL5 Treatments
Authors Barnikel M , Grabmaier U, Mertsch P, Ceelen F, Janke C, Behr J, Kneidinger N , Milger K
Received 5 July 2023
Accepted for publication 18 October 2023
Published 9 November 2023 Volume 2023:16 Pages 1229—1232
DOI https://doi.org/10.2147/JAA.S428607
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Michaela Barnikel,1,2 Ulrich Grabmaier,3 Pontus Mertsch,1,2 Felix Ceelen,4 Christian Janke,5 Jürgen Behr,1,2 Nikolaus Kneidinger,1,2 Katrin Milger1,2
1Department of Medicine V, LMU University Hospital, Munich, Germany; 2Comprehensive Pneumology Center, Member of the German Center for Lung Research (DZL), Munich, Germany; 3Department of Medicine I, LMU University Hospital, Munich, Germany; 4Department of Pneumology, Asklepios-Fachkliniken Munich-Gauting, Gauting, Germany; 5Department of Infectious Diseases and Tropical Medicine, LMU University Hospital, Munich, Germany
Correspondence: Katrin Milger, Department of Medicine V, LMU University Hospital, Marchioninistraße 15, Munich, 81377, Germany, Tel +49 89 4400 73071, Email [email protected]
Abstract: Eosinophilic inflammation is a hallmark of asthma, and blood eosinophilia has been established as a biomarker for phenotyping asthma and predicting the response to anti-IL5 treatments. Although parasitic infections are rare in European adults, they remain an important differential diagnosis for blood eosinophilia. We present three patients with both domestic parasitic infections and asthma to raise awareness of the potential challenge of eosinophilia and to provide experience in the management of parasitic infections in the setting of planned or ongoing anti-IL5 treatment. One, a patient from Croatia with moderate asthma but severe blood eosinophilia had an underlying Strongyloides stercoralis infection, with positive stool cultures. Second, a patient with severe allergic asthma and gastrointestinal symptoms had a positive S. stercoralis titer in serology with a clinical response to treatment with ivermectin. Third, a patient with severe nonallergic eosinophilic asthma and eosinophilic granulomatosis with polyangiitis (EGPA) showed an increasing hepatic tumour under anti-IL5-receptor therapy. Positive serology confirmed the diagnosis of Echinococcus multilocularis, and albendazole therapy was initiated. Anti-IL5 therapies were safely started (Patient 2) or resumed (Patient 3) after the initiation of antiparasitic treatment. Screening for parasitic infections is useful in cases of hypereosinophilia, extrapulmonary symptoms or stay in endemic regions.
Keywords: asthma, eosinophilia, parasitic infections, biologic, anti-IL5 treatment
A Letter to the Editor has been published for this article.
Introduction
Although parasitic infections are rare in European adults, they remain an important differential diagnosis for blood eosinophilia. In asthma, blood eosinophils are a crucial biomarker for phenotyping and a predictor of response to biological therapies in severe asthma. Eosinophils are also an important therapeutic target of some of these antibody therapies especially anti-IL5 and anti-IL5 receptor alpha therapies that improve asthma outcomes by reduction or depletion of eosinophils. Furthermore, for patients with severe asthma under biological therapies, eg anti-IL5-therapy, a risk of acquiring or persisting parasitic infection is conceivable because eosinophils are involved in immune defense against parasites.1 So far, no increased incidence of parasitic infections has been reported under anti-IL5 therapies in humans.2 In addition, data from preclinical models have introduced doubt as to whether eosinophil function is necessary or even beneficial to defend parasitic infection.2 Yet, there is a lack of practical experience regarding management if such an infection occurs under anti-IL5 treatment. We present three patients from our severe asthma unit at the University of Munich, Department of Internal Medicine V, with both domestic parasitic infection and asthma to raise awareness of the role and potential challenge of eosinophilia in the clinical management of these patients.
Case Descriptions
First, a 70-year-old male patient hospitalized in the cardiology unit because of dilated cardiomyopathy (DCM) of unknown origin. Myocardial biopsy showed inflammatory cardiomyopathy without a viral cause, and mycophenolate mofetil (MMF) therapy was initiated. During MMF treatment, blood testing showed an increase in blood eosinophilia of 2500/µL, but moderate eosinophilia had already been present retrospectively. The past medical history included asthma which had been diagnosed 20 years prior and was treated with low-to-medium dose ICS/LABA (budesonide/formoterol 160/4.5 µg 2–4 puffs daily). The lung function showed moderate obstruction with significant bronchodilator reversibility. The patient had no clinically relevant allergies. The patient reported good symptom control and no exacerbation of asthma during the previous three years. He underwent extensive evaluation for possible etiologies of DCM and hypereosinophilia; eosinophilic granulomatosis with polyangiitis (EGPA) and hypereosinophilic syndrome (HES) with cardiac involvement were considered as differential diagnoses. Antineutrophil cytoplasmic antibodies (ANCA) were negative, and computed tomography (CT) showed bronchopathy compatible with asthma but no infiltrates. Bronchoalveolar lavage (BAL) and endobronchial biopsies excluded pulmonary eosinophilia or pulmonary infection. Gastroscopy, bone marrow puncture, and abdominal ultrasonography revealed no abnormalities. Microscopy of the stool revealed Strongyloides stercoralis larvae (Figure 1A). The patient was a farmer from Croatia, a Strongyloides-endemic region. Besides blood eosinophilia, the patient had no clinical symptoms of parasitic infection, notably, no gastrointestinal symptoms. He was treated with ivermectin (200 µg/kg) for two days which rapidly reduced eosinophilia to 300/µL and the stool cultures were negative hereafter. MMF was temporarily paused owing to the risk of fatal hyperinfection syndrome but resumed after ivermectin treatment. Asthma treatment was administered continuously, and the asthma symptoms remained unchanged during follow-up.
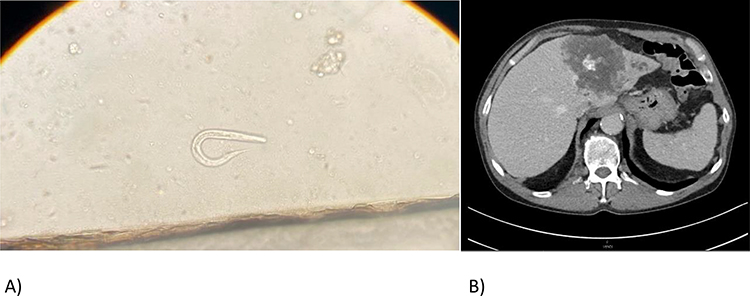 |
Figure 1 (A) Light microscopy picture of Strongyloides stercoralis larvae recovered from stool of patient 1.* (B) Computed tomography showing Echinococcus multilocularis infestation of patient 3. *Reference: Division of Infectious Diseases and Tropical Medicine, Medical Center of the University of Munich (LMU), Germany. |
Second, a 60-year-old woman presented to the severe asthma unit with a history of allergic asthma since adolescence. She had uncontrolled asthma symptoms with intermittent cough and dyspnea and reported comorbidities of rhinoconjunctivitis and nasal polyps. Furthermore, she experienced recurrent attacks of gastrointestinal symptoms, including abdominal cramps, malaise, and diarrhea. Mast cell activation syndrome has been proposed as a prior diagnosis based on a questionnaire; however, objective examination did not confirm clonal mastocytosis. Laboratory showed eosinophilia of 690/µL. Under high-dose ICS/LABA/LAMA, the pulmonary function test results were within the normal range. Previous treatment with the anti-IgE antibody omalizumab had resulted in insufficient treatment response with persistent exacerbations of asthma. Extensive examinations, including screening for EGPA and HES using CT, ANCA, and echo, showed normal results. Screening for parasitic infections before starting anti-iL5- biological therapy, serology showed positive Strongyloides spp. antibodies EIA (enzyme immune assay) with 53 AU (arbitrary units) (normal value <10 AU, borderline 10–14 AU), while stool cultures were negative. The time and location of probable parasitic exposure remain unclear. The patient was treated with ivermectin (200 µg/kg) for one day. Afterwards, gastrointestinal symptoms improved, blood eosinophilia decreased to 300/µL and Strongyloides antibodies decreased (10 AU) and anti-IL-5 therapy was started, resulting in significant improvement in asthma control and reduction of exacerbations.
Our third patient was a 56-year-old man who had been diagnosed with severe eosinophilic asthma and EGPA, including involvement of the lung, heart, skin, central nervous system, and paranasal sinuses, 27 years previously. Immunosuppression with azathioprine and cyclophosphamide has been used previously. At the time of first presentation to our severe asthma unit, he was treated with oral corticosteroids (15 mg daily) mainly for uncontrolled asthma; no other active systemic manifestations of EGPA were apparent. However, blood eosinophil count was increased to 740/µL and asthma symptoms were uncontrolled (ACT score, 12 points). Anti-IL5 therapy was initiated in the indication of severe eosinophilic asthma (first mepolizumab 100 mg s.c. every 4 weeks, later switched to benralizumab 30 mg every 8 weeks), resulting in a significant improvement in asthma control (Asthma Control Test; ACT, 25 points), and prednisolone was tapered off completely. Several years before the start of anti-IL5 therapy, diagnostic evaluation, including biopsy of a hepatic tumor, revealed a calcified granuloma without therapeutic consequences. Two years after starting anti-IL5 therapy the patient experienced deterioration of general condition and weight loss. Hepatic ultrasound and CT showed an increase in the size of the liver tumor with infiltration of the vena cava, vena mesenterica, and pancreas (Figure 1B). Laparoscopic biopsy was performed under the suspicion of malignancy, but E. multilocularis was detected. Serological results were also highly positive (1:2560; reference: 1:160). Anti-IL5 therapy was stopped temporarily, with the subsequent necessity of restarting systemic corticosteroids for asthma control. The patient was started on albendazole (400 mg twice daily for 28 days alternating with a 14 days albendazole interval), and no surgery was performed. Under albendazole, serological Echinococcus-titer decreased (1:512). A few weeks later, benralizumab was reintroduced, which resulted in regaining asthma control and tapering off prednisolone. Albendazole treatment has been ongoing for 2 years, concomitantly with benralizumab, and has led to improvements in the general condition, serology, and imaging.
Discussion
We presented three patients with asthma and comorbid parasitic infections. Our first patient highlighted the divergence between asthma severity (mild to moderate) and severe blood eosinophilia as a clue to an additional cause of eosinophilia other than asthma. Solomon et al confirmed higher absolute eosinophil counts in patients infected with intestinal parasite-infected patients.3 Symptoms including epigastric pain, diarrhea, constipation, skin pruritus, and urticaria may suggest S. stercoralis infection. Endogenous reinfection with Strongyloides larvae involves pulmonary migration, which manifests as cough, dyspnea, and wheezing, similar to the symptoms of asthma. Moreover, the clinical manifestation of parasitic infections is heterogeneous, and the diagnosis of chronic strongyloidiasis can be challenging given the limited sensitivity and specificity of diagnostic tests.4,5 The symptoms in our first patient may have occurred in both asthma/DCM and strongyloidiasis, and the stool culture was positive. Our second patient had marked gastrointestinal symptoms, but the stool culture was negative, while serology showed a high S. stercoralis titer. However, in the latter case, treatment with ivermectin also improved the gastrointestinal symptoms and reduced eosinophilia. Strongyloidiasis is endemic in tropical and subtropical regions with a high regional prevalence of 30%,6 and our cases without travel history support previous reports that domestic infection in middle Europe may occur, especially in individuals pursuing farming activities or miners.7 Our third patient underlines endemic infection with Echinococcus in European adults; therefore, echinococcosis should be considered as a differential diagnosis of unexplained liver lesions.
So far, we have found no publicly available reports on anti-IL5 treatment in cases of coexisting parasitic infections. Thus, an individualized clinical management weighing potential risk and benefit is necessary; in our cases anti- IL5 treatment was started (patient 2) or resumed (patient 3) after initiation of antiparasitic treatment and this approach proved safe. However, when anti-IL5 treatment is paused due to parasitic infection, as in patient 3, this bears the risk of loss of asthma control and results in the necessity to restart prednisolone. Prednisolone not only reduces eosinophils but further affects the function of other immune cells and might be even more hazardous in an ongoing infection than targeted anti-IL5 treatment. This reasoning led us to quickly reintroduce benralizumab in a shared decision with the patient.
Apart from the three cases presented here, no other cases of parasitic infections have occurred in our total cohort of >400 patients with severe asthma treated with biologics, hereof around 200 treated with anti-IL5 treatments.
Conclusion
Although parasitic infections are relatively rare in adults in Europe, they remain a relevant differential diagnosis for eosinophilia even in patients with asthma. We suggest screening for parasitic infection if the presentation of eosinophilic asthma is atypical, including gastrointestinal or other systemic symptoms, in cases of hypereosinophilia, especially with divergence between asthma severity and the amount of blood eosinophilia, or previous stay in endemic regions. In Europe, for such screening, it is reasonable to include serology for Echinococcus and Strongyloides spp., in addition to stool microscopy. After initiation of antiparasitic treatment, the initiation or continuation of anti-IL5 treatment for severe asthma was safe in our patients.
Consent from Patients
All patients gave written consent to participate as well as consent to publish the data. Consent was obtained prior to study commencement.
Ethics Statement
The Ethics Committee of the Ludwig-Maximilians University Munich confirmed that the project did not affect any ethical or legal issues (No. 23-0574 KB). Consequently, consultation with an ethics committee was unnecessary.
Funding
There was no funding.
Disclosure
KM received speaker fees from AstraZeneca, GSK, Novartis, and Sanofi, all outside of the submitted work.
References
1. Tan LD, Schaeffer B, Alismail A. Parasitic (Helminthic) infection while on asthma biologic treatment: not everything is what it seems. J Asthma Allergy. 2019;12:415–420. doi:10.2147/jaa.S223402
2. Jackson DJ, Pavord ID. Living without eosinophils: evidence from mouse and man. Eur Respir J. 2023;61(1):2201217. doi:10.1183/13993003.01217-2022
3. Solomon Y, Malkamu B, Berhan A, et al. Peripheral blood eosinophilia in adult asthmatic patients and its association with the severity of asthma. BMC Pulm Med. 2023;23(1):96. doi:10.1186/s12890-023-02383-x
4. Siddiqui AA, Berk SL. Diagnosis of Strongyloides stercoralis infection. Clin Infect Dis. 2001;33(7):1040–1047. doi:10.1086/322707
5. Buonfrate D, Formenti F, Perandin F, Bisoffi Z. Novel approaches to the diagnosis of Strongyloides stercoralis infection. Clin Microbiol Infect. 2015;21(6):543–552. doi:10.1016/j.cmi.2015.04.001
6. Munisankar S, Rajamanickam A, Balasubramanian S, et al. Seroprevalence of Strongyloides stercoralis infection in a South Indian adult population. PLoS Negl Trop Dis. 2022;16(7):e0010561. doi:10.1371/journal.pntd.0010561
7. Schär F, Trostdorf U, Giardina F, et al. Strongyloides stercoralis: global distribution and risk factors. PLoS Negl Trop Dis. 2013;7(7):e2288. doi:10.1371/journal.pntd.0002288
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.