")
Back to Journals » Research and Reviews in Parkinsonism » Volume 9
Communication gaps about OFF periods between physicians and patients with Parkinson’s disease: a patient–physician dialogue analysis
Authors Levit AV, Zebendon C, Walter L, O’Donnell P, Marras C
Received 27 September 2018
Accepted for publication 21 February 2019
Published 30 April 2019 Volume 2019:9 Pages 3—8
DOI https://doi.org/10.2147/JPRLS.S188923
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Peter Hedera
Anna V Levit,1 Cheryl Zebendon,1 Lauren Walter,2 Patricia O’Donnell,2 Connie Marras3
1Acorda Therapeutics, Inc., Ardsley, NY, USA; 2Verilogue, Inc., Horsham, PA, USA; 3The Edmond J Safra Program in Parkinson’s Research, University Health Network, Toronto Western Hospital, Toronto, ON, Canada
Background: As Parkinson’s disease (PD) progresses, patients may experience the return of PD symptoms (OFF periods) despite treatment. Recognizing and treating OFF periods requires effective communication between physicians and patients.
Methods: A linguistic analysis investigated communication gaps between patients and physicians using a database containing dialogues recorded during regular office visits. Follow-up interviews were conducted with selected physicians, patients, and caregivers.
Results: Four areas were identified showing communication gaps between patients and physicians: differences in language; patient knowledge about OFF periods; differences in approach to describing OFF periods; and attitude toward management of OFF periods.
Conclusion: Closing communication gaps may improve overall PD management.
Keywords: Parkinson’s disease, communication, motor fluctuations, clinical practice, OFF period
Plain language summary
A language analysis study was done to evaluate the quality of communication between patients with Parkinson’s disease (PD) and their doctors about times when PD medication works less well. These times are called OFF periods. OFF periods are upsetting to patients and difficult to cope with because patients become less able to manage ordinary daily activities. This study was conducted to identify areas where communication gaps about OFF periods between patients and their doctors exist. These gaps may prevent patients with PD from receiving the necessary help from their doctors for treatment of OFF periods. Researchers recorded office-visit conversations between patients with PD and their doctors over several months (with permission) to evaluate language and conversation patterns to determine if and where patient-physician communication gaps existed. Four areas were identified showing communication gaps between patients and physicians: differences in language; patient knowledge about OFF periods; differences in approach to describing OFF periods; and attitude toward management of OFF periods. These gaps are likely to interfere with ability of patients to receive the most suitable treatment.
Introduction
Dopaminergic drugs are the cornerstone of managing symptoms associated with Parkinson’s disease (PD).1 Despite treatment, many patients begin to experience motor fluctuations as the disease progresses. Motor fluctuations are alternating periods during the day when symptoms are controlled (known as ON periods) and times when symptoms return (OFF periods).2 As PD progresses, the proportion of patients who experience OFF periods increases.3 OFF periods can include an array of motor and nonmotor symptoms,2,4–6 and a number of treatment strategies exist for reducing the symptoms experienced during OFF periods.7 There is evidence suggesting, however, that identification of OFF periods is impeded by lack of patient education, awareness, patient–physician miscommunication, and limited time for assessment.5,8–10 Optimizing patient–physician communication is important because identification and management of OFF periods can improve patient functioning.
In this study, linguistic and thematic analysis of collected information was performed to identify communication gaps that occurred between patients with PD and their physicians when discussing OFF symptoms and their management during office visits.
Methods
This was a 2-part study involving linguistic analysis of pre-recorded dialogues from an existing database, followed by telephone interviews with a subset of participants identified as having spoken specifically about OFF periods. Recorded exam-room conversations were selected from the research database (Verilogue, Inc., Horsham, PA, USA; Data supporting reported results available at:
6–12 months after the initial recorded office visits, follow-up telephone interviews by Verilogue staff were conducted with physicians, patients, and caregivers. These follow-up interviews focused on perceptions of “typical” OFF period discussions and contained probes specific to the actual recorded office dialogue. To facilitate this process, respondents were provided with a transcript of their office-visit dialogue in advance of the follow-up interview (Figure 1). Probes to physicians focused on the main challenges in managing a specific patient’s PD as well as general attitudinal questions about physicians’ typical probing into OFF periods, experience of letting patients adjust their own medication regimen, patients’ general knowledge about PD and OFF periods specifically, and their information-seeking behavior. Probes to patients focused on how well they are able to understand their physician’s questions and instructions, how they feel during OFF periods, and what they wish other people understood about living with PD.
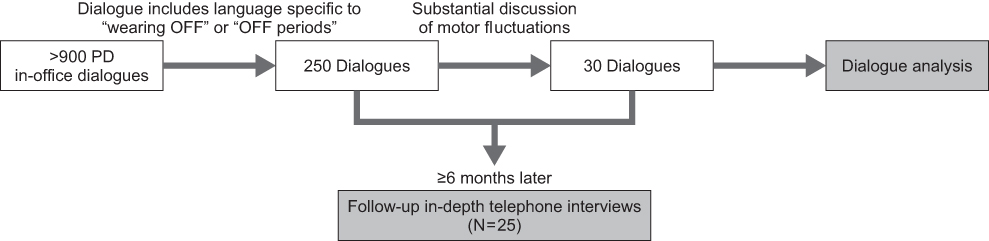 | Figure 1 Selection of office dialogues. Abbreviation: PD, Parkinson’s disease. |
New England Independent Review Board (Needham Heights, MA, USA) reviewed all study materials for both parts of the study and granted protocol exemptions in June 2016. The linguistic analysis of recorded in-office patient–physician conversations was exempted as it was research involving the collection or study of existing data, documents, records, pathological specimens, or diagnostic specimens, and the investigator recorded the information in such a manner that subjects could not be identified, directly or through identifiers linked to the subjects. For the follow-up telephone interviews with patients and physicians, it was exempted as it was research involving the use of educational tests (cognitive, diagnostic, aptitude, achievement), survey procedures, interview procedures or observation of public behavior, and the information obtained was not recorded such that subjects could be identified, directly or through identifiers linked to the subjects; and any disclosure of the human subjects’ responses outside the research could not reasonably place the subjects at risk of criminal or civil liability or be damaging to the subjects’ financial standing, employability, or reputation.
Results
The 30 analyzed dialogues consisted of conversations between 14 unique physicians (9 neurologists and 5 movement disorder specialists) and 29 unique patients with PD. For 17 of these dialogues, a caregiver was also present. One patient was recorded in two office visits with the same physician. In this case, the patient’s caregiver was not present at the first office visit, but was present at the second visit, and the conversations were different in a meaningful way due to the caregiver’s participation. Patient characteristics are shown in Table 1.
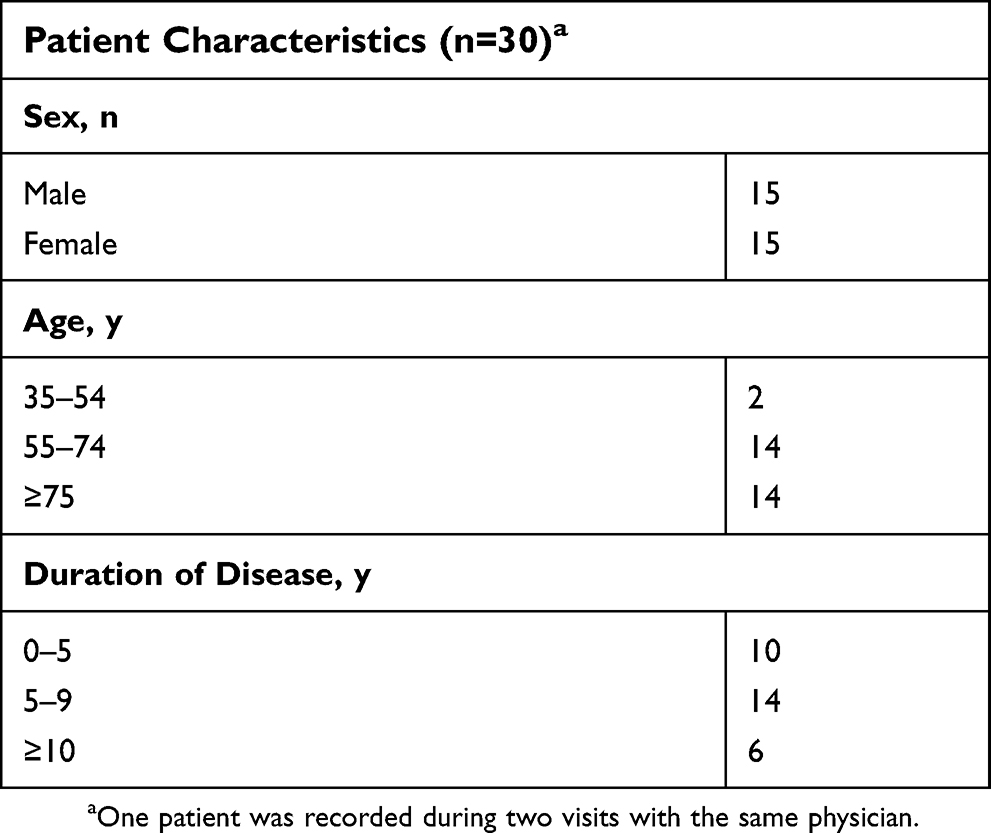 | Table 1 Patient characteristics for the recorded dialogues |
There were 25 follow-up telephone interviews with 15 physicians (10 neurologists, 5 movement disorder specialists) and 11 people impacted by PD: 7 patients, 2 caregivers, and 1 patient–caregiver pair (counted as 2) interviewed together. For the follow-up telephone interviews, most of those interviewed had been recorded in the 30 previously analyzed dialogues (13 of 15 physicians and 6 of 11 patients and caregivers).
Dialogue analysis and telephone interviews identified four main areas where patients and physicians were not aligned as to perception and understanding of OFF periods: 1) differences in language; 2) patient knowledge about OFF periods; 3) differences in approach to describing OFF periods; and 4) attitude toward management of OFF periods.
Differences in language
The lack of specific terminology to describe OFF periods was a barrier to effective communication. Physicians used a lexicon that focused on the timing and pattern of OFF symptoms, whereas patients used anecdotal life narratives to describe the unpredictability of OFF symptoms and the impact of symptoms on their lives. For example, physicians used episodic language using “time,” “days,” “morning,” “commonly,” “frequently,” and “sometimes” in queries to focus on timing and pattern of OFF symptoms. They also used motion metaphors to describe motor fluctuations such as: “up/down,” “freeze/frozen,” “hold,” “stop/go,” and “on/off.” Patients and caregivers reported they lack a term for OFF periods and used words and expressions such as “leak,” or “having a weird feeling.” Only 3 of 29 patients, and no caregivers, used the term “wearing OFF.”
Patient knowledge about OFF periods
Patients had different levels of understanding of disease symptoms and progression, and physicians did not ask questions in a way that connected patients’ experiences with OFF periods. Typically, physicians’ questions about symptom fluctuations were asked in the context of the patient’s medication regimen, such as how often patients took their medication (“What medication and dose are you taking?”) and when during the day they experienced more symptoms (“How often and at what time?”). Many patients did not understand why physicians were asking these questions, and some patients completely misunderstood the questions as relating to whether they were compliant with their medication instructions. Physicians also reported that patients are often unaware of PD symptom progression and did not have appropriate expectations (efficacy and time to effect) for their medication. Most physicians believe that patients need to be educated about OFF periods before they can recognize them, and most said they encourage patients to research outside of the office. Although most physicians said they provide clear education to patients about OFF periods in the interviews, patients did not report this, and only 2 out of 30 dialogues actually included any conversation about why OFF periods occur and how to manage them. Most patients were open to further education (specifically support groups), community awareness (“a lot of people don’t understand it [PD]”), and information about the long-term impact of the disease.
Differences in approach to describing OFF periods
When physicians asked how patients were doing, many patients replied by citing periods when symptoms were worse compared with other times, and these were usually described in the context of activities they could not do. Examples include: “Getting up sometimes is unreal…I mean just to stand up, takes effort…;” “[I] can’t even shave;” “I’m walking slower;” and “I can’t get out of my chair.” Patients reported OFF symptoms through anecdotal life narratives to describe the impact of symptoms on their lives, without describing specific symptoms, using such phrases as, “I like to walk, but I’m afraid to get too far from the house…I won’t get back…” or personal narratives, “I was standing at the kitchen sink doing something. All of a sudden, [I feel] very, very weak.” Physicians used terms such as “stiffness,” “weakness,” “tremor,” and “falling,” and concentrated only on whether OFF periods occurred, but did not probe regarding the intensity or impact of the OFF periods on their patients’ activities. Most patients described nonmotor symptoms, such as “not remembering how to do anything complicated,” confusion, anxiety, drooling, and “brain fog” in their interviews, whereas less than half of the interviewed physicians mentioned nonmotor symptoms at all.
Attitude toward management of OFF periods
Patients tended to perceive that OFF periods were an inescapable part of disease progression or did not realize the importance of communicating OFF periods. An interviewed physician stated, “[Patients] don’t want to think that the disease is getting the better of them, so they don’t mention the problems they’re having.” Many of the physicians commented during the office clinical encounter that a change in medication might help with OFF periods, but rarely explained why a treatment change might help, or why OFF periods occur. Typically, physicians discussed only short-term expectations for treatment, and they tended to plan visit-to-visit. Although most physicians said they ask patients about their symptoms and relate them to the dosing schedule, dialogue analysis indicated that these exchanges were often incomplete. In the dialogues, for example, many physicians asked patients about both symptoms and dosing times but did not make a conversational connection between the two.
The telephone interviews also widely reported that poor patient cognition and impaired speaking ability due to the disease were other factors that compromised communication. Caregivers play an important role in this regard, by acting as interpreters between patients and physicians during office visits, by reporting symptoms that patients may be unable to recognize or report, and by reinforcing the legitimacy of patients’ concerns.
Discussion
In this qualitative dialogue analysis, patients and physicians had different perspectives of OFF periods, leading to gaps in communication during a typical office visit. Physicians, patients, and caregivers were often not aligned in their perceptions of OFF periods. Physicians believed they provided education about OFF periods during office visits, but the dialogues and interviews showed that any education they provided was incomplete, poorly detailed, and often absent.
In a survey of 47 matched pairs of patients and caregivers in the UK (OFF-PARK Survey), 87% of patients and 74% of caregivers reported that they understood when their physician talked about “wearing OFF,” but when asked what it meant, 53% of patients and 36% of caregivers did not answer, and 17% and 47% of patients and caregivers, respectively, gave an incorrect answer.5 Our study suggests that part of the problem is that patients and physicians have different lexicons and that many patients are not well informed about OFF periods. Given that physicians appear not to discuss “wearing OFF” and OFF periods with patients and their caregivers in ways that they understand, it is perhaps not surprising that often patients and caregivers are not able to satisfactorily define these terms.
Another interesting point raised by the OFF-PARK survey is that about 85% of patients reported that they discussed their quality of life with their physician.5 In contrast, in our study, while patients and caregivers generally explained the impact of their symptoms on their daily life to the physician, physicians seemed to concentrate on the symptoms alone, and were not, in the patients’ opinion, absorbing what they had to say about the impact on their daily lives, which reinforces our conclusion that the two parties may have different priorities.
Other studies have suggested that physicians may need to ask more probing questions to determine if patients are experiencing OFF periods,11–13 and that patients may not be aware that troubling symptoms could be due to OFF periods.8 In our study, the manner in which physicians asked questions to assess “wearing OFF” often seemed to cause patient misunderstanding, suggesting that physicians need to be clearer. With an average consultation from this study lasting less than 10 mins, time for patient–physician interaction is limited, and it is not surprising that there are few substantial discussions of OFF periods, given what else needs to be covered during a visit.
Limitations
This study used a small, self-selecting sample population in the United States that may not be representative of physicians and patients as a whole. However, we have no reason to believe that the communication skills of this sample of physicians and patients, who were willing to be recorded, are worse than average. Also, the follow-up interviews were completed 6–12 months after the actual encounter, and participants’ recall likely relied heavily on reading of the transcripts rather than their memory of the in-office conversation.
Conclusion
To summarize, this study provides important insights into issues in physician–patient–caregiver communication about OFF periods in PD. Effective patient–physician communication and improved patient education are expected to help improve OFF-period treatment and overall PD management, so it is important for these gaps to be closed.5
Acknowledgments
This study was supported by Acorda Therapeutics, Inc. Editorial assistance was provided by The Curry Rockefeller Group, LLC, which was funded by Acorda Therapeutics, Inc. The abstract of this paper was presented at the American Academy of Neurology. Annual Meeting in Boston, MA, 22–28 April 2017. Squillacote D, Levit A, Walter L, Hedrick M-K, Marras C. Communication gaps on OFF periods in Parkinson’s disease: A linguistic patient-physician dialogue analysis (P6.015). Neurology. 2017;88 (16 Supplement):P6.015. Available:
Author contributions
AL, CZ, CM: conception and design. LW, POD: data acquisition. All authors contributed to data analysis, interpretation of data, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
AL and CZ are employees and stockholders of Acorda Therapeutics, Inc. LW and POD are employees of Verilogue, Inc. CM is a consultant to Acorda Therapeutics, Inc and Pfizer Inc., and has received grants from Canadian Institutes of Health Research, Michael J. Fox Foundation, National Parkinson Foundation, Parkinson Disease Foundation, Parkinson Society Canada, Parkinson Study Group, and Physician Services Inc. The authors report no other conflicts of interest in this work.
References
1. Lewitt PA. Levodopa for the treatment of Parkinson’s disease. N Engl J Med. 2008;359(23):2468–2476. doi:10.1056/NEJMct0800326
2. Jankovic J. Motor fluctuations and dyskinesias in Parkinson’s disease: clinical manifestations. Mov Disord. 2005;20(Suppl 11):S11–S16. doi:10.1002/mds.20458
3. Ahlskog JE, Muenter MD. Frequency of levodopa-related dyskinesias and motor fluctuations as estimated from the cumulative literature. Mov Disord. 2001;16(3):448–458.
4. Caillava-Santos F, Margis R, de Mello Rieder CR. Wearing-off in Parkinson’s disease: neuropsychological differences between on and off periods. Neuropsychiatr Dis Treat. 2015;11:1175–1180. doi:10.2147/NDT.S77060
5. Matthews H, Stamford J, Saha R, Martin A. Exploring issues around wearing-off and quality of life: the OFF-PARK survey of people with Parkinson’s disease and their care partners. J Parkinsons Dis. 2015;5(3):533–539. doi:10.3233/JPD-150547
6. Olanow CW, Stern MB, Sethi K. The scientific and clinical basis for the treatment of Parkinson disease. Neurology. 2009;72(21 Suppl 4):S1–136. doi:10.1212/WNL.0b013e3181a1d44c
7. Pahwa R, Factor SA, Lyons KE, et al. Practice Parameter: treatment of Parkinson disease with motor fluctuations and dyskinesia (an evidence-based review): report of the quality standards subcommittee of the American Academy of Neurology. Neurology. 2006;66(7):983–995. doi:10.1212/01.wnl.0000215250.82576.87
8. Pahwa R, Lyons KE. Levodopa-related wearing-off in Parkinson’s disease: identification and management. Curr Med Res Opin. 2009;25(4):841–849. doi:10.1185/03007990902779319
9. Stacy M, Hauser R, Oertel W, et al. End-of-dose wearing off in Parkinson disease: a 9-question survey assessment. Clin Neuropharmacol. 2006;29(6):312–321. doi:10.1097/01.WNF.0000232277.68501.08
10. Witjas T, Kaphan E, Azulay JP, et al. Nonmotor fluctuations in Parkinson’s disease: frequent and disabling. Neurology. 2002;59(3):408–413.
11. Dodel RC, Berger K, Oertel WH. Health-related quality of life and healthcare utilisation in patients with Parkinson’s disease: impact of motor fluctuations and dyskinesias. Pharmacoeconomics. 2001;19(10):1013–1038. doi:10.2165/00019053-200119100-00004
12. Hely MA, Morris JG, Reid WG, Trafficante R. Sydney Multicenter Study of Parkinson’s disease: non-L-dopa-responsive problems dominate at 15 years. Mov Disord. 2005;20(2):190–199. doi:10.1002/mds.20324
13. Wickremaratchi MM, Ben-Shlomo Y, Morris HR. The effect of onset age on the clinical features of Parkinson’s disease. Eur J Neurol. 2009;16(4):450–456. doi:10.1111/j.1468-1331.2008.02514.x
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.