")
Back to Journals » Nature and Science of Sleep » Volume 15
Comparative Efficacy and Safety of Multiple Wake-Promoting Agents for the Treatment of Excessive Daytime Sleepiness in Narcolepsy: A Network Meta-Analysis
Authors Zhan S, Ye H, Li N, Zhang Y, Cheng Y, Wang Y, Hu S , Hou Y
Received 26 January 2023
Accepted for publication 4 April 2023
Published 14 April 2023 Volume 2023:15 Pages 217—230
DOI https://doi.org/10.2147/NSS.S404113
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sarah L Appleton
Shuqin Zhan,1 Hui Ye,2 Ning Li,1 Yimeng Zhang,1 Yueyang Cheng,1 Yuanqing Wang,1,3 Shimin Hu,1 Yue Hou1
1Department of Neurology, Xuanwu Hospital, Capital Medical University, Beijing, 100053, People’s Republic of China; 2Ignis Therapeutics (Shanghai) Limited, Shanghai, 200000, People’s Republic of China; 3Department of Neurology, People’s Hospital of Rizhao, Rizhao, 276800, People’s Republic of China
Correspondence: Shuqin Zhan, Department of Neurology, Xuanwu Hospital, Capital Medical University, Beijing, 100053, People’s Republic of China, Tel +8613801027285, Email [email protected]
Purpose: Narcolepsy is a rare debilitating disorder for which multiple novel pharmacological options have been approved as treatment for the past few years. The current study systematically updates the comparative efficacy and detailed safety analysis of approved wake-promoting agents in narcolepsy.
Methods: Randomized controlled trials (RCTs) were searched for diagnosed narcolepsy with approved interventions. Efficacy outcomes included the Maintenance of Wakefulness Test (MWT), Epworth Sleepiness Scale (ESS), Clinical Global Impression of Change (CGI-C), and Patient Global Impression of Change (PGI-C). Safety outcomes including overall adverse event (AE) risk were measured. The study was registered at PROSPERO (CRD 42022334915).
Results: The final analysis included 17 RCTs with five drug treatments: modafinil/armodafinil, sodium oxybate, pitolisant, solriamfetol, and lower-sodium oxybate (LXB). For efficacy measures, interventions included in each outcome were effective compared with placebo. Furthermore, the magnitude of solriamfetol effect on MWT (9.11 minutes; 95% CI=7.05– 11.16), ESS (− 4.79; 95% CI=− 6.56 to − 3.01), and PGI-C (9.39; 95% CI= 2.37– 37.19), and LXB effect on CGI-C (9.67; 95% CI=2.73– 34.26) was greater than that of other treatments included in each outcome compared with placebo. For safety measures, all interventions had an acceptable safety profile with LXB having least risk for overall AEs (0.56; 95% CI=0.20– 1.53), serious AEs (0.33; 95% CI=0.09– 1.20), AEs leading to treatment discontinuation (0.11; 95% CI=0.01– 2.04), and all-cause discontinuation (0.04; 95% CI=0.00– 0.67) compared to placebo. Placebo had the lowest risk for exploratory AEs.
Conclusion: All approved interventions were effective in controlling the symptoms of narcolepsy at varying degrees with an acceptable safety profile.
Keywords: narcolepsy, network meta-analysis, wake-promoting agents, excessive daytime sleepiness, patient-centric scores, safety
Introduction
Narcolepsy is a rare, disabling chronic neurological disorder that is characterized by excessive daytime sleepiness (EDS), cataplexy, hypnagogic hallucinations, and sleep paralysis. Narcolepsy is estimated to affect 20 to 50 people per 100,000 worldwide, with incidences tending to increase with age.1–4 The primary symptom of narcolepsy is EDS shared by patients with either type 1 narcolepsy (with cataplexy, NT1) or type 2 narcolepsy5,6 (without cataplexy, NT2). Furthermore, a large-scale survey in the United States observed that >75% of patients with narcolepsy considered EDS to be significantly affecting their day-to-day life.6
Given the high prevalence and burden of the disease, treatment of EDS is a necessity and is highly recommended in treatment guidelines of narcolepsy.7,8 Multiple subjective and objective methods listed in the recently released compendium of clinical outcome assessment (COA) by the Food and Drug Administration (FDA) could be considered to evaluate EDS associated with narcolepsy, including patient-reported outcome for daytime sleepiness, Maintenance of Wakefulness Test (MWT) for wakefulness, and Patient Global Impression of Change (PGI-C) for global impression of change of symptom severity.9 The most widely used and validated self-addressed questionnaire is the Epworth Sleepiness Scale (ESS) for assessing subjective sleepiness over time.10 A threshold of ESS >10 indicates the EDS symptom as burdensome and interfering in daily life.11 Another helpful tool is the daytime polysomnographic, the MWT sleep latency, that assesses the capability to stay awake during the day and provides the complementary, objective measures of the degree of sleepiness.12,13 Compared with another widely used tool – the Multiple Sleep Latency Test, MWT may be indicated in patients to assess the response to the treatment.14 In addition to the Clinical Global Impression of Change (CGI-C), the patient-oriented assessment (ie, the PGI-C) is critical to COA. Both PGI-C and CGI-C are easy-to-use validated questionnaires, which show a bipolar scaling from 1 (very much improved) to 7 (very much worse).15
So far, there are no disease-modifying drugs for narcolepsy, with the current symptomatic treatment modalities aimed to improve EDS and reduce cataplexy as the primary therapeutic targets. Several wake-promoting agents have been approved by the FDA or the European Medicine Agency (EMA) for the treatment of narcolepsy: methylphenidate and amphetamines for narcolepsy in general, modafinil and armodafinil for EDS only, and sodium oxybate (SXB), pitolisant, and lower-sodium oxybate (LXB) for both EDS and cataplexy.16–18 Solriamfetol, a phenylalanine derivative with dopaminergic and noradrenergic activity, is a newly approved drug by the FDA and the EMA to treat EDS associated with NT1 and NT2. Recently updated guidelines of the United States and Europe both strongly recommend modafinil/SXB/pitolisant/solriamfetol as the main treatment for EDS symptoms in narcolepsy.7,8
Symptomatic treatment of narcolepsy is the mainstay strategy and the treatment choice is based on factors such as age, severity, tolerance, comorbidities, drug efficacy, safety, and abuse potential.19–22 Several clinical studies have established the efficacy and safety of the EMA-approved/FDA-approved medications in narcolepsy. However, there are few direct comparative clinical trials on the efficacy and safety between different wake-promoting agents in narcolepsy.23,24 Armodafinil, the r-enantiomer of modafinil (racemic), is known to have longer action than modafinil for excessive sleepiness.23 Dauvilliers et al25 observed the comparable efficacy between pitolisant and modafinil for the ESS outcome. A retrospective study observed that SXB improved the subjective ratings of excessive sleepiness versus modafinil compared with placebo.24 However, indirect treatment comparison performed by Lehert and colleagues showed that pitolisant, modafinil, and SXB were equally effective treatments for reducing the EDS.26,27 A good safety profile was reported with all the agents compared, except for SXB 9 g/d.26
Multiple treatment comparison meta-analysis has become a powerful tool for decision-making in medicine. As the last multiple treatment meta-analysis in narcolepsy published in 2018,26 solriamfetol and LXB have been newly-approved for treating EDS in narcolepsy. In addition, the EDS efficacy outcomes of previous meta-analysis are limited for ESS and MWT, whereas more extensive comparison of other outcomes such as disease severity changes as measured by CGI-C and PGI-C is lacking. Moreover, a thorough safety analysis of the narcolepsy drugs is required to ensure the effective risk control. In order to have up-to-date and more extensive understanding of the narcolepsy treatment, the aim of this network meta-analysis (NMA) is to compare the efficacy and safety of approved wake-promoting agents for the treatment of EDS in narcolepsy.
Methods
This NMA protocol was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses protocols (PRISMA-P),28 and was performed accordance to the PRISMA Extension version (PRISMA-NMA).29 This statistical analysis plan was registered in the Prospective Register of Systematic Reviews (PROSPERO) database (CRD 42022334915).
Eligibility Criteria
Studies included patients who were adults, aged ≥18 years, diagnosed with narcolepsy, irrespective of gender, and those were treated with the FDA-approved/EMA-approved agents such as modafinil, armodafinil, SXB, pitolisant, solriamfetol, LXB, methylphenidate, and amphetamine. Comparison between the identified treatments and placebo as well as any pair of treatments was sought. The outcomes included ESS, MWT, CGI-C, PGI-C, and safety measures.
Search Strategy
A comprehensive literature search on the English databases was performed since its inception through May 2022. Databases included PubMed, Embase, the Cochrane Central Register of Controlled Trials (CENTRAL, Cochrane Library), World Health Organization International Trials Registry Platform search portal, the United States FDA website, and the EMA website. In addition, ClinicalTrials.gov and the reference lists of previously published reviews related to the narcolepsy treatments were also screened for the eligible clinical trials. The search terms included narcolepsy, modafinil, pitolisant, sodium oxybate, solriamfetol, armodafinil, lower sodium oxybate, methylphenidate, amphetamine, randomized controlled trial (RCT), and clinical trial.
Study Selection
Double-blind RCTs providing the data on at least one of the following selected outcomes in both efficacy and safety were selected: ESS, MWT, CGI-C, PGI-C, and safety reporting at least existing adverse events (AEs) during the treatment exposure. We excluded case reports, post hoc reviews, systematic reviews, meta-analyses, non-comparative studies, and cost-related studies. Studies published in languages other than English were also excluded.
Data Collection Process
We collected the study design, publication year, sample size, patient disposition, and endpoints for each study in a standard data extraction form using Microsoft Excel 2013 (Microsoft Corp., Redmond, WA). Included trials were evaluated for the handling of incomplete outcome data, selective reporting, and other potential sources of bias. The literature collected was independently reviewed by two reviewers for titles and abstracts of retrieved records followed by the full texts of all potentially relevant trials, with discrepancies resolved by discussion. Detailed data extraction and risk of bias assessment were performed by two independent reviewers, with discrepancies resolved by discussion.
Risk of Bias in Individual Studies
The quality of each RCT included was evaluated by two independent reviewers using a Cochrane Risk of Bias 2 (RoB 2.0) tool. The tool includes (1) randomization process, (2) deviations from intended interventions, (3) missing outcome data, (4) measurement of the outcome, and (5) selection of the reported result.30 Bias is assessed either as “Low” or “High” risk of bias, or can express “Some concerns.”
Geometry of the Network
A network plot depicting the geometry of the treatment network of comparisons across the trials for each outcome was performed to ensure if an NMA is feasible. Network geometry depicts nodes to represent different wake-promoting agents and edges to represent the head-to-head comparisons between the network nodes.31,32
Outcomes
Primary efficacy outcome was EDS measured by MWT and ESS endpoints. The MWT studies related to the 20- and 40-minute protocols were pooled and analyzed as the MWT overall endpoint. The studies were also analyzed independently as subgroups (MWT-20 and MWT-40). Other efficacy outcomes were changes in disease severity on treatment, as measured by the CGI-C or PGI-C scores. Safety outcomes measured as risk ratio (RR) included overall AE risk, serious AEs (SAEs), AE leading to discontinuation, and all-cause discontinuation rate. Exploratory AEs of interest were analyzed by three categories such as (i) central nervous system (CNS): headache, agitation, insomnia, dizziness, irritability, insomnia, and fatigue, (ii) gastrointestinal system: nausea and dry mouth, and (iii) weight changes: weight gain (increased) and weight loss (decreased), as included in the study.
Evidence Synthesis
Crossover and parallel results were appropriately mixed and corrected under considerations of carryover effect.33 Values of all doses for each treatment were pooled and analyzed in each outcome. Value optimization across the trials was performed according to Lehert et al.26 Values not reported in the tables were estimated from the graphs in the finalized articles. Continuous variables included outcome measures that arose from ordinal scales (eg, efficacy measures); for which, change scores from baseline were combined to determine either mean difference (MD) or odds ratio (OR) with 95% confidence interval (CI). The mean, standard deviation, patient proportion, patient number, and p-value were extracted for each outcome at each timepoint where change in scores were not available. Data for all categories in CGI-C and PGI-C such as “mildly improved”, “moderately improved”, and “markedly improved” were pooled together and analyzed. For dichotomous scores (eg, AEs), treatment effect was evaluated using the RR with 95% CI. Although comparative analysis was performed between the treatment and the placebo, indirect pairwise comparisons between the treatments could be statistically assessed.
NMA was performed using R software (version R 4.1.2) using the netmeta package with a frequentist approach.34,35 Heterogeneity across the studies was tested by χ2 test and I2 statistic along with a Forest plot. Statistically significant heterogeneity was defined as a χ2 p-value <0.1 or an I2 statistic >50%.36 Random effect models were performed when I2 ≥50%; otherwise, a fixed effect model was applied to quantitate the effect size. For all pairwise comparisons, MD, OD, or RR with a 95% CI was used as the meta-analytic measure of association between the treatments and the outcomes. Using the netrank function, the P-score was obtained for each treatment to rank the treatment effects. A p-score of “one” is ranked as best, whereas “zero” is ranked as least.35 A two-sided p-value of <0.05 was considered significant.
Risk of Bias Across Studies
The publication bias was assessed using Egger regression test and funnel plot.37 MD, OR, and RRs from included studies were plotted as a function of their standard error in relation to the comparison-specific effect.
Results
Study Selection
A total of 2,140 publications were identified after removing duplications through literature search. In addition, after the title and abstract screening process, publications that did not adhere to the study’s hypothesis were removed. A total of 52 potentially relevant articles were identified on full text screening. Furthermore, based on the study outcomes, 20 RCTs were selected; of which, 17 RCTs were included in the final evidence synthesis. Studies by Malhotra et al38 (patients with obstructive sleep apnea and narcolepsy), Weaver and Cuellar39 (additional functional outcomes/quality-of-life measures from the same trial published by Thorpy et al),40 and Kushida et al41 (investigational drug FT218) were excluded from the study. The entire study process is shown in Figure 1. The characteristics of the 17 studies and the inclusive treatments in the analyses are presented in Table 1. All studies had placebo as the comparator arm. As reported earlier, the studies on armodafinil and modafinil were pooled for further analysis.26 In addition, comparison between the two enantiomers was performed to confirm the relevance between the two groups. No eligible studies of methylphenidate or amphetamine were identified. Detailed statistical analysis is provided in Supplementary File 1.
 |
Table 1 Comparison of Efficacy Measures Between Multiple Wake-Promoting Agents |
 |
Figure 1 PRISMA flow diagram of the study. |
Ten studies compared modafinil,25,42–51 one study compared three studies each of SXB,50,52,53 pitolisant,25,46,54 and solriamfetol,40,55,56 and one study compared LXB57 with placebo. Three studies compared multiple treatments with placebo,25,46,50 whereas others compared one treatment with placebo, respectively (Table S1). A network evidence graph of the treatment comparison based on the number of studies is provided in Figure 2. The mean age score of patients ranged from 33.0 to 50 years in these trials. Of the 17 trials, three trials were crossover design and four trials were parallel studies. The follow-up time of the studies varied from 4 to 12 weeks. The number of studies included in each endpoint for each treatment is provided in Table S2.
 |
Figure 2 Multiple treatment comparison network analysis. |
Risk of Bias in Individual Studies
Assessment of the risk of bias in RCTs has been presented in Figure S125,42–57 and Figure S2.25,42–57 The USMDF (1998) study showed a high risk of bias owing to the concerns over the randomization process and bias due to deviations from the intended intervention with some concerns over the missing data.49 Studies by Billiard et al,42 Broughton et al,43 Harsh et al,51 Moldofsky,45 US Xyrem,52 and Houghton 2005,53 showed some concerns in one of the categories. The remaining studies showed a low risk of bias. In terms of the overall risk of bias, 60% of the studies were at low risk, 30% were with some concerns, and 10% were at high risk.
Efficacy Assessment Results
The main efficacy endpoints measured in this study were MWT sleep latency (mean change in time [minutes] from baseline), change in ESS score, and percentage of patients reporting improvement on the CGI-C and PGI-C scores. The network of interventions included in each outcome is provided in Figure S3.
Six studies were included in the MWT-20 outcome. Both treatments identified, modafinil (3.35 min; 95% CI=2.31–4.38) and SXB (5.29 min; 95% CI=2.41–8.17), had a significant MD compared with placebo (Figure S4A, Table S3). Furthermore, eight studies including solriamfetol, modafinil, pitolisant, and placebo with MWT (40-minute) protocol were analyzed. Significant MD was achieved by solriamfetol (9.11 min; 95% CI=7.05–11.16), modafinil (3.57 min; 95% CI=2.03–5.12), and pitolisant (2.90 min; 95% CI=1.38–4.41) (Figure S4B, Table S4). Among the treatment comparisons, a significant effect was observed with solriamfetol versus modafinil (5.54 min; 95% CI=2.96–8.10) and solriamfetol versus pitolisant (6.21 min; 95% CI=3.65–8.76). For the overall MWT analysis (14 studies), a significant improvement was observed with solriamfetol (9.11 min; 95% CI=7.05–11.16), modafinil (3.57 min; 95% CI=2.95–4.19), SXB (5.43 min; 95% CI=3.09–7.77), and pitolisant (2.90 min; 95% CI=1.58–4.21) versus placebo. Among the treatment comparisons, a significant MD was observed with solriamfetol versus modafinil (5.54 min; 95% CI=3.39–7.68), solriamfetol versus pitolisant (6.21 min; 95% CI=3.77–8.65), and solriamfetol versus SXB (3.68 min; 95% CI=0.57–6.80) (Figure 3A, Table 1A).
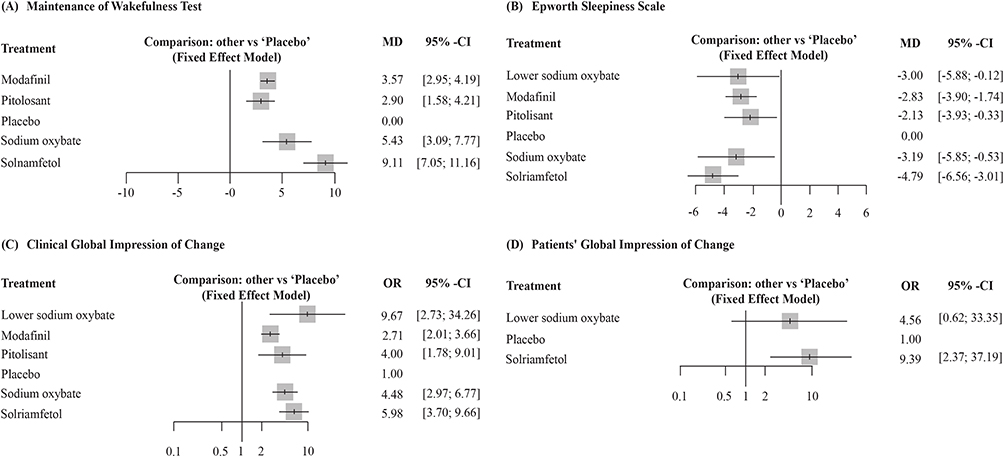 |
Figure 3 Forest plots for efficacy outcomes. (A) Maintenance of Wakefulness Test. (B) ESS, Epworth Sleepiness Scale. (C) Clinical Global Impression of Change. (D) Patients’ Global Impression of Change. Abbreviations: MD, mean difference; OR, odds ratio. |
For ESS (15 studies), solriamfetol (−4.79; 95% CI=−6.56 to −3.01), pitolisant (−2.13; 95% CI=−3.93 to −0.33), modafinil (−2.82; 95% CI=−3.90 to −1.74), SXB (−3.19 minutes; 95% C=−5.85 to −0.53), and LXB (−3.00; 95% CI=−5.88 to −0.12) reached a significant MD versus placebo. Among the pairwise treatment analysis, significant improvement was observed with solriamfetol versus pitolisant (−2.65; 95% CI=−5.18 to −0.13) and a favorable response was observed with solriamfetol versus LXB (−1.78; 95% CI=−5.16 to 1.59) (Figure 3B, Table 1A).
For CGI-C analysis (11 studies), a significant improvement was observed with LXB (9.67; 95% CI= 2.73–34.26), SXB (4.48; 95% CI=2.97–6.77), modafinil (2.71; 95% CI=2.01–3.66), pitolisant (4.00; 95% CI=1.78–9.01), and solriamfetol (5.98; 95% CI=3.70–9.66) versus placebo. Among the treatments, a significant improvement was observed with SXB versus modafinil (1.65; 95% CI=1.02–2.66) and solriamfetol versus modafinil (2.20; 95% CI=1.25–3.87) (Figure 3C, Table 1B). For PGI-C (3 studies and 2 interventions), a significant improvement was observed with solriamfetol versus placebo (9.39; 95% CI=2.37–37.19) (Figure 3D, Table 1B).
Among the outcomes, P-scores ranked SXB for MWT-20; solriamfetol for MWT-40, MWT overall, ESS, and PGI-C; and LXB for CGI-C as the best treatment (Table S5). Heterogeneity was significant across the studies for the MWT overall (p=0.0004), ESS (p=0.05), and PGI-C (p=0.05).
Safety Assessment Results
Network of interventions included in safety outcomes is represented in Figures S5 and S6. For overall AE (12 studies), a significant increased risk was observed with modafinil (1.63; 95% CI=1.15–2.32) versus placebo (Figure 4A, Table 2A). For SAEs (10 studies), a significant increase in risk was observed with modafinil (15.32; 95% CI=2.67–87.87) compared with placebo. Among the treatments, a significantly increased risk was observed with solriamfetol versus LXB (18.40; 95% CI=1.53–222), pitolisant versus LXB (11.03; 95% CI=1.19–102.58), modafinil versus SXB (19.78; 95% CI=2.09–187.58), and modafinil versus pitolisant (4.17; 95% CI=1.41–12.31) (Figure 4B, Table 2A). For AEs leading to treatment discontinuation (12 studies), a significantly increased risk was observed with modafinil (1.91; 95% CI=1.11–3.29) and SXB (4.92; 95% CI=2.00–12.07) compared with placebo. Among the treatments, a significantly increased risk was observed with SXB versus modafinil (2.58; 95% CI=1.01–6.61) and SXB versus LXB (44.24; 95% CI=2.11–928.73) (Figure 4C, Table 2B). For all-cause discontinuation (13 studies), a significant increase in risk was observed with SXB (3.87; 95% CI=1.57–9.51) versus placebo (Figure 4D). Among the treatments, a significant increased risk was observed with solriamfetol versus LXB (26.78; 95% CI=1.55–461.99), SXB versus LXB (96.69; 95% CI=5.04–1,853.92), SXB versus modafinil (3.34; 95% CI=1.34–8.32), SXB versus pitolisant (4.72; 95% CI=1.74–12.79), SXB versus solriamfetol (3.61; 95% CI=1.32–9.85), pitolisant versus LXB (20.48; 95% CI=1.16–353.82), and modafinil versus LXB (28.96; 95% CI=1.71–491.0) (Table 2B). LXB was the better treatment according to P-score analysis for safety endpoints (Table S6). Heterogeneity across the studies was significant for the overall AE risk (p<0.0001).
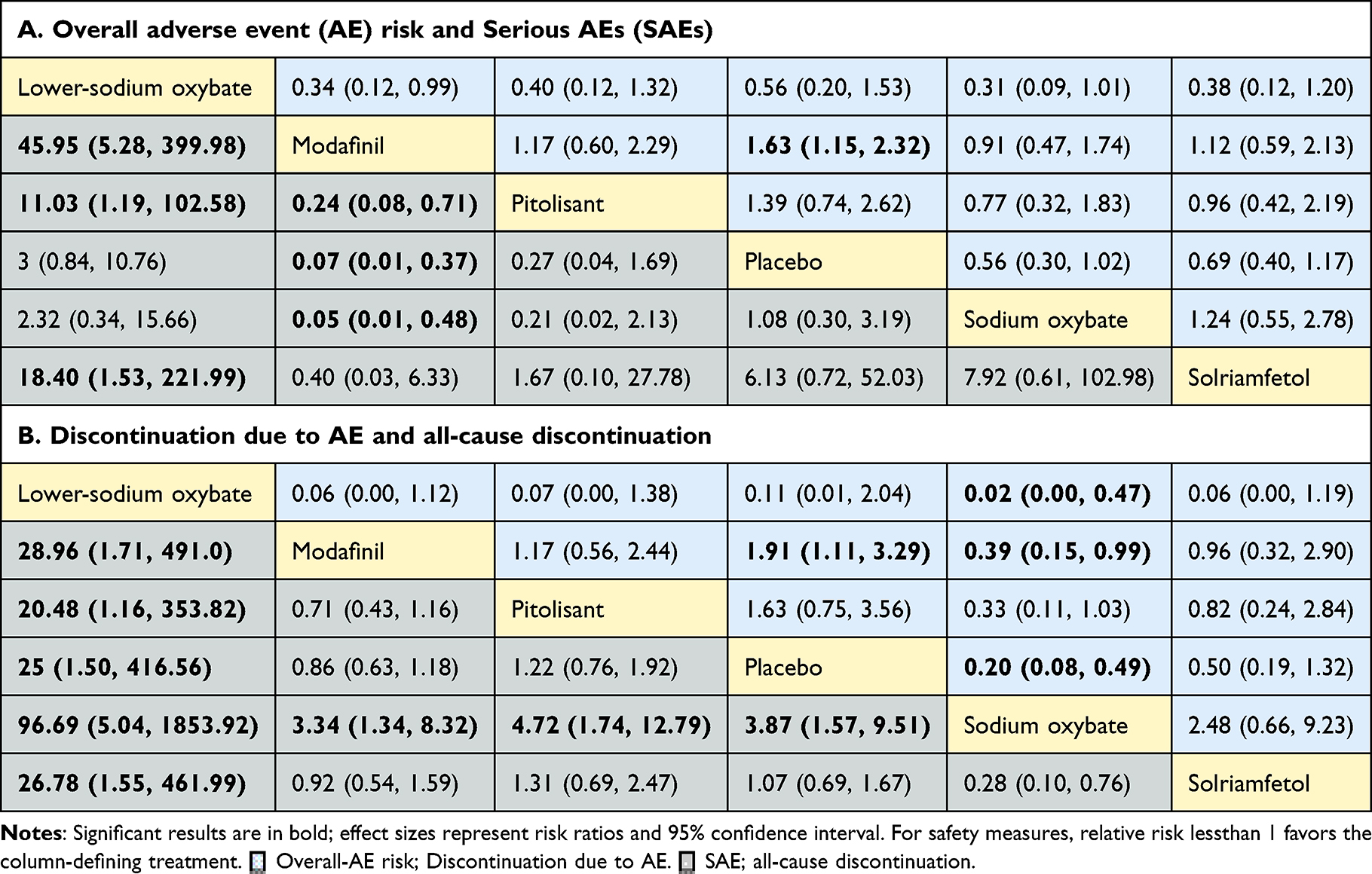 |
Table 2 Comparison of Safety Measures Between Multiple Wake-Promoting Agents |
 |
Figure 4 Forest plots for safety outcomes. (A) Overall AE risk. (B) Serious adverse events. (C) AE leading to discontinuation. (D) all-cause discontinuation. Abbreviations: AE, adverse event; RR, risk ratio. |
Regarding exploratory analysis of CNS events, with headache (12 studies),24,25,40,45,47,49,51,52,54–57 a significant risk was observed with solriamfetol (2.67; 95% CI=1.26–5.67) compared with placebo (Figure S7A). Among the treatment comparison, a significant risk was associated with solriamfetol versus modafinil (2.23; 95% CI=1.03–4.86) and solriamfetol versus SXB (3.58; 95% CI=1.37–9.36) (Table S7A). For dizziness (7 studies),24,25,40,45,52,54,56 all interventions, except LXB were identified. A significantly increased risk was observed with SXB (3.13; 95% CI=1.18–8.25) versus placebo (Figure S7B, Table S7A). For insomnia (6 studies),25,40,49,55–57 all interventions, except SXB, were included. A significantly increased risk was observed with solriamfetol (3.27; 95% CI=1.25–8.62) versus placebo (Figure S7C, Table S7B). For irritability (3 studies),25,54,56 no significant risk was observed among the treatments identified (modafinil, pitolisant, and solriamfetol) versus placebo (Figure S7D, Table S7B). Among the gastrointestinal (GI) events, for nausea (10 studies),25,40,45,47,49,50,52,54–56 a significantly increased risk was observed with modafinil (2.57; 95% CI=1.31–5.04), SXB (7.85; 95% CI=3.01–20.45), and solriamfetol (3.52; 95% CI=1.26–9.87) versus placebo (Figure S7E). Among the treatments, a significant risk was associated with SXB versus modafinil (3.06; 95% CI=1.11–8.41) (Table S7C). For dry mouth (3 studies),40,49,50 no significant risk was observed for modafinil, SXB, and solriamfetol versus placebo (Figure S7F, Table S7C). Higher risk of modafinil for dry mouth, SXB for dizziness and nausea, pitolisant for insomnia, and solriamfetol for headache was found in the p-score ranking.
SXB for headache and dry mouth, pitolisant for dizziness, and placebo for other AEs were suggested as the best treatment option (Table S6). Heterogeneity was not significant across the studies. Analysis could not be performed for AEs where studies identified were less than three.
Risk of Bias Across the Studies
Publication bias across the studies was assessed by funnel plots. Visual inspection and Egger test suggested no bias for efficacy measures except for ESS. In the ESS outcome, visual inspection suggested publication bias, which may be attributed to Black and Houghton's 2006 study,50 although Egger test (p=0.44) suggested otherwise (Figure S8). Similarly, publication bias was observed for the overall AE on visual inspection, which may be attributed to Bogan et al,55 whereas Egger test did not indicate the same (p=0.69) (Figures S9 and S10).
Discussion
Among the 17 RCTs that compared the efficacy and safety of wake-promoting agents for narcolepsy, all approved interventions were effective with the acceptable tolerability compared with placebo. For the efficacy outcomes, p-score ranked solriamfetol as highest for MWT, ESS, and PGI-C, whereas LXB was ranked highest for CGI-C. For the safety profile, all interventions except LXB showed increased overall AE risk compared with placebo. No significant difference between modafinil, pitolisant, solriamfetol, and placebo in all-cause discontinuation rate was observed indicating a tolerable safety profile. Higher risk of dry mouth associated with modafinil, dizziness and nausea with SXB, insomnia with pitolisant, and headache with solriamfetol was identified in individual AE risk of interest.
Overall, our study provides the most current evidence to date on the comparative effectiveness of the approved interventions reported to reduce narcolepsy-related EDS symptoms in double-blind RCTs. In addition, the present study offers the most extensive analysis on clinical outcomes of the EDS, including both subjective and objective measure of sleepiness and patient-reported and physician-reported changes of disease severity. Besides, the current study thoroughly investigates the risk profile of overall safety as well as individual AE of interest on the current available medications. The results of our study would largely fill the current evidence gap and provide insights in optimizing the management of EDS symptoms of narcolepsy.
Modafinil, SXB, pitolisant, solriamfetol, and LXB showed a significant efficacy compared with placebo for MWT and ESS outcomes at varying degrees, indicating these wake-promoting agents could effectively alleviate sleepiness and sustain wakefulness. Our results resonated with previously published meta-analyses in patients with narcolepsy.26,27 Difference in the values may be observed because of an update of studies to date as well as pooled dosage analysis for each treatment. Besides, the traditional stimulants such as amphetamine and methylphenidate have been approved and have a long history of use for EDS in narcolepsy.58–60 We attempted to analyze the studies related to methylphenidate and amphetamines for narcolepsy but failed to find any relevant RCTs. Clinical trials are warranted to understand the efficacy and safety of methylphenidate and amphetamines under controlled conditions.
The improvement of EDS is expected to translate into benefits in disease severity. By measuring CGI-C and PGI-C, the effects of medication on changes in disease severity could be obtained from patients’ and clinicians’ view. Compared with previous network meta-analyses,26,27 our study gained insights into comparison in effects of wake-promoting agents on changes of disease severity. For clinician-centric scores, all the interventions significantly improved the CGI-C scores with substantially larger scores observed with LXB (9.67) and solriamfetol (5.98) versus placebo. The general improvement in CGI-C is consistent with the earlier individual studies of SXB, solriamfetol, and modafinil.61–64 However, for PGI-C, most interventions did not have data except solriamfetol and LXB. A statistically significant greater response was observed with solriamfetol (9.39), whereas a favorable response was observed with LXB. These results suggest that there is consensus between physicians and patients regarding the patient’s conditions. Increasing attention is now being directed at the impact of sleep disorders through the patient-reported outcome measurement.65 Authorities such as FDA have initiated patient-focused drug development to ensure that patients’ voices could be incorporated in the drug development and evaluation.66 As part of the program, the COA Compendium suggested the use of patient-reported PGI-C for the evaluation of EDS associated with narcolepsy.9 Future clinical studies, other than solriamfetol and LXB, need to be performed to intervene inthe PGI-C scores, which will enable us to better understand the clinical benefits from the patients’ perspective.
The clinical significance threshold of efficacy measure, MWT is an increase of 2 minutes while with ESS it is a decrease of 2 points, which can be considered as the minimum level of improvement in the outcome.67 In our study, the results of all drugs met the clinical significance threshold, with solriamfetol showing a higher magnitude of benefit when compared with other medications.67 The current study also observed that solriamfetol had a higher magnitude of beneficial effect in controlling the EDS symptoms as evidenced across the efficacy measures (ESS, MWT, and PGI-C). Interestingly, these effects seem to be more pronounced in the objective method of MWT, in which pairwise treatment comparison showed statistical improvement of solriamfetol versus modafinil, pitolisant, and SXB. An earlier study reported sustained effects until the fifth trial of MWT at 7–9 hours post-dose with solriamfetol, whereas the effect of modafinil or armodafinil diminished by the fifth trial of MWT.45,68,69 Owing to the relatively small sample size and lack of head-to-head clinical trials, more direct comparison studies are required in the future to further elucidate the comparative efficacy of solriamfetol.
Another strength of our study is the extensive analysis of the safety profile of wake-promoting agents, including overall AE, SAE, AE leading to discontinuation, all-cause discontinuation, and several individual AE of interest. Consistent with the previous reports, our study found an increased but generally acceptable safety profile for modafinil, pitolisant, SXB, and solriamfetol for overall RR of AE.61,70 Though preliminary, the current study additionally observed a significantly increased risk of modafinil versus placebo in SAE, and modafinil and SXB versus placebo in AE leading to discontinuation. However, we observed similar all-cause discontinuation risk across modafinil, pitolisant, and solriamfetol compared with placebo (RR ~1), whereas a significant risk was found with SXB versus placebo. This indicates a good acceptability profile of modafinil, pitolisant, and solriamfetol for the treatment of narcolepsy-related EDS. To the best of our knowledge, it is the first NMA on comparison of acceptability of any interventions in narcolepsy. Interestingly, our results showed lower risk of LXB in almost all safety outcomes measured. However, given that one study of LXB was available57 and this may be too early for any conclusions, more evidence is needed in the future to clarify the safety profile of LXB.
Different from the previous NMA,26 the present study exploratively assessed the risk of commonly reported AE among wake-promoting agents individually. Among AEs related to CNS, headache was the most common AE associated with all the treatments, whereas dizziness and insomnia were observed with the treatments other than LXB. The p-scores ranking showed a higher risk of solriamfetol for headache, a higher risk of SXB for dizziness, and a higher risk of pitolisant for insomnia. Among the GI events, nausea was the most common GI event observed with all the treatments, except LXB. When selecting the treatment regimen for patients, a balanced approach of efficacy benefits and acceptable safety profile should be considered. Findings of the present study additionally enriched the information for the treatment strategy based on the specific safety profile.
Wakefulness-promoting drugs targeting the dopamine system have a potential for psychostimulant drug abuse. From this class of medication, modafinil and armodafinil are known to have a lower abuse potential.71,72 The recently approved drug solriamfetol is also known to have a lower abuse potential, as reported by Baladi et al,73 which can be attributed to lower binding affinity to dopamine and norepinephrine transporters as well as not having a monoamine-releasing effect. We attempted to assess the comparative abuse potential of medications in this study; however, the events related to the drug abuse could not be mapped as most of the studies have excluded the patients with a history of drug abuse and have not mapped the drug abuse events during the trial period. Although a trial related to solriamfetol observed no events related to euphoria and indication of abuse or addiction during the study period,56 assessment on comparative abuse potential remains worthy of future investigation.
There are several limitations in this study. Notably, the number of trials included for each treatment except modafinil varies from three to one. Caution should be exercised in strictly interpreting whether a treatment has led to greater improvement compared with others. Further, as the study focused on the most common and burdensome symptom, EDS and limited availability of the studies, we have pooled the studies regardless of the edition of ICSD diagnostic criteria for narcolepsy or the cataplexy status. This warrants the need for further investigation of effects of NT1 or NT2 on efficacy and safety. Also, research on the comparative effect of medications on other symptoms of narcolepsy would be necessary. Apart from the follow-up time for the studies identified being shorter (4–12 weeks), and the sample size being small, larger clinical trials with longer follow-up periods in the future are required. The current study also pooled the doses for each treatment which may not ascertain the impact of individual doses of treatment on efficacy and safety outcomes. Meta-analysis needs to be designed to investigate the optimal dosage for each treatment. Although the onset of narcolepsy often occurred in adolescents, the current study has focused on an adult patient population due to the lesser number of studies available in the adolescent population.74 Although the heterogeneity was high, we did not perform network meta-regression to explore the between-study heterogeneity variance, which may be a future recommendation. Further, one of the limitations of the current study is the lack of comparison of effect of different treatments on quality-of-life. Since EDS is not only an objective, but also a subjective perception, the treatment goal of narcolepsy should also aim to improve quality-of-life. Some studies included in our literature search have evaluated quality-of-life related outcomes, however, the tools utilized are quite diverse and inconsistent across different trials, such as the 36-Item Short Form Survey (SF-36), the Functional Outcome of Sleep Questionnaire Short Version (FOSQ-10), and the European Quality-of-Life Questionnaire (EQ-5D).57,75,76 Besides, none of these scales are narcolepsy-specific and thus may raise concerns when assessing the subtle aspects of the quality-of-life imposed by narcolepsy. Hence, more narcolepsy-specific measures for quality-of-life outcome should be developed and utilized in future research of narcolepsy treatment. Apart from the few points discussed in limitation which needs to be addressed in the future, the present study confirmed the improvement of EDS and patient-centric measures with the approved drugs; however, the treatment goal of narcolepsy should focus on improving the quality-of-life and functional outcomes with cost-effectiveness, which requires further investigation. Another area which requires attention is gender-specific treatment. Narcolepsy treatment might impact men and women differently, since women face maternal–fetal outcomes/risk factors during pregnancy and generally have a delayed diagnosis compared to men.77–79 Further, gender-specific medication is very important, since the effectiveness of steroidal contraceptives (sensitive CYP3A4 substrates) may be affected by the use of pitolisant and modafinil. Hence, gender-specific future clinical trials are warranted to understand the differential impact of narcolepsy treatment.
Conclusions
Following our observations, approved interventions are effective in varying degrees for treating excessive sleepiness symptoms and investigator/patient-centric scores with acceptable tolerability. Among the interventions analyzed, solriamfetol showed greater improvement with EDS outcomes and patient-centric scores with an acceptable safety profile.
Abbreviations
AE, adverse event; CGI-C, Clinical Global Impression of Change; CI, Confidence interval; CNS, Central nervous system; COA, Clinical outcome assessment; EDS, Excessive daytime sleepiness; EMA, European Medicine Agency; ESS, Epworth Sleepiness Scale; FDA, Food and Drug Administration; GI, Gastrointestinal; ICSD-III, International Classification of Sleep Disorders-Third Edition; MD, Mean difference; MWT, Maintenance of Wakefulness Test; NMA, Network meta-analysis; NT, Narcolepsy type; OR, Odds ratio; OSA, obstructive sleep apnea; PGI-C, Patient Global Impression of Change; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; LXB, Lower sodium oxybate; RCT, Randomized Controlled Trial; RR, Risk ratio; SAE, Serious adverse event; SXB, Sodium oxybate.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Trial Registration Information
The study was prospectively registered in the PROSPERO database (CRD 42022334915). https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=334915
Acknowledgments
The medical department of Ignis Therapeutics (Shanghai) Limited provided scientific support for this work, although they did not propose any specific therapy and therefore did not give any specific treatment recommendations. We would like to acknowledge Roopashree Subbaiaih, PhD and Amit Bhat, PhD from Indegene Pvt. Ltd for statistical analysis and medical writing assistance, which was funded by Ignis Therapeutics (Shanghai) Limited.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The current work was supported by National Natural Science Foundation of China (Grant No. 81571294), National Key R&D program of China (Grant No. 2021YFC2501400), and Research Fund for Chinese Sleep Research Society (Grant No. ZS-KY-2022-01).
Disclosure
Hui Ye is an employee of Ignis Therapeutics. The authors report no other potential conflicts of interest in this work.
References
1. Ohayon MM, Priest RG, Zulley J, Smirne S, Paiva T. Prevalence of narcolepsy symptomatology and diagnosis in the European general population. Neurology. 2002;58(12):1826–1833. doi:10.1212/WNL.58.12.1826
2. Ohayon MM. Epidemiology of narcolepsy. In: Bassetti C, Billiard M, Mignot E, editors. Narcolepsy and Hypersomnia. New York: Informa Healthcare; 2007:125–132.
3. Partinen M, Kronholm E. Epidemiology: Principles and Application in Sleep Medicine. Sleep Disorders Med. 2017:485.
4. Zhang Z, Mayer G, Dauvilliers Y, et al. Exploring the clinical features of narcolepsy type 1 versus narcolepsy type 2 from European Narcolepsy Network database with machine learning. Sci Rep. 2018;8:10628.
5. American Academy of Sleep Medicine. International Classification of Sleep Disorders.
6. Maski K, Steinhart E, Williams D, et al. Listening to the patient voice in narcolepsy: diagnostic delay, disease burden, and treatment efficacy. J Clin Sleep Med. 2017;13(3):419–425.
7. Maski K, Trotti LM, Kotagal S, et al. Treatment of central disorders of hypersomnolence: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2021;17(9):1881–1893.
8. Bassetti CLA, Kallweit U, Vignatelli L, et al. European guideline and expert statements on the management of narcolepsy in adults and children. Eur J Neurol. 2021;28(9):2815–2830.
9. Clinical Outcome Assessment Compendium; 2019. Available from: https://www.fda.gov/drugs/development-resources/clinical-outcome-assessment-compendium.
10. Patel S, Kon SSC, Nolan CM, et al. The Epworth Sleepiness Scale: minimum Clinically Important Difference in Obstructive Sleep Apnea. Am J Respir Crit Care Med. 2018;197(7):961–963.
11. Rosenberg R, Schweitzer PK, Steier J, et al. Residual excessive daytime sleepiness in patients treated for obstructive sleep apnea: guidance for assessment, diagnosis, and management. Postgrad Med. 2021;133(7):772–783.
12. Rosenberg R, Baladi M, Bron M. Clinically relevant effects of solriamfetol on excessive daytime sleepiness: a posthoc analysis of the magnitude of change in clinical trials in adults with narcolepsy or obstructive sleep apnea. J Clin Sleep Med. 2021;17(4):711–717.
13. Scammell TE. Narcolepsy. N Engl J Med. 2015;373(27):2654–2662.
14. Littner MR, Kushida C, Wise M, et al. Practice parameters for clinical use of the multiple sleep latency test and the maintenance of wakefulness test. Sleep. 2005;28(1):113–121.
15. Busner J, Targum SD. The Clinical Global Impressions Scale. Psychiatry. 2007;4(7):28–37.
16. Thorpy MJ. Recently Approved and Upcoming Treatments for Narcolepsy. CNS Drugs. 2020;34(1):9–27.
17. Pellitteri G, de Biase S, Valente M, Gigli GL. How treatable is narcolepsy with current pharmacotherapy and what does the future hold? Expert Opin Pharmacother. 2021;22(12):1517–1520.
18. EMA. Xyrem. European Medicines Agency. 2018. Available from: https://www.ema.europa.eu/en/medicines/human/EPAR/xyrem.
19. Maski K, Trotti LM, Kotagal S, et al. Treatment of central disorders of hypersomnolence: an American Academy of Sleep Medicine systematic review, meta-analysis, and GRADE assessment. J Clin Sleep Med. 2021;17(9):1895–1945.
20. Gandhi KD, Mansukhani MP, Silber MH, Kolla BP. Excessive Daytime Sleepiness: a Clinical Review. Mayo Clin Proc. 2021;96(5):1288–1301.
21. Franceschini C, Pizza F, Cavalli F, Plazzi G. A practical guide to the pharmacological and behavioral therapy of Narcolepsy. Neurotherapeutics. 2021;18(1):6–19.
22. Bhattarai J, Sumerall S. Current and Future Treatment Options for Narcolepsy: a Review. Sleep Sci. 2017;10(1):19–27.
23. Thorpy MJ. Modafinil/Armodafinil in the Treatment of Narcolepsy. In: Goswami M, Thorpy MJ, Pandi-Perumal SR, editors. Narcolepsy: A Clinical Guide. Springer International Publishing; 2016:331–339.
24. Black J, Swick T, Bogan R, et al. Impact of sodium oxybate, modafinil, and combination treatment on excessive daytime sleepiness in patients who have narcolepsy with or without cataplexy. Sleep Med. 2016;24:57–62.
25. Dauvilliers Y, Bassetti C, Lammers GJ, et al. Pitolisant versus placebo or modafinil in patients with narcolepsy: a double-blind, randomised trial. Lancet Neurol. 2013;12(11):1068–1075.
26. Lehert P, Falissard B. Multiple treatment comparison in narcolepsy: a network meta-analysis. Sleep. 2018;41:12.
27. Lehert P, Szoeke C. Comparison of modafinil and pitolisant in narcolepsy: a non-inferiority meta-analytical approach. Drugs Context. 2020;9:245.
28. Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 2009;6(7):e1000100.
29. Hutton B, Salanti G, Caldwell DM, et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med. 2015;162(11):777–784.
30. Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898.
31. Krahn U, Binder H, König J. A graphical tool for locating inconsistency in network meta-analyses. BMC Med Res Methodol. 2013;13:35.
32. Rücker G, Schwarzer G. Reduce dimension or reduce weights? Comparing two approaches to multi-arm studies in network meta-analysis. Stat Med. 2014;33(25):4353–4369.
33. Curtin F, Elbourne D, Altman DG. Meta-analysis combining parallel and cross-over clinical trials. III: the issue of carry-over. Stat Med. 2002;21(15):2161–2173.
34. Rücker G. Network meta-analysis, electrical networks and graph theory. Res Synth Methods. 2012;3(4):312–324.
35. Rücker G, Schwarzer G. Ranking treatments in frequentist network meta-analysis works without resampling methods. BMC Med Res Methodol. 2015;15:58.
36. Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–560.
37. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–634.
38. Malhotra A, Shapiro C, Pepin JL, et al. Long-term study of the safety and maintenance of efficacy of solriamfetol (JZP-110) in the treatment of excessive sleepiness in participants with narcolepsy or obstructive sleep apnea. Sleep. 2020;43(2):zsz220.
39. Weaver TE, Cuellar N. A randomized trial evaluating the effectiveness of sodium oxybate therapy on quality of life in narcolepsy. Sleep. 2006;29(9):1189–1194.
40. Thorpy MJ, Shapiro C, Mayer G, et al. A randomized study of solriamfetol for excessive sleepiness in narcolepsy. Ann Neurol. 2019;85(3):359–370.
41. Kushida CA, Shapiro CM, Roth T, et al. Once-nightly sodium oxybate (FT218) demonstrated improvement of symptoms in a Phase 3 randomized clinical trial in patients with narcolepsy. Sleep. 2022;45(6):zsab200.
42. Billiard M, Besset A, Montplaisir J, et al. Modafinil: a double-blind multicentric study. Sleep. 1994;17(8 Suppl):S107–112.
43. Broughton RJ, Fleming JA, George CF, et al. Randomized, double-blind, placebo-controlled crossover trial of modafinil in the treatment of excessive daytime sleepiness in narcolepsy. Neurology. 1997;49(2):444–451.
44. Saletu M, Anderer P, Saletu-Zyhlarz GM, Mandl M, Saletu B, Zeitlhofer J. Modafinil improves information processing speed and increases energetic resources for orientation of attention in narcoleptics: double-blind, placebo-controlled ERP studies with low-resolution brain electromagnetic tomography (LORETA). Sleep Med. 2009;10(8):850–858.
45. Moldofsky H. A randomized trial of the long-term, continued efficacy and safety of modafinil in narcolepsy. Sleep Med. 2000;1(2):109–116.
46. Kollb-Sielecka M, Demolis P, Emmerich J, Markey G, Salmonson T, Haas M. The European Medicines Agency review of pitolisant for treatment of narcolepsy: summary of the scientific assessment by the Committee for Medicinal Products for Human Use. Sleep Med. 2017;33:125–129.
47. US Modafinil in Narcolepsy Multicenter Study Group. Randomized trial of modafinil as a treatment for the excessive daytime somnolence of narcolepsy. Neurology. 2000;54(5):1166–1175.
48. US Xyrem® Multicenter Study Group. A randomized, double blind, placebo-controlled multicenter trial comparing the effects of three doses of orally administered sodium oxybate with placebo for the treatment of narcolepsy. Sleep. 2002;25(1):42–49.
49. US Modafinil in Narcolepsy Multicenter Study Group. Randomized trial of modafinil for the treatment of pathological somnolence in narcolepsy. US Modafinil in Narcolepsy Multicenter Study Group. Ann Neurol. 1998;43(1):88–97.
50. Black J, Houghton WC. Sodium oxybate improves excessive daytime sleepiness in narcolepsy. Sleep. 2006;29(7):939–946.
51. Harsh JR, Hayduk R, Rosenberg R, et al. The efficacy and safety of armodafinil as treatment for adults with excessive sleepiness associated with narcolepsy. Curr Med Res Opin. 2006;22(4):761–774.
52. US Xyrem® Multicenter Study Group. A randomized, double blind, placebo-controlled multicenter trial comparing the effects of three doses of orally administered sodium oxybate with placebo for the treatment of narcolepsy. Sleep. 2002;25(1):42–49.
53. Xyrem International Study Group. A double-blind, placebo-controlled study demonstrates sodium oxybate is effective for the treatment of excessive daytime sleepiness in narcolepsy. J Clin Sleep Med. 2005;1(4):391–397.
54. Szakacs Z, Dauvilliers Y, Mikhaylov V, et al. Safety and efficacy of pitolisant on cataplexy in patients with narcolepsy: a randomised, double-blind, placebo-controlled trial. Lancet Neurol. 2017;16(3):200–207.
55. Bogan RK, Feldman N, Emsellem HA, et al. Effect of oral JZP-110 (ADX-N05) treatment on wakefulness and sleepiness in adults with narcolepsy. Sleep Med. 2015;16(9):1102–1108.
56. Ruoff C, Swick TJ, Doekel R, et al. Effect of Oral JZP-110 (ADX-N05) on Wakefulness and Sleepiness in Adults with Narcolepsy: a Phase 2b Study. Sleep. 2016;39(7):1379–1387.
57. Bogan RK, Thorpy MJ, Dauvilliers Y, et al. Efficacy and safety of calcium, magnesium, potassium, and sodium oxybates (lower-sodium oxybate [LXB]; JZP-258) in a placebo-controlled, double-blind, randomized withdrawal study in adults with narcolepsy with cataplexy. Sleep. 2021;44(3):zsaa206.
58. Yoss RE, Daly D. Treatment of narcolepsy with Ritalin. Neurology. 1959;9(3):171.
59. Rasmussen N. America’s first amphetamine epidemic 1929–1971: a quantitative and qualitative retrospective with implications for the present. Am J of Public Health. 2008;98(6):974–985.
60. Morton WA, Stockton GG. Methylphenidate abuse and psychiatric side effects. Prim Care Companion J Clin Psychiatry. 2000;2(5):159–164.
61. Wang J, Yang S, Li X, et al. Efficacy and safety of solriamfetol for excessive sleepiness in narcolepsy and obstructive sleep apnea: findings from randomized controlled trials. Sleep Med. 2021;79:40–47.
62. Alshaikh MK, Tricco AC, Tashkandi M, Mamdani M, Straus SE, BaHammam AS. Sodium oxybate for narcolepsy with cataplexy: systematic review and meta-analysis. J Clin Sleep Med. 2012;8(4):451–458.
63. Chapman JL, Vakulin A, Hedner J, Yee BJ, Marshall NS. Modafinil/armodafinil in obstructive sleep apnoea: a systematic review and meta-analysis. Eur Respir J. 2016;47(5):1420–1428.
64. Boscolo-Berto R, Viel G, Montagnese S, Raduazzo DI, Ferrara SD, Dauvilliers Y. Narcolepsy and effectiveness of gamma-hydroxybutyrate (GHB): a systematic review and meta-analysis of randomized controlled trials. Sleep Med Rev. 2012;16(5):431–443.
65. Medarov BI, Victorson DE, Judson MA. Patient-reported outcome measures for sleep disorders and related problems: clinical and research applications. CHEST. 2013;143(6):1809–1818.
66. CDER Patient-Focused Drug Development. Available from: https://www.fda.gov/drugs/development-approval-process-drugs/cder-patient-focused-drug-development.
67. Maski K, Trotti LM, Kotagal S, et al. Treatment of central disorders of hypersomnolence: an American Academy of Sleep Medicine systematic review, meta-analysis, and GRADE assessment. J Clin Sleep Med. 2021;17(9):1895–1945.
68. Mignot EJM. A practical guide to the therapy of narcolepsy and hypersomnia syndromes. Neurotherapeutics. 2012;9(4):739–752.
69. Schwartz JRL, Feldman NT, Bogan RK, Nelson MT, Hughes RJ. Dosing regimen effects of modafinil for improving daytime wakefulness in patients with narcolepsy. Clin Neuropharmacol. 2003;26(5):252–257.
70. Subedi R, Singh R, Thakur RK, Jha KCB. D, Ray BK. Efficacy and safety of solriamfetol for excessive daytime sleepiness in narcolepsy and obstructive sleep apnea: a systematic review and meta-analysis of clinical trials. Sleep Med. 2020;75:510–521.
71. Kim D. Practical Use and Risk of Modafinil, a Novel Waking Drug. Environ Health Toxicol. 2012;27:e2012007.
72. Golicki D, Bala MM, Niewada M, Wierzbicka A. Modafinil for narcolepsy: systematic review and meta-analysis. Med Sci Monit. 2010;16(8):RA177–186.
73. Baladi MG, Forster MJ, Gatch MB, et al. Characterization of the Neurochemical and Behavioral Effects of Solriamfetol (JZP-110), a Selective Dopamine and Norepinephrine Reuptake Inhibitor. J Pharmacol Exp Ther. 2018;366(2):367–376.
74. Nishino S. Clinical and neurobiological aspects of narcolepsy. Sleep Med. 2007;8(4):373–399.
75. Szakacs Z, Dauvilliers Y, Mikhaylov V, et al. Safety and efficacy of pitolisant on cataplexy in patients with narcolepsy: a randomised, double-blind, placebo-controlled trial. Lancet Neurol. 2017;16(3):200.
76. Weaver TE, Cuellar N. A randomized trial evaluating the effectiveness of sodium oxybate therapy on quality of life in narcolepsy. Sleep. 2006;29(9):1189.
77. Kornum BR, Knudsen S, Ollila HM, et al. Narcolepsy. Nat Rev Dis Primers. 2017;3:16100.
78. Won C, Mahmoudi M, Qin L, Purvis T, Mathur A, Mohsenin V. The impact of gender on timeliness of narcolepsy diagnosis. J Clin Sleep Med. 2014;10(1):89–95.
79. Wilson A, Dongarwar D, Carter K, Marroquin M, Salihu HM. The association between narcolepsy during pregnancy and maternal-fetal risk factors/outcomes. Sleep Sci. 2022;15(3):297–304.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.