")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 14
Do Mindfulness Interventions Improve Obesity Rates in Children and Adolescents: A Review of the Evidence
Authors Keck-Kester T , Huerta-Saenz L , Spotts R, Duda L , Raja-Khan N
Received 20 May 2021
Accepted for publication 30 September 2021
Published 25 November 2021 Volume 2021:14 Pages 4621—4629
DOI https://doi.org/10.2147/DMSO.S220671
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ming-Hui Zou
Terrah Keck-Kester,1 Lina Huerta-Saenz,2 Ryan Spotts,1 Laura Duda,1 Nazia Raja-Khan3
1Department of Pediatrics, Division of Academic General Pediatrics, Penn State, Milton S. Hershey Medical Center, Hershey, PA, USA; 2Department of Pediatrics, Division of Pediatric Endocrinology and Diabetes, Penn State, Milton S. Hershey Medical Center, Hershey, PA, USA; 3Department of Medicine, Division of Diabetes, Endocrinology, and Metabolism, Penn State Milton S. Hershey Medical Center, Hershey, Pa, USA
Correspondence: Terrah Keck-Kester Email [email protected]
Abstract: Mindfulness interventions have shown promise in improving self-regulation, depression, anxiety, and stress levels across all ages. Obesity rates in children are rising worldwide. It has been postulated that through improvements in self-regulation with mindfulness interventions, obesity rates can be improved in children and adolescents. In this review, we attempt to explain how mindfulness interventions may impact obesity rates and obesity-related complications and give the current state of evidence for the following mindfulness interventions: Mindful Eating, Mindfulness-Based Stress Reduction, Yoga, Spirituality, and Dialectical Behavior Therapy.
Keywords: mindful eating, yoga, dialectic behavioral therapy, mindful based stress reduction, spirituality
Introduction
Over the last 20 years, childhood obesity has become a major public health concern in the United States. According to the most recent data from the Center for Disease Control and Prevention (CDC) in 2015–2016, 18.5% of American youth between the ages of 2 and 19 were classified as being obese using a body mass index (BMI) threshold >95% for age.1
The rate of obesity increases with age in children. Children between the ages of 2 and 5 have an obesity rate of 13.9% as compared to 20.6% in children between the ages of 12 and 19. In addition, obesity has some ethnic predispositions, with obesity rates being most prevalent among Hispanic and Non-Hispanic Black children with no significant difference between the sexes.1
Obesity begins in childhood due to a combination of genetic, social, physical, and psychological factors.2 As children with obesity age, they often develop obesity-related comorbidities including insulin resistance, early onset diabetes mellitus (DM), hypertension, hyperlipidemia, depression, and sleep apnea.3 These medical conditions often persist into childbearing years and adulthood.4 Pregnancies of women with obesity are more likely to have perinatal complications or be stillborn.5 Infants born to mothers with obesity have increased rates of neuropsychiatric disorders including autism, attention deficit hyperactivity disorder (ADHD), anxiety, depression, eating disorders,6 and adult obesity.7 This circular pattern perpetuates, increasing obesity rates in all ages.
With the increase in families with obesity, pediatric medical providers are consistently charged with finding evidence-based treatments. One area of interest is the use of mindfulness interventions to modulate eating behaviors.
According to Jon Kabat-Zinn, mindfulness is a psychological process of purposely bringing one’s attention to experiences occurring in the present moment without judgment.8 Mindfulness activities have been effective in altering human behavior to improve health promoting behaviors.9–11 In addition, mindfulness activities have consistently shown improvements in levels of stress and anxiety and increased stress has been associated with weight gain.9–12 For these reasons, it seems that mindfulness activities may provide value as a treatment option for patients with obesity.
Human Eating Behavior
To further understand how mindfulness may affect obesity, it seems paramount to understand the psychology of human eating behavior. Human eating behaviors are based on the existence of personal and psychological constraints that operate in addition to food availability. Figure 1 was created by Ulijaszek et al13 based on the initial work of Mela et al,14 and describes a mechanism where human body-weight homeostasis may be maintained or lost based on different factors including food availability, energy density of the diet, genetic, psychological, physiological, behavioral and cultural factors.
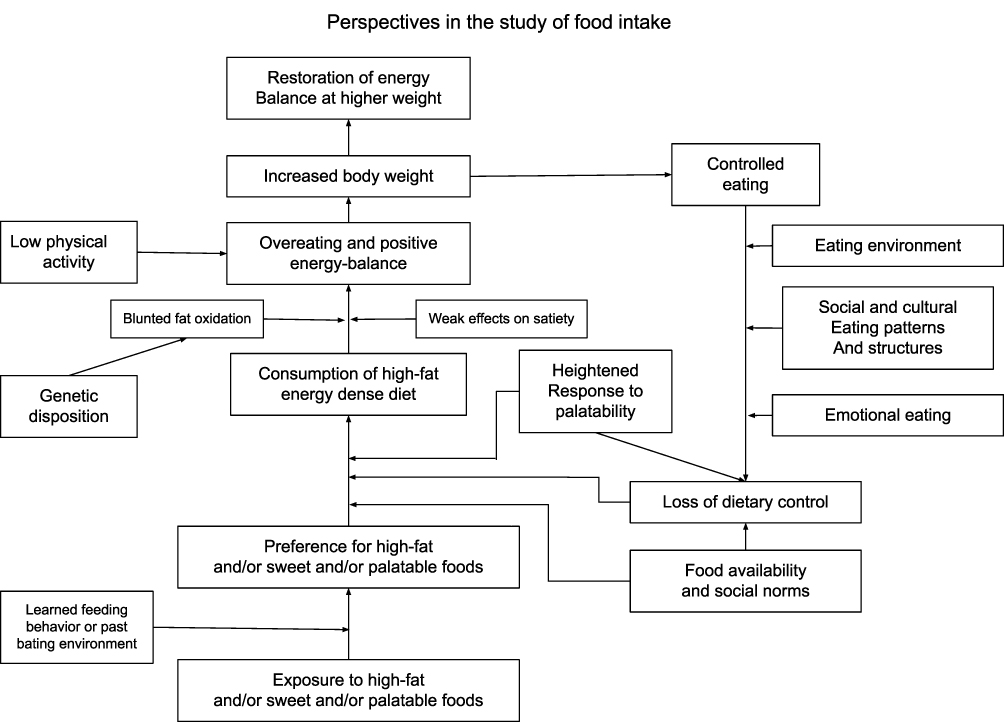 |
Figure 1 Human Eating Behavior and Fatness. |
Figure 1. This flow chart explains that when one is exposed to high fat, sweet, or highly processed foods combined with learned feeding behaviors, preferences for these foods may be established. The combination these preferences, Increased availability of unhealthy foods, loss of dietary control from social and cultural eating patterns, and emotional eating or eating environments, predisposes individuals to over-consumption of energy dense foods. This in turn leads to overeating, positive energy balance, and weight gain. Low physical activity and genetic predisposition may negatively impact the picture further.
Through this theory of the psychological contribution of weight gain, it would be a logical deduction that being more mindful of emotions and how emotions affect eating behaviors would allow one to control what he or she eats. As a consequence, there may be decreased consumption of high calorie foods and increased consumption of healthier, low-calorie foods. With time, this change in food preference may lead to weight control or weight loss and decreased amounts of obesity.
This has been reviewed in adults with mixed results. Weight control seems to improve when mindfulness is combined with weight loss guidance.15 We have not seen any review of this information in children and adolescents.
In this review, we will examine the evidence for a variety of mindfulness activities and their association with weight loss, obesity, and obesity-related complications. These include mindful eating, Mindfulness-Based Stress Reduction (MBSR), yoga, spirituality, and dialectic behavior therapy.
Mindfulness Based Stress Reduction (MBSR)
Mindfulness-Based Stress Reduction (MBSR) is a program developed by Jon Kabat Zinn in 1979. It is an eight-week evidence-based program that teaches a combination of mindfulness meditation, yoga, body awareness, and self-exploration.8 Over the past 50 years, MBSR has been used as an evidence-based mindfulness intervention to treat a variety of medical conditions from diabetes to depression to physician burn out.25–27 As evidence for its effectiveness increases, so do the number of studies on its use, with about 100 new articles each of the last 3 years.
A systematic review in 2012 found that MBSR programs were beneficial in adolescents and school-age children with ADHD, depression, and anxiety. The most prominent effect sizes were in cognitive performance, followed by stress and resilience.28
MBSR is also one of the only interventions that has been examined to improve weights in young children through modification of parental behavior. A study by Jastreboff et al used MBSR-based program, Parenting Mindfully for Health, plus nutrition and exercise counseling. It was aimed at low-income, stressed, parents with obesity and the goal was to evaluate weights in their 2–5 year old children with obesity vs a control group. What they found was significantly improved parental emotional eating and parental involvement. These children showed stabilization of their BMI vs the control group whose BMI increased.29
Another interesting approach is The Mindfulness-Based Eating Awareness (MB-EAT-A) program. The MB-EAT-A program is an adaptation of the MBSR program for adolescents and has been implemented in some high schools.24 In the study performed by Barnes and Kristeller in forty 9th grade adolescents, they showed this program was able to increase the number of servings per week of low-calorie foods (7.7 vs −0.05, p < 0.02) and foods low in saturated fats (4.6 vs −2.7, p < 0.2) after 6 months. After 3 months of the intervention, the MB-EAT-A group slightly decreased in weight 0.3 lbs compared to an increase of 0.4 lbs in the CTL group (p=ns).
In another study, Shomaker et al randomized 12–17-year-old type 2 diabetic females to a 6-week mindfulness intervention (Learning to Breathe) which is based on MBSR vs a Cognitive Behavioral Therapy (CBT) group. They found that right after treatment, those participants in the mindfulness group were significantly improved in depression symptoms and insulin resistance.9 This persisted at 6 months and 1-year post treatment.9,30 At 1-year post treatment, the mindfulness group showed a slight improvement in BMI and percentage body fat.30
From these studies, it seems that improving mindfulness through MBSR or MBSR adapted programs for parents of preschool children and adolescents has been shown stop increases in BMI and improve comorbid conditions including depression, insulin resistance, and parental emotional eating.
Yoga
The practice of Yoga can be traced back to the 3000 BC Sanskrit text of Patjali, an Indian physician and scholar31 Evolving over the years, there are many differences to individual practice of yoga. Most involve a combination of controlled breathing, static and dynamic stretching exercises, and meditation. There are greater than 40 recognized varieties of yoga described in the literature including the popular styles of Iyengar, Ashtanga, Anasara, Bikram, and Hatha to name a few. Many modern practices involve 60 to 90-minute sessions of asanas, or a series of yoga poses designed to be completed in sequence while centering the mind on the breath and mindful experience of muscle activation.
The practice of yoga in the United States has been growing in popularity. A 2016 survey estimates that approximately 13.2% have ever practiced yoga and 8.9% of American adults have practiced within the previous 12 months32 Similar to adults, the practice of yoga amongst children as also been increasing. A 2012 National Health Statistics Report shows an increase in the use of Yoga in children up to 3.1% compared to 2.3% in 2007.33
As the general popularity of yoga has increased, so has the interest in applying its principles to medicine. Between 1975 and 2014, 312 total randomized control trials have been completed. 31 of these trials were completed in children.34 Although not the most common area of investigation, yoga’s impact on adult obesity has been widely studied. A 2013 systematic review by Rioux and Ritenbaugh examined a combination of uncontrolled, controlled, and randomized control trials in order to conclude that yoga was effective in promoting weight loss and improving body composition in adults35 However, in contrast, a 2016 meta-analysis on the effects of yoga and weight-related outcomes by Lauche et al examined 30 trials with a total of 2173 participants and revealed no effects on weight, BMI, body fat percentage, or waist circumference.36
Yoga has been less rigorously studied in children. A 2008 systematic review, not restricted by body mass index, of the positive physical effects of yoga on children concluded possible improvements to cardiorespiratory fitness, physical function, and behavior in children and adolescence.37 A 2009 systematic review by Birdee et al came to similar conclusions on physical benefits and also highlighted potential benefits mental health.38
The relation of yoga’s impact on pediatric obesity is less established. Mind-body medicine in the form of yoga is more commonly used and studied in children as it relates to the potential positive impacts on comorbidities often more prevalent in children with obesity such as stress, depression, anxiety, low self-esteem, and coping.39 A study performed by Hainsworth et al looked at the negative impacts on kinematics of the lower extremities in children with obesity and how yoga may be beneficial. Through bi-weekly one hour classes, nine children participated in an eight-week Iyengar yoga intervention. Significant positive changes in joint motions at the hip, knee, and ankle were noted by the conclusion of the study.40
Mental health benefits have also been reported in small sample sizes. 16 children with obesity took part in an 8 week bi-weekly Iyengar style yoga class after which demonstrating improvements in quality of life and anxiety.40 There have been several small studies showing weight loss as a result of a yoga intervention41–43 Slawta et al included yoga as part of a 12-week focused on improving physical activity and nutrition. The results of this intervention showed significant improvements in body composition and fitness as well as significant reductions in total cholesterol and triglycerides.42 Similar impacts on the reduction of total cholesterol in boys with obesity after an 8-week yoga-asana style training. However, there was no significant difference in triglycerides.43 Despite promising findings of several small studies on weight loss, more recently children and adolescents were examined as part of the 2016 meta-analysis by Lauche et al which concluded no significant effects on weight, BMI, body fat percentage, or waist circumference.36
The heterogeneity of the practice of yoga makes drawing conclusions of effect rather difficult as it relates to obesity. Style variations and individual practice differences can yield wildly dissimilar amounts of physical exertion. For example, Ashtanga’s fast paced nature is likely to burn more calories per session than more traditional Hatha practices.37 Additionally, the time demands and often required formal instruction of yoga make implementation and maintenance of activity challenging across different groups and ages. Developmentally specific suggestions for practice have been described by Kaley-Isley et al as a gradual increase in the amount of time from 15 minutes in preschool aged individuals up to 90 minutes in adolescents. Additional guidance on children with obesity includes gradually increasing movements and gentle encouragement for deeper twists, new poses, and longer holding times of poses to increase capacity to go beyond self-perceived limits.44
Although yoga may not be evidence-based weight loss tool, there are certainly elements that may contribute to a healthier lifestyle with numerous other physical and mental benefits.36,40 Ideally, the clinical application of yoga should be adapted to meet the individual needs of each child and prescribing its use may be a critical part of a comprehensive plan to support the whole individual’s health.
Mindful Eating
One definition of Mindful eating (ME) is the “nonjudgmental awareness of internal and external cues influencing the desire to eat, food choice, and quality of consumption”.16 This process also refers to the process of eating consciously healthy food when it is truly needed.17
Therapeutic interventions utilizing mindful eating are new focus areas that address unhealthy eating behaviors and promote well-being. According to prior cross-sectional studies, mindful eaters prefer to eat food that has a positive impact on their body mass index, portion sizes, emotional eating, and mental wellbeing.18,19
Dispositional mental awareness also plays a significant role in eating behaviors, supporting the use of ME feeding techniques in diabetes self-management interventions.21 ME seems to be associated with weight changes and better glycemic control in patients with diabetes mellitus.22 ME appears to be also effective in addressing emotional eating (EE), binge eating and eating in response to external cues.21
Family-based ME interventions have been shown to result in weight loss among children with Prader-Willi syndrome. Using mindful eating in addition to nutrition guidance and exercise resulted in a patient dropping from 256 lb to 190 lb and continued weight loss 3 years after intervention. (20)
Based on prior experiences, Kumar et al performed a clinical trial in 14–17-year-old adolescents with obesity. Their mindful eating program was administered to the intervention group over four 90-minute sessions by a team comprised of a physician and a trained mind-body therapist. Adolescent/parent pairs in the control group arm received three 90-minute sessions of dietary counseling by a registered dietitian at baseline, 12 weeks, and 24 weeks. Adolescents in the intervention group demonstrated an increase in awareness at 24 weeks (p=0.01) and a decrease in distraction during eating at 12 weeks (p=0.04), when compared to the control group. They reported a 1.4 kg/m2 decrease in BMI in Latino adolescent females after ten-weeks of 90 minute mindful eating session.23
Appreciation for food reflects an individual’s values. According to Fung et al mindful eating also implies an awareness of the relationship between food, the blessings of nature, the lives of animals and plants, and one’s body.18 Kawasaki and Akamatsu describe the role of appreciation for food in the health of children from two perspectives: 1) to describe the association between children’s appreciation for food and their backgrounds, such as home and educational experiences related to food, and 2) to describe the association between their appreciation for food and outcomes, such as attitude toward food, eating behaviors, and health status.17 Their study found significant correlations between gender, educational experiences at home and at school, attitudes toward healthy food, recommended food preferences, breakfast consumption, and BMI (r=0.04, p < 0.05). Participants who had higher scores for appreciation for food, more home and educational experiences, better attitude towards healthy food items and recommended food preferences, and normal BMI consumed more frequently recommended foods. They also were more likely to eat breakfast.
Mindful eating has shown promise in decreasing BMI. This has been seen in places where appreciation for food is valued or when combined with nutritional guidance.
Spirituality
In the past 20 years there has been an increase in research of the effects of religion and spirituality on health.45 This research is challenging to conduct and also to interpret as religion and spirituality (R/S) are difficult to define let alone quantify. (2) Studies looking at religiosity and spirituality and weight management in adults have shown mixed results. The majority of these studies show a positive correlation between R/S and healthy eating, but some reveal a negative correlation.45 When looking specifically at obesity in adults, the studies again are mixed.46
Evidence from the National Study on Youth and Religion, a national longitudinal study of adolescents in the US, reveal that a majority of adolescents feel God and religion are important in their lives.47 It has been suggested that R/S can promote health and wellbeing in adolescents but most of these studies have focused on risk taking behaviors like smoking and substance abuse.48
The research examining R/S and weight management in children and adolescents is scarce. One study looking at family religious practices and BMI found that a parent who endorses a greater importance of religious faith was correlated with lower BMI. Paradoxically, the same study showed that increased religious services attendance correlated with higher BMI.49
The Jackson Heart KIDS study found that daily spirituality in African American adolescents and children was associated with increased rates of attempting to lose weight and using diet-focused weight management.50 A follow-up study using this same patient cohort showed that daily prayer correlated with lower rates of obesity in 12 −15 year olds but not in 16–18 year olds.50
There is a paucity of studies looking at religion and spirituality in weight management for children and adolescents. The studies that have been done reveal conflicting results on whether religion and spirituality promote better weight management. More research needs to be done to elucidate how religiosity and spirituality affect weight management in adolescents and children.
Dialectic Behavior Therapy
Dialectic Behavior Therapy (DBT) is a treatment modality developed by Marsha M Linehan at the University of Washington in the 1980’s to treat patients with borderline personality disorder and serial suicidality.51–54 It combines standard cognitive-behavioral techniques for emotional regulation and reality-testing with concepts of distress tolerance, acceptance, and mindful awareness largely derived from contemplative meditative practice.
DBT adaptations have shown promise in adolescents to decrease the frequency of suicidal behavior and self-harm55 and significantly improve symptoms of borderline personality disorder and depression.56 Due to DBT’s focus on emotional regulation, many have started examining its use in eating disorders, focusing on emotional dysregulation behaviors of restricting, binging-purging, and improvements in body weight in those with anorexia nervosa.57,58
In a recent pilot study, Kamody et al were able to show a significant change in binge eating episodes in those patients 14–18 years of age with Binge Eating Disorder. This change was sustained at 3 months post-intervention.59
Another study by Penell et al examined adolescents aged 13–17 years with eating disorders (mostly anorexia nervosa) at a day treatment facility in Ontario. They used a combination of family-based therapy and DBT. They were able to completely resolve binge eating behaviors of 5/7 patients with anorexia nervosa-binge-eating disorder and significantly decrease these behaviors in the other 2 patients. Patients had significantly improved weights, getting them closer to ideal body weights (p<0.01). Although this study looks at patients with low ideal body weights, it shows promise in the ability to modify the emotional dysregulation related to eating to move body weight closer to ideal.60
Adult studies have shown improvements in reversing weight gain in bariatric patients by modulating binge-eating behaviors in these patients with the use of DBT.61 Most adolescent studies have not specifically evaluated weight loss with DBT. If we extrapolate from adult studies that improving emotional regulation of binge eating behaviors and restrictive behaviors improves weight to baseline, overweight adolescents with emotional dysregulation contributing to weight gain should show improvements with DBT.
Discussion
Obesity in children is epidemic and poses a major public health concern. For many reasons identified in the introduction, the solution to treatment is complex and is at least partially dependent on modulation of human eating behavior. In further exploring the human being’s innate ability to control its behavior, this review attempted to evaluate the evidence for multiple different mind-body interventions that have potential utility in improving the health of children and adolescents with obesity.
We reviewed mind-body interventions ranging from more physically active mindfulness exercises like yoga to physically inactive, while mindfully alert activities such as mindful eating and spirituality. We also included programs like Mindfulness-Based Stress Reduction courses and Dialectic Behavior Therapy and their modifications for children and adolescents as these programs are increasing in popularity as well as the evidence to support their utility.
Mindfulness interventions have the benefit of potentially modulating human-eating behaviors through bringing intent to the act of eating. Intent brings purpose and with purpose we can see change. The challenge in treating patients with obesity is the multifactorial contribution that family, environment, and self play in the development of this condition. With attempting to evaluate the role of mindful interventions we are just touching on the precipice of what we can do to improve the health of these children.
As we have discussed in studies done by Kumar et al and the MB-EAT-A programs, the immediate evidence for weight loss is most impressive when activities such as mindful eating and MBSR are combined with nutrition counseling. This is not a weakness of this study. It does not take away from the power of this program. If our goal is to evaluate how mindfulness interventions can address childhood obesity and mindfulness interventions seem to work best by combining them with interventions that address the nutritional component of obesity than this is a powerful tool we can use to improve the health of children. It seems to be common sense that by spending more time on a multifaceted approach, we can improve not only how people think, feel, and experience the consumption of nutrients, but what they choose to eat.
Children in many ways are completely dependent on the adults in their lives to learn what it means to be a human, how to act in life, and where they can physically get food. We have reviewed that by treating families with preschool children with obesity, teaching the parental unit MBSR, we can effectively improve weight parameters in these children. Childhood behaviors are infinitely dependent on behavior modification of those adults around them. By allowing parents to lead by example, we are improving not only the health of children with obesity but the entire family unit. By investing in the family, we may be able to enhance healthy behaviors across all generations and hopefully stop the cyclical pattern of obesity that we described in the introduction.
Regular yoga practice is a true mind-body treatment. Through our review, we have noted that the kinematics of children with obesity are improved as well as positive changes in body composition were seen with regular yoga practice. These improvements can improve quality of life in children with obesity and in turn support increased weight loss efforts.
Mindfulness interventions also show positive changes in laboratory studies. These include decreased insulin resistance with mindful eating and MBSR and normalized lipid profiles in patients participating in yoga. These improvements objectify the mind-body connection, thus providing further evidence of their utility in maintaining and improving health in children and adolescents.
In addition to the physical complications of obesity, many individuals with obesity suffer from psychological comorbidities including depression and anxiety.3 Mindfulness interventions have been shown to improve depression, anxiety, and suicidality in adolescents through yoga practices, DBT, spirituality, and MBSR. These improvements may help to strengthen the wellbeing of the child or adolescent, allowing them to more fully focus on weight loss behaviors.
Limitations
While exploring the evidence for utilization of mind-body activities for modulation of weight in children and adolescents, it became apparent that the evidence for mindfulness interventions and improvement in obesity in children is scarce but increasing. Holes in the literature include the lack of longer term studies, as I would expect these interventions to have increased effects with time. Despite insufficient studies looking at purely weight or BMI, improvement in co-morbid physical and psychological characteristics are evolving.
One of the biggest challenges in implementing and studying mind-body modalities is the amount of attrition that occurs. In most studies 25–50% of participants fail to complete the intervention. This is improved with inpatient or intensive outpatient interventions, but this also increases the cost of the intervention. Determining factors that would lead to improved completion of the intervention may improve outcomes.
Another major limitation the paucity of studies looking at these interventions on adolescents or parents of younger children. Many of these studies are of small sample size, making the results difficult to interpret.
Conclusion
Mindfulness intervention studies in children are in their infancy, although they show promise. There have been a few studies that have shown positive results regarding stabilizing or decreasing BMI, but they are limited mostly to MBSR, Mindful Eating, and certain kinds of yoga. Other studies have shown more promise treating the psychologic and physiologic comorbidities associated with obesity, such as improvements in kinematics, decreasing rates of anxiety and depression, and improving blood cholesterol and glucose levels. Treating these comorbidities is integral to overall health and wellbeing of children with obesity. For this reason, mindfulness interventions are a reasonable addition to a holistic treatment plan of children with obesity.
Funding
This work was supported by NIH Grant R01DK119379 (NR).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hales CM, Carroll MD, Fryar CD, Ogden CL. Prevalence of Obesity Among Adults and Youth: United States, 2015–2016. NCHS Data Brief. 2017;1:1–8.
2. Jea S, Irby MB, Grzywacz JG, Miller G. Etiologies of Obesity in Children: nature and Nutrute. Pediatric Clin North Am. 2011;58(6):1333–1354. doi:10.1016/j.pcl.2011.09.006
3. Rea B. Severe childhood obesity: an under-recognized and growing health problem. Postgrad Med J. 2015;91(1081):639–645. doi:10.1136/postgradmedj-2014-133033
4. Apovian CM. Obesity: definition, comorbidities, causes, and burden. Am J Manag Care. 2016;22:s176–185.
5. Marchi J, Berg M, Dencker A, Olander EK, Begley C. Risks associated with obesity in pregnancy, for the mother and baby: a systematic review of reviews. Obes Rev. 2015;16:621–638. doi:10.1111/obr.12288
6. Edlow AG. Maternal obesity and neurodevelopmental and psychiatric disorders in offspring. Prenat Diagn. 2017;37:95–110. doi:10.1002/pd.4932
7. Tanvig M. Offspring body size and metabolic profile - effects of lifestyle intervention in obese pregnant women. Dan Med J. 2014;61:B4893.
8. Kabat-Zinn J. Full Catastrophe Living: Using the Wisdom of Your Body and Mind to Face Stress, Pain, and Illness. Revised Edition. U.S.A: Bantam; 2013.
9. Burton A, Burgess C, Dean S, Koutsopoulou GZ, Hugh-Jones S. How Effective are Mindfulness-Based Interventions for Reducing Stress Among Healthcare Professionals? A Systematic Review and Meta-Analysis. Stress Health. 2017;33:3–13. doi:10.1002/smi.2673
10. Oikonomou MT, Arvanitis M, Sokolove RL. Mindfulness training for smoking cessation: a meta-analysis of randomized-controlled trials. J Health Psychol. 2017;22:1841–1850. doi:10.1177/1359105316637667
11. Hofmann SG, Gómez AF. Mindfulness-Based Interventions for Anxiety and Depression. Psychiatr Clin North Am. 2017;40:739–749. doi:10.1016/j.psc.2017.08.008
12. Geiker NRW, Astrup A, Hjorth MF, Sjödin A, Pijls L, Markus CR. Does stress influence sleep patterns, food intake, weight gain, abdominal obesity and weight loss interventions and vice versa? Obes Rev. 2018;19:81–97. doi:10.1111/obr.12603
13. Ulijaszek SJ. Human eating behaviour in an evolutionary ecological context. Proceedings of Nutrition Society. 2002;61(4):517–526. doi:10.1079/PNS2002180
14. Mela DJ. Eating behaviour, food preferences and dietary intake in relation to obesity and body-weight status. Proc Nutr Soc. 1996;55:803–816. doi:10.1079/PNS19960080
15. Katterman SN, Kleinman BM, Hood MM, Nackers LM, Corsica JA. Mindfulness meditation as an intervention for binge eating, emotional eating, and weight loss: a systematic review. Eat Behav. 2014;15:197–204. doi:10.1016/j.eatbeh.2014.01.005
16. Hanh TN CLS. Mindful Eating Mindful Life. New York; 2010.
17. Kawasaki Y, Akamatsu R. Appreciation for food, an important concept in mindful eating: association with home and school education, attitude, behavior, and health status in Japanese elementary school children. Glob Health Promot. 2019;3:1757975919875650.
18. Beshara M, Hutchinson AD, Wilson C. Does mindfulness matter? Everyday mindfulness, mindful eating and self-reported serving size of energy dense foods among a sample of South Australian adults. Appetite. 2013;67:25–29. doi:10.1016/j.appet.2013.03.012
19. Khan ZZZ. Mindful eating and its relationship with mental well-being. Procedia Soc Behav Sci. 2014;159:69–73. doi:10.1016/j.sbspro.2014.12.330
20. Fung TT, Long MW, Hung P, Cheung LW. An expanded model for mindful eating for health promotion and sustainability: issues and challenges for dietetics practice. J Acad Nutr Diet. 2016;116:1081–1086. doi:10.1016/j.jand.2016.03.013
21. Fanning J, Osborn CY, Lagotte AE, Mayberry LS. Relationships between dispositional mindfulness, health behaviors, and hemoglobin A1c among adults with type 2 diabetes. J Behav Med. 2018;41:798–805. doi:10.1007/s10865-018-9938-3
22. Medina WL, Wilson D, de Salvo V, et al. Effects of mindfulness on diabetes mellitus: rationale and overview. Curr Diabetes Rev. 2017;13:141–147. doi:10.2174/1573399812666160607074817
23. Kumar S, Croghan IT, Biggs BK, et al. Family-based mindful eating intervention in adolescents with obesity: a pilot randomized clinical trial. Children. 2018;2:5.
24. Barnes VA, Kristeller JL. Impact of mindfulness-based eating awareness on diet and exercise habits in adolescents. Int J Complement Altern Med. 2016;1;3.
25. Khoury B, Sharma M, Rush SE, Fournier C. Mindfulness-based stress reduction for healthy individuals: a meta-analysis. J Psychosom Res. 2015;78:519–528. doi:10.1016/j.jpsychores.2015.03.009
26. Armani Kian A, Vahdani B, Noorbala AA, et al. The Impact of Mindfulness-Based Stress Reduction on Emotional Wellbeing and Glycemic Control of Patients with Type 2 Diabetes Mellitus. J Diabetes Res. 2018;2018:1986820. doi:10.1155/2018/1986820
27. Verweij H, Waumans RC, Smeijers D, et al. Mindfulness-based stress reduction for GPs: results of a controlled mixed methods pilot study in Dutch primary care. Br J Gen Pract. 2016;66:e99–105. doi:10.3399/bjgp16X683497
28. Zenner C, Herrnleben-Kurz S, Walach H. Mindfulness-based interventions in schools-a systematic review and meta-analysis. Front Psychol. 2014;5:603. doi:10.3389/fpsyg.2014.00603
29. Jastreboff AM, Chaplin TM, Finnie S, et al. Preventing Childhood Obesity Through a Mindfulness-Based Parent Stress Intervention: a Randomized Pilot Study. J Pediatr. 2018;202:136–142.e131. doi:10.1016/j.jpeds.2018.07.011
30. Shomaker LB, Bruggink S, Pivarunas B, et al. Pilot randomized controlled trial of a mindfulness-based group intervention in adolescent girls at risk for type 2 diabetes with depressive symptoms. Complement Ther Med. 2017;32:66–74. doi:10.1016/j.ctim.2017.04.003
31. Field T. Yoga clinical research review. Complement Ther Clin Pract. 2011;17:1–8. doi:10.1016/j.ctcp.2010.09.007
32. Cramer H, Ward L, Steel A, Lauche R, Dobos G, Zhang Y. Prevalence, Patterns, and Predictors of Yoga Use: results of a U.S. Nationally Representative Survey. Am J Prev Med. 2016;50:230–235. doi:10.1016/j.amepre.2015.07.037
33. Black LI, Clarke TC, Barnes PM, Stussman BJ, Nahin RL. Use of complementary health approaches among children aged 4–17 years in the United States: national Health Interview Survey, 2007–2012. Natl Health Stat Report. 2015;54:1–19.
34. Cramer H, Lauche R, Dobos G. Characteristics of randomized controlled trials of yoga: a bibliometric analysis. BMC Complement Altern Med. 2014;14:328.
35. Rioux JG, Ritenbaugh C. Narrative review of yoga intervention clinical trials including weight-related outcomes. Altern Ther Health Med. 2013;19:32–46.
36. Lauche R, Langhorst J, Lee MS, Dobos G, Cramer H. A systematic review and meta-analysis on the effects of yoga on weight-related outcomes. Prev Med. 2016;87:213–232. doi:10.1016/j.ypmed.2016.03.013
37. Galantino ML, Galbavy R, Quinn L. Therapeutic effects of yoga for children: a systematic review of the literature. Pediatr Phys Ther. 2008;20:66–80. doi:10.1097/PEP.0b013e31815f1208
38. Birdee GS, Yeh GY, Wayne PM, Phillips RS, Davis RB, Gardiner P. Clinical applications of yoga for the pediatric population: a systematic review. Acad Pediatr. 2009;9:
39. McClafferty HH. Integrative approach to obesity. Pediatr Clin North Am. 2007;54:969–981. doi:10.1016/j.pcl.2007.10.006
40. Hainsworth KR, Liu XC, Simpson PM, et al. A pilot study of Iyengar yoga for pediatric obesity: effects on gait and emotional functioning. Children. 2018;3:5.
41. Benavides S, Caballero J. Ashtanga yoga for children and adolescents for weight management and psychological well being: an uncontrolled open pilot study. Complement Ther Clin Pract. 2009;15:110–114. doi:10.1016/j.ctcp.2008.12.004
42. Slawta J, Bentley J, Smith J, Kelly J, Syman-Degler L. Promoting healthy lifestyles in children: a pilot program of be a fit kid. Health Promot Pract. 2008;9:305–312. doi:10.1177/1524839906289221
43. Seo DY, Lee S, Figueroa A, et al. Yoga training improves metabolic parameters in obese boys. Korean J Physiol Pharmacol. 2012;16:175–180. doi:10.4196/kjpp.2012.16.3.175
44. Kaley-Isley LC, Peterson J, Fischer C, Peterson E. Yoga as a complementary therapy for children and adolescents: a guide for clinicians. Psychiatry. 2010;7:20–32.
45. Koenig HG. Religion, spirituality, and health: a review and update. Adv Mind Body Med. 2015;29:19–26.
46. Cline KM, Ferraro KF. Does Religion Increase the Prevalence and Incidence of Obesity in Adulthood? J Sci Study Relig. 2006;45:269–281. doi:10.1111/j.1468-5906.2006.00305.x
47. Smith C, Denton ML. Soul Searching: The Religious and Spiritual Lives of American Teenagers. Oxford: Oxford University Press; 2005.
48. Rew L, Wong YJ. A systematic review of associations among religiosity/spirituality and adolescent health attitudes and behaviors. J Adolesc Health. 2006;38:433–442. doi:10.1016/j.jadohealth.2005.02.004
49. Limbers CA, Young D, Bryant W, Stephen M. Associations between family religious practices, internalizing/externalizing behaviors, and body mass index in obese youth. Int J Psychiatry Med. 2015;49:215–226. doi:10.1177/0091217415582191
50. Bruce MA, Beech BM, Wilder T, et al. Religiosity and Excess Weight Among African-American Adolescents: the Jackson Heart KIDS Study. J Relig Health. 2020;59:223–233.
51. Linehan MM. Dialectical behavior therapy for borderline personality disorder. Theory and method. Bull Menninger Clin. 1987;51:261–276.
52. Linehan MM. Dialectical behavior therapy for treatment of borderline personality disorder: implications for the treatment of substance abuse. NIDA Res Monogr. 1993;137:201–216.
53. Linehan MM, Schmidt H, Dimeff LA, Craft JC, Kanter J, Comtois KA. Dialectical behavior therapy for patients with borderline personality disorder and drug-dependence. Am J Addict. 1999;8:279–292. doi:10.1080/105504999305686
54. Linehan MM, Dimeff LA, Reynolds SK, et al. Dialectical behavior therapy versus comprehensive validation therapy plus 12-step for the treatment of opioid dependent women meeting criteria for borderline personality disorder. Drug Alcohol Depend. 2002;67:13–26. doi:10.1016/S0376-8716(02)00011-X
55. Mehlum L, Tørmoen AJ, Ramberg M, et al. Dialectical behavior therapy for adolescents with repeated suicidal and self-harming behavior: a randomized trial. J Am Acad Child Adolesc Psychiatry. 2014;53:1082–1091. doi:10.1016/j.jaac.2014.07.003
56. Moran LR, Kaplan C, Aguirre B, et al. Treatment effects following residential dialectical behavior therapy for adolescents with borderline personality disorder. Evid Based Pract Child Adolesc Ment Health. 2018;3:117–128. doi:10.1080/23794925.2018.1476075
57. Fischer S, Peterson C. Dialectical behavior therapy for adolescent binge eating, purging, suicidal behavior, and non-suicidal self-injury: a pilot study. Psychotherapy. 2015;52:78–92. doi:10.1037/a0036065
58. Peterson CM, Van Diest AMK, Mara CA, Matthews A. Dialectical behavioral therapy skills group as an adjunct to family-based therapy in adolescents with restrictive eating disorders. Eat Disord. 2020;28:67–79. doi:10.1080/10640266.2019.1568101
59. Kamody RC, Thurston IB, Pluhar EI, Han JC, Burton ET. Implementing a condensed dialectical behavior therapy skills group for binge-eating behaviors in adolescents. Eat Weight Disord. 2019;24:367–372. doi:10.1007/s40519-018-0580-4
60. Pennell A, Webb C, Agar P, Federici A, Couturier J. Implementation of dialectical behavior therapy in a day hospital setting for adolescents with eating disorders. J Can Acad Child Adolesc Psychiatry. 2019;28:21–29.
61. Himes SM, Grothe KB, Clark MM, Swain JM, Collazo-Clavell ML, Sarr MG. Stop regain: a pilot psychological intervention for bariatric patients experiencing weight regain. Obes Surg. 2015;25:922–927. doi:10.1007/s11695-015-1611-0
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.