")
Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 15
Current Validated Clinical and Patient Reported Disease Outcome Measures in Juvenile Idiopathic Arthritis
Authors Balay-Dustrude E , Shenoi S
Received 27 June 2023
Accepted for publication 29 September 2023
Published 9 October 2023 Volume 2023:15 Pages 189—206
DOI https://doi.org/10.2147/OARRR.S261773
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Chuan-Ju Liu
Erin Balay-Dustrude,1,2 Susan Shenoi1,2
1Department of Pediatrics, Division of Rheumatology, University of Washington, Seattle, WA, USA; 2Department of Pediatric Rheumatology, Seattle Children’s Hospital and Research Center, Seattle, WA, USA
Correspondence: Erin Balay-Dustrude, Seattle Children’s Hospital, MA 7.110, 4800 Sand Point Way NE, Seattle, WA, 98105, USA, Tel +1 206-987-6297, Email [email protected]
Abstract: Juvenile idiopathic arthritis (JIA) is a common chronic illness in childhood and comprises seven categories based on the International League of Associations for Rheumatology (ILAR) criteria. Accurate assessment and measurement of the clinical, functional, and quality of life outcomes of patients with JIA are paramount for understanding the disease course and formulating effective treatment strategies. Interest in the development and use of outcome measurements specifically focused on rheumatologic conditions has greatly expanded over the last two decades, adding to and improving upon the established disease measures. Furthermore, many of these measures have been validated using the widely accepted Outcome Measures in Rheumatology (OMERACT) core principles of instrument validation, allowing researchers and clinicians to gain confidence in these tools. This review summarizes the current validated disease outcome measures in JIA, including clinical, imaging, patient-reported, and functional outcome measurement tools, and highlights ongoing work that continues to refine and improve upon the available tools. The clinical disease outcome measures discussed in this review include physician global assessment (PhGA), American College of Rheumatology (ACR, Wallace) criteria for clinical inactive disease and clinical remission, juvenile arthritis disease activity scores (JADAS), juvenile spondyloarthritis disease activity index (JSPaDA), juvenile arthritis damage index (JADAI), and the ACR pediatric response scores. The imaging outcome measures discussed include the Dijkstra composite scores, childhood arthritis radiographic score of the hip (CARSH), and Poznanski Score. The patient-reported disease outcome measures discussed include patient global assessment (PtGA), patient-reported outcome measurement information system for JIA (PROMIS), juvenile arthritis parent/child centered disease assessment index (JAPAI, JACAI), juvenile arthritis multidimensional assessment report (JAMAR), and the Pediatric quality of life inventory rheumatology module (PedsQL). The functional outcome tools discussed include the Childhood Health Assessment Questionnaire (CHAQ), juvenile arthritis functionality scale and index (JAFS and JASI), and Juvenile Arthritis Functional Assessment Report and Scale (JAFAS and JAFAR).
Keywords: JIA, clinical outcome measures, patient reported outcomes
Introduction
Juvenile idiopathic arthritis (JIA) is a chronic childhood illness that affects approximately 16–50 children per 100,000 in high-income countries.1 Measurement of JIA patients’ clinical, functional, and quality of life outcomes is of paramount importance to patients, families, and treating rheumatologists. The goal of a successful outcome measure is to create an evaluable endpoint measurement that can be used to assess the effects of intervention or treatment. Ideally, the outcome measure instruments used in practice should be valid (accurately measure what they intend to measure), reliable (able to repeatedly and consistently measure the item), responsive (able to detect change over time and discriminate between items), and feasible (Figure 1). Validity includes criterion validity, which is the ability to measure future outcomes, including predictive and concurrent validity, and construct validity, which includes face, content, convergent, and divergent validity. Reliability includes internal intra-rater reliability and external reliability, including inter-rater and test-reset reliability. Finally, the feasibility of outcome measures in clinical or research settings is of paramount importance as it allows for practical, cost-effective, and accessible measurement instruments.
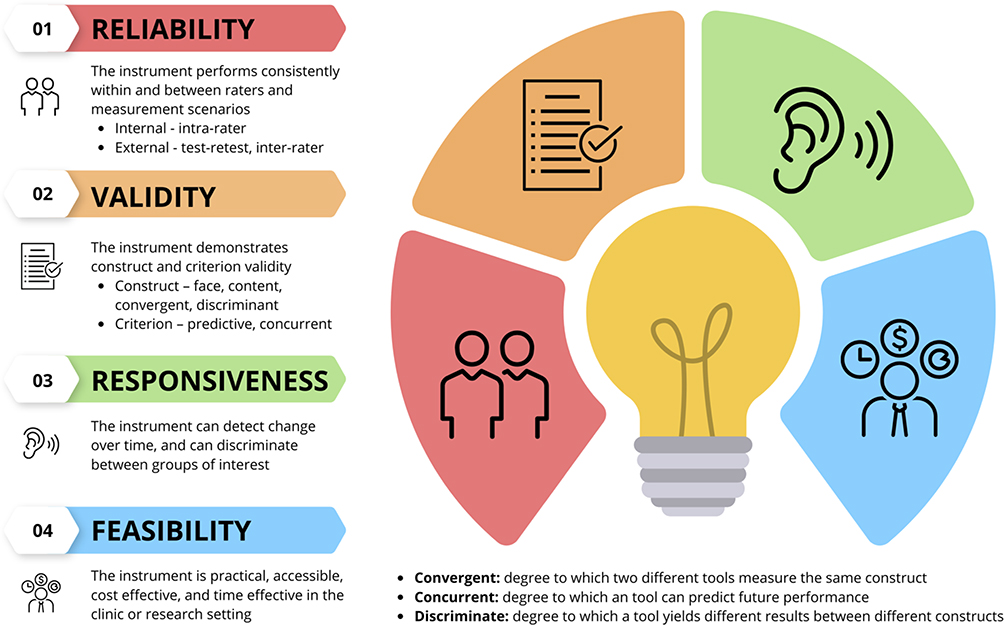 |
Figure 1 Features of an ideal outcome measure include reliability, validity, responsiveness and feasibility. Data from The Omeract Hand book.2 |
The OMERACT filter is a framework for evaluating the utility of outcome instruments in rheumatology. This filter, which was established in 1998 and updated in 2014 stands on three main pillars: truth, discrimination, and feasibility. The truth pillar is composed of face, content, construct, criterion validity, and reliability across the methods. The discrimination pillar comprises test–retest reliability, longitudinal validity, discriminatory ability, and thresholds for meaning. Finally, the feasibility pillar encompasses access, training, translation, length or duration of time required to complete the measure, and cost burden of the proposed outcome measurement tool.2 Groups presenting new and established disease outcome measures have employed this filter during the instrument development process to ensure the validity and utility of their outcome instrument. Furthermore, outcome measures should be evaluated for floor and ceiling effects. These occur when a large proportion of subjects report achieving the best or worst possible score and can indicate measurement inaccuracy at the end of the measurement spectrum.
Over the last several decades, numerous JIA clinical measures have been developed and validated to monitor the disease and treatment courses. Some of these measures are validated for parent reports as a proxy for younger children, an issue that pediatric populations grapple with around outcome measures. Recently, patient-reported outcomes have been incorporated into these tools to incorporate patients’ and families’ voices into their own chronic disease experience. This integration has allowed for a deeper evaluation and understanding of the disease course and its effects on the patients and their families. Furthermore, the use of established and validated outcome measures allows practitioners to identify individual patients as well as a population’s disease trajectory (improving, stable, or worsening), in addition to assessing treatment efficacy and allowing for comparisons between treatment modalities.
This review aimed to summarize the currently available and validated disease outcome measures in JIA, including clinical and patient-reported outcomes.
JIA Outcome Measures
We discuss the outcome measures as they pertain to clinical disease or damage, imaging, function, and patient-reported outcomes of JIA.
JIA Clinical Disease and Damage Outcome Measures (Table 1)
Currently, several well-established JIA clinical outcome measures are commonly used in practice and for clinical research that allow stakeholders (providers, patients, and researchers) to evaluate patient disease status at the point of care and over the long-term disease course.
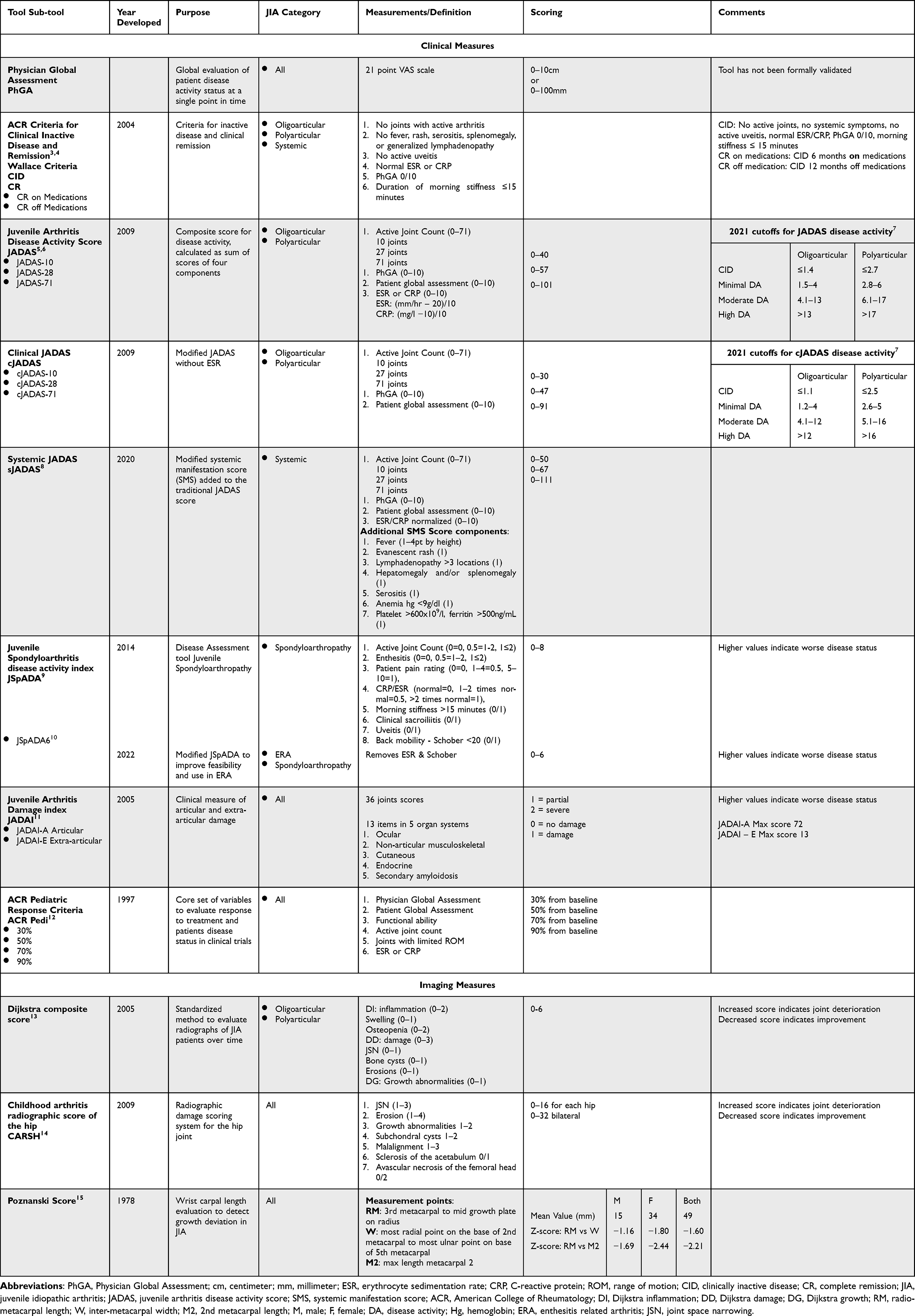 |
Table 1 Clinical Disease Outcome Measures in Juvenile Idiopathic Arthritis |
Each individual JIA International League of Associations for Rheumatology (ILAR) category encompasses patients with varying disease characteristics and severities, who may have unique disease attributes that require variation and individualization of clinical disease outcome measurement instruments. Thus, as clinical outcome measures have evolved for JIA, category-specific measures have ensued to allow for more specific, focused, and in-depth monitoring of disease status for each category. For example, the modification of the JADAS score with systemic manifestation score (SMS) created a more specific systemic juvenile arthritis disease activity score (sJADAS) for the systemic onset JIA ILAR category.8 Within the spondyloarthropathy population, there has been a recent focus on improving outcome measures specific to this population with the development of the JSPaDA index, the recently modified JSPaDA6, and development of imaging classification for this population.9,10,16 Additional refinement of outcome measures includes cut-offs for disease activity states such as the JADAS scoring cut-off for disease activity status (high, low, and moderate) established for both polyarticular and oligoarticular patients, recognizing that these subgroups of patients are likely to have different disease outcome experiences, thus allowing for more refined outcome assessment at the individual patient level.5,7,17,18
Physician Global Assessment (PhGA)
PhGA is a longstanding and broadly accepted measure of the overall JIA clinical disease status employed in clinical practice and research settings. PhGA is a general measure or “gestalt” sense of the treating provider’s evaluation of the patient’s disease activity at a single point in time, typically immediately after a clinic visit or evaluation, marked on a 21-point linear visual analog scale (VAS) scale, from 0 to 10 cm, or alternatively from 0 to 100 mm with 0 being no JIA related disease activity or quite disease. The PhGA is often used as the “gold standard” for disease activity assessment and is a component of multiple other composite disease status assessments such as the American College of Rheumatology (ACR) Pedi response criteria,12 juvenile arthritis disease activity score (JADAS),5 and ACR criteria for defining clinically inactive disease (CID).3,4,19
However, to date, there are no explicit objective criteria for the components or exact clinical and patient factors that should be included in the PhGA. This lack of clarity on specific individual disease elements that comprise the PhGA creates opportunities for both inter- and intra-rater discrepancies among pediatric rheumatology providers and may result in significant variability in the assessment of a single patient’s disease status at any time point in the disease process.20,21 The corollary of PhGA in adult rheumatoid arthritis (RA), the MD disease activity assessment of RA, has similar challenges as highlighted by Turk et al.22 Another reported issue with the PhGA is the resistance or hesitancy for providers to mark zero for no disease activity when the active joint count is zero, but other symptoms such as pain are present, as noted by Alongi et al.23 This type of issue may then misleadingly suggest active disease when there is none and complicate other measures that use PhGA as part of a composite measure. Better standardization of the PhGA score components could alleviate this issue. Currently, there is ongoing international collaborative work to establish a framework for the critical elements of the PhGA assessment via a Delphi survey in an attempt to improve characterization, standardization, and precision, and reduce inter- and intra-rater variability of the PhGA. Overall, the PhGA is a quick and efficient evaluation tool that can be used in daily practice in the routine clinical environment and tracked over time.
American College of Rheumatology Provisional Criteria for Defining Clinical Inactive Disease and Clinical Remission (CID, CR) Also Known as Wallace Criteria
The Wallace criteria for CID and CR were first introduced in 2004,4 and validated in 20063 for the ILAR JIA categories, including persistent and extended oligoarticular, polyarticular (rheumatoid factor-positive and rheumatoid factor-negative), and systemic JIA. CID is defined using five criteria: no joints with active arthritis, no fever, rash, serositis, splenomegaly, or generalized lymphadenopathy attributable to JIA; no active uveitis; normal erythrocyte sedimentation rate (ESR) or C-reactive protein (CRP) (if both are tested, both must be normal); and PhGA indicating no disease activity (ie, best score attainable on the scale used, typically 0/10). In 2011, morning stiffness <15 minutes was added to the CID criteria, which increased the face and content validity while maintaining the accuracy of the tool.19
Wallace et al used CID to define clinical disease remission (CR). CR on medication is defined as a CID for six continuous months while on rheumatic medications. CR off medications is defined as CID for 12 continuous months while off all rheumatic medications including those for arthritis and uveitis. The Wallace criteria have been widely accepted and used in observational studies and interventional trials over the last two decades, and it offers a quick and feasible assessment of patient disease activity. Furthermore, the addition of clinical remission criteria allows for benchmarks in disease course progress that are easy for providers, patients, and families to follow and understand. Many studies and trials have modified CR off medications to CID for six months as 12-month data collection is a prolonged time to follow-up for trials. Additionally, it has become clear over time that these CID and CR criteria, while a good start, probably do not encompass all the factors required to attain true biological JIA remission, a state in which the disease does not flare again, and there may be yet to be discovered measures to accurately determine this state in JIA.24,25 The Wallace criteria for CID and CR are widely known and accepted measurement tools used throughout the pediatric rheumatology population in both the clinical and research domains.
Juvenile Arthritis Disease Activity Scores (JADAS) and Its Clinical (cJADAS) and Systemic (sJADAS) Variations
Consolaro et al developed the first composite score for disease activity, the JADAS, in 2009 for use in all non-systemic JIA patients.5,6 This score allows clinicians to evaluate a patient’s disease activity at a single point in time and encompasses the active joint count (AJC), PhGA, patient/caregiver-proxy global assessment, and normalized ESR value. The JADAS was subsequently validated by several groups5,17,18 and has three validated variations of the scoring system that encompass more rigorous joint evaluations, with the number of joints evaluated (10, 27, and 71 joints) producing the JADAS-10, JADAS-27, and JADAS-71, respectively. Notably, the JADAS-71 does not formally assess the thoracic or lumbar spine and sacroiliac joints. Additionally, a modified version of the JADAS (JADAS-CRP), which allows for the use of CRP instead of ESR values, was validated by Nordal et al26 and demonstrated a high correlation with the original ESR containing JADAS.
JADAS10 is widely accepted as the most feasible version of the tool in clinical practice, allowing for rapid joint assessment. The JADAS scores are also frequently used as a tool for assessing treatment response and targets for treatment or goals of JIA care. Further utility of the JADAS is found in the validated ranges for clinically inactive disease, minimal disease activity, moderate disease activity, and high disease activity, which were most recently updated in 20217,17,27 (Table 1). These cut-off scores offer point-of-care evaluations for providers and families to discuss patient disease status and evaluate changes in disease burden over time. Furthermore, in 2008, Magni-Manzoni et al28 proposed and validated a definition for minimal disease activity (MDA), which has a corollary in adult RA disease management and is noted to be an acceptable state of disease control in which the physician does not change or may have discontinued therapy due to disease status. This minimal disease state may present a more achievable yet tolerable disease activity goal and is defined separately for oligoarticular and polyarticular patients. For oligoarticular patients, MDA was based on a PhGA ≤2.5, swollen joint count of 0, and for polyarticular patients, MDA was based on a PhGA ≤3.4, parent global assessment ≤2.1, and swollen joint count ≤1.
Modifications to the JADAS score over time have been made to improve its clinical feasibility and to better evaluate certain categories, such as the systemic JIA population. The clinical JADAS (cJADAS) score, introduced in 2009, eliminates the requirement for laboratory ESR measurements, thus improving the practicability and clinical feasibility. The cJADAS has been noted to correlate well with the JADAS score. As systemic JIA (sJIA) is notably different from other ILAR JIA categories, the systemic JADAS (sJADAS) score was introduced and validated in 20208 increasing the specificity of the JADAS instrument for patients with sJIA. The sJADAS uses an adjunct tool, the systemic manifestation scores (SMS), which are added to the JADAS score (Table 1), including fever (1–4 points), evanescent erythematous rash (1 point), generalized lymphadenopathy (>3 lymph node stations) (1 point), hepatosplenomegaly or splenomegaly (1 point), serositis (pleuritis, pericarditis, or peritonitis) (1 point), anemia (hemoglobin <9 g/dl) (1 point), thrombophilia (>600 × 109/l), or hyperferritinemia (>500ng/mL) (1 point). The JADAS scoring and its variations offer detailed and efficient scoring systems which can be easily completed and even automated into the electronic medical record for use in the clinical and research domains.
Juvenile Spondyloarthritis Disease Activity Index (JSPaDA, JSpADA6)
The JSPaDA index, established by Weiss et al in 20149 focused on defining disease activity in patients with juvenile spondyloarthropathy, which encompasses patients with juvenile ankylosing spondylitis (JAS), enthesitis-related arthritis (ERA), psoriatic arthritis, and undifferentiated arthritis by ILAR classification. The index equally weighs eight components for a maximum score of eight including AJC, active enthesitis count (AEC), patient pain rating (0–10 scale), CRP or ESR, morning stiffness for >15 minutes, clinical sacroiliitis (defined as two or more of the following: tenderness on examination, positive Patrick’s test or flexion abduction external rotation test, and inflammatory back pain),29 uveitis, and limited back mobility (modified Schober <20 cm). This index offers the first detailed pediatric-focused approach to disease status in juvenile spondyloarthropathy. However, its feasibility is limited, given the requirement for the collection of all components of the score at each clinic visit, which limits its utility in various situations, such as telemedicine or when laboratory access is limited. Given these limitations, Srinivasalu et al proposed and validated within the ERA population the simplified JSPaDA6 score.10 This tool removes the ESR/CRP and modified Schober requirements with an overall score of 0–6, thus improving feasibility and capture rates of full scoring. Implementation of the JSpADA tool and its modified version is a strong example of the utility of clinical disease measurement tools specifically tailored to a subset of the JIA population, allowing category-specific care and treatment. Notably, the JSPaDA and JSpADA6 tools were developed for the broader juvenile spondyloarthropathy population but do not specifically evaluate or encompass the skin component present in the psoriatic arthritis population. Thus, this tool may be limited in its use in this subpopulation. At this time to our knowledge, there are no pediatric specific psoriatic arthritis disease outcome measures available, and this is an area that should be explored further to improve care for these patients.
Juvenile Arthritis Damage Index, Articular and Extra-Articular Damage (JADI – A/E)
The JADI, introduced in 2005 by Viola et al, has established a clinical index for the assessment of long-term damage in JIA.11 Damage patterns, defined as being present for at least six months despite therapy and rehabilitation, include articular (JADI-A) and extra-articular (JADI-E) damage. Articular damage is scored as partial or severe at 36 joints, and extra-articular damage is scored in five organ systems, including ocular, non-articular musculoskeletal, cutaneous, endocrine, and secondary amyloidosis, using 13 items. This index was validated for all categories of JIA other than ERA and is simple and quick to administer taking only 5–15 minutes to complete and score. During validation, the JADI-A correlated highly with the AJC, with limited range of motion, and moderately with the Childhood Health Assessment Questionnaire (CHAQ) score, with good internal consistency and inter-rater reliability.11 As effective treatment availability has greatly improved over time, providers and patients now have an improved ability to prevent permanent damage such as those scored in the JADI, which may decrease the widespread utility of this tool. Nonetheless, this tool remains useful for monitoring patients with severe, longstanding JIA.
ACR Pediatric Response Criteria (JIA ACR30/50/70/90)
Giannini et al developed the ACR pediatric response criteria in 199712 which are comprised a core set of variables evaluating the response to treatment for JIA patients enrolled in clinical trials. The criteria consist of six variables: PhGA, Patient Global assessment (PtGA), functional ability, AJC, number of joints with limited range of motion (ROM), and ESR or CRP measurement at the time of assessment. Patient variables are compared between research visits, and the improvement percentage is defined as the improvement in three of the six variables and allows for worsening in up to one variable. The increments of change are set at 30%, 50%, 70%, 90%, and 100% response.12 Although not formally validated, this measurement was evaluated by Lurati et al in comparison with other adult outcome measures, including the ACR20, disease activity score (DAS), and DAS28. This group noted that the JIA ACR30 was most highly correlated with the DAS (71% concordance), followed by the DAS28 (55% concordance), and most poorly correlated with the ACR20 (53% concordance).30 The lack of concordance of the JIA ACR30 with both the DAS28 and the ACR20 is suggested to be related to the JIA ACR30’s inclusion of a parameter for the number of joints with limited range of motion and the specific inclusion of the ankle, foot, and TMJ, which are commonly evaluated and affected joints in the pediatric population but not included in the DAS28. Furthermore, the JIA ACR30 has recently been adapted for use in the sJIA population by adding the absence of fever (>38 °C) to the other six criteria for treatment response or improvement. This modified version has been successfully used in multiple-drug trials in the sJIA population.31–33
The JIA ACR30 is often considered the “gold standard” for the evaluation of treatment response in clinical trials and is accepted by the FDA and EMA for drug registration. However, it is neither practical to use in clinical settings, given the cumbersome calculations required, nor does the JIA ACR30 likely represent a clinically meaningful change to the patient and family.
JIA Imaging Disease Outcome Measures (Table 1)
Imaging is an important facet of clinical care and monitoring of children with JIA throughout the disease course and can assist in identifying the extent of disease activity (such as synovitis or enthesitis on MRI or ultrasound studies) and damage (erosions or joint space narrowing as seen on MRI, ultrasound, or X-rays). However, children fundamentally differ from adults because of their growth and progressive ossification, which results in joint space size variation. Hence, validated adult scoring systems, such as the Sharp34 and Larsen35 scores used in RA for disease-related damage monitoring and outcomes, must be adapted for pediatric use. Traditionally, X-rays have been used to score JIA damage in the pre-biologic era. There is an unmet need for an MRI or ultrasound scoring system which could identify early cartilage damage prior to the detection of erosions on X-ray, by which time the disease is well advanced. Rossi et al demonstrated that the Sharp and Larsen scores are potentially reliable for radiographic progression monitoring in patients with JIA with wrist involvement.36 The work of standardized scoring systems within each imaging modality is currently underway, and here, we discuss a few currently available JIA radiographic scoring systems.
Dijkstra Composite Score
This composite score was developed by van Rossum et all in 200513 to create a standardized evaluation of radiographs of patients with oligoarticular and polyarticular JIA over time. The score was composed of three composite items, Dijkstra inflammation (DI), Dijkstra Damage (DD), and Dijkstra growth (DG), with an increase in any of the individual item’s score indicating joint deterioration. This scoring system allows a patient’s radiographic disease status to be tracked over time using a numerical scale (0–6) for both worsening and improvement. The Dijkstra system has demonstrated validity for a broad range of joints including the knee, hand, foot, ankle, elbow, shoulder, hip, cervical spine, and sacroiliac joints. Further, this group proposed and demonstrated feasibility using a more concise and easily obtainable “standard” set of joints limited to radiographs of bilateral hands, feet and knees.
Childhood Arthritis Radiographic Score of the Hip (CARSH)
Introduced in 2009, the CARSH score is a radiographic damage scoring system for the hip joint in JIA.14 This score encompasses a scale of 0–16 points per hip (maximum score of 32), with points allotted for joint space narrowing (1–3), erosions (1–4), growth abnormalities (1–2), cyst presence (1–2), malalignment (1–3), sclerosis (0–1), and avascular necrosis (0–1). Together, these form a composite score that indicates the disease severity and damage. This score was preliminarily validated as reliable, with good intra- and inter-observer agreement and reliable identification of radiographic damage and progression over time. With the evolution of biological disease-modifying therapy that reverses erosions and improves outcomes, limiting damage such as cysts, malalignment, or necrosis of the hip, the utility of this score over time is likely to decline.
Poznanski Score
In 1992, Poznanski presented various approaches to radiological joint evaluation in patients with JIA37 and created the Poznanski score.15 The Poznanski score aimed to establish carpal length evaluations that are less dependent on age and skeletal maturation to evaluate deviations from the norm, which could help determine the radiographic progression of wrist damage in JIA. This score utilizes three measurements: RM, which measures 3rd metacarpal to mid-growth plate of the radius, W, which is identified by the line joining the most radial point of the base of the 2nd metacarpal and the most ulnar point on the base of the 5th metacarpal, and M2, which is defined as the maximal length of the 2nd metacarpal. RM:W and RM:M2 length comparisons (scores) were then compared with healthy population means according to sex to create z-scores. These z-scores are used to attempt to identify variations away from the normal, which would indicate skeletal changes independent of age or growth status and allow for following of possible radiographic damage due to JIA. There are several limitations to this score, including that it can only be used in patients with JIA wrist involvement; thus, it does not reflect the amount of damage or involvement of other JIA-afflicted joints, its limited utility in erosive carpometacarpal disease given that it measures carpal length, and the score requires the presence of an open growth plate for the second metacarpal, thus limiting its utility in post-pubertal age groups.
JIA Patient Reported Quality of Life Outcome Measures (Table 2)
Patient and caregiver-proxy reported outcomes (PRO) and quality of life (QOL) measures are vital to the care of children with JIA, as they invoke the voice of the family that is affected and living with the burden of disease. These measurement tools assist in creating a holistic view of the patient’s functioning and often take into account factors such as medication side effects, disease effects on quality of life, and emotional or psychological complications. These aspects of chronic diseases may be underappreciated or under evaluated by healthcare providers in clinical disease activity measurements. Multiple measurement tools have been established for this purpose, many of which employ a multidimensional approach to comprehensively assess the patient experience.
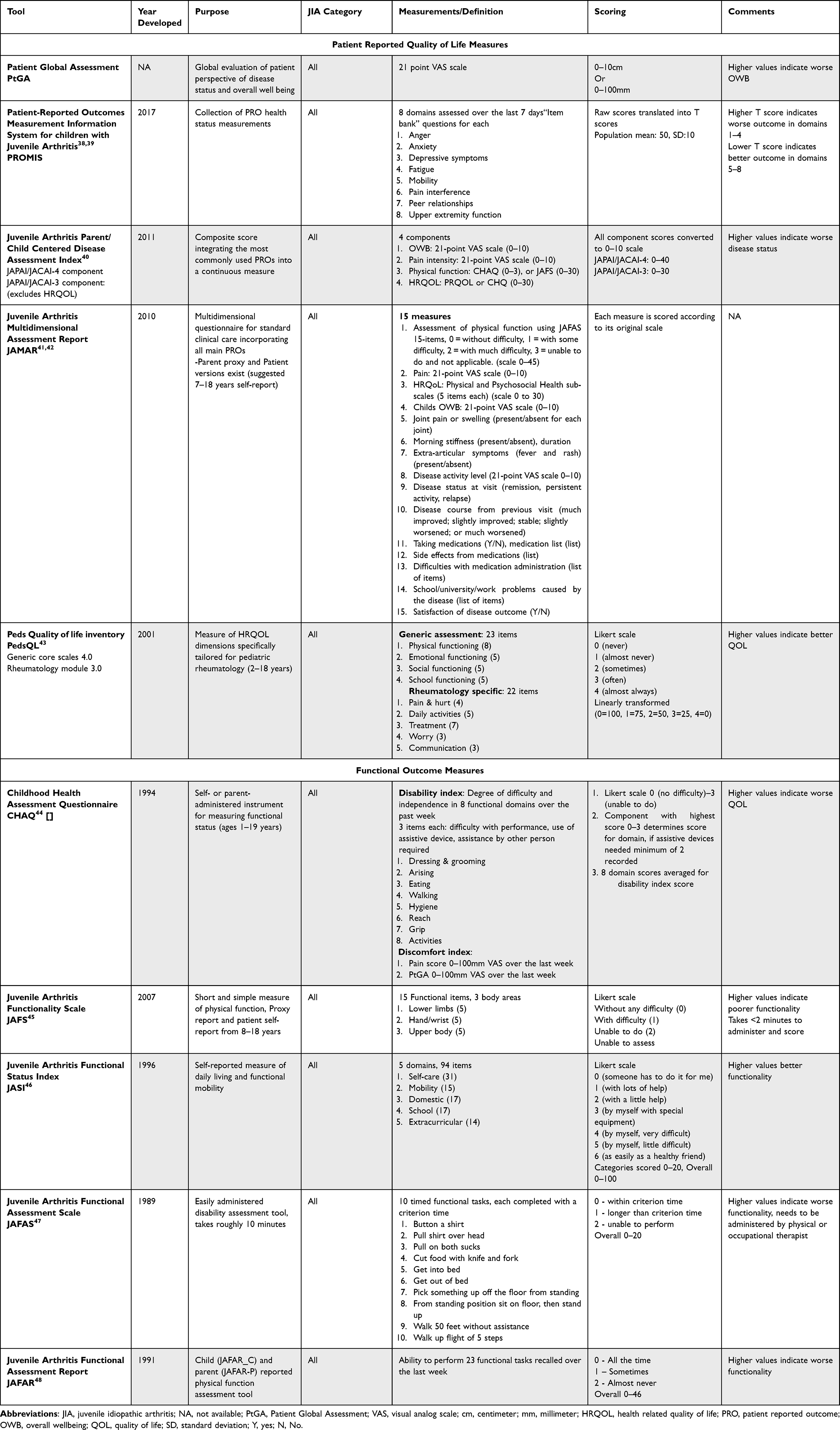 |
Table 2 Patient Reported Quality of Life and Functional Outcome Measures in Juvenile Idiopathic Arthritis |
The PRO measures discussed here demonstrate feasibility across JIA categories. This speaks to the generalizability of such measures across this population but may indicate a need for further refinement of differences among patient-reported outcomes between JIA categories, as has been demonstrated in clinical disease outcome measures. This is an opportunity for future work in the PRO space.
Patient/Caregiver-Proxy Global Assessment (PtGA)
The PtGA tool is similar to the PhGA and encompasses a 21-point VAS scale scored from 0 cm to 10 cm or 0–100 mm. It is employed both in clinical practice and research settings as a general measure of the patient’s or caregiver-proxy’s perception of the current JIA disease status and overall well-being, as it relates to their rheumatologic condition. This score is a component of the JADAS clinical measurement tool. Similar to the PhGA, this measure has not been formally validated and lacks parameters for the precise inclusion or exclusion of patient experience and quality of life factors encompassed in the score. Further, patients and caregiver-proxies may have a difficult time defining such a broad measure into a simple numeric scale, and in qualitative studies patients report struggling with anchoring of the tool and understanding of its form and functionality.49–51 Comorbid diseases with JIA such as central sensitization may also impact overall wellbeing of the patient and affect how families score this measure. The current work is underway within the OMERACT JIA working group to better define, establish, and validate a tool for measuring patient perception of disease activity and overall well-being. As with the PhGA tool, the PtGA is a quick and efficient PRO tool that can be used in daily practice in the routine clinical environment and tracked over time.
Discordance between PhGA and PtGA occurred frequently during the same visit with caregivers reporting divergent scores from providers in JIA patient assessments.23,52 A similar discordance has also been noted in the adult RA population.49 This discordance may undermine the potential value of these scores in composite measures and may indicate a disconnect between the two scores despite their similar design. This discordance may reflect multifactorial etiologies, including the lack of clarity regarding the specific items that should be considered in each score as they pertain to overall disease activity or well-being, the presence of comorbid conditions, differences in judgement between providers and patients regarding what constitutes disease activity, and the inclusion of social determinants of health that might affect patients’ disease activity but are often not sought by busy clinicians. Furthermore, this discordance may be further compounded in pediatric rheumatology with the potential for discordance between caregiver-proxy global assessment and the young child’s patient global assessment,52 thus further work and standardization of this measure is needed.
Patient Reported Outcomes Measurement Information System (PROMIS) for Children with Juvenile Arthritis
The PROMIS initiative, first presented in 2007 by the National Institutes of Health (NIH), aimed at assessing patient-reported health status using existing PRO tools, was developed for use across the general population and a variety of chronic disease states,38,39 and is available in paper and digital (computer-adapted test) forms. In 2017, Brandon et al validated the pediatric PROMIS short-form tool for JIA.53 Patients (8–17 years) and parents/caregiver proxies (5–17-year-old patients) assessed eight pediatric-specific domains over the seven days prior, including anger, anxiety, depressive symptoms, fatigue, mobility, pain interference, peer relationships, and upper extremity function. All raw scores generated from the PROMIS instruments are scaled into standardized T-scores with a mean of 50 and a standard deviation of 10 and compared to an established population mean. The population mean refers to the mean of the calibration sample, which is based on a population with a higher prevalence of chronic illness, to allow for more accurate peer comparisons with patients with JIA. Brandon et al53 demonstrated that within the JIA population, the PROMIS tool can be used to differentiate patients with poorer outcomes (higher scaled scores) and more active diseases as measured by the JADAS at the time of evaluation. All domains assessed behaved in this way, except for the upper extremity function domain, which did not correlate with disease outcome by the JADAS. A limitation of this instrument is its evaluation of upper extremity function alone, without evaluation of the axial or lower limbs, which are commonly affected by JIA.
In 2021, Craig et al compared PROMIS to the CHAQ assessment tool for patient preference and measurement properties and noted that patients preferred PROMIS to CHAQ54 because it was easier and more convenient to complete. There was a moderate correlation between the PROMIS mobility and the CHAQ-disability index, and a high correlation between the pain assessments for both tools. The PROMIS tool was found to have a lesser ceiling effect and improved upon pain interference, mobility, and physical activity evaluations than the CHAQ. Overall, the PROMIS tool is a relatively convenient and efficient system that encompasses multiple PRO tools and is feasible for use in the clinical and research setting.
Juvenile Arthritis Parent/Child Centered Disease Assessment Index (JAPAI/JACAI)
Introduced by Consolaro et al in 2011, the JAPAI/JACAI assessment tools are a composite PRO score that integrates the most commonly used tools to create a comprehensive PRO measure for assessing disease status.40 The tool can be administered to the caregiver proxy or the patient for self-reporting and has two versions. The 4-component version assesses patient overall well-being (OWB), pain intensity, physical function (via the CHAQ or juvenile arthritis functionality score (JAFS)), and health-related quality of life (HRQOL) (by the Pediatric Quality of Life Scale (PRQOL) or the Child Health Questionnaire (CHQ)). The 3-component version eliminates the HRQOL component improving on brevity and ease of administration. Each component of the score is normalized, and a single summative score is created from 0 to 40 (or 0–30 for the 3-component version). The validated JAPAI/JACAI tool demonstrates a high correlation with JADAS, indicating that it may improve upon the present issue of patient/caregiver-proxy and physician discordance in disease activity when using the much simpler PhGA and PtGA measurement tools and overall well-being measures, as previously noted. However, it should be noted that the time required to assess JAPAI/JACAI was considerably greater than that required for PhGA and PtGA.
Juvenile Arthritis Multidimensional Assessment Report (JAMAR)
The JAMAR is a comprehensive multidimensional questionnaire created for use in clinical practice to facilitate the incorporation of PROs into routine clinic visits. Introduced in 2010 by Filocamo et al41 and validated in American English in 2018,42 it employs 15 established measures of patient-reported disease status. This tool was designed to be used in a busy clinic, ideally administered prior to the patient’s clinic visit while waiting to be seen, and can be completed in <15 minutes. Despite its length, it remains feasible for daily clinical use without a significant impact on clinical flow. The tool has a high correlation between caregiver and patient self-reports (suggested for ages 7–18 years), indicating that either party can complete the tool reliably. The JAMAR has wide applicability and has been adapted to 54 languages across 52 countries through the Paediatric Rheumatology International Trials Organisation (PRINTO) organization.55 The items queried are comprehensive and provide a snapshot of several aspects of life for a child with JIA including school, medication side effects, medication adherence, pain, and disease activity. However, the authors noted that the components of fatigue, coping, sleep disturbances, and family life are not well captured by the instrument. Additionally, the mental health aspects of JIA as a chronic disease are not well captured by JAMAR.
Pediatric Quality of Life Inventory (PedsQL) Rheumatology Module
The PedsQL rheumatology module was adapted from the Pediatric Quality of Life Inventory and introduced in 2001.43 This extension module is specifically tailored for patients with rheumatological conditions, and evaluates QOL in the physical, mental, and social domains. This instrument includes both the original generic assessment and a 22-item rheumatology-specific section, assessing five domains, including pain and hurt, daily activities, treatment, worry, and communication, on a Likert scale of difficulty in performing each item. This assessment tool is both easy and quick to administer, has been validated for a wide range of ages (2–18 years) for self-report or caregiver-proxy reports, and exhibits good correlation between patient and caregiver-proxy reports. This tool, which adds a rheumatology-specific feature to a longstanding and trusted tool, proved to be useful and feasible, especially for use in clinical trials to improve the incorporation of PROs in patients with JIA.
JIA Functional Disease Outcome Measures (Table 2)
JIA is a chronic disease that affects children across their lifespan, directly affecting their functionality in daily life to varying extents during the disease process. This variability and potential for significant impact impart importance to the measurement of functional outcomes in patients with JIA. These measures must incorporate patient functionality reports and objective measures of function at discrete time points and across the disease course.
Childhood Health Assessment Questionnaire (CHAQ)
The CHAQ score developed in 1994 by Singh et al is one of the longest standing tools used for the measurement of self-reported functional status in JIA.44 This tool is composed of a disability index with eight domains: dressing and grooming, arising, eating, walking, hygiene, reach, grip, and activities. Each domain uses a Likert scale to rate the difficulty of completing tasks (0 = no difficulty to 3 = unable to do). The discomfort index has two domains: pain score and PtGA score, each using a 0–100 VAS scale. This measurement tool is a reliable, valid, and sensitive instrument that takes approximately 10 minutes to complete by either caregiver-proxy or child self-report and has been translated and culturally adapted into numerous languages since its introduction. The CHAQ is applicable for a broad range of 1–19 years and has a section for non-applicability, if deemed based on the age of the child for the disability index. The CHAQ score is often used as the “gold standard” for comparison in the validation and implementation of newer PRO measurement tools; however, its length and amount of time taken to complete are the most notable drawbacks for routine feasibility of use in clinical settings.
Juvenile Arthritis Functionality Scale (JAFS)
The JAFS score was developed and validated by Filocamo et al in 2007 with the intention of creating a simple measure of physical function in patients with JIA in the clinical setting in place of the more extensive CHAQ score.45 The scale takes less than two minutes to complete and uses 15 items on a Likert scale to explore physical function across three body areas: the lower limbs, hand/wrist, and upper body. The JAFS correlates highly with the CHAQ score45 and thus may present a more feasible way to quickly evaluate the functional status of patients in the clinical setting. The inclusion of jaw function with biting a sandwich or apple is a plus of this functional scale, as the temporomandibular joint is often affected in JIA.
Juvenile Arthritis Functional Status Index (JASI)
First introduced in 1996 by Wright et al, this validated self-reported functional index focuses on daily living and functional mobility of school-aged children and adolescents.46 Five domains encompass 94 items evaluating self-care, mobility, domestic tasks, school, and extracurricular activities. Each domain is scored from to 0–20, with a total score of 0–100. Originally, this index contained 100 items; however, during validation, six items were noted to not prove useful in discriminating between individuals with differing levels of disease activity or to be problematic for children with severe functional disability, thus reducing the total number of items to 94. Each component is scored on a Likert scale of ability to complete tasks (0: someone has to do it for me, to 6: I can do it as easily as a healthy friend). This index is the most reliable for polyarticular JIA. Oligoarticular patients may experience a ceiling effect, as these patients more frequently scored between 95% and 100% on the functionality scale, indicating that those with the highest functional scores may be missed in this assessment. Another drawback of this index is its length, as it can take between 30 and 90 minutes to complete, making it largely infeasible in the clinical setting and at risk of inducing survey fatigue for participants in clinical trials.
Juvenile Arthritis Functional Assessment Scale (JAFAS)
This score, introduced by Lovell et all47 in 1989, aims to create a simple functional assessment tool to assess a patient’s ability to complete daily functional activities compared with age-matched healthy peers. The score encompasses ten functional tests that are timed to compile a functionality score. Higher scores indicate poorer function due to the patient taking more time to complete each individual task, scored as 0 – (within criterion time), 1 (longer than criterion time), and 2 (unable to perform), with a maximum score of 20. The JAFAS is reliable and can be completed within 10 minutes with minimal equipment in clinical or research settings; however, it requires a trained medical professional, typically a physical or occupational therapist, for administration, thus limiting its function in the day-to-day clinical or home telemedicine setting.
Juvenile Arthritis Functional Assessment Report (JAFAR)
The JAFAR score, created in 1991, is an adaptation of the JAFAS score, which can be performed at home by caregivers and children as a self-reporting tool.48 This score evaluates a patient’s ability to complete 23 functional tasks of daily living on a 3-point scale. The tool can be completed by patients older than seven years (JAFAR-C) or the caregiver (JAFAR-P) within the home setting and is a reliable and valid measure of JIA-related disability. This report provides the ability for families to actively report on their child’s functionality and capture valuable data on physical function while minimizing provider personnel time when compared to the JAFAS. However, these measurements may be subject to recall bias given the assessment of functions over the last week, which may limit its reliability.
Conclusion and Future Directions
At present, there are a myriad of reliable and validated clinical, imaging, patient-reported, and functionality outcome measures used in the care and monitoring of patients with JIA. These measures are used in clinical and research settings and allow patients and providers to objectively monitor disease changes over time, which is paramount for evaluating treatment response and treating to target.56 As more advanced disease-modifying therapies develop and our understanding of the disease process and the experiences of JIA patients across their lifetime continue to expand, it is imperative that we iteratively re-evaluate, adapt, and modify current measures or develop novel measures that best reflect the experiences and perspectives of the patient. Diverse collaborative work is currently underway across the globe to advance this field and improve the care of patients with JIA.
Ethics
This manuscript has been reviewed and approved by all contributing authors, and all the work is original.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
Dr. Balay has no conflicts of interest related to this work or financial disclosures to report. Dr. Shenoi acts as a consultant for Pfizer, Novartis, and Amgen.
References
1. Prakken B, Albani S, Martini A. Juvenile idiopathic arthritis. Lancet. 2011;377(9783):2138–2149. doi:10.1016/S0140-6736(11)60244-4
2. The OMERACT Handbook. In: Beaton D, Maxwell L,Grosskleg S, Shea B, Tugwell B, Eds. Updated April 2021. Available from: https://omeract.org/wp-content/uploads/2021/12/OMERACT-Handbook-Chapter-5_Final_June-2-2021_a.pdf.
3. Wallace CA, Ravelli A, Huang B, Giannini EH. Preliminary validation of clinical remission criteria using the OMERACT filter for select categories of juvenile idiopathic arthritis. J Rheumatol. 2006;33(4):789–795.
4. Wallace CA, Ruperto N. Preliminary criteria for clinical remission for select categories of juvenile idiopathic arthritis. J Rheumatol. 2004;31(11):2290–2294.
5. Consolaro A, Ruperto N, Bazso A, et al. Final validation of a new composite disease activity score for juvenile idiopathic arthritis: the Juvenile Arthritis Disease Activity Score (JADAS). Pediatr Rheumatol. 2008;6(1):P115. doi:10.1186/1546-0096-6-S1-P115
6. Consolaro A, Ruperto N, Bazso A, et al. Development and validation of a composite disease activity score for juvenile idiopathic arthritis. Arthritis Care Res. 2009;61(5):658–666. doi:10.1002/art.24516
7. Trincianti C, Van Dijkhuizen EHP, Alongi A, et al. Definition and validation of the American college of rheumatology 2021 juvenile arthritis disease activity score cutoffs for disease activity states in juvenile idiopathic arthritis. Arthritis Rheumatol. 2021;73(11):1966–1975. doi:10.1002/art.41879
8. Tibaldi J, Pistorio A, Aldera E, et al. Development and initial validation of a composite disease activity score for systemic juvenile idiopathic arthritis. Rheumatology. 2020;59(11):3505–3514. doi:10.1093/rheumatology/keaa240
9. Weiss PF, Colbert RA, Xiao R, et al. Development and retrospective validation of the Juvenile Spondyloarthritis Disease Activity Index. Arthritis Care Res. 2014;66(12):1775–1782. doi:10.1002/acr.22411
10. Srinivasalu H, Treemarcki EB, Rumsey DG, Weiss PF, Colbert RA. Modified Juvenile Spondyloarthritis Disease Activity Index in the Childhood Arthritis and Rheumatology Research Alliance (CARRA) Registry. J Rheumatol. 2022. doi:10.3899/jrheum.220509
11. Viola S, Felici E, Magni-Manzoni S, et al. Development and validation of a clinical index for assessment of long-term damage in juvenile idiopathic arthritis. Arthritis Rheum. 2005;52(7):2092–2102. doi:10.1002/art.21119
12. Giannini EH, Ruperto N, Ravelli A, Lovell DJ, Felson DT, Martini A. Preliminary definition of improvement in juvenile arthritis. Arthritis Rheum. 1997;40(7):1202–1209. doi:10.1002/art.1780400703
13. van Rossum MAJ, Boers M, Zwinderman AH, et al. Development of a standardized method of assessment of radiographs and radiographic change in juvenile idiopathic arthritis: introduction of the Dijkstra composite score. Arthritis Rheum. 2005;52(9):2865–2872. doi:10.1002/art.21247
14. Bertamino M, Rossi F, Pistorio A, et al. Development and initial validation of a radiographic scoring system for the hip in juvenile idiopathic arthritis. J Rheumatol. 2010;37(2):432–439. doi:10.3899/jrheum.090691
15. Poznanski AK, Hernandez RJ, Guire KE, Bereza UL, Garn SM. Carpal length in children—a useful measurement in the diagnosis of rheumatoid arthritis and some congenital malformation syndromes. Radiology. 1978;129(3):661–668. doi:10.1148/129.3.661
16. Consensus-Driven Definition for Unequivocal Sacroiliitis on Radiographs for Classification in Juvenile Spondyloarthritis. ACR Meeting Abstracts. Available from: https://acrabstracts.org/abstract/consensus-driven-definition-for-unequivocal-sacroiliitis-on-radiographs-for-classification-in-juvenile-spondyloarthritis/.
17. Backström M, Tynjälä P, Aalto K, et al. Validating 10-joint juvenile arthritis disease activity score cut-offs for disease activity levels in non-systemic juvenile idiopathic arthritis. RMD Open. 2019;5(1):e000888. doi:10.1136/rmdopen-2018-000888
18. Capela RC, Corrente JE, Magalhães CS. Comparison of the Disease Activity Score and Juvenile Arthritis Disease Activity Score in the juvenile idiopathic arthritis. Rev Bras Reumatol Engl Ed. 2015;55(1):31–36. doi:10.1016/j.rbre.2014.08.009
19. Wallace CA, Giannini EH, Huang B, et al. American College of Rheumatology provisional criteria for defining clinical inactive disease in select categories of juvenile idiopathic arthritis. Arthritis Care Res. 2011;63(7):929–936. doi:10.1002/acr.20497
20. Miller ML, Ruprecht J, Wang D, et al. Physician assessment of disease activity in JIA subtypes. Analysis of data extracted from electronic medical records. Pediatr Rheumatol. 2011;9(1):9. doi:10.1186/1546-0096-9-9
21. Backström M, Tarkiainen M, Gottlieb BS, et al. Paediatric rheumatologists do not score the physician’s global assessment of juvenile idiopathic arthritis disease activity in the same way. Rheumatology. 2023:kead151. doi:10.1093/rheumatology/kead151
22. Turk M, Pope JE. Physician global assessments for disease activity in rheumatoid arthritis are all over the map! RMD Open. 2018;4(1):e000578. doi:10.1136/rmdopen-2017-000578
23. Alongi A, Giancane G, Naddei R, et al. Drivers of non-zero physician global scores during periods of inactive disease in juvenile idiopathic arthritis. RMD Open. 2022;8(1):e002042. doi:10.1136/rmdopen-2021-002042
24. Knowlton N, Jiang K, Frank MB, et al. The meaning of clinical remission in polyarticular juvenile idiopathic arthritis: gene expression profiling in peripheral blood mononuclear cells identifies distinct disease states. Arthritis Rheum. 2009;60(3):892–900. doi:10.1002/art.24298
25. Jiang K, Frank M, Chen Y, Osban J, Jarvis JN. Genomic characterization of remission in juvenile idiopathic arthritis. Arthritis Res Ther. 2013;15(4):R100. doi:10.1186/ar4280
26. Nordal E, Zak M, Berntson L, et al. Juvenile Arthritis Disease Activity Score (JADAS) based on CRP; validity and predictive ability in a Nordic population-based setting. Pediatr Rheumatol. 2011;9(S1):P155. doi:10.1186/1546-0096-9-S1-P155
27. Consolaro A, Ruperto N, Bracciolini G, et al. Defining criteria for high disease activity in juvenile idiopathic arthritis based on the Juvenile Arthritis Disease Activity Score. Ann Rheum Dis. 2014;73(7):1380–1383. doi:10.1136/annrheumdis-2013-204186
28. Magni-Manzoni S, Ruperto N, Pistorio A, et al. Development and validation of a preliminary definition of minimal disease activity in patients with juvenile idiopathic arthritis. Arthritis Care Res. 2008;59(8):1120–1127. doi:10.1002/art.23916
29. Sieper J, Van Der Heijde D, Landewe R, et al. New criteria for inflammatory back pain in patients with chronic back pain: a real patient exercise by experts from the Assessment of SpondyloArthritis international Society (ASAS). Ann Rheum Dis. 2009;68(6):784–788. doi:10.1136/ard.2008.101501
30. Lurati A, Pontikaki I, Teruzzi B, et al. A comparison of response criteria to evaluate therapeutic response in patients with juvenile idiopathic arthritis treated with methotrexate and/or anti–tumor necrosis factor α agents. Arthritis Rheum. 2006;54(5):1602–1607. doi:10.1002/art.21784
31. De Benedetti F, Brunner H, Ruperto N, et al. Efficacy and safety of tocilizumab (TCZ) in patients with systemic juvenile idiopathic arthritis (sJIA): TENDER 52-week data; 2012:10. Available from: https://www.cochranelibrary.com/central/doi/10.1002/central/CN-01028625/full.
32. Ruperto N, Brunner H, Quartier P, et al. Efficacy and safety of canakinumab, fully human anti-interleukin-1beta antibody, in systemic juvenile idiopathic arthritis. Ann Rheum Dis. 2013;71. doi:10.1136/annrheumdis-2012-eular.1180
33. Buckland J. Biologic therapy for systemic juvenile idiopathic arthritis—times they are a’changing! Nat Rev Rheumatol. 2013;9(2):63. doi:10.1038/nrrheum.2013.2
34. Sharp JT, Young DY, Bluhm GB, et al. How many joints in the hands and wrists should be included in a score of radiologic abnormalities used to assess rheumatoid arthritis? Arthritis Rheum. 1985;28(12):1326–1335. doi:10.1002/art.1780281203
35. Larsen A. How to apply Larsen score in evaluating radiographs of rheumatoid arthritis in long-term studies. J Rheumatol. 1995;22(10):1974–1975.
36. Rossi F, Di Dia F, Galipò O, et al. Use of the sharp and Larsen scoring methods in the assessment of radiographic progression in juvenile idiopathic arthritis. Arthritis Care Res. 2006;55(5):717–723. doi:10.1002/art.22246
37. Poznanski AK. Radiological approaches to pediatric joint disease. J Rheumatol Suppl. 1992;33:78–93.
38. What is PROMIS? PROMIS Health Organization. Available from: https://www.promishealth.org/57461-2/.
39. Ader DN. Introduction: developing the Patient-Reported Outcomes Measurement Information System (PROMIS). Med Care. 2007;45(5):S1–S2. doi:10.1097/01.mlr.0000260537.45076.74
40. Consolaro A, Ruperto N, Pistorio A, et al. Development and initial validation of composite parent- and child-centered disease assessment indices for juvenile idiopathic arthritis. Arthritis Care Res. 2011;63(9):1262–1270. doi:10.1002/acr.20509
41. Filocamo G, Consolaro A, Schiappapietra B, et al. A new approach to clinical care of juvenile idiopathic arthritis: the juvenile arthritis multidimensional assessment report. J Rheumatol. 2011;38(5):938–953. doi:10.3899/jrheum.100930
42. Lovell DJ, Brunner HI, Ringold S, et al. The American English version of the Juvenile Arthritis Multidimensional Assessment Report (JAMAR). Rheumatol Int. 2018;38(1):35–42. doi:10.1007/s00296-018-3984-6
43. Varni JW, Seid M, Smith Knight T, Burwinkle T, Brown J, Szer IS. The PedsQLTM in pediatric rheumatology: reliability, validity, and responsiveness of the Pediatric Quality of Life InventoryTM generic core scales and rheumatology module. Arthritis Rheum. 2002;46(3):714–725. doi:10.1002/art.10095
44. Singh G, Athreya BH, Fries JF, Goldsmith DP. Measurement of health status in children with juvenile rheumatoid arthritis. Arthritis Rheum. 1994;37(12):1761–1769. doi:10.1002/art.1780371209
45. Filocamo G, Sztajnbok F, Cespedes-cruz A, et al. Development and validation of a new short and simple measure of physical function for juvenile idiopathic arthritis. Arthritis Care Res. 2007;57(6):913–920. doi:10.1002/art.22900
46. Wright V, Longo Kimber J, Law M, Goldsmith C, Crombie V, Dent P. The Juvenile Arthritis Functional Status Index (JASI): a Validation Study. J Rheumatol. 1996;23(6):1066–1079.
47. Lovell DJ, Shear E, Hartner S, et al. Development of a disability measurement tool for juvenile rheumatoid arthritis. The juvenile arthritis functional assessment scale. Arthritis Rheum. 1989;32(11):1390–1395. doi:10.1002/anr.1780321107
48. Howe S, Levinson J, Shear E, et al. Development of a disability measurement tool for juvenile rheumatoid arthritis. The juvenile arthritis functional assessment report for children and their parents. Arthritis Rheum. 1991;34(7):873–880. doi:10.1002/art.1780340713
49. Kvrgic Z, Asiedu GB, Crowson CS, Ridgeway JL, Davis JM. “Like No One Is Listening to Me”: a qualitative study of patient-provider discordance between global assessments of disease activity in rheumatoid arthritis. Arthritis Care Res. 2018;70(10):1439–1447. doi:10.1002/acr.23501
50. Mosor E, Studenic P, Alunno A, et al. Young people’s perspectives on patient-reported outcome measures in inflammatory arthritis: results of a multicentre European qualitative study from a EULAR task force. RMD Open. 2021;7(1):e001517. doi:10.1136/rmdopen-2020-001517
51. Ferreira RJO, de Wit M, Henriques M, et al. “It can’t be zero!” Difficulties in completing patient global assessment in rheumatoid arthritis: a mixed methods study. Rheumatology. 2020;59(5):1137–1147. doi:10.1093/rheumatology/kez467
52. Sztajnbok F, Coronel-Martinez DL, Diaz-Maldonado A, et al. Discordance between physician’s and parent’s global assessments in juvenile idiopathic arthritis. Rheumatology. 2007;46(1):141–145. doi:10.1093/rheumatology/kel201
53. Brandon TG, Becker BD, Bevans KB, Weiss PF. Patient-reported outcomes measurement information system tools for collecting patient-reported outcomes in children with juvenile arthritis. Arthritis Care Res. 2017;69(3):393–402. doi:10.1002/acr.22937
54. Craig J, Feldman BM, Spiegel L, Dover S. Comparing the measurement properties and preferability of patient-reported outcome measures in pediatric rheumatology: PROMIS vs CHAQ. J Rheumatol. 2021;48(7):1065–1072. doi:10.3899/jrheum.200943
55. Bovis F, Consolaro A, Pistorio A, et al; For the Paediatric Rheumatology International Trials Organisation (PRINTO). Cross-cultural adaptation and psychometric evaluation of the Juvenile Arthritis Multidimensional Assessment Report (JAMAR) in 54 languages across 52 countries: review of the general methodology. Rheumatol Int. 2018;38(S1):5–17. doi:10.1007/s00296-018-3944-1
56. Ravelli A, Consolaro A, Horneff G, et al. Treating juvenile idiopathic arthritis to target: recommendations of an international task force. Ann Rheum Dis. 2018:annrheumdis-2018–213030. doi:10.1136/annrheumdis-2018-213030
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.