")
Back to Journals » Pragmatic and Observational Research » Volume 15
Difficult-To-Treat and Severe Asthma: Can Real-World Studies On Effectiveness of Biological Treatments Change the Lives of Patients?
Authors Pelaia C , Giacalone A, Ippolito G, Pastore D, Maglio A, Piazzetta GL, Lobello N , Lombardo N , Vatrella A , Pelaia G
Received 30 November 2023
Accepted for publication 28 February 2024
Published 11 March 2024 Volume 2024:15 Pages 45—51
DOI https://doi.org/10.2147/POR.S396799
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor David Price
Corrado Pelaia,1 Antonio Giacalone,2 Gianluca Ippolito,2 Daniela Pastore,2 Angelantonio Maglio,3 Giovanna Lucia Piazzetta,1 Nadia Lobello,1 Nicola Lombardo,1 Alessandro Vatrella,3 Girolamo Pelaia2
1Department of Medical and Surgical Sciences, University “Magna Græcia” of Catanzaro, Catanzaro, Italy; 2Department of Health Sciences, University “Magna Græcia” of Catanzaro, Catanzaro, Italy; 3Department of Medicine, Surgery and Dentistry, University of Salerno, Salerno, Italy
Correspondence: Corrado Pelaia, Department of Medical and Surgical Sciences, University Magna Graecia of Catanzaro, Viale Europa – Località Germaneto, Catanzaro, 88100, Italy, Tel + 39 0961 3647007, Email [email protected]
Abstract: Many different phenotypes that characterize severe asthma are supported by intricate pathomechanisms called endotypes. The latter are driven by molecular interactions, mediated by intercellular networks. With regard to the biological treatments of either allergic or non-allergic eosinophilic type 2 asthma, real-world studies have confirmed the positive effects of currently available antibodies directed against immunoglobulins E (IgE), interleukin-5 (IL-5) and its receptor, as well as the receptors of interleukins-4 (IL-4) and 13 (IL-13). The best way to treat severe asthma should be chosen based on the peculiar phenotypic and endotypic traits of each patient. This will lead to relevant improvements in both clinical and functional outcomes. In particular, biological therapies can change the lives of asthma patients with a strong impact on quality of life. Unfortunately, patients with severe non-type-2 asthma, who continue to have pertinent unmet needs, are not receiving satisfactory advances within the context of biological treatments. It is also hopeful that in the next future new therapeutic strategies will be specifically implemented for these people, perhaps offering them the opportunity to improve their current, mostly inadequate asthma management.
Keywords: type 2 severe asthma, monoclonal antibodies, pro-inflammatory cytokines, quality of life
Introduction
Asthma is one of the most common diseases in the world, as it affects about 300 million people. It is characterized by respiratory symptoms such as wheezing, difficult breathing, chest tightness, and coughing, which are usually associated with variable airflow limitations.1 In particular, a subset of patients with severe uncontrolled asthma (5–10%) pose the heaviest medical, social, and economic burden.2–5 Different subgroups of severe asthma are currently recognized: allergic eosinophilic, nonallergic eosinophilic, mixed eosinophilic and neutrophilic, neutrophilic, and paucigranulocytic.6 The bronchial epithelium of asthmatic patients is often fragile and highly permeable to environmental noxious agents. As a consequence, injured airway epithelial cells release high amounts of innate cytokines including thymic stromal lymphopoietin (TSLP), interleukin-25 (IL-25), and interleukin-33 (IL-33).7 These alarmins drive the tight crosstalk between innate and adaptive immune responses, which induce the development and progression of type 2 airway inflammation. Within this pathogenic context, group 2 innate lymphoid cells (ILC2) and T helper 2 (Th2) lymphocytes produce huge quantities of type 2 cytokines such as interleukin-5 (IL-5), interleukin-4 (IL-4), and interleukin-13 (IL-13). The latter trigger and amplify the differentiation and activation of eosinophils, as well as their recruitment inside inflamed airways.8
With regard to severe asthma, updated Global Initiative for Asthma (GINA) guidelines recommend at step 5 the addition of biological drugs to maximized and optimized standard treatments.9 Several monoclonal antibodies are currently available for biologic therapies of severe asthma. Omalizumab targets human immunoglobulins E (IgE), thus being indicated for treatment of severe allergic asthma.10 Other monoclonal antibodies target either IL-5 (mepolizumab, reslizumab) or its receptor (benralizumab), thereby providing very effective anti-eosinophilic therapies.11–15 Dupilumab is a dual receptor antagonist of both IL-4 and IL-13, and its specific mechanism of action guarantees an effective biologic treatment of severe type 2 asthma.16 Tezepelumab is a specific inhibitor of TSLP, which appears to be involved in the pathobiology of both T2-high and T2-low pheno/endotypes of asthma. Therefore, this drug is currently the only biologic which can be prescribed to severe asthmatic patients with either type 2 or non-type 2 disease.17
Severe asthma and its multiple comorbidities negatively impact on quality of life.18–20 The Asthma Quality of Life Questionnaire (AQLQ) is used to assess quality of life in asthma patients.21,22 This score considers 4 domains: symptoms (12 items), activity limitation (11 items), emotional function (5 items), and environmental stimuli (4 items). To each domain 7-point scale (7 = not impaired at all; 1 = severely impaired) is assigned, with higher scores indicating a better quality of life. However, in large clinical trials a greater efficiency is provided by the Mini Asthma Quality of Life Questionnaire (Mini-AQLQ). In addition to AQLQ, another important tool for assessing the health status of asthmatic patients is the Asthma Control Test (ACT).23 It consists of 5 questions on different domains (activity, shortness of breath, night or morning symptoms, medication use as needed, subjective control) on a scale of 1 to 5 points. ACT score ranges from 5 (poor asthma control) to 25 (complete asthma control), with higher scores reflecting greater asthma control. An ACT score >19 indicates that asthma is well controlled
On the basis of the above-mentioned considerations, the aim of this review is to evaluate the real-world impact of biological therapies on quality of life in patients with severe asthma (Table 1).
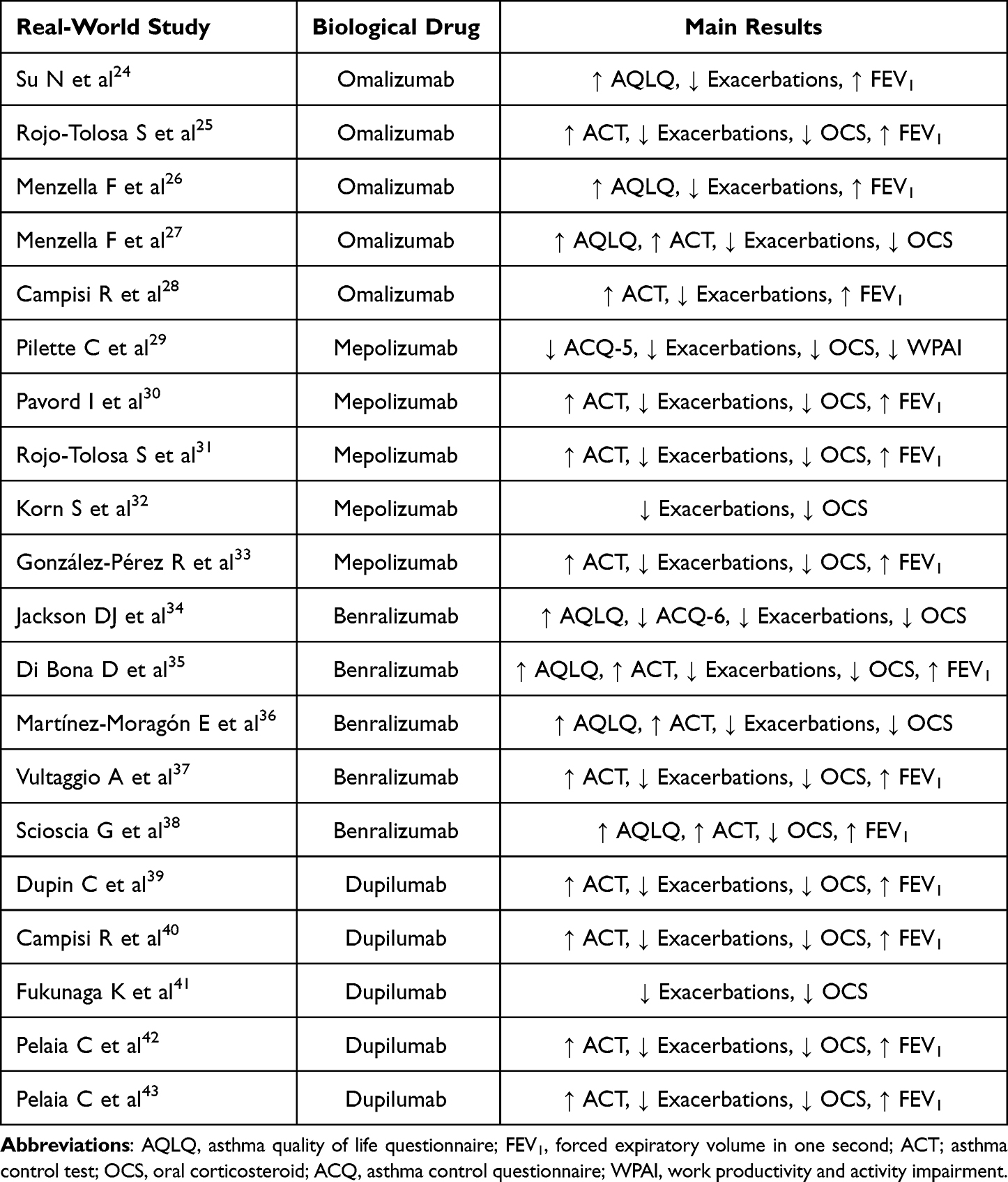 |
Table 1 Main Real-World Positive Therapeutic Effects of Biological Drugs in Patients with Severe Asthma |
Omalizumab
Omalizumab was the first biologic therapy authorized by regulatory bodies for the add-on treatment of severe asthma.44 Omalizumab inhibits IgE interactions with high-affinity receptor (FcεRI) and low-affinity receptor (FcεRII)/CD23 receptors by specifically binding to the constant region of human IgE.45 Omalizumab is thus particularly efficient in blocking the biological effects of IgE at the level of immune/inflammatory and structural cells within the airways.46 Allergic patients with impaired lung function, who are treated with high dosages of inhaled corticosteroids, but do not control asthma symptoms and experience frequent asthma exacerbations, are eligible to receive omalizumab.47
Several real-world studies conducted all around the globe have proven the positive therapeutic advantages of omalizumab.48 Specifically, these real-world studies have shown that omalizumab decreases oral corticosteroids (OCS) consumption and the number of missed work and school days, in addition to markedly decreasing the likelihood of asthma exacerbations and hospital ward visits.24,25,49 Additionally, empirical data clearly indicates that omalizumab may provide substantial and long-lasting improvements in forced expiratory volume in one second (FEV1), detectable up to 16 years after the initiation of anti-IgE treatment.26,27,50 Severe asthmatics patients under treatment with omalizumab manifest a high degree of treatment adherence, which can be explained by the above positive clinical and functional effects.28 Omalizumab also has a long-lasting, favourable safety and tolerability profile, which contributes to improve the quality of life of asthmatic patients.51
Mepolizumab
Mepolizumab is a humanized monoclonal antibody which specifically binds to IL-5, thus preventing its interaction with IL-5 receptor expressed by eosinophils. As a consequence, mepolizumab inhibits the proliferation and survival of these cells, thereby suppressing eosinophilic inflammation. This biological drug can be prescribed to people complaining of uncontrolled eosinophilic asthma, with a blood eosinophil count ≥150 cells/µL before the first administration and ≥300 cells/µL in the previous year, and with at least 2 asthma exacerbations requiring oral steroids in the past year. In addition to severe eosinophilic asthma, mepolizumab is also indicated for other three eosinophil-driven diseases, including chronic rhinosinusitis with nasal polyps (CRSwNP), eosinophilic granulomatosis with polyangiitis (EGPA), and hypereosinophilic syndrome (HES).52 Mepolizumab is administered by a subcutaneous injection at a fixed dose of 100 mg every 28 days. During these years, lots of studies analysed mepolizumab about its efficacy in uncontrolled severe eosinophilic asthma, showing very positive effects on symptom control, exacerbation rate, OCS maintenance dose, hospitalization number, lung function.29,53 Furthermore, mepolizumab is characterized by a very safe profile.30 In particular, several studies suggest that patients treated with mepolizumab can achieve real-life clinical benefits regardless of the presence of a range of common comorbidities, including upper and lower airway diseases, atopic disorders, chronic sinusitis, chronic obstructive pulmonary disease, nasal polyps, obesity, anxiety, and depression.54 These investigations focused on the impact that this biological therapy has on quality of life. Indeed, a significant change in the ACT questionnaire score and an improvement in pulmonary function were found in all studies.31–33,55 All these considerations highlight that treatment with mepolizumab improves the quality of life in a real-world setting.32
Benralizumab
Benralizumab is a humanized monoclonal antibody (IgG1k) that binds very strongly to the α subunit of IL-5 receptor, thus impeding its interaction with IL-5. Moreover, the molecular structure has been engineered without fucose sugar residues in the CH2 domain of the constant region, thus enhancing the affinity binding for FcγRIIIa (CD16a) expressed by natural killer (NK) cells. As a consequence, antibody-dependent cell-mediated cytotoxicity (ADCC) of eosinophils and basophils results to be markedly potentiated.56
Real-life experiences with benralizumab in patients with severe eosinophilic asthma (SEA) showed that overall disease control was much better after anti-IL5 receptor treatment. In particular, it was reported that there was a drastic reduction in annualized exacerbation rate and OCS intake, with associated improvements in lung function, Asthma Control Questionnaire (ACQ) score, ACT score and mAQLQ score.34–36 Another real-world study conducted on a large SEA population evaluated the effectiveness of benralizumab. This drug dramatically decreased the frequency of exacerbations, improved asthma control and lung function. The proportion of patients achieving well-controlled asthma increased from 16.7% at baseline to 78.7% after 96 weeks of therapy. Moreover, long-term treatment with benralizumab has proven to promote OCS elimination, thereby reducing OCS median daily dosage by 100% at both 48 and 96 weeks.37
In addition to retrospective real-world studies, an Italian observational real-life study enrolled 10 consecutive patients that began treatment with benralizumab. During the follow-up, ACT score enhanced from 13.5 ± 1.5 (baseline) to 20.3 ± 1.4 (12 weeks) and to 24.2 ± 0.6 (24 weeks), ACQ score reduced from 3.48 ± 0.65 (baseline) to 2.32 ± 0.57 (12 weeks) and to 1.42 ± 0.92 (24 weeks), EuroQol-Visual Analogue Scales (EQ-VAS) increased from 44.5 ± 7.7 (baseline) to 60.5 ± 6.6 (12 weeks) and to 86.7 ± 7.2 (24 weeks), and Beck Depression Inventory scale (Beck DI) reduced from 14.6 ± 3.68 (baseline) to 9.1 ± 1.64 (12 weeks) and to 3.7 ± 1.8 (24 weeks). Moreover, AQLQ total score improved from 3.65 ± 0.56 (baseline) to 4.61 ± 0.67 (12 weeks) and to 5.17 ± 0.87 (24 weeks). The percentage of patients complaining of serious problems in all domains of the EuroQol-5Dimensions-3Levels (EQ-5D-3L) at baseline significantly decreased after both 12 and 24 weeks of treatment. Lastly, FEV1 significantly increased during the follow-up.38
Dupilumab
Dupilumab is a fully human IgG4 monoclonal antibody that binds to IL-4Rα, thereby functioning as an IL-4 and IL-13 dual receptor antagonist. Dupilumab is beneficial for severe asthmatics with a blood eosinophil count of at least 150 cells/µL and/or fractional exhaled nitric oxide (FeNO) concentration of at least 25 parts per billion (ppb), who also eventually begin long-term OCS treatment regimens. Dupilumab exerts positive therapeutic action, such as timely and significant improvements in asthma exacerbations, symptom control, airflow limitation, lung hyperinflation, and OCS consumption.57,58 Nowadays, dupilumab may be suggested as an add-on biological treatment for people with nasal polyposis or atopic dermatitis, two major conditions that often coexist with asthma, as well as for people with severe asthma.39–41,59,60 When evaluating dupilumab’s practical effects on severe asthma, it is important to keep in mind that nasal polyposis and chronic rhinosinusitis are both significantly impacted by its mode of action. In fact, a study showed how a group of 20 individuals had substantial improvements in both nasal polyposis and severe asthma within only 4 weeks.42 Specifically, there was a substantial reduction in Sinonasal Outcome Test-22 (SNOT-22) score, as well as a significant increase in ACT score. Within 4 weeks, OCS consumption was interrupted. Moreover, forced vital capacity (FVC) and FEV1 significantly increased at week 4. Furthermore, dupilumab increased forced expiratory flow between 25% and 75% of FVC (FEF25–75) and decreased residual volume, respectively. Another real-life investigation assessed the effects of 6-month treatment with dupilumab in 127 patients affected by severe asthma, eventually associated with nasal polyps.43 Asthma exacerbations and daily intake of prednisone zeroed during the follow-up period. SNOT-22 score decreased from 55.84 to 19.76, and ACT score improved from 14 to 22. These results were paralleled by an improvement of lung function, in terms of FEV1, FVC and FEF25-75.
Conclusions
The recent advances in our understanding of the pathomechanisms underlying severe asthma have driven the development of several biologic medications, including omalizumab, mepolizumab, benralizumab, and dupilumab. Randomized controlled trials and observational real-life data have provided compelling evidence for the safety and effectiveness of these antibodies as additional therapies for type 2 airway inflammation. Furthermore, the aforementioned biologic treatments are capable of inducing noteworthy advantages in the management of several asthma comorbidities, namely nasal polyposis. In particular, real-world studies have confirmed the positive therapeutic effects of biological drugs in patients with severe asthma, highlighting great improvements also in quality of life and global health status (Figure 1).
 |
Figure 1 Real-world treatment effectiveness of biological therapies for severe type 2 asthma contribute to improve quality of life of patients. Omalizumab, mepolizumab, benralizumab, and dupilumab are able to reduce exacerbations and daily oral corticosteroid (OCS) intake, ameliorating lung function and asthma control test (ACT) score. These positive effects translate into notable improvements in terms of quality of life. Created with BioRender.com. |
Overall, the very relevant therapeutic benefits enjoyable by patients with type 2 severe asthma and related comorbidities, treated with biological therapies, can be summarized as follows: (i) suppression of eosinophilic inflammation and restoration of airway epithelium; (ii) decrease of severe asthma exacerbations; (iii) decrement of OCS use; (iv) improvement of asthma symptom control; (v) improvement of lung function; (vi) reduction of emergency visits and hospitalizations; (vii) improvement of health status and quality of life; (viii) remarkable attenuation of the social and economic burden associated with severe asthma.
Unfortunately, individuals with predominant neutrophilic bronchial inflammation are not taking advantage by the considerable treatment prospects now enjoyed by subjects with allergic and eosinophilic asthma. Thus, more studies are needed to attain improved outcomes in the therapy of severe T2-low asthma as well.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Holgate ST, Wenzel S, Postma DS, et al. Asthma. Nat Rev Dis Primers. 2015;1:15025. doi:10.1038/nrdp.2015.25
2. Stern J, Pier J, Litonjua AA. Asthma epidemiology and risk factors. Semin Immunopathol. 2020;42:5–15. doi:10.1007/s00281-020-00785-1
3. Soremekun S, Heaney LG, Skinner D, et al. Asthma exacerbations are associated with a decline in lung function: a longitudinal population-based study. Thorax. 2023;78(7):643–652. doi:10.1136/thorax-2021-217032
4. Chen W, Sadatsafavi M, Tran TN, et al. Characterization of patients in the international severe asthma registry with high steroid exposure who did or did not initiate biologic therapy. J Asthma Allergy. 2022;15:1491–1510. doi:10.2147/JAA.S377174
5. Perez-de-Llano L, Scelo G, Canonica GW, et al. Impact of pre-biologic impairment on meeting domain-specific biologic responder definitions in patients with severe asthma. Ann Allergy Asthma Immunol. 2023;S1081–1206(23):1508–1509.
6. Papi A, Brightling C, Pedersen SE, Reddel HK. Asthma. Lancet. 2018;391:783–800. doi:10.1016/S0140-6736(17)33311-1
7. Pelaia C, Pelaia G, Crimi C, et al. Tezepelumab: a potential new biological therapy for severe refractory asthma. Int J Mol Sci. 2021;22(9):4369. doi:10.3390/ijms22094369
8. Pelaia C, Heffler E, Crimi C, et al. Interleukins 4 and 13 in asthma: key pathophysiologic cytokines and druggable molecular targets. Front Pharmacol. 2022;13:851940. doi:10.3389/fphar.2022.851940
9. Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention; 2023. Available from: www.ginasthma.org.
10. Bousquet J, Rabe K, Humbert M, et al. Predicting and evaluating response to omalizumab in patients with severe allergic asthma. Respir Med. 2007;101(7):1483–1492. doi:10.1016/j.rmed.2007.01.011
11. Pfeffer PE, Ali N, Murray R, et al. Comparative effectiveness of anti-IL5 and anti-IgE biologic classes in patients with severe asthma eligible for both. Allergy. 2023;78(7):1934–1948. doi:10.1111/all.15711
12. Menzies-Gow AN, McBrien C, Unni B, et al. Real world biologic use and switch patterns in severe asthma: data from the international severe asthma registry and the US CHRONICLE Study. J Asthma Allergy. 2022;15:63–78. doi:10.2147/JAA.S328653
13. Porsbjerg CM, Menzies-Gow AN, Tran TN, et al. Global variability in administrative approval prescription criteria for biologic therapy in severe asthma. J Allergy Clin Immunol Pract. 2022;10(5):1202–1216.e23. doi:10.1016/j.jaip.2021.12.027
14. Chen W, Tran TN, Sadatsafavi M, et al. Impact of initiating biologics in patients with severe asthma on long-term oral corticosteroids or frequent rescue steroids (GLITTER): data from the international severe asthma registry. J Allergy Clin Immunol Pract. 2023;11(9):2732–2747. doi:10.1016/j.jaip.2023.05.044
15. Nagase H, Suzukawa M, Oishi K, Matsunaga K. Biologics for severe asthma: the real-world evidence, effectiveness of switching, and prediction factors for the efficacy. Allergol Int. 2023;72(1):11–23. doi:10.1016/j.alit.2022.11.008
16. Brusselle GG, Koppelman GH. Biologic therapies for severe asthma. N Engl J Med. 2022;386(2):157–171. doi:10.1056/NEJMra2032506
17. Kardas G, Kuna P, Panek M. Biological therapies of severe asthma and their possible effects on airway remodeling. Front Immunol. 2020;11:1134. doi:10.3389/fimmu.2020.01134
18. Cushen B, Koh MS, Tran TN, et al. Adult severe asthma registries: a global and growing inventory. Pragmat Obs Res. 2023;14:127–147. doi:10.2147/POR.S399879
19. Scelo G, Torres-Duque CA, Maspero J, et al. Analysis of comorbidities and multimorbidity in adult patients in the international severe asthma registry. Ann Allergy Asthma Immunol. 2024;132(1):42–53. doi:10.1016/j.anai.2023.08.021
20. Wechsler ME, Scelo G, Larenas-Linnemann DES, et al. Association between T2-related comorbidities and effectiveness of biologics in severe asthma. Am J Respir Crit Care Med. 2024;209(3):262–272. doi:10.1164/rccm.202305-0808OC
21. Coleman C, Khaleva E, Rattu A, et al. Narrative review to capture patients’ perceptions and opinions about non-response and response to biological therapy for severe asthma. Eur Respir J. 2023;61(1):2200837. doi:10.1183/13993003.00837-2022
22. Juniper EF, Guyatt GH, Cox FM, Ferrie PJ, King DR. Development and validation of the mini asthma quality of life questionnaire. Eur Respir J. 1999;14(1):32–38. doi:10.1034/j.1399-3003.1999.14a08.x
23. Nathan RA, Sorkness CA, Kosinski M, et al. Development of the asthma control test: a survey for assessing asthma control. J Allergy Clin Immunol. 2004;113(1):59–65. doi:10.1016/j.jaci.2003.09.008
24. Su N, Zhi L, Liu F, et al. Real-world safety and effectiveness of omalizumab in moderate to severe allergic asthma patients in china: a post-authorization study. J Asthma Allergy. 2023;16:625–636. doi:10.2147/JAA.S406628
25. Rojo-Tolosa S, González-Gutiérrez MV, Sánchez-Martínez JA, et al. Impact of omalizumab in patients with severe uncontrolled asthma and possible predictive biomarkers of response: a real-life study. Pharmaceutics. 2023;15(2):523. doi:10.3390/pharmaceutics15020523
26. Menzella F, Galeone C, Formisano D, et al. Real-life efficacy of omalizumab after 9 years of follow-up. Allergy Asthma Immunol Res. 2017;9(4):368–372. doi:10.4168/aair.2017.9.4.368
27. Menzella F, Fontana M, Contoli M, et al. Efficacy and safety of omalizumab treatment over a 16-year follow-up: when a clinical trial meets real-life. J Asthma Allergy. 2022;15:505–515. doi:10.2147/JAA.S363398
28. Campisi R, Crimi C, Intravaia R, et al. Adherence to omalizumab: a multicenter ”real-world” study. World Allergy Organ J. 2020;13(2):100103. doi:10.1016/j.waojou.2020.100103
29. Pilette C, Canonica GW, Chaudhuri R, et al. REALITI-A study: real-world oral corticosteroid-sparing effect of mepolizumab in severe asthma. J Allergy Clin Immunol Pract. 2022;10(10):2646–2656. doi:10.1016/j.jaip.2022.05.042
30. Pavord I, Gardiner F, Heaney LG, et al. Remission outcomes in severe eosinophilic asthma with mepolizumab therapy: analysis of the REDES study. Front Immunol. 2023;14:1150162. doi:10.3389/fimmu.2023.1150162
31. Rojo-Tolosa S, González-Gutiérrez MV, Jiménez-Gálvez G, et al. Impact of Anti-IL5 therapies on patients with severe uncontrolled asthma and possible predictive biomarkers of response: a real-life study. Int J Mol Sci. 2023;24(3):2011. doi:10.3390/ijms24032011
32. Korn S, Milger K, Skowasch D, et al. Real-world experience on the use of mepolizumab from the severe asthma registry of the German asthma net (MepoGAN-Study). J Asthma Allergy. 2023;16:541–552. doi:10.2147/JAA.S403286
33. González-Pérez R, Poza-Guedes P, Mederos-Luis E, Sánchez-Machín I. Real-life performance of mepolizumab in T2-high severe refractory asthma with the overlapping eosinophilic-allergic phenotype. Biomedicines. 2022;10(10):2635. doi:10.3390/biomedicines10102635
34. Jackson DJ, Burhan H, Menzies-Gow A, et al. Benralizumab effectiveness in severe asthma is independent of previous biologic use. J Allergy Clin Immunol Pract. 2022;10(6):1534–1544.e4. doi:10.1016/j.jaip.2022.02.014
35. Di Bona D, Minenna E, Albanesi M, Nettis E, Caiaffa MF, Macchia L. Benralizumab improves patient reported outcomes and functional parameters in difficult-to-treat patients with severe asthma: data from a real-life cohort. Pulm Pharmacol Ther. 2020;64:101974. doi:10.1016/j.pupt.2020.101974
36. Martínez-Moragón E, García-Moguel I, Nuevo J, Resler G. ORBE study investigators. Real-world study in severe eosinophilic asthma patients refractory to anti-IL5 biological agents treated with benralizumab in Spain (ORBE study). BMC Pulm Med. 2021;21(1):417. doi:10.1186/s12890-021-01785-z
37. Vultaggio A, Aliani M, Altieri E, et al. Long-term effectiveness of benralizumab in severe eosinophilic asthma patients treated for 96-weeks: data from the ANANKE study. Respir Res. 2023;24(1):135. doi:10.1186/s12931-023-02439-w
38. Scioscia G, Carpagnano GE, Quarato CMI, et al. Effectiveness of benralizumab in improving the quality of life of severe eosinophilic asthmatic patients: our real-life experience. Front Pharmacol. 2021;12:631660. doi:10.3389/fphar.2021.631660
39. Dupin C, Belhadi D, Guilleminault L, et al. Effectiveness and safety of dupilumab for the treatment of severe asthma in a real-life French multi-centre adult cohort. Clin Exp Allergy. 2020;50(7):789–798. doi:10.1111/cea.13614
40. Campisi R, Crimi C, Nolasco S, et al. Real-world experience with dupilumab in severe asthma: one-year data from an Italian named patient program. J Asthma Allergy. 2021;14:575–583. doi:10.2147/JAA.S312123
41. Fukunaga K, Tagaya E, Ishida M, Sunaga Y, Koshiba R, Yokoyama A. Real-world impact of dupilumab on asthma disease burden in Japan: the CROSSROAD study. Allergol Int. 2023;72(4):537–544. doi:10.1016/j.alit.2023.04.001
42. Pelaia C, Lombardo N, Busceti MT, et al. Short-term evaluation of dupilumab effects in patients with severe asthma and nasal polyposis. J Asthma Allergy. 2021;14:1165–1172. doi:10.2147/JAA.S328988
43. Pelaia C, Benfante A, Busceti MT, et al. Real-life effects of dupilumab in patients with severe type 2 asthma, according to atopic trait and presence of chronic rhinosinusitis with nasal polyps. Front Immunol. 2023;14:1121237. doi:10.3389/fimmu.2023.1121237
44. Pelaia C, Calabrese C, Terracciano R, de Blasio F, Vatrella A, Pelaia G. Omalizumab, the first available antibody for biological treatment of severe asthma: more than a decade of real-life effectiveness. Ther Adv Respir Dis. 2018;12:1753466618810192. doi:10.1177/1753466618810192
45. Pelaia G, Canonica GW, Matucci A, Paolini R, Triggiani M, Paggiaro P. Targeted therapy in severe asthma today: focus on immunoglobulin E. Drug Des Devel Ther. 2017;11:1979–1987. doi:10.2147/DDDT.S130743
46. Samitas K, Delimpoura V, Zervas E, Gaga M. Anti-IgE treatment, airway inflammation and remodelling in severe allergic asthma: current knowledge and future perspectives. Eur Respir Rev. 2015;24(138):594–601. doi:10.1183/16000617.00001715
47. Buhl R, Marco AG, Cohen D, Canonica GW. Eligibility for treatment with omalizumab in Italy and Germany. Respir Med. 2014;108(1):50–56. doi:10.1016/j.rmed.2013.10.026
48. Al Ahmad M, Borboa Olivares LM, Cardoso AP, et al. Real-life effectiveness of omalizumab in patients with severe allergic asthma: RELIEF study. Open Respir Med J. 2022;16:e187430642206130.
49. Cabrejos S, Moreira A, Ramirez A, et al. FENOMA Study: achieving Full Control in Patients with Severe Allergic Asthma. J Asthma Allergy. 2020;13:159–166. doi:10.2147/JAA.S246902
50. Pelaia C, Calabrese C, Barbuto S, et al. Omalizumab lowers asthma exacerbations, oral corticosteroid intake and blood eosinophils: results of a 5-YEAR single-centre observational study. Pulm Pharmacol Ther. 2019;54:25–30. doi:10.1016/j.pupt.2018.11.002
51. Domínguez-Ortega J, Mullol J, Álvarez Gutiérrez FJ, et al. The effect of biologics in lung function and quality of life of patients with united airways disease: a systematic review. J Allergy Clin Immunol Glob. 2023;3(1):100174. doi:10.1016/j.jacig.2023.100174
52. Israel E, Canonica GW, Brusselle G, et al. Real-life effectiveness of mepolizumab in severe asthma: a systematic literature review. J Asthma. 2022;59(11):2201–2217. doi:10.1080/02770903.2021.2008431
53. Harrison T, Canonica GW, Chupp G, et al. Real-world mepolizumab in the prospective severe asthma REALITI-A study: initial analysis. Eur Respir J. 2020;56(4):2000151. doi:10.1183/13993003.00151-2020
54. Casale T, Molfino NA, Silver J, et al. Real-world effectiveness of mepolizumab in patients with severe asthma and associated comorbidities. Ann Allergy Asthma Immunol. 2021;127(3):354–362.e2. doi:10.1016/j.anai.2021.05.021
55. Crimi C, Campisi R, Cacopardo G, et al. Real-life effectiveness of mepolizumab in patients with severe refractory eosinophilic asthma and multiple comorbidities. World Allergy Organ J. 2020;13(9):100462. doi:10.1016/j.waojou.2020.100462
56. Menzella F, Lusuardi M, Galeone C, Facciolongo N, Zucchi L. The clinical profile of benralizumab in the management of severe eosinophilic asthma. Ther Adv Respir Dis. 2016;10(6):534–548. doi:10.1177/1753465816667659
57. Castro M, Corren J, Pavord ID, et al. Dupilumab efficacy and safety in moderate-to-severe uncontrolled asthma. N Engl J Med. 2018;378(26):2486–2496. doi:10.1056/NEJMoa1804092
58. Menzies-Gow A, Mansur AH, Brightling CE. Clinical utility of fractional exhaled nitric oxide in severe asthma management. Eur Respir J. 2020;55(3):1901633. doi:10.1183/13993003.01633-2019
59. Wechsler ME, Klion AD, Paggiaro P, et al. Effect of dupilumab on blood eosinophil counts in patients with asthma, chronic rhinosinusitis with nasal polyps, atopic dermatitis, or eosinophilic esophagitis. J Allergy Clin Immunol Pract. 2022;10(10):2695–2709. doi:10.1016/j.jaip.2022.05.019
60. Guttman-Yassky E, Bissonnette R, Ungar B, et al. Dupilumab progressively improves systemic and cutaneous abnormalities in patients with atopic dermatitis. J Allergy Clin Immunol. 2019;143(1):155–172. doi:10.1016/j.jaci.2018.08.022
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.