")
Back to Journals » International Journal of Women's Health » Volume 16
Disparities in Survival Outcomes Between Locally Advanced Cervical Squamous Cell Carcinoma and Adenocarcinoma Treated with Chemoradiotherapy
Authors Hong SS, Li Y, Lin YY, Wu SG , Chen LY, Zhou J
Received 29 November 2023
Accepted for publication 25 February 2024
Published 6 March 2024 Volume 2024:16 Pages 401—410
DOI https://doi.org/10.2147/IJWH.S450457
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Shan-Shan Hong,1,* Yang Li,2,* Yu-Yi Lin,3 San-Gang Wu,4 Li-Ying Chen,1 Juan Zhou5
1Department of Obstetrics and Gynecology, Quanzhou Women’s and Children’s Hospital, Quanzhou, 362000, People’s Republic of China; 2School of Basic Medical Sciences, Fujian Medical University, Fuzhou, 350122, People’s Republic of China; 3Department of Radiation Oncology, the Second Affiliated Hospital of Xiamen Medical College, Xiamen, 361021, People’s Republic of China; 4Department of Radiation Oncology, Xiamen Cancer Center, Xiamen Key Laboratory of Radiation Oncology, the First Affiliated Hospital of Xiamen University, School of Medicine, Xiamen University, Xiamen, 361003, People’s Republic of China; 5Department of Obstetrics and Gynecology, the First Affiliated Hospital of Xiamen University, School of Medicine, Xiamen University, Xiamen, 361003, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Li-Ying Chen, Department of Obstetrics and Gynecology, Quanzhou Women’s and Children’s Hospital, Quanzhou, 362000, People’s Republic of China, Email [email protected] Juan Zhou, Department of Obstetrics and Gynecology, the First Affiliated Hospital of Xiamen University, School of Medicine, Xiamen University, Xiamen, 361003, People’s Republic of China, Email [email protected]
Purpose: To determine the disparities in survival outcomes between stage IIB-IVA cervical squamous cell carcinoma (SCC) and adenocarcinoma (AC) treated with chemoradiotherapy.
Methods: Patients diagnosed between 2004 and 2015 were retrospectively included from the Surveillance, Epidemiology, and End Results databases. Propensity score matching (PSM) was used in this study. The primary endpoints were cervical cancer-specific survival (CCSS) and overall survival (OS).
Results: A total of 2752 patients were identified, including 87.5% (n=2408) were SCC and 12.5% (n=344) were AC. Patients with AC had inferior 5-year CCSS (67.5% vs 54.8%, P< 0.001) and OS (58.4% vs 47.2%, P< 0.001) compared to those with the SCC subtype. The hazard curve of cervical cancer-related death in AC peaked at 2 years (19%) and still small peaks in the 7 and 11 years of follow-up. Regarding SCC, cervical cancer-related deaths peaked at 2 years (15%) and the hazard rate was 2.0% during the six years of follow-up. The multivariate Cox regression analyses indicated that histology was an independent prognostic factor associated with survival outcomes. Patients with AC had significantly poor CCSS (P< 0.001) and OS (P< 0.001). Similar results were found after PSM.
Conclusion: Our study demonstrates a significantly better prognosis for cervical SCC patients compared to those with cervical AC undergoing chemoradiotherapy. These results highlight the importance of histological subtyping in predicting treatment outcomes and tailoring therapeutic strategies.
Keywords: cervical cancer, squamous cell carcinoma, adenocarcinoma, chemotherapy, radiotherapy, hazard curve
Background
Cervical cancer (CC) represents an important global health issue and remains the main cause of cancer-related deaths in women. There are approximately 604,217 new cases of CC worldwide annually, including 111,820 cases in China.1,2 It is a heterogeneous disease that can be classified into various histological subtypes, with the most common being squamous cell carcinoma (SCC) (70%), followed by adenocarcinoma (AC) (10–25%).3–5 SCC originates from the squamous epithelium of the cervix, while AC arises from the glandular cells. Tumors containing glandular elements are associated with resistance to radiotherapy and poorer survival outcomes.6,7 In those receiving definitive radiotherapy or postoperative radiotherapy, several studies have shown AC patients had a higher risk of pelvic recurrence and a lower survival outcome than those in the SCC group both in early- and locally advanced-stage CC.8,9 Moreover, several studies also have highlighted the distinct biological characteristics of cervical AC and SCC, suggesting potential variations in growth patterns, response to therapies, and likelihood of metastasis.10–13 These findings indicated that the clinical behavior of the tumor cells and the effectiveness of radiotherapy may be different between SCC and AC.
In the current treatment guidelines for stage IIB-IVA CC, concurrent chemoradiotherapy (CCRT) is a widely accepted treatment approach for this patient setting and the recommended treatment strategies for SCC are similar to those with AC.14–16 In our previous study, we found that the survival of the cervical AC who received definitive radiotherapy had an inferior prognosis compared to those with SCC.17 However, the information regarding chemotherapy was not included in the analysis.17 Therefore, it is essential to investigate if there are any survival differences between SCC and AC of the cervix when subjected to chemoradiotherapy. In light of this, this study aimed to investigate the differential clinical outcomes of patients with locally advanced cervical AC and SCC who received chemoradiotherapy. This knowledge could inform personalized treatment decisions and contribute to improved management strategies for CC patients.
Materials and Methods
Patients
Patients diagnosed with CC from 2004 to 2015 were retrospectively included using the Surveillance, Epidemiology, and End Results (SEER) database.18 The SEER Research Plus Data contains population-based data from 18 cancer registries covering approximately 27.8% of the United States population. This dataset provides information regarding demographics, tumor characteristics, treatment, and follow-up of the patients. We have obtained permission to access the SEER database with the approval number 21354-Nov2021. We included patients who met the following inclusion criteria: 1) patients who were diagnosed with stage IIB-IVA cervical SCC or AC; 2) patients who received definitive radiotherapy and chemotherapy. Patients who had non-positive pathological diagnoses or who did not receive implants or isotopes irradiation were excluded from this study. This study was approved by the Ethics Committee of the First Affiliated Hospital of Xiamen University (approval number 2022J011379).
Measures
The following demographic and clinicopathological variables were included in the analysis: age, race, histological subtypes, grade, and Federation of International of Gynecologists and Obstetricians (FIGO) stage. The FIGO staging was based on the sixth edition of the American Joint Committee on Cancer tumor node metastasis (TNM) classification staging. Before 2018, the FIGO staging and TNM staging for the same patient with CC were identical. The primary endpoints were cervical cancer-specific survival (CCSS) and overall survival (OS).
Statistical Analysis
Categorical variables were compared by the Chi-square tests. The Kaplan–Meier method with the Log rank test was performed to compare the CCSS and OS. The life-table method was conducted to estimate the annual CC-related death hazard rate. We used propensity score matching (PSM) to minimize selection bias including the following variables: age, race, tumor grade, and FIGO stage. Multivariate Cox regression analyses were performed to determine the independent prognostic factors associated with survival outcomes. Sensitivity analyses were performed to determine the impact of histology on survival outcomes after stratification by age, race, tumor grade, and FIGO stage. All statistical analyses were performed using the SPSS statistical software package (version 26.0; IBM Corporation, Armonk, NY, USA). A P-value of <0.05 was considered statistically significant.
Results
Patient Baseline Characteristics
A total of 2752 patients were included in this study (Figure 1), including 87.5% (n=2408) of SCC and 12.5% (n=344) of AC (Table 1). The median age at CC diagnosis was 52 years (range, 19–91 years). Patients with the AC subtype were more likely to be older age (P=0.001), white race (P=0.019), and well-differentiated disease (P=0.001). The mean age was 52.2 years and 55.4 years in patients with SCC and AC, respectively (P<0.001). A total of 340 pairs of patients were completely matched using PSM (Table 1).
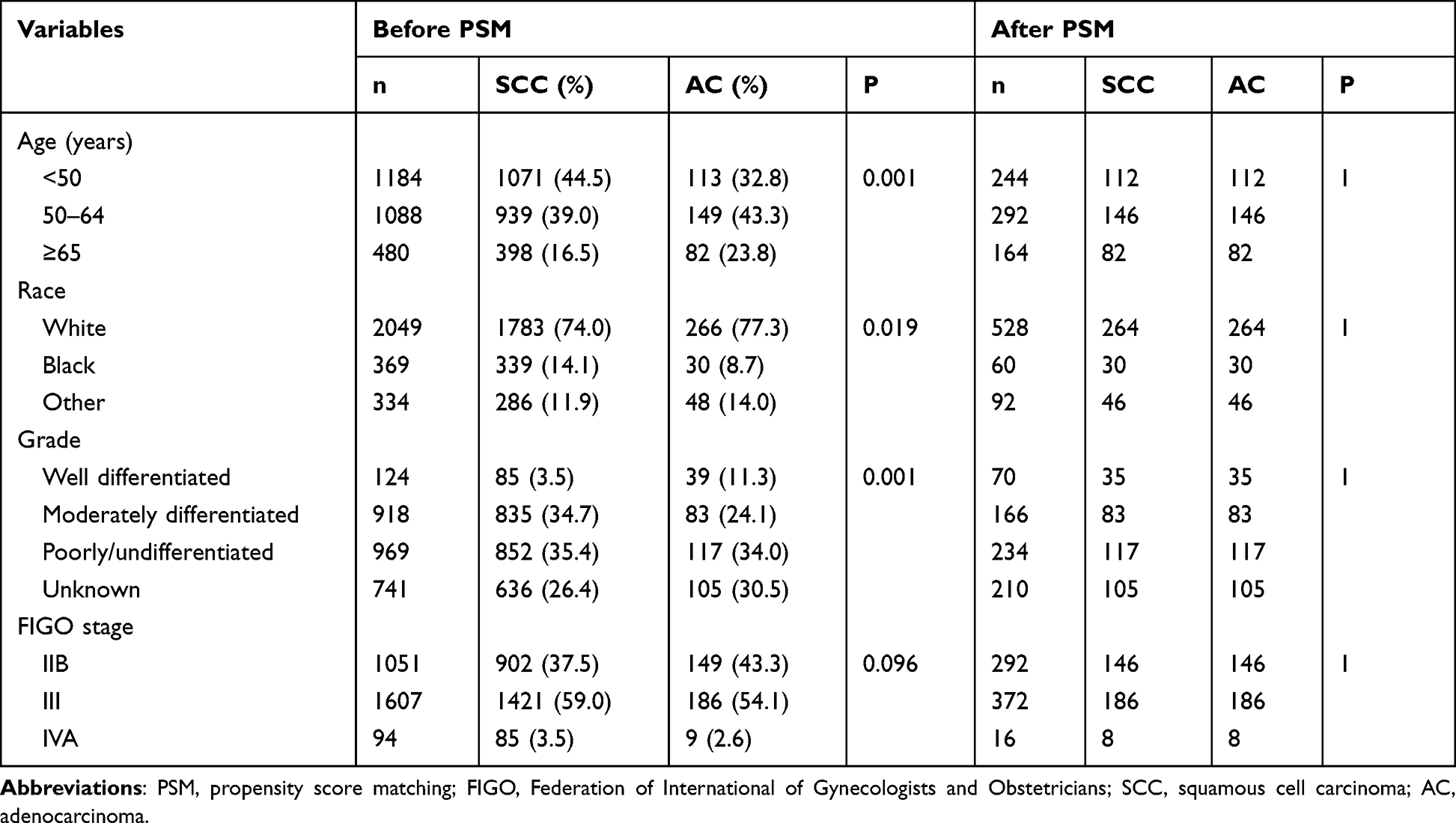 |
Table 1 Patient Baseline Characteristics Before and After Propensity Score Matching |
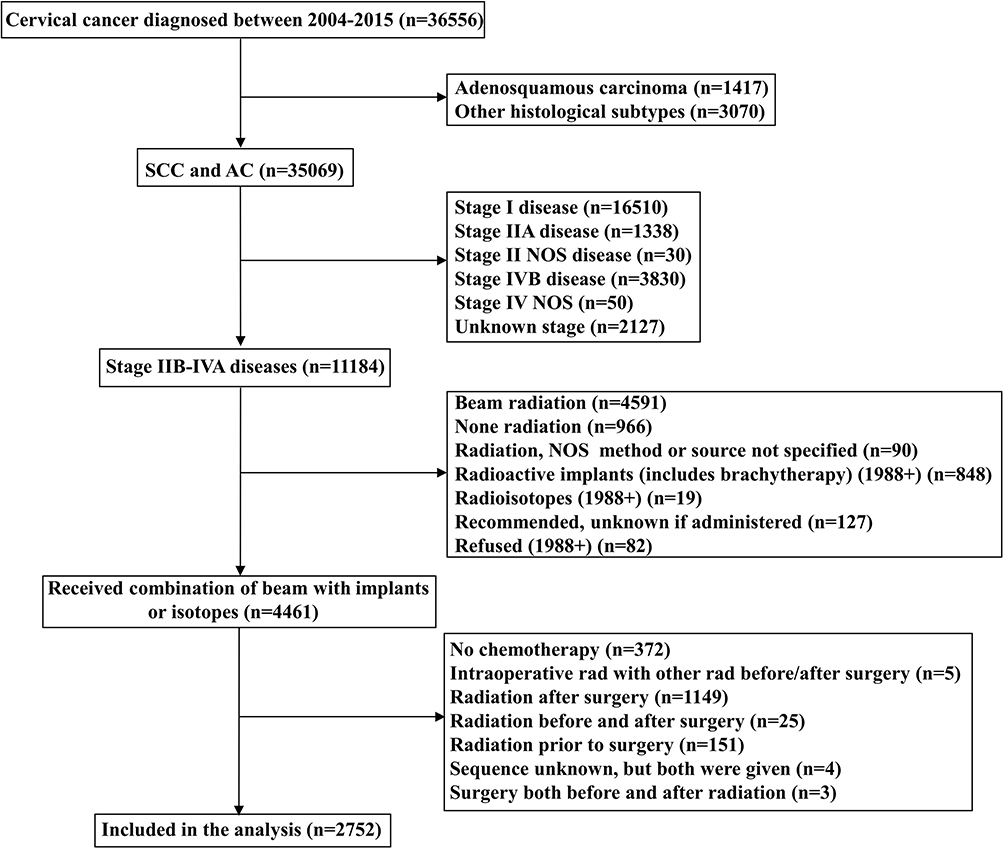 |
Figure 1 The patient selection flowchart. Abbreviations: NOS, no other specific; SCC, squamous cell carcinoma; AC, adenocarcinoma. |
Survival Analyses
The median follow-up was 56 months (range, 2–191 months). A total of 1376 patients died, including 791 from SCC and 163 from AC. The 5-year CCSS and OS were 65.9% and 57.3% in the entire cohort. Patients with AC had inferior CCSS (5-years: 67.5% vs 54.8%, P<0.001) (Figure 2A) and OS (5-years: 58.4% vs 47.2%, P<0.001) (Figure 2B) compared to those with SCC subtype. Similar results were found after PSM (Figure 3A and B).
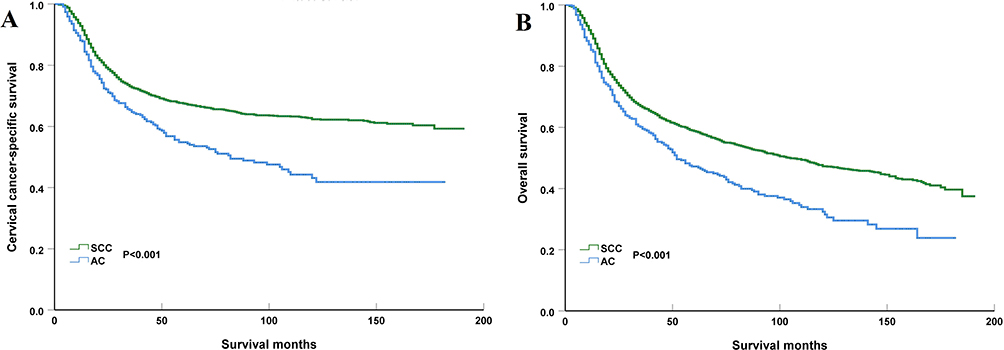 |
Figure 2 Comparison of cause-specific survival (A) and overall survival (B) between cervical squamous cell carcinoma (SCC) and adenocarcinoma (AC) before propensity score matching. |
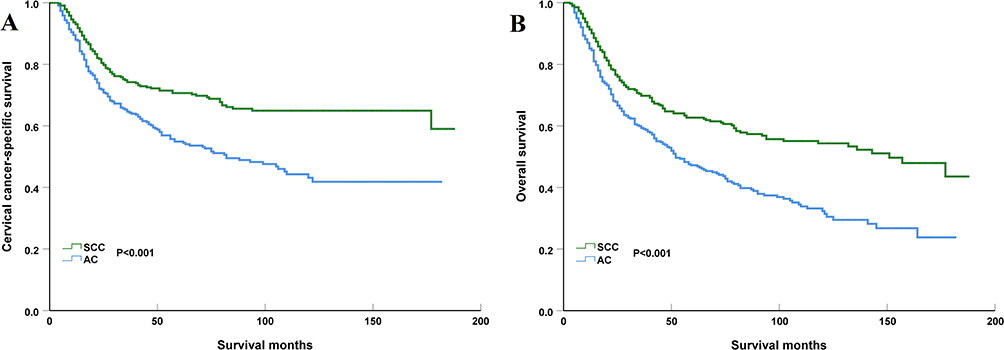 |
Figure 3 Comparison of cause-specific survival (A) and overall survival (B) between cervical squamous cell carcinoma (SCC) and adenocarcinoma (AC) after propensity score matching. |
Hazard Function
There were significant differences in hazard function between SCC and AC. The hazard curve of CC-related death in AC peaked at 2 years (19%) but then slowly decreased over time. However, there were still small peaks in the 7 and 11 years of follow-up and the risk of death reached 0 in the 12th year. Regarding SCC, the CC-related deaths peaked at 2 years (15%), and then slowly decreased over time, where the hazard rate was 2.0% during the six years of follow-up. Figure 4 lists the hazard curve of CC-related deaths by specific histological subtypes.
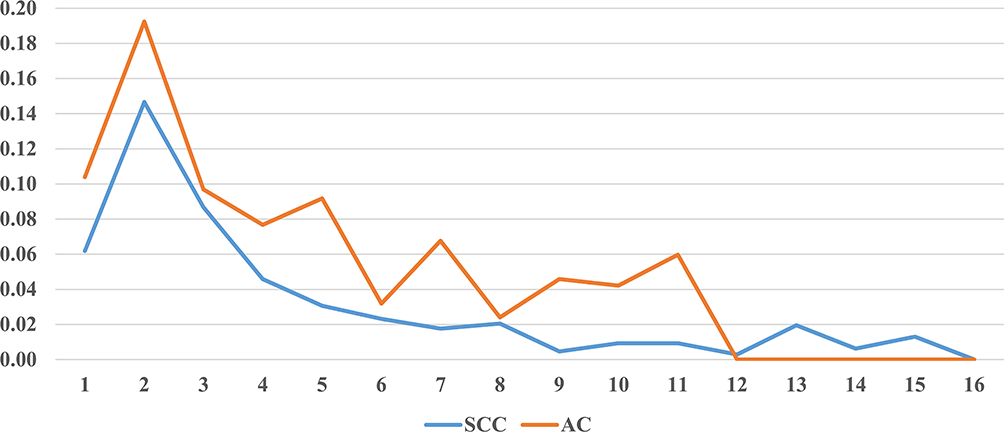 |
Figure 4 Annual hazard rates for cervical cancer-related death between cervical squamous cell carcinoma (SCC) and adenocarcinoma (AC) (the horizontal axis refers to the year of follow-up; the vertical axis refers to annual hazard rates). |
Prognostic Analyses
We performed Multivariate Cox regression analyses to determine the independent prognostic factors related to CCSS and OS (Table 2). The results showed that histology was an independent prognostic factor associated with survival outcomes. Patients with AC had significantly poor CCSS (hazard ratio [HR] 1.683, 95% confidence interval [CI] 1.417–1.999, P<0.001) and OS (HR 1.486, 95% CI 1.279–1.727, P<0.001). Using sensitivity analysis, we also found that those with AC had inferior CCSS and OS compared to those with SCC after stratification by age, race, tumor grade, and FIGO stage (Table 3). Age and FIGO stage were also independent prognostic factors related to survival outcomes. We also found that patients with AC had significantly poor CCSS (HR 1.755, 95% CI 1.370–2.248, P<0.001) and OS (HR 1.759, 95% CI 1.421–2.178, P<0.001) after PSM (Table 4).
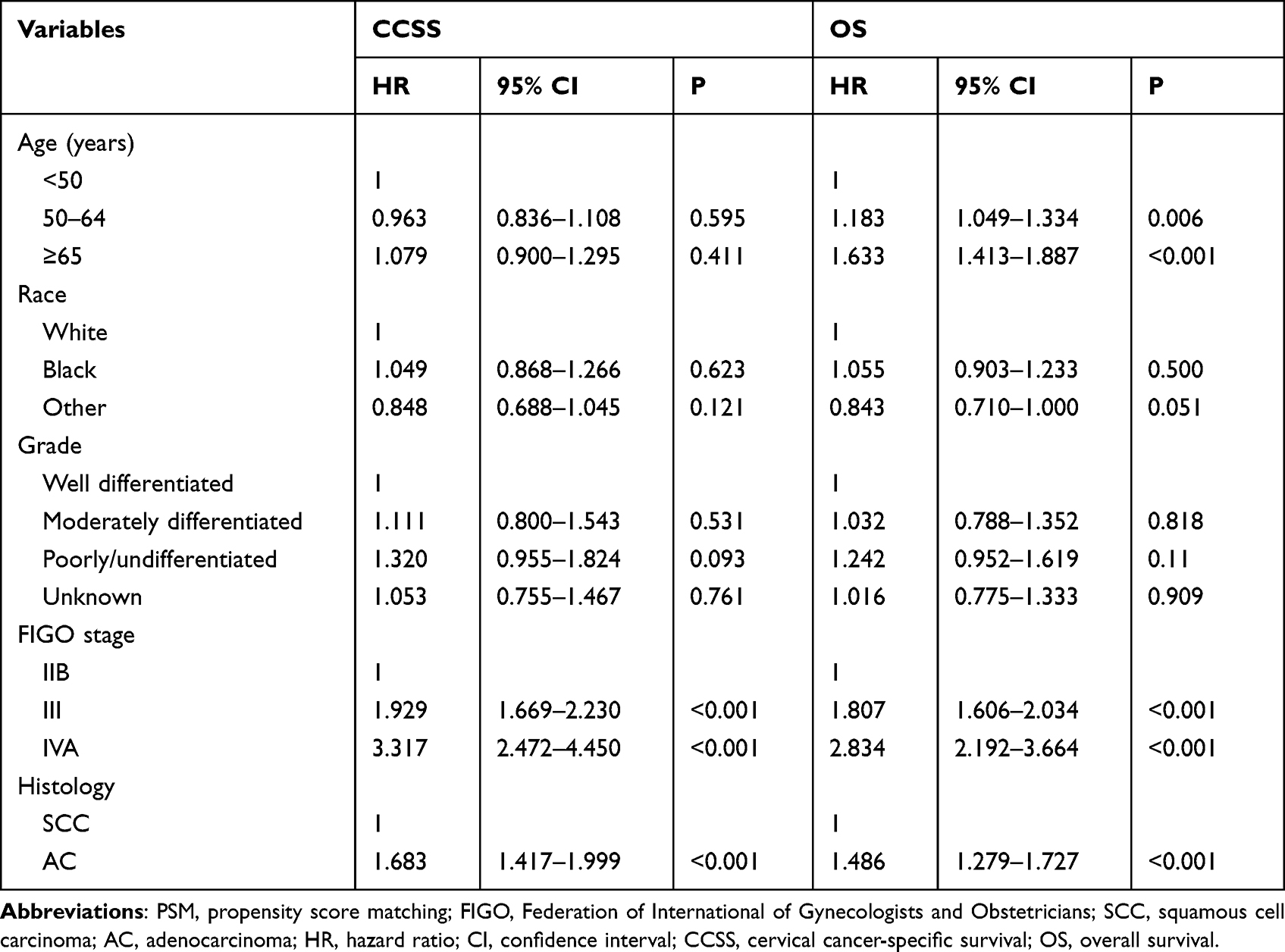 |
Table 2 Multivariate Prognostic Analysis for Independent Prognostic Factors Associated with Cervical Cancer-Specific Survival and Overall Survival Before Propensity Score Matching |
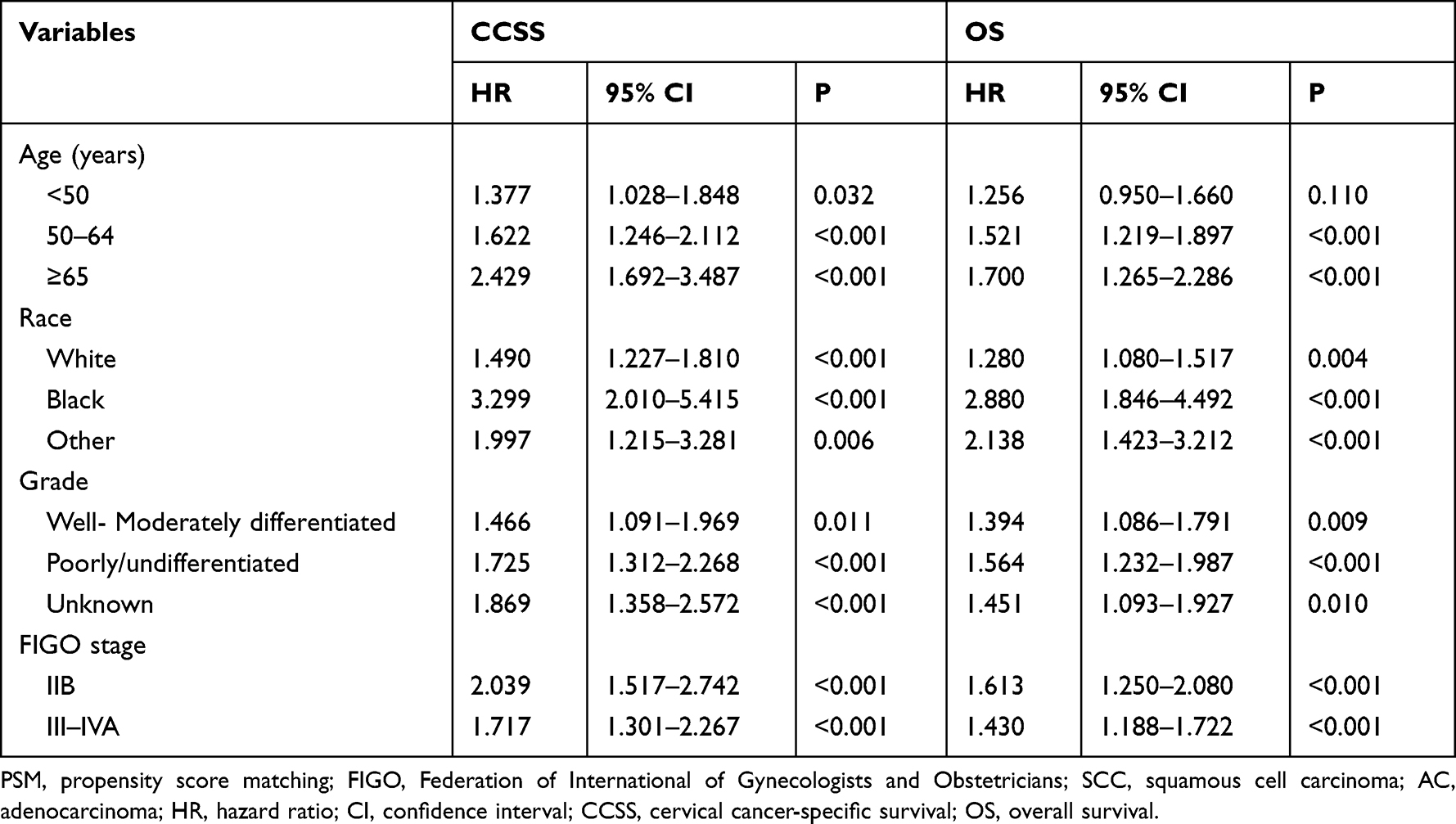 |
Table 3 Sensitivity Analysis of the Impact of Histology (Adenocarcinoma vs Squamous Cell Carcinoma) on Cervical Cancer-Specific Survival and Overall Survival After Stratification by Age, Race, Tumor Grade, and FIGO Stage |
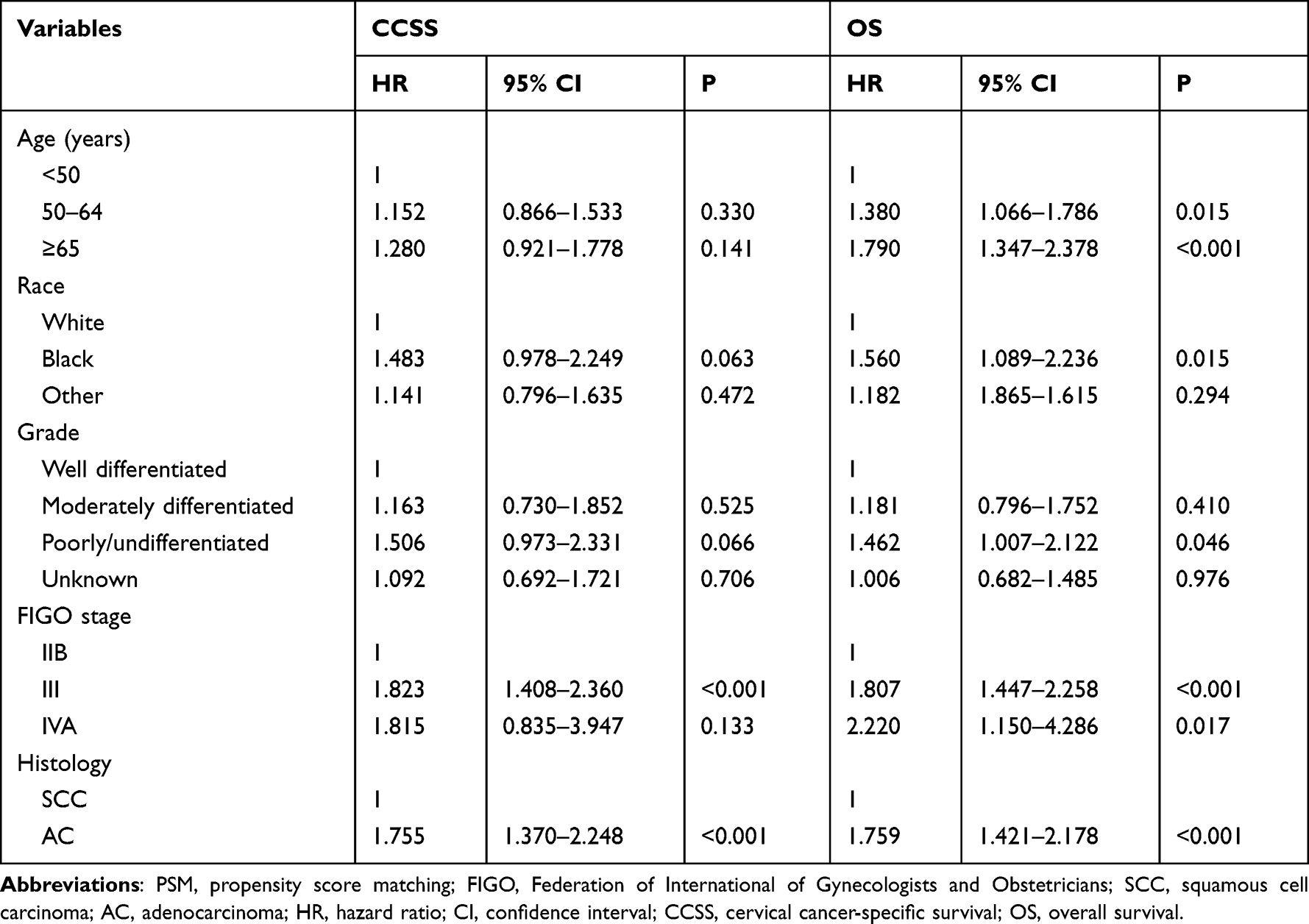 |
Table 4 Multivariate Prognostic Analysis for Independent Prognostic Factors Associated with Cervical Cancer-Specific Survival and Overall Survival After Propensity Score Matching |
Discussion
In this study, we used a population-based cohort to investigate the effect of histology on survival outcomes in stage IIB-IVA CC patients who received chemoradiotherapy. We found significant differences in the patterns of hazard function between SCC and AC. In addition, patients with cervical AC had inferior survival outcomes compared to those with SCC. Our study highlighted the importance of histological subtyping in predicting treatment outcomes and determining optimal therapeutic strategies.
There were conflicting results regarding age distribution between SCC and AC of the cervix. Several small sample size studies have found that the age distribution of SCC and AC was similar.9,19,20 Moreover, two recent population-based studies showed that patients with AC were more likely to be diagnosed at a young age.21,22 However, our study found that women with AC are more likely to be older compared to those with SCC (the mean age was 52.2 years in SCC and 55.4 years in AC, P<0.001). It is necessary to elaborate on the differences in age distribution between the two histological subtypes. The study by the National Cancer Database showed that AC patients of older age were less likely to be diagnosed with early-stage disease compared to those with SCC.22 Therefore, the impact of CC screening may play an important role in the difference in age distribution between SCC and AC. Moreover, this age disparity may be also attributed to differences in the cell of origin and the pathogenesis of these subtypes. It is well-known that SCC is strongly associated with human papillomavirus (HPV) infection (95%) and affects younger individuals. However, the percentage of HPV-negative disease was found in approximately 20–30% of patients with cervical AC.23–25
The predominance of well-differentiated tumors in AC patients compared to SCC patients was another interesting finding in our study, which was similar to several previous studies including ours.26,27 Well-differentiated tumors are typically associated with a lower grade, implying a lower histological abnormality and a closer resemblance to the tissue of origin. In contrast, SCC is often associated with moderate to poorly differentiated tumors, which exhibit more severe cellular abnormalities. This histological difference may reflect variations in the pathogenesis, genetic alterations, and molecular profiles between the subtypes, potentially influencing tumor behavior, treatment response, and prognosis.10–13 However, the AC subtype can be further subclassified into 12 different subtypes according to the International Endocervical Adenocarcinoma Criteria and Classification system after stratification by tumor morphology, HPV status, and a panel of immunohistochemical markers.28 This adds complexity to our understanding of AC and its biology and outcome to treatment. Therefore, it is crucial to comprehend the molecular factors, linkage with HPV, tumor characteristics, and epidemiological implications for proper treatment and prediction of outcomes.
In our entire cohort, the hazard curve for CC-related death between SCC and AC exhibited a distinct pattern. The curve of CC-related death in AC peaked at 2 years, with an alarming 19% mortality rate. However, the risk of death gradually decreased over time. Notably, there were also small peaks observed in the 7th and 11th years of follow-up. Despite these intermittent peaks, the risk of death eventually reached 0 in the 12th year. Regarding SCC, the peak of mortality, occurring at 2 years, was slightly lower at 15% compared to AC. Similarly, the risk of death gradually declined over time. It is noteworthy that the hazard rate during the six years of follow-up for SCC patients was 2.0%, indicating a relatively lower risk compared to AC patients. This observation suggested that patients with AC face the highest risk of mortality during the early years of diagnosis, with a subsequent decrease in death rates over time. These findings underscore the importance of recognizing and understanding the differences in survival outcomes between SCC and AC of the cervix. The peak in CC-related death occurring at 3 years for both histological types calls for heightened vigilance, potentially warranting more aggressive treatment options or closer monitoring during this period. In addition, long-term follow-up is also required for cervical AC.
Our study demonstrated an inferior CCSS and OS in patients with AC than in those with SCC, which was similar to previous studies.19,29,30 The observed disparity in prognosis may be attributed to several factors. First, the distinct biological characteristics of SCC and AC might contribute to differential prognosis. The study by Hu et al found that the risk of patients with para-aortic metastatic lymph nodes was significantly higher in AC compared to those with SCC (14.1% vs 5.9%, P=0.008).19 In addition, a previous study included 30 patients with AC receiving CCRT, 13 patients and 15 patients developed local recurrence and distant recurrence, respectively.31 The above results showed that AC is a more aggressive disease phenotype compared to SCC. Secondly, the intrinsic radioresistance exhibited by AC compared to SCC might play a role in the differential outcomes. Previous studies have reported that AC tumors tend to have lower radiosensitivity and are associated with decreased response rates to radiotherapy. A previous study from Japan showed that the response to treatment after definitive CCRT was 88.9%, 8.9%, and 1.3% with complete response (CR), partial response, and stable disease in SCC, and 66.7%, 20.8%, and 12.5% in AC/adenosquamous carcinoma.9 In addition, adjuvant hysterectomy was performed more frequently in AC/adenosquamous carcinoma patients than in SCC patients. Several studies also showed that those with AC had lower CR and local control rates and required a longer time to achieve CR compared to those with SCC after definitive radiotherapy or CCRT.9,19,32 Moreover, the discrepancy in prognosis between SCC and AC could also be influenced by the presence of underlying molecular alterations. Recent research has identified different molecular profiles in SCC and AC, including distinct patterns of gene mutations and altered expression of key molecules involved in tumor growth and response to therapy.10–13 These molecular differences may contribute to variations in treatment response, metastatic potential, and overall survival rates observed between the two subtypes.
While our study highlights the significant difference in prognosis between SCC and AC patients undergoing CCRT, some limitations should be acknowledged. Firstly, inherent biases are unavoidable in any retrospective study, including issues related to data completeness and accuracy, the extended duration of data collection, and the potential changes in treatment and diagnostic methods throughout the study period. In this study, we collected the database based on a population-based database and further employed PSM to reduce potential selection bias. Secondly, the population in our study was from the United States, potentially limiting the generalizability of the general population worldwide. However, several studies from China, Japan, and Korea have also found that survival rates in patients with AC receiving definitive radiotherapy were significantly lower than those with the SCC subtype.9,9,19,30 Moreover, other confounding variables, such as performance status and comorbidities, were not included in our analysis.
Conclusions
In conclusion, our study demonstrates a significantly better prognosis for cervical SCC patients compared to those with cervical AC undergoing chemoradiotherapy. These results highlight the importance of histological subtyping in predicting treatment outcomes and tailoring therapeutic strategies. Future research should focus on elucidating the underlying molecular mechanisms, improving treatment approaches, and addressing healthcare disparities to further enhance outcomes in CC patients by different histological subtypes.
Data Sharing Statement
This database is from a publicly available SEER database (https://seer.cancer.gov/seerstat/databases/oncotype-dx/index.html). The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Acknowledgments
This work was partly supported by grants from the Natural Science Foundation of Fujian Province (No. 2022J011379) and the Commission Young and Middle-aged Talents Training Project of Fujian Health Commission (No. 2021GGB027).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was partly supported by grants from the Natural Science Foundation of Fujian Province (No. 2022J011379) and the Commission Young and Middle-aged Talents Training Project of Fujian Health Commission (No. 2021GGB027).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Singh D, Vignat J, Lorenzoni V, et al. Global estimates of incidence and mortality of cervical cancer in 2020: a baseline analysis of the WHO Global Cervical Cancer Elimination Initiative. Lancet Glob Health. 2023;11(2):e197–e206. doi:10.1016/S2214-109X(22)00501-0
2. Xia C, Dong X, Li H, et al. Cancer statistics in China and the United States, 2022: profiles, trends, and determinants. Chin Med J. 2022;135(5):584–590. doi:10.1097/CM9.0000000000002108
3. Fujiwara K, Monk B, Devouassoux-Shisheboran M. Adenocarcinoma of the uterine cervix: why is it different? Curr Oncol Rep. 2014;16(12):416.
4. Gadducci A, Guerrieri ME, Cosio S. Adenocarcinoma of the uterine cervix: pathologic features, treatment options, clinical outcome and prognostic variables. Crit Rev Oncol Hematol. 2019;135:103–114. doi:10.1016/j.critrevonc.2019.01.006
5. Shoji T, Takatori E, Saito T, et al. Neoadjuvant chemotherapy using platinum- and taxane-based regimens for bulky stage Ib2 to IIb non-squamous cell carcinoma of the uterine cervix. Cancer Chemother Pharmacol. 2013;71(3):657–662. doi:10.1007/s00280-012-2052-2
6. Okada S, Tsuda H, Ohmi K, et al. Immature glandular features in squamous cell carcinoma of the uterine cervix as an independent indicator of resistance to radiotherapy. Int J Gynecol Cancer. 2002;12(3):277–285. doi:10.1136/ijgc-00009577-200205000-00007
7. Davy ML, Dodd TJ, Luke CG, Roder DM. Cervical cancer: effect of glandular cell type on prognosis, treatment, and survival. Obstet Gynecol. 2003;101(1):38–45. doi:10.1016/s0029-7844(02)02275-5
8. Shimada M, Nishimura R, Nogawa T, et al. Comparison of the outcome between cervical adenocarcinoma and squamous cell carcinoma patients with adjuvant radiotherapy following radical surgery: SGSG/TGCU Intergroup Surveillance. Mol Clin Oncol. 2013;1(4):780–784. doi:10.3892/mco.2013.112
9. Yokoi E, Mabuchi S, Takahashi R, et al. Impact of histological subtype on survival in patients with locally advanced cervical cancer that were treated with definitive radiotherapy: adenocarcinoma/adenosquamous carcinoma versus squamous cell carcinoma. J Gynecol Oncol. 2017;28(2):e19. doi:10.3802/jgo.2017.28.e19
10. Li J, Xue X, Zhang Y, et al. The differences in immune features and genomic profiling between squamous cell carcinoma and adenocarcinoma - A multi-center study in Chinese patients with uterine cervical cancer. Gynecol Oncol. 2023;175:133–141. doi:10.1016/j.ygyno.2023.05.071
11. Nicolás-Párraga S, Alemany L, de Sanjosé S, Bosch FX, Bravo IG; RIS HPV TT and HPV VVAP study groups. Differential HPV16 variant distribution in squamous cell carcinoma, adenocarcinoma and adenosquamous cell carcinoma. Int J Cancer. 2017;140(9):2092–2100. doi:10.1002/ijc.30636
12. Stolnicu S, Hoang L, Soslow RA. Recent advances in invasive adenocarcinoma of the cervix. Virchows Arch. 2019;475(5):537–549. doi:10.1007/s00428-019-02601-0
13. Wright AA, Howitt BE, Myers AP, et al. Oncogenic mutations in cervical cancer: genomic differences between adenocarcinomas and squamous cell carcinomas of the cervix. Cancer. 2013;119(21):3776–3783. doi:10.1002/cncr.28288
14. de Juan A, Redondo A, Rubio MJ, et al. SEOM clinical guidelines for cervical cancer (2019). Clin Transl Oncol. 2020;22(2):270–278. doi:10.1007/s12094-019-02271-z
15. Fujiwara H, Yokota H, Monk B, et al. Gynecologic Cancer InterGroup (GCIG) consensus review for cervical adenocarcinoma. Int J Gynecol Cancer. 2014;24(9 Suppl 3):S96–S101. doi:10.1097/IGC.0000000000000263
16. National Comprehensive Cancer Network (NCCN). Clinical practice guidelines in oncology. Cervical Cancer 2023. Version 1. Available from: https://www.nccn.org/professionals/physician_gls/pdf/cervical.pdf.
17. Zhou J, Wu SG, Sun JY, et al. Comparison of clinical outcomes of squamous cell carcinoma, adenocarcinoma, and adenosquamous carcinoma of the uterine cervix after definitive radiotherapy: a population-based analysis. J Cancer Res Clin Oncol. 2017;143(1):115–122. doi:10.1007/s00432-016-2246-9
18. Surveillance, Epidemiology, and End Results (SEER) Program. SEER*Stat Database: Incidence - SEER Research Plus Data, 18 Registries, Nov 2020 Sub (2000–2018) - Linked To County Attributes - Total U.S., 1969–2019 Counties, National Cancer Institute, DCCPS, Surveillance Research Program, released April 2021, based on the November 2020 submission. Available from: www.seer.cancer.gov.
19. Hu K, Wang W, Liu X, Meng Q, Zhang F. Comparison of treatment outcomes between squamous cell carcinoma and adenocarcinoma of cervix after definitive radiotherapy or concurrent chemoradiotherapy. Radiat Oncol. 2018;13(1):249. doi:10.1186/s13014-018-1197-5
20. Rose PG, Java JJ, Whitney CW, Stehman FB, Lanciano R, Thomas GM. Locally advanced adenocarcinoma and adenosquamous carcinomas of the cervix compared to squamous cell carcinomas of the cervix in gynecologic oncology group trials of cisplatin-based chemoradiation. Gynecol Oncol. 2014;135(2):208–212. doi:10.1016/j.ygyno.2014.08.018
21. Suh DH, Ha HI, Lee YJ, Lim J, Won YJ, Lim MC. Incidence and treatment outcomes of uterine cervical cancer in Korea 1999–2018 from the national cancer registry. J Gynecol Oncol. 2023;34(2):e39. doi:10.3802/jgo.2023.34.e39
22. Smith AJB, Beavis AL, Rositch AF, Levinson K. Disparities in diagnosis and treatment of cervical adenocarcinoma compared with squamous cell carcinoma: an analysis of the National Cancer Database, 2004–2017. J Low Genit Tract Dis. 2023;27(1):29–34. doi:10.1097/LGT.0000000000000702
23. Molijn A, Jenkins D, Chen W, et al. The complex relationship between human papillomavirus and cervical adenocarcinoma. Int J Cancer. 2016;138(2):409–416. doi:10.1002/ijc.29722
24. Jenkins D, Molijn A, Kazem S, et al. Molecular and pathological basis of HPV-negative cervical adenocarcinoma seen in a global study. Int J Cancer. 2020;147(9):2526–2536. doi:10.1002/ijc.33124
25. Chen W, Molijn A, Enqi W, et al. The variable clinicopathological categories and role of human papillomavirus in cervical adenocarcinoma: a hospital based nation-wide multi-center retrospective study across China. Int J Cancer. 2016;139(12):2687–2697. doi:10.1002/ijc.30401
26. Wu SG, Sun JY, He ZY, Chen QH, Zhou J. Early-stage node negative cervical adenocarcinoma and squamous cell carcinoma show similar survival outcomes after hysterectomy: a population-based study. J Gynecol Oncol. 2017;28(6):e81. doi:10.3802/jgo.2017.28.e81
27. Meng Y, Chu T, Lin S, et al. Clinicopathological characteristics and prognosis of cervical cancer with different histological types: a population-based cohort study. Gynecol Oncol. 2021;163(3):545–551. doi:10.1016/j.ygyno.2021.10.007
28. Stolnicu S, Barsan I, Hoang L, et al. International Endocervical Adenocarcinoma Criteria and Classification (IECC): a New Pathogenetic Classification for Invasive Adenocarcinomas of the Endocervix. Am J Surg Pathol. 2018;42(2):214–226. doi:10.1097/PAS.0000000000000986
29. Hsieh HY, Lu CH, Wang L. Long-term treatment outcomes/toxicities of definite chemoradiotherapy (intensity-modulated radiation therapy) for early-stage ”bulky” cervical cancer and survival impact of histological subtype. J Formos Med Assoc. 2023;122(3):221–229. doi:10.1016/j.jfma.2022.10.012
30. Kang JH, Cho WK, Yeo HJ, et al. Prognostic significance of tumor regression rate during concurrent chemoradiotherapy in locally advanced cervix cancer: analysis by radiation phase and histologic type. J Clin Med. 2020;9(11):3471. doi:10.3390/jcm9113471
31. Arakaki Y, Ariga T, Heianna J, et al. Long-term outcomes of cervical adenocarcinoma treated with concurrent chemoradiotherapy using paclitaxel and cisplatin. In Vivo. 2020;34(5):2739–2743. doi:10.21873/invivo.12096
32. Xiong Y, Liu J, Chen S, et al. Combination of external beam radiotherapy and Californium (Cf)-252 neutron intracavity brachytherapy is more effective in control of cervical squamous cell carcinoma than that of cervical adenocarcinoma. Med Oncol. 2015;32(9):231. doi:10.1007/s12032-015-0670-3
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.