")
Back to Journals » Breast Cancer: Targets and Therapy » Volume 16
Clinical Outcomes of Patients with HER2 Positive Metastatic Breast Cancer to the Brain, with First-Line Trastuzumab, Pertuzumab and Chemotherapy, in a Real-World Setting
Authors Sharman Moser S, Apter L, Livnat I, Ginsburg R, Yarden A, Drori M, Drizon A, Chodick G, Siegelmann-Danieli N
Received 6 November 2023
Accepted for publication 25 January 2024
Published 6 March 2024 Volume 2024:16 Pages 105—116
DOI https://doi.org/10.2147/BCTT.S439158
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Harikrishna Nakshatri
Sarah Sharman Moser,1 Lior Apter,1,2 Idit Livnat,3 Roni Ginsburg,3 Adva Yarden,3 Michal Drori,1 Anat Drizon,1 Gabriel Chodick,1,4 Nava Siegelmann-Danieli1,4
1Maccabi Institute for Research and Innovation (Maccabitech), Maccabi Healthcare Services, Tel Aviv, Israel; 2Department of Health Systems Management, Ben-Gurion University of the Negev, Beer-Sheva, Israel; 3Medical Affairs, AstraZeneca, Kefar Sava, Israel; 4Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel
Correspondence: Sarah Sharman Moser, Email [email protected]
Background: In this observational study, we analyzed the treatment patterns and clinical outcomes of patients with human epidermal growth factor receptor 2 (HER2)-positive metastatic breast cancer (mBC) who developed brain metastases during their disease in a 2.7 million-member public health-provider in Israel.
Methods: Newly diagnosed patients with mBC who initiated first-line treatment between January 2013 and June 2021 were identified. Time on treatment (ToT) and overall survival (OS) were assessed at a minimum of 6 months follow-up (cutoff: December 2021).
Results: We identified a total of 61 patients: 98.4% females, median age 50 years (IQR = 44– 63), 85% invasive ductal tumors, 44% hormone receptor positive, 51% performance status 0– 1. The median duration of follow-up was 6.2 years. All patients initiated a combination treatment of trastuzumab, pertuzumab, and chemotherapy (TPC), and 72% moved to second-line treatment during the study follow-up period (82% ado-trastuzumab emtansine). The median ToT for first-line and second-line treatments were 16.9 months (95% CI = 13.9– 27.7) and 7.9 months (95% CI = 5.6– 10.9), respectively. The median overall survival (OS) was 45.5 months (95% CI = 35.4– 71.2) from the initiation of first-line treatment. When considering the timing of brain metastases, the median OS was 36.3 months (95% CI = 10.0–NR) for those diagnosed upfront (n = 15, 25%), 59.1 months (95% CI = 32.5–NR) for those diagnosed while on TPC (n = 25, 41%), and 40.8 months (95% CI = 35.4–NR) for those diagnosed at a later stage (n = 21, 34%). The median OS from brain metastases diagnosis was 25.1 months (95% CI = 17.0– 34.6).
Conclusion: Patients with upfront brain involvement at the time of mBC diagnosis had shorter survival compared to those who started TPC without brain metastases. Nonetheless, the overall results from this study compare favorably with previous studies and contribute to understanding the value of traditional treatment options, which will serve as a baseline for future treatment strategies in the real-world setting.
Keywords: HER2 positive, metastatic, breast cancer, observational study, real-world
Background
Human epidermal growth factor receptor 2-positive breast cancer (HER2+) represents about 15–20% of all breast cancer cases.1 Before the era of HER2-directed therapies, this type of breast cancer was associated with a higher risk of early recurrence and mortality when compared to patients with other subtypes of breast cancer.2,3 With modern anti-HER2 directed therapies, with the inclusion of trastuzumab, pertuzumab, and taxane in the first-line setting, based on the Cleopatra study, overall survival in patients with metastatic breast cancer (mBC) over-expressing HER2-proto-oncogen was reported to extend to a median of 57 months, with 37% of patients surviving 8 years.4 Subsequent treatments available in recent years, including the anti-body drug conjugate (ADC) trastuzumab-emtansine (T-DM1), additional trastuzumab-chemotherapy combinations, and HER2-directed tyrosine-kinase inhibitors (TKI’s) such as lapatinib and neratinib, further extended treatment options for those patients.5,6 Despite these advancements, a significant proportion of women diagnosed with HER2+ mBC have to face the devastating development of brain metastases (25–50%).7–10 This rate is higher when compared to other subtypes of metastatic breast cancer.11 It has been suggested that this could be associated with the inherent phenotype of HER2 amplified breast tumors and augmented with longer survival associated with effective HER2+ directed treatments in the metastatic setting, and/or the lack of intra-brain effective penetration of the large anti-HER2 directed antibodies.12–15 Brain metastases are associated with a decreased quality-of-life, progressive neurological impairments, and a poor prognosis, and up until recently required brain irradiation to involved lesions.5,16–18 Historical median survival following brain metastases diagnosis was 11–18 months.7,19–21 Recently, exciting results have reported prolonged overall survival in all patients with HER2+ mBC, and additionally in a sub-group of patients with brain metastases, which has been reported in several prospective clinical trials, including Destiny Breast −03 with the new ADC, fam-trastuzumab-deruxtecan-nxki (T-DXd),22 and in the HER2Climb trial with the new generation TKI, tucatinib, in combination with trastuzumab and capecitabine.23 These two regimens are currently recommended for second-line treatment for patients with HER2+ mBC and brain metastases, and may result in intra-brain response with a sparing of radiotherapy of the brain metastases. The current first-line regiment is still a trastuzumab, pertuzumab, and chemotherapy (TPC) combination based on the Cleopatra trial, however, the original trial did not allow inclusion of patients with brain metastases.2,4
This retrospective real-world observational study aims to shed light on the survival outcomes of patients who were diagnosed with HER2+ mBC and treated for brain metastases during the years when trastuzumab, pertuzumab, and chemotherapy were available in the first-line setting, and T-DM1 for second-line. We aim to offer insights into contemporary treatment practices aligned with current guidelines, and provide a benchmark for evaluating the efficacy of newer anti-HER2 directed therapies.
Materials and Methods
Data Source
In this retrospective cohort study, the computerized databases of Maccabi Healthcare Services (MHS), a healthcare insurer-provider serving a quarter of Israel’s population, with 2.7 million members, were utilized.24 The MHS database was established in 1993 and includes complete and automatic capture of diagnosis data (using the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) coding system), pharmacy prescription and purchase data, laboratory results, hospitalizations, procedures, imaging, and physician consultations. MHS has developed several computerized registries of major chronic diseases that identify patients via automatic search formulas, such as ischemic heart disease, oncologic diseases, diabetes, and osteoporosis.25–27 Unstructured data, such as confirmation of breast cancer histology, tumor characteristics like hormone sensitivity, Eastern Cooperative Oncology Group (ECOG) performance status (PS), biomarkers, and disease stage, were manually extracted from individual patient data stored in Portable Document Format (PDF) files by trained data extractors.
Study Population
In this retrospective cohort study, we identified MHS members with HER2+ mBC from the cancer registry, with central nervous system (CNS) metastases over the course of their metastatic disease (identified from receiving brain radiotherapy and/or undergoing brain surgery), that initiated first-line systemic treatment with TPC between January 1, 2013 to June 30, 2021.
The cancer registry is compiled from the national cancer registry (all pathology results from cancer patients are submitted to the national register) and from cancer treatment drug approvals by the MHS Drug Approval Committee. All patients included in this study were insured by MHS and treated in nationwide oncology units. Due to a regulatory limitation that prohibits collection of HER2+ data, we used trastuzumab purchases as a proxy for HER2+ disease which is reasonable due to the regulatory limitations and necessary approval from the MHS Drug Approval Committee.
To be eligible for inclusion in this study, patients had to be 18 years of age or older at the time of diagnosis and maintain continuous healthcare enrollment with MHS for a minimum of 1 year before the index date. Data collection continued until December 31, 2021 to allow for at least 6 months of follow-up. The index date was set as the date of first purchase of first-line treatment (Figure 1).
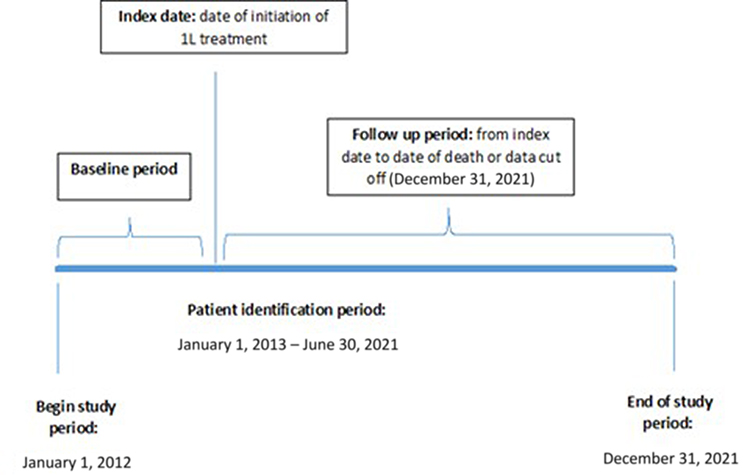 |
Figure 1 Study design. |
Study Variables
At the index date, the socio-demographic and clinical information collected included age, sex, socioeconomic status (SES), geographic district, the presence of comorbid conditions, body mass index (BMI), and smoking status. The determination of socioeconomic status (categorized as low, medium, or high) was derived from the poverty index, which took into account various factors, including income, education, housing conditions, and car ownership.28 Smoking data were based on primary care physician reporting and classified into current/past, never, and unknown. The last BMI measured prior to index date within the 5-year period was collected. Comorbidities such as diabetes mellitus, cardiovascular disease, and hypertension were identified through the MHS registries.
Trained data extractors manually extracted data not available in the main MHS database from patient medical summaries including disease staging, histology (invasive ductal, invasive lobular, lobular and ductal, other/unknown), imaging results (computed tomography [CT], Positron emission tomography–computed tomography [PET-CT], Magnetic resonance imaging [MRI]), biopsy, metastases (visceral [lung/liver/abdomen/skin], lymph, bone), Eastern cooperative oncology group (ECOG) performance status (PS) results, or hormone receptor response (Positive: estrogen receptor [ER+]/progesterone receptor [PR+], ER+, PR+; negative or unknown).
Statistical Analysis
In this study, we report demographic, clinical, and treatment characteristics. Descriptive analyses included categorical variables (expressed as frequency and percentage) and continuous variables (expressed as mean [standard deviation] or median [interquartile range] according to the distribution of the data).
We defined treatment lines according to the sequence of dispensed medications from the MHS pharmacy database, and in addition included information on medications provided by private insurance and clinical studies from data extraction where available. Any drug purchased within 1 month of a new line was considered part of that line. Cessation of a drug from a combination regimen was not considered a change of line as it was likely due to tolerance issues or adverse effects. A new treatment line was characterized as either the initiation of a new treatment regimen or the incorporation of a new medication into an existing regimen.
Time to event analysis for time on treatment and overall survival was assessed using Kaplan-Meier analysis and we present median time with 95% confidence intervals (CI). Individuals were followed from the index date until the earliest occurrence of one of the following events: the specified outcome, death, being lost to follow-up, or the conclusion of the study period (December 31, 2021). Time on treatment analysis was defined as the duration from the commencement of the first-line treatment to the date of the last treatment + 1 day. The discontinuation of treatment was determined by any of the following criteria: the commencement of the next line of therapy (second-line), death while still on treatment, or a lapse of at least 120 days between the last drug administration and the follow-up date.29–31 Patients that did not discontinue were censored at the last purchase date. Overall survival was evaluated by utilizing data on all-cause mortality obtained monthly from the National Insurance Institute in Israel and was defined as the duration from the initiation of the first-line treatment to the date of death from any cause. Patients that were still alive were censored at the follow-up date. Overall survival was also determined starting from the date of brain metastases diagnosis.
The treatment cohort was stratified into patients that were diagnosed with brain metastases prior to initiation (or within 1 month) of first-line treatment (“before first-line treatment initiation”), patients who were diagnosed with brain metastases more than 6 months after initiation of first-line treatment to cessation of first-line treatment (“during first-line treatment”), and patients who were diagnosed with brain metastases on second-line treatment or during subsequent treatment (”during second-line or subsequent treatment”). No patients were diagnosed with brain metastases between 1–6 months of first-line treatment initiation.
IBM SPSS Statistics for Windows, Version 22.0 (IBM Corp, Armonk, NY) and R version 3.5.1 were used for all analyses, and a p value <0.05 was considered statistically significant.
This observational study was performed in accordance with the ethical principles consistent with the Declaration of Helsinki. The local institutional review board of MHS in Israel approved this study and consent was waived due to the retrospective nature of the study. Data was anonymized and maintained with confidentiality.
Results
A total of 61 patients with metastatic breast cancer and brain metastases that received first-line TPC were identified between January 1, 2013 and June 30, 2021. Median follow-up time for this cohort was 6.2 years (95% CI = 4.4–7.9). Median (IQR) age was 50 (44–63), 98.4% were female, 85.2% had invasive ductal disease, 44.3% had hormone receptor positive tumors, 50.8% had ECOG PS 0–1, and 62.3% had visceral metastases (Table 1).
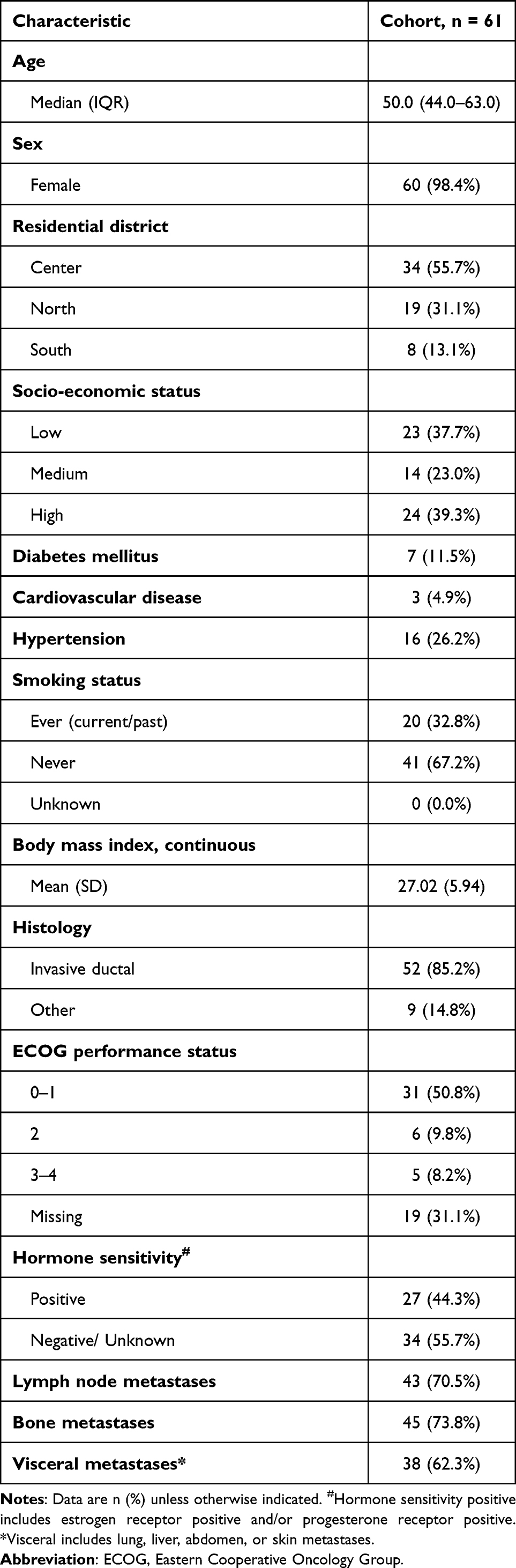 |
Table 1 Baseline Characteristics of Patients Diagnosed with HER2 Positive Metastatic Breast Cancer from January 2013 to June 2021 That Initiated Systemic 1L Treatment (n = 61) |
A total of 15 (25%) patients had brain metastases diagnosed before first-line treatment initiation (including one patient who was diagnosed a week after treatment initiation), 25 (41%) were diagnosed with brain metastases during first-line treatment (from at least 6 months from treatment initiation) and 21 (34%) during second-line or subsequent treatment (data not shown).
Median time on first-line treatment was 16.9 months (13.9–27.7), and 26.1% and 19.2% of patients were still receiving treatment at 3 and 4 years, respectively (Table 2, Figure 2). Time on treatment was longer from initiation of first-line treatment for patients diagnosed with brain metastases during first-line treatment (30.3 months [21.8–57.8]) than those diagnosed before first-line treatment initiation (9.5 months [8.7–NR]) or those diagnosed during second-line or subsequent treatment (13.9 months [9.6–24.9], p = 0.005, data not shown).
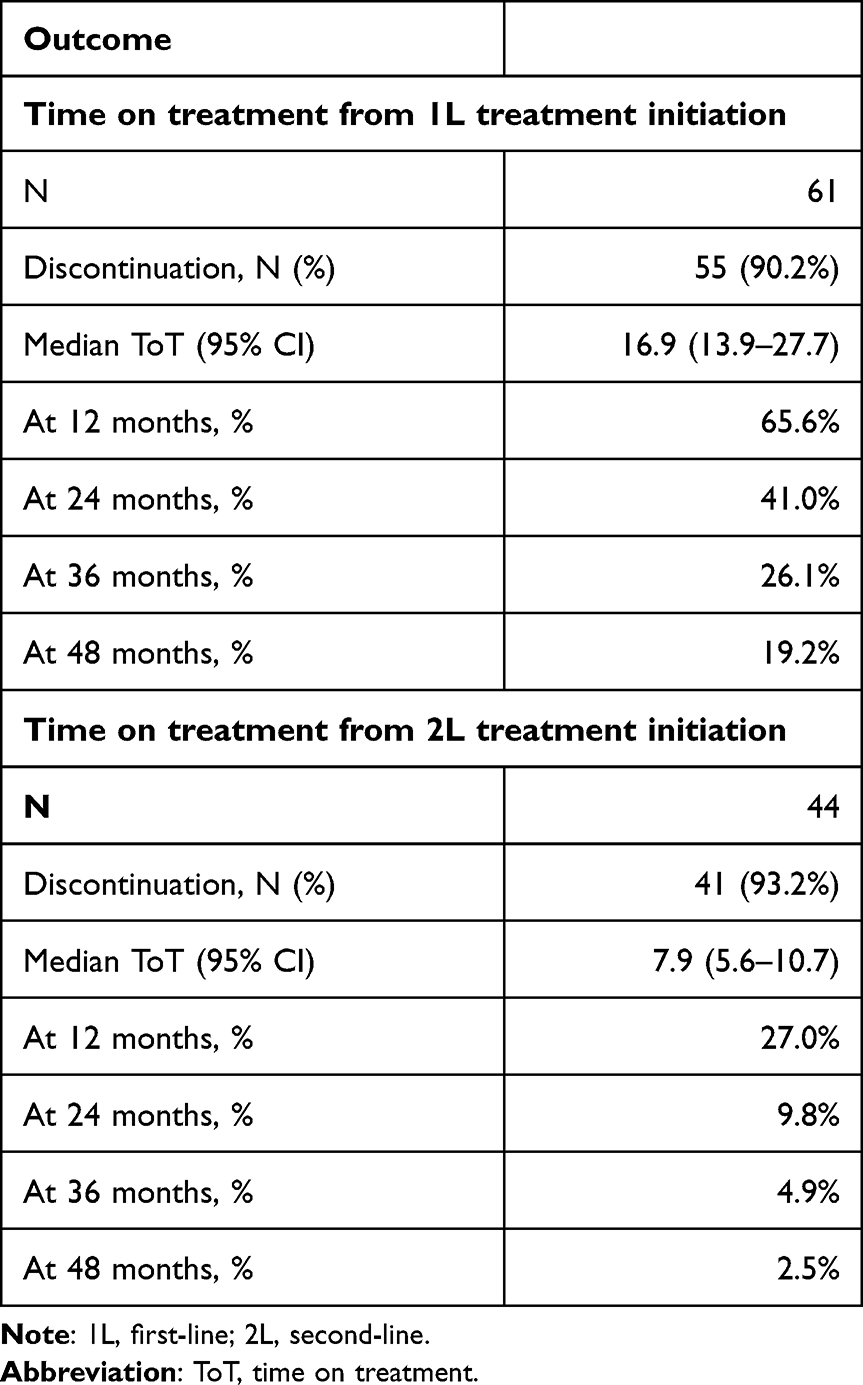 |
Table 2 Time on Treatment from First-Line and Second-Line Treatment Initiation for Patients Diagnosed with HER2 Positive Metastatic Breast Cancer with Brain Metastases Diagnosed during Their Metastatic Disease, from January 2013 to June 2021 (n = 61) |
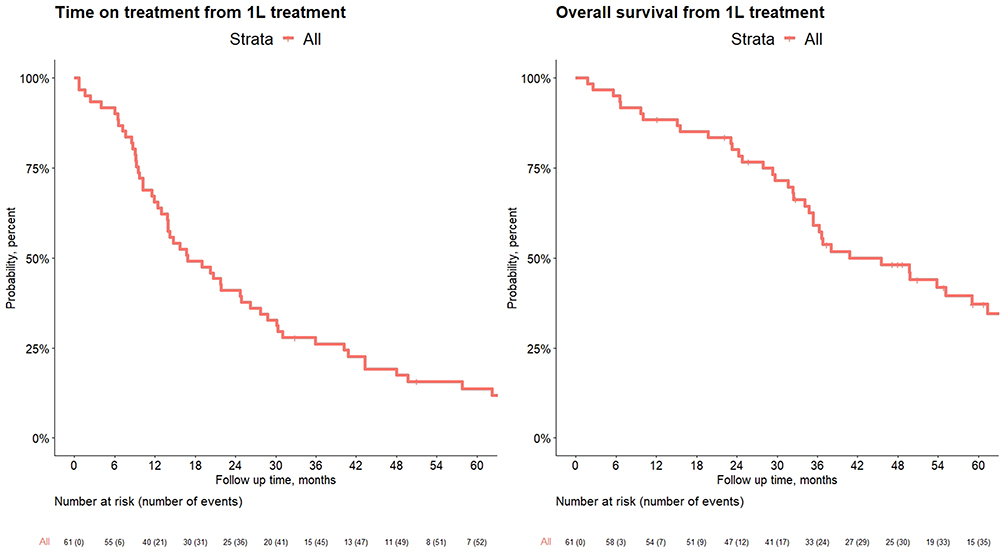 |
Figure 2 Time on treatment and overall survival from first-line treatment initiation for patients diagnosed with HER2 positive metastatic breast cancer with brain metastases diagnosed during their metastatic disease, from January 2013 to June 2021 (n = 61). |
A total of 44 patients (72.1%) moved to second-line treatment, consisting of 81.8% T-DM1 treatment, and 18.2% other treatment (different trastuzumab-based combinations with chemotherapy and hormonal therapy). Time on treatment from initiation of second-line therapy was 7.9 months (5.6–10.9, Table 2).
Overall Survival from Initiation of First-Line Treatment
Overall survival from initiation of first-line treatment was 45.5 months (35.4–71.2) and 59.1% and 48.2% of patients were still alive at 36 and 48 months, respectively (Table 3, Figure 2). Patients’ diagnosed with brain metastases before initiation of first-line treatment had lower overall survival from first-line treatment initiation (36.3 months [10.0–NR]) than those diagnosed during first-line treatment (59.1 months [32.5–NR]) or during second-line or subsequent treatment (40.8 months [35.4–NR], Table 4).
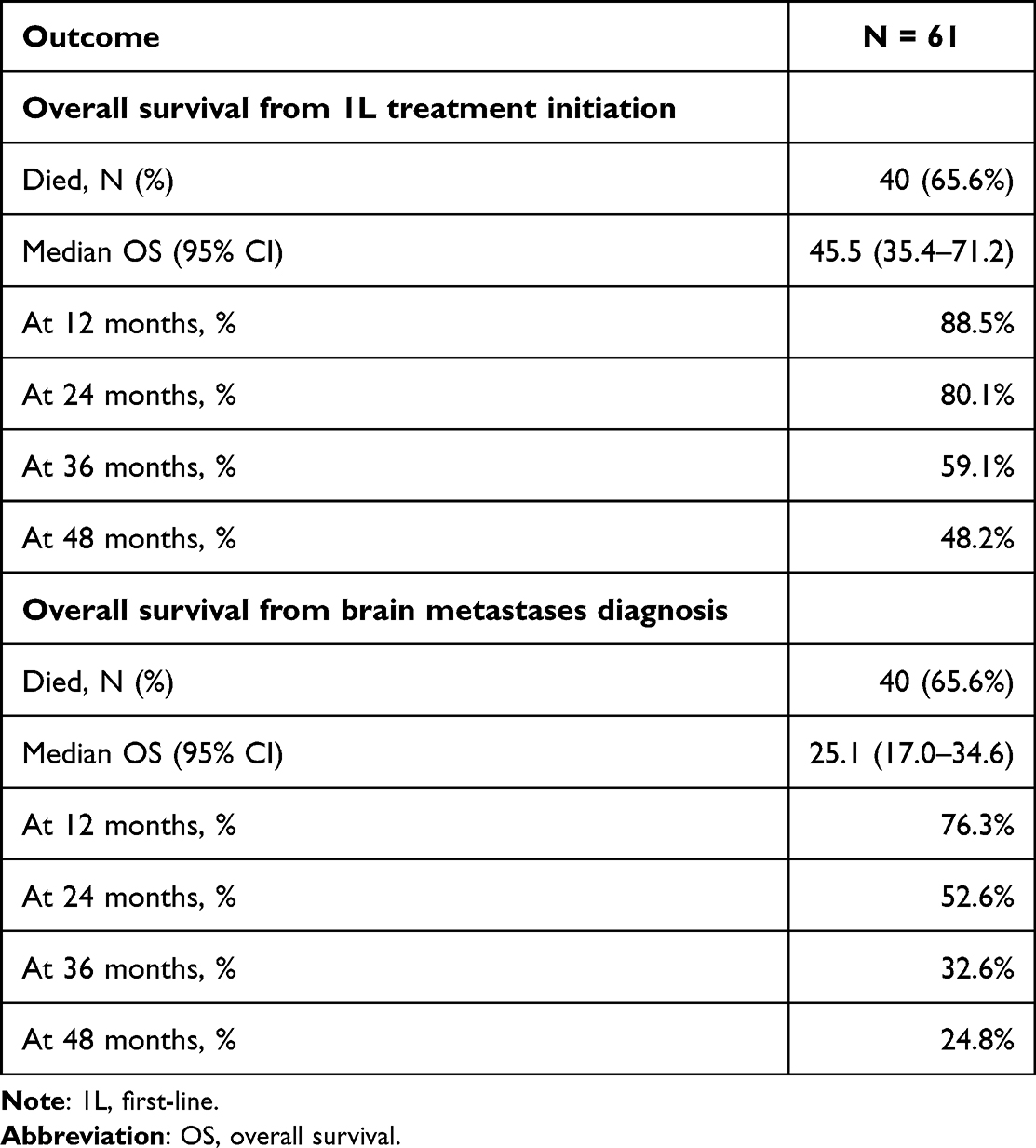 |
Table 3 Overall Survival from First-Line Treatment Initiation, and Overall Survival from Brain Metastases Diagnosis for Patients Diagnosed with HER2 Positive Metastatic Breast Cancer with Brain Metastases Diagnosed during Their Metastatic Disease, from January 2013 to June 2021 (n = 61) |
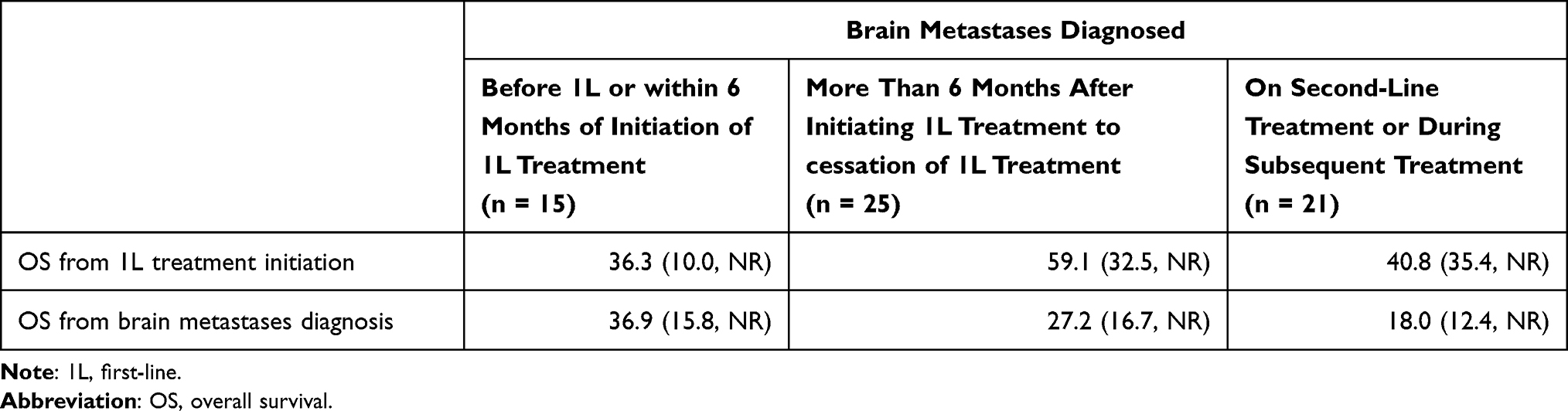 |
Table 4 Overall Survival from First-Line Treatment Initiation, and Overall Survival from Brain Metastases Diagnosis, Stratified by Time of Brain Metastases Diagnosis, for Patients Diagnosed with HER2 Positive Metastatic Breast Cancer from January 2013 to June 2021 (n = 61) |
Overall Survival from Diagnosis of Brain Metastases
Median overall survival from brain metastases diagnosis was 25.1 months (17.0–34.6, Table 3), and was longer for those diagnosed before first-line treatment initiation (36.9 months [15.8–NR]) than those diagnosed during first-line treatment (27.2 months [16.7–NR]) or those diagnosed during second-line or subsequent treatment (18.0 months [12.4–NR], p= 0.007, Table 4). A total of 24.8% of patients were still alive at 4 years from brain metastases diagnosis (Table 3).
Discussion
Brain metastases are relatively common in patients with HER2+ mBC, diagnosed in approximately 25–55% of those patients.7–10 Our study of a cohort of patients with HER2+ mBC+ who developed brain metastases during the course of their disease and received local measures (mostly with brain irradiation) describes treatment lines, time on first and second-line treatment, and overall survival in a real-world setting with relatively up-to-date treatment protocols. TPC combination was given in first-line, and T-DM1 in the majority of patients in second-line regimens, which was the standard of care in the second-line setting until recently. This cohort had a long follow-up of over 6 years allowing us to examine patients’ outcomes during first and second-line treatment.
We used time on treatment as a proxy for progression-free survival in the real-world setting, similar to previous studies.32–34 Our assumption is that patients continued on their assigned treatment as long as they had clinical benefit and only switched to subsequent treatment on disease progression or significant toxicity, and therefore time on treatment is an accurate substitute for progression-free survival.
The Cleopatra study which proved the efficacy of the addition of pertuzumab to first-line treatment of trastuzumab with chemotherapy, reported progression free survival of 18.7 months and overall survival of 56.5 months (49.3–NR) for patients in the pertuzumab arm.4 These results led to the treatment guidelines of first-line treatment of TPC. Median age and the percentage of patients with PS 0–1 were slightly lower in our study, as expected as our study included patients with brain metastases at baseline (25%) and in addition we had unreported PS in about a third of the patients.35 While the Cleopatra study excluded patients with upfront brain metastases, current guidelines recommend that if peripheral disease is controlled and the brain is the only site of progression, patients should receive local brain treatment (surgery and/or radiation) and continue the TPC treatment, as anti-HER2 anti-bodies do not have optimal penetration to the CNS.12,13 In our study, 41% (n = 25) of patients developed brain metastases during first-line TPC treatment, continued the same systemic therapy along with local treatment, and achieved an overall survival of 59.1 months, which is comparable to the overall survival of patients in the Cleopatra study.36 As expected, patients with upfront brain metastases had inferior survival of 36.3 months.
The most common second-line treatment in our patients was T-DM1 based on the Emilia trial.37 The later reported median PFS of 9.6 months, and the more recent “DESTINY-Breast03” study reported progression free survival of 6.8 months with T-DM1 and 28.8 months with the new ADC T-DXd (for second-line or above).22 In those trials, the majority of patients were brain-metastases free. We found real-world time on treatment from second-line treatment initiation for patients with brain metastases of 7.9 months, which is comparable with the above studies.
Patients diagnosed with brain metastases at diagnosis had a worse prognosis and shorter survival from first-line treatment initiation than those diagnosed later in the disease pathway, however systemic treatment and brain radiotherapy showed quite a long response and survival for these patients. Patients that had brain metastases diagnosed during first-line treatment had a better prognosis and longer overall survival from treatment initiation than those diagnosed with brain metastases at diagnosis, but at some point ceased to respond to treatment.
Survival from brain metastases diagnosis with reference to the patient’s place in the disease pathway is an important measure. When measured from brain metastases diagnosis, survival was lower for those with brain metastases diagnosis during first- and second-line treatment (27.2 and 18.0 months, respectively) than those with a brain metastases diagnosis before first-line treatment initiation (36.9 months). This may be explained by partial exhaustion of treatment options in patients diagnosed in later stages of metastatic disease, hence, treatment naïve patients had many treatment options available.
We found relatively longer survival from brain metastases diagnosis compared to previous reports. In one historical study of patients with HER2+ mBC who were treated with trastuzumab with or without chemotherapy between 1998–2000, 34% of patients with HER2+ mBC were identified with brain metastases, and survival from brain metastases was 13 months.7 Another study from Japan for the period of 2001–2012 of patients with mBC of various sub-types diagnosed with brain metastases, found more favorable overall survival in patients with HER2+ tumors (16.5 and 11.5 months for HER2+/ER+ and HER2+/ER−, respectively) compared with other sub-types (9.3 and 4.9 months for patients with luminal and triple negative tumors, respectively),19 still lower than in our cohort. Another observational study reported outcomes for patients with HER2+ mBC between 2003–2006, with similar characteristics to our cohort: young age, similar hormone receptor status and ECOG PS 0–1. That study found that 7% of patients were diagnosed with brain metastases up front, and another 30% further along the disease pathway, and local treatment to the central nervous system was not reported in all cases. Overall survival from brain metastases was 17.5 months, however, patients had less treatment options compared with our cohort (as this previous study was carried out in the pre-pertuzumab and lapatinib era).38 In addition, as our cohort is relatively recent, all patients received TPC in the first-line setting, the majority received T-DM1 in the second-line setting, and all received brain irradiation with modern techniques.
Currently newer treatment options are emerging for patients with HER2+ mBC and may be beneficial also for patients with brain metastases, includingT-DXd and tucatinib in combination with trastuzumab and capecitabine.23,39,40 T-DXd was incorporated in the Israel National Drugs Formula in January 2022, and tucatinib in January 2023, and we look forward to evaluating their future benefit in the real-world setting.
One of the most common sites for metastases in breast cancer is the brain, and recent studies have researched the use of predictive diagnostics, targeted prevention, and patient stratification in order to tailor treatment to individual patient needs.41,42 One study summarized risk factors associated with the development of brain metastases in patients with primary breast cancer including age, menopausal status, molecular biological stratification, and protein biomarkers.41 In the past 5 years, predictive, preventative, and personalized medicine methods have evolved from identifying specific mutations to targeting specific genes, including identifying N7-methylguanosine modification and cell-free nucleic acids with various technologies, and their validation in the role of brain involvement prediction in breast cancer is required.43–45
Strengths of this study include up-to-date real-world data representative of the general population which is linked to mortality data in this comprehensive database. Limitations include the retrospective nature of the study and the small number of patients involved. All patients identified for the study period were included (ie, the entire population) and hence this small population points to the rarity of the condition. In addition, due to a regulatory limitation that prohibits collection of HER2+ data, we used trastuzumab purchases as a proxy for HER2+ disease, which is reasonable due to the regulatory limitations and necessary approval from the MHS Drug Approval Committee in order to treat these patients. We identified brain metastases from procedures to the central nervous system (radiation or surgery), and it is possible that we missed patients that did not receive any therapy or included those that did not have brain metastases. Excluding patients who did not receive any local therapy for brain metastases or who were too sick to receive local treatment would exclude those with a poor prognosis and affect the survival outcomes reported in this study.
In addition, this study did not include patients with leptomeningeal disease, which occurs in about 10–25% of patients with mBC and CNS metastases.46 These patients have a poor prognosis (with a life expectancy of 1.75–4.5 months) and limited treatment options, though a recent report of seven patients included in the DEBBRAH study and treated with T-DXd suggested a favorable outcome with this regimen.47
Conclusion
This cohort describes treatment benefit as assessed by time on treatment and overall survival of patients with HER2+ mBC+ and brain metastases treated since 2013 with upfront TPC and mostly T-DM1 in the second-line setting. While patients with upfront brain involvement at time of mBC diagnosis had shorter survival compared with those starting TPC with no brain metastases, overall findings compare favorably with historical controls and demonstrate improvements in the management of these patients in recent years. Our results provide excellent base-line/historical outcome data and could be used for future comparisons of patients switched to second-line therapy with T-DXd or tucatinib, and for further addressing the added-value of the care of those patients.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due to the Israeli Ministry of Health and MHS’s data privacy policy but are available from the corresponding author on reasonable request.
Ethics Approval
The study was approved by the local ethics review board of MHS in Israel.
Consent to Participate
Consent was waived by the ethics review board of Maccabi Healthcare Services in Israel due to the retrospective nature of this study.
Acknowledgments
The abstract of this paper was published in “Poster Abstracts” in the Journal of Clinical Oncology for the 2023 ASCO Annual Meeting: Hyperlink with DOI: https://ascopubs.org/doi/abs/10.1200/JCO.2023.41.16_suppl.e13040.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was sponsored by AstraZeneca, Israel.
Disclosure
Idit Livnat, Roni Ginsburg, and Adva Yarden are employees of AstraZeneca Israel. The other authors declare they have no conflicts of interest in this work.
References
1. Wolff AC, Hammond MEH, Hicks DG., et al. recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American society of clinical oncology/college of American pathologists clinical practice guideline update. Arch Pathol Lab Med. 2014;138(2):241–256. doi:10.5858/arpa.2013-0953-SA
2. NCCN. Breast Cancer Version 1.2019; 2019.
3. Slamon DJ, Clark GM, Wong SG, Levin WJ, Ullrich A, McGuire WL. Human breast cancer: correlation of relapse and survival with amplification of the HER-2/ neu Oncogene. science. 1987;235(4785):177–182. doi:10.1126/science.3798106
4. Swain SM, Baselga J, Kim S-B, et al. Pertuzumab, trastuzumab, and docetaxel in HER2-positive metastatic breast cancer. N Engl J Med. 2015;372(8):724–734. doi:10.1056/NEJMoa1413513
5. Pestalozzi BC, Holmes E, de Azambuja E, et al. CNS relapses in patients with HER2-positive early breast cancer who have and have not received adjuvant trastuzumab: a retrospective substudy of the HERA trial (BIG 1-01). Lancet Oncol. 2013;14(3):244–248. doi:10.1016/S1470-2045(13)70017-2
6. Gennari A, André F, Barrios C, et al. ESMO Clinical practice guideline for the diagnosis, staging and treatment of patients with metastatic breast cancer☆. Ann Oncol. 2021;32:1475–1495.
7. Bendell JC, Domchek SM, Burstein HJ, et al. Central nervous system metastases in women who receive trastuzumab‐based therapy for metastatic breast carcinoma. Cancer. 2003;97(12):2972–2977. doi:10.1002/cncr.11436
8. Altaha R, Crowell E, Ducatman B, Higa G, Abraham J. Risk of brain metastases in HER2/neu-positive breast cancer. J clin oncol. 2004;22(14_suppl):682. doi:10.1200/jco.2004.22.90140.682
9. Clayton AJ, Danson S, Jolly S, et al. Incidence of cerebral metastases in patients treated with trastuzumab for metastatic breast cancer. Br. J. Cancer. 2004;91(4):639–643. doi:10.1038/sj.bjc.6601970
10. Brosnan EM, Anders CK. Understanding patterns of brain metastasis in breast cancer and designing rational therapeutic strategies. Ann Translat Med. 2018;6(9):163. doi:10.21037/atm.2018.04.35
11. Kennecke H, Yerushalmi R, Woods R, et al. Metastatic behavior of breast cancer subtypes. J Clin Oncol. 2010;28(20):3271–3277. doi:10.1200/JCO.2009.25.9820
12. Pestalozzi BC, Brignoli S. Trastuzumab in CSF. J Clin Oncol. 2000;18(11):2349–2351. doi:10.1200/JCO.2000.18.11.2349
13. Stemmler J, Schmitt M, Willems A, Bernhard H, Harbeck N, Heinemann V. Brain metastases in HER2-overexpressing metastatic breast cancer: comparative analysis of trastuzumab levels in serum and cerebrospinal fluid. J Clin Oncol. 2006;24(18_suppl):1525. doi:10.1200/jco.2006.24.18_suppl.1525
14. Zimmer AS, Van Swearingen AE, Anders CK. HER2‐positive breast cancer brain metastasis: a new and exciting landscape. Cancer Rep. 2022;5:e1274.
15. Galanti D, Inno A, La Vecchia M, et al. Current treatment options for HER2-positive breast cancer patients with brain metastases. Crit Rev Oncol Hematol. 2021;161:103329. doi:10.1016/j.critrevonc.2021.103329
16. Anders CK. Management of brain metastases in breast cancer. Clin Adv Hematol Oncol. 2016;14:686–688.
17. Lin NU, Winer EP. Brain metastases: the HER2 paradigm. Clin Cancer Res. 2007;13(6):1648–1655. doi:10.1158/1078-0432.CCR-06-2478
18. Klos KJ, O’Neill BP. Brain metastases. Neurologist. 2004;10(1):31–46. doi:10.1097/01.nrl.0000106922.83090.71
19. Niikura N, Hayashi N, Masuda N, et al. Treatment outcomes and prognostic factors for patients with brain metastases from breast cancer of each subtype: a multicenter retrospective analysis. Breast Cancer Res Treat. 2014;147(1):103–112. doi:10.1007/s10549-014-3090-8
20. Aversa C, Rossi V, Geuna E, et al. Metastatic breast cancer subtypes and central nervous system metastases. Breast. 2014;23(5):623–628. doi:10.1016/j.breast.2014.06.009
21. Sperduto PW, Kased N, Roberge D, et al. The effect of tumor subtype on the time from primary diagnosis to development of brain metastases and survival in patients with breast cancer. J Neuro-oncol. 2013;112(3):467–472. doi:10.1007/s11060-013-1083-9
22. Hurvitz SA, Hegg R, Chung W-P, et al. Trastuzumab deruxtecan versus trastuzumab emtansine in patients with HER2-positive metastatic breast cancer: updated results from DESTINY-Breast03, a randomised, open-label, Phase 3 trial. Lancet. 2022;2:5
23. Curigliano G, Mueller V, Borges V, et al. Tucatinib versus placebo added to trastuzumab and capecitabine for patients with pretreated HER2+ metastatic breast cancer with and without brain metastases (HER2CLIMB): final overall survival analysis. Ann Oncol. 2022;33(3):321–329. doi:10.1016/j.annonc.2021.12.005
24. Rosen B, Waitzberg R, Merkur S. Health systems in transition. Israel. 2015;1:3
25. Shalev V, Chodick G, Goren I, Silber H, Kokia E, Heymann AD. The use of an automated patient registry to manage and monitor cardiovascular conditions and related outcomes in a large health organization. Int J Cardiol. 2011;152(3):345–349. doi:10.1016/j.ijcard.2010.08.002
26. Chodick G, Heymann AD, Shalev V, Kookia E. The epidemiology of diabetes in a large Israeli HMO. Eur j epidemiol. 2003;18(12):1143–1146. doi:10.1023/B:EJEP.0000006635.36802.c8
27. Goldshtein I, Chandler J, Shalev V, et al. Osteoporosis in the community: findings from a novel computerized registry in a large Health Organization in Israel. J Aging Res Clin Pract. 2015;3:4.
28. Israel Central Bureau of Statistics. Characterization and Classification of Geographic Units by the Soci-Economic Level of the Population 2008. Publication No. 1530. Jerusalem, Israel: Israel Central Bureau of Statistics; 2013.
29. Machado M, de Moura CS, Chan K, et al. Real-world analyses of therapy discontinuation of checkpoint inhibitors in metastatic melanoma patients. Sci Rep. 2020;10(1):14607. doi:10.1038/s41598-020-71788-z
30. Pan X, Lin M, Yin Y, Hou P, Baumann P, Jahanzeb M. Real-world immuno-oncology (IO) therapy treatment patterns and outcomes in patients with anaplastic lymphoma kinase positive (ALK+) non-small cell lung cancer (NSCLC) in the United States. Ann Oncol. 2019;30:ii52–ii3.
31. Moser SS, Apter L, Arunachalam A, et al. Real-world study of PD-L1 testing patterns and treatment distribution in patients with metastatic non-small-cell lung cancer in Israel. Immunotherapy. 2021;13(10):851–861. doi:10.2217/imt-2020-0347
32. Amiri-Kordestani L, Wilkerson J, Balasubramaniam S, Bates SE, Fojo AT. Difference between duration of treatment (DOT) and progression-free survival (PFS) as a marker of unbalanced censoring. J clin oncol. 2012;30(15_suppl):2548. doi:10.1200/jco.2012.30.15_suppl.2548
33. FOCR. Establishing a framework to evaluate real-world endpoints; 2018.
34. Velcheti V, Chandwani S, Chen X, Pietanza MC, Burke T. First-line pembrolizumab monotherapy for metastatic PD-L1-positive NSCLC: real-world analysis of time on treatment. Immunotherapy. 2019;11(10):889–901. doi:10.2217/imt-2019-0061
35. Baselga J, Cortés J, Kim S-B, et al. Pertuzumab plus trastuzumab plus docetaxel for metastatic breast cancer. N Engl J Med. 2012;366(2):109–119. doi:10.1056/NEJMoa1113216
36. Ramakrishna N, Anders CK, Lin NU, et al. Management of advanced human epidermal growth factor receptor 2–positive breast cancer and brain metastases: ASCO guideline update. J clin oncol. 2022;40(23):2636–2655. doi:10.1200/JCO.22.00520
37. Diéras V, Miles D, Verma S, et al. Trastuzumab emtansine versus capecitabine plus lapatinib in patients with previously treated HER2-positive advanced breast cancer (EMILIA): a descriptive analysis of final overall survival results from a randomised, open-label, phase 3 trial. Lancet Oncol. 2017;18(6):732–742. doi:10.1016/S1470-2045(17)30312-1
38. Brufsky AM, Mayer M, Rugo HS, et al. Central nervous system metastases in patients with HER2-positive metastatic breast cancer: incidence, treatment, and survival in patients from registHER. Clin Cancer Res. 2011;17(14):4834–4843. doi:10.1158/1078-0432.CCR-10-2962
39. Murthy RK, Loi S, Okines A, et al. Tucatinib, trastuzumab, and capecitabine for HER2-positive metastatic breast cancer. N Engl J Med. 2020;382(7):597–609. doi:10.1056/NEJMoa1914609
40. Lin NU, Borges V, Anders C, et al. Intracranial Efficacy and Survival With Tucatinib Plus Trastuzumab and Capecitabine for Previously Treated HER2-Positive Breast Cancer With Brain Metastases in the HER2CLIMB Trial. J clin oncol. 2020;38(23):2610–2619. doi:10.1200/JCO.20.00775
41. Polivka J, Kralickova M, Polivka J, Kaiser C, Kuhn W, Golubnitschaja O. Mystery of the brain metastatic disease in breast cancer patients: improved patient stratification, disease prediction and targeted prevention on the horizon? EPMA J. 2017;8(2):119–127. doi:10.1007/s13167-017-0087-5
42. Kapinova A, Mazurakova A, Halasova E, et al. Underexplored reciprocity between genome-wide methylation status and long non-coding RNA expression reflected in breast cancer research: potential impacts for the disease management in the framework of 3P medicine. EPMA J. 2023;14(2):249–273. doi:10.1007/s13167-023-00323-7
43. Huang X, Chen Z, Xiang X, et al. Comprehensive multi-omics analysis of the m7G in pan-cancer from the perspective of predictive, preventive, and personalized medicine. EPMA J. 2022;13(4):671–697. doi:10.1007/s13167-022-00305-1
44. Crigna AT, Samec M, Koklesova L, et al. Cell-free nucleic acid patterns in disease prediction and monitoring-hype or hope? EPMA J. 2020;11(4):603–627. doi:10.1007/s13167-020-00226-x
45. Mazurakova A, Koklesova L, Samec M, et al. Anti-breast cancer effects of phytochemicals: primary, secondary, and tertiary care. EPMA J. 2022;13(2):315–334. doi:10.1007/s13167-022-00277-2
46. Figura NB, Rizk VT, Armaghani AJ, et al. Breast leptomeningeal disease: a review of current practices and updates on management. Breast Cancer Res Treat. 2019;177(2):277–294. doi:10.1007/s10549-019-05317-6
47. Pérez-García JM, Batista MV, Cortez-Castedo P, et al. Abstract PD7-02: trastuzumab deruxtecan in patients with unstable central nervous system involvement from HER2-Low Advanced Breast Cancer: the DEBBRAH trial. Cancer Res. 2023;83(5_Supplement):PD7. doi:10.1158/1538-7445.SABCS22-PD7-02
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.