")
Back to Journals » Journal of Healthcare Leadership » Volume 15
Does Organizational Commitment to Mental Health Affect Team Processes? A Longitudinal Study
Authors Volpi L, Giusino D , Pietrantoni L , De Angelis M
Received 6 July 2023
Accepted for publication 6 October 2023
Published 23 November 2023 Volume 2023:15 Pages 339—353
DOI https://doi.org/10.2147/JHL.S429232
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pavani Rangachari
Lucia Volpi, Davide Giusino, Luca Pietrantoni, Marco De Angelis
Department of Psychology, University of Bologna, Bologna, Italy
Correspondence: Marco De Angelis, Viale Berti Pichat, 5 40127, Bologna, Italy, Tel +39 3288967582, Email [email protected]
Purpose: Team processes, such as reflexivity and participation, are critical for organizational sustainability, especially in high-reliability professions such as healthcare. However, little is known about health-related predictors of team processes. Basing our hypotheses on the Input-Process-Output (IPO) model, this study investigates the influence of perceived organizational commitment to mental health (OCMH) on healthcare workers’ team reflexivity and participation via mental health-specific leadership (MHsL) and team autonomy.
Patients and Methods: The study involved 82 participants (ie, physicians, nurses, healthcare assistants, healthcare technicians, and physiotherapists) working in the Medicine, Emergency, and Neurological Departments at a large public healthcare organization in Italy. Data was gathered at 2-time points, 14 months apart.
Results: The results suggest that healthcare workers’ perception of their organization’s support for mental health at T1 significantly impacts team participation at T2 through MHsL and team autonomy. Likewise, the indirect effect of OCMH through MHsL and team autonomy was also significant in the model predicting team reflexivity. However, in both models, no direct relationship of OCMH on the dependent variables was found.
Conclusion: The findings highlight the importance of a mental health-supportive environment and leadership to foster team autonomy and, subsequentially, team processes, which are fundamental for performance and patient care.
Keywords: mental health-oriented leadership, team autonomy, team reflexivity, team participation, healthcare, workplace mental health
Introduction
The healthcare sector shares important features with High Reliability Organizations (HROs). Firstly, work in healthcare is executed in an environment where the consequences of errors are of high stakes, while their frequency remains notably low.1 Secondly, non-technical skills such as teamwork and leadership are paramount in enhancing effectiveness in HROs.1–3 For instance, in healthcare, efficient teamwork is critical for patient safety and quality of care.4 This effectiveness can also lead to organizational benefits, such as reduced hospitalization time, costs, and fewer unplanned admissions, as well as improved well-being among team members.5 This suggests that high reliability cannot be achieved unless healthcare professionals and technical units coordinate their actions efficiently and effectively to improve or save a patient’s life.1
The Input-Process-Output (IPO) model has been extensively employed to examine team performance.6–12 Meta-analytic findings and literature reviews have identified various team-level input factors that influence team performance, including team autonomy,13 team composition,14 team design,15 and team diversity, among others.16 Similarly, non-team-related variables like leadership and organizational factors have been studied as input indicators.17,18 Studies indicate that transformational leadership positively predicts team performance17 and that efficient team management and a supportive organizational culture can boost team member satisfaction and overall team effectiveness.18 In recent years, attention has shifted to team processes as potential mediating variables between inputs and outputs.19 Factors such as team learning,20 team cohesion,21 team cognition,22 and team adaptation23 may account for significant variance in team performance.
In healthcare, team reflexivity and participation are thought to be particularly influential. Andela and Truchot found that team reflexivity moderated the relationship between emotional dissonance and burnout, thereby lessening the impact of emotional dissonance on emotional exhaustion.24 Similarly, team participation in a sample of 40 healthcare teams was a more significant predictor of improvements in mentally ill patients’ daily activities than the team’s overall smooth functioning.25 While the link between physical and psychological health and individual performance is well-established,26 there is a paucity of research on health-related predictors of team performance, especially those processes crucial for performance.
Mental Health-specific Leadership (MHsL) encompasses leadership practices and competencies particularly suited for managing and supporting mental health in organizational or community contexts.27 Despite emerging evidence pointing to a relationship between MHsL and teamwork via interpersonal conflict and cooperation, no studies have yet examined health-related predictors of team process variables. This research gap is concerning, given the healthcare sector’s heavy reliance on teams28–30 and the psychological stress inherent in the profession. Healthcare workers face daily psychosocial risks, including work overload, interpersonal conflicts, time pressure, and inadequate supervisory support, potentially leading to poor mental health.31 These factors also extend to exposure to traumatic events, long working hours, and heightened work and emotional demands.31 Studies show that up to one-third of healthcare professionals experience emotional exhaustion,32 and the Covid-19 pandemic has exacerbated the sector’s psychosocial risks, worsening healthcare workers’ health outcomes and psychological trauma.32–34
Against the recent changing dynamics within healthcare structures, there is evidence that professionals are navigating a landscape of great transformation.35 The multi-actor approach, increasingly adopted by hospitals, is a testament to this shift. This model, which has been accelerated in part due to the pandemic, sees a redistribution of traditional tasks to a broader spectrum of team members. Such a change is not without its challenges, especially when considering the disparities between urban and rural settings, as well as the dispersion of teams across various locations. In other words, the success of this multi-actor approach depends on several factors, including effective communication between team members.36
Therefore, institutions and companies are now being assessed on their strategies for ensuring staff mental well-being and streamlining team operations amidst these transformative changes. This responsibility extends beyond the organizational framework, placing significant emphasis on the managers and coordinators of these teams. Their leadership methodologies and capacity for adaptability are critical determinants in the efficacy of this transition.37
Recent years have seen the development of health-oriented organizational models designed to assess employee behaviors and practices effectively. One such model, Organizational Commitment to Mental Health (OCMH), emphasizes prioritizing mental health across all organizational levels through leadership support, comprehensive policies, inclusive culture, mental health literacy, accessible services, work-life balance promotion, and periodic evaluation of mental health needs and initiatives.38 Evidence suggests that managerial practices addressing health-detrimental working conditions result in reduced pain, fewer occupational injuries, and greater employee participation, thereby lowering costs.39
This study aims to bridge the identified gaps by examining the relationship between team members’ perception of Organizational Commitment to Mental Health and healthcare workers’ team reflexivity and participation.31,32 Additionally, MHsL and team autonomy are investigated as sequential mediators in this relationship. These hypothesized pathways are rooted in literature that highlights MHsL’s role in influencing teamwork,27 the IPO framework positing team autonomy as an input variable,6,7 and the established relationship between need-supportive leadership and self-determination.37
Background
Team Processes in the Healthcare Sector
In the realm of healthcare, efficient teamwork, as a non-technical skill, is of paramount importance because it directly influences patient safety and the quality of care provided.4,5 The Input-Process-Output model is a framework for understanding variables influencing overall team performance.6,7 This particular model was selected primarily because this study’s variables are explicitly included in its overall conceptualization. Secondly, given its prominence in the field of team performance research,40 employing this framework would allow for comparison with other studies by effectively systematizing factors according to input-process-output variables.
According to this model, team inputs (eg, team characteristics, task design) influence team performance and efficiency through team processes (eg, team reflexivity, team participation) and emergent states (eg, cohesiveness). The revised conceptualization of this model has emphasized the importance of process variables in explaining the I-O relationship as well as the model’s circularity, underlining how team outputs and performance can, in turn, be predictors of team inputs over time. Similarly, Hoegl and Gemuenden elaborated a framework of teamwork quality which assesses the effectiveness of interactions and collaboration within a team.41 Specifically, this model emphasizes six team-level non-technical skills, namely, communication, coordination, and balance of member contributions, interaction, mutual support, effort, and cohesion as fundamental to teamwork quality.
More recent findings have supported the above-mentioned models by highlighting the key role of knowledge sharing,42,43 leadership,44,45 interpersonal relations,46 situational awareness and communication,42 psychological safety,47 and team emotional intelligence,48 in influencing performance in healthcare units. Among other team processes, team reflexivity and team participation have been particularly investigated in the healthcare sector.
Team reflexivity refers to the degree to which teams set aside time to reflect on objectives, working methods, team effectiveness, and communication among members.7 In the context of healthcare teams, team reflexivity mediated the relationship between transactive memory systems (ie, the team members’ shared understanding of who knows what) and team innovation, a necessary skill in the healthcare sector.49 Moreover, Vashdi found that team feedback reflexivity, as opposed to peer assessment, is associated with higher levels of team attention to detail, cooperation, and psychological safety.50 Additionally, evidence shows that a facet of team reflexivity, namely social reflexivity, which involves reflecting on social processes within teams, was found to effectively buffer emotional exhaustion and emotional dissonance among nurses and healthcare assistants.24 Recent reviews have found strong evidence for reflexivity-based interventions, especially video reflexive ethnography filming, to foster teamwork and communication in interprofessional hospital-based healthcare teams.51 Specifically, this implies video recording the team while working and replaying crucial moments to the team members afterwards to highlight functional and helpful routine practices and to identify commonly occurring features to they could better enact and manage them collectively.51
Team participation refers to the extent to which a team encourages collaboration and contribution from all its members.7 Evidence shows that team participation can lead to better patient outcomes. In their study, Alexander et al found that team participation was more important for patient improvements in activities of daily living than the team’s smooth functioning.25 Participatory approaches have increasingly been included in team-level intervention protocols to ultimately widen multidisciplinary team participation and increase the realism and affordability of training.52,53 Moreover, evidence suggests that participatory team-based interventions may decrease emotional exhaustion in healthcare teams.54
Beyond the team process variables, team-level task design represents an important input factor.7 In this regard, a facet of team task design, namely autonomy, refers to the extent to which a team is given the freedom to make decisions on how to accomplish its tasks and the level of collective responsibility it holds. It has been suggested that team autonomy may influence team cohesion, information elaboration (eg information exchange) and boundary management, intended as the process whereby team member engagement in active management of team relationships with external stakeholders.13
Although the importance of team reflexivity, participation and autonomy in healthcare teams is well documented in the literature investigating team performance in the healthcare sector, their determinants have been overlooked. Most studies addressing their predictors were carried out in research and development or new product development teams. For instance, Wu et al identified project management skills, task familiarity and procedural justice as significant predictors of team reflexivity.55 Similarly, interactional justice, team empowerment, goal clarity and transactive memory systems were all related to team reflexivity.56 Moreover, a study conducted with Turkish teams found that organizational justice may function as a predictor of the quality of teamwork in teams engaged in the development of new products.57 Specifically, team members who perceived organizational procedures as fair (procedural justice) also participated in higher-quality interactions as measured by the teamwork quality framework. Furthermore, the role of leadership in increasing team member participation has been underlined.58 Empirical evidence found that supportive leaders who strived to gain consensus and look after the followers’ well-being and satisfaction showed greater levels of team participation in virtual teams than authoritarian leaders.58 Although leadership is believed to have an important role in enabling job autonomy at the individual level,59–64 little is known about antecedents of autonomy at the team level. In this sense, organizational structural changes defining clearer job task (eg, product boundaries) and reducing dependencies on other teams was found to enhance team autonomy in a large public organization.65 This has been supported by other studies providing evidence for the role of team trust in facilitating team autonomy.66
Frameworks such as the IPO model help identify important factors impacting the mentioned team variables. Specifically, the extent of organizational support, which includes providing team members with training information, ensuring frequent communication, and offering general support, can significantly impact team-level processes. This support, combined with the provision of material and human resources, can serve as an enabler for more efficient operations within the team.
Organizational Commitment and Mental Health-Specific Leadership
In the last decade, a rising trend has been observed in the implementation of work-related health promotion practices within organizations. These practices aim to augment workers’ health and well-being through a multi-tiered approach, encompassing primary (eg, wellness programs), secondary (eg, job redesign), and tertiary (eg, cognitive behavioral therapy) prevention programs 65.
Against this background, meta-analytic studies have scrutinized the efficacy of various organizational interventions, such as communication and teamwork interventions67,68 workload and schedule adjustments,69 and participatory organizational strategies like work breaks, workload changes, and task variations.70 Despite the low certainty of the existing evidence, these interventions are generally considered more beneficial than harmful in enhancing psychological well-being among health, humanitarian, and emergency workers.
Recent scholarly work has led to the development of frameworks for evaluating organizational policies, programs, and practices that address the facilitators of worker safety, health, and well-being. Sorensen et al, for instance, provided a comprehensive list of indicators that measure the extent to which occupational health and safety practices are integrated within worksite health promotion.38 These indicators cover multiple dimensions, such as organizational leadership, collaborative efforts between health protection and worksite promotion, supportive policies, and program comprehensiveness.
Leadership plays a pivotal role in shaping organizational culture and practices.71 Numerous studies have examined leaders’ impact on employee mental health.72–79 Recognizing this, the World Health Organization’s most recent guidelines on mental health at work recommend equipping leaders with knowledge and skills, such as early identification of emotional distress and active listening, to promote help-seeking behavior among employees.30
Emerging from this discourse is the concept of health-oriented leadership.80–84 Gurt et al conceptualized this as leaders actively considering and engaging in practices specifically aimed at employee health.80 Their findings suggest distinct effects of general leadership practices and those specifically tailored to mental health. The former was linked to lower employee strain, better psychological climates for health, and higher job satisfaction, whereas the latter were primarily correlated with psychological climate health and increased role ambiguity.
Surprisingly, despite the established role of health-oriented leadership and organizational commitment in influencing employee health, sparse research has delved into their impact on performance metrics, particularly on team performance and team processes. One notable study synthesized finding from 11 qualitative studies focusing on healthcare workers and explored the influence of organizational and leadership commitment on employee participation and voice.85 However, the study did not exclusively focus on mental health. This is a noteworthy gap, especially considering meta-analytic evidence that underscores the mediating role of mental health between leadership and performance.76 This research void becomes more conspicuous when considering the role of health-related variables, like reflexivity and autonomy, as predictors of team processes.
Thus, given the relevance of the health-oriented framework,38 in understanding the potential effect of health-related practices and policies at the organizational level on the workforce’s performance and health, and recent findings linking mental health-specific leadership to teamwork,27 we expect OCMH to boost team reflexivity and participation. In this sense, we hypothesize that the extent to which team members perceive their organization as dedicated to providing the required resources for cultivating favorable working conditions that promote employee safety, health, and well-being will influence the extent to which their team will engage in participatory and reflexive behaviors:
H1a: OCMH predicts team participation so that higher levels of perceived OCMH lead to higher team participation.
H1b: OCMH predicts team reflexivity so that higher levels of perceived OCMH leads to higher team reflexivity.
Moreover, multisource evidence has shown that organizational health climate may have ripple effects on leaders’ health awareness and that this, in turn, leads to subordinate-rated health-promoting leadership behaviors.86 Additionally, considering that organizational practices and culture are represented and embodied by leaders,67 and the models pointing at organizational culture and context in influencing health-oriented leadership,83,87 we expect OCMH to predict the degree to which leaders engage in mental health-promoting behaviors (eg, holding open discussions related to mental health and well-being with subordinates), as rated by their followers:
H2: OCMH predicts MHsL, so higher levels of perceived OCMH lead to greater leader engagement in mental health-specific behaviors.
Lastly, studies have highlighted the role of leadership, especially authentic,62 transformational,59,60 and empowering,88 in increasing individual-level autonomy. In this sense, these leadership styles all stress the importance of leaders’ engagement in need-supportive individualized behaviors toward increasing self-determination and removing potential barriers that may prevent followers from capitalizing on their potential.89,90 In this sense, a recent review on leadership in the healthcare sector91 underscored the importance of a leadership approach that helps create inclusive and secure workplace cultures by stimulating leaders to embody qualities like humility, self-awareness, authenticity, open-mindedness, compassion, courage, credibility, curiosity, creativity, flexibility, and resourcefulness. Similarly, MHsL might also fall in this category, given the crucial need that mental health represents for employees,72 and the operationalization of MHsL as a type of leadership that prescribes leaders’ engagement in behaviors that promote mental well-being and reduce stressors.
However, even though the strong relationship between individual-level autonomy and team autonomy might suggest a leadership effect on team-level autonomy,92 no study, to the authors’ knowledge, has yet to investigate leadership styles in predicting team-level autonomy. Similarly, despite the IPO model pointing to task design variables, such as autonomy, in predicting team processes,6,7,19 no research has yet explored whether team autonomy predicts team participation and reflexivity as process variables. Thus, considering these gaps in research and the leadership literature reported above, we expect MHsL to predict team autonomy and that sequentially, these two variables will mediate the main relationship under investigation:
H3: MHsL predicts team autonomy so that those team members who perceive their leader as being engaged in promoting mental health will also perceive their team to be more autonomous.
H4a: MHsL and team autonomy sequentially mediate the relationship between OCMH and team participation.
H4b: MHsL and team autonomy sequentially mediate the relationship between OCMH and team reflexivity.
Materials and Methods
Participants
The initial sample included 109 respondents, which was reduced to 82 after excluding incomplete answers. Seventy-eight percent of the sample was predominantly female (N = 64), with males being 18 overall (22%). The largest proportion identified themselves within the age range of 45–54 years (34.1%), followed by those in the 55–64 years bracket (24.4%), then those within the 25–34 years (20.7%) and finally 35–44 years (19.5%). In terms of education, most of the sample (36.6%) had concluded a short-cycle tertiary education or held a bachelor’s degree or equivalent (20%).
Participants were all employed at one of the largest public healthcare organizations in Italy. A more detailed breakdown shows that 41% were part of the Department of Medicine, 39% were associated with the Emergency Department, and 19.5% belonged to the Institute of Neurological Sciences (IRCC). The study included a total of 44 nurses (53.7%), 17 physicians (20.7%), 6 healthcare technicians (7.3%), 5 healthcare assistants (4.9%), 6 physiotherapists (6.1%), and 3 health coordinators (3.6%). Additionally, it is important to note that one-fifth (20%) of the respondents held managerial roles within the healthcare institution.
Procedure
The data was collected from a wider seven-measurement-point database as part of the H-WORK 2020 project,93 funded by the EU Horizon 2020 research and innovation program. The H-WORK 2020 aims at designing and validating multilevel interventions for promoting mental health in the workplace. Only the data collected at the first and sixth measurement points were analyzed for the present research (in the present study named T1 and T2). This choice was selected as the 1st and 6th measurement points coincided with pre/post-intervention measurement occasions. The data collected between the pre- and post-measurement time points was intended to monitor the overall intervention implementation process, such as perceptions of the intervention, facilitator, and training design. This information was crucial in providing feedback to the test sites.
The first data collection period (T1) started in March 2021 and ended in July 2021, and the second (T2) started in May 2022 and ended in August 2022. After having given informed consent, participants completed the questionnaires via Qualtrics. To allow data matching across time points, participants were asked at T1 to generate a personal code they had to fill in at the start of survey completion at the next time points. The personal code did not contain any information that would allow participants to be traced down. Participants filled out the questionnaires at their convenience and could drop out anytime. This research received formal endorsement from the Bioethics Panel of the Alma Mater Studiorum—University of Bologna, adhering to ethical standards (Prot. n. 0185076) and aligning with the principles of the Declaration of Helsinki.
Measures
Along with single questions that collected demographic information (ie, age, gender, and education), the questionnaire contained the following scales.
Organizational Commitment to Mental Health
It is defined as the commitment that makes worker safety, health, and well-being a clear priority for the entire organization, drives accountability, and provides the necessary resources and environment to create positive working conditions.38 The scale was adapted from the Leadership Commitment scale validated by Sorensen et al.38 The Italian translation was carried out by trained researchers for administration at the targeted healthcare organization, following a back-translation procedure. It comprised four items, with responses ranging from 1 (never) to 4 (all the time). An example item is
The organization allocates enough resources (such as enough workers and money) to implement policies or programs to protect and promote worker mental health and wellbeing.
Cronbach’s α was 0.87 at T1.
Mental-Health Specific Leadership
In the present study, MHsL refers to all those leadership behaviors that consider employees’ mental health over the long term. This scale’s items were adapted from Gurt et al.80 The Italian translation was carried out by trained researchers for administration at the targeted healthcare organization, following a back-translation procedure. The responses were collected through a 5-point Likert scale ranging from 1 (completely disagree) to 5 (completely agree). Examples of items were as follows “My supervisor discusses topics related to mental health and well-being with us” or “My supervisor is reflecting on how to increase mental health and well-being at our department”. Cronbach’s α was 0.95 at T1.
Team Processes
This study used three dimensions included in the Aston Team Performance Inventory: Team participation, reflexivity, and autonomy.7 For the Italian healthcare organization involved, the Italian validation by Callea et al was used.40 The team participation items measure whether the team encourages the collaboration and contribution of all members to the decision-making process (eg, “Everyone in the team contributes to decision-making”). The team reflexivity scale assesses the extent to which the team allocates time to rethink its objectives, methods, and communication (eg, “The team often reviews its objectives”). The team autonomy items measure the extent to which the team members think that the team has the autonomy to decide the best way to perform a given task (eg, “In this team, we set our own goals”). The response scale ranged from 1 (completely disagree) to 5 (completely agree).
Although previous validations confirmed the measurement of the three scales with four items,7,40 our Confirmatory Factor Analysis (CFA) indicated a need for refinement. Specifically, to enhance the factor structure and mitigate cross-loadings, the team participation scale was reduced from four to two items, excluding “We meet together frequently to ensure effective communication and cooperation” and “We are careful to keep each other informed about work issues”. This adjustment was based on their loading into other factors beyond acceptable thresholds, suggesting they might conceptually tap into different constructs. Post this modification, the CFA results were: χ² = 0.000, CFI = 0.935, TLI = 0.909, RMSEA = 0.126, SRMR = 0.088. The correlations in this revised model ranged between 0.547 and 0.742, which are generally lower than the original ones.
At T2, Cronbach’s α values were 0.84, 0.90 and 0.90 for team participation, reflexivity, and autonomy, respectively.
Analyses
The statistical analysis was performed using PROCESS macro v3.5 in SPSS version 28.94 Model 6 was used to test the effect of organizational commitment to mental health (OCMH) on Team Reflexivity (TR) and Team Participation (TP) through the two mediators, MHsL and Team Autonomy (TA). Following the bootstrapping method, we accepted the indirect effect (IE) as statistically significant only if its bias corrected 95% CI excluded zero. The serial indirect effect size was calculated using k2, a common measure of effect size for mediation that represents the proportion of mediated variance relative to the total effect variance. Higher values indicate stronger mediation.95 The data was examined for normality, utilizing tests such as Shapiro–Wilk and visual assessment of Q-Q plots. Furthermore, all the variables’ skewness and kurtosis values were within the acceptable range, which is generally considered to be −2 and +2, suggesting no significant deviation from a normal distribution.96
Results
Table 1 below provides an overview of the means, standard deviations, Cronbach’s α values, intercorrelations, and potential range of the main variables of this study.
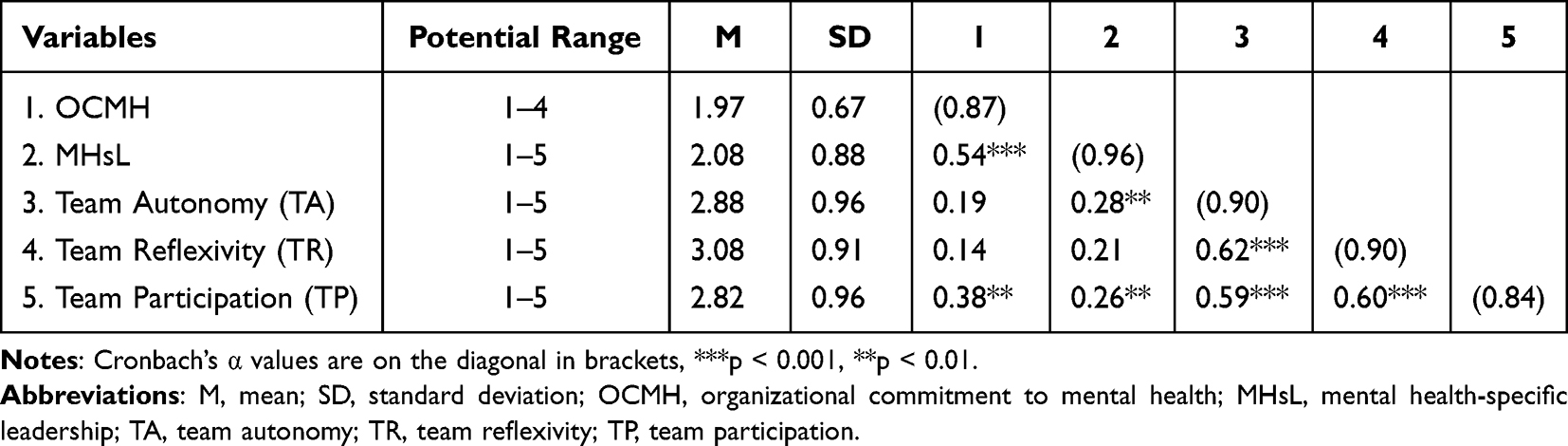 |
Table 1 Correlations and Descriptive Statistics for Key Study Variables (N = 82) |
First, the model predicting TP was tested, the standardized coefficients of the direct effects are presented in Figure 1. OCMH did not show a significant direct effect on TP, β=0.040, p = 0.723, thus failing to support hypothesis 1a. However, hypothesis 2, predicting OCMH direct effects on MHsL, was supported, β=0.544, p < 0.001. Moreover, Hypothesis 3 was confirmed with MHsL significantly predicting TA at T2, β=0.260, p = 0.046. The indirect effect through the two mediators was significant, β = 0.032, SE = 0.027, 95% CI [0.00, 0.11], showing a moderate size (k2= 0.807), suggesting that OCMH influences TP through the serial mediators MHsL and TA, lending support for Hypothesis 4a. The model for the dependent variable explains about 6.28% of the variance (R2=0.063).
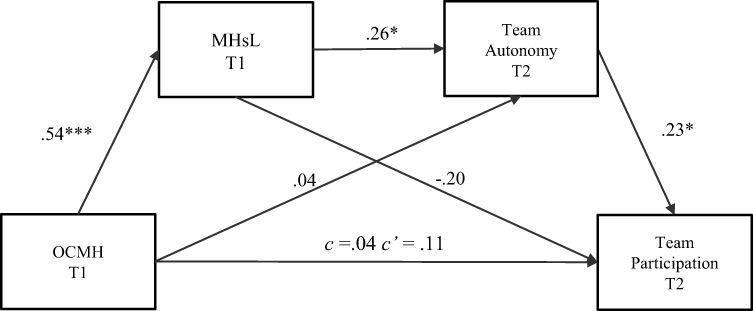 |
Figure 1 Hypothesized serial mediation model: team participation. Abbreviations: OCMH, organizational commitment to mental health, MHsL, Mental health-specific leadership. Notes: ***p < 0.001, *p < 0.05. c, total effect between the independent variable and the dependent variable without considering the mediators, c’, direct effect between the independent variable and the dependent variable after accounting for the mediators. |
Further, the indirect effects of the individual mediators were examined (See Table 2). First, the indirect effect of OCMH on TP via MHsL was not significant, β = −0.108, SE = 0.070, 95% CI [−.22, 0.09], as it was the indirect effect via TA, β = 0.010, SE = 0.040, 95% CI [−.07, 0.10].
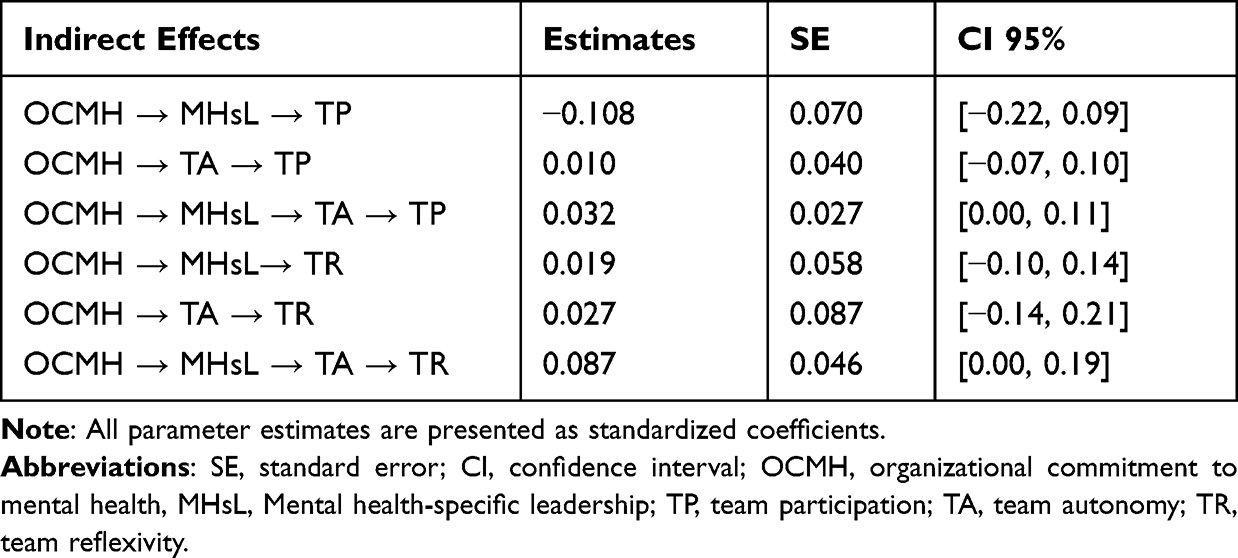 |
Table 2 Bootstrapped Indirect Effect of the Different Dimensions of Team Performance |
In the second model (Figure 2), where TR was predicted, the direct effect of OCMH on TR was non-significant, β = 0.001, p = 0.951, failing to support Hypothesis 2b.
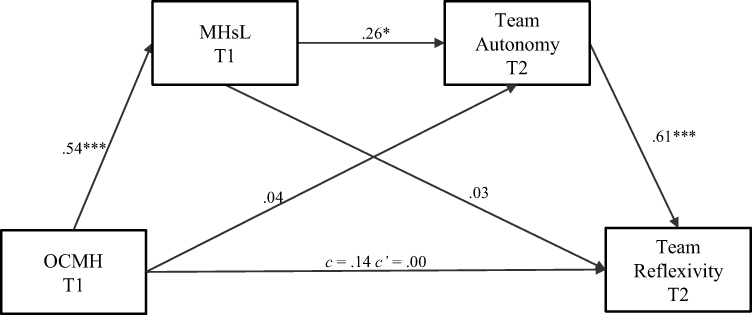 |
Figure 2 Hypothesized serial mediation model: team reflexivity. Abbreviations: OCMH, organizational commitment to mental health, MHsL, Mental health-specific leadership. Notes: ***p < 0.001, *p < 0.05.c, total effect between the independent variable and the dependent variable without considering the mediators, c’, direct effect between the independent variable and the dependent variable after accounting for the mediators. |
As for the indirect effects (see Table 2 for a summary), both paths through the individual mediators, namely MHsL and TA, did not approach significance, with their coefficients being respectively β = 0.019, SE = 0.058, 95% CI [−.10, 0.14] and β = 0.0274, SE = 0.087, 95% CI [−.14, 0.21]. However, the indirect effect accounting for the two mediators showed a significant effect on TR, β = 0.087, SE = 0.046, 95% CI [0.00, 0.19], thus finding evidence for Hypothesis 4b. The serial indirect effect showed moderate size (k2= 0.621), the explained variance of the dependent variable was R2= 0.392.
Discussion
The primary objective of this study was to examine the extent to which the perception of an organization’s commitment to mental health (OCMH) impacts team participation and reflexivity. Additionally, this research sought to explore whether the relationships were mediated by leaders’ enactment of mental health-promoting behaviors, as evaluated by followers, and the perceived autonomy within teams. Our analyses yielded partial confirmation of the proposed models. While the hypothesized direct effects of OCMH on the dependent variables—team participation and reflexivity—were not confirmed by the data, the significance of both sequential models suggests the necessity for intermediate factors, such as leadership behaviors and team autonomy, to mediate the influence of OCMH on team processes.
These findings are congruent with the framework advanced by Sorensen et al, affirming that OCMH is a critical element for healthcare organizations aiming to enhance both participation and reflexivity among health teams.38 This research offers empirical support to the notion that organizational commitment to mental health indeed impacts team-level processes, thereby bolstering the case for its operational importance.
Furthermore, our results align with existing literature advocating a multilevel positive approach to organizational health.86,97 Although the measures employed for multilevel variables are predicated on individual perceptions—hence, are not objective indicators—the evidence suggests that fostering an organizational-level commitment to mental health may cascade down to influence the actions of line managers and supervisors. This trickle-down effect could, in turn, catalyze positive shifts in team dynamics.
The second key finding of the present research is the relationship between MHsL and team autonomy, and the lack of effects between MHsL and the team process variables. In this sense, it appears that leadership that supports psychological and mental well-being primarily influences and motivates followers to cultivate team autonomy, measured by the extent to which the team establishes its own objectives, independently assigns tasks to members, and determines how to execute team assignments.7 These results are consistent with the literature highlighting the role of need-supportive leadership and self-determination,89 and autonomy.59,60,63,88 Moreover, existing literature demonstrates the intrinsic connection between mental health, psychological well-being, and self-determination behaviors. For example, Hindmarch et al discovered that depression weakens individuals’ decision-making capacity, particularly in terms of appreciating relevant information necessary for making informed choices.98
Team autonomy was found to be the only team variable to be directly influenced by MHsL. This differential effect of MHsL may indicate that mental health exerts a significant influence on team input variables, such as autonomy, rather than team processes.
Regarding the indirect effects, neither model found a significant indirect effect of OCMH via MHsL or TA when analyzed independently. However, a significant indirect effect was observed when MHsL and TA were considered sequentially, showing moderate effect sizes. This indicates that OCMH can influence team processes through leadership behaviors and team-level input variables following a complex process involving MHsL and team autonomy.
This study, while offering novel insights, is not without its limitations. The sample size, though modest (N = 82), is particularly noteworthy given the challenges posed by the ongoing pandemic. Conducting a longitudinal study in the healthcare sector during such tumultuous times was a significant undertaking. The healthcare landscape was in constant flux, with frequent organizational changes, staff relocations between urban and rural settings, and the overarching strain of the pandemic itself. However, the sample size does limit the generalizability of our results to larger healthcare organizations. Additionally, the uneven gender and age distributions of our sample might introduce biases. It is worth noting that the healthcare sector is predominantly female, with women accounting for 67% of global employment.99 Therefore, the female overrepresentation in our study can be considered as a reflective element of the broader workforce in this sector.
Given the unprecedented challenges and the emerging nature of this research area, our findings open up a vital opening for further study, especially considering the current strains on healthcare staff and the importance of organizational mental health. Future studies should be mindful of the challenges inherent in collecting longitudinal data in such unstable contexts (eg staff turnover or relocation).
Furthermore, participants involved in this study answered questionnaires representing their perceptions of the teams’ variables, and no unit-level analysis was run, thus limiting the possibility of checking for team-level agreement via multilevel testing. This was mainly due to the fast-changing configuration of teams occurring at the healthcare organization data was collected. The data were collected at two points, but the cross-sectional nature of the study, especially considering the independent variable and the first mediator on one hand and the second mediator and the outcome variables on the other, limits the understanding of how these multilevel variables evolve. Moreover, the organizational commitment and MHsL were solely measured by questionnaires filled out by participants, inflating the possibility of common method bias.100
Despite the study’s limitations, its findings offer valuable insights with practical and theoretical ramifications for healthcare leadership and High-Reliability Organizations (HROs). In an HRO setting, where staff often work under considerable psychological pressures and depend heavily on team dynamics, the importance of fostering a supportive environment for mental health becomes pronounced. This study accentuates the pivotal role of healthcare leaders in championing a mentally healthy organizational culture. Managers and leaders should not only refine their emotional intelligence and communication skills specific to mental health topics but also proactively engage with their teams to set well-being goals and address mental health needs. Implementing such leadership practices contributes to a culture that prioritizes mental health, thereby potentially enhancing team autonomy, participation, and reflexivity.
From a theoretical standpoint, this research bridges existing gaps by elucidating the impact of health-oriented organizational commitment on team-level processes via leadership mechanisms. It also bolsters the argument for multilevel interventions. Our findings have the potential to guide future intervention studies by illustrating how team participation and reflexivity can be nurtured through comprehensive training programs for organizations and leaders specifically tailored to mental health. Moreover, this study advances the field by exploring predictive behaviors and practices related to mental health, enriching the corpus of literature focused on determinants of team-level variables.
In terms of future research directions, several pathways warrant exploration. Firstly, understanding the mediators, such as team self-efficacy or psychological safety, in the relationship between Mental Health-supportive Leadership (MHsL) and team autonomy could be beneficial. The leadership literature could particularly gain from dissecting how different types of leadership—especially those focused on mental health—impact team performance and autonomy in comparison to other styles, like transformational leadership. This is pertinent, given recent meta-analyses that identified relational-oriented and task-oriented leadership as strong predictors of positive mental health outcomes among followers.
Additionally, there is a pressing need for empirical studies to pinpoint the specific leadership behaviors that amplify team performance through mental health support. Determining the essential competencies and skill sets required for leaders to adeptly manage mental health challenges can inform the design of targeted leadership development programs. Future research should also identify potential moderators—such as team characteristics, organizational culture, and industry-specific constraints—that could influence the association between organizational commitment to mental health and team performance. Given the fluctuating nature of team processes, methodological approaches like experience sampling should be employed to capture dynamic interactions among static variables like organizational commitment and culture and more fluid elements such as a leader’s engagement in mental health-related activities and their impact on daily changes in team participation and reflexivity.
In sum, this study serves as a catalyst for healthcare leadership to recognize and act upon the intricate relationship between organizational commitment to mental health and team-level outcomes. The study also paves the way for a richer, more nuanced understanding of how mental health-focused leadership can shape team dynamics in healthcare settings.
Conclusion
To conclude, this study found that an organization’s commitment to mental health can positively influence team participation and reflexivity through the sequential mediating roles of mental health-specific leadership behaviors and team autonomy. Although the direct relationships between organizational commitment and team processes were not significant, the indirect effects suggest that cultivating a workplace environment that prioritizes mental health may motivate leaders to enact supportive behaviors that foster autonomy within teams, thereby enhancing participation and reflexivity. While limited by sample size and cross-sectional data, these findings highlight the potential trickle-down benefits of an organizational commitment to mental health across multiple levels. More research is needed to clarify the mechanisms linking leadership and team processes and to identify optimal strategies for improving team performance through multilevel mental health interventions. Overall, this study underscores the importance of a systemic approach to mental health in healthcare organizations and the catalytic role leaders can play in translating high-level commitment into positive team processes.
Abbreviations
OCMH, Organizational Commitment Tt Mental Health; MHsL, Mental Health-specific Leadership; TA, Team Autonomy; TR, Team Reflexivity; TP, Team Participation.
Data Sharing Statement
The dataset is available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
As part of the H-Work project, this study has received ethical approval from the Bioethics Committee of the Alma Mater Studiorum- University of Bologna, following ethical requirements (Prot. n. 0185076) and in compliance with the Declaration of Helsinki. All participants gave their informed consent, presenting the participation procedures, study content, data collection purposes, future data dissemination methods, participant rights, and contact information. Participation was voluntary, and participants had the option to withdraw at any time without repercussions. The data collected was anonymized.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This paper has received funding from the European Union’s Horizon 2020 research and innovation program under the project H-WORK—Multilevel Interventions to Promote Mental Health in SMEs and Public Workplaces (grant agreement No 847386). The material presented and views expressed here are the responsibility of the authors only. The EU Commission takes no responsibility for any use made of the information set out.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Baker DP, Day R, Salas E. Teamwork as an essential component of High-Reliability organizations. Health Serv Res. 2006;41(4p2):1576–1598. doi:10.1111/j.1475-6773.2006
2. Cooper S, Endacott R, Cant R. Measuring non-technical skills in medical emergency care: a review of assessment measures. Open Access Emergenc Med. 2010;2:7–16. doi:10.2147/OAEM.S6693
3. Hunziker S, Johansson A, Tschan F, et al. Teamwork and Leadership in Cardiopulmonary Resuscitation. J Am Coll Cardiol. 2011;57(24):2381–2388. doi:10.1016/j.jacc.2011.03.017
4. Schmutz JB, Meier LL, Manser T. How effective is teamwork really? The relationship between teamwork and performance in healthcare teams: a systematic review and meta-analysis. BMJ Open. 2019;9(9):e028280. doi:10.1136/bmjopen-2018-028280
5. Mickan S. Evaluating the effectiveness of health care teams. Aust Health Rev. 2005;29(2):211–217. doi:10.1071/AH050211
6. McGrath JE. Groups: Interaction and Performance. New Jersey: Prentice Hall; 1984.
7. Dawson JF, West, MA, Markiewicz, L. Aston Team Performance Inventory: Management Set. ASE; 2006.
8. Kauffeld S, Lehmann-Willenbrock N. Meetings matter. Small Group Res. 2011;43(2):130–158. doi:10.1177/1046496411429599
9. Mathieu JE, Gilson LL, Ruddy TM. Empowerment and team effectiveness: an empirical test of an integrated model. J Appl Psychol. 2006;91(1):97–108. doi:10.1037/0021-9010.91.1.97
10. Hülsheger UR, Anderson N, Salgado JF. Team-level predictors of innovation at work: a comprehensive meta-analysis spanning three decades of research. J Appl Psychol. 2009;94(5):1128–1145. doi:10.1037/a0015978
11. Dulebohn JH, Hoch JE. Virtual teams in organizations. Hum Resour Manag Rev. 2017;27(4):569–574. doi:10.1016/j.hrmr.2016.12.004
12. Powell A, Piccoli G, Ives B. The DATA BASE for Advances in Information Systems. Virtual Teams. 2004;35(1):6–36. doi:10.1145/968464.968467
13. Van Zijl A, Vermeeren B, Koster F, Steijn B. Towards sustainable local welfare systems: the effects of functional heterogeneity and team autonomy on team processes in Dutch neighbourhood teams. Health Soc Care Community. 2019;27(1):82–92. doi:10.1111/hsc.12604
14. Bell S. Deep-level composition variables as predictors of team performance: a meta-analysis. J Appl Psychol. 2007;92(3):595–615. doi:10.1037/0021-9010.92.3.595
15. Stewart GL. A Meta-Analytic Review of Relationships Between Team Design Features and Team Performance. J Manage. 2006;32(1):29–55.
16. Horwitz SK, Horwitz IB. The Effects of Team Diversity on Team Outcomes: a Meta-Analytic Review of Team Demography. J Manage. 2007;33(6):987–1015.
17. Schaubroeck J, Lam SW, Cha SE. Embracing transformational leadership: team values and the impact of leader behavior on team performance. J Appl Psychol. 2007;92(4):1020–1030. doi:10.1037/0021-9010.92.4.1020
18. Doolen TL, Hacker ME, Van Aken EM. The impact of organizational context on work team effectiveness: a study of production team. IEEE Trans on Eng Manag. 2003;50(3):285–296. doi:10.1109/TEM.2003.817296
19. Ilgen DR, Hollenbeck JR, Johnson MK, Jundt DK. Teams in Organizations: from Input-Process-Output Models to IMOI Models. Ann Rev Psychol. 2005;56(1):517–543. doi:10.1146/annurev.psych.56.091103.070250
20. Edmondson AC, Dillon JC, Roloff KS. 6 Three Perspectives on Team Learning. Acad Manag Ann. 2007;1(1):269–314. doi:10.5465/078559811
21. Mathieu JE, Kukenberger M, D’Innocenzo L, Reilly G. Modeling reciprocal team cohesion–performance relationships, as impacted by shared leadership and members’ competence. J Appl Psychol. 2015;100(3):713–734. doi:10.1037/a0038898
22. DeChurch LA, Mesmer-Magnus J. The cognitive underpinnings of effective teamwork: a meta-analysis. J Appl Psychol. 2010;95(1):32–53. doi:10.1037/a0017328
23. Burke CS, Stagl KC, Salas E, Pierce LL, Kendall DL. Understanding team adaptation: a conceptual analysis and model. J Appl Psychol. 2006;91(6):1189–1207. doi:10.1037/0021-9010.91.6.1189
24. Andela M, Truchot D. Emotional Dissonance and Burnout: the Moderating Role of Team Reflexivity and Re-Evaluation. Stress Health. 2017;33(3):179–189. doi:10.1002/smi.2695
25. Alexander JC, Lichtenstein R, Jinnett K, Wells RG, Zazzali JL, Liu D. Cross-Functional Team Processes and Patient Functional Improvement. Health Serv Res. 2005;40(5 Pt 1):1335–1355. doi:10.1111/j.1475-6773.2005.00418.x
26. Ford MJ, Cerasoli CP, Higgins JA, Decesare AL. Relationships between psychological, physical, and behavioural health and work performance: a review and meta-analysis. Work Stress. 2011;25(3):185–204. doi:10.1080/02678373.2011.609035
27. Paganin G, De Angelis M, Pische E, Violante FS, Guglielmi D, Pietrantoni L. The Impact of Mental Health Leadership on Teamwork in Healthcare Organizations: a Serial Mediation Study. Sustainability. 2023;15(9):7337. doi:10.3390/su15097337
28. Ervin JN, Kahn JM, Cohen TR, Weingart LR. Teamwork in the intensive care unit. Am Psychol. 2018;73(4):468–477. doi:10.1037/amp0000247
29. Kilpatrick K, Paquette L, Jabbour M, et al. Systematic review of the characteristics of brief team interventions to clarify roles and improve functioning in healthcare teams. PLoS One. 2020;15(6):e0234416. doi:10.1371/journal.pone.0234416
30. Rosen MJ, DiazGranados D, Dietz AS, et al. Teamwork in healthcare: key discoveries enabling safer, high-quality care. Am Psychol. 2018;73(4):433–450. doi:10.1037/amp0000298
31. World Health Organization. Guidelines on Mental Health at Work. Available from: https://www.who.int/publications/i/item/9789240053052.
32. De Hert S. Burnout in healthcare workers: prevalence, impact, and preventative strategies. Local Reg Anesth. 2020;13:171–183. doi:10.2147/LRA.S240564
33. Franklin P, Gkiouleka A. A Scoping Review of Psychosocial Risks to Health Workers during the Covid-19 Pandemic. Int J Environ Res Public Health. 2021;18(5):2453. doi:10.3390/ijerph18052453
34. Ulfa M, Azuma M, Steiner AK. Burnout status of healthcare workers in the world during the peak period of the COVID-19 pandemic. Front Psychol. 2022;13:952783. doi:10.3389/fpsyg.2022.952783
35. Knop M, Mueller M, Niehaves B. Investigating the use of telemedicine for digitally mediated delegation in team-based primary care: mixed methods study. J Med Internet Res. 2021;23(8):e28151. doi:10.2196/28151
36. Mohr DC, Young GJ, Meterko M, Stolzmann KL, White B. Job satisfaction of primary care team members and quality of care. Am J Med Qual. 2011;26(1):18–25. doi:10.1177/1062860610373378
37. Perez J. Leadership in Healthcare: transitioning From Clinical Professional to Healthcare Leader. J Healthc Manag. 2021;66(4):280–302. doi:10.1097/JHM-D-20-00057
38. Sorensen G, Sparer EH, Williams JA, et al. Measuring Best Practices for Workplace Safety, Health, and Well-Being. J Occup Environ Med. 2018;60(5):430–439. doi:10.1097/JOM.0000000000001286
39. Goetzel RZ, Ozminkowski RJ. The Health and Cost Benefits of Work Site Health-Promotion Programs. Annu Rev Public Health. 2008;29(1):303–323. doi:10.1146/annurev.publhealth.29.020907.090930
40. Callea A, Urbini F, Benevene P, Cortini M, Di Lemma LCG, West M. Psychometric properties, and factor structure of the Italian version of the “Aston Team Performance Inventory”. Team Perform Manag. 2014;20(1/2):6–18. doi:10.1108/TPM-05-2013-0016
41. Hoegl M, Gemuenden HG. Teamwork Quality and the Success of Innovative Projects: a Theoretical Concept and Empirical Evidence. Organ Sci. 2001;12(4):435–449. doi:10.1287/orsc.12.4.435.10635
42. Dijkstra F, Renden PG, Meeter M, et al. Learning about stress from building, drilling, and flying: a scoping review on team performance and stress in non-medical fields. Scand J Trauma Resusc Emerg Med. 2021;29(52). doi:10.1186/s13049-021-00865-7
43. Jamshed S, Nazri M, Bakar RA. The Effect of Knowledge Sharing on Team Performance through Lens of Team Culture. Arab J Bus Manag Rev: Oman Chapter. 2018;7(3):64–80.
44. Aufegger L, McKenzie TJ, Bicknell C, Ashrafian H, Darzi A. Can shared leadership enhance clinical team management? A systematic review. Leadersh Health Serv. 2019;32(2):309–335. doi:10.1108/LHS-06-2018-0033
45. De Brún A, O’Donovan R, McAuliffe E. Interventions to develop collectivistic leadership in healthcare settings: a systematic review. BMC Health Serv Res. 2019;19(72). doi:10.1186/s12913-019-3883-x
46. Lee CE, Doran D. The Role of Interpersonal Relations in Healthcare Team Communication and Patient Safety. Can J Nurs Res. 2017;49(2):75–93. doi:10.1177/0844562117699349
47. Kessel M, Kratzer J, Schultz C. Psychological Safety, Knowledge Sharing, and Creative Performance in Healthcare Teams. Creativity Innov Manag. 2012;21(2):147–157. doi:10.1111/j.1467-8691.2012.00635.x
48. Jamshed S, Majeed N. Relationship between team culture and team performance through lens of knowledge sharing and team emotional intelligence. J Knowl Manag. 2019;23(1):90–109. doi:10.1108/JKM-04-2018-0265
49. Marques-Quinteiro P, Curral L, Passos A, Lewis K, Gomes A. How transactive memory systems and reflexivity relate with innovation in healthcare teams. Análise Psicológica. 2019;37(1):41–51. doi:10.14417/ap.1519
50. Vashdi DR. Teams in Public Administration: a Field Study of Team Feedback and Effectiveness in the Israeli Public Healthcare System. Int Public Manag J. 2013;16(2):275–306. doi:10.1080/10967494.2013.817255
51. McHugh S, Lawton R, O’Hara J, Sheard L. Does team reflexivity impact teamwork and communication in interprofessional hospital-based healthcare teams? A systematic review and narrative synthesis. BMJ Qual Saf. 2020;29(8):672–683. doi:10.1136/bmjqs-2019-009921
52. McAuliffe E, Ward M, DeBrun A, Cunningham U. ISQUA17-2839collective Leadership And Safety Cultures: developing An Alternative Model Of Leadership For Healthcare Teams. Int J Qual Health Care. 2017;29(suppl_1):52–53. doi:10.1093/intqhc/mzx125.84
53. Walker S, Sevdalis N, McKay A, et al. Unannounced in situ simulations: integrating training and clinical practice. BMJ Qual Saf. 2013;22(6):453–458. doi:10.1136/bmjqs-2012-000986
54. van Mierlo H, Rutte CC, Vermunt JK, Kompier MAJ, Doorewaard JACM. A multi-level mediation model of the relationships between team autonomy, individual task design and psychological well-being. J Occup Organ Psychol. 2007;80(4):647–664. doi:10.1348/096317907X196886
55. Wu WY, Rivas A, Chen YC. The role of team reflexivity as a mediator between project management skills, task familiarity, procedural justice, and product performance. J Manag Organ. 2019;25(6):876–895. doi:10.1017/jmo.2017.34
56. Dayan M, Basarir A. Antecedents, and consequences of team reflexivity in new product development projects. J Bus Ind Mark. 2010;25(1):18–29. doi:10.1108/08858621011009128
57. Dayan M, Di Benedetto A. Procedural and interactional justice perceptions and teamwork quality. J Bus Ind Mark. 2008;23(8):566–576. doi:10.1108/08858620810913371
58. Furumo K, De Pillis E, Buxton M The Impact of Leadership on Participation and Trust in Virtual Teams.
59. Asif M, Jameel A, Hussain A, Hwang J, Sahito N. Linking Transformational Leadership with Nurse-Assessed Adverse Patient Outcomes, and the Quality of Care: assessing the Role of Job Satisfaction and Structural Empowerment. Int J Environ Res Public Health. 2019;16(13):2381. doi:10.3390/ijerph16132381
60. Boamah SA, Laschinger HKS, Wong CA, Clarke SP. Effect of transformational leadership on job satisfaction and patient safety outcomes. Nurs Outlook. 2018;66(2):180–189. doi:10.1016/j.outlook.2017.10.004
61. Liu XQ, Baranchenko Y, An F, Lin Z, Ma J. The impact of ethical leadership on employee creative deviance: the mediating role of job autonomy. Leadersh Organ Dev J. 2020;42(2):219–232. doi:10.1108/LODJ-01-2020-0026
62. Malik N, Dhar RL. Authentic leadership and its impact on extra role behaviour of nurses. Pers Rev. 2017;46(2):277–296. doi:10.1108/PR-05-2015-0140
63. Pattnaik SC, Sahoo R. Transformational leadership and organizational citizenship behaviour: the role of job autonomy and supportive management. Manag Res Rev. 2021;44(10):1409–1426. doi:10.1108/MRR-06-2020-0371
64. Shakil RM, Memon MA, Ting H. Inclusive leadership, and innovative work behaviour: the mediating role of job autonomy. Qual Quant. 2021. doi:10.1007/s11135-021-01102-0
65. Mohagheghi P, Lassenius C, Bakken IU. Enabling Team Autonomy in a Large Public Organization. In: Lecture Notes in Business Information Processing. Springer Science+Business Media; 2020:245–252.
66. Prabhu N, Modem R. Shared transformational leadership and emergent team processes: determinants of team viability and team satisfaction. J Asia Bus Stud. 2022;17(2):225–255. doi:10.1108/JABS-04-2021-0141
67. McCulloch PM, Rathbone J, Catchpole K. Interventions to improve teamwork and communications among healthcare staff. BJS Open. 2011;98(4):469–479. doi:10.1002/bjs.7434
68. Romppanen J, Häggman-Laitila A. Interventions for nurses’ well-being at work: a quantitative systematic review. J Adv Nurs. 2017;73(7):1555–1569. doi:10.1111/jan.13210
69. Panagioti M, Panagopoulou E, Bower P, et al. Controlled Interventions to Reduce Burnout in Physicians. JAMA Inter Med. 2017;177(2):195. doi:10.1001/jamainternmed.2016.7674
70. Verbeek JS, Ruotsalainen J, Laitinen J, et al. Interventions to enhance recovery in healthy workers; a scoping review. Occup Med. 2019;69(1):54–63. doi:10.1093/occmed/kqy141
71. Schein EH. Organizational Culture and Leadership. John Wiley & Sons; 2010.
72. Kuoppala J, Lamminpää A, Liira J, Vainio H. Leadership, Job Well-Being, and Health Effects—A Systematic Review and a Meta-Analysis. J Occup Environ Med. 2008;50(8):904–915. doi:10.1097/JOM.0b013e31817e918d
73. Lecours A, Daneau P. Fostering mental health at work: the butterfly effect of management behaviors. Int J Hum Resour. 2021;33(13):2744–2766. doi:10.1080/09585192.2021.1886151
74. Kelloway EK, Barling J. Leadership development as an intervention in occupational health psychology. Work Stress. 2010;24(3):260–279. doi:10.1080/02678373.2010.518441
75. Montano D, Reeske A, Franke FA, Hüffmeier J. Leadership, followers’ mental health and job performance in organizations: a comprehensive meta-analysis from an occupational health perspective. J Organ Behav. 2017;38(3):327–350. doi:10.1002/job.2124
76. Montano D, Schleu JE, Hüffmeier J. A Meta-Analysis of the Relative Contribution of Leadership Styles to Followers’ Mental Health. J Leadersh Organ Stud. 2022;30(1):90–107. doi:10.1177/15480518221114854
77. Nielsen K, Randall RV, Yarker J, Brenner SO. The effects of transformational leadership on followers’ perceived work characteristics and psychological well-being: a longitudinal study. Work Stress. 2008;22(1):16–32. doi:10.1080/02678370801979430
78. Westerlund H, Nyberg A, Bernin P, et al. Managerial leadership is associated with employee stress, health, and sickness absence independently of the demand-control-support model. Work. 2010;37(1):71–79. doi:10.3233/WOR-2010-1058
79. Silva JO, Agreli HF, Harrison R, Peduzzi M, Mininel VA, Xyrichis A. Collective leadership to improve professional practice, healthcare outcomes, and staff well-being. The Cochrane Library; 2021.
80. Gurt J, Schwennen C, Elke G. Health-specific leadership: is there an association between leader consideration for the health of employees and their strain and well-being? Work Stress. 2011;25(2):108–127. doi:10.1080/02678373.2011.595947
81. Butts MM, Hurst CS, Eby LT. Supervisor health and safety support: scale development and validation. J Appl Manag Entrep. 2013;18(1):97–118. doi:10.9774/gleaf.3709.2013.ja.00007
82. Franke FA, Felfe J, Pundt A. The Impact of Health-Oriented Leadership on Follower Health: development and Test of a New Instrument Measuring Health-Promoting Leadership.Zeitschrift Fur Personalforschung.2014;28(1–2):139–161.
83. Rudolph CW, Murphy LA, Zacher H. A systematic review and critique of research on Healthy leadership. Leadersh Q. 2020;31(1):101335. doi:10.1016/j.leaqua.2019.101335
84. Yao L, Li P, Wildy H. Health-Promoting Leadership: concept, Measurement, and Research Framework. Front Psychol. 2021;12:602333. doi:10.3389/fpsyg.2021.602333
85. Morrow KJ, Gustavson AM, Jones J. Speaking up behaviours (safety voices) of healthcare workers: a metasynthesis of qualitative research studies. Int J Nurs Stud. 2016;64:42–51. doi:10.1016/j.ijnurstu.2016.09.014
86. Kaluza AJ, Schuh SC, Kern M, Xin K, Van Dick R. How do leaders’ perceptions of organizational health climate shape employee exhaustion and engagement? Toward a cascading‐effects model. Hum Resour Manage. 2019;59(4):359–377. doi:10.1002/hrm.22000
87. Eberz S, Antoni CH. Das Systemisch-Salutogene Interaktions-Modell (SSIM) – ein ganzheitlicher Ansatz zur Erklärung und Entwicklung gesundheitsförderlicher Interaktionsdynamiken zwischen Führungskräften und Mitarbeitenden. Gruppe Interaktion Organisation Zeitschrift Für Angewandte Organisationspsychologie. 2016;47(3):265–273. [German]. doi:10.1007/s11612-016-0326-6
88. Zhang X, Bartol KM. Linking Empowering Leadership and Employee Creativity: the Influence of Psychological Empowerment, Intrinsic Motivation, and Creative Process Engagement. Acad Manage Rev. 2010;53(1):107–128.
89. Deci EL, Olafsen AH, Ryan RM. Self-Determination Theory in Work Organizations: the State of a Science. Annu Rev Organ Psychol Organ Behav. 2017;4(1):19–43. doi:10.1146/annurev-orgpsych-032516-113108
90. Conger JA, Kanungo RN. The Empowerment Process: integrating Theory and Practice. Acad Manage Rev. 1988;13(3):471–482. doi:10.2307/258093
91. Gottlieb LN, Gottlieb B, Bitzas V. Creating Empowering Conditions for Nurses with Workplace Autonomy and Agency: how Healthcare Leaders Could Be Guided by Strengths-Based Nursing and Healthcare Leadership (SBNH-L). J Healthc Leadersh. 2021;13:169–181. doi:10.2147/JHL.S221141
92. van Mierlo H, Rutte CC, Vermunt JK, Kompier MAJ, Doorewaard JACM. Individual autonomy in work teams: the role of team autonomy, self-efficacy, and social support. Eur J Work Organ Psychol. 2006;15(3):281–299. doi:10.1080/13594320500412249
93. De Angelis M, Giusino D, Nielsen K, et al. H-WORK Project: multilevel Interventions to Promote Mental Health in SMEs and Public Workplaces. Int J Environ Res Public Health. 2020;17(21):8035. doi:10.3390/ijerph17218035
94. Hayes AF. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach.
95. Preacher KJ, Kelley K. Effect size measures for mediation models: quantitative strategies for communicating indirect effects. Psychol Methods. 2011;16(2):93–115. doi:10.1037/a0022658
96. Field A. Discovering Statistics Using IBM SPSS Statistics.
97. Nielsen K, Christensen M. Positive Participatory Organizational Interventions: a Multilevel Approach for Creating Healthy Workplaces. Front Psychol. 2021;12.
98. Hindmarch T, Hotopf M, Owen GI. Depression and decision-making capacity for treatment or research: a systematic review. BMC Med Ethics. 2013;14(1). doi:10.1186/1472-6939-14-54
99. International Labor Organization, World Health Organization. The Gender Pay Gap in the Health and Care Sector: A Global Analysis in the Time of COVID-19. International Labor Organization; 2022.
100. Podsakoff PM, MacKenzie SB, Lee JY, Podsakoff NP. Common method biases in behavioral research: a critical review of the literature and recommended remedies. J App Psychol. 2003;88(5):879–903. doi:10.1037/0021-9010.88.5.879
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.