")
Back to Journals » Psychology Research and Behavior Management » Volume 17
Do Adverse Childhood Experiences Make Us More Utilitarian in Moral Dilemmas?
Authors Wu Z , Song J , Chen X, Ding D, Zhang X
Received 15 December 2023
Accepted for publication 22 April 2024
Published 24 April 2024 Volume 2024:17 Pages 1745—1756
DOI https://doi.org/10.2147/PRBM.S455057
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Zhihui Wu,1– 3 Junyao Song,4 Xiyou Chen,1 Daoqun Ding,1– 3,5 Xiangyi Zhang1,6
1Department of Psychology, School of Education Science, Hunan Normal University, Changsha, People’s Republic of China; 2Institute of Interdisciplinary Studies, Hunan Normal University, Changsha, People’s Republic of China; 3Center for Mind and Brain Science, Hunan Normal University, Changsha, People’s Republic of China; 4School of Psychology, Central China Normal University, Wuhan, People’s Republic of China; 5Research Base for Mental Health Education of Hunan Province, Changsha, People’s Republic of China; 6Cognition and Human Behavior Key Laboratory of Hunan Province, Hunan Normal University, Changsha, People’s Republic of China
Correspondence: Daoqun Ding; Xiangyi Zhang, Department of Psychology, School of Education Science, Hunan Normal University, 36 Lushan Road, Changsha, Hunan, 410081, People’s Republic of China, Email [email protected]; [email protected]
Purpose: Adverse childhood experiences (ACEs) have been associated with various aspects of morality, but their precise impact on moral decision-making remains unclear. This study aims to explore how ACEs influence moral decision-making in sacrificial dilemmas.
Methods: Study 1 employed traditional dilemma analysis to quantify utilitarian responses and compare them among groups with no, low, and high ACEs. Study 2 utilized the CNI model to quantify three determinants of moral decision-making: sensitivity to consequences (C parameter), sensitivity to norms (N parameter), and general action tendencies (I parameter). Differences in these parameters among groups with no, low, and high ACEs were investigated.
Results: Both Study 1 and Study 2 revealed that the high-ACE and low-ACE groups showed significantly higher utilitarian responses compared to the no-ACE group. However, no notable differences emerged between the high-ACE and low-ACE groups. Study 2 found that the N parameter was significantly lower in the high-ACE group compared to the low and no-ACE groups. Similarly, the low-ACE group exhibited significantly lower scores in the N parameter compared to the no-ACE group. Additionally, no significant differences were observed in the C and I parameters among groups with no, low, and high ACEs.
Conclusion: These findings suggest that individuals with a high number of ACEs tend to exhibit more utilitarian responses, attributed to decreased affective response to the violation of moral rules, rather than increased deliberative cost-benefit reasoning or a general preference for action. Such insights deepen our understanding of the precise aspects of moral decision-making influenced by ACEs.
Keywords: adverse childhood experiences, moral decision-making, CNI model
Introduction
Previous studies on moral decision-making suggest that deontological and utilitarian responses can be evaluated through moral dilemmas, where considerations for the greater good conflicts with adherence to moral norms.1 An example is the footbridge dilemma,2 where a large man is pushed off the bridge onto the tracks below to save five workers. This dilemma prompts the question: is it acceptable to push a large man in order to save five workers? From a utilitarian perspective, pushing the large man is morally acceptable because it maximizes overall well-being (eg, sacrificing one man could save five). However, from a deontological standpoint, such an action is morally unacceptable as it violates the moral norm prohibiting the harm of innocents.3,4 Responses favoring this action are labeled as utilitarian, prioritizing the greater good, while opposing responses are categorized as deontological, emphasizing adherence to moral norms.5
To explain the empirically observed differences in moral decision-making, the dual-process theory posits that utilitarian responses predominantly stem from cognitive cost-benefit analysis, whereas deontological responses primarily arise from automatic emotional reactions to harm-related scenarios.3,6 This theory suggests that moral decision-making is influenced by various factors, such as empathic concern and cognitive reasoning style.4,7 Additionally, a significant contributor to moral decision-making is an individual’s life experiences, particularly adverse life experiences during childhood and adolescence.8,9
Adverse Childhood Experiences (ACEs) refer to potentially traumatic events encountered by individuals during childhood and adolescence.10–12 It is widely accepted that ACEs are best understood as risk factors.13 ACEs typically categorized into three main categories, comprising a total of 10 risk factors: abuse, which encompasses physical abuse, emotional abuse, and sexual abuse; neglect, including physical neglect and emotional neglect; and household dysfunction, which consists of parental separation or divorce, domestic violence, parental substance abuse, mental illness, and criminal activity.10,11
Numerous studies highlight the significant impact of ACEs on individuals’ mental and physical health. For instance, a meta-analysis revealed that individuals with four or more ACEs are at a heightened risk of various health outcomes compared to those with no ACEs, such as cancer, heart disease, and interpersonal violence.14 The primary theoretical framework for understanding ACEs’ impact is the cumulative risk theory, which suggests that the accumulation of adverse events increases the likelihood of negative outcomes.15,16 ACEs also profoundly affect fundamental psychological processes in adulthood, such as reward and emotion. Individuals with four or more ACEs tend to explore less and undervalue feedback, indicating potential dampening of reward sensitivity.17 They also exhibit decreased sensitivity to emotional valence when processing outgroup members.18 According to dual-process theory, these processes of reward and emotion play a crucial role in moral decision-making.3,6,8,19
Adverse Childhood Experiences and Moral Decision-Making
Previous studies have correlated ACEs with various aspects of morality, including sociomoral capacities like empathic concern, perspective taking, and personal distress,20 as well as morally relevant traits in adulthood like agreeableness, altruism, and prosociality.21,22 Given the influence of these factors on moral decision-making—for instance, individuals with lower empathic concern tending to favor utilitarian over deontological responses7—it’s plausible that ACEs, closely linked to empathic concern, may similarly impact moral decision-making. Consistent with this possibility, several studies have found that individuals who experienced more childhood adversity tend to exhibit more utilitarian responses.8,9 From a utilitarian perspective, this suggests that individuals with more ACEs may be more inclined to prioritize maximizing consequences for the greater good.23 Larsen et al propose an explanation for this utilitarian bias based on the dual-process theory, suggesting that individuals with high ACEs may demonstrate reduced reliance on affective systems. This reduced reliance might lead them to override emotional deontological impulses, thereby directing their moral decision-making through other competing processes that prioritize cognitive assessment of outcomes. Consequently, this may result in a higher frequency of utilitarian choices.8
Although these findings provide an initial perspective on how ACEs influence moral decision-making, their interpretation may be constrained by several methodological issues. Firstly, the traditional dilemma paradigm used in previous research posits utilitarian and deontological responses as bipolar opposites. Here, endorsing the outcome-maximizing option inevitably involves rejecting the norm-adhering option, and vice versa.23,24 Therefore, Larsen et al’s explanation for individuals with more ACEs exhibiting more utilitarian responses may appear incomplete. This is because individuals with a higher number of ACEs exhibiting more utilitarian responses may reflect either (1) an increased cognitive assessment of outcomes or (2) a reduced affective response to the violation of moral norm, or both. Secondly, in the traditional dilemma paradigm, maximizing consequences for the greater good typically implies action (eg, pushing the large man to save five), while adherence to moral norms typically implies inaction (eg, not pushing the large man to save five). Consequently, utilitarian responses become conflated with a general tendency toward action, whereas deontological responses are conflated with a general tendency toward inaction.25,26
Combining these limitations, it remains unclear whether the observed trend of individuals with more ACEs making more utilitarian responses than those with fewer ACEs is driven by differences in (1) the tendency to maximize consequences for the greater good, (2) the inclination to comply with moral norms and duties, or (3) general action tendencies. Recently, several studies have demonstrated that the CNI model is an essential tool for quantifying these three factors underlying responses to moral dilemmas.24–28
CNI Model
The CNI is a multinomial model designed to quantitatively estimate three independent determinants of moral decision-making: sensitivity to consequences (C parameter), sensitivity to moral norms (N parameter), and general preference for inaction versus action without considering consequences and norms (I parameter).26 Each parameter is estimated from participants’ responses to four parallel versions of the dilemmas, each presenting different moral norms (proscriptive versus prescriptive) and consequences (benefits greater than or less than costs).26–28
The model’s C parameter reflects sensitivity to consequences, representing the probability of accepting actions when the benefits outweigh the costs and rejecting them when the costs outweigh the benefits in four parallel versions of moral dilemmas. A higher C parameter indicates a greater impact of consequences on responses, with the range being from 0 to 1. The model’s N parameter reflects sensitivity to norms, representing the probability of accepting inactions if prohibited by moral norms and accepting actions if prescribed by moral norms in four parallel versions of moral dilemmas. A higher N parameter indicates a greater impact of moral norms on responses, with the range also being from 0 to 1. The model’s I parameter reflects a general preference for inaction versus action without considering consequences and norms, representing the probability of accepting actions (versus inactions) in four parallel versions of moral dilemmas. If the I parameter is significantly greater than 0.5, it reflects a general tendency toward inaction, while a value less than 0.5 reflects a general tendency toward action, with the range being from 0 to 1. According to Gawronski et al,23 sensitivity to consequences represents the key aspect of utilitarianism, sensitivity to moral norms represents the key aspect of deontology, and the general preference for inaction is highly correlated with the omission bias.26–28
The Current Research
To address previous research limitations, this study aimed to investigate the impact of ACEs on moral decision-making. Study 1 employed traditional dilemma analysis to quantify utilitarian responses and examine differences among groups with no, low, and high ACEs. In Study 2, the CNI model was utilized to independently quantify three determinants of moral decision-making: sensitivity to consequences (C parameter), sensitivity to norms (N parameter), and general action tendencies (I parameter), also exploring differences among ACEs groups.
Previous studies suggest that individuals with high ACEs show deficiencies in reward and emotion processing.17,18 According to dual-process theory, these deficits may lead to reduced deontological tendencies.23 However, in traditional dilemma analysis, fewer deontological tendencies often result in more utilitarian responses.23,25,29 Hence, we hypothesize that individuals with high ACEs may exhibit higher utilitarian responses compared to those with low or no ACEs in Study 1.
In Study 2, we quantified the C, N, and I parameters separately. Previous research links the N parameter primarily to emotional processing. Deficits in emotional processing may decrease the N parameter while leaving the C and I parameters unaffected.26–28 For example, high levels of alexithymia correlate with low N parameters but show no correlation with the C and I parameters.29 Moreover, ACEs are closely associated with alexithymia.30 Therefore, we hypothesize that individuals in the high ACE group may exhibit significantly lower N parameters compared to those in the low and no ACE groups. However, there may be no differences among the three groups in terms of the C and I parameters.
Study 1: Traditional Dilemma Analysis
Method
Participants
The study initially recruited a total of 2017 participants. 137 participants were excluded from the analysis due to incomplete responses on the ACE questionnaire (participants were given the option to omit questions they preferred not to answer due to the potential pressure induced by recalling ACE experiences), the final sample size comprised 1880 participants (708 females; age range: 17–28 years; Mage = 18.62 years, SDage = 1.15). Based on previous research,16,31 for group-level analyses, participants were categorized based on their ACE scores as follows: those with scores of 0 were assigned to the no ACE group, those with scores ranging from 1 to 3 were assigned to the low ACE group, and participants with scores of 4 or higher were assigned to the high ACE group. The sample consisted of 853 participants in the no-ACE group (277 females; Mage = 18.57 years, SDage = 1.06), 905 participants in the low-ACE group (367 females; Mage = 18.68 years, SDage = 1.25), and 122 participants in the high-ACE group (64 females; Mage = 18.63 years, SDage = 1.03). There were no significant differences in age among the three groups, F (2, 1877) = 2.08, p = 0.125, ηp2 = 0.002, nor in the level of education, F (2, 1877) = 0.92, p = 0.398, ηp2 = 0.001. Because there were fewer females and males in the high-ACE group compared to the other two groups, χ2 (2, N = 1880) = 24.38, p < 0.001, we controlled for sex in the subsequent analyses. Sensitivity analysis performed in G*Power 3.1 revealed that the study, with 1880 participants, achieved 90% power (1 – β = 0.90) to detect a small effect size of f = 0.08 (two-tailed).32 This study was approved by the ethics committee of the first author’s university. All participants carefully read and signed an electronic informed consent form, and they received 2 RMB (Chinese currency) as compensation for their participation.
Materials and Procedure
The sample was recruited through university courses and collected via the wjx.cn platform, a professional online survey platform in China. Participants entered the questionnaire interface by clicking on a provided link. Upon entering the interface, they were required to carefully read the instructions and electronically sign the informed consent form. Subsequently, participants completed a demographic questionnaire, including inquiries about gender, age, and education level. Following this, they filled out the Chinese version of the Adverse Childhood Experiences Questionnaire (ACEQ).11,12,33 This questionnaire assesses the 10 types of adverse childhood experiences encountered by individuals during the initial 18 years of life. The ACEQ consists of 24 items, categorizing experiences into abuse, neglect, and household dysfunction. Responses to abuse, neglect, and household domestic violence items were rated on a 5-point Likert scale, ranging from 1 (never) to 5 (very often). In contrast, responses to other household dysfunction items required dichotomous responses of 0 (no) or 1 (yes). Following the procedures from the previous study,17 participants were provided the option to skip questions they preferred not to answer, as recalling ACE experiences might induce pressure. After conversion to binary format (did not occur: 0, occurred: 1), participants’ ACEQ scores ranged from 0 to 10, providing an assessment of the cumulative impact of multiple ACEs. In previous studies, it is common to use 4 as the threshold to distinguish between high and low ACE scores. The Chinese version of the ACEQ demonstrated reliability and validity for the Chinese population, with a Cronbach’s alpha of 0.65 in this study. Finally, participants responded to four traditional conflict scenarios (Crying baby, Abortion, Vaccine policy, and Animal research), selected from previous studies.19,23,34 Participants were instructed to indicate whether the described action was acceptable or unacceptable by choosing “yes” or “no”. Utilitarian response scores were calculated by summing the “yes” responses across the four moral dilemmas, with higher scores indicating a stronger preference for utilitarian responses.19,23
Results
Descriptive Data
Among the 1880 participants, 54.62% reported experiencing at least one ACEs, while 6.49% reported encountering four or more ACEs before the age of 18. The average number of ACEs reported was 1.07 (SD = 1.33; range = 0–10). Physical abuse was the most frequently reported ACE (27.45%), followed by emotional abuse (22.82%), physical neglect (15.53%), and emotional neglect (9.57%). Additional information on the prevalence of other ACEs and ACE scores can be found in Table 1. Furthermore, Table 2 presents the proportions of utilitarian choices made by the no, low, and high-ACE groups in each dilemma.
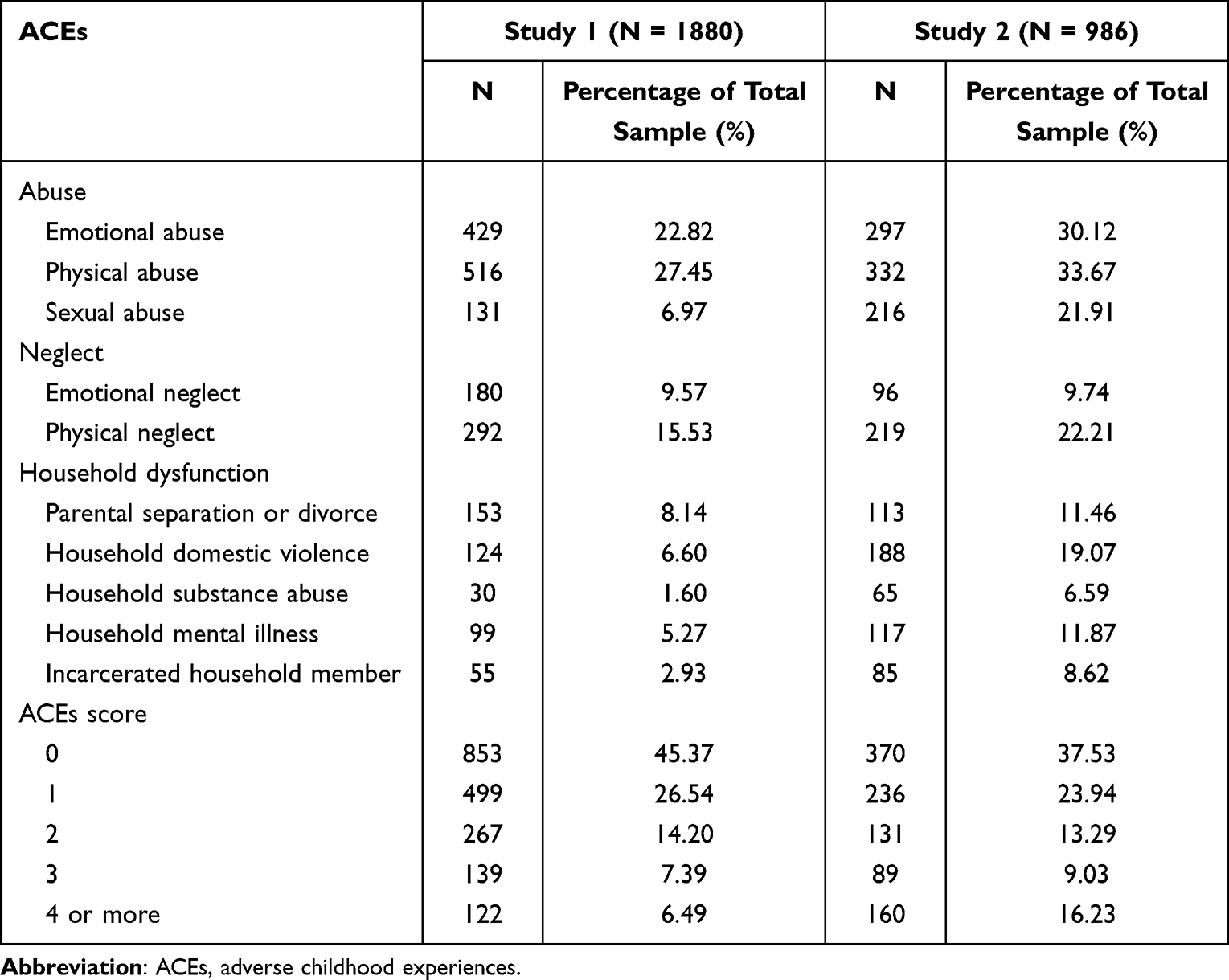 |
Table 1 Prevalence of Each ACE and ACE Scores in the Study 1 and Study 2 |
 |
Table 2 The Proportions of Utilitarian Choices in Each Dilemma Made by the No, Low, and High- ACE Groups |
Traditional Dilemma Analysis
Following previous studies,19,23 utilitarian response scores were calculated by summing the “yes” responses across the four moral dilemmas, with higher scores indicating a stronger preference for utilitarian responses. A univariate analysis of variance (ANOVA) was conducted with group (no-ACE = 1, low-ACE = 2, high-ACE = 3) as the independent variable, utilitarian response scores as the dependent variable and sex as the covariate variable. The analysis revealed a significant main effect of group, F (2, 1876) = 56.42, p < 0.001, ηp2 = 0.06. Post-hoc comparisons showed that the high-ACE group (M = 3.25, SD = 0.97, 95% CI [3.07, 3.42]) scored significantly higher in utilitarian response scores compared to the no-ACE group (M = 2.53, SD = 1.17, 95% CI [2.45, 2.61]), p < 0.001, while no significant differences were found between the high and low-ACE groups (M = 3.05, SD = 1.08, 95% CI [2.98, 3.12]), p = 0.055. Similarly, the low-ACE group scored significantly higher in utilitarian response scores compared to the no-ACE group, p < 0.001. In traditional terms, this result suggests that individuals with a higher number of ACEs demonstrate a greater inclination toward utilitarian over deontological responses.
Discussion
Study 1 employed traditional dilemma analysis to quantify utilitarian responses and investigate differences among groups with no, low, and high ACEs. We observed that both the high and low ACE groups scored significantly higher in utilitarian responses compared to the no-ACE group. Although there were no significant differences between the high and low ACE groups, the trend suggests that the scores of utilitarian responses in the high ACE group remained higher than those of the low ACE group. These results may suggest that individuals with more ACEs may exhibit a stronger preference for utilitarian responses.3,6,8,19,23 This finding is consistent with our hypothesis and previous research.8,9 However, a notable critique of the current findings is that utilitarian response scores were computed by summing “yes” responses to the moral dilemmas. This approach may introduce confounding factors, as utilitarian responses could be conflated with a general inclination toward action, while deontological responses could be conflated with a general inclination toward inaction.25 Combining these confounds makes it challenging to determine whether the observed trends are driven by (1) a tendency to maximize consequences for the greater good, (2) a tendency to comply with moral norms and duties, or (3) a general action tendencies. Recognizing this limitation, Study 2 aimed to address these confounds by employing the CNI model to independently quantify sensitivity to consequences, sensitivity to moral norms, and general preferences for inaction versus action.
Study 2: CNI
Method
Participants
The study initially recruited a total of 1034 participants. 48 participants were excluded from the analysis due to incomplete responses on the ACE questionnaire, the final sample size comprised 986 participants (554 females; age range: 18–38 years; Mage = 20.93 years, SDage = 2.63). For group-level analyses identical to those in Study 1, the sample consisted of 370 participants in the no-ACE group (231 females; Mage = 21.00 years, SDage = 2.71), 456 participants in the low-ACE group (253 females; Mage = 20.91 years, SDage = 2.75), and 160 participants in the high-ACE group (70 females; Mage = 20.83 years, SDage = 2.07). There were no significant differences in age among the three groups, F (2, 983) = 0.27, p = 0.766, ηp2 = 0.001, nor in the level of education, F (2, 983) = 0.65, p = 0.522, ηp2 = 0.001. Because there were fewer females and males in the high-ACE group compared to the other two groups, χ2 (2, N = 986) = 16.01, p < 0.001, we controlled for sex in the subsequent analyses. Sensitivity analysis performed in G*Power 3.1 revealed that the study, with 986 participants, achieved 90% power (1 – β = 0.90) to detect a small effect size of f = 0.11 (two-tailed).32 This study was approved by the ethics committee of the first author’s university. All participants carefully read and signed an electronic informed consent form, and they received 10 RMB for their participation.
Materials and Procedure
The sample was recruited through university courses and collected via the wjx.cn platform. Participants accessed the questionnaire interface by clicking on a provided link. Upon entering the interface, they were required to diligently read the instructions and electronically sign the informed consent form. First, participants filled out a demographic questionnaire, which included questions about sex, age, and education level. Subsequently, they completed the Chinese version of the ACEQ (Cronbach’s alpha was 0.84 in this study).26–28 Participants were provided the option to omit questions they preferred not to answer, as recalling ACE experiences might induce pressure. Finally, participants engaged with six scenarios, each presenting four variants, resulting in a total of 24 moral dilemmas.26 The four variants of each dilemma manipulated different aspects of moral norms (ie, prohibited vs prescribed) and consequences (ie, benefits of action greater vs smaller than costs). The 24 moral dilemmas are presented in a pseudorandom order.26 Participants were instructed to respond with a “yes” or “no” to indicate whether the described action was acceptable or unacceptable The CNI model analysis was conducted using the software multiTree, and the multiTree template file for CNI model analysis was provided by Gawronski et al.26
Results
Descriptive Data
Among the 986 participants, 62.47% disclosed experiencing at least one ACE, with 16.23% indicating four or more ACEs before turning 18. On average, participants reported 1.74 ACEs (SD = 2.20; range = 0–10). Physical abuse also was the most frequently reported ACE (33.67%), followed by emotional abuse (30.12%), sexual abuse (21.91%), physical neglect (21.91%), and domestic violence (19.07%). The prevalence of other ACEs and ACE scores is detailed in Table 1.
Moral dilemma responses were aggregated by calculating the sum of action responses to the four parallel moral dilemmas among the no, low, and high-ACE groups.26 Each dilemma comprised six scenarios, resulting in total scores ranging from 0 to 6. Higher scores indicated a greater preference for action over inaction. The means and 95% confidence intervals among the no, low and high-ACE groups are presented in Table 3.
 |
Table 3 Means and 95% Confidence Intervals of Action Responses to the Four Types of Moral Dilemmas Among the No, Low, and High-ACE Groups |
Traditional Analysis
Following Gawronski et al’s23 methodology, traditional scores were calculated by summing the “yes” responses to moral dilemmas. Specifically, these dilemmas presented scenarios in which a proscriptive norm only prohibited action, and the benefits of taking action outweighed the costs to well-being (similar to the conflict dilemma in study 1, see the second column of Table 3). Higher scores indicate a stronger inclination toward action over inaction, suggesting a greater preference for utilitarian responses over deontological ones.3 A univariate analysis of variance (ANOVA) was conducted with group (no-ACE = 1, low-ACE = 2, high-ACE = 3) as the independent variable, traditional scores as the dependent variable and sex as the covariate variable. The analysis revealed a significant main effect of group, F (2, 982) = 5.66, p = 0.004, ηp2 = 0.01. Post-hoc comparisons showed that the high-ACE group (M = 3.04, SD = 1.35, 95% CI [2.83, 3.25]) scored significantly higher in traditional scores compared to the no-ACE group (M = 2.60, SD = 1.46, 95% CI [2.45, 2.75]), p = 0.002, while no significant differences were found between the high and low-ACE groups (M = 2.84, SD = 1.51, 95% CI [2.71, 2.98]), p = 0.145. Similarly, the low-ACE group scored significantly higher in traditional scores compared to the no-ACE group, p = 0.018. These results are similar to those of Study 1, suggesting that individuals with a higher number of ACEs demonstrate a greater inclination toward utilitarian over deontological responses.
CNI Model
Differences in the C, N, and I parameters among the no, low and high-ACE groups were examined. The data were well-fitted to the CNI model, with G2(3) = 2.73, p = 0.435 (see Table 4). The analysis revealed that the high-ACE group scored significantly lower in the N parameter compared to the low-ACE group (ΔG2(1) = 16.52, p < 0.001, d = 0.37) and the no-ACE group (ΔG2(1) = 48.36, p < 0.001, d = 0.66). The low-ACE group also scored significantly lower in the N parameter compared to the no-ACE group (ΔG2(1) = 16.27, p < 0.001, d = 0.28) (see Figure 1).
 |
Table 4 Means and 95% Confidence Intervals of C, N, and I Parameters Among the No, Low, and High-ACE Groups |
 |
Figure 1 Parameter estimates of sensitivity to consequences (C), sensitivity to norms (N), and general preference for inaction versus action (I) among the no, low, and high-ACE groups. Error bars depict 95% confidence intervals. ***p < 0.001. |
However, there were no significant differences in the C parameter among the three groups: between the high-ACE and low-ACE groups (ΔG2(1) = 1.23, p = 0.268, d = 0.10); between the high-ACE and no-ACE groups (ΔG2(1) = 0.69, p = 0.405, d = 0.08); and between the low-ACE and no-ACE groups (ΔG2(1) = 0.12, p = 0.734, d = 0.02).
Similarly, there were no significant differences in the I parameter among the three groups: between the high-ACE and low-ACE groups (ΔG2(1) = 0.02, p = 0.887, d = 0.01); between the high-ACE and no-ACE groups (ΔG2(1) = 0.09, p = 0.759, d = 0.03); and between the low-ACE and no-ACE groups (ΔG2(1) = 0.05, p = 0.831, d = 0.02).
In summary, these results indicate that individuals with a higher number of ACEs tend to exhibit a stronger inclination toward utilitarian over deontological responses. This inclination is linked to their reduced sensitivity to norms compared to those who reported fewer and no ACEs.
Discussion
Study 2 produced more nuanced results by employing the CNI model, enabling a distinction between general preferences for inaction versus action and specific utilitarian and deontological responses. Significantly, the results of the CNI model revealed pairwise differences in the N parameter among the no, low, and high ACE groups, indicating that individuals exhibit decreased sensitivity to norms as ACEs increase. However, no significant differences were found in the C and I parameters among the three groups. Taken together, these findings suggest that individuals with a higher number of ACEs tend to exhibit more utilitarian responses, attributed to their reduced sensitivity to norms rather than heightened sensitivity to consequences or general action tendencies.26,29
General Discussion
Drawing from cumulative risk theory and dual-process theory,3,6,15,16,19 this study systematically examined the impact of ACEs on moral decision-making in adulthood. The results of traditional dilemma analysis in Studies 1 and 2 revealed that both the high-ACE and low-ACE groups scored significantly higher in utilitarian responses compared to the no-ACE group. Although there were no significant differences between the high and low ACE groups, the trend suggests that the scores of utilitarian responses in the high ACE group remained higher than those of the low ACE group. Furthermore, the results of the CNI model in Study 2 indicated that pairwise differences in the N parameter among the no, low, and high ACE groups, while no significant differences were observed in the C and I parameters among the three groups. Overall, these findings suggest that individuals with more ACEs make more utilitarian responses due to their decreased sensitivity to norms, rather than heightened sensitivity to consequences or general action tendencies. This study contributes to a more nuanced understanding of the psychological consequences of adverse childhood experiences on moral decision processes. Identifying decreased sensitivity to norms as a key factor sheds light on the specific mechanisms through which ACEs may shape moral decision-making patterns.
The current findings are largely consistent with both our hypothesis and previous research.8,9 However, our study provides a more precise explanation compared to prior studies. For example, Larsen et al observed that individuals with a history of childhood trauma tend to make utilitarian choices more frequently. They propose that individuals with a higher incidence of childhood trauma, possibly due to emotional deficits, rely less on their emotional system, allowing their cognitive system to dominate and resulting in more utilitarian responses.8 Our study’s findings indicate that individuals with high ACEs may indeed exhibit more utilitarian responses due to emotional deficits, as supported by results regarding the N parameter. However, their cognitive evaluation of outcomes and general action tendencies do not appear to be enhanced, as indicated by results concerning the C and I parameters.26,29
Why are individuals with higher ACE scores less sensitive to norms? Dual-process theory may provide a possible explanation, suggesting that the effects on the N parameter are mediated by automatic emotional responses to ideas that cause harm.3,6,19,23 This implies that emotional deficits could impair sensitivity to norms. According to cumulative risk theory, individuals with more ACEs often report impaired abilities to effectively identify and regulate their emotions.35,36 Additionally, they commonly report higher levels of alexithymia and lower levels of empathic concern.30 In fact, these characteristics would reduce sensitivity to moral norms.7,29 Consequently, individuals with more ACEs may exhibit reduced sensitivity to norms, possibly due to emotional deficits resulting in diminished emotional responses to harmful thoughts.
Cognitive social learning theory presents an alternative explanatory framework. Moral development constitutes a crucial aspect of a child’s overall development. Children acquire moral values through attentive observation and examples,37 with caregivers such as parents or other adults playing a central role in imparting these morals. When children experience various types of adversity (eg, abuse) from their caretakers or others, their morals and sense of right and wrong can become polluted, leading to poor values or morals in general.38 As a result, they may emulate the deviant and antisocial behaviors of their caretakers and are more likely to violate social norms. Notably, ACEs are positively associated with moral disengagement, suggesting that individuals with more ACEs are more likely to use seemingly reasonable excuses to engage in substance abuse or harm others.39 Thus, individuals with more ACEs may exhibit reduced sensitivity to social norms.
Research on ACEs has predominantly concentrated on their health effects, with the cumulative risk theory serving as the primary theoretical framework for understanding their impact.15,16,40 However, little is known about their impact on a central aspect of social life: morality. Hence, this study systematically examined how ACEs influence moral decision-making, aiming to clarify why individuals with more ACEs tend to show a stronger inclination towards utilitarian responses. Our research findings suggest that the cumulative risk theory is equally applicable in the domain of moral decision-making. We demonstrate that as ACEs accumulate, individuals increasingly tend towards utilitarian responses, accompanied by a diminished sensitivity to norms. Furthermore, our study consistent with the dual-process theory,3,6,19,23 which suggests that emotional deficits may influence deontological inclinations but do not affect utilitarian tendencies. Overall, understanding the influence of ACEs on morality not only enriches psychological and moral frameworks but also informs social interventions and support mechanisms for individuals with a history of adverse experiences.
Limitations and Future Directions
Although this study provides deeper insights into how ACEs influence moral decision-making, three potential limitations should be noted. Firstly, although we collected certain demographic variables such as sex, age, and education level based on previous studies,17 there may still be important information that was overlooked. For instance, the ACE questionnaire assesses the 10 types of adverse childhood experiences encountered by individuals during the initial 18 years of life, however, the age at which adverse experiences occurred may be a significant influencing factor.31 Additionally, family income and parental education levels may also be important factors to consider.13 To enhance the reliability of findings, future studies may benefit from gathering additional demographic variables. Secondly, the cumulative risk model has encountered criticism for treating all ACE events as equally significant.15 Conversely, the multiple individual risk model addresses this limitation by examining the impact of each specific event.16 Future research could benefit from employing the multiple individual risk model to explore how various ACEs affect moral decision-making. Thirdly, while this study identified differences in sensitivity to norms among the three groups, it did not further explore the mechanisms underlying this difference. According to the dual-process theory, effects on sensitivity to norms may be mediated by automatic emotional responses to ideas that cause harm.3,6,19 Future research should explore the relevant psychological and neural mechanisms of the differences in sensitivity to norms between individuals with high and low ACEs.
Conclusion
While numerous studies have examined the proximate psychological processes underlying responses to moral dilemmas, little is known about how early developmental factors influence these processes.9 In this study, we provide deeper insights into how childhood experiences, particularly adverse ones, influence people’s approaches to morality in adulthood. Taken together, these findings suggest that individuals with a high number of ACEs tend to exhibit more utilitarian responses due to reduced affective response to the violation of moral rules, rather than heightened deliberative cost-benefit reasoning or a general preference for action.
Data Sharing Statement
The data is available at https://doi.org/10.17605/OSF.IO/FPE5D.
Ethics Approval and Informed Consent
This study complied with the Declaration of Helsinki. This study was approved by the Ethics Committee of Hunan Normal University, and all participants read and signed the informed consent form.
Acknowledgments
The authors would like to thank the editors and reviewers for their valuable works, as well as all those who participated in the study.
Funding
These studies were supported by the National Natural Science Foundation of China (31900792), the National Social Science Foundation of China (19BSH127) and Postgraduate Scientific Research Innovation Project of Hunan Province (CX20220487).
Disclosure
The authors declare no competing interests in this work.
References
1. Luke DM, Gawronski B. Psychopathy and moral dilemma judgments: a CNI model analysis of personal and perceived societal standards. Soc Cognit. 2021;39(1):41–58. doi:10.1521/soco.2021.39.1.41
2. Thomson J. Killing, letting die, and the trolley problem. In: Reprinted in Rights, Restitution, and Risk. Cambridge: Harvard University Press; 1976:78–93.
3. Greene JD, Sommerville RB, Nystrom LE, Darley JM, Cohen JD. An fMRI investigation of emotional engagement in moral judgment. Science. 2001;293(5537):2105–2108. doi:10.1126/science.1062872
4. Patil I, Zucchelli MM, Kool W, et al. Reasoning supports utilitarian resolutions to moral dilemmas across diverse measures. J Personal Soc Psychol. 2021;120(2):443–460. doi:10.1037/pspp0000281
5. Conway P, Goldstein-Greenwood J, Polacek D, Greene JD. Sacrificial utilitarian judgments do reflect concern for the greater good: clarification via process dissociation and the judgments of philosophers. Cognition. 2018;179:241–265. doi:10.1016/j.cognition.2018.04.018
6. Greene JD. The secret joke of Kant’s soul. Moral Psychol. 2008;3:35–79.
7. Körner A, Deutsch R, Gawronski B. Using the CNI model to investigate individual differences in moral dilemma judgments. Personal Soc Psychol Bulletin. 2020;46(9):1392–1407. doi:10.1177/0146167220907203
8. Larsen EM, Ospina LH, Cuesta-Diaz A, et al. Effects of childhood trauma on adult moral decision-making: clinical correlates and insights from bipolar disorder. J Affective Disorders. 2019;244:180–186. doi:10.1016/j.jad.2018.10.002
9. Maranges HM, Hasty CR, Maner JK, Conway P. The behavioral ecology of moral dilemmas: childhood unpredictability, but not harshness, predicts less deontological and utilitarian responding. J Personal Soc Psychol. 2021;120(6):1696–1719. doi:10.1037/pspp0000368
10. Boullier M, Blair M. Adverse childhood experiences. Paediatrics Child Health. 2018;28(3):132–137. doi:10.1016/j.paed.2017.12.008
11. Dube SR, Williamson DF, Thompson T, Felitti VJ, Anda RF. Assessing the reliability of retrospective reports of adverse childhood experiences among adult HMO members attending a primary care clinic. Child Abuse Negl. 2004;28(7):729–737. doi:10.1016/j.chiabu.2003.08.009
12. Felitti VJ, Anda RF, Nordenberg D, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: the Adverse Childhood Experiences (ACE) Study. Am J Preventive Med. 1998;14(4):245–258. doi:10.1016/S0749-3797(98)00017-8
13. Portwood SG, Lawler MJ, Roberts MC. Science, practice, and policy related to adverse childhood experiences: framing the conversation. Am Psychologist. 2021;76(2):181–187. doi:10.1037/amp0000809
14. Hughes K, Bellis MA, Hardcastle KA, et al. The effect of multiple adverse childhood experiences on health: a systematic review and meta-analysis. Lancet Public Health. 2017;2(8):e356–e366. doi:10.1016/S2468-2667(17)30118-4
15. Evans GW, Li D, Whipple SS. Cumulative risk and child development. Psychol Bull. 2013;139(6):1342–1396. doi:10.1037/a0031808
16. LaNoue MD, George BJ, Helitzer DL, Keith SW. Contrasting cumulative risk and multiple individual risk models of the relationship between Adverse Childhood Experiences (ACEs) and adult health outcomes. BMC Me Res Method. 2020;20(1):1–10. doi:10.1186/s12874-020-01120-w
17. Lloyd A, McKay RT, Furl N. Individuals with adverse childhood experiences explore less and underweight reward feedback. Proc Natl Acad Sci. 2022;119(4):e2109373119. doi:10.1073/pnas.2109373119
18. Krautheim JT, Straube B, Dannlowski U, et al. Outgroup emotion processing in the vACC is modulated by childhood trauma and CACNA1C risk variant. Soc Cognit Affective Neurosci. 2018;13(3):341–348. doi:10.1093/scan/nsy004
19. Greene JD, Nystrom LE, Engell AD, Darley JM, Cohen JD. The neural bases of cognitive conflict and control in moral judgment. Neuron. 2004;44(2):389–400. doi:10.1016/j.neuron.2004.09.027
20. Narvaez D, Wang L, Cheng Y. The evolved developmental niche in childhood: relation to adult psychopathology and morality. Appl Develop Sci. 2016;20(4):294–309. doi:10.1080/10888691.2015.1128835
21. Kochanska G. Mutually responsive orientation between mothers and their young children: a context for the early development of conscience. Curr Direct Psychol Sci. 2002;11(6):191–195. doi:10.1111/1467-8721.00198
22. McCauley TG, McCullough ME. Retrospective self-reported childhood experiences in enriched environments uniquely predict prosocial behavior and personality traits in adulthood. Evolution Psychol. 2022;20(3):14747049221110603. doi:10.1177/14747049221110603
23. Conway P, Gawronski B. Deontological and utilitarian inclinations in moral decision making: a process dissociation approach. J Personal Soc Psychol. 2013;104(2):216–235. doi:10.1037/a0031021
24. Luke DM, Neumann CS, Gawronski B. Psychopathy and moral-dilemma judgment: an analysis using the four-factor model of psychopathy and the CNI model of moral decision-making. Clin Psychol Sci. 2022;10(3):553–569. doi:10.1177/21677026211043862
25. Crone DL, Laham SM. Utilitarian preferences or action preferences? De-confounding action and moral code in sacrificial dilemmas. Pers Individ Dif. 2017;104:476–481. doi:10.1016/j.paid.2016.09.022
26. Gawronski B, Armstrong J, Conway P, Friesdorf R, Hütter M. Consequences, norms, and generalized inaction in moral dilemmas: the CNI model of moral decision-making. J Personal Soc Psychol. 2017;113(3):343–376. doi:10.1037/pspa0000086
27. Gawronski B, Beer JS. What makes moral dilemma judgments “utilitarian” or “deontological”? Soc Neurosci. 2017;12(6):626–632. doi:10.1080/17470919.2016.1248787
28. Gawronski B, Conway P, Armstrong J, Friesdorf R, Hütter M. Effects of incidental emotions on moral dilemma judgments: an analysis using the CNI model. Emotion. 2018;18(7):989–1008. doi:10.1037/emo0000399
29. Chen X, Wu Z, Zhan B, Ding D, Zhang X. Effects of alexithymia on moral decision-making in sacrificial dilemmas: high alexithymia is associated with weaker sensitivity to moral norms. Psychol Res Behav Manage. 2023;2315–2325. doi:10.2147/PRBM.S407744
30. Cerqueira A, Almeida TC. Adverse childhood experiences: relationship with empathy and alexithymia. J Child Adol Trauma. 2023;2:1–10.
31. Yu Z, Wang L, Chen W, Perrin N, Gross D. Childhood adversity and mental health among Chinese young adults: the protective role of resilience. J Adv Nurs. 2021;77(12):4793–4804. doi:10.1111/jan.15070
32. Faul F, Erdfelder E, Lang A-G, Buchner A. G* Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–191. doi:10.3758/BF03193146
33. Qin X, Ma-Xia D, Jie Y, Wen-Xian L, Parental Alcoholism D-QY. adverse childhood experiences, and later risk of personal alcohol abuse among Chinese medical students. Biomed Environ Sci. 2008;21(5):411–419. doi:10.1016/S0895-3988(08)60062-8
34. Li Z, Xia S, Wu X, Chen Z. Analytical thinking style leads to more utilitarian moral judgments: an exploration with a process-dissociation approach. Pers Individ Dif. 2018;131:180–184. doi:10.1016/j.paid.2018.04.046
35. Poole JC, Dobson KS, Pusch D. Anxiety among adults with a history of childhood adversity: psychological resilience moderates the indirect effect of emotion dysregulation. J Affective Disorders. 2017;217:144–152. doi:10.1016/j.jad.2017.03.047
36. Poole JC, Dobson KS, Pusch D. Do adverse childhood experiences predict adult interpersonal difficulties? The role of emotion dysregulation. Child Abuse Negl. 2018;80:123–133. doi:10.1016/j.chiabu.2018.03.006
37. Wang X, Yang J, Wang P, Lei L. Childhood maltreatment, moral disengagement, and adolescents’ cyberbullying perpetration: fathers’ and mothers’ moral disengagement as moderators. Computers Human Behav. 2019;95:48–57. doi:10.1016/j.chb.2019.01.031
38. Stogsdill S The impact of childhood abuse on moral development; 2019.
39. Fang J, Wang X, Yuan K-H, Wen Z. Childhood psychological maltreatment and moral disengagement: a moderated mediation model of callous-unemotional traits and empathy. Pers Individ Dif. 2020;157:109814. doi:10.1016/j.paid.2020.109814
40. Struck S, Stewart-Tufescu A, Asmundson AJN, Asmundson GGJ, Afifi TO. Adverse childhood experiences (ACEs) research: a bibliometric analysis of publication trends over the first 20 years. Child Abuse Negl. 2021;112:104895. doi:10.1016/j.chiabu.2020.104895
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.