")
Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 15
Diagnostic Performance of Anti-Topoisomerase-I, Anti-Th/To Antibody and Anti-Fibrillarin Using Immunoblot Method in Systemic Sclerosis Related Interstitial Lung Disease Patients
Authors Logito V , Tjandrawati A, Sugianli AK , Tristina N, Dewi S
Received 6 January 2023
Accepted for publication 14 April 2023
Published 28 April 2023 Volume 2023:15 Pages 43—49
DOI https://doi.org/10.2147/OARRR.S403403
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Chuan-Ju Liu
Verina Logito,1,* Anna Tjandrawati,1,* Adhi Kristianto Sugianli,1 Nina Tristina,1 Sumartini Dewi2
1Department of Clinical Pathology, Faculty of Medicine Universitas Padjadjaran/ Dr. Hasan Sadikin General Hospital, Bandung, West Java, Indonesia; 2Division of Rheumatology, Allergy, and Immunology, Department of Internal Medicine, Faculty of Medicine Universitas Padjadjaran/ Dr. Hasan Sadikin General Hospital, Bandung, West Java, Indonesia
*These authors contributed equally to this work
Correspondence: Adhi Kristianto Sugianli, Email [email protected]
Purpose: Systemic Sclerosis related Interstitial Lung Disease (SSc-ILD) is the most common clinical manifestation of SSc with a high morbidity and mortality rate. However, the Thorax High-Resolution Computed Tomography (HCRT) as the gold standard diagnostic tool for SSc-ILD is not widely equipped in health-care facilities. Recently, specific autoantibody examination (anti-topoisomerase-1 (ATA), anti-Th/To antibody, and anti-fibrillarin) has been studied and used for SSc-ILD diagnosis. This study aims to evaluate the diagnostic performance of specific autoantibody examination among SSc-ILD.
Patients and Methods: This retrospective study reviews data from local dedicated SSc database (Sclerosis Systemic Register System Development Electronic Medical Record) which were collected between March 2019 and August 2021. Population of this study include adult inpatients and outpatients at Dr. Hasan Sadikin General Hospital, who have been diagnosed with SSc based on ACR/EULAR 2013 criteria, which met inclusion and exclusion criteria. The SSc patients were grouped into SSc-ILD and SSc non-ILD based on HRCT and tested for SSC-ILD specific autoantibody test (ATA, anti-Th/To antibody, and anti-fibrillarin) to obtain the diagnostic performance (sensitivity, specificity, and positive- and negative-predictive value).
Results: A total of 74 subject grouped into 47 SSc-ILD and 27 SSc-non ILD patients. ATA validity test results showed 85.1% sensitivity, 19.2% specificity, 65.6% PPV, and 41.7% NPV. Anti-Th/To antibody obtained 27.7% sensitivity, 88.9% specificity, 81.3% PPV, and 41.4% NPV. The anti-fibrillarin validity test result showed a 12.8% sensitivity, 96.3% specificity, 85.7% PPV, and 38.8% NPV. The combination of the three parameters had 95.7% sensitivity, 18.5% specificity, 67.1% PPV, and 71.4% NPV.
Conclusion: The combination of the SSc-ILD specific autoantibody test and HCRT is expected to detect all affected patients. Based on these results, SSc-ILD autoantibody-specific test can be used as an alternative examination for screening and diagnosis in health-care facilities that are not equipped with HRCT.
Keywords: SSC-ILD, ATA, anti-Th/To antibody, anti-fibrillarin
Introduction
Systemic Sclerosis (SSc) is an autoimmune disease with progressive chronic characteristics that affects several organs, including skin connective tissue, visceral, and blood vessel walls.1 Furthermore, the condition is characterized by three primary processes: (1) endothelial dysfunction, (2) fibrosis, and (3) autoantibody production. Previous studies revealed that it is very common among people of productive age, with the highest incidence rate occurring in third to fifth decades of life. Women have also been reported to be more susceptible than men with 3–5:1 ratio.2 The disease is often established based on the American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) 2013 criteria, which involves the presence of clinical symptoms and SSc-specific autoantibodies.3 Systemic Sclerosis related Interstitial Lung Disease (SSc-ILD) is the most frequent manifestation of SSc with poor prognosis as well as high morbidity and mortality rate, hence, immediate diagnosis is necessary.4,5
Previous findings showed that there is no consensus describing SSc-ILD diagnosis flow and therapy, but the Thoracic High-Resolution Computed Tomography (HCRT) examination is the accepted gold standard test.6–8 However, this test has a few limitations, including the lack of the required facilities in some hospitals, high costs, and the need for experienced radiologists.9 This indicates that the specific autoantibody test is expected to be one of the modalities to diagnose SSc-ILD patients because it is easier and less expensive. The diagnosis process begins with Indirect Immunofluorescence Anti-Nuclear Antibodies (IIF-ANA) screening, which is later confirmed by SSc-specific autoantibody evaluation, namely ANA/SSc profile.3
A previous study revealed that specific autoantibodies in SSc-ILD include anti topoisomerase-1 (ATA), anti-Th/To antibody, and anti-fibrillarin,5,10,11 and the presence of one of them indicates the tendency for the disease.7 This shows that the test plays an important role in helping clinicians to establish SSc-ILD diagnosis and prognosis.8 It is also expected to be an alternative diagnostic tool for SSc-ILD. Therefore, this study aims to evaluate the diagnostic performance of ATA, anti-Th/To antibody, and anti-fibrillarin with thorax HRCT examination in SSc-ILD.
Materials and Methods
Study Design and Population
This retrospective study reviews data from local dedicated SSc database (Sclerosis Systemic Register System Development Electronic Medical Record) which were collected between March 2019 and August 2021. The population of the database were as follows: (1) adults (aged >18 years old) who were admitted to the inpatients ward in Dr. Hasan Sadikin Hospital Bandung with SSc; (2) adults (aged >18 years old) who were visit to the outpatients Rheumatology clinic in Dr. Hasan Sadikin Hospital Bandung with SSc. The diagnosis of SSc was made based on ACR/EULAR 2013 criteria. The serum among SSc population were collected and archived in the laboratory, according to the laboratory standard operational procedure. From here, all the data were screened for the inclusion and exclusion criteria. The inclusion criteria were (1) reactive IIF-ANA test result of SSc patient with nucleolar pattern (titer ≥1/100), and (2) performed HRCT examination. The exclusion criteria were (1) patient SSc with clinical and/or history of pneumonia, tuberculosis, COVID-19, and malignancy; (2) archive serum collection among SSc population indicate hemolysis, lipemic, and icteric.
Specific Autoantibodies Testing
The archived serum among included population were tested for SSc profile using the immunoblot method (Euroimmun, Germany). The SSc profile strip contains 13 autoantigens, ie Topoisomerase-1/ Scl-70, CENP A, CENP B, RP11 (RNAP-III), RP155 (RNAP-III), fibrillarin, NOR-90, Th/ToRNP, PM-Scl100, PM-Scl75, Ku, PDGFR, and Ro-52, which are expected to react with IgG autoantibodies in human serum. Three SSc-ILD-specific autoantigens, ie Topoisomerase-1, Th/ToRNP, and fibrillarin, were also present on the same strip; hence, the testing was carried out simultaneously. If autoantibodies are present in the serum, their binding to the antigen is captured by alkaline phosphatase-conjugated anti-human-IgG antibodies and appears as blue lines (positive result). The procedure, interpretation, and quality controls for specific autoantibodies testing were performed according to manufacturer’s recommendation.10
Statistical Analysis
The data variables obtained in this study include age, gender, history of therapy, organ involvement, HRCT, and specific autoantibodies testing (ATA, anti-Th/To antibody, and anti-fibrillarin). The age was grouped based on cut-off of 45 years according to disease age prevalence for SSc.1 The SSc population was categorized based on HRCT examination into (1) with interstitial lung disease manifestation (SSc-ILD) and (2) without interstitial lung disease manifestation (SSc non-ILD). The diagnostic performance was carried out using 2×2 tables to obtain sensitivity (Sn), specificity (Sp), positive predictive value (PPV), and negative predictive value (NPV) between SSC-ILD specific autoantibody test (ATA, anti-Th/To antibody, and anti-fibrillarin) against interstitial lung disease manifestation based on HRCT, as the gold standard. The diagnostic performance was analyzed using the Statistical Package for Social Science (SPSS) program (IBM, 2022).
Results
Population Characteristics
A total of 84 subjects were screened from the SSc database, of which 10 were excluded for the following reasons: 1) reactive IIF-ANA test result with titer >1/100 and patterns other than nucleolar; 2) previous history or clinical report of tuberculosis and malignancy. Therefore, 74 subjects was included and categorized into 47 subject SSc-ILD and 27 subject SSc without ILD. The subjects in this study were predominantly female patients of reproductive age (18–45 years) with clinical symptoms characteristic of systemic sclerosis. Most of the patients already have a history of medical therapy. The characteristics of patients used in this study are presented in Table 1.
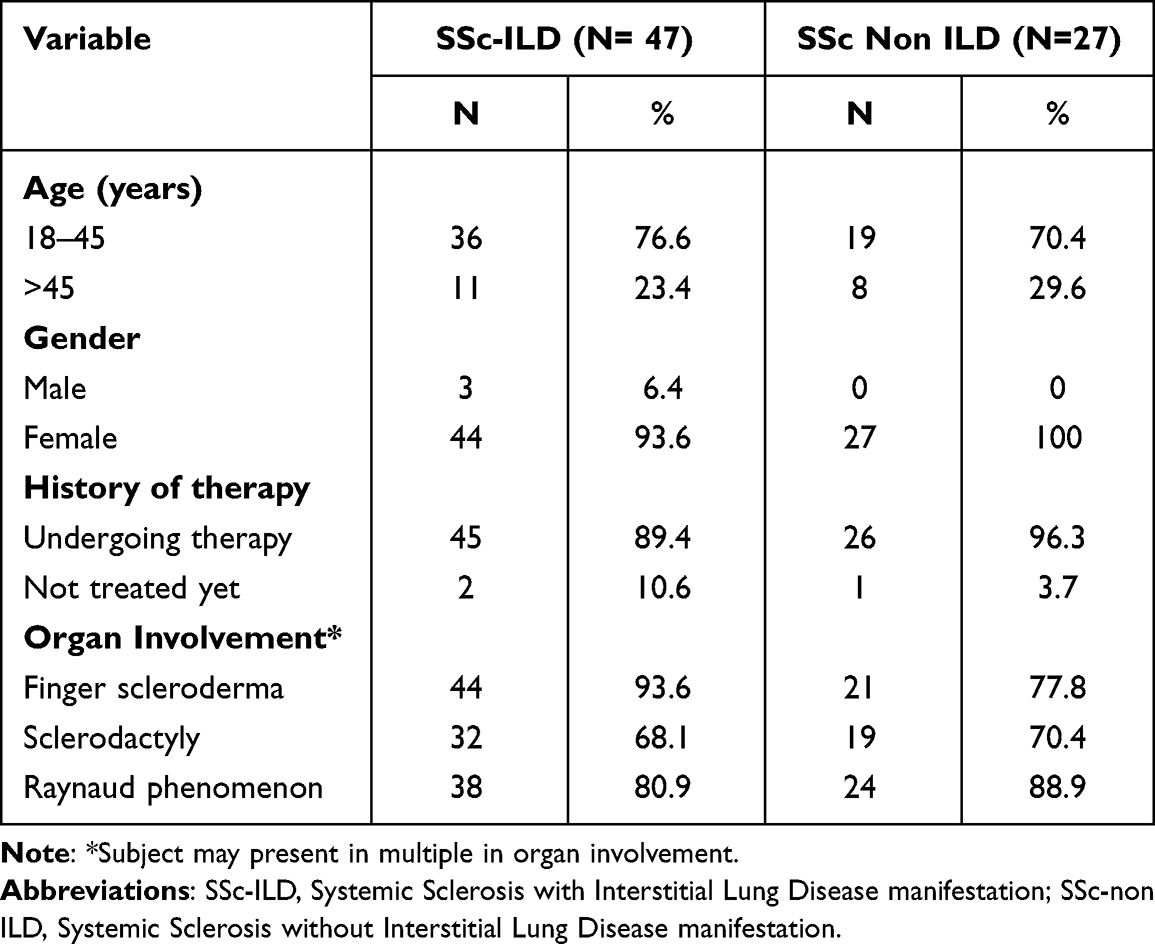 |
Table 1 Subject Characteristics |
Diagnostic Performance of Specific Autoantibodies
We performed systemic Sclerosis related Interstitial Lung Disease-specific autoantibodies (ATA, anti-Th/To antibody, and anti-Fibrillarin) testing against HRCT as a gold standard for diagnosing SSc-ILD (Tables S1–S3). The Anti-Topoisomerase-I sensitivity in SSc-ILD patients was 85,1%, with 19.2% specificity, 65.6% PPV, and 41.7% NPV. The sensitivity of anti-Th/To antibody in SSc-ILD patients was 27.7%, with 88.9% specificity, 81.3% PPV, and 41.4% NPV. The anti-fibrillarin test in SSc-ILD patients had 12.8% sensitivity, 96.3% specificity, 85.7% PPV, and 38.8% NPV. The combination of anti-Th/To antibody and anti-fibrillarin had 31.9% sensitivity, 88.8% specificity, and 83.3% PPV. The combination of ATA, anti-Th/To antibody, and anti-fibrillarin had 95.7% sensitivity, 18.5% specificity, 67.1% PPV, and 71.4% NPV, as shown in Table 2. Furthermore, Table 2 shows that ATA is the SSc-ILD-specific autoantibody with the highest sensitivity, and anti-fibrillarin has the highest specificity.
Discussion
We observe Systemic Sclerosis (SSc) related Interstitial Lung Disease, as an autoimmune disease with progressive chronic characteristics. In this study, the population was dominated by females (95.9%) with aged 18–45 years old. Based on epidemiological data in 2012, Quintero et al reported that SSc was more common among women due to genetic influence and hormones.12 Vinet et al in 2013 stated that the highest incidence rate occurred among women in the productive age group and the rate decreased after menopause.13 Furthermore, all the samples used in the study were diagnosed with diffuse SSc. This finding is consistent with Bahmer et al that 65% of the disease cases were diffuse, and SSc-ILD was the most common manifestation. A previous study revealed that Interstitial Lung Diseases manifested clinically among 40–70% of SSc patients and with 50% mortality in all cases.7
Based on Table S1, a total of 5 samples had a negative ATA specific autoantibody test and the HRCT examination showed SSc non-ILD results. Furthermore, Anti-Topoisomerase-I was frequently found in SSc and SSc-ILD.14 The negative results of anti-Topoisomerase-I are consistent with the SSc non-ILD. HRCT examination with SSc-ILD images and positive ATA tests were found in 40 subjects. In 2016, Bahmer et al revealed that 40–85% of SSc patients with ATA developed into SSc-ILD.7 Seven samples in this study had HRCT examination with SSc-ILD images as well as negative ATA tests, indicating that they were false negatives. Systemic Sclerosis related Interstitial Lung Disease had some specific autoantibodies apart from ATA.15 This showed that seven subjects were SSc-ILD patients with specific autoantibodies aside from ATA, such as anti-fibrillarin, anti-Th/To antibody, anti-PMScl, and anti-Ro52, or other organs are involved in the condition. The results also revealed that 22 samples had HRCT examination with SSc-non ILD images and positive ATA tests, hence, they were false positive. As stated in ACR/EULAR 2013 criteria, SSc-specific autoantibodies include ATA, ACA, and anti-RNAP. Anti-topoisomerase-1 was found in 15–42% of the patients, with specificity ranging between 90% and 100%.14 This indicated that 22 patients had SSc, but not necessarily SSc-ILD. Other possibilities showed they were SSc patients with positive ATA that developed into SSc-ILD. This is consistent with Bahmer et al, 2016 study in Germany, where 40–85% of people with the conditions characterized by ATA developed SSc-ILD after 6 months to 5 years.7
Anti-Topoisomerase-I sensitivity in SSc-ILD patients was 85.1%, with 19.2% specificity, 65.6% PPV, and 41.7% NPV (Table 2). The sensitivity of a test indicates its ability to positively certify sick subjects. Tests with higher values are expected to find more positive test results on affected samples and less of false negatives.16 ATA results in this study had a high sensitivity of 85.1%, and this is consistent with Varga et al, 2015 in America, where ATA was found in 15–42% SSc patients with 90–100% sensitivity.17 The results also showed that this autoantibody had a specificity of 19.2% towards SSc-ILD. The specificity of a test indicates its ability to negatively certify non-sick subjects. Tests with higher values can find more negative test results in non-sick subjects and less of false positives.18 The low specificity of ATA towards SSc-ILD was caused by the presence of several SSc-non ILD subjects (false positive), as well as other autoantibodies. This is consistent with the ACR/EULAR 2013 criteria, where SSc-specific autoantibodies include ATA, ACA, and anti-RNAP.3 Based on the high level of ATA sensitivity towards SSc-ILD, it is expected to serve as a screening marker for the disease.
 |
Table 2 SSc-ILD Specific Autoantibodies Validity Test Against HRCT |
Table S2 shows that there are 24 samples with negative anti-Th/To antibody-specific autoantibody test and HRCT examination with SSc non-ILD images. Furthermore, anti-Th/To antibody was specific, particularly towards SSc-ILD clinical images. Stochmal et al, 2020 showed that the autoantibody had a 2–5% prevalence.5 Negative results for anti-Th/To antibodies were normal for SSc non-ILD patients. A total of 13 samples had HRCT examination with SSc-ILD images and positive anti-Th/To antibody tests. Several studies have revealed that Anti-Th/To antibody was related to ILD. The results also showed that 34 patients had HRCT exam with SSc-ILD images and negative Th/ToRNP, indicating they were false negatives. SSc-ILD has several specific autoantibodies including Th/ToRNP, ATA, and anti-fibrillarin.11 A total of 3 samples had HRCT examination with SSc non-ILD images and positive anti-Th/To antibody, indicating they were false positive. Several studies have revealed that anti-Th/To antibodies are one of SSc autoantibodies with the ability to overlap polymyositis.19,20 Positive anti-Th/RoRNP tests in SSc non-ILD patients could be potentially caused by overlapping case of SSc and polymyositis.
In this study, the sensitivity of anti-Th/To antibody in SSc-ILD patients was 27.7%, with 88.9% specificity, 81.3% PPV, and 41.4% NPV. Based on the high specificity, the autoantibody can be a confirming mark in diagnosing SSc-ILD. Anti-Th/To antibody negative predictive value of 41.4% was caused by the high false-negative numbers in the study. One of the factors that can account for false negatives was autoantigen recombinants in the SSc Profile test. Meanwhile, from HRCT examination factor, this study was considered to be subjective and heavily dependent on operators’ interpretations.9
Based on Table 2, 26 samples had negative anti-fibrillarin specific autoantibody and HRCT examination with SSc non-ILD results. Anti-fibrillarin was frequently found in SSc and was one of the SSc-ILD specific autoantibodies.11 The negative results of anti-fibrillarin were the normal characteristics of SSc non-ILD patients. A total of 6 samples had HRCT examination with SSc-ILD images and positive anti-fibrillarin tests. Anti-fibrillarin has been reported to be associated with ILD. The results also revealed that 41 samples had HRCT exam with SSc-ILD images and negative anti-fibrillarin tests, indicating they were false negatives. A total of 1 patient had an HRCT exam with SSc-non-ILD image and positive anti-fibrillarin test, showing false positive. The anti-fibrillarin test in SSc-ILD patients had 12.8% sensitivity, 96.3% specificity, 85.7% PPV, and 38.8% NPV. Based on the high specificity, anti-fibrillarin can be a confirming marker towards SSc-ILD diagnosis.
The combination of anti-Th/To antibody and anti-fibrillarin had 31.9% sensitivity, 88.8% specificity, and 83.3% PPV, as shown in Table 2. This had no significant difference compared to anti-Th/To antibody or only anti-fibrillarin. The high specificity level was supported by high NPV level. However, this study had higher PPV than NPV due to 1) high level of false negatives; 2) positive anti-Th/To antibody samples and/or low anti-fibrillarin causing higher PPV than NPV, as seen in six subjects with true positive results. The high specificity rate of anti-Th/To antibody and anti-fibrillarin indicates that both specific autoantibodies can be confirming markers of SSc-ILD diagnosis. Based on the results, the high number of true negative results on anti-Th/To and anti-fibrillarin test indicates that the patients are SSc-non ILD if they do not have anti-Th/To and anti-fibrillarin.
Investigation of three SSc-ILD specific autoantibodies, namely ATA, anti-Th/To antibody, and anti-fibrillarin was carried out simultaneously in SSc profile strip test (parallel) to increase their combined sensitivity. This is consistent with results shown in Table 2, where three SSc-ILD specific autoantibodies were combined, and the sensitivity increased up to 95.74%. Anti-topoisomerase-1 had higher and better sensitivity compared to anti-Th/ToRNP and anti-fibrillarin. The combination of the two autoantibodies and HRCT is expected to filter all patients with SSc-ILD diagnosis. Systemic Sclerosis related Interstitial Lung Disease-specific autoantibodies can increase test positivity rate in SSc-ILD. The clinical impact of these results, especially for clinician in Indonesia, is the specific autoantibody test is expected to be one of the modalities to diagnose SSc-ILD patients because it is easier and less expensive. Hopefully, this specific autoantibody examination can help patients who live in remote areas and have economic limitations.
The limitation of this study is that the sample used were from diagnosed SSc patients based on ACR/EULAR 2013 criteria. This caused high sensitivity and low specificity of ATA, while determining if it can be SSc screening mark; hence, other autoimmune diseases must be included.
Conclusion
The results showed that anti-topoisomerase-I had higher and better sensitivity compared to anti-Th/ToRNP and anti-fibrillarin. The combination of this autoantibody with HRCT exam is expected to filter more patients with SSc-ILD diagnosis. Furthermore, the combined use of Th/ToRNP and anti-fibrillarin did not increase specificity towards SSc-ILD. This indicated that the presence of a positive result for one autoantibody can be an indication for SSc-ILD diagnosis. The absence of anti-Th/To and anti-fibrillarin in patients does not exclude diagnosis of SSc-ILD but the high specificity of these autoantibodies from this study can give indications that the patient probably is SSc-non ILD. The use of three SSc-ILD specific autoantibodies, namely ATA, anti-Th/ToRNP, and anti-fibrillarin, can increase positivity rate of specific autoantibody test in SSc-ILD.
Suggestion
SSc-ILD specific autoantibodies of ATA, anti-Th/ToRNP and anti-fibrillarin tests have good validity that can be used as screening test and diagnosing SSc-ILD if a health facility is not equipped with HRCT as gold standard examination.
Ethics Approval and Consent to Participate
The institutional review board of the Faculty of Medicine Universitas Padjadjaran/Dr. Hasan Sadikin General Hospital Bandung, Indonesia approved the protocol #2392020 entitled “Pengembangan Sistem Registri SSc berbasis Electronic Medical Record.” This study was approved by the Health Research Ethics Committee of Dr. Hasan Sadikin General Hospital Bandung with approval no. LB.02.01/X.6.5/239/2020. All procedures followed were in accordance with the ethical standards put forth by the Helsinki Declaration of 1975, as revised in 2000. All patients gave their informed consent to participate in the study, which was approved by the local Ethics Committee of Faculty of Medicine Universitas Padjadjaran/Dr. Hasan Sadikin General Hospital Bandung, Indonesia.
Acknowledgment
This study was supported by an internal research grant from Universitas Padjadjaran Bandung, West Java, Indonesia.
Disclosure
The authors declare no relevant financial disclosures or conflicts of interest.
References
1. Bergamasco A, Hartmann N, Wallace L, Verpillat P. Epidemiology of systemic sclerosis and systemic sclerosis-associated interstitial lung disease. Clin Epidemiol. 2019;11:257. doi:10.2147/CLEP.S191418
2. Jaeger VKWE, Allanore Y; and the EUSTAR co-authors. Incidences and risk factors of organ manifestations in the early course of systemic sclerosis: a longitudinal EUSTAR study. PLoS One. 11;2016:e0163894. doi:10.1371/journal.pone.0163894
3. Van Den Hoogen F, Khanna D, Fransen J, et al. classification criteria for systemic sclerosis: an American College of Rheumatology/European League against Rheumatism collaborative initiative. Arthritis Rheum. 2013;65(11):2737–2747. doi:10.1002/art.38098
4. Diot E, Giraudeau B, Diot P, et al. Is anti-topoisomerase I a serum marker of pulmonary involvement in systemic sclerosis? Chest. 1999;116(3):715–720. doi:10.1378/chest.116.3.715
5. Stochmal A, Czuwara J, Trojanowska M, Rudnicka L. Antinuclear antibodies in systemic sclerosis: an update. Clin Rev Allergy Immunol. 2020;58(1):40–51. doi:10.1007/s12016-018-8718-8
6. Perelas A, Silver RM, Arrossi AV, Highland KB. Systemic sclerosis-associated interstitial lung disease. Lancet Respir Med. 2020;8(3):304–320. doi:10.1016/S2213-2600(19)30480-1
7. Bahmer T, Romagnoli M, Girelli F, Claussen M, Rabe KF. The use of auto-antibody testing in the evaluation of interstitial lung disease (ILD)–A practical approach for the pulmonologist. Respir Med. 2016;113:80–92. doi:10.1016/j.rmed.2016.01.019
8. Cottin V, Brown KK. Interstitial lung disease associated with systemic sclerosis (SSc-ILD). Respir Res. 2019;20(1):13. doi:10.1186/s12931-019-0980-7
9. Takei R, Arita M, Kumagai S, et al. Radiographic fibrosis score predicts survival in systemic sclerosis‐associated interstitial lung disease. Respirology. 2018;23(4):385–391. doi:10.1111/resp.13175
10. Tjandrawati A, Logito V, Saragih WAM, Rahmadi AR, Dewi S. Laboratory strategy for autoantibodies testing as a diagnostic marker of pulmonary fibrosis in systemic sclerosis: a preliminary study prior to cohort registry of systemic sclerosis in West Java Indonesia. Biomed Res Ther. 2021;8(8):4505–4513. doi:10.15419/bmrat.v8i8.689
11. Yang H. Autoantibodies in systemic sclerosis. In: Takehara K, Fujimoto M, Kuwana M, editors. Systemic Sclerosis. Tokyo: Springer; 2016:231–247.
12. Quintero OL, Amador-Patarroyo MJ, Montoya-Ortiz G, Rojas-Villarraga A, Anaya J-M. Autoimmune disease and gender: plausible mechanisms for the female predominance of autoimmunity. J Autoimmun. 2012;38(2–3):J109–J119. doi:10.1016/j.jaut.2011.10.003
13. É V, Bernatsky S, Hudson M, Pineau CA, Baron M. Effect of menopause on the modified Rodnan skin score in systemic sclerosis. Arthritis Res Ther. 2014;16(3):1–7.
14. Aleksandrov A, Shilova L, Aleksandrov V. Oral and poster abstracts. J Scleroderma Relat Disord. 2020;5(1_suppl):1–307. doi:10.1177/2397198319898367
15. Didier K, Bolko L, Giusti D, et al. Autoantibodies associated with connective tissue diseases: what meaning for clinicians? Front Immunol. 2018;9:541. doi:10.3389/fimmu.2018.00541
16. Wong HB, Lim GH. Measures of diagnostic accuracy: sensitivity, specificity, PPV and NPV. Proc Singapore Healthc. 2011;20(4):316–318. doi:10.1177/201010581102000411
17. Varga JLR. Etiology and pathogenesis of systemic sclerosis. In: Rheumatology. Philadelphia: Elsevier; 2015:1177–1185.
18. Simon R. Sensitivity, specificity, PPV, and NPV for predictive biomarkers. JNCI. 2015;107:8. doi:10.1093/jnci/djv153
19. Hudson M, Pope J, Mahler M, et al. Clinical significance of antibodies to Ro52/TRIM21 in systemic sclerosis. Arthritis Res Ther. 2012;14(2):R50. doi:10.1186/ar3763
20. Mecoli C, Gutierrez-Alamillo L, Yang Q, et al. PM-Scl and Th/To in systemic sclerosis: a comparison of different autoantibody assays. Clin Rheumatol. 2021;40:1–7.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.