")
Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 16
Common Reasons for Permanent Tooth Extraction and Its Correlation with Demographical Factors in Kabul, Afghanistan
Authors Fayaz Y , Ahmadi NA, Ahmadi SU, Atiq MA
Received 26 November 2023
Accepted for publication 13 February 2024
Published 21 February 2024 Volume 2024:16 Pages 25—31
DOI https://doi.org/10.2147/CCIDE.S442179
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Christopher E. Okunseri
Yahya Fayaz,1 Naseer Ahmad Ahmadi,1 Shahab Uddin Ahmadi,1 Mohammad Asif Atiq2
1Department of Stomatology, Khatam Al Nabieen University, Kabul, Afghanistan; 2Department of Clinical Pharmacology, Kabul University of Medical Sciences, Kabul, Afghanistan
Correspondence: Mohammad Asif Atiq, Department of Clinical Pharmacology, Kabul University of Medical Sciences, Kabul, Afghanistan, Tel +93777378141, Email [email protected]
Objective: The aim of this survey was to investigate the main reasons for extraction of permanent teeth, and its correlation with age, gender, education level, smoking habits, and time of last dental visit, family income, and professions in Kabul, Afghanistan.
Subjects and Methods: The study proposal was approved by Research Ethics Committee of Khatam AL Nabieen and was conducted over a period of 5 months; its population consisted 594 patients, aged 10– 70 years, who underwent extraction. The frequency distribution was calculated using X2 test, ANOVA and t-test for differences in mean number of patients.
Results: A total of 594 patients underwent extraction. The highest rate (53.8%) of extraction occurred for those 21– 40 years old. Females compromised 51.3% of patients. Two hundred (33.6%) patients were uneducated. Tooth loss due to caries was 30.1%; patient-request was 18.3%; impacted teeth was 14.4%. Other causes were periodontal reasons, failed root canal therapy (RCT), Tooth mobility, and Root fractures.
Conclusion: The result of this survey indicated that caries, patient request, and impaction were the leading reasons for tooth extraction. The majority of patients were uneducated, and had insufficient family income. Most of the patients were housewives and laborers.
Keywords: Tooth Extraction, Dental Caries, Periodontal Disease
Introduction
Tooth loss remains the foremost problematic dental issue universally.1 Previous studies regarding teeth extraction have been conducted in various regions and concluded that caries, periodontal disease, trauma, orthodontic and prosthodontic treatments, endodontic treatment complications, root fracture and malposition are the main reasons for tooth loss.2–7
Numerous studies have shown that tooth decay and periodontal disease were the most common reasons for teeth extraction.7–11 Generally, the majority of the studies revealed that dental caries was the primary reason for tooth loss among 20 to 60-year-old patients. Moreover, periodontal disease was the main reason for tooth loss among patients in their late 40s and older as there was a correlation between age and periodontal disease. On the other hand, root canal treatment complications and orthodontic treatment were observed as the major reasons for tooth extraction among adolescent patients.12–14
Some studies have concluded that there is an association between tooth loss and gender, where women lose more teeth due to tooth decay while men had more teeth loss due to periodontal disease.12–14 Other reasons such as previous prosthetics and esthetic reasons, root fracture, and tooth malposition were found to have less effect on tooth loss.2–6
Only a few studies investigated the reasons for tooth extraction in Afghanistan. The study which is conducted by Safari S et al in the west of Kabul indicated that periodontal disease and caries were the principal reasons for tooth extraction.15 Similarly the study of Da’ameh D which was conducted in the north of Afghanistan reflected the extent and severity of caries and periodontal disease as the most common reasons for tooth loss.16 Therefore, this study aimed to explore the reasons for tooth extraction and investigate the correlation between tooth loss and several variables including age, gender, education level, family income, and smoking habit.
Materials and Methods
The study protocol conforms to The Code of Ethics of World Medical Association (Declaration of Helsinki) for studies involving humans. The study proposal was approved by Research Ethics Committee of Khatam AL Nabieen. Participants in the research study signed an informed consent form prior to their participation. For patients under the age of 18, the parent or legal guardian of the patients provided their informed consent.
The present study was conducted in the National Curative and Specialized Stomatology Hospital in Kabul, Afghanistan. The selection of this hospital was based on its location, and the number of patients who could be recruited into the study. Moreover, the patients of this hospital come from different provinces of Afghanistan seeking free dental treatment services.
Dentists who were in-charge in Out Patient Department in the hospital cooperated in data collection. Patients aged between 10–70 years with tooth problems, after physical examination in the OPD and with final decision of tooth extraction as their treatment plan, were included in this study. Then, data were collected from each patient including age, gender, education level, tooth extracted, reason of extraction, level of family income, profession, smoking habit, time of last dental visit, and previous extraction. The diagnosis by the in-charge dentist in the OPD was considered as the reason for tooth extraction. Data were collected over a 5-month period (July – December 2022).
The inclusion criteria was those patient who were above 10 years old and can provide informed consent to participate in the study, with final management of tooth extraction.
The collected data were entered into SPSS (version 25) software. The relationships of the categorical background variables, such as age range, gender and education level, family income, profession, smoking habit, and time of last dental visit with reasons for tooth extraction were analyzed by the X2 test, while differences in the mean number of patients were analyzed with ANOVA and t-test methods. A p-value of less than 0.05 was considered to be statistically significant.
Findings
A total of 594 patients were included in the study. Females had more teeth extracted (51.3%) than men (p > 0.05). According to Table 1, the average number of patients who had teeth extracted during the survey was 5.54 ± 1.87 (5.41 males and 5.68 females). In total, patients from 21 to 30 of age lost 8.08 teeth, more than all other groups, as measured by the mean number of patients (p < 0.05). The highest rate of extraction during the survey were among patients from 21–30 (6.41 teeth). Moreover, under-graduated patients had lost 8.18 teeth in total, which is significantly higher than in other groups (p < 0.05). Besides, patients with an insufficient family-income had more teeth extracted (74.2%) than those who had adequate earnings (p > 0.05). Although non-smoker patients had more extracted teeth (67%) than smokers, it was not significant statistically (p > 0.05). Overall, patients who had never or not more than a year visited dentists had tooth loss more (7.27 ± 2.46 and 7.14 ± 2.35 teeth, respectively) than the other group, as measured by mean number (p > 0.05). Altogether, teachers lost 7.88 teeth more than all other professional groups (p < 0.05).
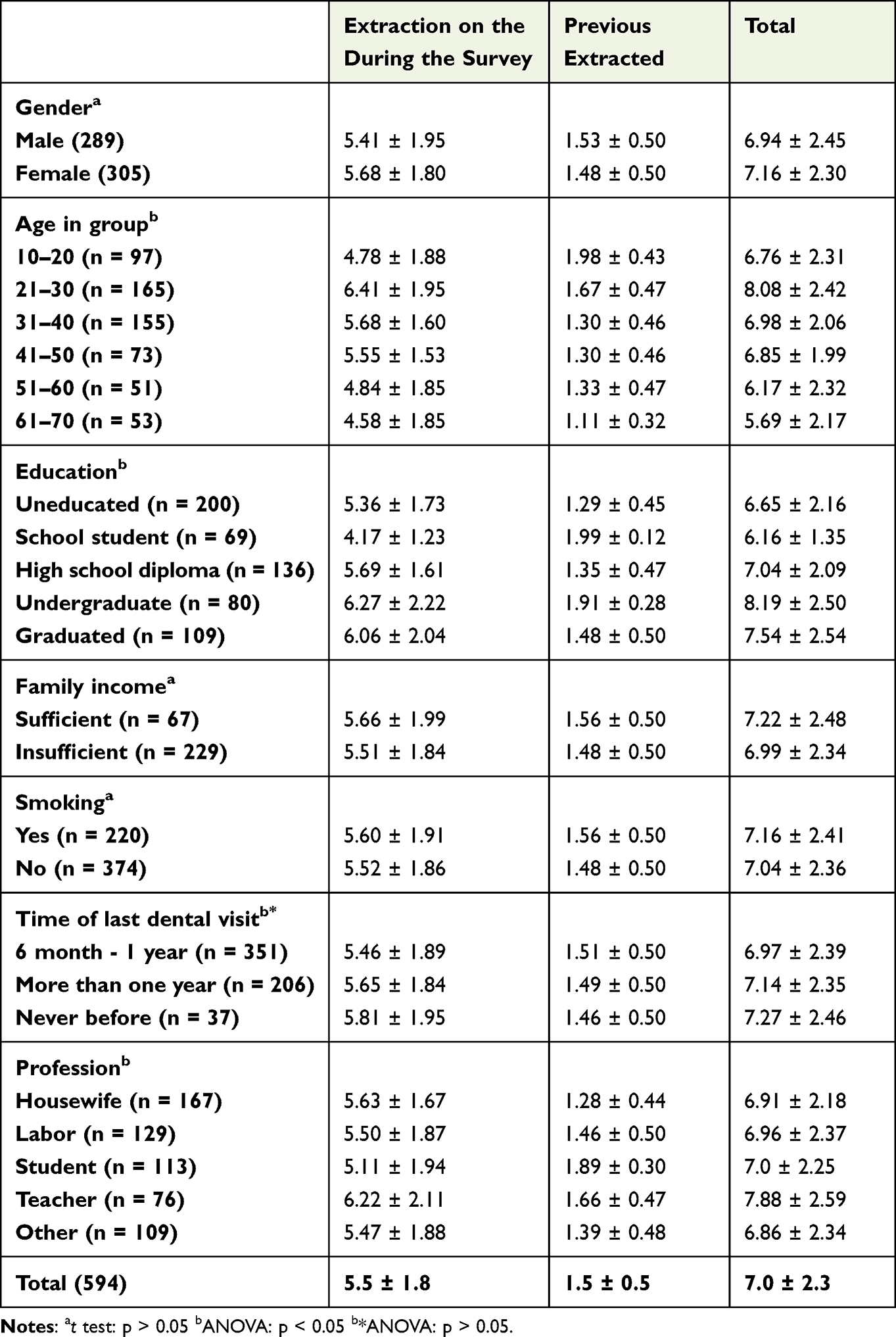 |
Table 1 Mean Number of Patients |
Dental caries was responsible for 30.1% of all extractions, while patient-request accounted for 18.3%. Nevertheless, Dental caries was responsible for most extractions in both genders, impacted teeth were more prevalent among males than females. Moreover, patient request and tooth mobility were the main causes of tooth extraction among females. While caries was the leading cause of tooth extraction among patients from 10 to 20 years and 31 to 50 of age, impacted tooth and tooth mobility were the common reasons for tooth loss in patients from 21 to 30 and above 60 years of age, respectively (Table 2). The common reason for tooth extraction among uneducated patients was patient request. On the other hand, Patients having high school diplomas and school students had lost more teeth due to caries compared with patients having a higher level of education but this was not significant statistically (p > 0.05). However, dental caries was the main cause for most tooth loss in both groups who thought to have sufficient family income and insufficient income, impacted tooth and tooth mobility were common among those who had insufficient family income (p < 0.05). Even so, dental caries was the principal reason for tooth loss among smokers and non-smokers, periodontal reasons were more prevalent among smokers than non-smokers (p < 0.05). Also, dental caries was the most prevalent cause of tooth loss among patients based on last time dental visit, but impacted tooth, periodontal reasons, failed RCT and tooth mobility were more frequent among patients whose last time dental visit was more than a year ago than others (p > 0.05). After all, the major reason for tooth loss among teachers was impacted teeth, but caries caused patient tooth extraction in all professions (p < 0.05).
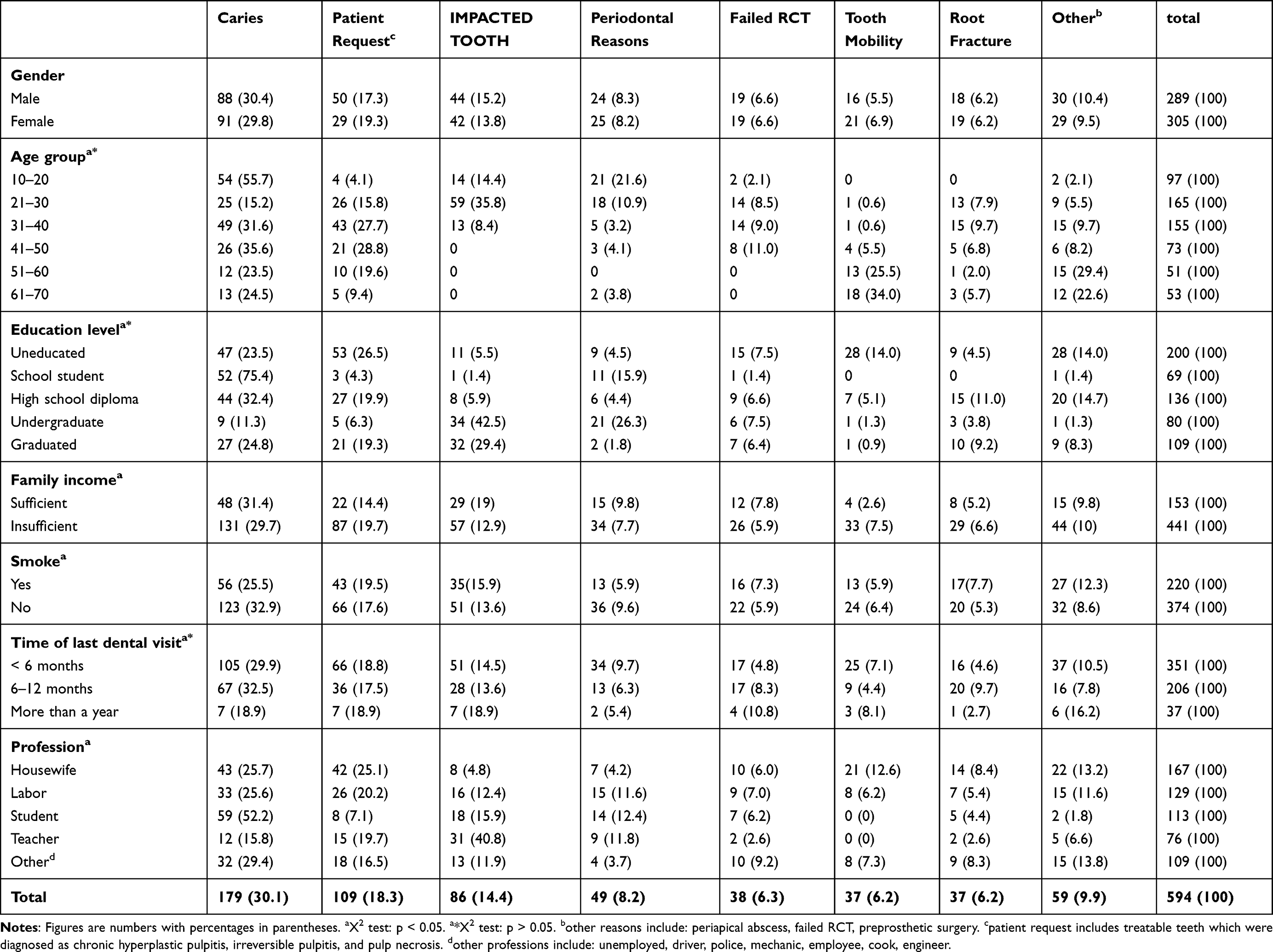 |
Table 2 Reasons for Tooth Extraction by Age, Gender, Education Level, Family Income, Smoke, Time of Last Dental Visit and Profession |
The most frequently extracted teeth were first and second molars (109, 18.3%), followed by upper first and second molars (106, 17.8%), while lower incisors and canine were least frequently extracted (16, 2.6%). Impaction was the main cause of the loss of upper and lower third molars (Table 3). Premolars of both jaws were the most frequently extracted teeth due to dental caries. Additionally, periodontal disease was the main cause of the loss of all incisors and canines (p < 0.05).
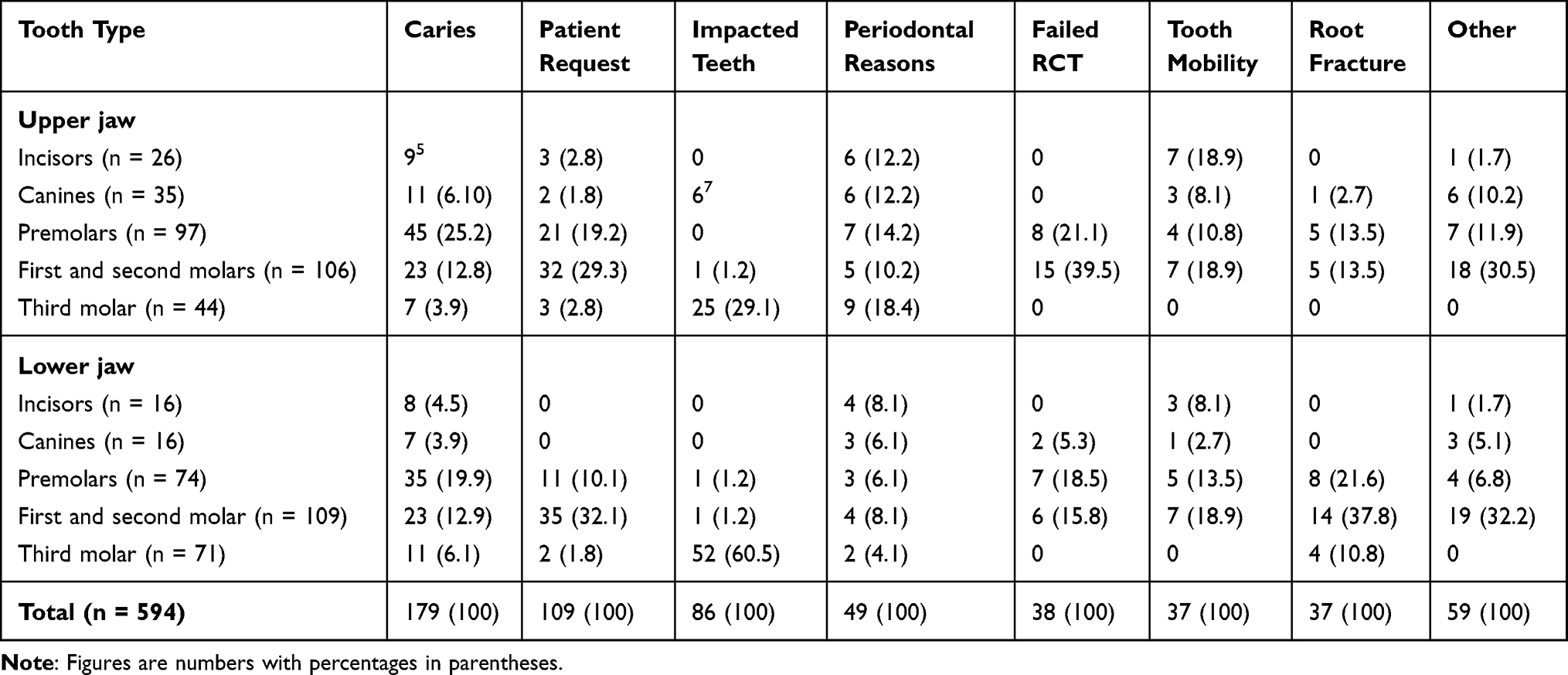 |
Table 3 Reasons for Extraction by Tooth Type, Number (%) |
Discussion
The results of this survey indicated that in Kabul, Afghanistan, dental caries were the leading reason for extraction. Patient-request was the next most common reason. The finding that caries was the most common cause is consistent with the majority of similar studies.6,7,16–20 Surveys in Japan,21 Italy,22 and Singapore23 indicated that both caries and periodontal disease were almost equally important reasons for tooth loss. Studies in Canada,13,24 Jordan,25 and west of Kabul15 showed that the main cause of tooth loss was periodontal disease. West Kabul15 had a lower percentage of dental caries compared to our study and the earlier study.16 This difference may be attributed to diet, and socio-economic factors because the study in the west of Kabul was conducted in private clinics and the present study and the study in north Afghanistan were conducted in a governmental sector where people seek free dental treatment services.
In the present study, most patients whose teeth were extracted were 21–40 years old, while extraction in elderly patients (over 60) accounted for 8.9% of all tooth loss. While 83.7% of teeth extracted for tooth mobility were in patients over 50 years of age, caries was the main reason for extraction in patients from 10–20 and 31–40 years of age and impacted teeth in patients aged 21 to 30 years old. This result was also reported by Chrysanthakopoulos NA.10 However, our study, as previously mentioned, is not in agreement with studies where caries was the principle cause of extraction in patients over 50 years old.9,26
Periodontal disease was the main cause of tooth loss in incisors in our study which is similar to the findings of Cobet E,20 Angelillo IF,22 and Morita M27 and teeth extracted for orthodontic reasons were mainly first and second molars17,22 which was patient request in our study. A likely reason for the high periodontal extraction in anterior teeth is that they are less susceptible to dental caries, retained longer in the mouth, and then may be subjected to periodontal disease risks.7,10,23,28
Overall, the highest number of extractions were in uneducated patients and the reason was patient-request in the present study, but in the study of Dena A the majority of extractions were in middle and high school groups where the reason was caries.26 The overriding reasons for extraction was caries in different levels of education26 which was caries in school student, high school diplomas, and uneducated patients, and impaction in graduated and under-graduated students in this study. According to our findings, the number of extractions was higher in smoker patients than in non-smokers which was in accordance with the result of Dena A’s study.26
Not all patients have regular dental visits, which are essential to diagnose dental caries at its early stage in order to prevent and decrease tooth extraction. Moreover, many patients had their teeth extracted at their request, which is uncommon. Hence, it is an urgent need to have some programs to increase oral health/hygiene awareness among people. Further studies are recommended to be carried out in other provinces to use their results in planning for developing oral health in Afghanistan.
Despite, this study offers valuable insights into common reasons for tooth extraction among Afghans, the potential limitations include sample size and being single-center may not support broad generalizations.
Conclusion
The result of this survey indicated that caries, patient request, and impaction were the leading reasons for tooth extraction. The majority of patients were uneducated, and had insufficient family income. Most of the patients were housewives and laborers.
Funding
No funding Was Received for This Study.
Disclosure
The authors declare that they have no conflicts of interest related to this research.
References
1. Gerritsen AE, Allen PF, Witter DJ, Bronkhorst EM, Creugers NH. Tooth loss and oral health-related quality of life: a systematic review and meta-analysis. Health Qual Life Outcomes. 2010;8(1):1. doi:10.1186/1477-7525-8-126
2. Passarelli PC, Lajolo C, Pasquantonio G, et al. Influence of mandibular third molar surgical extraction on the periodontal status of adjacent second molars. J Periodontol. 2019;90(8):847–855. doi:10.1002/JPER.18-0415
3. Lee CY, Chang YY, Shieh TY, Chang CS. Reasons for permanent tooth extractions in Taiwan. Asia Pac J Public Health. 2015;27(2):NP2350–NP2357. doi:10.1177/1010539512448814
4. McCaul LK, Jenkins WM, Kay EJ. The reasons for extraction of permanent teeth in Scotland: a 15-year follow-up study. Br. Dent. J. 2001;190(12):658–662. doi:10.1038/sj.bdj.4801068a
5. Richards W, Ameen J, Coll AM, Higgs G. Reasons for tooth extraction in four general dental practices in South Wales. Br. Dent. J. 2005;198(5):275–278. doi:10.1038/sj.bdj.4812119
6. Jovino-Silveira RC, de França Caldas Jünior A, de Souza EH, Gusmão ES, Caldas AD. Primary reason for tooth extraction in a Brazilian adult population. Oral Health Prev Dent. 2005;3(3):567.
7. Al-Shammari KF, Al-Ansari JM, Al-Melh MA, Al-Khabbaz AK. Reasons for tooth extraction in Kuwait. Med Princ Pract. 2006;15(6):417–422. doi:10.1159/000095486
8. Passarelli PC, Pagnoni S, Piccirillo GB, et al. Reasons for tooth extractions and related risk factors in adult patients: a cohort study. Int J Environ Res Public Health. 2020;17(7):2575. doi:10.3390/ijerph17072575
9. Jafarian M, Etebarian A. Reasons for extraction of permanent teeth in general dental practices in Tehran, Iran. Med Princ Pract. 2013;22(3):239–244. doi:10.1159/000345979
10. Chrysanthakopoulos NA. Reasons for extraction of permanent teeth in Greece: a five-year follow-up study. Int Dental J. 2011;61(1):19–24. doi:10.1111/j.1875-595X.2011.00004.x
11. Aida J, Morita M, Akhter R, Aoyama H, Masui M, Ando Y. Relationships between patient characteristics and reasons for tooth extraction in Japan. Community Dent Health. 2009;26(2):104.
12. Ong G. Periodontal reasons for tooth loss in an Asian population. J Clin Periodontol. 1996;23(4):307–309. doi:10.1111/j.1600-051X.1996.tb00550.x
13. Matthews DC, Smith CG, Hanscom SL. Tooth loss in periodontal patients. J-Can Dental Assoc. 2001;67(4):207–210.
14. Stadler AF, Mendez M, Oppermann RV, Gomes SC. Tooth loss in patients under periodontal maintenance in a private practice: a retrospective study. Brazilian Dental J. 2017;28(4):440–446. doi:10.1590/0103-6440201701476
15. Safari S, Mohebi MM, Nazhand NA, Mazaher N. Reasons for Permanent Tooth Extraction in the West of Kabul. J Biosci Med. 2020;8(5):54–63. doi:10.4236/jbm.2020.85006
16. Da’ameh DA. Reasons for permanent tooth extraction in the North of Afghanistan. J Dent. 2006;34(1):48–51. doi:10.1016/j.jdent.2005.02.009
17. Agerholm DM, Sidi AD. Reasons given for extraction of permanent teeth by general dental practitioners in England and Wales. Br. Dent. J. 1988;164(11):345–348. doi:10.1038/sj.bdj.4806451
18. Chen S-C, Chueh L-H, Hsiao CK, Wu H-P, Chiang C-P. First untoward events and reasons for tooth extraction after nonsurgical endodontic treatment in Taiwan. J endodontics. 2008;34(6):671–674. doi:10.1016/j.joen.2008.03.016
19. Chestnutt I, Binnie V, Taylor M. Reasons for tooth extraction in Scotland. J Dent. 2000;28(4):295–297. doi:10.1016/S0300-5712(99)00069-X
20. Corbet E, Davies W. Reasons given for tooth extraction in Hong Kong. Community Dent Health. 1991;8(2):121–130.
21. Aida J, Ando Y, Akhter R, Aoyama H, Masui M, Morita M. Reasons for permanent tooth extractions in Japan. J Epidemiol. 2006;16(5):214–219. doi:10.2188/jea.16.214
22. Angelillo IF, Nobile CG, Pavia M. Survey of reasons for extraction of permanent teeth in Italy. Comm Dentist Oral Epidemiol. 1996;24(5):336–340. doi:10.1111/j.1600-0528.1996.tb00872.x
23. Ong G, Yeo JF, Bhole S. A survey of reasons for extraction of permanent teeth in Singapore. Comm Dentist Oral Epidemiol. 1996;24(2):124–127. doi:10.1111/j.1600-0528.1996.tb00828.x
24. Murray H, Locker D, Kay E. Patterns of and reasons for tooth extractions in general dental practice in Ontario, Canada. Comm Dentist Oral Epidemiol. 1996;24(3):196–200. doi:10.1111/j.1600-0528.1996.tb00841.x
25. Haddad I, Haddadin K, Jebrin S, Ma’ani M, Yassin O. Reasons for extraction of permanent teeth in Jordan. Int Dental J. 1999;49(6):343–346. doi:10.1111/j.1875-595X.1999.tb00535.x
26. Ali D. Reasons for extraction of permanent teeth in a university dental clinic setting. Clin Cosmetic Invest Dentistry. 2021;Volume 13:51–57. doi:10.2147/CCIDE.S294796
27. Morita M, Kimura T, Kanegae M, Ishikawa A, Watanabe T. Reasons for extraction of permanent teeth in Japan. Comm Dentist Oral Epidemiol. 1994;22(5PT1):303–306. doi:10.1111/j.1600-0528.1994.tb02056.x
28. Kay EJ, Blinkhorn AS. The reasons underlying the extraction of teeth in Scotland. Br Dent J. 1986;160(8):287–290. doi:10.1038/sj.bdj.4805837
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.