")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 15
Clinical, Economic, and Humanistic Outcomes Associated with Obesity Among People with Bipolar I Disorder in the United States: Analysis of National Health and Wellness Survey Data
Authors Doane MJ, Thompson J, Jauregui A, Gasper S, Csoboth C
Received 29 March 2023
Accepted for publication 30 August 2023
Published 18 September 2023 Volume 2023:15 Pages 681—689
DOI https://doi.org/10.2147/CEOR.S411928
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Giorgio Colombo
Michael J Doane,1 Jeffrey Thompson,2 Adam Jauregui,2 Sabina Gasper,1 Csilla Csoboth1
1Alkermes, Inc., Waltham, MA, USA; 2Cerner Enviza, North Kansas City, MO, USA
Correspondence: Michael J Doane, Health Economics and Outcomes Research, Alkermes, Inc, 825 Winter Street, Waltham, MA, 02451-1420, USA, Tel +1-781-290-7183, Email [email protected]
Introduction: People living with bipolar I disorder (BD-I) have an increased risk for obesity compared with the general population that may be related to genetic, lifestyle, and treatment factors. Few studies have examined possible effects of obesity on those living with BD-I. This study examined relationships between obesity and clinical, humanistic, and economic outcomes among adults with BD-I.
Methods: This retrospective, cross-sectional study analyzed survey responses from a nationally representative sample of US adults participating in the 2016 or 2020 National Health and Wellness Survey. Respondents (18– 64 years) with a self-reported physician diagnosis of BD-I were included and categorized by body mass index: underweight/normal weight (< 25 kg/m2), overweight (25 to < 30 kg/m2), or obese (≥ 30 kg/m2). Adjusted analyses assessed comorbidities, health-related quality of life (HRQoL), work productivity, health care resource utilization (HCRU), and economic outcomes.
Results: In total, responses from 1,853 participants were analyzed; most were female (65%) and white (62%). Respondents with obesity had the highest prevalence of medical comorbidities, including high blood pressure (52%), sleep apnea (37%), hypercholesterolemia (34%), and type 2 diabetes (12%). Obesity was generally associated with the lowest scores of physical health and HRQoL. Activity impairment scores were highest among respondents with obesity, as were numbers of hospitalizations and emergency department visits in the previous 6 months. Respondents with obesity incurred higher annual indirect and direct medical costs ($28,178 and $37,771, respectively) when compared with the underweight/normal weight ($23,823 and $32,227, respectively) and overweight ($24,312 and $35,231, respectively) groups.
Conclusion: In this nationally representative sample, obesity was associated with several outcomes that may negatively affect people living with BD-I, including medical comorbidities, higher HCRU, HRQoL impairments, and greater indirect and direct medical costs. These findings highlight the importance of considering the presence of or risk for obesity and associated medical comorbidities when treating BD-I.
Keywords: body mass index, comorbidity, health care costs, health-related quality of life
Introduction
People living with bipolar I disorder (BD-I) have an increased risk of obesity compared with the general population.1 Increased body weight is a significant risk factor for developing cardiovascular disease, a leading cause of morbidity and mortality in people with BD-I.2–4 Higher body mass index (BMI), specifically obesity, is associated with adverse cardiometabolic outcomes, including hypertension, dyslipidemia, type 2 diabetes, coronary heart disease, and stroke.5
Genetic and lifestyle factors contribute to the increased risk of obesity in people with BD-I. For example, female sex has been associated with a greater risk of obesity in this population,1,6 while suboptimal diet and exercise habits in people with BD-I may also contribute.7 Additionally, treatment-related factors, including the weight gain liability of many antipsychotic medications, antidepressants, and mood stabilizers, may increase the risk of obesity.8–10 Weight gained during antipsychotic treatment often persists even after discontinuing or switching treatment and is cited as one of the most common and bothersome adverse effects experienced by patients.11,12
Negative effects of weight gain among people with BD-I may include increased clinical burden, increased health care resource utilization (HCRU), and reduced health-related quality of life (HRQoL).12–14 Despite the link between BD-I and obesity, few studies have examined the outcomes associated with obesity in this population. In this study, we investigated the associations between obesity and clinical, humanistic, and economic outcomes among adults with BD-I.
Methods
This study was a retrospective, cross-sectional analysis of responses to the 2016 or 2020 National Health and Wellness Survey (NHWS). The NHWS is a self-administered, internet-based survey conducted annually among a nationally representative sample of adults in the United States based on age, sex, and race. The survey includes information on self-reported health outcomes, medical conditions, and HCRU. Study procedures were reviewed by the Pearl Institutional Review Board (Indianapolis, IN), which provided an exempt status for this study per Federal Regulation 45 CFR 46 Subpart A §46.104(d)(2) governing deidentified survey data.15
Respondents aged 18 to 64 years who self-reported a physician diagnosis of BD-I were included in the analysis. Data from 2016 and 2020 were combined, as respondents with a diagnosis of bipolar disorder provided specific subtype information in those years (eg, BD-I vs BD-II). A total of 21 respondents completed both the 2016 and 2020 NHWS but were excluded from the final analysis because of data concerns (ie, inconsistent responses regarding bipolar subtype and/or chronic medical diagnoses across the 2 years).
Primary Analysis
Respondents were categorized by BMI: underweight/normal weight (<25 kg/m2), overweight (25 to <30 kg/m2), or obese (≥30 kg/m2). Physician diagnoses of obesity-related medical comorbidities, including high blood pressure, hypercholesterolemia, type 2 diabetes, cardiovascular events (ministroke, stroke, heart attack, or congestive heart failure), asthma, liver disease, cancer, osteoarthritis, and sleep apnea, were assessed according to patients’ self-report.
Evaluations of HRQoL were conducted using the 36-item Short Form Version 2 (SF-36v2) and the EuroQol EQ-5D health surveys. Physical and Mental Component summary scores from the SF-36v2 were calculated using a norm-based scoring algorithm. Specifically, a linear T-score transformation was employed so that the mean of each summary score was set at 50, representing the population mean for the US population, with an SD set at 10. Lower scores represented worse health status in both surveys.
Work productivity was assessed using the Work Productivity and Activity Impairment (WPAI) questionnaire. The WPAI questionnaire consists of the following 4 scales: absenteeism (missed work due to illness), presenteeism (lost productivity at work), overall work impairment (absenteeism and presenteeism combined), and activity impairment (health-related impairment in daily activities). Work impairment questions were assessed among respondents who were employed at the time of the survey, while activity impairment questions were asked of all respondents. Higher scores on the WPAI scales represent greater levels of impairment. Total indirect costs, as well as indirect costs associated with absenteeism and presenteeism, were estimated using 2019 hourly wage data from the US Bureau of Labor Statistics16 and by extrapolating the number of self-reported work hours affected among respondents who were employed.
HCRU (hospitalizations, emergency department [ED] visits, and visits to health care professionals) in the previous 6 months were also assessed. Direct medical costs associated with HCRU were estimated from the 2018 Medical Expenditure Panel Survey17 and based on national cost averages.
Statistical Analysis
Multivariable regression models were used to adjust study outcomes for age, sex, race, residential status, marital status, education, employment status, insurance status, smoking status, alcohol use, exercise frequency, and modified Charlson Comorbidity Index. To control for the potential effect of the COVID-19 pandemic on study outcomes, NHWS year (2016 vs 2020) was also included as a covariate in regression models.
Study outcomes, including frequency and percentage for categorical outcomes as well as mean and SD/SEM for continuous outcomes, were summarized descriptively; no formal hypothesis testing is reported across the 3 BMI subgroups.
A sensitivity analysis was conducted with obesity further stratified by class. The following 5 subgroups were included in the sensitivity analysis: underweight/normal weight, overweight, obese class 1 (BMI: 30 to <35 kg/m2), obese class 2 (BMI: 35 to <40 kg/m2), and obese class 3 (BMI: ≥40 kg/m2).
Results
Respondent Demographics
A total of 1,853 respondents reported having received a physician diagnosis of BD-I and completed the 2016 or 2020 NHWS (Table 1 and Supplemental Table 1). Of these respondents, 29.7% were underweight/normal weight, 25.5% were overweight, and 44.8% were obese. Their mean (SD) age was 34.1 (12.6) years, and most respondents were female (65%) and white (62%). The majority of respondents (82%) lived in an urban area, and 45% reported being married or living with a partner; 46% had completed some college or obtained their associate degrees. Commercial insurance coverage was reported by 35% of respondents, while coverage by Medicaid or Medicare was reported by 24% and 23%, respectively. Overall, 63% used alcohol, and 45% were current smokers. The mean (SD) modified Charlson Comorbidity Index was 0.38 (1.12). Fewer than half (46%) of all respondents were employed at the time of the survey; obese patients with BD-I had the lowest rate of employment (42%) compared with the overweight (48%) and underweight/normal weight (50%) groups. Overall, 19% of respondents were on short- or long-term disability, with higher rates noted for respondents with obesity (24%) compared with overweight (19%) and underweight/normal weight (12%) respondents. Overall, 50% of respondents reported actively trying to lose weight; the proportion was highest among those with obesity (66%) compared with overweight (54%) and underweight/normal weight (24%) respondents. Despite efforts to lose weight, fewer obese respondents reported exercising vigorously in the previous month (51%) in comparison with those who were overweight (61%) or underweight/normal weight (63%).
 |
Table 1 Respondent Demographics |
Medical Comorbidities
Compared with those who were underweight/normal weight or overweight, respondents with obesity had the highest adjusted prevalence of high blood pressure (52%), sleep apnea (37%), hypercholesterolemia (34%), cardiovascular events (ie, ministroke, stroke, or congestive heart failure; 15%), and type 2 diabetes (12%) (Figure 1). The adjusted prevalence estimates of asthma (29%), osteoarthritis (16%), and liver disease (6%) were also highest in respondents with obesity.
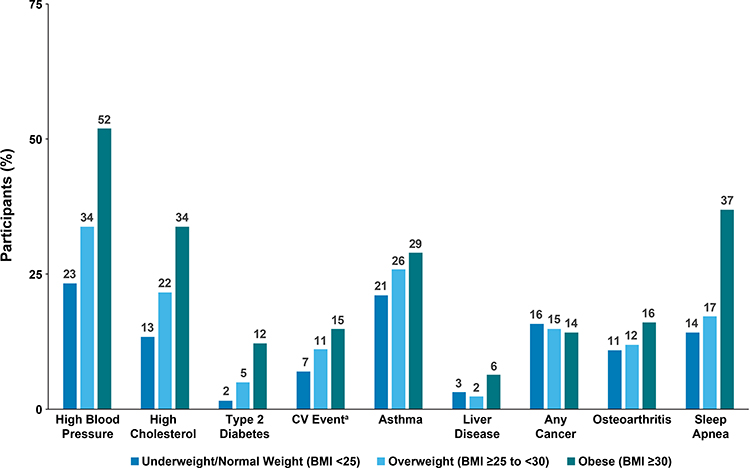 |
Figure 1 Adjusted proportions of self-reported obesity-related medical comorbidities. Abbreviations: BMI, body mass index; CV, cardiovascular; NHWS, National Health and Wellness Survey. Notes: Adjusted for age, sex, race, residential status, marital status, education, employment status, insurance status, smoking status, alcohol use, exercise frequency, modified Charlson Comorbidity Index, and NHWS year. aIncludes ministroke, stroke, heart attack, or congestive heart failure. |
Health-Related Quality of Life
Obesity was generally associated with lower physical health and HRQoL scores on the SF-36v2 and EQ-5D, respectively, compared with overweight or underweight/normal weight status (Table 2 and Supplemental Table 2). On the Physical Component Summary of the SF-36v2, the mean (SEM) score for respondents with obesity (40.6 [0.72]) was lower than the scores of those who were overweight (42.5 [0.78]) or underweight/normal weight (44.3 [0.75]). Although scores on the Mental Component Summary of the SF-36v2 were similar across the 3 BMI groups, they were lower than the population mean of 50 for US adults across each group. The mean (SEM) score on the EQ-5D was 0.62 (0.01) for respondents with obesity versus scores of 0.65 (0.01) for overweight and 0.67 (0.01) for underweight/normal weight respondents.
 |
Table 2 Adjusted Health-Related Quality of Life and Work Productivity Scoresa |
Work Productivity and Indirect Costs
A total of 807 employed survey respondents completed the work-related items of the WPAI questionnaire (Table 2). Mean (SEM) absenteeism scores were similar for respondents who were underweight/normal weight or obese (37.1% [4.70] and 36.4% [4.63], respectively) but were lowest for respondents who were overweight (31.7% [4.62]). A similar pattern was observed for presenteeism; respondents who were underweight/normal weight or obese had similar mean presenteeism (SEM) scores (56.2% [4.12] and 56.1% [4.14], respectively), with the lowest scores for respondents who were overweight (52.7% [4.14]). Likewise, mean (SEM) scores of overall work impairment were higher for those who were underweight/normal weight or obese (64.3% [1.05] and 64.2% [1.07], respectively) than for those who were overweight (58.9% [1.06]). Among all respondents, activity impairment scores were highest in respondents who were obese. Mean (SEM) activity impairment scores were 62.2% (2.49) for respondents with obesity compared with 58.8% (2.59) and 58.0% (2.42) for overweight and underweight/normal weight respondents, respectively.
Obesity was associated with the highest estimates of indirect medical costs (Figure 2). Annual indirect cost estimates of absenteeism and presenteeism were $15,688 and $17,063, respectively, among respondents with BD-I and obesity. Total indirect costs were estimated to be $28,178 per year for respondents with obesity. Obese respondents with BD-I had excess associated total indirect costs that were $3,867 and $4,356 higher, respectively, than annual costs for respondents who were overweight or underweight/normal weight.
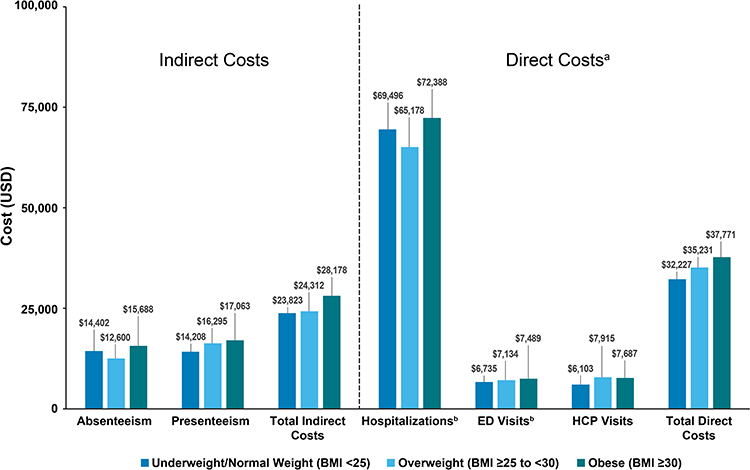 |
Figure 2 Adjusted direct and indirect costs (in USD), annualized. Abbreviations: BMI, body mass index; ED, emergency department; HCP, health care professional; NHWS, National Health and Wellness Survey; USD, US dollars. Notes: Adjusted for age, sex, race, residential status, marital status, education, employment status, insurance status, smoking status, alcohol use, exercise frequency, modified Charlson Comorbidity Index, and NHWS year. aAnalyzed using a generalized linear model with a negative binomial distribution. bAnalyzed using a zero-inflated model with a negative binomial distribution. |
HCRU and Direct Costs
Data on HCRU in the 6 months before survey participation are presented in Table 3 and Supplemental Table 3. The average numbers of both hospitalizations and ED visits were highest among respondents with obesity. The mean (SEM) number of hospitalizations for respondents with obesity was 0.84 (0.16) versus 0.72 (0.15) and 0.80 (0.16) for overweight and underweight/normal weight respondents, respectively. The mean (SEM) number of ED visits for respondents with obesity was 1.58 (0.23) compared with 1.44 (0.23) and 1.23 (0.19) for overweight and underweight/normal weight respondents, respectively. Overall, the numbers of visits to any health care professional were high in respondents with BD-I across the BMI categories. The mean (SEM) numbers of visits to health care professionals in the 6 months prior to survey completion were 9.67 (0.85) (underweight/normal weight), 12.55 (1.15) (overweight), and 12.26 (1.03) (obese).
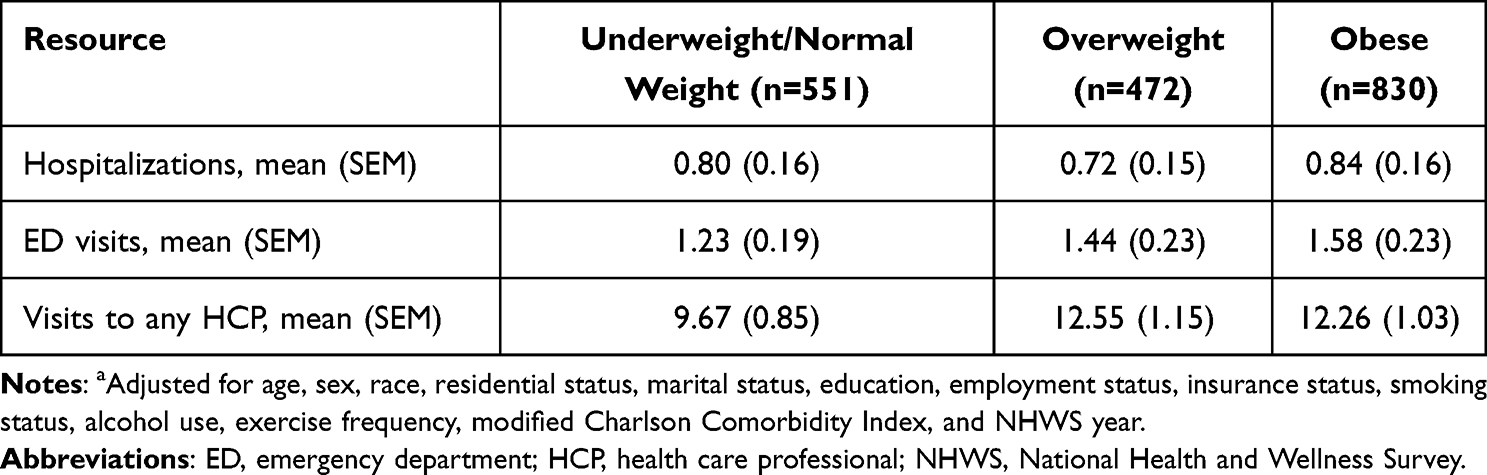 |
Table 3 Adjusted Health Care Resource Use, Previous 6 Monthsa |
Obesity was also associated with higher direct medical costs for respondents with BD-I than for those who were overweight or underweight/normal weight (Figure 2). Obesity was associated with the highest total direct medical costs ($37,771) annually, with the excess estimated to be $2,540 and $5,544 higher, respectively, than for those who were overweight or underweight/normal weight.
Sensitivity Analysis
The results of the sensitivity analysis with obesity stratified by class were consistent with those of the primary analysis (Supplemental Figures 1 and 2). In general, respondents who were in obesity class 3 reported the highest prevalence of several medical comorbidities and lower HRQoL scores than those of respondents in obesity class 1 or 2. Scores of absenteeism, overall work impairment, and activity impairment were highest among respondents in obesity class 3. Obesity class 3 was also associated with the highest estimates of obesity-related absenteeism and total indirect costs. The average numbers of hospitalizations and ED visits in the previous 6 months were highest in respondents in obesity class 2, while respondents in obesity class 3 reported the highest number of visits to any health care professional in the 6 months prior to survey participation. Obesity classes 2 and 3 were associated with the highest estimated hospitalization costs, as well as total direct medical costs.
Discussion
In the current study, obesity was associated with several outcomes that appear to negatively affect people living with BD-I. When the analysis was adjusted for demographic and health characteristics, respondents with obesity reported the highest prevalence of high blood pressure, sleep apnea, hypercholesterolemia, type 2 diabetes, asthma, osteoarthritis, and liver disease compared with those who were underweight/normal weight or overweight. Respondent self-assessment scores indicated poorer physical health and overall HRQoL among respondents with obesity compared with those in the other groups. Survey respondents with BD-I and obesity had the highest activity impairment scores. Overall, numbers of visits to any health care professional in the previous 6 months were high across the 3 BMI categories, but obesity was associated with the highest average numbers of hospitalizations and ED visits. In addition, obesity was associated with higher healthcare costs compared with those who were overweight or underweight/normal weight.
The prevalence of cardiometabolic comorbidities, low HRQoL, and higher estimated medical costs observed in obese patients with BD-I in this analysis align with those found in previous studies of the clinical, humanistic, and economic burdens of obesity in people living with BD-I. Cardiovascular disease is a leading cause of morbidity and mortality in people with BD-I,2–4 and the development of obesity-related cardiometabolic comorbidities that may emerge secondary to weight gain from antipsychotic and mood stabilizer treatments significantly increases HCRU and direct medical costs.13,18 Antipsychotic-associated weight gain is reported consistently by patients as bothersome and often persists despite potential efforts (eg, discontinuation, switching) to manage or reverse it.11,12 The physical functioning and work productivity impairments reported here are also consistent with previously reported findings in people with BD-I and obesity.19,20 Additionally, obesity is associated with increased severity of BD-I symptoms and less improvement in functioning and life satisfaction even after treatment with antipsychotic medication(s).14
Several strengths of this study are worth mentioning. The NHWS is a survey conducted among a nationally representative sample of US adults who were recruited and stratified based on sex, age, and race. Thus, the results may be generalizable to a larger population of patients with BD-I. Because only respondents with a self-reported diagnosis of BD-I were included, the reported outcomes are specific to BD-I and not bipolar disorder in general or other subtypes of bipolar disorder. By controlling for demographic and health characteristics, we were able to capture unique relationships between obesity and study outcomes. In addition, data and associated outcomes were reported by the patients, which may be difficult to capture via other types and sources of data.
Limitations
Limitations of the current study should be noted. This analysis was cross-sectional; therefore, no causal links between obesity and reported outcomes can be made. However, obesity is associated with an increased risk for many of the medical comorbidities21 that were found with higher prevalence in obese patients with BD-I than in those who were in a lower BMI category. Because the NHWS is a self-reported survey, responses could not be validated. For example, survey respondents may have underreported their weight, leading to BMI category misclassification and potential underestimation of the relationship between BMI and study outcomes. Medication history was not available for both years of the NHWS; therefore, we were unable to control for this variable. Furthermore, study outcomes were not compared between respondents with or without BD-I. Living with BD-I may be associated with additional burdens not captured in this analysis.
Conclusions
There are important clinical, humanistic, and economic outcomes associated with obesity in adults living with BD-I. Obesity may adversely affect adults living with BD-I by potentially increasing their risk of medical comorbidities, increasing HCRU, lowering quality of life, and increasing indirect and direct medical costs. These findings illustrate the importance of considering weight gain and associated medical comorbidities in treatment decisions for people living with BD-I.
Abbreviations
BD-I, bipolar I disorder; BMI, body mass index; CFR, Code of Federal Regulations; ED, emergency department; HCRU, health care resource utilization; HRQoL, health-related quality of life; NHWS, National Health and Wellness Survey; SF-36v2, 36-item Short Form Version 2; WPAI, Work Productivity and Activity Impairment.
Data Sharing Statement
Data for these analyses were made available to the authors through third-party license from Cerner Enviza, a commercial data provider in the United States. As such, the authors cannot make these data publicly available. Other researchers can access these data by purchasing a license through Cerner Enviza. Inclusion criteria specified in the Methods section would allow other researchers to identify the same cohort of patients we used for these analyses. Interested individuals may refer to https://www.cernerenviza.com/real-world-data/national-health-and-wellness-survey-nhws for more information on accessing these data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosures
M.J. Doane, S. Gasper, and C. Csoboth are or were employees of Alkermes, Inc., and may own stock/options in the company. J. Thompson and A. Jauregui are or were at the time of the study employed by Cerner Enviza, which received payment from Alkermes, Inc., for participation in conducting this research. The authors report no other conflicts of interest in this work.
Funding
This study was sponsored by Alkermes, Inc. Medical writing and editorial support were provided by Omar H. Cabrera, PhD, and John H. Simmons, MD, of Peloton Advantage, LLC, an OPEN Health company, and funded by Alkermes, Inc.
References
1. Goldstein BI, Liu SM, Zivkovic N, Schaffer A, Chien LC, Blanco C. The burden of obesity among adults with bipolar disorder in the United States. Bipolar Disord. 2011;Vol. 13(4):387–395.
2. De Hert M, Correll CU, Bobes J, et al. Physical illness in patients with severe mental disorders. I. Prevalence, impact of medications and disparities in health care. World Psychiatry. 2011;10(1):52–77. doi:10.1002/j.2051-5545.2011.tb00014.x
3. Newcomer JW. Second-generation (atypical) antipsychotics and metabolic effects: a comprehensive literature review. CNS Drugs. 2005;19(Suppl 1):1–93. doi:10.2165/00023210-200519001-00001
4. Westman J, Hallgren J, Wahlbeck K, Erlinge D, Alfredsson L, Osby U. Cardiovascular mortality in bipolar disorder: a population-based cohort study in Sweden. BMJ Open. 2013;3(4):e002373. doi:10.1136/bmjopen-2012-002373
5. National Heart, Lung, and Blood Institute. Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults: the Evidence Report. In: NHLBI Obesity Education Initiative Expert Panel on the Identification, Evaluation, and Treatment of Obesity in Adults. Bethesda, MD: National Institutes of Health; 1998.
6. Baskaran A, Cha DS, Powell AM, Jalil D, McIntyre RS. Sex differences in rates of obesity in bipolar disorder: postulated mechanisms. Bipolar Disord. 2014;16(1):83–92. doi:10.1111/bdi.12141
7. Kilbourne AM, Rofey DL, McCarthy JF, Post EP, Welsh D, Blow FC. Nutrition and exercise behavior among patients with bipolar disorder. Bipolar Disord. 2007;9(5):443–452. doi:10.1111/j.1399-5618.2007.00386.x
8. Bak M, Fransen A, Janssen J, van Os J, Drukker M. Almost all antipsychotics result in weight gain: a meta-analysis. PLoS One. 2014;9(4):e94112. doi:10.1371/journal.pone.0094112
9. Holt RI, Peveler RC. Obesity, serious mental illness and antipsychotic drugs. Diabetes Obes Metab. 2009;11(7):665–679. doi:10.1111/j.1463-1326.2009.01038.x
10. McElroy SL. Obesity in patients with severe mental illness: overview and management. J Clin Psychiatry. 2009;70(Suppl 3):12–21. doi:10.4088/JCP.7075su1c.03
11. Bessonova L, Velligan DI, Weiden PJ, et al. Antipsychotic treatment experiences of people with bipolar I disorder: patient perspectives from an online survey. BMC Psychiatry. 2020;20(1):354. doi:10.1186/s12888-020-02767-x
12. Doane MJ, Bessonova L, Friedler HS, et al. Weight gain and comorbidities associated with oral second-generation antipsychotics: analysis of real-world data for patients with schizophrenia or bipolar I disorder. BMC Psychiatry. 2022;22(1):114. doi:10.1186/s12888-022-03758-w
13. Bessonova L, Ogden K, Doane MJ, O’Sullivan AK, Tohen M. The economic burden of bipolar disorder in the United States: a systematic literature review. Clinicoecon Outcomes Res. 2020;12:481–497. doi:10.2147/CEOR.S259338
14. McElroy SL, Kemp DE, Friedman ES, et al. Obesity, but not metabolic syndrome, negatively affects outcome in bipolar disorder. Acta Psychiatr Scand. 2016;133(2):144–153. doi:10.1111/acps.12460
15. US Department of Health and Human Services. §46 104 exempt research. Code of federal regulations; 1982. Available from: https://www.ecfr.gov/current/title-45/subtitle-A/subchapter-A/part-46/subpart-A/section-46.104#p-46.104(d)(7).
16. US Bureau of Labor Statistics. Highlights of women’s earnings in 2019. Report 1089; 2020. Available from: https://www.bls.gov/opub/reports/womens-earnings/2019/home.htm.
17. Mean expenditure per event by event type and age groups, United States. Medical expenditure panel survey; 2018. Available from: https://datatools.ahrq.gov/meps-hc.
18. Crump C, Sundquist K, Winkleby MA, Sundquist J. Comorbidities and mortality in bipolar disorder: a Swedish national cohort study. JAMA Psychiatry. 2013;70(9):931–939. doi:10.1001/jamapsychiatry.2013.1394
19. Bond DJ, Kunz M, Torres IJ, Lam RW, Yatham LN. The association of weight gain with mood symptoms and functional outcomes following a first manic episode: prospective 12-month data from the Systematic Treatment Optimization Program for Early Mania (STOP-EM). Bipolar Disord. 2010;12(6):616–626. doi:10.1111/j.1399-5618.2010.00855.x
20. Kolotkin RL, Corey-Lisle PK, Crosby RD, et al. Impact of obesity on health-related quality of life in schizophrenia and bipolar disorder. Obesity. 2008;16(4):749–754. doi:10.1038/oby.2007.133
21. Hyppönen E, Mulugeta A, Zhou A, Santhanakrishnan VK. A data-driven approach for studying the role of body mass in multiple diseases: a phenome-wide registry-based case-control study in the UK Biobank. Lancet Digit Health. 2019;1(3):e116–e126. doi:10.1016/S2589-7500(19)30028-7
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.