")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Disease Burden and Coping Strategies of Spouses of Patients with Psoriasis: A Qualitative Study
Authors Wu M, Zeng S, Zhang Y, Liu Y, Li B, Yi X, Shi Y , Zhu X
Received 4 January 2024
Accepted for publication 9 April 2024
Published 17 April 2024 Volume 2024:17 Pages 1653—1662
DOI https://doi.org/10.2147/JMDH.S458075
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Min Wu,1,2,* Sining Zeng,3,* Yi Zhang,1,2,* Yanru Liu,1,2 Bingbing Li,1,2 Xuemei Yi,1,2 Yuling Shi,1,2 Xiaoping Zhu3
1Department of Dermatology, Shanghai Skin Disease Hospital, Tongji University School of Medicine, Shanghai, 200443, People’s Republic of China; 2Institute of Psoriasis, Tongji University School of Medicine, Shanghai, 200443, People’s Republic of China; 3Nursing Department, Shanghai Tenth People’s Hospital, Tongji University School of Medicine, Shanghai, 200072, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaoping Zhu, Nursing Department, Shanghai Tenth People’s Hospital, Tongji University School of Medicine, 301 Yanchang Middle Road, Jing’an District, Shanghai, People’s Republic of China, Tel +86-021-66300588, Fax +86-021-66307542, Email [email protected] Yuling Shi, Department of Dermatology, Shanghai Skin Disease Hospital, Tongji University School of Medicine, 1278 Baode Road, Jing’an District, Shanghai, People’s Republic of China, Tel +86-021-36803020, Fax +86-021-36803021, Email [email protected]
Background: Psoriasis is a chronic autoimmune inflammatory skin condition characterized by erythema, papules, and scales. It imposes a heavy psychological and social strain on both patients and their families. Surprisingly, there’s limited research delving into the disease burden and coping strategies of spouses contending with psoriasis.
Objective: The objective is to explore the disease burden faced and coping strategies utilized by spouses of individuals living with psoriasis. This exploration aims to offer insights crucial for devising mental health support and intervention strategies.
Methods: The research methodology employed in this study was phenomenological, a qualitative approach. A total of fifteen spouses of patients with psoriasis were selected using an objective sampling method for in-depth, semi-structured interviews. Thematic analysis was then applied to the recorded interview data to derive meaningful themes.
Results: This study has identified and analyzed three core themes concerning the disease burden and coping strategies of spouses of patients with psoriasis: Overwhelming disease burden; Lack of support system; Coping strategies (Problem - centered coping strategies: Proactive acquisition of disease knowledge; Active confrontation of illness - related issues; Behavioral habit alteration; and Emotional - centered coping strategies: Active acceptance and normalization; Passive acceptance and internalized stigma; Avoidance of disease - related problems).
Conclusion: This study adds valuable insights into comprehending the disease burden encountered by spouses of patients with psoriasis and sheds light on the coping strategies they employ. Healthcare providers should proactively recognize and address the burden experienced by spouses early on. Establishing a robust support network is crucial, and promoting adaptive coping strategies can significantly aid spouses in effectively navigating and managing the complexities associated with psoriasis.
Keywords: psoriasis, spouse, disease burden, coping strategies, qualitative research
Introduction
Psoriasis is a chronic autoimmune inflammatory skin condition characterized by erythema, papules, and scales,1 It affects approximately 0.47% of the Chinese population.2 It exerts considerable psychological and social strains on patients and their families, causing isolation, curbed daily activities, and emotional turmoil like anxiety and depression.3,4 The spouse, a pivotal family member, not only acts as the primary caregiver but also serves as crucial support. However, previous research predominantly focuses on the impact of psoriasis on the life experiences of family caregivers,4 neglecting the specific burden and coping strategies of spouses. Thus, this study aims to delve into the unique challenges faced and coping strategies employed by spouses of patients with psoriasis. It strives to enrich clinical practices with comprehensive insights and lay groundwork for developing psychological support and intervention measures.
Methods
Study Design
This qualitative study employed semi-structured, in-depth interviews and thematic analysis to delve into the disease burden and coping strategies among spouses of patients with psoriasis. Adhering to the Consolidated Criteria for Conducting and Reporting Qualitative Research (COREQ) guidelines,5 the research methodology ensured a comprehensive exploration of this subject matter.
Participants
Participants were selected by purposive sampling and recruited from the Department of Dermatology at Shanghai Skin Disease Hospital during the period from November 2022 and March 2023. Spouses met specific inclusion criteria: (1) Being married to a patient who has been diagnosed with psoriasis for over 6 months and residing together; (2) Agreed to participate in the study and express genuine emotions. Exclusions comprised individuals with severe, uncontrolled progressive disorders, malignancies, psychiatric diagnoses, any skin conditions (including psoriasis), or chronic non-dermatological condition.
Procedure
The initial contact with potential participants was made by the first and second authors. Upon establishing a connection with interested individuals, researchers provided comprehensive details about the study and extended invitations to participate. Once their willingness was confirmed, spouses signed informed consent forms. Recruitment continued consecutively until data saturation, where no new themes emerged during analysis.
A total of 20 spouses of patients with psoriasis were approached. However, 5 declined participation citing reasons such as (lack of interest [n = 2], time constraints [n = 1], and reluctance to discuss the topic [n =2]). Eventually, the study comprised 15 spouses who willingly participated in interviews and were included in the subsequent analysis.
Data Collection
All interviews were conducted individually by the first author, a female postgraduate student specializing in dermatology nursing. These in-depth interviews took place in a quiet hospital room, with audio recordings made and observational notes taken during the sessions.
Each interview comprised two sections. The first section gathered sociodemographic details of the spouses, including gender, age, educational level, occupation, and duration of marriage. Besides, the spouses were also asked to complete the Chinese version of the Family Dermatology Life Quality Index (FDLQI)6 and The Hospital Anxiety and Depression Scale (HADS).7 The second part, derived from a review of pertinent literature, extensive team discussions, and pilot interviews involving two spouses of psoriasis patients (whose data were not incorporated into the research), encompassed four questions outlined in Box 1. Each interview commenced with an introductory dialogue, encouraging participants to discuss their understanding of psoriasis and how their spouses’ condition impacted their daily lives. To ensure open expression of thoughts and emotions, follow-up inquiries, rhetorical questions, and clarifications were employed throughout. Interview duration spanned between 45 to 60 minutes, averaging at 52.1 minutes.
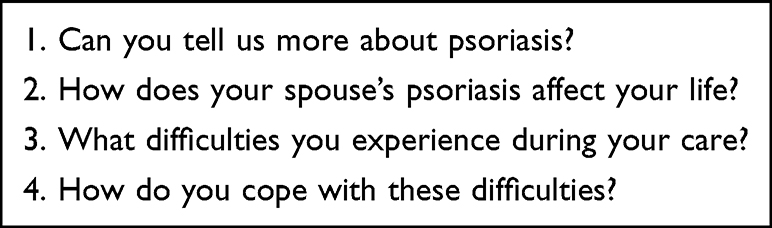 |
Box 1 Research Questions for Spouses of Patients with Psoriasis |
Data Analysis
The sociodemographic data analysis was conducted using SPSS version 26.0, while NVIVO software version 12 facilitated the interview data analysis, guided by Braun and Clarke’s stages for thematic analysis which included six-step process: 1) familiarizing yourself with the data; 2) generating initial codes; searching for themes; 3) reviewing themes; 4) defining themes; 5) naming those thematic and; 6) producing the report.8 Before transcription, the interview audio recordings were listened to at least twice by researchers M W and SN Z, who transcribed them verbatim. The transcriptions were cross-checked for accuracy. Subsequently, these researchers independently analyzed the transcripts to generate initial codes and themes using NVivo software. Themes and subthemes were established through consensus in team discussions. To ensure accuracy, transcripts were returned to participants for review, each assigned a specific identifier (P1-P15).
The study adhered to Lincoln and Guba’s four criteria for trustworthiness.9 Dependability was assured through independent coding by two researchers, along with regular team meetings to discuss analysis and findings. Credibility was enhanced by inviting an experienced qualitative researcher, not involved in the study, for peer debriefing, and by seeking confirmation of interview data from participants. Confirmability and transferability were maintained by thoroughly documenting the entire research process, including reflections, and maintaining an audit trail of procedures followed.
Ethical Consideration
This study was performed in accordance with the principles of the Declaration of Helsinki. This study received approval from the Medical Ethical Committee of Shanghai Skin Disease Hospital (approval #2020-36). Prior to their interviews, all participants provided signed written informed consent forms included the publication of anonymized responses. Researchers explicitly outlined participants’ rights to withdraw from the study at any point and for any reason, as well as the anonymity of the study, ensuring confidentiality throughout the research process. Importantly, there were no pre-existing relationships or conflicts of interest between the researchers and participants.
Results
The study encompassed spouses with an average age of 50.2 ± 11.0 years, while the mean duration of their marriages was 23.1 ± 9.9 years. Approximately two-thirds of the spouses were female, and 73.3% had educational qualifications below the university level. Regarding occupation, 10 participants (75%) were employed. The FDLQI score ranged from 7 to 30 points, and their respective mean points were 18.4 points. As for the score on the HADS, 9 (60%) scored higher than 7 on the anxiety subscale and 10 (66.67%) scored higher than 7 on the depression subscale. It can be seen that the spouses of patients with psoriasis experience severe quality of life impairment and a high degree of anxiety and depression. For a comprehensive breakdown of participants’ socio-demographic and clinical characteristics details, refer to Table 1.
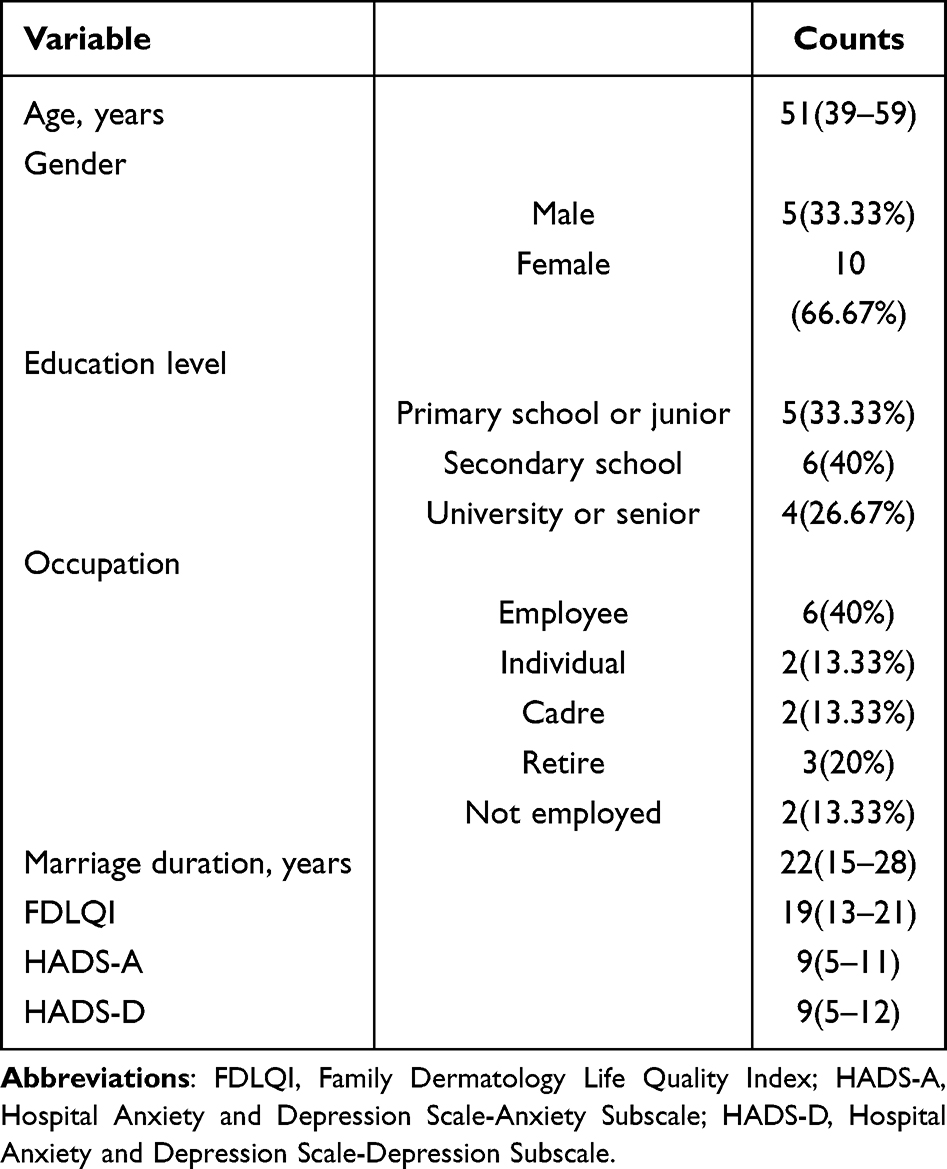 |
Table 1 Socio-Demographic and Clinical Characteristics of the Participants |
The study identified three primary themes and twelve sub-themes related to the disease burden and coping strategies of spouses of individuals with psoriasis (as outlined in Table 2): (1) Overwhelming disease burden, including the sub-themes: (a) Affected couple relationship, (b) Challenges in skin care, (c) Issues with treatment adherence, (d) Financial Strain; (2) Lack of support system: (a) Looking forward to professional guidance, (b) Desiring social support; (3) Coping strategies: (a) Emotional - centered coping strategies including: (A) Active acceptance and normalization, (B) Passive acceptance and internalized stigma, (C) Avoidance of disease - related problems; (b) Problem - centered coping strategies including (A) Proactive acquisition of disease knowledge, (B) Active confrontation of illness - related issues, (C) Behavioral habit alteration.
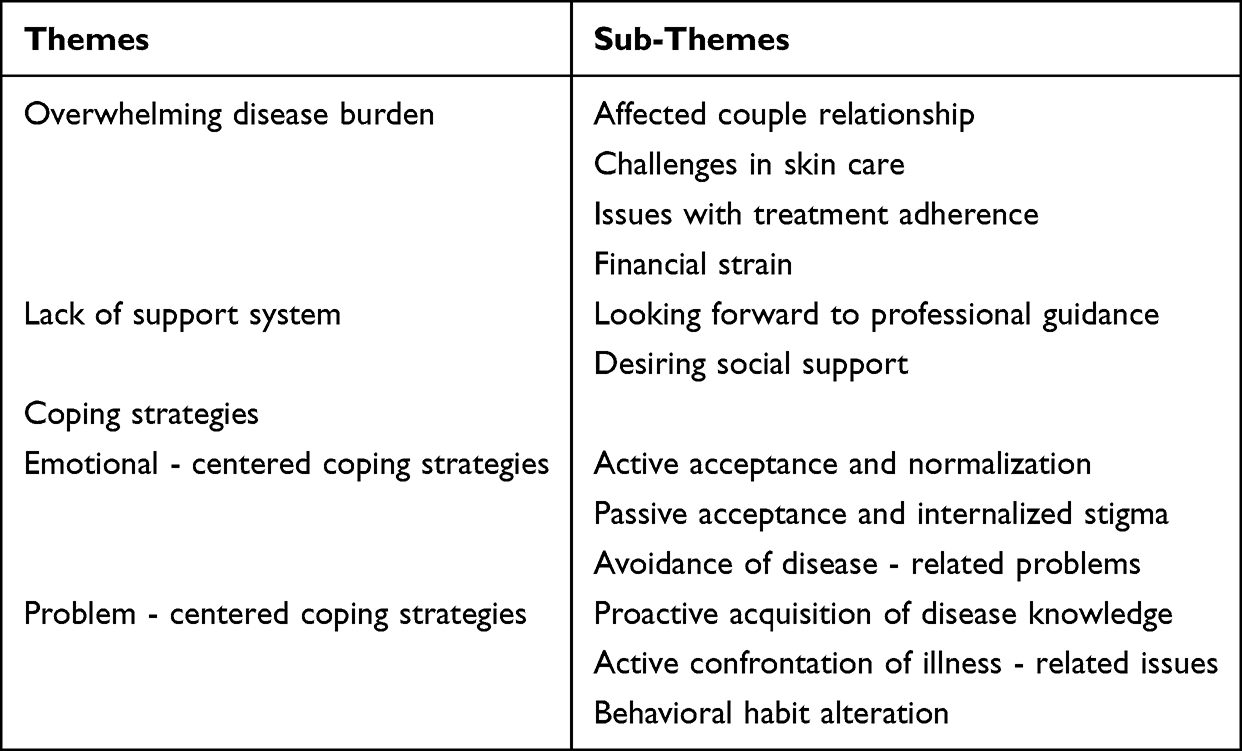 |
Table 2 Themes and Sub-Themes |
Overwhelming Disease Burden
Affected Couple Relationship
Some participants mentioned a decrease in intimacy level and frequency, as well as the unpleasant impact on sexual contact. During the onset of psoriasis, patients’ skin displayed noticeable erythema and scales, leading participants to intentionally keep their distance from the patients and avoid physical contact.
He has erythema and scales covering about 70–80% of his body, and aside from applying ointment for him, I have minimal physical contact with him. (P 7)
Since a rash appeared on his private area, our intimate life has been interrupted. (P 10)
Challenges in Skin Care
Many participants reported that they had to make numerous sacrifices and compromises in their personal lives. They spent a significant amount of time every day assisting patients in skin care, which greatly increased their caregiving burden.
I spend a lot of time every day helping him with basic skin treatments at home, such as applying ointment and skin encapsulation therapy (P 9)
His shoulder joint has developed a lesion, making it difficult for him to apply medication himself, so he is completely reliant on me to help him apply ointments and moisturizers, which makes me feel inadequate. (P 12)
Issues with Treatment Adherence
Some study participants indicated that psoriasis was prone to recurring episodes and required lifelong management once contracted, with overall poor patient adherence to treatment. As a result, they had to spend a significant amount of time urging patients to cooperate with their doctors for treatment. Noncompliance with treatment regimens could lead to increased recurrence of symptoms and worsening of the condition.
He always becomes lazy when his condition improves slightly and refuses to seek further treatment at the hospital. (P 13)
He always referred to this illness as the undying cancer, insisting that regardless of medication or treatment, the outcome would be the same. As a result, I had to devote a significant amount of effort to persuading him to undergo regular treatment. (P 5)
Financial Strain
Psoriasis is a chronic skin condition that often requires long-term medication and in some cases, hospitalization. In this study, the majority of participants indicated that the high cost of treatment for patients, as well as the potential risk of unemployment, placed a significant financial burden on the entire family.
She has now started using biologic agents for treatment, which cost several thousand yuan each time and need to be administered every two months. The expenses are really too high for us. (P 14)
My husband works in logistics and currently has a sever lesion on his hands. It easily breaks and causes discomfort with even minor friction. This condition is making it difficult for him to continue with his work. (P 4)
Lack of Support System
Looking Forward to Professional Guidance
Most of the participants indicated that they received limited professional support in terms of medication and skin management for patients with psoriasis during their attendance and treatment. In addition, healthcare providers often overlooked the challenges they faced in dealing with psoriasis.
I have been accompanying him to medical appointments for so many years, and never has a doctor or nurse cared about what I have been through or what kind of help I need. (P 13)
Every time I accompany him to see the doctor, I have a lot of questions to ask, but the doctor is always too busy to answer my questions. It’s difficult for me to receive professional guidance on how to better manage psoriasis. (P 11)
Desiring Social Support
Family members and friends are the primary sources of social support for spouses. They can provide emotional support and behavioral assistance, such as helping with patient’s skin care, daily household chores, and emotional outlet. However, in this study, the majority of participants indicated that they did not receive sufficient social support when dealing with the challenges of the patient’s illness.
I often find myself overwhelmed and would appreciate it if my family could lend a hand. (P 8)
Whenever I am feeling depressed and in need of encouragement and support, I always hope that friends or family members could be by my side. However, it often doesn’t happen as I wish. (P 1)
Coping Strategies
Spouses use various coping strategies in their daily lives to deal with the challenges of living with patients with psoriasis. These coping strategies can generally be categorized as emotion - centered coping strategies and problem - centered coping strategies.10
Emotional - Centered Coping Strategies
The emotion - centered coping strategies involve regulating or suppressing negative emotions related to the problem.
Active Acceptance and Normalization
In this study, some of the participants indicated that they accepted the fact that their spouses had psoriasis and had adapted to their spouse’s skin changes.
It has happened on him, and it may not look good externally, but fortunately, it has no impact on other aspects of his body. (P 9)
It has been around for decades, and I have already accepted it. (P 3)
Passive Acceptance and Internalized Stigma
The majority of the participants indicated that they might have some irrational worries or suspicions about people around them, leading them to believe that their own family and friends looked down on them. In other words, they experienced the stigma of expectations and internalization. Consequently, they coped with these emotional burdens by passively accepting and internalizing the stigma.
Being with him is my destiny, and I cannot change it. (P 15)
Sometimes, when my friends or relatives discuss my husband’s illness with me, I sometimes have a feeling that they are using a condescending tone, but in reality, it is my misunderstanding (P 10)
Avoidance of Disease - Related Problems
When discussing long-term disease management, most participants tended to avoid the topic because they lack an understanding of the necessary knowledge for illness management.
I don’t want to dwell too much on this issue. There are many things that I don’t understand and can’t solve. (P 6)
In addition, most participants tend to utilize avoidance mechanisms to cope with the pressures arising from public stigma and affiliate stigma associated with their illness. They avoid social activities and try to stay at home as much as possible, perpetuating a vicious cycle that ultimately leads to their social isolation.
She is currently experiencing severe skin irritation and is afraid of what people might say, so we spend most of our time at home and have almost completely stopped socializing with friends. (P 7)
Problem -Centered Coping Strategies
The problem-centered coping strategies involves actively facing problems and improving adaptation to the current situation through rational cognition.
Proactive Acquisition of Disease Knowledge
Some participants stated that they acquire knowledge about disease management through their own experiences or those of others. They actively reflect on past caregiving experiences and further educate and manage psoriasis through the internet or books.
Every time he eats seafood, his psoriasis tends to flare up, so we have never bought any seafood at home. (P 2)
Additionally, a small number of participants indicated that they would share their caregiving experiences with the spouses of other patients with psoriasis, which can not only alleviate their psychological burden, but also increase their understanding of psoriasis care.
I sometimes attend psoriasis lectures in the community, where I often communicate with spouses of other patients with psoriasis, who often teach me some care tips and help me better care for my lover. (P 15)
Active Confrontation of Illness - Related Issues
Some participants indicated that they would actively express their actions or ideas in various ways, such as purchasing assistive therapy devices, to encourage patients to actively engage in treatment.
Currently, his lesion is localized on his lower extremities, so I purchased a home phototherapy device for him to receive treatment at home, improving his treatment compliance. (P 10)
I have always believed that actively cooperating with treatment will lead to a definite improvement in the situation. My attitude has also influenced him, making him more actively address the illness. (P 8)
Behavioral Habit Alteration
Some participants expressed that they choose to actively take on household chores, stay busy with work, or distract themselves (such as by listening to music or exercising) in order to prevent experiencing negative emotions while caring for their loved ones.
I keep myself constantly busy, with no time to think. (P 12)
I take it upon myself to assume all household cleaning responsibilities, allowing him to have more time to rest. (P 3)
Discussion
In our study, a significant majority of spouses revealed substantial caregiving burdens and encountered profound emotional challenges while supporting patients with psoriasis. These difficulties could not only negatively affect their physical and mental well-being, but also could potentially increase the likelihood of mental health disorders between spouses.
Recent research even indicated a higher frequency of anxiety and depression among partners of psoriasis patients compared to healthy controls.11 This underscores the imperative for healthcare professionals to extend their focus beyond patients, considering the psychological and emotional welfare of spouses. Hence, screening for psychological health issues in spouses becomes integral in the comprehensive management of psoriasis within families.
Moreover, our findings revealed that psoriasis significantly altered patients’ skin appearance, consequently impacting the intimate relationships shared between patients and their spouses. Intimate relationships represent a crucial aspect of individuals’ lives and substantially influence overall quality of life. Therefore, when offering psychological care, it becomes particularly crucial to sensitively address and identify the intimate relationship challenges faced by spouses of individuals with psoriasis.
Additionally, a study examining the disease burden of patients with psoriasis across eight geographic regions of China highlighted that the total annual expenditures of patients due to psoriasis accounted for an average of 29.7% of their income.3 This resonates with the substantial economic burden described by spouses in our study. However, the incomplete nature of the healthcare system limits some patients from benefiting from policies. Hence, policymakers must expand medical insurance coverage, enhance reimbursement policies, and refine healthcare insurance mechanisms to alleviate the financial strain experienced by individuals affected by psoriasis and their families.
Notably, our study identified that spouses encountered diverse social and psychological pressures, desiring to seek support and solace from family and friends. However, most spouses faced restricted access to social support. According to Pearlin’s stress theory, social support plays a pivotal role as a mediator in the stress process of caregivers.12 This theory underscores the significance of social support as a mediating factor that influences the outcomes of caregiver anxiety and depression.12 Hence, establishing and nurturing a robust social support network for spouses is crucial. In addition, some spouses expressed a need for deeper understanding of psoriasis but received inadequate information from healthcare providers, often being overlooked. Insufficient knowledge among spouses might hinder their ability to care for patients, ultimately impacting the patients’ quality of life. Therefore, healthcare professionals should extend their services to encompass spouses of psoriasis patients. Emphasizing disease education is vital to help spouses comprehend and manage the illness effectively.
Moreover, our findings affirmed that spouses employ adaptive coping strategies to confront the burden of the disease. These strategies include maintaining a positive attitude, actively acquiring psoriasis-related knowledge, modifying behavioral habits, and embracing and adjusting to the illness. A study found that adaptive problem-solving coping strategies correlate with enhanced patient functioning,13 aligning with our research.
Our results underscored that some spouses display a positive attitude towards illness may have a positive impact on patients’ treatment adherence. Furthermore, proactive learning about psoriasis by spouses may not only enhances their caregiving skills and disease management but may also aids in their adaptation to psoriasis, lessening the psychological burden of the disease. However, we also observed that spouses encountered varying levels of illness stigma in their daily lives and social interactions. Common coping strategies for stigma included avoidance, passive acceptance, and internalization, ultimately leading to increased social isolation. Stigma denotes inherent impressions, biases, and discrimination against a particular group.14 Stigmatization poses a significant obstacle for family caregivers in seeking help, actively engaging in caregiving, and patients adhering to treatment.15
Previous reports have highlighted the impact of psoriasis on lifestyle, relationships, and psychological well-being among family members,16 which is consistent with our research findings. This underscores the pressing need for effective social educational initiatives to foster a correct understanding of psoriasis among the public and diminish stigmatizing attitudes and behaviors towards it. Simultaneously, healthcare providers should also offer proactive psychological education interventions for caregivers to alleviate their subjective burden and negative emotions associated with caregiving.17
The significance of coping strategies adopted by spouses was evident. Maladaptive coping strategies could exacerbate the psychological strain on spouses, potentially leading to the perpetuation of illness stigma. Conversely, adaptive coping strategies not only enhanced the psychological well-being of spouses,18 but also positively impacted the quality of life for both spouses and patients.19 Hence, healthcare providers should dedicate ample time to encourage spouses in embracing adaptive or problem-centered coping strategies.
Dyadic coping involves how couples collectively handle and decide on stressful events, encompassing positive and negative coping approaches.20 Studies have demonstrated that a proactive approach by couples in jointly managing stress related to illness can effectively enhance their physical and mental health, elevate their quality of life, and diminish negative emotions.21 In our study, spouses highlighted that providing continuous positive assistance and support during the illness significantly influenced how patients coped. This is consistent with the findings of previous study by pereira et al.22 Their study focused on dyadic adjustment between patients with psoriasis and their partners and their findings suggested that the positive involvement or coping strategies of partners, including constructively solving problems, led to better adjustment for patients with psoriasis. Hence, healthcare providers should prioritize understanding the coping mechanisms of both spouses, promoting positive dyadic coping, and consistently considering the patient and spouse as a “unit” when implementing nursing intervention to enhance their collaborative approach in managing psoriasis.
However, this study has several limitations. Our study has generated a number of hypotheses that have not been tested in larger populations, which will be tested in studies with larger samples in the future. The limited sample size and the single-center nature of the study, which make that the patients come from a single geographic area, limits the generability of the results. Additionally, our study did not concurrently examine the coping strategies adopted by patients with psoriasis. Eventually, our study limited the work to wives, but unmarried, cohabiting couples may suffer the same consequences.
Future studies should expand the sample size to include unmarried, cohabiting couples and explore dyadic coping among both spouses to deepen our comprehension of how patients with psoriasis and their spouses collectively cope.
Conclusion
This study offers compelling evidence regarding the disease burden faced by spouses of individuals with psoriasis and sheds light on the coping strategies they employ. It became evident that spouses encounter substantial disease-related challenges and often lack a robust support system while navigating the complexities of psoriasis. Moreover, our findings revealed a tendency among spouses to resort to maladaptive coping mechanisms in handling these challenges. As a result, it is imperative for healthcare providers to promptly identify and address the illness burden experienced by spouses. They should proactively establish support networks and promote adaptive coping strategies to facilitate better adaptation and management of psoriasis among spouses. The insights gleaned from this study serve as a valuable reference for crafting comprehensive nursing interventions aimed at enhancing the quality of life for both psoriasis patients and their spouses in the future.
Data Sharing Statement
For the privacy of individuals that participated in the study, the data will be shared on reasonable request to the corresponding author.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was sponsored by grants from Clinical Research Plan of SHDC (No. SHDC2020CR1014B). The study sponsor took part in the design of the study.
Disclosure
All the authors declare no conflicts of interest in this work.
References
1. Boehncke WH, Schon MP. Psoriasis. Lancet. 2015;386(9997):983–994. doi:10.1016/S0140-6736(14)61909-7
2. Ding X, Wang T, Shen Y, et al. Prevalence of psoriasis in China: a population-based study in six cities. Eur J Dermatol. 2012;22(5):663–667. doi:10.1684/ejd.2012.1802
3. Chen XL, Zheng LY, Zhang H, et al. Disease burden and quality of life for psoriasis patients in China. Value Health. 2019;22:S379. doi:10.1016/j.jval.2019.04.1852
4. Eghlileb AM, Davies EE, Finlay AY. Psoriasis has a major secondary impact on the lives of family members and partners. Br J Dermatol. 2007;156(6):1245–1250. doi:10.1111/j.1365-2133.2007.07881.x
5. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
6. Bd A. The Impact of Some Skin Diseases on the Quality of Life of Patients and Their Families. Shenyang: China Medical University; 2017.
7. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
8. Kiger ME, Varpio L. Thematic analysis of qualitative data: AMEE Guide No. 131. Med Teach. 2020;42(8):846–854. doi:10.1080/0142159X.2020.1755030
9. Lincoln YS, Guba EG. Naturalistic Inquiry. Newbury Park (CA): Sage; 1985.
10. Melendez JC, Mayordomo T, Sancho P, Tomas JM. Coping strategies: gender differences and development throughout life span. Span J Psychol. 2012;15(3):1089–1098. doi:10.5209/rev_SJOP.2012.v15.n3.39399
11. Alariny AF, Farid CI, Elweshahi HM, Abbood SS. Psychological and Sexual Consequences of Psoriasis Vulgaris on Patients and Their Partners. J Sex Med. 2019;16(12):1900–1911. doi:10.1016/j.jsxm.2019.08.017
12. Pearlin LI, Mullan JT, Semple SJ, Skaff MM. Caregiving and the stress process: an overview of concepts and their measures. Gerontologist. 1990;30(5):583–594. doi:10.1093/geront/30.5.583
13. Rao P, Grover S, Chakrabarti S. Coping with caregiving stress among caregivers of patients with schizophrenia. Asian J Psychiatr. 2020;54.
14. Aranda AM, Helms WS, Patterson KDW, Roulet TJ, Hudson BA. Standing on the Shoulders of Goffman: advancing a Relational Research Agenda on Stigma. Bus Soc. 2023;62(7):1339–1377. doi:10.1177/00076503221148441
15. Corrigan P. How stigma interferes with mental health care. Am Psychol. 2004;59(7):614–625. doi:10.1037/0003-066X.59.7.614
16. Snyder AM, Brandenberger AU, Taliercio VL, et al. Quality of Life Among Family of Patients with Atopic Dermatitis and Psoriasis. Int J Behav Med. 2023;30(3):409–415. doi:10.1007/s12529-022-10104-7
17. Gurusamy J, Gandhi S, Damodharan D, Palaniappan M, Venkatasubramanian G. Grounded theory of ‘lifestyle adaptation’ - Perspectives from persons with schizophrenia and their caregivers. Asian J Psychiatr. 2021;56.
18. Fairfax A, Brehaut J, Colman I, et al. A systematic review of the association between coping strategies and quality of life among caregivers of children with chronic illness and/or disability. BMC Pediatr. 2019;19(1):215. doi:10.1186/s12887-019-1587-3
19. van Andel J, Westerhuis W, Zijlmans M, Fischer K, Leijten FSS. Coping style and health-related quality of life in caregivers of epilepsy patients. J Neurol. 2011;258(10):1788–1794. doi:10.1007/s00415-011-6013-1
20. Bodenmann G. A systemic - transactional conceptualization of stress and coping in couples. Swiss J Psychol. 1995;54(1):16.
21. Lee E, Roberts LJ. Between individual and family coping: a decade of theory and research on couples coping with health-related stress. J Family Theory Rev. 2018;10(1):141–164. doi:10.1111/jftr.12252
22. Pereira MG, Brito L, Smith T. Dyadic adjustment, family coping, body image, quality of life and psychological morbidity in patients with psoriasis and their partners. Int J Behav Med. 2012;19(3):260–269. doi:10.1007/s12529-011-9174-5
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.