")
Back to Journals » Local and Regional Anesthesia » Volume 17
Combined Supra-Inguinal Fascia Iliaca, Sciatic Nerve, and Posterior Femoral Cutaneous Nerve Blocks in Austere Settings for Hemodynamically Unstable Patients with Vascular Injuries from Weapon Wounds: A Case Series
Authors Shabani M , Beye SA , Traore A, Raingeval X, Coulibaly D , Crespo S
Received 19 December 2023
Accepted for publication 22 February 2024
Published 2 March 2024 Volume 2024:17 Pages 19—27
DOI https://doi.org/10.2147/LRA.S452367
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Stefan Wirz
Majaliwa Shabani,1,* Seydina Alioune Beye,2,* Abdoulaye Traore,3,* Xavier Raingeval,4,* Daouda Coulibaly,5,* Sophie Crespo6,*
1Health_Unit, International Committee of the Red Cross, Bamako, Mali; 2Anesthesia Department, Clinique Périnatale Mohamed VI, Bamako, Mali; 3Anesthesia Department, Hôpital Somine Dolo de Mopti, Mopti, Mali; 4Association de Développement et de Recherche en Anesthésie Locorégionale Echoguidée, Paris, France; 5Surgery Department, Centre de Santé de Référence de Kidal, Kidal, Mali; 6Health Unit, International Committee of the Red Cross, Geneva, Switzerland
*These authors contributed equally to this work
Correspondence: Majaliwa Shabani, Health Unit, International Committee of Red Cross (ICRC), Rue 239, Hamdallaye /ACI2000 – B.P. 58, Bamako, Mali, Email [email protected]
Purpose: The management of unstable patients with weapon-wounded lower limb vascular injuries presents significant anesthetic challenges. Regional anesthesia blocks, which combine lumbar and sacral plexus blocks, or their respective branches, minimize systemic effects and are deemed appropriate for high-risk patients requiring lower limb surgery. This case series aims to share our preliminary experiences with a combined anesthetic technique—sciatic nerve (SN), posterior femoral cutaneous nerve (PFCN), and supra-inguinal fascia iliaca (SIFI) blocks —in patients sustaining weapon wounds and undergoing lower limb vascular injury repair in austere environments.
Patients and Methods: Seven patients with lower limb vascular injuries resulting from weapons who required surgery at district hospitals supported by the International Committee of the Red Cross were included in this study. Included patients underwent surgery for vascular repair and debridement using a combined nerve block technique involving the SN, PFCN, and SIFI blocks between May and December 2023. The blocks were administered using a 1:1 mixture of 1% lidocaine and 0.5% levobupivacaine.
Results: The combined block technique for the Sciatic Nerve (SN), Posterior Femoral Cutaneous Nerve (PFCN), and the Supra-Inguinal Fascia Iliaca (SIFI) were performed without complications in all patients. Three of the patients received light sedation prior to the initiation of the block procedure. All surgeries were completed successfully without the need for additional analgesics or conversion to general anesthesia.
Conclusion: The combined block technique for the Sciatic Nerve (SN), Posterior Femoral Cutaneous Nerve (PFCN), and the Supra-Inguinal Fascia Iliaca (SIFI) appears to be a safe anesthetic option for unstable or high-risk patients requiring lower limb surgery. Further research with a larger cohort is necessary to validate our findings and to potentially standardize this approach.
Keywords: war surgery, posterior femoral cutaneous nerve block, anesthesia in austere environments
Introduction
In conflict zones, managing vascular injuries, which range from 2% to 5% of all injuries, presents substantial challenges across surgery, anesthesia, and intensive care due to the urgent need to restore arterial blood flow. Delays can critically escalate the risk of limb loss despite surgical efforts. Factors exacerbating morbidity and mortality include delayed evacuation, diagnosis, and treatment; insufficiently trained personnel; and inadequate equipment.1–5
In austere, resource-limited settings, the management of vascular repairs in hemodynamically unstable patients with weapon wounds is particularly complex, affecting anesthesia choices and requiring careful consideration of patient stability, safety of the technique, environmental constraints, and the specifics of the surgery.1,2
Recent medical literature has highlighted advanced regional anesthesia techniques suitable for patients at high surgical risk undergoing lower extremity procedures. These techniques often involve a combination of supra-inguinal fascia iliaca (SIFI) blocks or lumbar plexus blocks with sacral plexus blocks.6–10
When performing ultrasound-guided sacral or lumbar plexus blocks, practitioners must consider risks such as unintentional internal organ injury, vessel puncture, and the need for proficient hemostasis, requiring a high level of skill in regional anesthesia. These precautions are crucial for maximizing patient safety and success of the procedure.11
An approach that combines the supra-inguinal fascia iliaca (SIFI) block with the subgluteal or transgluteal sciatic (SN) and posterior femoral cutaneous nerve (PFCN) blocks can offer a technically viable and safer alternative.8,9,12–14
This case series examines the management of seven patients with hemodynamic instability who sustained lower extremity vascular injuries from weapon wounds and underwent vascular repair surgery with debridement in low resource and austere environment. For anesthesia, a combination of SIFI, transgluteal SN, and PFCN nerve blocks was employed as sole anesthetic technique, optionally supplemented with light sedation. All patients provided written consent for publication, and the study was approved by Ethics Committee of Somine Dolo Hospital in Mopti, and fully complies with the Declaration of Helsinki.
Case Series
Data from May to December 2023 were retrospectively collected from the International Committee of the Red Cross (ICRC)-supported hospitals, Kidal referral Health Center and Somine Dolo Hospital in Mali. The findings are concisely displayed in Table 1.
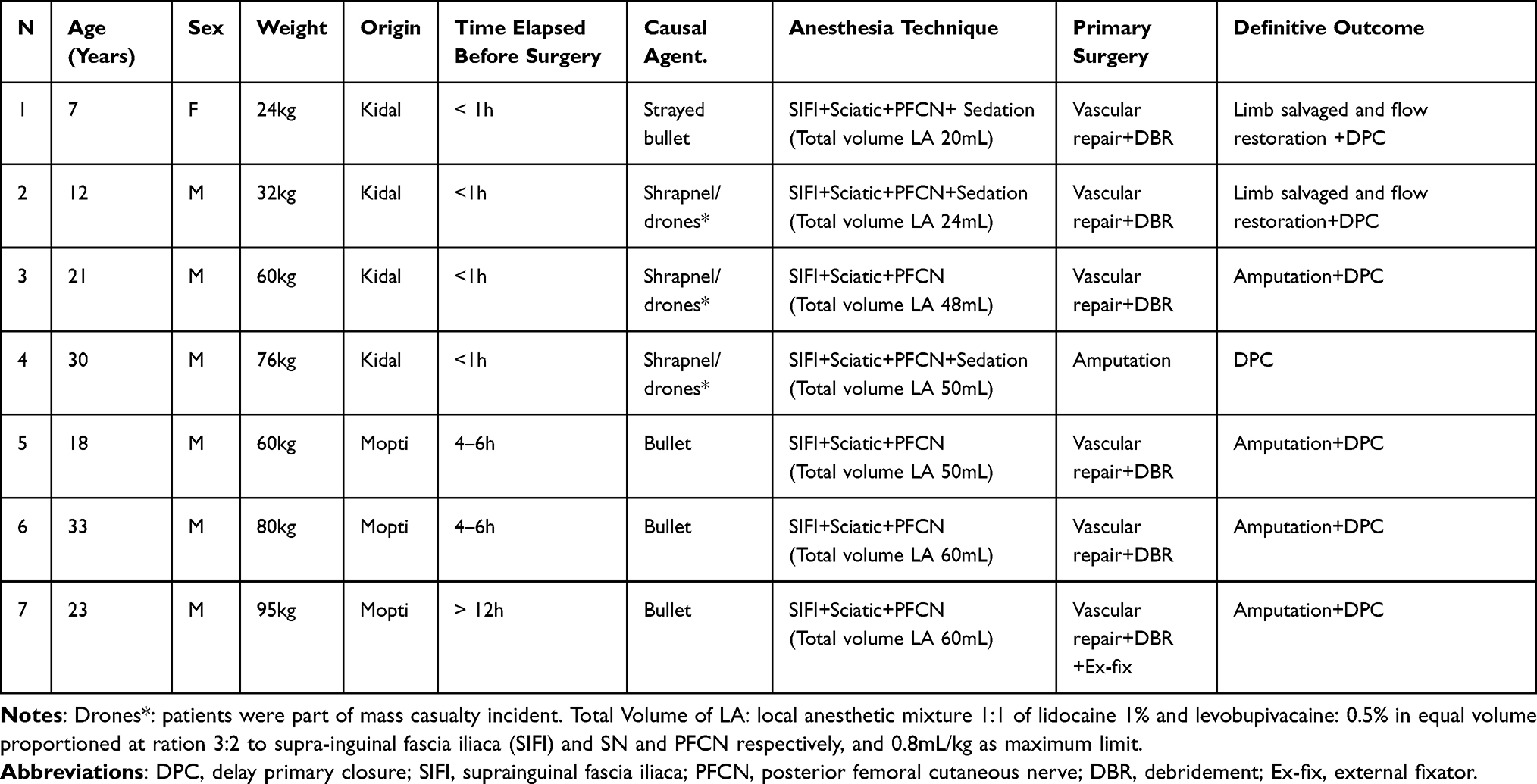 |
Table 1 Summary of Case Series |
All seven patients in the series received supra-inguinal fascia iliaca (SIFI) block along with transgluteal SN and PFCN blocks as the exclusive anesthetic technique. Of these, two children and one adult were also given light sedation prior to the administration of the blocks. Standard monitoring comprising Spo2, NIBP, EKG was applied. The blocks were performed by non-physician anesthetists and physician anesthetists for this case series.
Anesthesia Technique
Preparation
In this nerve block protocol, a mixture of 0.5% levobupivacaine and 1% lidocaine in equal volume (1:1 proportion) was administered for a total volume of 0.8mL/kg as maximum limit. The volume was then divided in a 3:2 ratio for the supra-inguinal fascia iliaca (SIFI) block and the combined SN and PFCN nerve blocks, respectively. For adults and pediatric, a 100mm and 50mm length nerve block needle was used, respectively (Stimuplex Ultra 360, insulated echogenic needle; size 22 G, bevel angle 30°, B. Braun Medical Inc., Melsungen, Germany). The procedure did not involve the use of nerve stimulation, and aseptic precautions were meticulously maintained.
Technique
We performed an ultrasound-guided supra-inguinal fascia iliaca (SIFI) block combined with a transgluteal sciatic and PFCN nerves block using a Sonosite M-Turbo ultrasound Machine (Sonosite M-Turbo V R Fujifilm Inc., USA). Preoperative informed consent was obtained for all patients. Single short sedation was initiated for 2 pediatric patients (ketamine 5mg+ midazolam 1mg and fentanyl 10Micrograms) and one adult patient (Ketamine 10mg, midazolam 4mg and fentanyl 50micrograme).
Supra-Inguinal Fascia Iliaca (SIFI) Block
The SIFI block was performed as described by Amato PE and Thames MR as depicted in Figure 1, using a 100mm nerve stimulator needle for adults and a 50mm needle for pediatric patients.15 A high frequency linear probe (HFL38 Transducer 13–6 MHz) was used for both adults and pediatric patients, utilizing an in-plane approach. A linear probe is placed 2/3 internally and 1/3 externally perpendicular to a line between the anterosuperior iliac spine (ASIS) and the pubic tubercle (inguinal ligament). The following sono-anatomical landmarks indicate proper probe positioning:
- The iliacus muscle is superficial to the ilium with hyperechoic fascia iliaca at the superficial border of the muscle.
- Cranially, the abdominal wall muscle, with the deep circumflex artery located between the internal oblique muscle and fascia iliaca.
- Deep into the iliacus muscle lies the anterior inferior iliac spine.



Under ultrasound guidance, the needle is advanced under the fascia iliaca between the abdominal wall muscles and the iliacus muscle, clear of the deep circumflex artery. Careful hydro-dissection allows the potential space between the fascia iliaca and the iliacus muscle to be opened: the ascent of the artery upon injection of the local anesthetic indicates good diffusion.
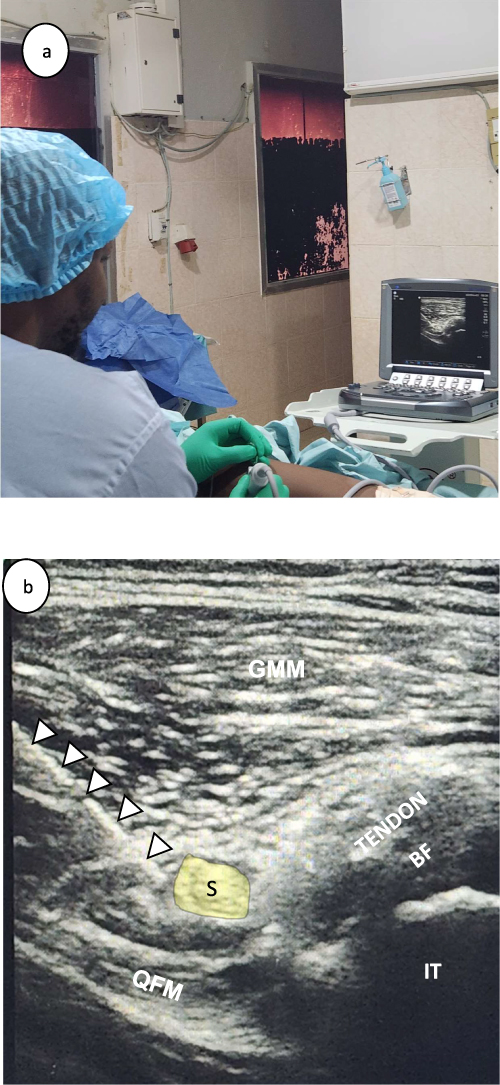
Transgluteal Approach to the Sciatic Nerve and Posterior Femoral Cutaneous Nerve
With the transgluteal approach (Figure 2), the sciatic nerve is identified deep to the gluteus maximus muscle, above the quadratus femoris and between two bony structures: the ischium and the greater trochanter. A curvilinear probe (C60x Transducer 5–2 MHz) was used for all adult patients, while a linear probe was used for the two pediatric cases. Both nerves are approached from the same injection point. The needle is directed deep and medially between the gluteus maximus muscle and the biceps femoris tendon within the deep investing fascia of the gluteus maximus muscle. At this level, the inferior gluteal artery can be perceived.14,16 5 to 10 mL of local anesthetic are injected with diffusion remaining above the deep investing fascia of the gluteus maximus muscle, which serves as an anatomical barrier between the PFCN and the sciatic nerve.14 The needle is then redirected toward the sciatic nerve by traversing the deep investing fascia of the gluteus maximus muscle, where the remainder of the local anesthetic is injected.

Subgluteal Approach to the Sciatic Nerve and Posterior Femoral Cutaneous Nerve
In non-obese patients, a high-frequency linear ultrasound probe can be used for the blockade of SN and PFCN at the gluteal crease. The subgluteal approach allows the identification of the greater trochanter, the long head of the biceps femoris muscle, the sciatic nerve (SN) and the posterior femoral cutaneous nerve (PFCN). The SN is usually found lateral or deep to the biceps femoris, while the PFCN lies superficial or slightly lateral to the SN and beneath the gluteus maximus and fascia lata, as indicated in Figure 3. A 22-gauge, 50mm echogenic needle is advanced in an in-plane, lateral-to-medial orientation to separately block the SN and PFCN.12–14,17
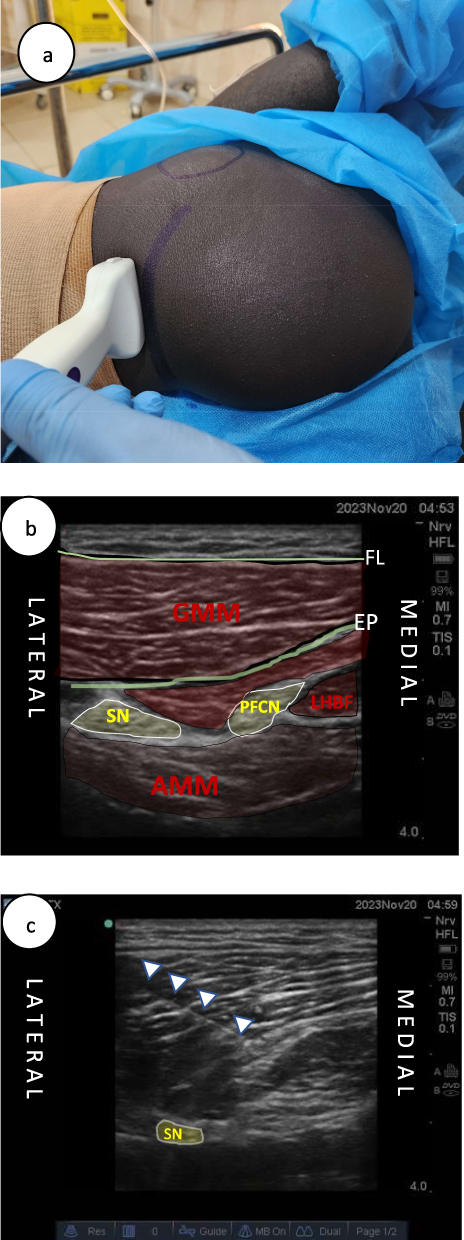 |
Figure 3 Subgluteal approach of Sciatic Nerve and Posterior Femoral Cutaneous Nerve at gluteal crease. (a) Probe position and landmarks. (b) Sono-anatomy. (c) Needle progression towards the posterior femoral cutaneous nerve (PFCN). Abbreviations: SN, Sciatic Nerve; PFCN, Posterior Femoral Cutaneous Nerve; GMM, Gluteus Maximus Muscle; AMM, Adductor Magnus Muscle; LHBF, Long Head of Biceps Femoris; FL, Fascia lata; EP, epimysium of gluteus maximus. |
While both subgluteal and transgluteal approaches are accepted, the transgluteal approach was exclusively used for all patients in this case series, reflecting practitioner preference rather than a prescriptive standard.
Discussion
Our case series open a perspective of using an approach combining SIFI block and SN and PFCN blocks as sole anesthetic technique and safe alternative to general anesthesia in high-risk patients, particularly for hemodynamically unstable weapon-wounded patients undergoing lower limb surgery in austere environment.
The current body of medical literature includes various accounts of employing either the Fascia Iliaca Block or the lumbar plexus block, sometimes in conjunction with a parasacral plexus block or sciatic block, for surgeries involving the lower limbs. These techniques are documented as part of an analgesic regimen or, in some cases, as the primary anesthetic method.6–10 However, to the best of our understanding, this case series marks the initial instance of documenting a comprehensive approach that integrates the SIFI block with both the SN and PFCN blocks.
In our series, our technique successfully blocked the sciatic nerve, the PFCN, and the three nerve derivatives from the lumbar plexus: obturator nerve, femoral nerve, and lateral femoral cutaneous nerve. No additional analgesic was given intraoperatively.
In a randomized controlled trial for total hip replacement, ultrasound-guided SIFI block resulted in a 67% success rate for blocking all three nerves.18,19 Additionally, a recent cadaver study demonstrated successful blockage of the femoral nerve, lateral cutaneous nerve of the thigh, and obturator nerve using ultrasound-guided SIFI block when 40 mL of local anesthetic was administered.20 In our protocol, we adhered to a maximum volume of 0.8 mL/kg for local anesthetics in our combined technique for SIFI, SN, and PFCN, with 60% of the volume (0.5 mL/kg) allocated to the SIFI block. The volume of local anesthetic used in the SIFI block plays a crucial role in achieving effective blockade of the femoral nerve, lateral cutaneous nerve of the thigh, and obturator nerve.20,21
In the medical literature, there are cases describing the management of patients with cardiovascular high risk. As reported by Ho et al and Asao et al, a combined paravertebral lumbar plexus and parasacral sciatic nerve block successfully managed the reduction of a hip fracture in elderly patients with severe heart failure.22,23 Unlike our approach, the combined paravertebral lumbar plexus and parasacral sciatic nerve block are advanced techniques that require expertise in regional anesthesia and have the potential for serious complications.24
Chia et al and Rizzo et al used a combined sciatic–femoral and lateral femoral cutaneous nerve block for the management of a patient with severe sepsis and recent myocardial infarction for an above knee amputation procedure and a patient with Eisenmenger’s syndrome with a left-type-only ventricle for meniscus extirpation by arthroscopic surgery, respectively.25,26 Compared to our approach which successfully blocks all the nerves of interest for above knee surgery, a combined sciatic–femoral and lateral femoral cutaneous nerve block cannot cover the obturator territory, and the block of PFCN from the SN block is inconsistent, with a reported failure rate of approximately 85% and 32% with anterior and posterior approaches to the sciatic nerve, respectively.27
Clinical Implications
The integration of the SIFI block with SN and PFCN blocks emerges as a promising and safe option to spinal anesthesia or to general anesthesia, especially for high-risk patients with lower limb injury in the challenging conditions typical of warzones.
Regional anesthesia has heralded a new era in the anesthetic management of wartime surgical interventions, extending the range of surgical possibilities and enhancing patient survivability. Its strategic advantages include a reduced recovery time, superior postoperative pain control, an accelerated patient turnover, vital in mass casualty scenarios, and the optimized allocation of medical resources.28–30
Strengths and Limitations
The SIFI block, along with the transgluteal or the alternative subgluteal approach to the SN and PFCN blocks, presents an accessible option compared to more complex and hazardous blocks like the lumbar plexus or parasacral plexus blocks, which require a higher degree of proficiency and expertise in regional anesthesia.6–10 However, the findings from our case series must be contextualized within its limitations, which include its retrospective and non-comparative design and the constraints imposed by the modest sample size. Furthermore, the technique involves the combination of three blocks using a large volume of local anesthetics, which raises concerns about the risk of local anesthetic systemic toxicity.
Future Research
Further research on a larger scale may be required to corroborate our findings and to perform a comparative analysis of our combined three-block technique against other anesthetic methods. Our study employed the transgluteal approach, which lays the groundwork for future comparisons with the subgluteal approach that targets the SN and the PFCN individually.
Conclusion
The technique that combines the SIFI block with blocks of the SN and the PFCN offers a valuable alternative for hemodynamically unstable patients who need lower limb surgery, particularly in settings with limited resources. This approach enhances the existing repertoire of anesthesia techniques, providing options beyond general and spinal anesthesia.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rai KM, Mohanty SK, Kale R, Chakrabarty A, Prasad D. Management of vascular injuries in a forward hospital. Med J Armed Forces India. 2006;62(3):246–251. PMID: 27365688; PMCID: PMC4922881. doi:10.1016/S0377-1237(06)80012-2
2. Jawas A, Abbas AK, Nazzal M, Albader M, Abu-Zidan FM. Management of war-related vascular injuries: experience from the second gulf war. World J Emerg Surg. 2013;8(1):22. PMID: 23816260; PMCID: PMC3700839. doi:10.1186/1749-7922-8-22
3. Fox CJ, Gillespie DL, O’Donnell SD, et al. Contemporary management of wartime vascular trauma. J Vasc Surg. 2005;41(4):638–644. PMID: 15874928. doi:10.1016/j.jvs.2005.01.010
4. Nguyen T, Kalish J, Woodson J. Management of civilian and military vascular trauma: lessons learned. Semin Vasc Surg. 2010;23(4):235–242. PMID: 21194641. doi:10.1053/j.semvascsurg.2010.11.004
5. Alarhayem AQ, Cohn SM, Cantu-Nunez O, Eastridge BJ, Rasmussen TE. Impact of time to repair on outcomes in patients with lower extremity arterial injuries. J Vasc Surg. 2019;69(5):1519–1523. PMID: 30497861. doi:10.1016/j.jvs.2018.07.075
6. Hall MR, Kalbaugh CA, Tsujimoto THM, McGinigle KL. Regional anaesthesia alone is reasonable for major lower extremity amputation in high risk patients and may initiate a more efficacious enhanced recovery programme. Eur J Vasc Endovasc Surg. 2020;60(5):747–751. PMID: 32763119. doi:10.1016/j.ejvs.2020.06.034
7. Zhao J, Huang Y, Fu M, Tao F. Ultrasound-guided supra-inguinal fascia iliaca block combined with a sacral plexus block for lower extremity surgery: a case report. Medicine. 2020;99(35):e21921. doi:10.1097/MD.0000000000021921
8. DeLong L, Krishna S, Roth C, et al. Short communication: lumbar plexus block versus supra-inguinal fascia iliaca block to provide analgesia following hip and femur surgery in pediatric-aged patients - an analysis of a case series. Local Reg Anesth. 2021;14:139–144. PMID: 34703306; PMCID: PMC8541757. doi:10.2147/LRA.S334561
9. Genc C, Akdeniz S, Canikli S, et al. Ultrasound-guided supra-inguinal fascia iliaca block as part of anesthesia management for lower extremity surgeries: a single-center retrospective cohort feasibility study. Cureus. 2023;15(10):e47795. doi:10.7759/cureus.47795
10. Bravo D, Layera S, Aliste J, et al. Lumbar plexus block versus supra-inguinal fascia iliaca block for total Hip arthroplasty: a single-blinded, randomized trial. J Clin Anesth. 2020;66:109907. PMID: 32502775. doi:10.1016/j.jclinane.2020.109907
11. Grant SA, Auyoung DB. Ultrasound Guided Regional Anesthesia. Oxford University Press, Inc; 2012:108–118.
12. Topçu I, Aysel I. Ultrasound guided posterior femoral cutaneous nerve block. Agri. 2014;26(3):145–148. PMID: 25205415. doi:10.5505/agri.2014.26122
13. Wang TC, Yang CC. Letter to the editor: ultrasound-guided posterior femoral cutaneous nerve block. Agri. 2018;30(2):102–103. PMID: 29738064. doi:10.5505/agri.2018.75688
14. Johnson CS, Johnson RL, Niesen AD, Stoike DE, Pawlina W. Ultrasound-guided posterior femoral cutaneous nerve block: a Cadaveric Study. J Ultrasound Med. 2018;37(4):897–903. PMID: 29027690. doi:10.1002/jum.14429
15. Amato PE, Thames MR. How I do it: supra-inguinal fascia iliaca block. ASRANews. 2020;45(4). doi:10.52211/asra110120.063
16. Windhofer C, Brenner E, Moriggl B, Papp C. Relationship between the descending branch of the inferior gluteal artery and the posterior femoral cutaneous nerve applicable to flap surgery. Surg Radiol Anat. 2002;24(5):253–257. PMID: 12497213. doi:10.1007/s00276-002-064-z
17. Lee B. Chapter 47 - Posterior Femoral Cutaneous Nerve Block, Atlas of Ultrasound-Guided Regional Anesthesia.
18. Tarekegn F, Sisay A. Amanuel Sisay, A review of evidence-based clinical practice on fascia iliaca compartment block for lower limb injury. Ann Med Surg. 2021;69:102758. doi:10.1016/j.amsu.2021.102758
19. Desmet M, Vermeylen K, Van Herreweghe I, et al. A longitudinal supra-inguinal fascia iliaca compartment block reduces morphine consumption after total Hip arthroplasty. Reg Anesth Pain Med. 2017;42(3):327–333. doi:10.1097/AAP.0000000000000543
20. Vermeylen K, Soetens F, Leunen I, et al. The effect of the volume of supra-inguinal injected solution on the spread of the injectate under the fascia iliaca: a preliminary study. J Anesth. 2018;32(6):
21. Ponde V, Gursale A, Chavan D, Johari A, Osazuwa M, Nagdev T. Fascia iliaca compartment block: how far does the local anaesthetic spread and is a real time continuous technique feasible in children? Indian J Anaesthesia. 2019;63(11):932–937. doi:10.4103/ija.IJA_344_19
22. Ho AMH, Karmakar MK. Combined paravertebral lumbar plexus and parasacral sciatic nerve block for reduction of Hip fracture in a patient with severe aortic stenosis. Can J Anesth. 2002;49(9):946–950. doi:10.1007/BF03016880
23. Asao Y, Higuchi T, Tsubaki N, Shimoda Y. [Combined paravertebral lumbar plexus and parasacral sciatic nerve block for reduction of Hip fracture in four patients with severe heart failure]. Masui. 2005;54(6):648–652. Japanese. PMID: 15966383
24. Gupta N, Panwar V, Mishra S. Total spinal anaesthesia: a rare complication of psoas compartment block. Turk J Anaesthesiol Reanim. 2021;49(2):163–165. PMID: 33997847; PMCID: PMC8098733. doi:10.5152/TJAR.2020.26918
25. Chia N, Low TC, Poon KH. Peripheral nerve blocks for lower limb surgery--a choice anaesthetic technique for patients with a recent myocardial infarction? Singapore Med J. 2002;43(11):583–586. Erratum in: Singapore Med J. 2002 Dec;43(12):604. PMID: 12680529
26. Rizzo D, Giustiniano E, Pellicori D, Misiti CM, Cosco G. Blocco dei nervi sciatico, femorale e cutaneo laterale della coscia per meniscectomia in artroscopia in un paziente affetto da sindrome di Eisenmerger. Caso clinico [Sciatic, femoral and cutaneous nerve block for arthroscopic meniscectomy in a patient with Eisenmerger’s syndrome. Case report]. Minerva Anestesiol. 1999;65(10):733–736. Italian. PMID: 10598431
27. Ota J, Sakura S, Hara K, Saito Y. Ultrasound-guided anterior approach to sciatic nerve block: a comparison with the posterior approach. Anesthesia Analg. 2009;108(2):660–665. doi:10.1213/ane.0b013e31818fc252
28. Wu JJ, Lollo L, Grabinsky A. Regional anesthesia in trauma medicine: review article. Anesthesiol Res Pract. 2011;7. doi:10.1155/2011/71328
29. Buckenmaier C. Battlefield regional anesthesia: evolution and future concepts. In: Techniques in Regional Anesthesia and Pain Management. Elsevier; 2012.
30. Tarmey N, Park C, McFarland C, Mahoney P. Field anesthesia and military injury. In: Smith C, editor. Trauma Anesthesia. Cambridge: Cambridge University Press; 2015:640–656. doi:10.1017/CBO9781139814713.043
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.