")
Back to Journals » Clinical Optometry » Volume 16
Dichoptic Rescue for Spectacle-Flip Sabotage of Anisometropic Amblyopia Therapy
Authors Arnold RW
Received 11 December 2023
Accepted for publication 19 February 2024
Published 5 March 2024 Volume 2024:16 Pages 83—87
DOI https://doi.org/10.2147/OPTO.S454342
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Mr Simon Berry
Video abstract presented by Arnold.
Views: 82
Robert W Arnold
Alaska Blind Child Discovery, Alaska Children’s EYE & Strabismus, Anchorage, AK, 99508, USA
Correspondence: Robert W Arnold, Alaska Blind Child Discovery, Alaska Children’s EYE & Strabismus, 3500 Latouche Street #280, Anchorage, AK, 99508, USA, Tel +1 (907)561-1917, Fax +1 (907)563-5373, Email [email protected]
Background: To be successful, amblyopia therapeutic techniques must respond when ingenious (shrewd) amblyopic children sabotage treatment effect by discovering ways(1) to alter those therapy aspects they find frustrating.
Methods: Her guardian consented to IRB-approved study outside typical FDA enrollment guidelines for CureSight dichoptic therapy. Acuity (EVA) and stereopsis was by PEDIG protocols.
Results: A 6-year-old rural Alaska native girl in foster care had previously been diagnosed with anisometropic amblyopia and treated with spectacles and patching but had poor compliance with BCVA 0.9– 1.0 logMAR. She demonstrated exceptional creativity and hyperactivity but had no other medical issues. Atropine was prescribed in addition to her spectacles +5.50+1.00x90 and +0.50+1.00x90, but the patient discovered the rare “Spectacle Flip” method that sabotaged therapeutic impact. She had EVA enrollment acuities of logMAR 0.9 right and − 0.1 left with stereo 400 seconds of arc. After just one month dichoptic therapy 1.5 hours 6 days per week, acuity improved to logMAR 0.7 and − 0.1 with stereo up to 140 second of arc. Four months later acuity was 0.6 right and − 0.2 left. Stereoacuity improved from 400 to 200 arc seconds.
Conclusion: Even when conventional compliance methods fail, dichoptic therapy with eye-tracking has the novel and unique potential to improve amblyopia treatment compliance with real-time monitored fixation compliance and confirmation of correct spectacle wear.
Clinical Trial Registration: NCT06165705.
Plain Language Summary: Dichoptic therapy with eye-tracking improved compliance and achieved de novo acuity and stereo gains in a girl with severe refractory anisometropic amblyopia compounded by the rare complication of topical atropine therapy called “spectacle-flip sabotage”
Keywords: anisometropic amblyopia, compliance, eye tracking, anaglyph
Introduction
Successful amblyopia therapy is at the mercy of compliance.1
The Pediatric Eye Disease Investigator Group (PEDIG) amblyopia treatment studies (ATS) have demonstrated that successful amblyopia therapy for patients younger than 10 years of age with strabismic and/or refractive etiologies involves correction of refractive error, and then consistent part-time occlusion and/or atropine penalization of a non-myopic sound eye.2 Dichoptic therapy, especially the recently approved Curesight (Novasight, Airport City, Israel) can improve amblyopic visual acuity and stereopsis.3 Part of the advantage of Curesight with eye tracking is virtual, real-time monitoring of treatment compliance.
Hyperopic anisometropia is a common cause of profound amblyopia. If spectacles are not prescribed early enough, then anti-suppression therapy such as part-time patching is usually added to the spectacles. If patching compliance is not satisfactory, then atropine 1% is often prescribed for the sound eye. The only way an atropinized, hyperopic sound eye could resolve near images would be to have a high plus lens over it.
A novel treatment is described for a young patient who discovered that Spectacle-flip allowed her to enjoy near video games during amblyopia therapy. The spectacle-flip effectively sabotaged or incapacitated the beneficial value of anisometropic hyperopic glasses plus atropine penalization.
Case Report
A bright 5-year-old Alaska Native girl with severe anisometropic refractive amblyopia had been referred to our pediatric ophthalmology specialty clinic. One year earlier, her optometrist diagnosed her with amblyopia, gave her spectacles and offered part-time patch therapy over her left, sound eye. Unfortunately, in her foster living situation, she peeled off her occlusion patches so the therapy produced family frustration but not better visual acuity.
A confirmatory exam revealed cycloplegic refraction right eye of +6.00 +0.50 x 88 and left eye of +1.00 +0.50 x 92. Her patched HOTV acuities were logMAR 0.9 right eye and logMAR 0.0 left eye. She had stereo acuity 400 seconds of arc and alignment of 5 PD micro-esotropia without nystagmus. Her optic nerves and maculae appeared normal. She was prescribed new spectacles and informed of various additional amblyopia treatment options. The time course of her best corrected visual acuity and stereo acuity are shown in Figure 1. Details (metric and USA) of her clinical course are shown in Table 1.
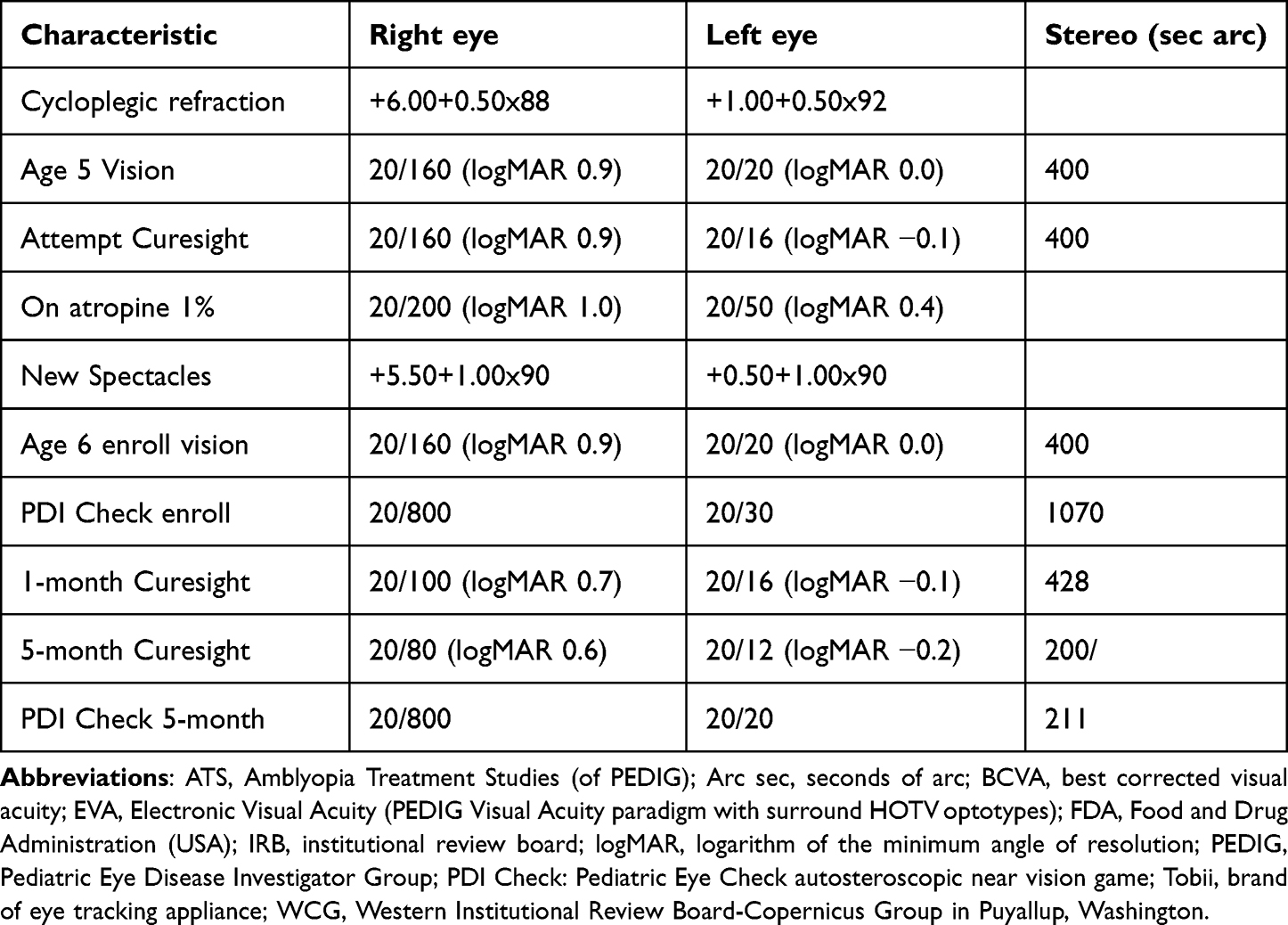 |
Table 1 Characteristics of Anisometropic Amblyopia Patient |
She returned to be considered for the multi-center, USA randomized clinical trial of CureSight dichoptic therapy. Patched, calibrated M&S Clinical Trials Suite EVA surround HOTV acuities were logMAR 0.9 right eye and left eye logMAR −0.1. She had 5 prism diopter distance esodeviation and 400 seconds of arc stereo. Unfortunately, the poor amblyopic visual acuity disqualified her for the Curesight clinical trial, therefore atropine 1% drop daily on weekends was prescribed for the sound, left eye.
 |
Figure 1 Time course of prior and dichoptic amblyopia therapy including spectacle-flip sabotage while on atropine for anisometropia therapy. Notes: Best corrected visual acuity (logMAR) is plotted versus age in months with the amblyopic right [R] eye in blue and the sound left [L] eye in dark red. Stereo acuity in arc seconds shown at the top with details in the text. Comparative mean visual acuity and age for the Israel multicenter CureSight study are superimposed in orange, data from Wygnanski-Jaffe et al.3 |
Over the next three months, she observed that her dominant left eye was blurry for screen viewing with the atropine drop however she discovered she could flip her spectacles placing the higher plus lens in front of her cyclopleged, sound left eye making near work more enjoyable. She either slid her glasses sideways or flipped them upside down. Her spectacles measured +4.50+1.00×90 right amblyopic eye and +0.50+1.00×90 sound left eye. Her guardian was favorably impressed with her new-found interest in near activities. On examination, patched HOTV was logMAR 1.0 right eye and the left atropinized eye diminished to logMAR 0.4. Her guardian was warned about the adverse impact of the flipped-spectacles method of viewing near detail. Atropine was stopped and she was instructed to desist from flipping her spectacles. A special IRB was sought to allow her an option at dichoptic therapy.
The legal guardian provided signed, informed consent to a modification of the CureSight clinical trial that allowed enrollment with worse levels of amblyopia in children over a wider range of entry ages (WCG IRB study number 1349156, Protocol #20230623, Clinical Trials registration NCT06165705). Her enrollment visual acuity was logMAR 0.9 right eye and logMAR 0.0 left eye.
A CureSight table top computer console left over from the USA FDA clinical trial was retro-fit with a new Tobii eye tracking device that was held with magnets below the monitor screen. The patient and guardian were oriented to the device and commenced therapy prescribed as 90 minutes per day, six days per week using home internet delivered content (YouTube videos) that CureSight real-time split into a blue channel for the right amblyopic eye and a red channel that presented eye-tracking aimed central blur when viewed through specifically prescribed anaglyph goggles over her existing spectacles.
After one month of prescribed CureSight, right eye acuity was 0.7 logMAR while the left eye was −0.1 with 140 sec arc Titmus stereo. PDI Check dynamic autostereoscopic stereo was 428 sec arc.4
One month later, WiFi had been less reliable in different home and she was wearing an old pair of spectacles. However she was enjoying 90 minutes per day viewing YouTube on the CureSight. Visual acuity right eye was 0.8 logMAR and left eye −0.2 logMAR however she required being held from creeping up to lean too close to the M&S screen for patched acuity testing. The PDI Check dynamic stereo was 85 seconds of arc stereo.
One month later her compliance for home therapy remained a challenge even though she enjoyed watching the YouTube videos. She tried to view with her spectacles off but the CureSight would remind her not play until correct spectacles were on. She would also dislodge the Tobii eye tracker from its magnetic position, and again the CureSight would not play video until the eye-tracker was in position. Visual acuity right while she tried to peak with sweaty eye patches was logMAR 0.8 in her old glasses and acuity left was logMAR −0.2. PDI Check stereo was 71 seconds of arc. New spectacles were provided.
Two months later with the new spectacles compliance on her CureSight online monitor was a consistent 90 minutes per day and she was enjoying Kindergarten. Visual acuity right eye improved to logMAR 0.6 and left eye logMAR −0.2. Titmus stereo was 200 seconds of arc while PDI Check was 211. Her ocular alignment and refraction remained stable At the conclusion of this intervention, both patient and guardian continued to enjoy the CureSight dichoptic therapy especially compared to their prior experience with patching or atropine.
Discussion
When amblyopia therapy requires compliance several methods have been devised to enhance, monitor and follow patients.5, 6 Occlusion therapy can have compliance improved with elbow splint arm restraints,7 shutter goggles,8 taping over the patch,9 glue on the patch,10 sewn-on occlusion shields11 or opaque contact lenses.12 Blurring the sound eye with a cycloplegic drop like atropine may have better compliance than patching13 and compliance with blur can be enhanced by modifying the lens on the sound eye,14 using Bangerter foils15 and dichoptically blurring part or all of the sound eye image.16 The motivation to comply with therapy can be improved by child-preferred patches,17 more interesting content,18 parent education19 and reward systems.1 The duration of wearing an eye patch or drops for amblyopia therapy can be monitored with a calendar,20 a temperature-under-patch device,21 supervision,22 and eye tracking behavior.3 Clinicians should adapt some of these techniques especially for patients with compliance challenges. The Curesight therapy offers several of these (Central monitoring center calendar and education, interesting content, supervision and eye-tracking) and improves stereo in addition to visual acuity in contrast to the consistent, month-long occlusion of the intra-operative sew-on shield.
Supervision may be the key to superior vision recovery in amblyopia therapy.22 The eye-tracking component of CureSight not only directs the region of sound-eye blur real-time in dichoptic content delivery, but can also monitor level of alertness with fixation losses and blinking, and also whether the spectacles are over the correct eye. Spectacles remain a critical component of amblyopia therapy.23, 24
Spectacle-flip is a rare but feared complication. Our patient loved watching videos, and discovered ways to improve her view. Though not by her deliberate intent, the spectacle-flip effectively sabotaged her conventional atropine/hyperopic anisometropic spectacle therapy. In my experience as a PEDIG investigator since 2000, this patient is my first to suffer from spectacle-flip sabotage of therapeutic efficacy. CureSight for our patient achieved 3 logMAR lines de-novo improvement from her severe amblyopia with a consistent increase in stereopsis. The patient and guardian were still motivated to continue even more dichoptic therapy with child-friendly content. The maximum residual amblyopia acuity retrieval – perhaps even rivalling the sound eye – for a 7-year-old, treated amblyopic child is not yet known.
In conclusion, the orientation and location of sturdy spectacles is a critical aspect of successful amblyopia therapy and must be monitored in some reliable way. Eye tracking, as a component of some types of dichoptic therapy, is a practical real-time tool for precise monitoring of the amblyopia treatment process and duration.
Ethics and Consent
The parent and legal guardian provided signed informed consent for the study. The legal guardian provided signed consent for sharing and publishing of patient images/video for educational purposes. Approval for this study was given by the Alaska Blind Child Discovery department of the Alaska Children’s EYE & Strabismus institution.
Disclosure
Dr. Arnold coordinates the Alaska Blind Child Discovery which has received discounted vision screening technology from several vendors. He was an investigator for the USA Curesight multi-center clinical trial and received Curesight dichoptic devices one of which was modified and used free-of-charge in this separate study. He is a board member for PDI check; In addition, Dr Robert Arnold has a patent Systems and Methods for Eye Evaluation and Treatment issued to Robert W. Arnold and Alex Damarjian.
References
1. Tjiam AM, Holtslag G, Van Minderhout HM, et al. Randomised comparison of three tools for improving compliance with occlusion therapy: an educational cartoon story, a reward calendar, and an information leaflet for parents. Graefes Arch Clin Exp Ophthalmol. 2013;251(1):321–329. doi:10.1007/s00417-012-2107-4
2. Holmes JM, Repka MX, Kraker RT, Clarke MP. The treatment of amblyopia. Strabismus. 2006;14(1):37–42. doi:10.1080/09273970500536227
3. Wygnanski-Jaffe T, Kushner BJ, Moshkovitz A, Belkin M, Yehezkel O, CureSight Pivotal Trial G. An eye-tracking-based dichoptic home treatment for amblyopia: a multicenter randomized clinical trial. Ophthalmology. 2023;130(3):274–285. doi:10.1016/j.ophtha.2022.10.020
4. Smith KA, Damarjian AG, Molina A, Arnold RW. Calibrated measurement of acuity, color and stereopsis on a Nintendo 3DS game console. Clin Optom. 2019;11:47–55. doi:10.2147/OPTO.S199992
5. Le T, Orge F. Treatment compliance in amblyopia: a mini-review and description of a novel online platform for compliance tracking. Surv Ophthalmol. 2022;67(6):1685–1697. doi:10.1016/j.survophthal.2022.08.003
6. Arnold RW, Lichtenstein SJ, Nelson LB. Treatment options for dense amblyopia in uncooperative children. J Pediatr Ophthalmol Strabismus. 2010;47(3):134–138. doi:10.3928/01913913-20100505-01
7. Sabri K, Easterbrook B, Wakeman B, Mehta V, Riyaz R. Elbow splinting as a method to increase patching compliance in amblyopia therapy. Eye. 2017;31(3):406–410. doi:10.1038/eye.2016.222
8. Brown R, Blanchfield P, Fakis A, McGraw P, Foss AJE, Group IBS. Clinical investigation plan for the use of interactive binocular treatment (I-BiT) for the management of anisometropic, strabismic and mixed amblyopia in children aged 3.5-12 years: a randomised controlled trial. Trials. 2019;20(1):437. doi:10.1186/s13063-019-3523-0
9. Clorfeine GS, Parker WT. Use of a transparent film dressing to enhance compliance with occlusion therapy for amblyopia. Am J Ophthalmol. 1992;114(2):229–230. doi:10.1016/S0002-9394(14)73995-9
10. Rubab S, French D, Levin AV. Glued patches for children resistant to amblyopia occlusion therapy. Arch Ophthalmol. 2008;126(1):133–134. doi:10.1001/archophthalmol.2007.27
11. Arnold RW, Armitage MD, Limstrom SA. Sutured protective occluder for severe amblyopia. Arch Ophthalmol. 2008;126(7):891–895. doi:10.1001/archopht.126.7.891
12. Eustis H, Chamberlain D. Treatment for amblyopia: results using occlusive contact lens. J Pediatr Ophthalmol Strabismus. 1996;33:319–322. doi:10.3928/0191-3913-19961101-09
13. Holmes JM, Beck RW, Kraker RT, et al. Impact of patching and atropine treatment on the child and family in the amblyopia treatment study. Arch Ophthalmol. 2003;121(11):1625–1632.
14. G WDK, Lazar EL, Repka MX, et al.; Pediatric Eye Disease Investigator. A randomized trial of adding a Plano lens to atropine for amblyopia. J AAPOS. 2015;19(1):42–48. doi:10.1016/j.jaapos.2014.10.022
15. Rutstein RP, Quinn GE, Lazar EL, et al. A randomized trial comparing Bangerter filters and patching for the treatment of moderate amblyopia in children. Comparative Study. Ophthalmology. 2010;117(5):998–1004 e6.
16. Pineles SL, Aakalu VK, Hutchinson AK, et al. Binocular treatment of amblyopia: a report by the American academy of ophthalmology. Ophthalmology. 2020;127(2):261–272. doi:10.1016/j.ophtha.2019.08.024
17. Dixon-Woods M, Awan M, Gottlob I. Why is compliance with occlusion therapy for amblyopia so hard? A qualitative study. Arch Dis Child. 2006;91(6):491–494. doi:10.1136/adc.2005.090373
18. G HJM, Manny RE, Lazar EL, et al.; Pediatric Eye Disease Investigator. A randomized trial of binocular dig rush game treatment for amblyopia in children aged 7 to 12 years. Ophthalmology. 2019;126(3):456–466. doi:10.1016/j.ophtha.2018.10.032
19. Loudon SE, Passchier J, Chaker L, et al. Psychological causes of non-compliance with electronically monitored occlusion therapy for amblyopia. Br J Ophthalmol. 2009;93(11):1499–1503. doi:10.1136/bjo.2008.149815
20. Holmes JM, Edwards AR, Beck RW, et al. A randomized pilot study of near activities versus non-near activities during patching therapy for amblyopia. J AAPOS. 2005;9(2):129–136. doi:10.1016/j.jaapos.2004.12.014
21. Stewart CE, Moseley MJ, Georgiou P, Fielder AR. Occlusion dose monitoring in amblyopia therapy: status, insights, and future directions. J AAPOS. 2017;21(5):402–406. doi:10.1016/j.jaapos.2017.06.018
22. El-Ghrably IA, Longville D, Gnanaraj L. Does compliance with amblyopia management improve following supervised occlusion treatment? Eur J Ophthalmol. 2007;17(5):823–827. doi:10.1177/112067210701700522
23. Pedig Cotter SA, Edwards AR, et al. Treatment of anisometropic amblyopia in children with refractive correction. Ophthalmology. 2006;113(6):895–903. doi:10.1016/j.ophtha.2006.01.068
24. Yap TP, Luu CD, Suttle C, Chia A, Boon MY. Effect of stimulus orientation on visual function in children with refractive amblyopia. Invest Ophthalmol Vis Sci. 2020;61(5):5. doi:10.1167/iovs.61.5.5
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.