")
Back to Journals » Infection and Drug Resistance » Volume 17
Comparative Analysis of Two Commercial Automated Systems with Agar Dilution for Oxacillin Susceptibility and Their Association with Genotypes of Invasive Staphylococcus aureus Isolates (2011–2021)
Authors Wang WY , Chen YH, Lee YL, Chiu CF, Tsao SM
Received 10 November 2023
Accepted for publication 7 March 2024
Published 20 March 2024 Volume 2024:17 Pages 1121—1129
DOI https://doi.org/10.2147/IDR.S445211
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Wei-Yao Wang,1,2 Yi-Hsin Chen,3– 5 Yu-Lin Lee,1,2 Chen-Feng Chiu,6 Shih-Ming Tsao1,2
1School of Medicine, Chung Shan Medical University, Taichung, Taiwan; 2Department of Internal Medicine, Chung Shan Medical University Hospital, Taichung, Taiwan; 3Department of Nephrology, Taichung Tzu Chi Hospital, Taichung, Taiwan; 4School of Medicine, Tzu Chi University, Hualien, Taiwan; 5Department of Artificial Intelligence and Data Science, National Chung Hsing University, Taichung, Taiwan; 6Department of Internal Medicine, Feng Yuan Hospital, Ministry of Health and Welfare, Taichung, Taiwan
Correspondence: Shih-Ming Tsao, Department of Internal Medicine, Chung Shan Medical University Hospital, # 110, Section 1, Jianguo North Road, Taichung City, 40201, Taiwan, Tel +886 4 24739595 ext.34718, Fax +886-4-23248172, Email [email protected]
Background: Determining oxacillin susceptibility using reference methods and automated systems is crucial for treating invasive infections caused by Staphylococcus aureus. This study compares the oxacillin susceptibility results from the two automated systems with agar dilution and correlates them with genotypes of invasive S. aureus.
Methods: Non-duplicate S. aureus invasive isolates were collected over an 11-year period. The oxacillin susceptibility was determined with Phoenix 100 (Jan 2011 to Aug 2018) or Vitek 2 (Sep 2018 to Dec 2021), and susceptibility for oxacillin and cefoxitin was determined with agar dilution. Methicillin-resistant S. aureus (MRSA) was confirmed with mecA existence, and the genotype was determined using SCCmec. The association between genotype and antibiotic susceptibility using two automated systems and agar dilution was evaluated.
Results: A total of 842 invasive S. aureus, including 443 mecA+ MRSA and 399 mecA- MSSA, were collected. The susceptibility rates of oxacillin determined by two automated systems and agar dilution were 68.8% (76.8% for Phoenix 100 and 57.6% for Vitek 2) and 54.0%, respectively. When compared with the oxacillin susceptibility using agar dilution, the categorical agreement for Phoenix 100 and Vitek 2 were 0.46% and 0.88%, respectively (p < 0.001). One hundred and forty-three isolates were misinterpreted as oxacillin-susceptible S. aureus (OSSA) using automated systems while comparing with agar dilution, among which molecularly community-associated MRSA (CA-MRSA) outnumbered healthcare-associated MRSA (HA-MRSA) (99 vs 34, p < 0.001). There were 70 mecA+ OSSA (OS-MRSA) using agar dilution, among which 42 harbored SCCmec types were predominantly categorized as CA-MRSA (38, p < 0.001).
Conclusion: The categorical agreement of Vitek 2 in determining oxacillin susceptibility and predicting mecA existence is comparable with agar dilution, whereas Phoenix 100 is not. Most of those ORSA determined by agar dilution but misinterpreted as OSSA by automated systems and OS-MRSA are categorized as CA-MRSA.
Keywords: oxacillin susceptibility, automated systems, agar dilution, SCCmec, CA-MRSA
Introduction
Staphylococcus aureus, encompassing methicillin-susceptible (MSSA) and methicillin-resistant S. aureus (MRSA), is the predominant pathogen causing various invasive infections in both community and healthcare settings1,2 The crude mortality rates of invasive infections by MRSA range from 10.2% for bacteremia to 55.6% for septic shock.2 MRSA has not only replaced MSSA, but its hospitalization rates have also surpassed those by MSSA.3 Determining methicillin resistance, mediated by penicillin-binding protein 2a (PBP2a), is essential for appropriate antibiotic treatment in clinical practice.4 Automated systems have been implemented for accurate species identification and rapid determination of antibiotic susceptibility,5 but discrepancies between automated systems and the reference antibiotic susceptibility test (AST) have also been reported.6 The goals of this study are to compare the oxacillin susceptibility results between the two commercial automated systems and the reference AST (categorical agreement, CA) and to investigate the association between the discrepancy of AST results and the genotypes of MRSA.
Materials and Methods
Isolate Identification and Antimicrobial Susceptibility Tests
Invasive Staphylococcus aureus isolates cultivated from sterile sites were identified using standard microbiologic methods and two commercial automated identification and antibiotic susceptibility test systems. These two systems, Phoenix 100 (BD Diagnostic Systems, Sparks, Md, USA, from Jan 1st, 2011, to Aug 31st, 2018) and Vitek 2 (bioMérieux, Marcy L’Etoile, France, from Sep 1st, 2018 to Dec 31st, 2021), over an 11-year period (2011–2021) were applied in the Chung Shan Medical University Hospital, a medical center affiliated with 1300 beds in central Taiwan. The antibiotic susceptibility tests for S. aureus were performed using agar dilution for vancomycin, oxacillin, and cefoxitin according to the Clinical Laboratory Standards Institute (CLSI).4 Modified microbroth dilution tests, including the PMIC/ID-25 panel of Phoenix 100 and the AST-P267 card of Vitek 2, were used for antibiotic susceptibility tests of automated systems according to the respective manufacturer's guides.7 Phenotypes of oxacillin-susceptible (OSSA) and resistant S. aureus (ORSA) were defined as minimal inhibitory concentration (MIC) against oxacillin ≤2 and ≥4 mg/L, respectively, whether using agar dilution or the automated systems.
Molecular Typing
The authors extracted the genomic DNA from each S. aureus isolate using as a template for primers annealing and amplification of the mecA gene with polymerase-chain reaction (PCR).8 Methicillin-resistant (MRSA) and susceptible S. aureus (MSSA) were defined based on the presence or absence of mecA. Multiplex PCR was employed to identify the SCCmec types of MRSA strains.9 SCCmec types I–V were identified by comparing the PCR banding patterns of S. aureus reference strains: ATCC 10442 (SCCmec type I), N315 (SCCmec type II), 85/2082 (SCCmec type III), MW2 (SCCmec type IVa), WIS (SCCmec type V). Isolates initially determined to be SCCmecV were further analyzed using specific primers (ccrC-FR) and were compared with the SCCmecVT reference strain TSGH-17.10 Molecularly community-associated MRSA (CA-MRSA) was defined as those harboring SCCmec IV, V, and VT, and healthcare-associated MRSA (HA-MRSA) was defined as those harboring SCCmec I, II, and III.11 Oxacillin-susceptible mecA-positive S. aureus (OS-MRSA) was defined as an isolate harboring mecA with oxacillin MIC ≤ 2 mg/L using agar dilution.12
Statistical Methods
SPSS software (PAWS Statistics 18.0.0; SPSS Inc., Chicago, IL, USA) was employed for statistical analyses. The difference between two categorical variables was determined using Fisher’s exact test. A p-value <0.05 indicated a significant difference. The categorical (inter-rater) agreement of susceptibility results from automated systems and agar dilution (reference) was measured using Cohen’s kappa coefficient.
Results
Specimen Distribution
A total of 842 non-duplicate invasive S. aureus isolates were collected during the study period (2011–2021). The majority of the invasive isolates originated from blood (732, 86.9%), followed by those from bronchoalveolar lavage (BAL) (60, 7.1%), pleural effusion (16, 1.9%), ascites (12, 1.4%), synovial fluid (12, 1.4%), and cerebrospinal fluid (10, 1.2%) (Table 1). Of these, 443 (52.6%) S. aureus harbored the mecA gene (MRSA), and the remaining 399 S. aureus isolates without mecA were classified as MSSA.
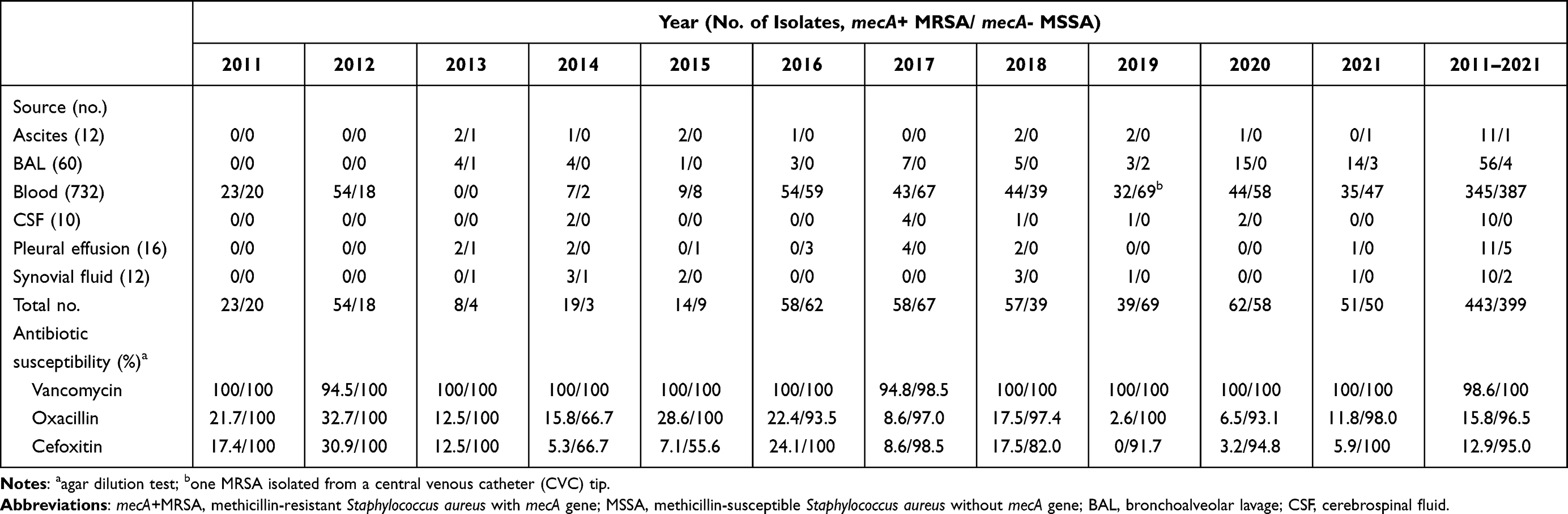 |
Table 1 The Yearly Distribution of Sources and the Antibiotic Susceptibility Rates of 842 Invasive Staphylococcus aureus Isolates (443 mecA+MRSA and 399 mecA-MSSA) (2011–2021) |
Antimicrobial Susceptibility Results Using Two Automated Systems and Agar Dilution
Table 1 demonstrates the yearly distribution and total susceptibility results of 842 invasive S. aureus isolates (including 443 MRSA and 399 MSSA) using agar dilution. Vancomycin remained the most effective antibiotics against MRSA and MSSA, with susceptibility rates of 99.3% and 100%, respectively. The susceptibility rates of oxacillin, and cefoxitin for MRSA/MSSA were for 15.8%/96.5% and 12.9%/95.0%, respectively. Six (1.4%) vancomycin-intermediate S. aureus (VISA) isolates with vancomycin MIC of 4 mg/L were identified, but no vancomycin-resistant S. aureus (VRSA) was found. Table 2 lists the yearly distribution of oxacillin susceptibility determined with agar dilution and two automated systems (Phoenix 100 and Vitek 2). A significant discrepancy in OSSA/ORSA phenotypes between agar dilution (455/387) and automated systems (579/263) was observed. Similarly, significant inconsistency existed between mecA gene presence and oxacillin resistance determined by either agar dilution or the two automated systems. For example, the number/percentage of mecA+OSSA (ie OS-MRSA) determined by agar dilution and two automated systems were 70/15.8% and 190/42.9%, respectively (Table 2).
 |
Table 2 Comparative Analysis of Distribution of the Phenotypes Determined by BD PhoenixTM 100 or Vitek 2 Automated Systems and Agar Dilution and with Genotypes of 842 Invasive Staphylococcus aureus Isolates (2011–2021) |
Comparative Analysis of Antimicrobial Susceptibility with Molecular Typing Results
Table 3 presents the comparative analysis and categorical agreement of antibiotic susceptibility results from agar dilution and two automated systems with mecA presence. The sensitivity of ORSA detection using two automated systems compared with the reference method (agar dilution) was low (63.0%), especially with Phoenix 100 (46.9%) (p < 0.001). The sensitivity of predicting mecA presence using two automated systems was insufficient (57.1%), which was significantly lower with Phoenix 100 (41.0%) (p < 0.001). In contrast, the sensitivity rates of agar dilution using oxacillin and cefoxitin for mecA gene prediction were comparable (84.2% with oxacillin and 87.1% with cefoxitin, respectively). A similar sensitivity rate in predicting mecA gene presence using Vitek 2 was also observed (82.9%). The categorical agreement (CA) represented as Cohen’s kappa coefficient (κ) of oxacillin susceptibility between automated systems and the agar dilution test was 0.603, significantly lower among Phoenix 100 and agar dilution than Vitek 2 (p < 0.001). A significant decrease in CA with mecA gene presence was also observed in the subgroup of the Phoenix system (κ= 0.379, p < 0.001) (Table 3). The analysis of CA among agar dilution and mecA gene presence showed that the κ value is slightly higher among cefoxitin (0.815) than oxacillin (0.799) (Table 3).
 |
Table 3 Comparative Analysis and Categorical Agreement (Kappa Coefficient) of Antibiotic Susceptibility Results from Agar Dilution and Compact Automated Systems (Phoenix® and Vitek® 2) with mecA Gene Existence of 842 Invasive Staphylococcus aureus Isolates (2011–2021) |
Among the 443 mecA+ MRSA isolates, 412 (93.0%) were classified as SCCmec type I to V, including SCCmec I (3, 0.7%), SCCmec II (41, 9.2%), SCCmec III (80, 18.0%), SCCmec IV (185, 41.8%), SCCmec V (53, 12.0%), and SCCmec VT (50, 11.3%). Thirty-one (7.0%) mecA+ MRSA isolates could not be typed by multiplex PCR, and no mecC gene was identified within this subset. The association between false-negative results (ie, 143 ORSA by agar dilution but misinterpreted as OSSA by Phoenix 100 or Vitek 2) and mecA gene presence/SCCmec types is shown in Table 4. Those with false-negative results assigned by the two automated systems (including 120 isolates by Phoenix 100 and 23 isolates by Vitek 2) were significantly associated with mecA+ presence (p = 0.01) and CA-MRSA (p < 0.001).
 |
Table 4 The Association Between False Negative Results/True Positive Results by Phoenix 100/Vitek 2 Automated Systems and mecA Existence/SCCmec Types |
A total of 70 OS-MRSA (oxacillin MIC ≤ 2 mg/L) isolates were identified using agar dilution, and their distribution and proportion stratified by oxacillin MICs were as follows: MIC ≤ 0.25 mg/L, 13.4% (9/67); MIC = 0.5 mg/L, 13.6% (30/220); MIC = 1 mg/L, 14.6% (19/130); and MIC = 2 mg/L, 31.6% (12/38). Among the 70 OS-MRSA, 42 isolates were classified with SCCmec types (2 with SCCmec I; one each with SCCmec II and III; 23 with SCCmec IV; 9 with SCCmec V; 6 with SCCmec VT, and 28 untyped). OS-MRSA was more strongly associated with CA-MRSA than HA-MRSA (38 vs 4, p < 0.001). The prevalence and trends of CA-MRSA, HA-MRSA, and OS-MRSA are depicted in Figure 1. The prevalence of CA-MRSA surpassed that of HA-MRSA starting in 2014, and OS-MRSA steadily increased from 2011 to 2016 before decreasing thereafter.
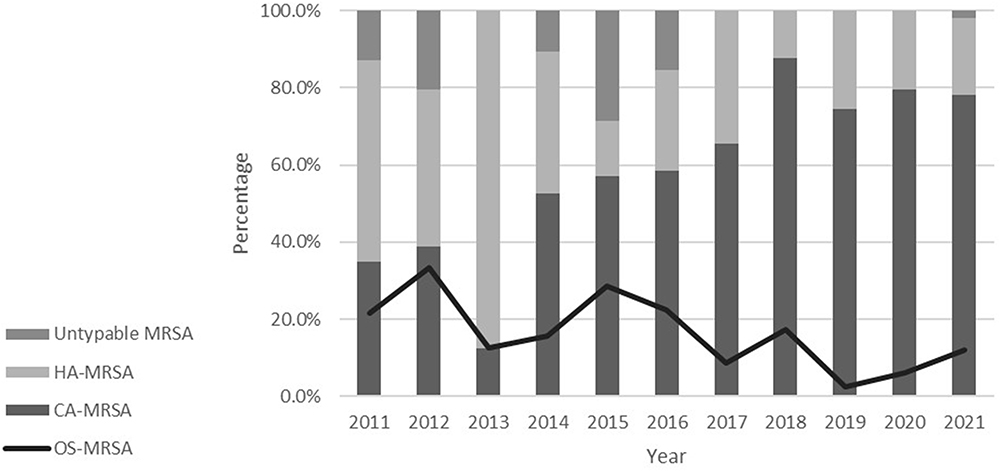 |
Figure 1 The prevalence and the trends of molecularly community-associated (CA-MRSA), molecularly healthcare-associated methicillin-resistant S. aureus (HA-MRSA), and oxacillin-susceptible mecA-positive S. aureus (OS-MRSA) during 11 years (2011–2021). |
Discussion
Invasive infections caused by S. aureus have affected specific populations in both community and healthcare settings, exerting a substantial negative impact on patient outcomes and public health.2,13,14 Appropriate empirical and targeted antibiotics, based on susceptibility results, are essential for clinical cure and microbial eradication.2,11,14,15 Commercial automated systems aid medical technicians in accurately identifying microorganisms and in determining antimicrobial susceptibility efficiently.5,16,17 Although previous literatures have reported excellent CA among automated systems and reference methods in determining the susceptibility of clinical S. aureus strains,6,7,17–19 some discrepancies have also been reported.12,20 We have observed significant inconsistency in oxacillin susceptibility results between the two automated systems, BD Phoenix 100 and Vitek 2. Consequently, we conducted a longitudinal study to analyze the CA of antibiotic susceptibility among two automated systems and agar dilution and to correlate the susceptibility inconsistency with genotypes of invasive S. aureus.
The proportion of OSSA in this study was 54.5%, aligning closely with a 5-year national surveillance in Taiwan from 2016 to 2021 (57%),21 but higher than the SMART study (46.1%) in 2020.22 A slight increase in VISA (1.4%) prevalence was noted compared with the SMART study (0.3%).22 These results suggest that susceptibility rates of S. aureus to oxacillin (OSSA phenotype) vary by region and setting, and that VISA was rarely identified in Taiwan.23
Previous publications demonstrated excellent CA between automated systems and reference methods. Fahr et al conducted a European collaborative two-center trial and revealed a CA of 97% between the Phoenix system and the broth microdilution (BMD) test.19 Comparative performance analysis of the Phoenix PMIC/ID102 panel and Vitek 2 system also exhibited excellent CA with BMD (99.8% for Phoenix and 99.7% for Vitek 2, respectively).7 However, our results differed considerably from these findings. The CA between the Phoenix system and the reference agar dilution was very low (46.9%), significantly lower than that of the Vitek 2 system (85.7%, p < 0.001). Additionally, we noted a lesser degree of discrepancy between the present study and previous reports regarding CA between the Vitek 2 system and agar dilution. We speculate that differences in CA between the Phoenix system and reference methods in the present study and previous reports may result from the prevalence and evolutionary changes of S. aureus strains, especially OS-MRSA, in different geographic areas.
Borderline oxacillin-resistant S. aureus (BORSA), first described in 1986, does not harbor mecA and exhibits borderline or intermediate susceptibility to oxacillin with MIC of 1–8 mg/L.24 Resistance mechanisms to methicillin and β-lactams include overproduction of staphylococcal β-lactamase,24 penicillin-binding protein (PBP) mutations,25 and methicillinase production.26 Treatment failures with penicillinase-resistant penicillins (PRPs) have been reported for invasive infections caused by BORSA.27 We identified only 14 (1.6%) mecA-negative invasive ORSA isolates, supporting the theory that mecA-mediated resistance accounts for the majority of ORSA.
The CLSI and several other publications have recommended using cefoxitin susceptibility (disk diffusion or dilution methods) to enhance the detection of mecA-mediated ORSA, with sensitivity rates ranging from 98% to 100%.4–7,12,20 As depicted in Table 3, the sensitivity rates of oxacillin and cefoxitin using agar dilution in detecting mecA presence are 84.2% and 87.1%, respectively, significantly lower than previous reports. This discrepancy can be attributed to the increasing prevalence of mecA+ OSSA (OS-MRSA) (70, 15.8%) in Taiwan compared to 0% in the U.S.7 and in Northern Bavaria, Germany,28 1.2–1.8% in Shanghai,12,29 and 9.0% in Kunming,20 China. These results underscore the challenges in accurately identifying mecA using reference methods. The mechanism of OS-MRSA has been delineated by Chen et al, revealing that CA-MRSA strains harboring ST59-SCCmec IV and V genotypes with mecA promoter mutations are responsible for the OS-MRSA phenotype.30 Our study has further confirmed that the OS-MRSA phenotype primarily occurs among molecularly CA-MRSA (SCCmec IV, V, and VT) (Table 4) and centralizes at an oxacillin MIC of 2 mg/L, which is consistent with previous literatures.12,20,29,31,32 Clinical application of penicillinase-resistant penicillins and β-lactams for treating invasive OS-MRSA should be approached with caution, as the oxacillin resistance (growing on tryptone soy agar with oxacillin of 32 mg/L) is inducible among OS-MRSA with little antibiotic resistance.12
Junkins et al found that cefoxitin was useful in automated systems to enhance the detection of ORSA and mecA. In 16 instances (9 on Phoenix and 7 on Vitek 2), an oxacillin MIC in the susceptible range was correctly altered to resistant based on the cefoxitin susceptibility result.7 Our study has indicated significant discordance between automated systems and mecA (CA 0.531, Table 3), with more pronounced discordance observed using the Phoenix 100 than the Vitek 2 (CA, 0.379 vs.0.894, p < 0.001). Most false-negative OSSA determined by the automated systems harbor mecA (p < 0.001) (Table 4), suggesting a re-evaluation of cefoxitin for enhancing the detection of mecA using particular automated systems.
After correlating the false-negative OSSA phenotype using automated systems with genotypes, most of these isolates were found to belong to CA-MRSA (SCCmec IV, V, and VT). As molecularly CA-MRSA has gradually surpassed HA-MRSA in communities and healthcare settings,3,11,12,29 the prevalence of false-negative OSSA phenotypes with the use of automated systems is expected to increase. Therefore, the development of new and practical phenotypic tools for detecting OS-MRSA is urgently needed.
This study had several limitations. First, the number of isolates collected during 2013–2015 was relatively small due to a faculty shortage, which might cause sample size bias. Second, further molecular profiles, such as multilocus sequencing typing (MLST) and whole-genome sequencing (WGS), were lacking and have been scheduled for the next project due to budget constraints. Third, the epidemiologic and clinical characteristics of the host were not surveyed for risk stratification or outcome evaluation due to anonymized data. Lastly, few mecA/mecC negative ORSA and VISA isolates were identified in this single-center study, necessitating further studies such as WGS and proteomic profiles for clarification of the resistance mechanisms.
Conclusion
The present study provides insights into the inconsistency in antibiotic susceptibility, mainly OS-MRSA, among automated systems and the agar dilution test. Vitek 2, unlike Phoenix 100, has comparable categorical agreement with agar dilution concerning oxacillin susceptibility and mecA gene detection. OS-MRSA is closely related to CA-MRSA and centralizes at an oxacillin MIC of 2 mg/L, raising concerns about the treatment efficacy for invasive OS-MRSA infections using semi-synthetic penicillins and β-lactams.
Ethical Approval
This study was conducted and complied in accordance with the Declaration of Helsinki. The study protocol was extensively reviewed and approved by the Institutional Review Board (IRB) of Chung Shan Medical University Hospital (reference number CS1-21176). The IRB of Chung Shan Medical University Hospital did not require written informed consent from patients because the data of the patients used in the study were anonymized, and no samples from human or animals were specially collected for this research.
Acknowledgment
We thank Mr. Aaron Coughman for his assistance in editing English grammar of this manuscript.
Funding
This project was funded by Chung Shan Medical University (grant number: CSMU-TSMH-104-02). This funding source played no role in study design or conduction, data collection, analysis or interpretation, writing of the manuscript, or decision to submit it for publication.
Disclosure
The authors declare no conflicts of interest in relation to this study.
References
1. Lowy FD. Staphylococcus aureus infections. N Engl J Med. 2020;339(8):520–532. doi:10.1056/NEJM199808203390806
2. Klevens RM, Morrison MA, Nadle J, et al. Invasive methicillin-resistant Staphylococcus aureus infections in the United States. JAMA. 2007;298(15):1763–1771. doi:10.1001/jama.298.15.1763
3. Mera RM, Suaya JA, Amrine-Madsen H, et al. Increasing role of Staphylococcus aureus and community-acquired methicillin-resistant Staphylococcus aureus infections in the United States: a 10-year trend of replacement and expansion. Microb Drug Resist. 2011;17(2):321–328. doi:10.1089/mdr.2010.0193
4. CLSI. Performance Standards for Antimicrobial Susceptibility Testing; CLSI Document M100-Ed 30. Wayne, PA: Clinical and Laboratory Standards Institute; 2022.
5. Winstanley T, Courvalin P. Expert systems in clinical microbiology. Clin Microbiol Rev. 2011;24(3):515–556. doi:10.1128/CMR.00061-10
6. Swenson JM, Lonsway D, McAllister S, et al. Detection of mecA-mediated resistance using reference and commercial testing methods in a collection of Staphylococcus aureus expressing borderline oxacillin MICs. Diagn Microbiol Infect Dis. 2007;58(1):33–39. doi:10.1016/j.diagmicrobio.2006.10.022
7. Junkins AD, Lockhart SR, Heilmann KP, et al. BD Phoenix and Vitek 2 detection of mecA-mediated resistance in Staphylococcus aureus with cefoxitin. J Clin Microbiol. 2009;47(9):2879–2882. doi:10.1128/JCM.01109-09
8. Oliveira DC, Lencastre HD. Multiplex PCR strategy for rapid identification of structural types and variants of the mec- element in methicillin-resistant Staphylococcus aureus. Antimicrobial Agents and Chemotherapy. 2002;46(7):2155–2161. doi:10.1128/aac.46.7.2155-2161.2002
9. Kondo Y, Ito T, Ma XX, et al. Combination of multiplex PCRs for staphylococcal cassette chromosome mec type assignment: rapid identification system for mec, ccr, and major differences in junkyard regions. Antimicrob Agents Chemother. 2007;51(1):264–274. doi:10.1128/AAC.00165-06
10. Boyle-Vavra S, Ereshefsky B, Wang CC, et al. Successful multiresistant community-associated methicillin-resistant staphylococcus aureus lineage from tTaipei, tTaiwan, that carries either the novel staphylococcal chromosome cassette mec (SCCmec) ttype VT or SCCmec type IV. J Clin Microbiol. 2005;43(9):4719–4730. doi:10.1128/JCM.43.9.4719-4730.2005
11. DeLeo FR, Chambers HF. Reemergence of antibiotic-resistant Staphylococcus aureus in the genomics era. J Clin Invest. 2009;119(9):2464–2474. doi:10.1172/JCI38226
12. Liu JL, Li TM, Zhong N, et al. Current status of oxacillin-susceptible mecA-positive Staphylococcus aureus infection in Shanghai, China: a multicenter study. J Microbiol Immunol Infect. 2021;54(6):1070–1077. doi:10.1016/j.jmii.2020.07.021
13. Chen CJ, Su LH, Chiu CH, et al. Clinical features and molecular characteristics of invasive community-acquired methicillin-resistant Staphylococcus aureus infections in Taiwanese children. Diagn Microbiol Infect Dis. 2007;59(3):287–293. doi:10.1016/j.diagmicrobio.2007.05.015
14. Liao CH, Chen SY, Chang SC, et al. Characteristics of community-acquired and health care-associated Staphylococcus aureus bacteremia in patients treated at the emergency department of a teaching hospital. Diagn Microbiol Infect Dis. 2005;53(2):85–92. doi:10.1016/j.diagmicrobio.2005.06.009
15. Seybold U, Kourbatova EV, Johnson JG, et al. Emergence of community-associated methicillin-resistant Staphylococcus aureus USA300 genotype as a major cause of health care-associated blood stream infections. Clin Infect Dis. 2006;42(5):647–656. doi:10.1086/499815
16. Junkins AD, Arbefeville SS, Howard WJ, et al. Comparison of BD Phoenix AP Workflow with Vitek 2. J Clin Microbiol. 2010;48(5):1929–1931. doi:10.1128/JCM.00111-10
17. Ligozzi M, Bernini C, Bonora MG, et al. Evaluation of the VITEK 2 system for identification and antimicrobial susceptibility testing of medically relevant gram-positive cocci. J Clin Microbiol. 2002;40(5):1681–1686. doi:10.1128/JCM.40.5.1681-1686.2002
18. Enright MC, Robinson DA, Randle G, et al. The evolutionary history of methicillin-resistant Staphylococcus aureus (MRSA). Proc Natl Acad Sci U S A. 2002;99(11):7687–7692. doi:10.1073/pnas.122108599
19. Fahr AM, Eigner U, Armbrust M, et al. Two-center collaborative evaluation of the performance of the BD Phoenix automated microbiology system for identification and antimicrobial susceptibility testing of Enterococcus spp. and Staphylococcus spp. J Clin Microbiol. 2003;41(3):1135–1142. doi:10.1128/JCM.41.3.1135-1142.2003
20. Ma M, Chu M, Tao L, et al. First report of oxacillin susceptible meca -positive staphylococcus aureus in a children’s hospital in Kunming, China. Infect Drug Resist. 2021;14:2597–2606. doi:10.2147/IDR.S317670
21. Taiwan Centers for Disease Control (TCDC). Antimicrobial resistance surveillance annual report, Taiwan; 2021. Available from: http://www.cdc.gov.tw.
22. Chen CH, Wu PH, Lu MC, Ho M-W, Hsueh P-R; for SPS Group. National surveillance of antimicrobial susceptibilities to ceftaroline, dalbavancin, telavancin, tedizolid, eravacycline, omadacycline, and other comparator antibiotics, and genetic characteristics of bacteremic Staphylococcus aureus isolates in adults: results from the Surveillance of Multicenter Antimicrobial Resistance in Taiwan (SMART) program in 2020. Int J Antimicrob Agents. 2023;61(4):106745. doi:10.1016/j.ijantimicag.2023.106745
23. Wang WY, Chiu CF, Lee YT, et al. Molecular epidemiology and phenotypes of invasive methicillin-resistant vancomycin-intermediate Staphylococcus aureus in Taiwan. J Microbiol Immunol Infect. 2022;55(6 Pt 2):1203–1210. doi:10.1016/j.jmii.2021.09.003
24. McDougal LK, Thornsberry C. The role of β-lactamase in staphylococcal resistance to penicillinase-resistant penicillins and cephalosporins. J Clin Microbiol. 1986;23(5):832–839. doi:10.1128/jcm.23.5.832-839.1986
25. Nadarajah J, Lee MJS, Louie L, et al. Identification of different clonal complexes and diverse amino acid substitutions in penicillin-binding protein 2 (PBP2) associated with borderline oxacillin resistance in Canadian Staphylococcus aureus isolates. J Med Microbiol. 2006;55(Pt 12):1675–1683. doi:10.1099/jmm.0.46700-0
26. Keseru JS, Gál Z, Barabás G, et al. Investigation of β-Lactamases in clinical isolates of staphylococcus aureus for further explanation of borderline methicillin resistance. Chemotherapy. 2005;51(6):300–304. doi:10.1159/000088951
27. Skinner S, Murray M, Walus T, et al. Failure of cloxacillin in treatment of a patient with borderline oxacillin-resistant staphylococcus aureus endocarditis. J Clin Microbiol. 2009;47(3):859–861. doi:10.1128/JCM.00571-08
28. Szumlanski T, Neumann B, Bertram R, et al. Characterization of PVL-positive MRSA isolates in Northern Bavaria, Germany over an eight-year period. Microorganisms. 2022;11(1):54. doi:10.3390/microorganisms11010054
29. Liu R, Zhang J, Du X, et al. Clonal diversity, low-level and heterogeneous oxacillin resistance of oxacillin sensitive MRSA. Infect Drug Resist. 2021;14:661–669. doi:10.2147/IDR.S288991
30. Chen FJ, Wang CH, Chen CY, et al. Role of the mecA gene in oxacillin resistance in a Staphylococcus aureus clinical strain with a pvl -positive ST59 genetic background. Antimicrob Agents Chemother. 2014;58(2):1047–1054. doi:10.1128/AAC.02045-13
31. Chen FJ, Huang IW, Wang CH, et al. mecA-positive Staphylococcus aureus with low-level oxacillin MIC in Taiwan. J Clin Microbiol. 2012;50(5):1679–1683. doi:10.1128/JCM.06711-11
32. Pardo L, Giudice G, Mota MI, et al. Phenotypic and genotypic characterization of oxacillin-susceptible and mecA positive Staphylococcus aureus strains isolated in Uruguay. Rev Argent Microbiol. 2022;54(4):293–298. doi:10.1016/j.ram.2022.05.004
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.