")
Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 14
Comparing Dual-Zone Immediate Implant Placement and Socket Shield Technique for Ridge Width Changes in the Maxilla: A Prospective Cohort Study
Authors Shadid RM
Received 26 September 2022
Accepted for publication 16 November 2022
Published 21 November 2022 Volume 2022:14 Pages 321—336
DOI https://doi.org/10.2147/CCIDE.S390131
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Rola Muhammad Shadid1,2
1Department of Prosthodontics, Faculty of Dentistry, Arab American University, Jenin, Palestinian Territory; 2Private Practice, Palestine, Palestinian Territory
Correspondence: Rola Muhammad Shadid, Department of Prosthodontics, Faculty of Dentistry, Arab American University, P.O Box: 240, Jenin, Palestinian Territory, Tel +970 594494066, Email [email protected]
Purpose: The aim of this prospective cohort study was to assess the facial-palatal ridge dimensional changes that occurred at 8– 10 months following flapless dual-zone (DZ) immediate implant placement and socket-shield (SS) immediate placement in the maxilla.
Materials and Methods: A total of 19 patients who received 20 implants were included, with 10 implants (MegaGen AnyRidge) placed for each treatment, DZ and SS. Cast models were made at 8– 10 months after implant placement to assess the dimensional ridge changes by measuring the facial-palatal ridge width on implant sites (T) at six designated points starting from the gingival margin (0, 1, 2, 3, 5 and 7) and comparing it with the corresponding measurement on the contralateral tooth site (C).
Results: All 20 implants demonstrated successful osseointegration at 8– 10 months follow-up (survival rate 100%). Two out of ten cases of SS group presented with minor manageable complications of external shield exposure. DZ group showed an average of 0.3 mm facial-palatal ridge width reduction, while SS group revealed a mean gain in ridge width of approximately 0.2 mm at 8– 10 months follow-up.
Conclusion: When comparing between two treatments, there was a significant difference in ridge width change at 8– 10 months following implant placement, indicating better preservation of the ridge contour for socket shield technique.
Keywords: follow-up studies, investigative techniques, dental implantation, osseointegration
Introduction
After tooth extraction, alveolar ridge resorption vertically and horizontally will certainly occur,1,2 mainly on the facial side.1 This is highly expected because once the tooth is extracted, the alveolar ridge loses one of the main vascular supplies to the facial plate, which is the periodontal ligament.3 In addition, the facial plate thickness in the anterior maxilla has been reported to be 1 mm or less for nearly ninety percent of the patients,4 making it more prone to surgical trauma and resorption.3 Furthermore, this 1-mm facial plate is composed mainly of cortical bone without any vascular supply from the bone marrow.3 This ridge resorption will have a negative effect on the implant position and on the emergence profile of implant restoration,5 leading to esthetic and biological complications, mainly in the maxillary anterior region. Consequently, every effort has been made to preserve or limit the physiological ridge collapse that occurs following tooth extraction, including socket preservation techniques6,7 and bone augmentation using different bone materials and different membranes.8,9 When accompanied by immediate implant placements, numerous recommendations and techniques have also been introduced for the same purpose of preserving the peri-implant hard and soft tissues. These include atraumatic tooth extraction, meticulous case selection,10 flapless implant placement,11 ideal 3-D implant positioning,11 filling the jumping gap and the area up to the gingival margin level with bone substitute (dual-zone),12 connective tissue grafting at the time of immediate implantation,13 immediate provisionalization,14 and the use of implants with platform switching designs.15 However, none of those procedures could prevent the physiological bone remodel that occurs postextraction since the main causes of the periodontal ligament loss and the thin facial bundle bone are still prevailing.16,17
As a result, this has led to the rethinking of a previously introduced technique of root submergence which was firstly used in completely edentulous ridges to maintain the denture supporting area.18 Then, this technique was used to preserve the alveolar ridges under pontics of fixed partial dentures.19 Based on the same concept of maintaining the periodontium of periodontal ligament, cementum and bundle bone, Hurzeler et al20 in 2010 introduced the “socket shield (SS)” technique. This technique involves maintaining the facial segment of the root that is intended to be extracted and immediately replaced with an implant by decoronating the tooth, sectioning the root mesiodistally, then removing the palatal segment with the apex while maintaining the facial segment. The implant is then placed palatal to the shield.20
Systematic reviews,21,22 case series,15,23–26 case reports,27–37 technical reports,38,39 animal randomized controlled trials,40,41 and human randomized clinical studies42,43 were conducted to assess the socket shield technique and all showed promising outcomes.
Bramanti et al42 in their randomized controlled trial compared socket shield immediate implant placement technique with conventional immediate implant placement. They reported 100% implant survival rate without any complications up to three years follow-up for both groups; however, the socket shield technique revealed better marginal bone levels and better pink esthetic scores.42 The other RCT43 which also compared between the same previously mentioned two groups demonstrated 100% implant survival rate without any complications up to two years follow-up for both groups; however, the socket shield technique resulted in less midfacial mucosal recession and less dimensional shrinkage of the facial plate.43
A recent systematic review22 concluded that in spite of the high survival rates reported for implants placed with SS technique with only 6.96% of implant failures and complications, this technique still requires more scientific based evidence to be recommended as everyday clinical practice. Thus, the aim of this prospective cohort study (PCS) was to compare the facial-palatal dimensional ridge changes that occurred at 8–10 months following the dual-zone (DZ) immediate implant placement with those occurring following the socket shield (SS) immediate implant placement in the maxilla. Also, this study aimed to report the incidence of any complications that occurred in the 8–10 months follow-up.
The primary outcome was the dimensional facial-palatal ridge change that occurred at 8–10 months following immediate implant placement with the two techniques, and the secondary outcome was the incidence of any biological or biomechanical complications in the 8–10 months follow-up. Additionally, the influence of probable confounders, such as tooth type, gingival biotype, facial plate thickness, and healing pattern on the dimensional facial-palatal ridge changes was also evaluated. The null hypothesis of this PCS was that there were no differences in the facial-palatal dimensional changes at 8–10 months post-implantation between the DZ immediate implant placement and SS immediate implant placement in the maxilla against the alternative hypothesis of a difference.
Materials and Methods
This single-center prospective cohort clinical study was conducted between June 2019 and June 2020 for patients referred to the Faculty of Dentistry, Arab American University, Palestinian Territory. The study was approved by the Arab American University scientific research committee (SRC17/18-10) and performed according to the ethical principles of the Declaration of Helsinki of 1975, as revised in 2013.
The inclusion criteria were any patient requiring at least one immediate implant in the maxilla from the right second premolar to the left second premolar for a nonmobile tooth between two natural teeth, with an existing contralateral tooth; was at least 20 years old; and was able to sign an informed consent form. The tooth site had an acceptable quantity of native bone to attain primary stability, and had an adequate mesio-distal space (≥ 6.5mm) with at least 1.5 mm on each side for 3.5 mm implant platform placement. The exclusion criteria were general contraindications to implant surgery, radiotherapy in the head or neck area, chemotherapy for malignancy in the previous 5 years, uncontrolled diabetes, severe psychiatric disease, patients taking intravenous bisphosphonates, smoker of more than 9 cigarettes a day, pregnant or lactating women, severe parafunctional activity, acute infection or fistula in the site planned for implant insertion, vertical root fracture including the facial root or horizontal fracture apical to facial bone crest, mobility of grade two or more, moderate or severe periodontitis with more than three millimeters attachment loss, extensive apical lesion, ankylosed tooth, class II or III extraction sockets, and not attending the follow-up appointments.
A sum of 40 patients were assessed, of whom 21 were excluded because they did not meet the inclusion criteria (Figure 1). A total of 19 patients who received 20 implants were included. Selected patients received thorough explanations about the provided treatment and signed a written informed consent form in which all treatment risks were explained prior to being enrolled in the study. The 20 implant sites were randomly distributed between the two groups, while if any case of the SS group the facial shield got mobile, it was removed; and the case was transferred to the DZ technique. Overall, ten implants were placed for each treatment, DZ and SS.
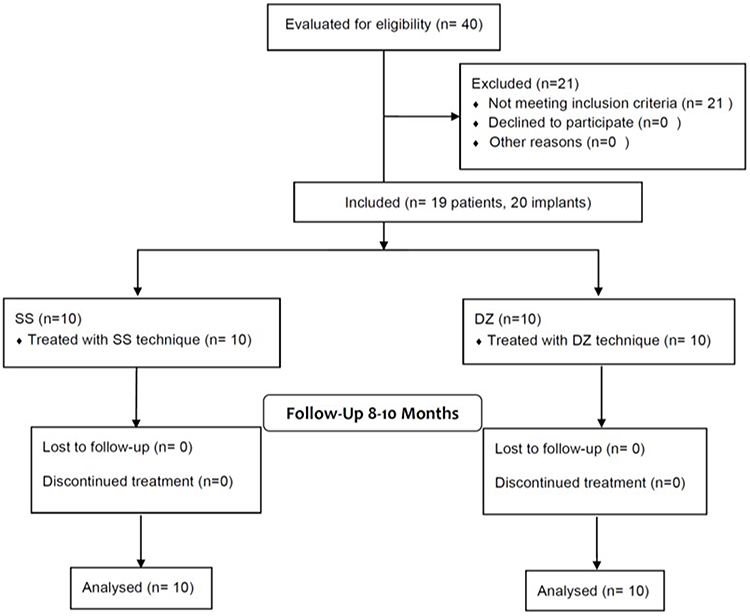 |
Figure 1 Flow diagram of patient selection. |
All the surgical and prosthetic procedures were performed by one experienced dentist (R.S.). Patients were followed for 8–10 months after implant placement; and the patients, the outcome assessor (F.M.) who executed the measurements, and the biostatistician were blinded.
Treatment Procedures
Scaling and oral hygiene instructions were given for each patient two weeks before the surgery. Cone beam computed tomography (CBCT) was ordered for each patient to evaluate the site for the presence of intact bone plates, if there was any pathology, and to assess the sagittal position of the root. All patients received a single dose of prophylactic antibiotic 1 hour prior to the intervention (2 g of amoxicillin or 600 mg of clindamycin, if allergic to penicillin). In addition, patients rinsed with chlorhexidine mouthwash 0.2% for 1 minute prior to the intervention.
Dual-Zone Immediate Implant Placement (DZ)
After the administration of local anesthesia, intrasulcular incision was made around the tooth or retained root to severe the supracrestal fibers. The tooth was carefully luxated using a periotome and removed with forceps. Then, thorough debridement, curettage, and rinsing with sterile saline were performed; and the socket walls were checked with a round-ended probe for the presence of any fenestration or dehiscence defects. The case was included in the study if it had intact socket walls or just a small fenestration on the facial wall with intact marginal bone. The osteotomies were then prepared according to the manufacturer’s instructions of the implant system (MegaGen AnyRidge, MegaGen Implant Co., Ltd., South Korea) and the implants were placed with a handpiece toward the palatal wall up to 4 mm apical to the mid-facial gingival margin. Periapical radiographs were made to verify the position and angulation of the implants; insertion torque (IT) and ISQ values (MegaISQ; MegaGen Implant Co., Ltd) were also registered for each implant. Any implant with IT≥ 25 N/cm and ISQ≥ 65 was attached with an S-shaped customized healing abutment, and any implant with less than those readings was selected for submerged healing.44 For both situations, granules of FDBA (Mineross 300–1000 μm, Biohorizons IPH, Birmingham, AZ, USA) were loosely packed into the jumping gap regardless of its size and up to the gingival margin (dual-zone technique). For implants selected for submerged healing, no primary closure was tried; instead, a collagen sponge was placed on top of bone granules and stabilized with 5/0 polyamide nylon horizontal mattress and interrupted sutures (Filapeau, PETERS, France). For provisionalization, a resin-bonded bridge was stabilized to adjacent teeth. Postsurgery, the patients were asked to take antibiotics (amoxicillin 500 mg three times daily for 7 days), chlorhexidine gluconate 0.2% oral rinse 2 times daily for two weeks, and nonsteroidal anti-inflammatory drugs (ibuprofen 400 mg four times daily for 3 days). Patients were also instructed to avoid brushing the area for 2 weeks. Postsurgical evaluation was made at 1, 3, and 6 weeks to verify if there was any complication or infection. Sutures were removed during the 2-week postoperative visits.
Socket-Shield Immediate Implant Placement (SS)
After local anesthesia administration, the involved tooth was decoronated up to the gingival margin with a high-speed diamond chamfer bur. Then, the root canal was widened with successively increasing diameter Gates Glidden burs up to the apical region to remove all canal contents verifying the correct length by periapical radiographs. To section the root mesiodistally, a long shank high-speed root resection bur (Komet Dental, Germany) was inserted into the same path created by the Gates Glidden until the root was sectioned completely (Figure 2). If possible, the apical portion was aimed to be removed with the palatal portion from the first cut. A small periotome was used to luxate the palatal section toward the space created by sectioning while maintaining finger support on the facial side of the socket to verify if there was any movement during luxating the palatal segment. If the apical portion was not removed with the palatal portion, it was removed by inserting a long shank high-speed bur. Thorough debridement, curettage, and rinsing with sterile saline were made to remove any infectious residues. To prepare the coronal portion of the shield, a microfacial flap was raised to ensure cutting the facial shield up to the facial bone crest without traumatizing the gingiva. Then, a bevel was made on the coronal 2 mm portion of the shield internally with a high-speed round diamond bur. This bevel intended to create a more prosthetic space while reducing the risk of shield exposure. A minimum thickness of 1.5 mm and a length of 6 mm were aimed. All procedures were conducted with magnification and high illumination. If there was any fenestration, it was managed by raising a semilunar flap in the apical area with access to the defect to ensure complete removal of the infected tissue. After assessing the stability of the shield, an implant osteotomy was made in the same manner as in DZ with trying to place an implant without touching the shield. Implant diameter (AnyRidge MegaGen, MegaGen Implant Co., Ltd., South Korea) was selected such that the implant would not contact the shield at the same time to be appropriate for the replaced tooth (Figure 3). The fenestrations when encountered, were grafted using guided bone generation with saline prehydrated FDBA (300–1000 μm, Mineross, Biohorizons IPH, Birmingham, AZ, USA) and collagen membrane (Mem-Lok RCM, Biohorizons IPH, Birmingham, AZ, USA), then primary closure was achieved with a 5/0 polyamide nylon simple interrupted suture (Filapeau, PETERS, France). Granules of FDBA (Mineross, Biohorizons IPH, Birmingham, AZ, USA) were loosely packed into the jumping distance, regardless of its size, and up to the gingival margin. All subsequent steps were made the same as with DZ group. The protocol that was followed for performing SS technique in the present study was according to the most recent proposed guidelines.23,39
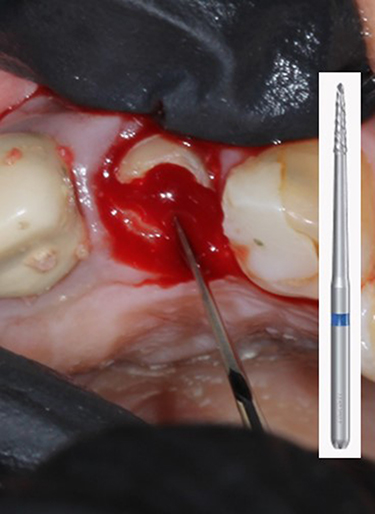 |
Figure 2 Long shank high-speed root resection bur (Komet Dental, Germany) inserted to section the root mesiodistally. |
 |
Figure 3 Incisal view showing implant placement palatal to the prepared facial shield. |
After approximately 4 months, all patients were asked to visit the center to start with the prosthetic part. For nonsubmerged implants, the customized healing abutment was removed, and the ISQ was evaluated to verify that the implant was ready for definitive prosthesis. Submerged implants were uncovered with the punch technique without any soft tissue enhancement, and the ISQ was also assessed. If ISQ was ≥70, the definitive prosthesis impression was made. All implants were ready for loading. To shape the soft tissue, a customized healing abutment was attached to the implant for nearly four weeks before making the final impression. Pick-up implant-level impression copings were joined to the implants with flowable composite injected into the sulcus to transfer the soft tissue emergence profile to the soft tissue cast, and then impressions were made with putty soft/light body addition silicone material (Elite HD+, Zhermack SpA, Italy). Subsequently, screw-retained zirconia or metal-ceramic crowns were joined to the implants and the screws were torqued to 35 N/Cm using a calibrated torque wrench (MegaGen Implant Co., Ltd., South Korea). The access holes were sealed with Teflon tape and flowable bulk fill composite (Palfique Bulk Flow, Tokuyama Dental Corporation, Japan). Periapical radiographs were taken immediately after crown delivery as a postprosthetic baseline.
Casts Analysis
Maintenance and follow-up appointments were scheduled every three months whereas impressions were made with putty soft/light body addition silicone material (Elite HD+, Zhermack SpA, Italy) at 8–10 months after implant placement to assess the dimensional ridge changes that occurred postimplantation according to the method described by Tarnow et al.3 Measurements were made on type 3 gypsum (Marmodent, Siladent, Germany) casts with an electronic digital caliper of 0.01 mm resolution (Salvin Dental Specialties, USA) on both the implant sites (test) and the contralateral tooth sites (control) at six designated points starting from the free gingival margin and advancing toward the apical area (0, 1, 2, 3, 5 and 7 mm)3 (Figures 4 and 5). All measurements were made three times at each point by a trained blinded assessor (F.M.), and the mean of the distances was recorded.
 |
Figure 4 Cast with six designated points starting from gingival margin (0, 1, 2, 3, 5 and 7mm) on both the implant site (T) and contralateral tooth site (C). |
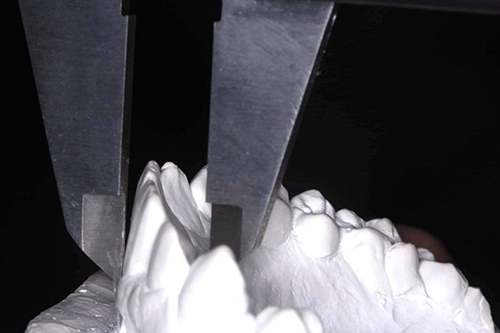 |
Figure 5 Measurement of facial-palatal ridge width with an electronic digital caliper of 0.01 mm resolution. |
Sample Size Calculation
Sample size was calculated using an online calculator (http://riskcalc.org:3838/samplesize/),45 considering Type I error rate, α= 0.05, power=90% (β = 0.1), ratio of case to control, k=1, mean (μ) DZ = 0.6, mean (μ) SS = 0.1 based on previous studies evaluating the facial-palatal ridge dimensional change as a primary outcome,3,24 and expected population standard deviation, SD=0.3;24 the result was 16 for the total sample size with 8 for each group. Considering the possibility of drop out, ten for each group was selected.
Statistical Analysis
Data were analyzed statistically using the Statistical Package for Social Sciences (SPSS), version 22.0. Means and standard deviation (mean ± SD) were used to describe the continuous data, and the percentages were used to present categorical data. Data were examined for normality using the Kolmogorov–Smirnov test. For normally distributed data, the differences in the means between T and C in the same group or (T-C) between groups were evaluated with Independent Samples t-test, while Mann–Whitney U-test was performed for non-normally distributed data. The level of statistical significance was considered at P < 0.05.
To measure the consistency between the three measurements of the facial-palatal ridge width at each point, a two-way mixed effects model of consistency was used to calculate an intraclass correlation coefficient (ICC).
Presentation of Two Treated Cases
Presentation of an SS case (Figure 6) and DZ case (Figure 7). The SS case replacing the maxillary right central incisor revealed superb preservation of the ridge contour with optimum functional and esthetic outcomes. The DZ case replacing the maxillary left first premolar also revealed excellent functional and esthetic results but with some collapse of the ridge facio-palatally.
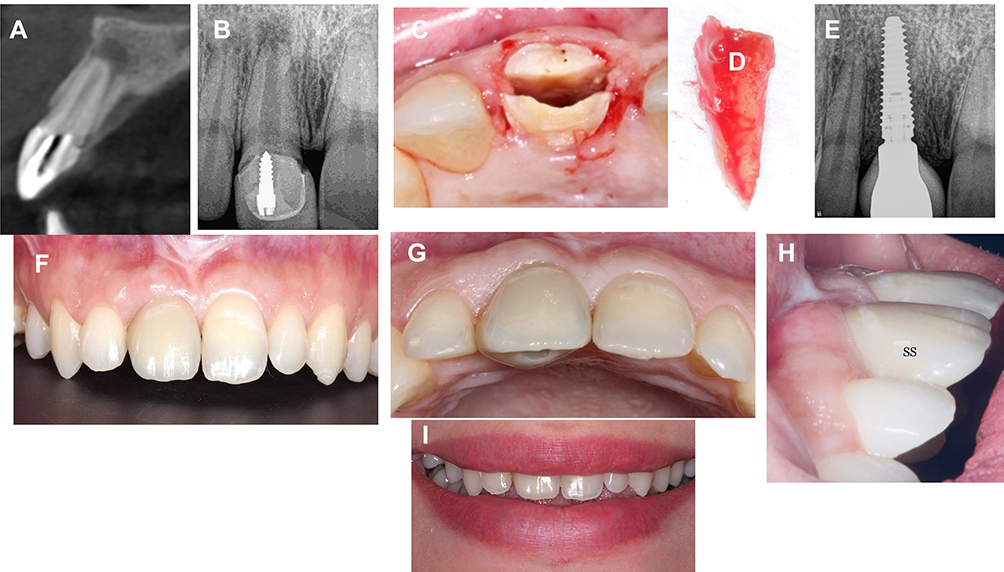 |
Figure 6 Clinical images and radiographs of SS case replacing maxillary right central incisor (A) Cross-sectional view of the preoperative CBCT of right central incisor; (B) Pre-operative periapical radiograph; (C) the sectioned root before palatal fragment removal; (D) The removed palatal segment; (E) postoperative periapical radiograph at 7 months; (F) frontal view of the definitive crown at 14 months; (G) incisal view of definitive crown at 14 months; (H) lateral view of definitive crown at 10 months; (I) smile frontal view. CBCT, cone beam computed tomography. |
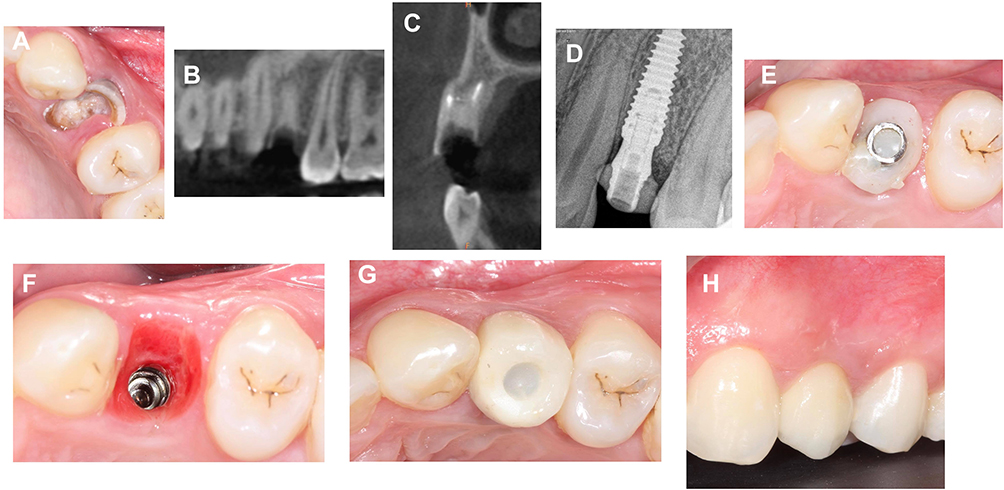 |
Figure 7 Clinical images and radiographs of DZ case replacing maxillary left first premolar (A) Pre-operative occlusal view; (B) panoramic view of the preoperative CBCT; (C) cross-sectional view of the preoperative CBCT of left first premolar; (D) periapical radiograph post-surgery; (E) occlusal view with customized healing abutment at 3 months; (F) occlusal view of the healed peri-implant mucosa at 7 months; (G) occlusal view of the definitive crown at 15 months. Note the ridge contour collapse that occurred facial to the implant; (H) buccal view of definitive restoration at 15 months. CBCT, cone beam computed tomography. |
Results
The study encompassed 19 patients, four men and 15 women, with a mean age of 35.70 ± 11.91 years (range, 20–62 years). Twenty immediate implants were placed in 19 patients with one implant for each patient except a patient who had two implants. The characteristics of the enrolled cases, tooth type, causes of extraction, implant dimensions, healing pattern, and the definitive restoration type are demonstrated in Table 1.
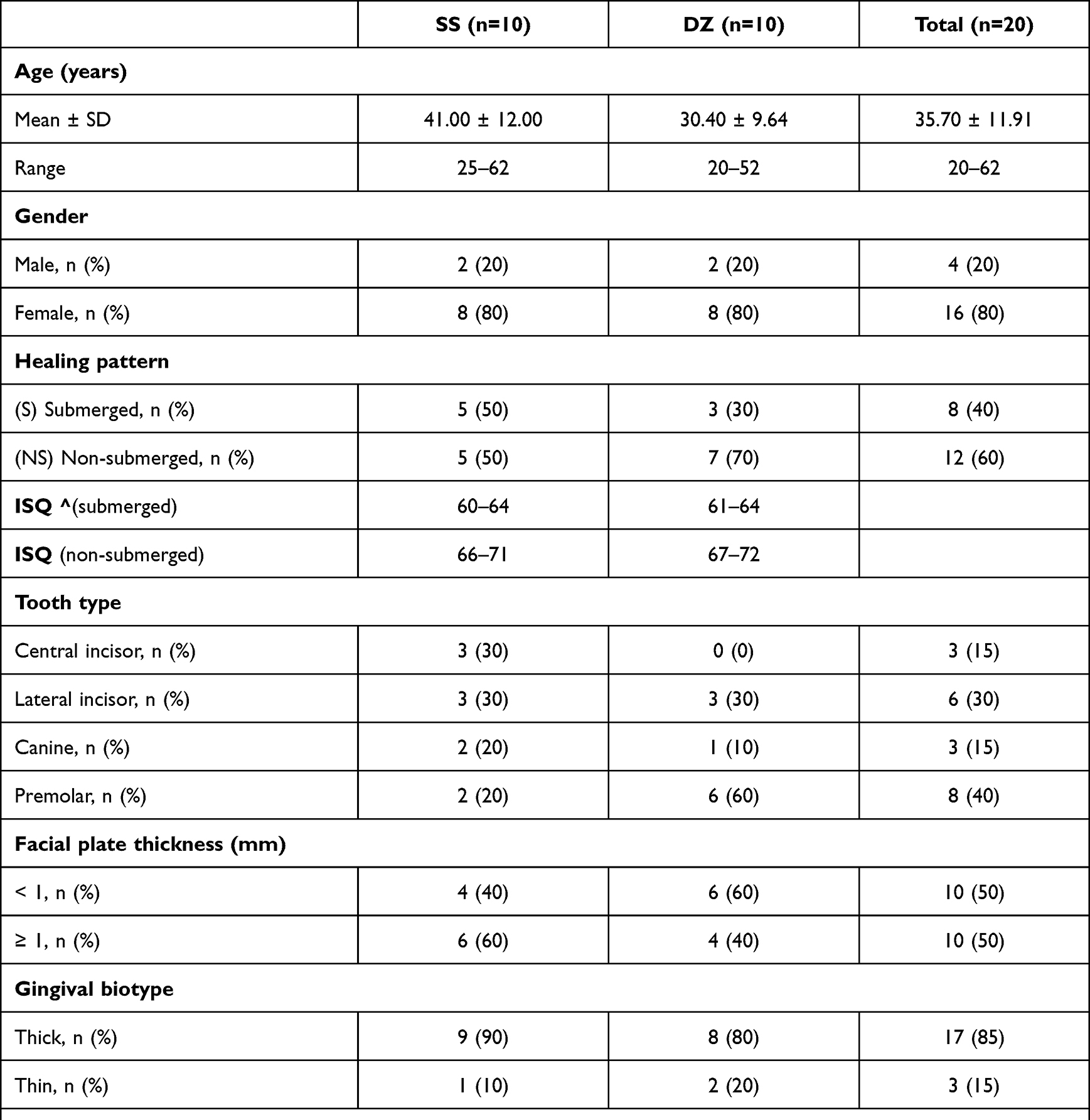 |
Table 1 The Characteristics of the Enrolled Cases, Implant Dimensions, Definitive Restorations, and Complications |
All patients presented for follow-up appointments. Uneventful healing without any postoperative complications occurred for all the ten implants in the DZ group and for 8 implants in the SS group, with an external shield exposure encountered for 2 implants in the one-month follow-up postimplantation. The two external shield exposures where the coronal portion of the shieldperforated the soft tissue were managed by just reducing the exposed part with a high-speed diamond bur, and both healed well with soft tissue coverage. More dimensional ridge shrinkage occurred for those two patients (0.6, 0.7) but without any soft tissue recession or esthetic compromise. The patients were satisfied with the esthetic result and refused any connective tissue grafting. All 20 implants demonstrated successful osseointegration with ISQ values ranging between 70 and 76 at 4 months postimplantation (survival rate 100%).
Twenty type 3 gypsum casts that were made at 8–10 months following implant insertion and at 4 months following crown delivery were evaluated for the facial-palatal ridge dimensions at implant sites (test) and the contralateral tooth sites (control) for both treatments (DZ and SS) and at varying locations from the free gingival margin (0–7 mm). The results demonstrated that the DZ group when averaged over all the reference points showed a facial-palatal reduction of nearly 0.3 mm; however, there were no significant differences between the T and C (P =0.47); while the SS group revealed a mean gain in ridge contour of approximately 0.2 mm with also no significant differences existed between the T and C (P = 0.64) at 8–10 months follow-up (Table 2, Figures 8 and 9).
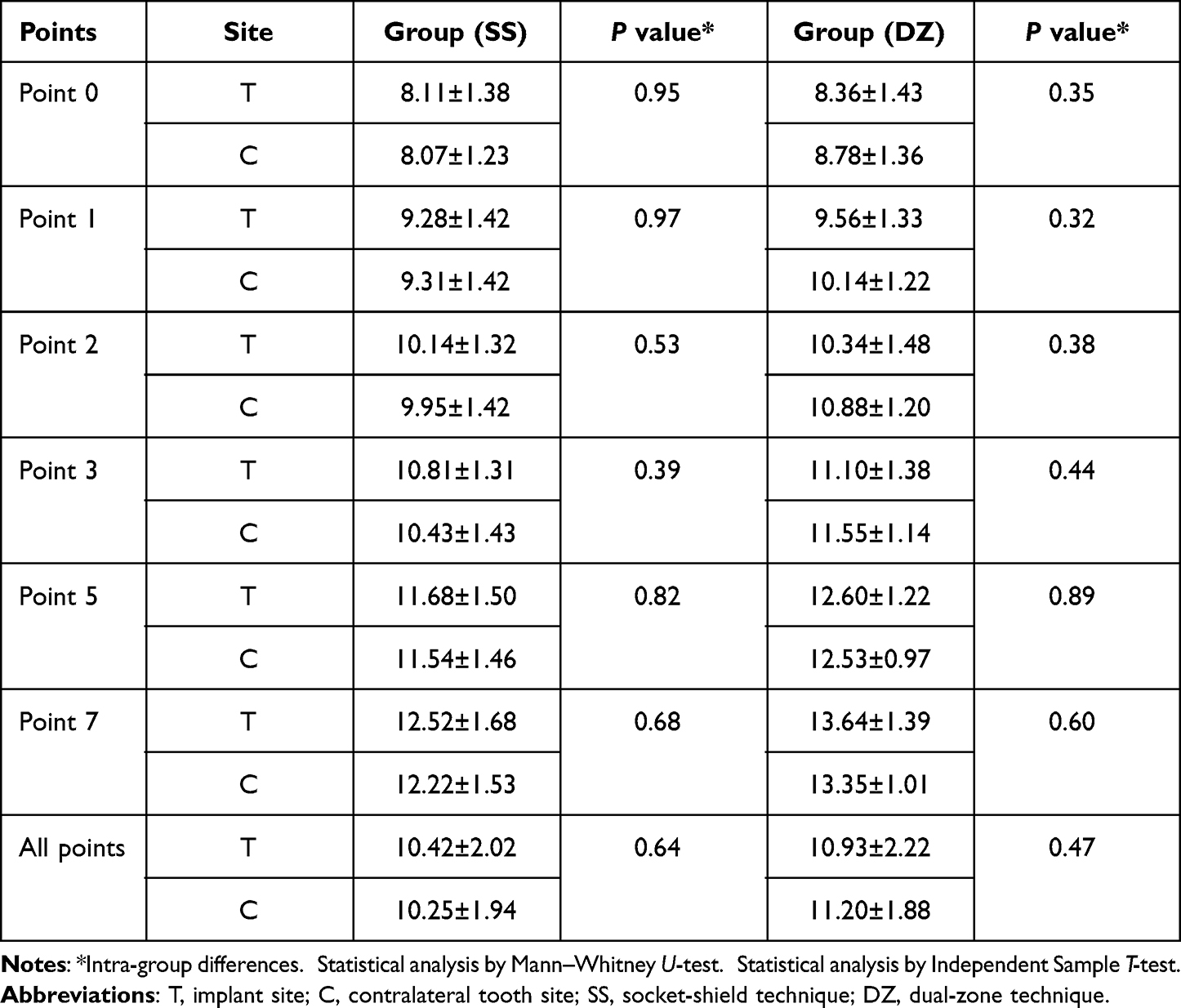 |
Table 2 Comparison of Facial-Palatal Ridge Width Between T and C at Different Points (Mean ± SD) |
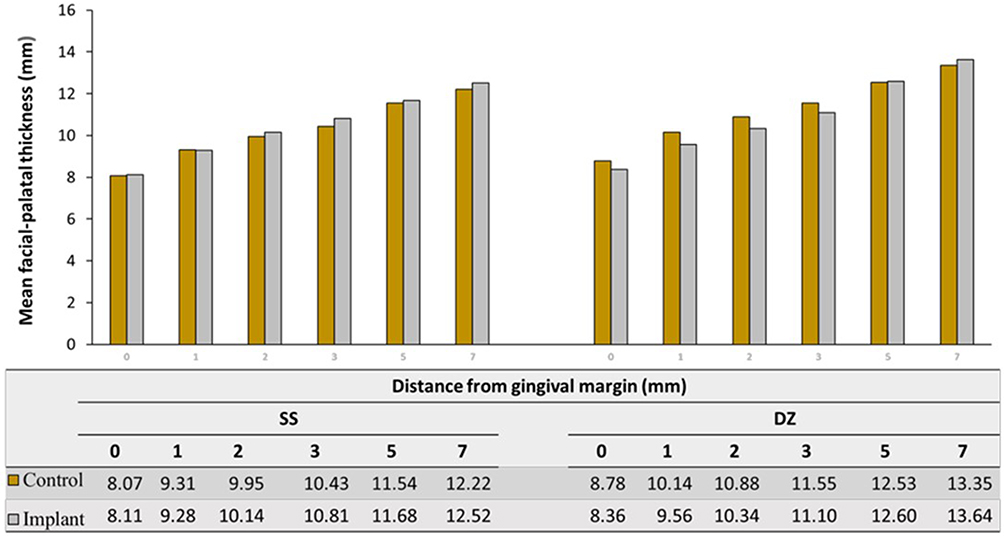 |
Figure 8 Mean thickness of the ridge facio-palatally on the implant sites (T) and tooth sites (C) at all distances from gingival margin for SS and DZ groups. |
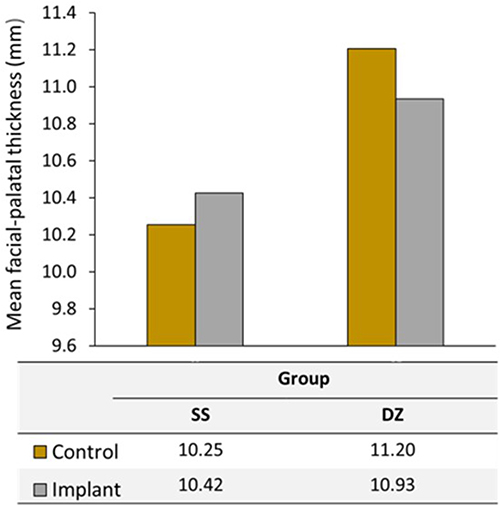 |
Figure 9 Mean thickness of the ridge facio-palatally on the implant sites (T) and the tooth sites (C) arranged by group type (SS, DZ). |
When comparing between the two groups, there were significant differences in ridge contour changes (T-C) between the two groups when averaged over all the distances from the gingival margin (P =0.013), indicating a better preservation of the ridge contour for SS treatment at 8–10 months. The null hypothesis that there were no significant differences in the facial-palatal ridge dimensional changes at 8–10 months postimplantation between the DZ immediate implant placement and the SS immediate placement could be rejected (P < 0.05).
Regarding the dimensional changes of the ridge contour in relation to the distance from the gingival margin, the pattern of change was not consistent across the groups and revealed a high variation between the patients. The most reduction in the ridge contour of about 0.6 mm was shown at point 1 mm in the DZ group (Figure 10).
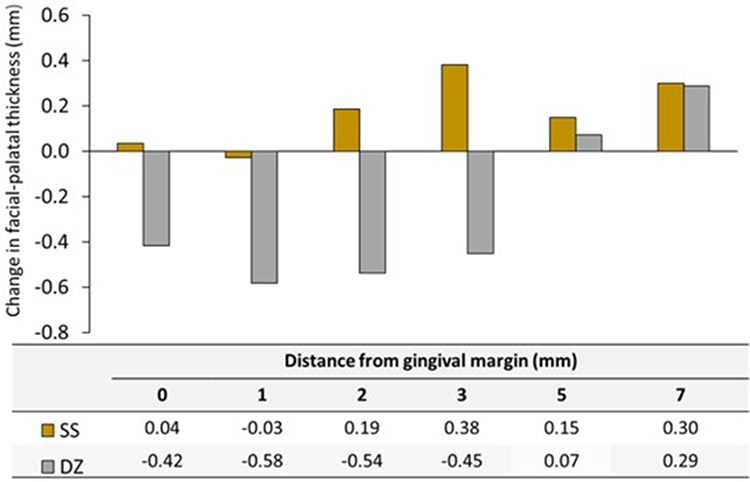 |
Figure 10 Mean facial-palatal ridge contour change (T–C) at all distances from gingival margin for SS and DZ groups. |
Mann–Whitney U-test showed a significant effect of the healing pattern (submerged vs nonsubmerged) on the facial-palatal ridge changes for DZ group only, where submerged cases showed better preservation (P =0.00). No effect was found for the gingival biotype, the facial plate thickness, or the tooth type (anterior vs premolar) on the facial-palatal ridge width changes for both groups (P >0.05).
The intra-investigator intraclass correlation coefficient (ICC) obtained was 0.998 (95% CI, 0.997 to 0.999) for SS group and 0.995 (95% CI, 0.994 to 0.997) for DZ group. This showed a high agreement between the different measurements.
Discussion
This prospective cohort clinical study aimed to assess the horizontal ridge changes that occurred at 8–10 months following flapless immediate implant placement with dual-zone technique and socket-shield technique in the maxilla; and to report the incidence of any biological or biomechanical complications in the 8–10 months follow-up. Therefore, single-tooth implants were inserted for patients requesting replacement of their hopeless teeth in the maxillary esthetic zone with considering the contralateral natural tooth as a control. The results of this study showed that the SS technique produced a better preservation of the facial-palatal ridge contour at 8–10 months postimplantation compared with the DZ technique.
Immediate implant placement survival rates are comparable to those of delayed implant placement while reducing the number of surgical procedures and the treatment time.46–48 However, immediate implant placement presents with some shortcomings, including peri-implant mucosal recession, unpredictable esthetic results,11,49 and alveolar ridge resorption and collapse.50 A clinical study revealed that at least 1.9 mm and 0.9 mm ridge’s horizontal collapse occurred facially and palatally, respectively after 4 months of immediate implant placement with flap elevation and without any bone or soft tissue augmentation.51
Therefore, several techniques have been proposed to reduce the collapse of the ridge postimplantation. Grunder13 in a clinical study compared the horizontal dimensional shrinkage that occurred at 6 months postimplantation between flapless immediate placement with just healing abutment and without bone grafting and immediate placement with only connective tissue grafting. The results revealed an average 1.1 mm collapse of the ridge facio-palatally in the nongrafted group, while a slight increase of 0.34 mm occurred in the connective tissue-grafted group.13 Another retrospective cross-sectional clinical cohort study showed that flapless dual-zone immediate implant placement either with a prefabricated healing abutment or with a provisional restoration yielded just an average of 0.4 mm of horizontal dimensional shrinkage at 12 months postimplantation.3 However, the same study3 showed that flapless immediate placement without bone grafting in the facial gap either with or without a provisional restoration resulted in approximately 1 mm of facial-palatal collapse at 12 months postimplantation.
Immediate implant placement with the socket shield technique aims to prevent or minimize the postextraction resorption of the alveolar bone.20 In spite of no comparable group for the conventional technique, a retrospective case series study evaluated the facial-palatal dimensional changes after 5 years of ten SS immediate implant placement in the maxilla and revealed an average loss of 0.37 mm facially, suggesting that this technique could effectively preserve the peri-implant tissue contours.15 Another prospective cohort study showed that the average collapse that occurred facially at 3 months following SS immediate implant placement with an immediate provisional restoration was 0.07 mm.24 A recent randomized controlled clinical trial compared the conventional flapless immediate implant placement and the socket shield technique for facial plate width changes at 6 months postimplantation; it reported that the SS group had significantly higher values of facial plate width, indicating better preservation of the ridge contour.43
Although a direct comparison with those studies is not feasible due to different measurement techniques and different follow-up periods, the results of the present study are in agreement with the findings of those studies. The current study revealed that the SS technique produced a statistically significant superior maintenance of the ridge width at 8–10 months follow-up compared with the DZ technique (P =0.013). When averaged over all reference points at 8–10 months follow-up, the SS group demonstrated a mean gain of the facial-palatal ridge contour of 0.17 mm, while DZ showed a mean reduction of 0.27 mm. The slight width increase with the SS group that was also encountered with some samples in previous studies,15,24 might be due to an unavoidable measurement error rather than an actual gain. The 0.27 mm mean facial-palatal reduction reported for the DZ group is in accordance with that of a clinical retrospective study by Tarnow et al3 who demonstrated that flapless dual-zone immediate implant placement yielded an average 0.4 mm of horizontal dimensional shrinkage at 12 months postimplantation. This result was justified by the supporting function of the bone graft particles that were placed in the facial jumping gap and also in the tissue zone coronal to the implant-abutment junction.12
Regarding the potential confounders, none of them had a significant influence except the healing pattern (submerged vs nonsubmerged) for DZ group only, where submerged cases showed a positive effect on the ridge width preservation. This result could not be explained for this small sample size and calls for additional investigations. However, the potential confounding effect of the healing pattern was attempted to be minimized by avoiding the primary soft tissue closure over the implants selected for submerged healing; instead, collagen sponge was placed on top of the bone granules and stabilized with horizontal mattress and interrupted sutures. Subsequently, those implants were uncovered with a punch technique without any soft tissue enhancement. In addition, an immediate provisional resin-bonded bridge was stabilized to the adjacent teeth to act as a customized healing abutment in sealing the socket and containing the bone graft during the healing process.
With respect to the implant survival rate, both techniques yielded 100% survival rate. Thus, this study revealed that socket shield in association with an immediate implant placement did not disturb the implant osseointegration clinically. This finding is in agreement with that of previous studies that investigated the socket shield technique.15,20,24,26,42,43 Concerning the nature of the intervening tissue between the socket shield and the implant, only two human histological case reports were found in the literature.29,36 One report revealed mature bone intervening between the shield and the implant in the middle and the apical thirds, whereas soft tissue dominated in the coronal third.29 Another human histologic report of unplanned socket shield demonstrated that mature bone resided between the implant threads and the root dentin at two years postimplantation.36
Though both techniques yielded 100% implant survival rate, the SS resulted in two external shield exposures that were managed by just reducing the exposed part with a high-speed diamond bur, and both healed well with soft tissue coverage. However, more dimensional ridge shrinkage occurred for those two cases but without any soft tissue recession or esthetic compromise; and the two patients were satisfied with the esthetic result and declined any connective tissue grafting. Gluckman et al23 in a retrospective study of 128 socket shield cases reported 16 occurrences of exposure, four were external and 12 were internal. The authors advocated to reduce the facial shield to the level of the bone crest and to create a bevel in the coronal 2 mm of the shield to reduce the incidence of those complications.
Although 100% implants survival rates with minor manageable complications and maintenance of the ridge contour were demonstrated, the current study presents with some limitations. It was performed on a fairly small sample size in a particular center and followed for a short period of time. In addition, the applied dimensional ridge width analysis concentrated only on the mid-root portion rather than the entire ridge contour; and some procedures like impression making and cast production could not be performed without some inaccuracies. Furthermore, the contralateral tooth might represent a source of bias for this evaluation. A more accurate technique is to scan the ridge pre- and postimplantation and calculate the horizontal width changes with a reverse engineering software of the two superimposed images; or to compare the pre- and the postimplantation CBCT images.
Conclusion
Within the limitations of this study, it can be concluded that the socket shield immediate implant placement is a safe minimally invasive technique that could prevent or minimize the facial-palatal ridge collapse that occurs postimplantation up to 8–10 month follow-up. Although the socket shield technique produced a better preservation of the ridge contour at 8–10 months, dual-zone technique yielded a non clinically significant reduction in the ridge contour at the same time period. Two out of ten cases of the socket shield group presented with minor manageable complications of external shield exposure; therefore, more clinical studies comprising larger population with more variables and longer follow-ups in multiple centers are advocated to gather more scientific based evidence on the long-term performance, success rate, complications, and stability of the esthetic outcome. In addition, animal histological investigations are recommended to know more about the nature of the intervening tissue between the implant and the shield.
Abbreviations
PCS, prospective cohort study; SS, socket-shield; DZ, dual-zone; FDBA, freeze dried bone allograft; CBCT, cone beam computed tomography; T, implant site (test); C, contralateral tooth site (control); T-C, change in facial-palatal ridge width; IT, Insertion torque; ISQ, Implant stability quotient; GBR, Guided bone regeneration; SD, Standard deviation; ICC, intraclass correlation coefficient.
Acknowledgments
I would like to acknowledge Doctor Fadda Al-Mahdi (previous teaching and research assistant, Faculty of Dentistry, Arab American University, Jenin, Palestinian Territory), who did the cast measurements, Maryam Fasfous (Lecturer, Department of Data and Statistics, Palestine Polytechnic University, Hebron, Palestinian Territory) who did the statistical analysis, and Megagen Palestine (Hebron, Palestinian Territory) for providing the implants.
Funding
The study was funded by Arab American University, Jenin, Palestinian Territory.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Araújo MG, Sukekava F, Wennström JL, Lindhe J. Tissue modeling following implant placement in fresh extraction sockets. Clin Oral Implants Res. 2006;17(6):615–624. doi:10.1111/j.1600-0501.2006.01317.x
2. Passoni BB, Marques de Castro DS, de Araújo MA, de Araújo CD, Piatelli A, Benfatti CA. Influence of immediate/delayed implant placement and implant platform on the peri-implant bone formation. Clin Oral Implants Res. 2016;27(11):1376–1383. doi:10.1111/clr.12750
3. Tarnow DP, Chu SJ, Salama MA, et al. Flapless postextraction socket implant placement in the esthetic zone, part 1. The effect of bone grafting and/or provisional restoration on facial-palatal ridge dimensional change-a retrospective cohort study. Int J Periodontics Restorative Dent. 2014;34(3):323–331. doi:10.11607/prd.1821
4. Braut V, Bornstein MM, Belser U, Buser D. Thickness of the anterior maxillary facial bone wall-a retrospective radiographic study using cone beam computed tomography. Int J Periodontics Restorative Dent. 2011;31(2):125–131.
5. Alshiddi IF, Dent DC. Accurate registration of peri‐implant soft tissues to create an optimal emergence profile. Contemp Clin Dent. 2015;6:S122–S125. doi:10.4103/0976-237X.152967
6. Cosyn J, Pollaris L, Van der Linden F, De Bruyn H. Minimally Invasive Single Implant Treatment (M.I.S.I.T.) based on ridge preservation and contour augmentation in patients with a high aesthetic risk profile, one-year results. J Clin Periodontol. 2015;42(4):398–405. doi:10.1111/jcpe.12384
7. Lee AMH, Poon CY. The clinical effectiveness of alveolar ridge preservation in the maxillary anterior esthetic zone-a retrospective study. J Esthet Restor Dent. 2017;29:137–145. doi:10.1111/jerd.12280
8. Cooper LF, Reside G, Raes F, et al. Immediate provisionalization of dental implants in grafted alveolar ridges in the esthetic zone, a 5-year evaluation. Int J Periodontics Restorative Dent. 2014;34(4):477–486. doi:10.11607/prd.2022
9. Mangano FG, Zecca P, Luongo F, Iezzi G, Mangano C. Single-tooth Morse taper connection implant placed in grafted site of the anterior maxilla, clinical and radiographic evaluation. Case Rep Dent. 2014;2014:183872. doi:10.1155/2014/183872
10. Buser D, Chappuis V, Belser UC, Chen S. Implant placement post extraction in esthetic single tooth sites, when immediate, when early, when late? Periodontol 2000. 2017;73(1):84–102. doi:10.1111/prd.12170
11. Evans CD, Chen ST. Esthetic outcomes of immediate implant placements. Clin Oral Implants Res. 2008;19(1):73–80. doi:10.1111/j.1600-0501.2007.01413.x
12. Chu SJ, Salama MA, Salama H, et al. The dual-zone therapeutic concept of managing immediate implant placement and provisional restoration in anterior extraction sockets. Compend Contin Educ Dent. 2012;33(7):524–532.
13. Grunder U. Crestal ridge width changes when placing implants at the time of tooth extraction with and without soft tissue augmentation after a healing period of 6 months, report of 24 consecutive cases. Int J Periodontics Restorative Dent. 2011;31(1):9–17.
14. Jemt T. Restoring the gingival contour by means of provisional resin crowns after single-implant treatment. Int J Periodontics Restorative Dent. 1999;19(1):20–29.
15. Bäumer D, Zuhr O, Rebele S, Hürzeler M. Socket shield technique for immediate implant placement - clinical, radiographic and volumetric data after 5 years. Clin Oral Implants Res. 2017;28(11):1450–1458. doi:10.1111/clr.13012
16. Ferrus J, Cecchinato D, Pjetursson EB, Lang NP, Sanz M, Lindhe J. Factors influencing ridge alterations following immediate implant placement into extraction sockets. Clin Oral Implants Res. 2010;21(1):22–29. doi:10.1111/j.1600-0501.2009.01825.x
17. Lee CT, Chiu TS, Chuang SK, Tarnow D, Stoupel J. Alterations of the bone dimension following immediate implant placement into extraction socket, systematic review and meta-analysis. J Clin Periodontol. 2014;41(9):914–926. doi:10.1111/jcpe.12276
18. Casey DM, Lauciello FR. A review of the submerged-root concept. J Prosthet Dent. 1980;43(2):128–132. doi:10.1016/0022-3913(80)90174-2
19. Salama M, Ishikawa T, Salama H, Funato A, Garber D. Advantages of the root submergence technique for Pontic site development in esthetic implant therapy. Int J Periodontics Restorative Dent. 2007;27(6):521–527.
20. Hürzeler MB, Zuhr O, Schupbach P, Rebele SF, Emmanouilidis N, Fickl S. The socket-shield technique, a proof-of-principle report. J Clin Periodontol. 2010;37(9):855–862. doi:10.1111/j.1600-051X.2010.01595.x
21. Gharpure AS, Bhatavadekar NB. Current evidence on the socket‐shield technique, a systematic review. J Oral Implantol. 2017;43:395–403. doi:10.1563/aaid-joi-D-17-00118
22. Mourya A, Mishra SK, Gaddale R, Chowdhary R. Socket-shield technique for implant placement to stabilize the facial gingival and osseous architecture, A systematic review. J Investig Clin Dent. 2019;10(4):e12449. doi:10.1111/jicd.12449
23. Gluckman H, Salama M, Du Toit J. A retrospective evaluation of 128 socket‐shield cases in the esthetic zone and posterior sites, partial extraction therapy with up to 4 years follow‐up. Clin Implant Dent Relat Res. 2018;20:122–129. doi:10.1111/cid.12554
24. Hinze M, Janousch R, Goldhahn S, Schlee M. Volumetric alterations around single‐tooth implants using the socket‐shield technique, preliminary results of a prospective case series. Int J Esthet Dent. 2018;13:146–170.
25. Han CH, Park KB, Mangano FG. The modified socket shield technique. J Craniofac Surg. 2018;29:2247–2254. doi:10.1097/SCS.0000000000004494
26. Siormpas KD, Mitsias ME, Kotsakis GA, Tawil I, Pikos MA, Mangano FG. The root membrane technique, a retrospective clinical study with up to 10 years of follow‐up. Implant Dent. 2018;27:564–574. doi:10.1097/ID.0000000000000818
27. Petsch M, Spies B, Kohal RJ. Socket shield technique for implant placement in the esthetic zone, a case report. Int J Periodontics Restorative Dent. 2017;37:853–860. doi:10.11607/prd.2729
28. Saeidi Pour R, Zuhr O, Hürzeler M, et al. Clinical benefits of the immediate implant socket shield technique. J Esthet Restor Dent. 2017;29(2):93–101. doi:10.1111/jerd.12291
29. Mitsias ME, Siormpas KD, Kotsakis GA, Ganz SD, Mangano M, Iezzi G. The root membrane technique, human histologic evidence after 5 years of function. Biomed Res Int. 2017;2017:1–8. doi:10.1155/2017/7269467
30. Kumar PR, Kher U. Shield the socket, procedure, case report and classification. J Indian Soc Periodontol. 2018;22:266–272. doi:10.4103/jisp.jisp_78_18
31. Esteve‐Pardo G, Esteve‐Colomina L. Clinical application of the socket‐shield concept in multiple anterior teeth. Case Rep Dent. 2018;2018:1–7.
32. Verma N, Lata J, Kaur J. Socket shield technique‐a new approach to immediate implant placement. Indian J Compr Dent Care. 2018;8:1181–1183.
33. Aslan S. Improved volume and contour stability with thin socket‐ shield preparation in immediate implant placement and provisional‐ ization in the esthetic zone. Int J Esthet Dent. 2018;13:172–183.
34. Dayakar MM, Waheed A, Bhat HS, Gurpur PP. The socket‐ shield technique and immediate implant placement. J Indian Soc Periodontol. 2018;22:451–455. doi:10.4103/jisp.jisp_240_18
35. Guo T, Nie R, Xin X, et al. Tissue preservation through socket-shield technique and platelet-rich fibrin in immediate implant placement, A case report. Medicine. 2018;97(50):e13175. doi:10.1097/MD.0000000000013175
36. Schwimer C, Pette GA, Gluckman H, Salama M, Du Toit J. Human histologic evidence of new bone formation and osseointegration between root dentin (unplanned socket‐shield) and dental implant, case report. Int J Oral Maxillofac Implants. 2018;33:e19–e23. doi:10.11607/jomi.6215
37. Arabbi KC, Sharanappa M, Priya Y, Shah TD, Subbaiah SK. Socket shield, a case report. J Pharm Bioall Sci. 2019;11:S72–S75. doi:10.4103/JPBS.JPBS_228_18
38. Schwimer CW, Gluckman H, Salama M, Nagy K, Du Toit J. The socket‐shield technique at molar sites, a proof‐of‐principle technique report. J Prosthet Dent. 2019;121:229–233. doi:10.1016/j.prosdent.2018.05.006
39. Gluckman H, Du Toit J, Salama M, Nagy K, Dard M. A decade of the socket-shield technique, a step-by-step partial extraction therapy protocol. Int J Esthet Dent. 2020;15(2):212–225.
40. Tan Z, Kang J, Liu W, Wang H. The effect of the heights and thicknesses of the remaining root segments on buccal bone resorption in the socket‐shield technique, an experimental study in dogs. Clin Implant Dent Relat Res. 2018;20:352–359. doi:10.1111/cid.12588
41. Calvo‐Guirado JL, Benítez‐García JA, Maté Sánchez de Val JE, et al. Socket‐shield technique, the influence of the length of the remaining buccal segment of healthy tooth structure on peri‐implant bone and socket preservation. A study in dogs. Ann Anat. 2019;221:84–92. doi:10.1016/j.aanat.2018.09.003
42. Bramanti E, Norcia A, Cicciù M, et al. Postextraction dental implant in the aesthetic zone, socket shield technique versus conventional protocol. J Craniofac Surg. 2018;29:1037–1104. doi:10.1097/SCS.0000000000004419
43. Sun C, Zhao J, Liu Z, et al. Comparing conventional flap-less immediate implantation and socket-shield technique for esthetic and clinical outcomes, A randomized clinical study. Clin Oral Implants Res. 2020;31(2):181–191. doi:10.1111/clr.13554
44. Crespi R, Capparé P, Gherlone E, Romanos GE. Immediate versus delayed loading of dental implants placed in fresh extraction sockets in the maxillary esthetic zone, a clinical comparative study. Int J Oral Maxillofac Implants. 2008;23(4):753–758.
45. Sample size calculators, observational study, cohort study, independent, continuous outcome, two-sided. Available from: http://riskcalc.org:3838/samplesize/.
46. Wohrle PS. Single-tooth replacement in the aesthetic zone with immediate provisionalization, Fourteen consecutive case reports. Pract Proced Aesthet Dent. 1998;10:1107–1114.
47. Kan JY, Rungcharassaeng K, Lozada J. Immediate placement and provisionalization of maxillary anterior single implants, 1-year prospective study. Int J Oral Maxillofac Implants. 2003;18:31–39.
48. Block MS, Mercante DE, Lirette D, Mohamed W, Ryser M, Castellon P. Prospective evaluation of immediate and delayed provisional single tooth restorations. J Oral Maxillofac Surg. 2009;67:89–107. doi:10.1016/j.joms.2009.07.009
49. Chen ST, Buser D. Esthetic outcomes following immediate and early implant placement in the anterior maxilla--a systematic review. Int J Oral Maxillofac Implants. 2014;29:186–215. doi:10.11607/jomi.2014suppl.g3.3
50. Chappuis V, Araújo MG, Buser D. Clinical relevance of dimensional bone and soft tissue alterations post-extraction in esthetic sites. Periodontol 2000. 2017;73(1):73–83. doi:10.1111/prd.12167
51. Botticelli D, Berglundh T, Lindhe J, et al. Hard tissue alterations following immediate implant placement in extraction sites. J Clin Periodontol. 2004;31:820–828. doi:10.1111/j.1600-051X.2004.00565.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.