")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 12
Comparison of the effect of two therapeutic exercises on the inflammatory and physiological conditions and complications of diabetic neuropathy in female patients
Authors Nadi M , Bambaeichi E, Marandi SM
Received 22 February 2019
Accepted for publication 29 June 2019
Published 20 August 2019 Volume 2019:12 Pages 1493—1501
DOI https://doi.org/10.2147/DMSO.S206454
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Maryam Nadi,1 Effat Bambaeichi,2 Seyyed Mohammad Marandi2
1Exercise Physiology, University of Isfahan, Isfahan, Iran; 2Faculty of Sport Sciences Department, University of Isfahan, Isfahan, Iran
Correspondence: Effat Bambaeichi
Faculty of Sport Sciences Department, University of Isfahan, Azadi Square, Isfahan 8174673441, Iran
Tel +98 913 205 0472
Email [email protected]
Introduction and aim: The purpose of this study was to compare the effect of 12 weeks of low-intensity resistance training and exercises for peripheral neuropathy (EPN) on the inflammatory and physiological conditions, balance, and complications of diabetic neuropathy in female patients.
Materials and methods: 45 women with mild to moderate diabetic neuropathy and an average age of 55.46±3.06 years voluntarily participated in the study. They were randomly assigned to either control (n=15), resistance (n=15), and EPN (n=15) groups. Both experimental groups were trained for 12 weeks (three sessions per week). EPN group did peripheral neuropathic exercises (12 lower extremity movements), and the resistance group performed their exercises with a 30% repetition maximum. During the intervention period, the control group only performed their daily activities. Blood samples were taken in both pre-test and post-test to investigate the levels of Tumor necrosis-α (TNF-α), Interleukin-10 (IL-10), C Reactive Protein (CRP), fast blood glucose (FBG) and Glycated hemoglobin (HbA1c). Complications of diabetic neuropathy were measured using the Michigan questionnaire and the Monofilament 10 g. In order to measure the balance, De Morton mobility index (DEMMI) was used.
Results: The statistical analyses showed a significant decrease of FBG and HbA1c in the two experimental groups, as compared to the control group. TNF-α and CRP levels were decreased in both EPN and resistance groups, as compared to the control group. The observed increase in the serum IL-10 levels of the two experimental groups was not, however, significant, as shown in intra-group and inter-group comparisons. On the other hand, the two complications of pain and tingling in the lower limb extremities were improved in both experimental groups (p<0.05). However, the numbness complication showed no significant change (p=0.10). Static and dynamic balance was improved in the EPN group as well (p<0.05).
Conclusion: Since EPN exercises, in contrast to resistance exercises, are focused on the lower limb extremities and designed for diabetic neuropathy patients, they can improve the imbalance, pain and tingling, by significantly reducing TNF-α and CRP and improving the physiological conditions.
Keywords: TNF-α, IL-10, CRP and diabetic neuropathy exercises
Introduction
Diabetic neuropathy is seen in 50% of the patients with type 1 and type 2 diabetes.1,2 In diabetic neuropathy, bad physiological conditions (chronic hyperglycemia, glycogenic hemoglobin) are imposed on the patient, which can damage the nerve tissue and create various clinical manifestations such as pain, numbness and tingling of the organs, as well as imbalance in these patients.3 Also, these physiological disorders can be associated with inflammatory and proinflammatory responses such as increased Tumor necrosis factor-α (TNF-α) and Interleukin-10 (IL-10), and C-reactive protein (CRP).4–6
Increased TNF-α and IL-10 and CRP are the phenomena related to the pro-inflammatory response to diabetes and changes associated with diabetic neuropathy.5,7 Evidence suggests the excessive expression of TNF-α mRNA in neuropathic pain conditions.8 Duksal et al (2016) have reported that a decrease in the serum levels of IL-10 and an increase in TNF-α in the patients with pre-diabetes and type 2 diabetes are accompanied with sensory and motor neurological symptoms.9 In a study done by Kang et al (2005), it was found that serum CRP levels in the patients with metabolic syndrome were significantly higher than those in the healthy subjects. It was also reported that only diabetic neuropathy correlated with serum increased the CRP levels among the microvascular complications.10
Among the recommended therapies for the treatment of diabetic neuropathy, exercise can be effective with a non-pharmacological and low-cost approach.11 In fact, exercise can improve the physiologic state of the patient by providing a protective role against this complication and even delay its onset.12,13
Although athletic exercises are very useful for controlling diabetes, its effects on diabetic neuropathy, especially on its painful type, are not fully understood. Resistance exercises can cause chronic muscle tension, such as maximum strength, hypertrophy, strength and local endurance.14,15 It is advisable to use resistance training for all patients with any complication, but we should seek for appropriate and special conditions for diabetic neuropathy patients; for example, exercise should not expose the patient to the diabetic foot ulcer.
Exercise for peripheral neuropathy (EPN), focusing on the lower extremities, provide the conditions for exercising without wearing shoes and using the hard equipment. In fact, such exercises allow the patient to regularly check his limbs and be aware of wounds and bleeding.16,17
EPN exercises use the entire range of joints motion and these exercises are followed with and without weight bearing (sitting on the chair), while they do not follow a uniform and automatic pattern (as in cycling).18,19 In the previous studies, the use of such exercises has been accompanied by improvements in the balance and the cardio-respiratory health of the patients.20
Given the little information about the exercise for diabetic neuropathy patients and the extent of the complications of this disease in the patients, we decided to provide a therapeutic approach and compare it with the common practice, in order to investigate the inflammatory and physiological conditions, balance and complications of diabetic neuropathy in the female patients.
Materials and methods
Subjects
45 women with mild to moderate neuropathy (55.46±3.06 years,161.30±4.94 cm height, 72.6±31.50 kg weight, and the duration of diabetes 11.24±2.46 years) voluntarily participated by filling the consent letter in this study. All subjects were disabled with no regular activity during the past six months. These subjects had not participated in any specific exercise plan before and used no anti-inflammatory drugs. This study was approved by the Human Ethics Committee of the University of Isfahan with the ethics code 1397.156.IR.UI.REC.
Design
The research was applied in terms of purpose and quasi-experimental in terms of data collection method. After the initial stages, 45 tests were randomly divided into 3 groups (control group, EPN training group and resistance training group) (Figure 1). The subjects of the two training groups, in separate sessions, had full knowledge of how the exercises were supposed to be conducted and the conditions under which they had to the training sessions. At the beginning and end of the sessions, during 10 mins, warm-up and rehearsal exercises were practiced, which included simple movements and light stretching exercises. EPN group exercises included 12 movements (hamstring stretching, knee swirling, gradual stretching of the sciatic nerve, stretching of the leg muscles, ankle range movements, bending of the toes, special movements of the big toe, alternate heel-toe movement, inversion and eversion movements of the ankles, squatting with the help of the wall, and standing on one leg). These moves were first performed in a set of 30 seconds, but every two weeks, one set was added; so there were 5*30-second sets at the end. The resting time between the sets was 30 seconds.20
 |
Figure 1 Chart of subject’s selection. |
The movements of the resistance group consisted of leg press, arm curls, military press, push-ups, squats, knee extensions, heel raises, back extensions, knee sit-ups, and upright rowing.15 To determine the intensity of the resistance training, 30 percent of the maximum repetition exercise was used;21 the overload was followed like the training sessions of the EPN group (Table 1).
 |
Table 1 Summary of the training sessions |
At the beginning and end of each session, blood glucose levels were measured. When blood glucose was not in the range of 110–260 milligrams per deciliter before training, the patients were prohibited from exercising. If any of the subjects suffered from any specific disease, such as autoimmune diseases, serious liver problems, renal failure, inappropriate thyroid gland function, untreatable blood pressure, any infection, cerebrovascular injury, columnar fractures and tumor, they would not be allowed to participate in the research. Voluntary withdrawal, irregular participation at meetings, failure to complete tests, weight changes of more than 3 kg during the course of intervention, other complications of diabetes, change in the type of drug taken, the use of anti-inflammatory drugs and blood glucose imbalance before the onset of the training session in three successive times were the other conditions determined for non-participation in the research22 (Figure 1).
Data collection tools
To determine neuropathy, Michigan neuropathy screening instrument and the 10-gram monofilament device were used. The Michigan Neuropathy Review Toolkit, developed by the researchers at the University of Michigan in 2000, was used to diagnose peripheral neuropathy in the diabetics’ patients. This tool examines the 4 factors representing the expression of the foot skin (dryness, cracks, bumps, infections and deformities), scarring, Achilles tendon reflex, and vibration sensation condition. If the patient had the sign, she would score one; otherwise, the score would be zero. For the examination of the Achilles tendon reflex and vibration of the patient’s big toe, a 128 Hz diapason and a monofilament instrument were used. In the case of the positive vibration of the big toe and the positive results of monofilament in each part, the subject received a zero score, but if the test were negative, she would get a score of one. In the case of getting at least two scores, the person would be a peripheral neuropathy patient.23
De Morton mobility index (DEMMI) test was also used to measure static and dynamic balance. In this method, the static balance is measured on one leg and two legs, as well as at the closing of the eyes; on the other hand, the dynamic balance is measured and evaluated when the patient jumps and moves four steps back.24
In order to further control the nutrition, FFQ was completed and the patients were requested during the study not to change their nutritional process and to continue this procedure until the post-test.25
Height was estimated with the approximation of 0.1 centimeters and weight was calculated with the approximation of 0.1 kg. BMI was calculated through dividing the weight by the square of height to the power of 2. By using (Beurer PM 80 Heart Monitor) the heart rate was recorded before and after exercise.
In order to understand the stress and difficulty of the exercise, the Borg scale was used; the intensity and severity of the exercises in both training groups were similar.
HbA1C was measured by the high performance liquid chromatography reference (HPLC) method, using quantitative detection kits of these variables by the photometric method, as provided by Pars Kit Tests. The levels of IL-10 and TNF-α were measured by using the relevant kits from ESTBIOPHARM Co, which were (Cat.No:C0K-E10140) and (Cat.No:CK-E10110), respectively, through the ELISA method. The CRP measurement kit was also provided by the same company with the number (Cat.No:CK-E11196); in the same way, two other inflammatory variables were measured.
Date analysis
Statistical analyses were performed using SPSS, version 21. The Shapiro-Wilks test was also used to evaluate the normal distribution of all parameters. When data were normally distributed, one-way analysis of variance (ANOVA) was used to test the differences in the continuous variables between the groups, and the Student’s paired t-test was used to test for the differences in the continuous variables within groups. Post-hoc analyses were also performed using the LSD test. The differences between the categorical variables were analyzed using the χ2 test. P<0.05 was considered statistically significant.
Results
The mean and standard deviation of anthropometric indices, body composition, and … related to the subjects studied are presented in Table 2.
 |
Table 2 Clinical characteristics of the studied subjects |
According to Table 2, we found that there was no significant difference between the groups. The results of the statistical analysis in the evaluated factors are presented in Table 3.
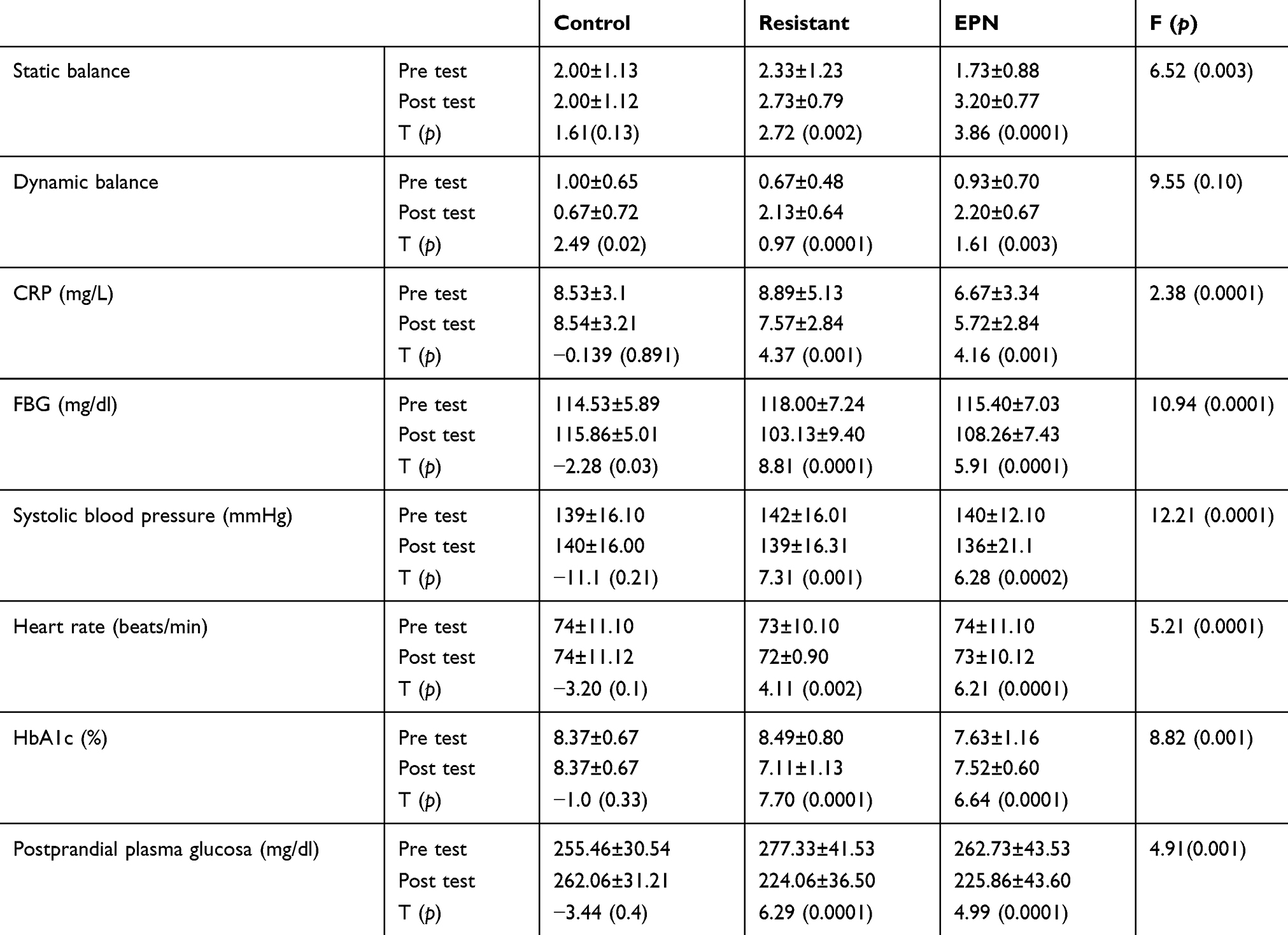 |
Table 3 Comparison of the inflammatory and anti-inflammatory factors and physiological and glycemic conditions of the patients before and after intervention |
The observed changes in the level of all variables except IL-10 were significant. Tukey’s post hoc test showed that the observed difference in TNF-α, CRP and FBG variables was between the two control and EPN groups (p<0.05). Also, heart rate, systolic blood pressure and blood glucose variables after the meal were significantly different in the two groups (p<0.05) (Figure 2 and Table 3). Static and dynamic balance was increased based on intra-group comparison in both resistance and EPN groups. Comparison between the groups showed a significant difference between the EPN group and the other two groups (p=0.003).
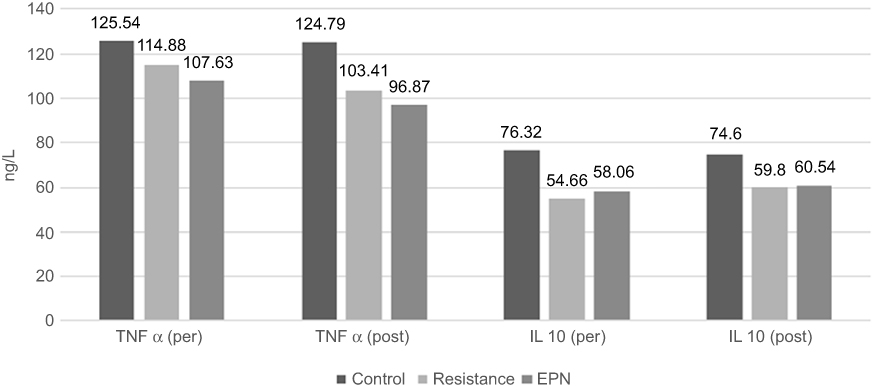 |
Figure 2 Concentration of cytokine in the pre-test and post-test in the three groups. (p<0.05). Abbreviations: TNF-α, tumor necros is factor-α; IL-10, interleukin 10. |
The data obtained from the analysis of diabetic neuropathy symptoms are presented in Table 4.
 |
Table 4 Symptoms of diabetic neuropathy |
As shown in Table 3, two complications of pain and tingling of the organs were associated with the improvement in both experimental groups. Also, the numbness effect showed visible changes (p<0.05).
Discussion
This research is one of the first studies comparing the effects of different training practices on the inflammatory and physiological conditions, and the complications of diabetic neuropathy in the diabetic women. In the present study, the levels of FBG, HbA1C, TNF-α, CRP, systolic blood pressure and heart rate were found to be decreased in both experimental groups, as compared with the control group. However, IL-10 did not significantly increase in both experimental groups. Static and dynamic balance was improved in the EPN group (p<0.05). Complications of diabetic neuropathy, such as pain and tingling, were reduced following the improvement of the patients’ physiological and inflammatory conditions. The main finding of this study was that EPN exercises could improve glycemic conditions (decreasing FBG and HbA1C), inflammation (reducing TNF-α and CRP) and balance in the diabetic neuropathy patients more than the other types of exercises (low-intensity exercise training). Thus, these could improve the complications of diabetic neuropathy.
Since EPN exercises are precisely aligned with the physical conditions of the patients and keep the patient from performing difficult movements on devices and sports equipment (such as dumbbells or weights), in addition to ensuring the safety and health of the patient; Doing such exercises is feasible and easy for the patient; the patient is also able to do more of the activity.
Exercise can create a variety of metabolic adaptations in the body, as well as improving the sensitivity to insulin and glycemic control. Recent research has shown that resistance exercises have different benefits in the patients. Even more, in some studies, the superiority of resistance training over aerobics training has been proven; resistance training reduces HbA1c, lipid volume and systolic blood pressure.15,26,27 However, in this study, by using EPN exercises and focusing on the lower extremities of the patients, in addition to the benefits of resistance training in the patients, we could significantly decrease the serum levels of TNF-α and CRP in them, ultimately leading to improving the sensation of pain and tingling in the patients. TNF-α is an anti-inflammatory cytokine that can cause pain by affecting sensory neurons. Research indicates that this factor is elevated in plasma and its mRNA levels in diabetic neuropathy patients, as compared with the healthy controls. It is correlated with the severity of pain.28 Pedersen et al (2017) also found that exercise with the increased levels of IL-6 could reduce the chronic and malignant increase of TNF-α in the patients with diabetes.29 On the other hand, in different studies, CRP levels in diabetic neuropathic patients have been reported to be higher than those in the control group.10 In addition, compared to the CRP levels in the painful and painless neuropathy, the amount of this inflammatory factor is significantly higher in the people with a painful neuropathy.30 Many factors contribute to the increase or decrease of CRP. Smith et al (1999) reported that after long-term exercise, a 35 percent reduction in CRP levels was observed in the people at the risk for heart diseases.31 This inflammatory factor is secreted from the liver and can cause resistance to insulin.32 In the present study, it was found that EPN exercises could create a higher level of activity and promote the motivation of the patient to perform movements by creating a safe mindset in the patients and preventing them from wounds, infection, and the constant fear of imbalance during work.
IL-10, with its anti-inflammatory effects, can help patients. Studies have shown that the injection of this cytokine can prevent the death of a patient; for example, in the mice that are genetically affected by proteinuria, the IL-10 injection decreases the severity of the disease, as observed in diabetic nephropathy.33 Physical activity can promote the anti-inflammatory activity by increasing the levels of IL-10 and IL-6, as well as decreasing TNF-α production.34 The presence of high glucose in the cells of microglia and astrocytes triggers the activation of Glycogen synthase kinase (GSK-3), which releases some inflammatory factors, such as TNF-α, and can act against the non-release of anti-inflammatory factors such as IL-10. Physical activity and exercise, by placing the body in a catalytic state, can reduce the excessive activity of this kinase.33 On the other hand, physical activity, by removing glucose from the bloodstream, can reduce the production of advanced glycation end products (AGE) and more inflammatory factors.35 In this study, despite an increase in the amount of IL-10 in both experimental groups, there was no significant change, which might be due to the low sample size and statistical power.
Static and dynamic balance was significant in both experimental groups based on intra-group comparisons; however, according to in the inter-group comparisons, only the EPN group showed a significant difference (p=0.003). In the previous studies, samples of these exercises have been effective for the patients.
In a study conducted by Aly et al (2007), which was carried out on 30 men with diabetic neuropathy, as compared to the healthy people, it was found that people with diabetic neuropathy had a lower stability; moreover, over time, instability could get worse, and complications such as falling, multiple fractures and ultimately, death would occur.36
As shown by the results, EPN exercises are not merely a kind of exercise without weight bearing or resistance; in fact, by combining different training types and without a complex appearance, these exercises can improve balance in patients even more than the low-intensity resistance exercises.
Regarding the above, it can be confirmed that exercise and physical activity can reduce the complications of the disease by improving the inflammatory and glycemic conditions of diabetic neuropathy patients. In our study, resistance exercises also led to similar results in the patients with diabetic neuropathy. The EPN training group also experienced a decrease in similar physiological characteristics, with the difference that the rate of these improvements in this group was greater; these positive results were probably due to the concentration of these exercises on the lower extremities and the patient’s comfort during these exercises.
Conclusion
Among the various ways used to improve the condition of diabetic neuropathy patients, exercise and physical activity are a low-cost and non-complicated intervention. In fact, exercise with its sharp and prolonged effects, can have positive effects on the improvement of glycemic conditions and inflammation, thus reducing the complications of diabetic neuropathy. Sports prescribed for the patients with neuropathy should be compatible with the conditions of these patients (wounds, numbness in the legs, sweating and infection, etc.); no shoes wearing, no need for special equipment and the possibility of exercising at home are the most important advantages of training for these patients. According to the results of this study, EPN exercises are, therefore, highly suitable for diabetic neuropathy patients and can control the inflammatory and glycemic conditions by focusing on the lower limbs.
Compliance with ethical standards
This study was conducted in accordance with the Declaration of Helsinki.
Ethical approval
The experimental procedures were in advance approved by the Isfahan University Ethics committee.
Acknowledgments
The authors would like to thank all participants who took part in the study. This work was supported by the Isfahan University.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ang L, Jaiswal M, Martin C, Pop-Busui R. Glucose control and diabetic neuropathy: lessons from recent large clinical trials. Curr Diab Rep. 2014;14(9):528. doi:10.1007/s11892-014-0528-7
2. Andreassen CS, Jakobsen J, Ringgaard S, Ejskjaer N, Andersen H. Accelerated atrophy of lower leg and foot muscles-a follow-up study of long-term diabetic polyneuropathy using magnetic resonance imaging (MRI). Diabetologia. 2009;52(6):1182–1191. doi:10.1007/s00125-009-1320-0
3. Parasoglou P, Rao S, Slade JM. Declining skeletal muscle function in diabetic peripheral neuropathy. Clin Ther. 2017;39(6):1085–1103. doi:10.1016/j.clinthera.2017.05.001
4. Cameron N, Cotter M. Pro-inflammatory mechanisms in diabetic neuropathy: focus on the nuclear factor kappa B pathway. Curr Drug Targets. 2008;9(1):60–67. doi:10.2174/138945008783431718
5. Pop-Busui R, Ang L, Holmes C, Gallagher K, Feldman EL. Inflammation as a therapeutic target for diabetic neuropathies. Curr Diab Rep. 2016;16(3):1–10. doi:10.1007/s11892-016-0727-5
6. Duncan BB, Schmidt MI, Pankow JS, et al. Low-grade systemic inflammation and the development of type 2 diabetes: the atherosclerosis risk in communities study. Diabetes. 2003;52(7):1799–1805. doi:10.2337/diabetes.52.7.1799
7. Shoelson SE, Lee J, Goldfine AB. Review series inflammation and insulin resistance. J Clin Invest. 2006;116(7):1793–1801. doi:10.1172/JCI29069
8. Wilson NM, Wright DE. Inflammatory mediators in diabetic neuropathy. Diabetes Metab. 2011;01(S:5):1–6. doi:10.4172/2155-6156.S5-004
9. Duksal T, Tiftikcioglu BI, Bilgin S, Kose S, Zorlu Y. Role of inflammation in sensory neuropathy in prediabetes or diabetes. Acta Neurol Scand. 2016;133(5):384–390. doi:10.1111/ane.12474
10. Kang TW, Lee EH, Kim MS, Paik SG, Kim S, Kim CB. Relationship of serum high sensitivity C-reactive protein to metabolic syndrome and microvascular complications in type 2 diabetes. Diabetes Res Clin Pract. 2005;69(1):151–156. doi:10.1016/j.diabres.2004.11.014
11. Perkins BA, Olaleye D, Zinman B, Bril V. Simple screening tests for peripheral neuropathy in the diabetes clinic. Diabetes Care. 2001;24(2):250–256. doi:10.2337/diacare.24.2.250
12. Hopps E, Canino B, Caimi G. Effects of exercise on inflammation markers in type 2 diabetic subjects. Acta Diabetol. 2011;48(3):183–189. doi:10.1007/s00592-011-0278-9
13. Sigal RJ, Cep MJA, Bacon SL, et al. Physical activity and diabetes diabetes. Can J Diabetes J. 2018;42:54–63. doi:10.1016/j.jcjd.2017.10.008
14. Turner R. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352(9131):837–853. doi:10.1016/S0140-6736(98)07019-6
15. Ishii T, Yamakita T, Sato OS, Tanaka S, Fujii S. Resistance training improves insulin sensitivity in NIDDM subjects without altering maximal oxygen uptake. Diabetes Care. 1998;21(8):1353–1355. doi:10.2337/diacare.21.8.1353
16. James G, Richard J. Exercises for peripheral neuropathy - physical therapy. Found Peripher Neuropathy. 2016;24:1–6.
17. Streckmann F, Zopf EM, Lehmann HC. Exercise intervention studies in patients with peripheral neuropathy : a systematic review. Sports Med. 2014:1289–1304. doi:10.1007/s40279-014-0207-5
18. Crews RT, Schneider KL, Yalla SV, Reeves ND, Vileikyte L. Physiological and psychological challenges of increasing physical activity and exercise in patients at risk of diabetic foot ulcers: a critical review. Diabetes Metab Res Rev. 2016;32:791–804. doi:10.1002/dmrr.2817
19. Gallen IW. Cycling for people with type 1 diabetes. Pract Diabetes. 2013;30(7):273–277. doi:10.1002/pdi.1791
20. Hansen BMD. Exercising while Living with Neuropathy. IG Living; 2015.
21. Marwick TH, Hordern MD, Miller T, et al. Exercise training for type 2 diabetes mellitus: impact on cardiovascular risk: a scientific statement from the american heart association. Circulation. 2009;119(25):3244–3262. doi:10.1161/CIRCULATIONAHA.109.192521
22. Whiting DR, Guariguata L, Weil C, Shaw J. IDF diabetes atlas: global estimates of the prevalence of diabetes for 2011 and 2030. Diabetes Res Clin Pract. 2011;94(3):311–321. doi:10.1016/j.diabres.2011.10.029
23. Perkins BA, Bril V. Diabetic neuropathy: a review emphasizing diagnostic methods. Clin Neurophysiol. 2003;114(7):1167–1175. doi:10.1016/S1388-2457(03)00025-7
24. Caronni A, Cattalini C, Previtera AM. Balance and mobility assessment for ruling-out the peripheral neuropathy of the lower limbs in older adults. Gait Posture. 2016;50:109–115. doi:10.1016/j.gaitpost.2016.08.029
25. Cade JE, Burley V. Food-frequency questionnaires : a review of their design. Nutr Res Rev. 2004;17:5–22. doi:10.1079/NRR200370
26. Silvestre JGO, Speretta GFF, Fabrizzi F, et al. Acute effects of resistance exercise performed on ladder on energy metabolism, stress, and muscle damage in rats. Motriz, Rio Claro. 2017;23(e101602):1–8. doi:10.1590/s1980-6574201700si0010
27. Perez-Gomez J, Vicente-Rodríguez G, Ara Royo I, et al. Effect of endurance and resistance training on regional fat mass and lipid profile. Nutr Hosp. 2013;28(2):340–346. doi:10.3305/nh.2013.28.2.6200
28. Sorkin LS, Xiao WH, Wagner R, Myers RR. Tumour necrosis factor-α induces ectopic activity in nociceptive primary afferent fibres. Neuroscience. 1997;81(1):255–262. doi:10.1016/S0306-4522(97)00147-4
29. Pedersen BK. Anti-inflammatory effects of exercise: role in diabetes and cardiovascular disease. Eur J Clin Invest. 2017;47(8):600–611. doi:10.1111/eci.12781
30. Doupis J, Lyons TE, Wu S, Gnardellis C, Dinh T, Veves A. Microvascular reactivity and inflammatory cytokines in painful and painless peripheral diabetic neuropathy. J Clin Endocrinol Metab. 2009;94(6):2157–2163. doi:10.1210/jc.2008-2385
31. Smith JK, Dykes R, Douglas JE, Krishnaswamy G, Berk S. Long-term exercise and atherogenic activity of blood mononuclear cells in persons at risk of developing ischemic heart disease. J Am Med Assoc. 1999;281(18):1722–1727. doi:10.1001/jama.281.18.1722
32. Kim ES, Im J-A, Kim KC, et al. Improved insulin sensitivity and adiponectin level after exercise training in obese Korean youth. Obesity. 2007;15(12):3023–3030. doi:10.1038/oby.2007.360
33. Dobson JL, McMillan J, Li L. Benefits of exercise intervention in reducing neuropathic pain. Front Cell Neurosci. 2014;8(102):1–9. doi:10.3389/fncel.2014.00102
34. Jorge MLMP, De Oliveira VN, Resende NM, et al. The effects of aerobic, resistance, and combined exercise on metabolic control, inflammatory markers, adipocytokines, and muscle insulin signaling in patients with type 2 diabetes mellitus. Metabolism. 2011;60(9):1244–1252. doi:10.1016/j.metabol.2011.01.006
35. Huebschmann AG, Regensteiner JG, Vlassara H, Reusch JEB. Diabetes and advanced glycoxidation end products. Diabetes Care. 2006;29(6):1420–1432. doi:10.2337/dc05-2096
36. Aly FA, Fawzy E, Ibrahim M, Mohamed A. Assessment of stability deficits in patients with diabetic peripheral neuropathy. Bull Fac Cairo Univ. 2007;12(1):29–39.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.