")
Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 15
Dental Caries in Children with Sickle Cell Disease and Its Association with the Use of Hydroxyurea and Penicillin Prophylaxis in Dar Es Salaam
Authors Minja IK , Wilson EM, Machibya FM, Jonathan A, Cornel F, Ruggajo P, Makani J , Balandya E
Received 4 October 2023
Accepted for publication 8 February 2024
Published 22 March 2024 Volume 2024:15 Pages 121—128
DOI https://doi.org/10.2147/PHMT.S443139
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Irene Kida Minja,1,2,* Evarist Mulyahela Wilson,1,2,* Ferdinand M Machibya,3 Agnes Jonathan,2 Fortunata Cornel,1 Paschal Ruggajo,2,4 Julie Makani,2,5 Emmanuel Balandya2,6
1Department of Restorative Dentistry, Muhimbili University of Health and Allied Sciences, Dar es Salaam, Tanzania; 2The Sickle Pan African Research Consortium (SPARCO) – Tanzania Site Project, Muhimbili University of Health and Allied Sciences, Dar es Salaam, Tanzania; 3Department of Orthodontics, Pedodontics and Community Dentistry, Muhimbili University of Health and Allied Sciences, Dar es Salaam, Tanzania; 4Department of Internal Medicine, Muhimbili University of Health and Allied Sciences, Dar es Salaam, Tanzania; 5Department of Hematology and Blood Transfusion, Muhimbili University of Health and Allied Sciences, Dar es Salaam, Tanzania; 6Department of Physiology, Muhimbili University of Health and Allied Sciences, Dar es Salaam, Tanzania
*These authors contributed equally to this work
Correspondence: Irene Kida Minja, Department of Restorative Dentistry, Muhimbili University of Health and Allied Sciences, P. O. Box 65014, Dar es Salaam, Tanzania, Tel +255 763 00 0333, Fax +255 22 215 0465, Email [email protected]
Purpose: This comparative study sets out to report dental caries status among individuals with Sickle Cell Disease (HbSS) against those with sickle cell trait (HbSA) and those without the disease (HbAA) as controls. The study further assessed the impact of penicillin chemoprophylaxis and hydroxyurea use on dental caries among Sickle Cell Disease participants.
Methods: This was a comparative cross-sectional study in which 93 children aged 30 to 60 months were recruited. There were 60 participating children who had SCD (HbSS), 17 with SCD trait (HbAS) and 16 were without SCD or SC trait (HbAA). A questionnaire was used to record sociodemographic details including mean age in months and sex and on haemoglobin genotype for all the participants. Specifically, for the participants with HbSS, information on their whether they are taking hydroxyurea (HU), and penicillin chemoprophylaxis was recorded. To assess the prevalence of dental caries, clinical examination of all primary maxillary and mandibular teeth to determine the presence or absence of dental caries lesions was also recorded.
Results: A total of 1197 teeth from 93 children were examined, whereby, 45 (2.4%) of them had dental caries. The participating children with HbAA genotype (6.6%, N=21) had more dental caries than their HbSS counterparts (2.0%, N=24), while none of the participants with HbAS exhibited dental caries. Among the participants with HbSS, males and those who use HU were 3.79 and 3.07 times more likely to have dental caries than their counterparts, female and non-users of HU, respectively.
Conclusion: Dental caries was observed to be low among participants with HbSS when compared to those with HbAA. More research utilizing more robust methodologies is recommended.
Keywords: caries, dental health, hemoglobin, oral health, sickle cell anaemia, sickle cell disease
Introduction
Sickle cell disease (SCD) a condition resulting from the inheritance of mutant hemoglobin following the replacement of glutamic acid at position six of the beta globin chain is a global health concern.1 The estimated global incidence of SCD is 515,000 (425,000–614,000) neonates annually, the majority of which are from sub-Saharan Africa, according to the Global Burden of Disease 2021, SCD Collaborators.2 There are different hemoglobin genotypes of SCD, which differ geographically and how they manifest clinically. The predominating ones include SCD-Hemoglobin SS (HbSS), HbSC, Hb β+-Thalassemia and Hb β0-Thalassemia, and rarely HbSD and HbSE to name a few.3 Tanzania ranks fourth in patients with HbSS birth rates in Africa, while 13% to 20% exhibit SCD trait Haemoglobin AS (HbAS).4,5 SCD affects almost every organ and system in the human body resulting from abnormal structure and functionality of sickle erythrocytes by impairing the rheology, elasticity and oxygen-carrying capacity of erythrocytes, ultimately reducing patient survival and jeopardizing their quality of life.6,7 In oral and maxillofacial region, SCD is reported to be associated with midfacial overgrowth, asymptomatic pulp necrosis, gingival enlargement, paresthesia of the mandibular nerve, and osteomyelitis of the jaws, mostly mandible.8,9 Other conditions reported to be associated with SCD are delayed tooth eruption, hypo calcification, and hypo maturation of both enamel and dentine.10
Dental caries is a microbiological condition that involves demineralization of tooth tissue by acids produced by cariogenic bacteria action (mainly, the Streptococcus mutans) on fermentable carbohydrates, with outcomes ranging from a small enamel lesion and cavitation to pulp involvement. Studies on the association between SCD and dental caries are still inconclusive.11 However, it has been noted that enamel and dentine hypoplasia and hypocalcification common in individuals with SCD increase their susceptibility to dental caries by providing a suitable environment for attachment and colonization for cariogenic bacteria.12 Thus, in the presence of cariogenic sugars, fermentation occurs and produces acids that change pH in favor of demineralization, with the subsequent dissolution of the organic part of the tooth leading to cavitation on the tooth.13 Studies that compared dental caries status among participants with SCD and those without it showed that the condition affected participants with SCD more than those without SCD.14 Several cost-effective interventions to reduce mortality and harmful complications of SCD have been used with evidence-based beneficial effects. These include newborn screening for early detection and patient care. Care for patients with SCD comprise continuous monitoring of clinical parameters such as hemoglobin (Hb) levels, provision of medication to modify disease severity and to prevent infection including folic acid supplementation, pneumococcal and other vaccinations, malaria prevention and use of penicillin chemoprophylaxis to prevent infections and hydroxyurea (HU).15 Information on how these clinical parameters and systemic therapies impact oral health is limited.16 For instance, penicillin chemoprophylaxis against frequent infections might be protective against the chief cariogenic bacteria, Streptococcus mutans thus lowering the risk for dental caries.16,17 However, de Matos and coworkers observed no difference in dental caries prevalence and bacteria (Lactobacilli and Streptococcus) count between individuals on long-term penicillin prophylaxis and controls.18 Another medication HU is a disease-modifying drug that induces fetal haemoglobin (HbF). HbF is the type of Hb responsible for reducing SCD complications by preventing red blood cells (RBCs) from undergoing sickling.19 The presence of HbF has been seen to minimize the effects of HbS hence the use of HU has been reported to reduce the frequency of pain crises and minimize the need for hospitalization as well as blood transfusion to name a few.20 However, studies on the oral health effects of HU report a higher percentage of SCD individuals on HU exhibiting a reduction in salivary buffering capacity (pH less than 5.5) and low salivary flow rate, compared to those who were not on HU.14 Furthermore, a higher decayed, missing, and filled teeth (dmft) score was found among the SCD group on HU.14 Altered saliva plays a role in the development of caries lesions, hence oral health-care interventions are necessary to offset these effects.14
Of recent, studies that assess dental caries among patients with SCD in Tanzania could not be retrieved. This study comparably reports dental caries status among individuals with HbSS, with HbAS and HbAA as controls. The study also assessed the impact of penicillin prophylaxis and hydroxyurea use among SCD patients against non-users.
Materials and Methods
This was a comparative cross-sectional study of 93 children (1857 teeth) aged 30 to 60 months, among which 60 participants (1197 teeth) had SCD (HbSS); against 17 participants (340 teeth) with SCD trait (HbAS) and 16 participants (320 teeth) without SCD (HbAA) as controls. The sample size was calculated by considering the prevalence of decayed teeth among those without SCD to be 50% and the difference in prevalence of 30% with the power of 80%, significance level of 0.05 and attrition rate of 10%. This yielded a total sample size of 73 participants per group (73 participants with HbSS, and controls 37 participants with HbAS and 37 with HbAA). Participants with HbSS with confirmed hemoglobin electrophoresis results were recruited from Sickle cell clinics at the Muhimbili National Hospital, and two Regional Referral Hospitals (Temeke and Amana) in Dar es Salaam. Children (30 to 60 months) were recalled from the Muhimbili Sickle Cell Program database and enrolled to serve as controls with HbAS and HbAA genotypes. Details on participants and recruitment process have been described previously.21
The Questionnaire
A questionnaire was used to record sociodemographic details including age in months and sex and on hemoglobin genotype for all the participants. Among participants with HbSS, information on whether they are taking medication for SCD ie, hydroxyurea, and penicillin chemoprophylaxis was obtained from the parent/care giver and confirmed on the patient record at the clinic.
Clinical Examination
After the interviews, one trained and calibrated author (EW) conducted clinical examination of all primary maxillary and mandibular teeth for the presence or absence of carious lesions. The presence of an active carious lesion on any of the primary teeth by visual examination was recorded. The examination was conducted with a child lying on a hospital bed or dental chair. Teeth were cleaned and dried with sterile gauze prior to recording caries status. Natural light was used for all participants. The criteria for diagnosis of an active carious lesion included color change, visual-tactile and obvious cavitation on the tooth with or without pain. Participants with tooth developmental defects and severe SCD symptoms were excluded from the study.
Data Analysis
Data were analyzed with the tooth as a unit of analysis, using StataCorp. 2017. Stata Statistical Software: Release 15. College Station, TX: StataCorp LLC. Age, sex, hemoglobin genotype, and medications were considered independent variables, whereas dental caries status was the dependent variable. Age of participants was summarized as mean, and sex was analyzed using the frequency distribution of boys and girls, and hemoglobin genotype as the frequency distribution of those with HbSS, HbAS, and HbAA as controls. Comparison of the prevalence of teeth with dental caries across the three groups (HbSS, HbAS, and HbAA) was done by chi-square test. Additionally, cross-tabulations on dental caries against users of Hydroxyurea (HU) and penicillin prophylaxis were conducted among participants with HbSS. The level of statistical significance was set at P < 0.05. Variables found to be significant at the bivariate level were further entered into multiple regression analysis.
Ethical Consideration
This study made sure to comply with the Declaration of Helsinki. Ethical approval for this study (MUHAS-REC-07-2020-317) was provided by the Research and Ethics Committee of the Muhimbili University of Health and Allied Sciences (MUHAS). Permission to conduct the study was obtained from hospitals hosting SCD clinics. Written informed consent to participate in the study was obtained from parents before participation. Tailored oral health information, advice, and oral hygiene instructions were provided to the parent/guardian and children after the interview and oral examination.
Results
Socio-Demographic Characteristics and Prevalence of Dental Caries Among HbSS, HbAS and HbAA Participants
Table 1 shows the characteristics of participants’ sociodemographic details, with participants in the HbAS group having more girls (64.7%, N=11) than boys (35.3%, N=6). Furthermore, Table 1 shows that children with HbSS had a statistically higher mean age of 50.1±8.7SD months than those with HbAS (39.9± 5.4SD months) and HbAA (38.9±6.9SD months) with p=0.006.
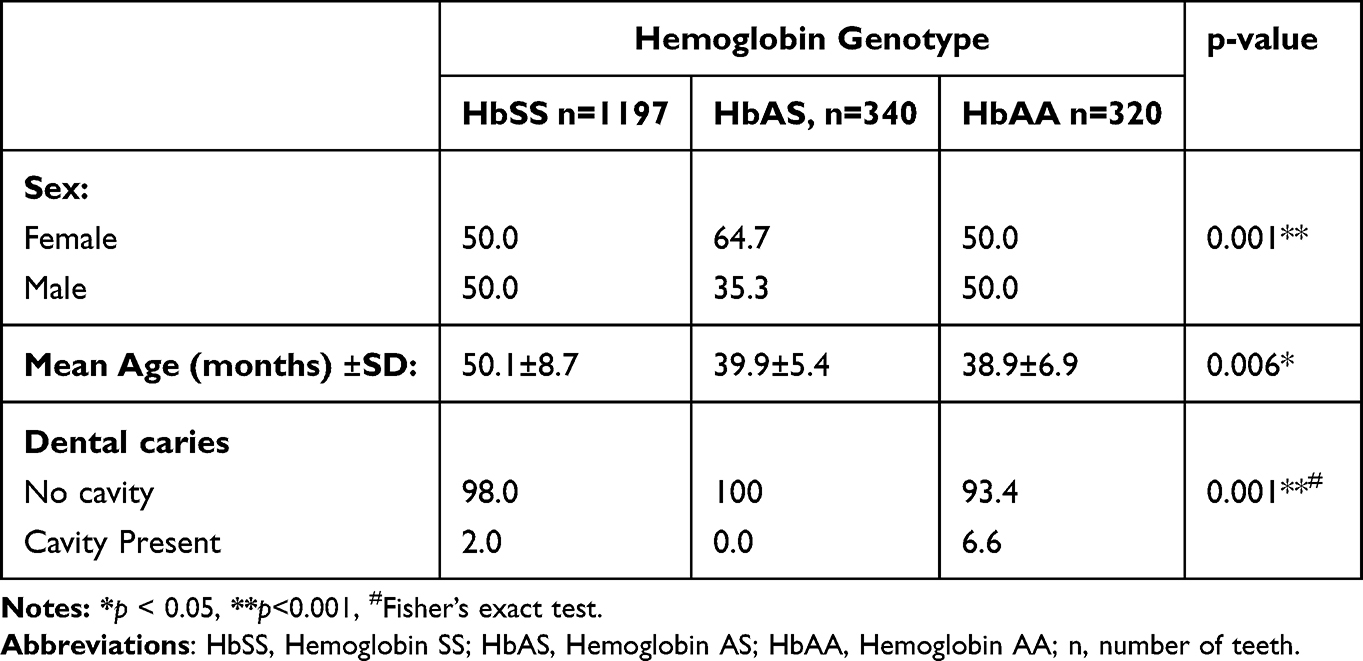 |
Table 1 Percent Distribution of Study Participants in Different Categories of Hemoglobin Genotype by Sex and Age. Chi-Square Test and Independent t-test of the Mean |
Overall, a total of 1857 teeth were examined in 93 children for dental caries distributed as follows: 1197 (HbSS), 340 (HbAS), and 320 (HbAA). Furthermore, a total of three (3) teeth were found to be unerupted among the participants with the HbSS genotype. Among all the examined participants, there were 45 teeth diagnosed with dental caries, giving an overall prevalence of 2.4% (Table 1). There was a statistically significant difference in prevalence of dental caries across the three groups, where HbSS, HbAS, and HbAA, had a prevalence of 2%, 0%, and 6.6%, respectively, p = 0.000 (Table 1)
Predictors of Dental Carries Among Participants with Sickle Cell Disease
Further analysis specifically for children with HbSS, 16.7% (N=10) reported the use of HU, while those who reported the use of penicillin prophylaxis were 95% (N=57) (Table 2). As depicted in Table 2, male participants and HU users showed statistically significantly more caries teeth than their counterparts’ female participants and HU non-users, respectively. Age and those on penicillin chemoprophylaxis showed no significant association with dental caries. According to Table 3, when sex and HU-use were entered into a multivariable logistic regression model, being male and users of HU were 3.79 (CI: 1.24–11.6) and 3.07 (CI: 1.32–7.17) times more likely to have teeth with dental caries than their counter parts female and non-users of HU after adjusting for other factors, respectively.
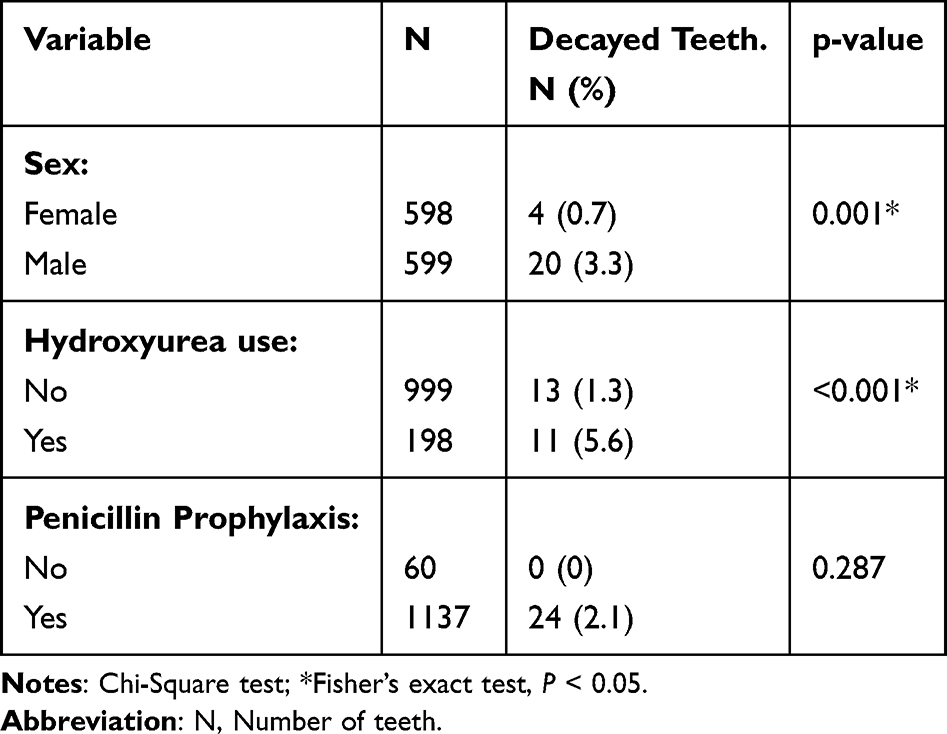 |
Table 2 Number of Decayed Teeth (Percent) of Children with Sickle Cell Disease (HbSS) According to Their Socio Demography, and the Use of Hydroxyurea and Penicillin Prophylaxis. Chi-Square Total N = 1197 |
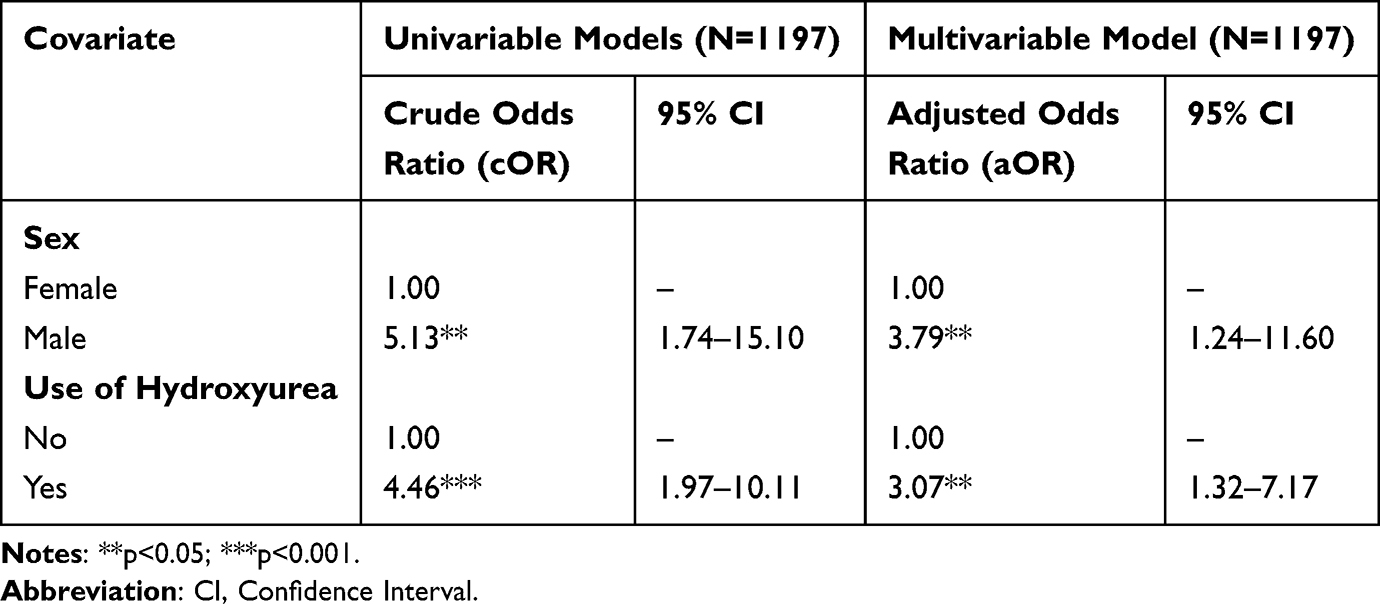 |
Table 3 Univariate and Multivariable Logistic Regression Analysis of Factors Associated with Decayed Teeth Among Children with SCD (HbSS) |
Discussion
Sickle cell disease (SCD) negatively affects organs and tissues in the body including oral health structures.22,23 Here, we show for the first time that the prevalence of dental caries in children with SCD (HbSS) in Tanzania was low compared to their HbAS and HbAA counterparts. Furthermore, we show that dental caries in children with SCD were significantly associated with male sex and use of hydroxyurea. Although the prevalence of dental caries was lower in patients with SCD, our findings call for future studies to investigate the increased risk of caries among male SCD patients and those on hydroxyurea.
This study included teeth of children aged 30 to 60 months with the expectation that, at this age, all children will have all their deciduous teeth erupted. On the contrary, a total of three teeth were missing and all were observed among children with HbSS genotype (n=1197). The latter was observed despite the significantly higher mean age among children with HbSS who are expected to have all their teeth erupted (Table 1). Delayed eruption has been observed to be common among children with SCD, however, this could not be ascertained in the current study warranting further investigations in this aspect.24,25
The prevalence of dental caries, in terms of number of decayed teeth, among the participants in this study is low (2.4%) when compared to that of the under-five year olds in the Tanzanian general population. According to Tanzania National Oral Health Survey, three out of ten under-fives have caries experience. This difference could probably be due to the recruitment criteria of obtaining participants who are regular SCD clinic attendees.21 Regarding dental caries according to participant genotype, the current study showed a low prevalence of dental caries among participants with HbSS genotype, a figure that was significantly lower than that of participants with HbAA genotype. Previous reports showed higher numbers of decayed teeth among individuals living with SCD than among non-SCD patients.14,26 However, other scholars could not establish a significant difference in dental caries experience among SCD patients when compared to non-SCD individuals.27 A scoping review of studies that investigated the level of caries among SCD patients showed inconsistent results in terms of the correlation between dental cavities and SCD.16 These contradicting findings could be due to differences in methodologies and geographical regions.
This study went further into analyzing the role of dental caries among participants with HbAS genotype, which has not been studied much. None of the children with HbAS was found to have dental caries. The lower proportion of caries among participants with HbSS as well as those with HbAS could be due to a number of factors: The fact that the participants were recruited from the SCD clinics could be the reason for the low disease burden. Similarly, children with HbAS, the majority of whom were siblings of those with HbSS could be protected through this concept. This finding could provide an opportunity for planned interventions to improve oral health of children with HbSS which could spill over to their siblings, though more research is needed to affirm this hypothesis. Other scholars in countries with community water fluoridation as caries preventive strategy attributed the low caries among SCD patients who are routinely encouraged to drink plenty of water to prevent sickling of RBCs, ultimately increasing exposure to preventive effects of fluoride.28 The latter could not be a possible reason for the current lower level of caries among children with HbSS, since water fluoridation is not advocated in Tanzania. Thus, more research is required to confirm protective effects of frequent oral re-hydration with or without fluoridation.
Further analysis of participants with HbSS showed that male participants were at higher odds of having dental caries, which corroborates with findings among children in Brazil reporting boys having more caries, though not statistically significant.29 While sociodemographic characteristics of populations such as sex and age may count as risk factors to dental caries, the answer as to why boys were most affected among children with SCD in Tanzania, requires more research to elucidate this result.
Almost all (95%) of the children with HbSS were under penicillin chemoprophylaxis to prevent infection, which is highly commendable. The use of penicillin chemoprophylaxis early in childhood is reported to have protective effect from dental caries.30 This is due to the effect that the medication has on preventing the accumulation of Streptococcus mutans, a microbe that is responsible for causing dental caries.17,18 These studies found lower levels of Streptococcus mutans specifically during the active period of administration of the drug, probably the reason for low level of dental caries among participants in this study. On the contrary, since penicillin prophylaxis’ effectiveness in reducing Streptococcus mutans diminishes with age, this underscores the need for continuous oral health care for adolescents and adults, especially those with SCD.14
The current study showed that very few participants with HbSS report the use of HU, though showing improvement when compared to what has been reported in previous findings among Tanzanian individuals living with SCD.15 The current findings differ from what was reported by Brandao et al, who reported a higher percentage of SCD individuals are routinely using HU.14 This discrepancy could be attributed to the difference in the mean age of participants, whereby the current study involved much younger participants. This difference could also be ascribed to different geographical regions with differing health-care policies for individuals with SCD. Regarding the association between the use of HU and dental caries in this study, earlier findings observed similar trends on higher dental caries among HU users.14 HU has been linked to low salivary flow and reduced salivary buffer capacity, putting oral tissues at risk for oral pathologies including dental caries.14 Furthermore, due to the high morbidity of SCD, concerns on oral/dental health are usually impaired, hence increasing the risk of oral disease including dental caries among SCD individuals.13
The use of HU in the country is still low, though with the current remarkable developments in the country, whereby HU is now included in the National Health Insurance coverage, an increase in its use is anticipated. The benefits of HU in reducing morbidity, mortality, and improving quality of life among patients with SCD significantly offset its negative effects.31 It is, therefore, pertinent to advocate for the necessity of paying closer attention to oral health care for individuals with SCD. Thus, underscoring extra efforts for oral health promotion and preventive measures among this group of population. This finding further highlights the importance of a multidisciplinary approach in the care of patients with SCD as it affects the whole body13,32
Studies have revealed the importance of regular dental visits, in that SCD patients who had free access to basic oral health-care services had fewer hospitalizations due to SCD crisis.33 Even though oral health behaviors and status of available dental services for SCD patients were not assessed in this study, what is reported here indicates limited attention to dental health care among participants, showing the need for future studies on these concepts. Early dental disease prevention and care is, therefore, recommended to avoid attendance when in severe pain, when the disease status is at late stages and hence requiring complex procedures.13 Routine oral health care, in collaboration with other cadres (physicians, hematologists, and the like), should be included as part of comprehensive care for SCD.
These results are not without limitations. The prevalence of dental caries might have been underestimated due to the method used, whereby dental caries was recorded if it was evident visually or whether it has caused cavitation. Notwithstanding these limitations, the study has managed to show the differences in dental caries across and within the different groups and hence a recommendation for future studies to utilize other robust dental caries indexes such as the decayed, missing and filled teeth (dmft) and bitewing radiography that will effectively capture the progression of the dental caries. Assessment of salivary flow should be included in future studies to ascertain the association of dental caries with SCD management. Further, the desired sample size was not attained especially for the control groups since newborn screening for SCD is not routinely done in Tanzania, resulting in low level of awareness of SCD status among families. Nonetheless, future studies are recommended that will use larger sample sizes.
Conclusion
Dental caries was low among participants with sickle cell disease (HbSS) when compared to those without SCD (HbAA) and higher in the group of HbSS males and HU users. More research utilizing larger sample sizes and robust methodologies is recommended.
Acknowledgments
The authors would like to thank parents/guardians and children for their participation, and members of staff-Sickle cell clinics at Muhimbili National Hospital, Temeke, and Amana Regional Referral Hospitals for their support during data collection. We would also like to thank Mr. John Charles, Mr. Amon Exavery – Pact. Inc. and Prof. Stein Artle Lie – University of Bergen for assisting in data analysis.
Funding
The research reported in this publication was supported by the National Heart, Lung, and Blood Institute of the National Institutes of Health under Award Number U24 HL135881 (Sickle Pan-African Research Consortium – SPARCO) and U01 HL156853 (SPARO-Tanzania). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Modell B, Darlison M. Global epidemiology of haemoglobin disorders and derived service indicators. Bull World Health Organ. 2008;86(6):480–487. doi:10.2471/BLT.06.036673
2. Thomson AM, McHugh TA, Oron AP, et al. Global, regional, and national prevalence and mortality burden of sickle cell disease, 2000–2021: a systematic analysis from the Global Burden of Disease Study 2021. Lancet Haematol. 2023;10(8):e585–e599. doi:10.1016/S2352-3026(23)00118-7
3. Saraf SL, Molokie RE, Nouraie M, et al. Differences in the clinical and genotypic presentation of sickle cell disease around the world. Paediatr Respir Rev. 2014;15(1):4–12.
4. Makani J, Cox SE, Soka D, et al. Mortality in sickle cell anemia in Africa: a prospective cohort study in Tanzania. PLoS One. 2011;6(2):e14699. doi:10.1371/journal.pone.0014699
5. Nkya S, Mtei L, Soka D, et al. Newborn screening for sickle cell disease: an innovative pilot program to improve child survival in Dares Salaam, Tanzania. Int Health. 2019;11(6):589–595. doi:10.1093/inthealth/ihz028
6. Adekile AD. What’s new in the pathophysiology of sickle cell disease? Med Princ Pract. 2013;22(4):311–312. doi:10.1159/000350283
7. Sundd P, Gladwin MT, Novelli EM. Pathophysiology of Sickle Cell Disease. Annu Rev Pathol Mech Dis. 2019;14(1):263–292. doi:10.1146/annurev-pathmechdis-012418-012838
8. Al-Ismaili H, Nasim O, Bakathir A. Jaw osteomyelitis as a complication of sickle cell anaemia in three Omani patients: case reports and literature review. Sultan Qaboos Univ Med J. 2017;17(1):e93–e97. doi:10.18295/squmj.2016.17.01.016
9. Javed F, Correa FOB, Nooh N, Almas K, Romanos GE, Al-Hezaimi K. Orofacial manifestations in patients with sickle cell disease. Am J Med Sci. 2013;345(3):234–237. doi:10.1097/MAJ.0b013e318265b146
10. Souza SFC, de Carvalho HLCC, Costa CPS, Thomaz EBAF. Association of sickle cell haemoglobinopathies with dental and jaw bone abnormalities. Oral Dis. 2018;24(3):393–403. doi:10.1111/odi.12742
11. Fernandes MLMF, Kawachi I, Corrêa-Faria P, Pattusi MP, Paiva SM, Pordeus IA. Caries prevalence and impact on oral health-related quality of life in children with sickle cell disease: cross-sectional study. BMC Oral Health. 2015;15(1). doi:10.1186/s12903-015-0052-4
12. Miller C, Rhodus NL, Treister NS, Stoopler ET, Ross Kerr A. Little and Falace’s Dental Management of the Medically Compromised Patient. Elsevier Health Sciences; 2023.
13. Kakkar M, Holderle K, Sheth M, Arany S, Schiff L, Planerova A. Orofacial manifestation and dental management of sickle cell disease: a scoping review. Anemia. 2021;2021:1–8. doi:10.1155/2021/5556708
14. Brandão CF, Oliveira VMB, Santos ARRM, et al. Association between sickle cell disease and the oral health condition of children and adolescents. BMC Oral Health. 2018;18(1):1–9. doi:10.1186/s12903-018-0629-9
15. Osati E, Kija E, Urio F, et al. Clinical epidemiology of individuals with Sickle cell anemia using Hydroxyurea at Muhimbili National Hospital, Dar es Salaam, Tanzania. Tanzania Med J. 2020;31(1):106–119. doi:10.4314/tmj.v31i1.346
16. Hsu LL, Fan-Hsu J. Evidence-based dental management in the new era of sickle cell disease: a scoping review. J Am Dent Assoc. 2020;151(9):668–677.e9. doi:10.1016/j.adaj.2020.05.023
17. Hanumanta S, Shetty RM, Khandwal O, Rath S, Shetty SY, Diwan RK. Acquisition of Streptococcus mutans and dental caries experience in pediatric sickle cell anaemia patients under various prophylactic therapies. Eur Arch Paediatr Dent. 2019;20(5):409–415. doi:10.1007/s40368-019-00415-x
18. De Matos BM, Ribeiro ZEA, Balducci I, et al. Oral microbial colonization in children with sickle cell anaemia under long-term prophylaxis with penicillin. Arch Oral Biol. 2014;59(10):1042–1047. doi:10.1016/j.archoralbio.2014.05.014
19. Zumberg MS, Reddy S, Boyette RL, Schwartz RJ, Konrad TR, Lottenberg R. Hydroxyurea therapy for sickle cell disease in community-based practices: a survey of Florida and North Carolina hematologists/oncologists. Am J Hematol. 2005;79(2):107–113. doi:10.1002/ajh.20353
20. Costa E, Tibalinda P, Sterzi E, et al. Making hydroxyurea affordable for sickle cell disease in Tanzania is essential (HASTE): how to meet major health needs at a reasonable cost. Am J Hematol. 2021;96(1):E2–E5. doi:10.1002/ajh.26007
21. Wilson EM, Minja IK, Machibya FM, et al. Oxygen saturation in primary teeth of individuals with sickle cell disease and sickle cell trait. J Blood Med. 2022;13:407–412. doi:10.2147/JBM.S365040
22. Kawar N, Alrayyes S, Yang B, Aljewari H. Oral health management considerations for patients with sickle cell disease. Disease-a-Month. 2018;64(6):296–301. doi:10.1016/j.disamonth.2017.12.005
23. Mulimani P, Ballas SK, Abas ABL, Karanth L. Treatment of dental complications in sickle cell disease. Cochrane Database Syst Rev. 2019;12. doi:10.1002/14651858.CD011633.pub3
24. da Costa TM, Nascimento MD, Peralta-Mamani M, Rubira-Bullen IR, Junqueira JL, Soares MQ. Prevalence of orofacial alterations in patients with sickle-cell disease: systematic review and meta-analysis. Oral Surg Oral Med Oral Pathol Oral Radiol. 2023;135(5):642–660.
25. Lopes CMI, Cavalcanti MC, Alves E, et al. Enamel defects and tooth eruption disturbances in children with sickle cell anemia. Braz Oral Res. 2018;32:e87.
26. Al-Alawi H, Al-Jawad A, Al-Shayeb M, Al-Ali A, Al-Khalifa K. The association between dental and periodontal diseases and sickle cell disease. A pilot case-control study. Saudi Dent J. 2015;27(1):40–43. doi:10.1016/j.sdentj.2014.08.003
27. Yue H, Xu X, Liu Q, Li X, Jiang W, Hu B. Association between sickle cell disease and dental caries: a systematic review and meta-analysis. Hematol. 2020;25(1):309–319. doi:10.1080/16078454.2020.1748927
28. Ralstrom E, da Fonseca MA, Rhodes M, Amini H. The impact of sickle cell disease on oral health-related quality of life. Pediatr Dent. 2014;36(1):24–28.
29. Luna ACAE, Rodrigues MJ, Menezes VA, Marques KMG, Santos FAD. Caries prevalence and socioeconomic factors in children with sickle cell anemia. Braz Oral Res. 2012;26(1):43–49. doi:10.1590/S1806-83242012000100008
30. Fukuda JT, Sonis AL, Platt OS. Acquisition of mutans streptococci and caries prevalence in pediatric sickle cell anemia patients receiving long-term antibiotic therapy. Pediatr Dent. 2005;27(3):186–190.
31. Kilonzi M, Mlyuka HJ, Felician FF, et al. Barriers and facilitators of use of hydroxyurea among children with sickle cell disease: experiences of stakeholders in Tanzania. Hemato. 2021;2(4):713–726. doi:10.3390/hemato2040048
32. Alrayyes S, Compton AA, Kawar N. Oral health considerations for pediatric patients with sickle cell disease. Disease-a-Month. 2018;64(6):302–305. doi:10.1016/j.disamonth.2017.12.006
33. Whiteman LN, Haywood C, Lanzkron S, et al. Effect of free dental services on individuals with sickle cell disease. South Med J. 2016;109(9):576–578. doi:10.14423/SMJ.0000000000000510
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.