")
Back to Journals » Journal of Hepatocellular Carcinoma » Volume 11
Clinical Characteristics of Non-B and Non-C Biopsy-Proven Primary Liver Cancers in an HBV- Endemic Area: A Retrospective Study
Received 31 January 2024
Accepted for publication 19 April 2024
Published 24 April 2024 Volume 2024:11 Pages 767—774
DOI https://doi.org/10.2147/JHC.S455741
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David Gerber
Zhen Hu, Huaying Zhou
Department of Infectious Diseases, The Second Xiangya Hospital, Central South University, Changsha, Hunan, 410011, People’s Republic of China
Correspondence: Huaying Zhou, Department of Infectious Diseases, The Second Xiangya Hospital, Central South University, Changsha, Hunan, 410011, People’s Republic of China, Email [email protected]
Objective: To explore the distribution of probable causes and clinical characteristics of non-B and non-C (NBNC) primary liver cancer (PLC) patients in the HBV-endemic region.
Methods: A total of 86 individuals with biopsy-proven NBNC-PLC were enrolled. NBNC-PLC patients were defined as negative for both anti-HCV antibodies and five serum hepatitis B markers. Patients’ characteristics were collected from medical records.
Results: Among them, most of the NBNC-PLC patients had intrahepatic cholangiocarcinoma (ICC) (81.4%), and 12.8% had hepatocellular carcinoma (HCC). The NBNC ICC group had more platelet count, GGT, and CA199 levels; approximately two-thirds were female, and it was more often present in patients with biliary inflammatory diseases, especially intrahepatic biliary lithiasis. The NBNC HCC group was older and had a higher proportion of dyslipidemia, obesity, cirrhosis, and AFP levels.
Conclusion: Our data revealed that most of the NBNC PLC patients were ICC. Female patients with biliary inflammatory diseases and higher CA199 levels had an increased risk of ICC, and patients with metabolic risk factors and elevated AFP levels were more likely to develop HCC. Additional research should be performed to verify this finding.
Keywords: non-B, non-C, primary liver cancers, hepatocellular carcinoma, intrahepatic cholangiocarcinoma, retrospective study
Introduction
Over the past few decades, there has been a marked increase in both the incidence and mortality of liver cancer. Primary liver malignancies are expected to become the second most common cause of cancer-related deaths in the United States by 2030.1 Hepatocellular carcinoma (HCC) is the most common type of primary liver cancer in adults, which accounts for about 80–90% of cases.2 Intrahepatic cholangiocarcinoma (ICC) is the second most prevalent primary liver cancer, accounting for 10–15% of the cases.
Hepatocellular carcinoma (HCC) is a classic example of a virus-related tumor.3 The geographical distribution of the hyper-endemic region of HCC coincides with that of chronic hepatitis B and C.4 As the implementation of neonatal HBV vaccination programmes and treatments for viral hepatitis become more available, HBV and HCV’s impact on the development of HCC is diminishing. Furthermore, it is widely recognized that it has a significant correlation with one’s lifestyle, metabolic factors (diabetes and obesity), and lifestyle factors (alcohol intake and smoking) have been linked to an increased risk of HCC.5–7
ICC arises near the segmental biliary channels. Most ICCs occur spontaneously and lack a discernible risk factor. Common risk factors for the development of ICC include chronic hepatitis and cirrhosis, infections caused by hepatobiliary flukes, biliary inflammatory diseases, primary biliary cholangitis, primary sclerosing cholangitis, cholelithiasis, bile duct adenoma, biliary papillomatosis, inflammatory bowel disease, drugs and toxins (Thorotrast), and others.8–11
In the present study, we explored the distribution of probable etiology and clinical characteristics of non-B and non-C (NBNC) primary liver cancer patients in the HBV-endemic region, with particular focus on biopsy-proven primary liver cancers.
Patients and Methods
Case Enrollment
This retrospective study was approved by the Second Xiangya Hospital of Central South University Ethics Committee. The requirement of informed consent was waived due to the retrospective nature of the study, the data was anonymized, and the absence of any risk.
We retrospectively gathered data from 1854 patients newly diagnosed with primary liver cancers from January 2015 to December 2021 at the Second Xiangya Hospitals, Central South University. A total of 1224 patients (66.0%) had PLC with positive hepatitis B markers (HBsAg or HBcAb), Of these, 204 patients (11.0%) also had positive anti-HCV antibodies, and 22 patients (1.2%) had both positive HBsAg and positive anti-HCV antibodies. 426 (22.9%) patients had NBNC PLC (hepatitis B markers—all negative and anti-HCV-negative) (Figure 1). Of the 426 individuals with NBNC PLC, 340 patients had either no liver pathological examination or Incomplete information. 86 were biopsy-diagnosed non-B, non-C (NBNC)-PLC, and the patients’ medical records were analyzed and assessed in the present study (Figure 2). We collected detailed information on NBNC PLC patients defined as negative for both five serum hepatitis B markers (anti-HBc, anti-HBe, HBsAg, HBeAg, and anti-HBs) and anti-HCV antibodies.
 |
Figure 1 Aetiology of 1854 patients with primary liver cancer (PLC), treated at the Second Xiangya Hospitals, Central South University from 2015 to 2021. The major cause of HCC is hepatitis B virus (HBV) infection, followed by non-B non-C (NBNC) and hepatitis C virus (HCV) infection. |
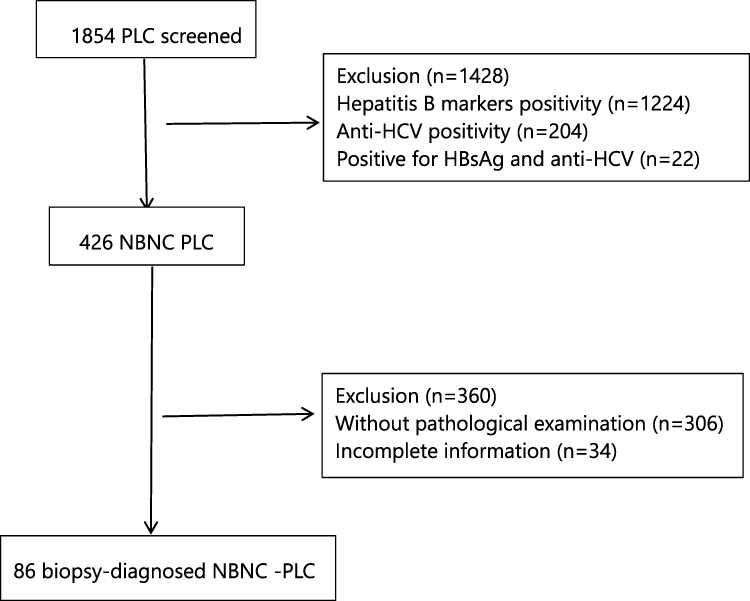 |
Figure 2 Flowchart of NBNC primary liver cancer screened. |
Data Collection
The following details at diagnosis were gathered: gender, age, body height, daily alcohol consumption, etiology of background liver disease; comorbidities such as fatty liver by ultrasonography, liver cirrhosis, hypertension, diabetes and dyslipidemia; bile duct stones; cholangitis; tumor information (tumor number, tumor size, satellite nodule, vascular invasion, tumor encapsulation, tumor stages, tumor differentiation, and Histopathology); symptoms such as ascites, laboratory data such as total bilirubin, alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), gamma- glutamyl transpeptidase (GGT), serum albumin, prothrombin activity, platelet count, cancer antigen 199 (CA199), alphafetoprotein (AFP), Barcelona- Clinic– Liver Cancer (BCLC) stages, and Child–Turcotte–Pugh (CTP) score. Dyslipidemia, hypertension, diabetes, and background liver disease were identified by the attending physician.
Statistical Analysis
Continuous data were presented as means ± SD (standard deviation), whereas categorical variables were presented as frequency and percentage. Differences between groups were assessed using one-way analysis of variance (ANOVA) for continuous data and the Chi-squared test for categorical data. P-values < 0.05 were deemed statistically significant. All analyses were carried out using IBM SPSS statistical software, version 26.0.
Results
Patient Profiles
Table 1 summarizes the clinical characteristics of the 86 enrolled individuals with NBNC PLC. The average age was 57.48 years, 87.2% were more than 50 years old, and about half (57%) were female. Chronic alcohol intake history was reported in 8.2% (7/86) of patients, obesity in 44.2%, diabetes in 23.3%, hypertension in 17.4%, and dyslipidemia in 37.2%. Overall, 77.9% (67/86) of NBNC PLC patients had a metabolic risk factor at the time of diagnosis. 9.3% showed significantly elevated AFP levels, and one-third (31.4%) had increased CA199. Only 11.6% had background cirrhosis, and 18.4% had Child-Pugh class B/C liver disease at the time of diagnosis. 73.3% of patients had a single nodular PLC, and 83.7% had a PLC with a maximum diameter of 5 cm or more. Gross portal vein invasion was seen in 34.9% (30/86) of patients. According to the BCLC stage, 45.4% and 54.6% of patients were in stages 0-B and C-D, respectively. The majority of NBNC-PLC patients were ICC (81.4%), 12.8% were HCC, and others accounted for 5.8%. 13.9% had poor tumor differentiation.
 |
Table 1 Characteristics of 86 Patients with Non-B Non-C Primary Liver Cancer |
Comparison of Clinical Features of NBNC-PLC Between ICC and HCC Groups
Table 2 evaluates the clinical characteristics of 70 individuals with NBNC ICC and 11 patients with NBNC HCC. Between the two groups, the NBNC ICC group showed a higher platelet count (P = 0.002), GGT (P = 0.016), and CA199 levels (P=0.002). Approximately two-thirds were females (P = 0.008) and were more common in individuals with biliary inflammatory disorders (P = 0.002), particularly intrahepatic biliary lithiasis (P = 0.035). The NBNC HCC group was older (P = 0.007) and had a greater prevalence of dyslipidemia (P = 0.032), obesity (P = 0.001), cirrhosis (P = 0.019), and AFP levels (P = 0.005). There was an increase in diabetes and hypertension, but it was not statistically significant in the NBNC-HCC. There were no significant differences between the two groups in terms of AST, ALT, total bilirubin, albumin levels, history of chronic alcohol use, tumor number, tumor diameter, or tumor differentiation status.
 |
Table 2 Comparison of the Clinical Features of NBNC PLC Among ICC and HCC Groups |
Discussion
In this study, we investigated 86 biopsy-proven NBNC PLC patients. Our findings revealed that the majority of NBNC PLC patients were ICC, with just a few percent being HCC. Almost half of ICC patients suffer from biliary inflammatory disorders, whereas the majority of NBNC HCC patients have a metabolic risk factor.
In our cohort, only a small percentage of NBNC-PLC were HCC, which was lower than those described in the literature,12 which might be attributed to the fact that patients with occult HBV infection were excluded from our study, and the majority of the NBNC-HCC patients had positive anti-HBc findings.12 As a risk factor for HCC, the obese population is rapidly increasing as a result of dietary changes.13 Over the past three decades, the proportion of people with diabetes has also increased. It is plausible that the fast-increasing incidence of HCC patients with non-viral etiologies is mostly related to the rapidly growing obese population. However, due to the small number of NBNC HCC cases, the relationship between excessive drinking and HCC cannot be proven. It is worth noting that two-thirds of NBNC HCC patients had no evidence of cirrhosis, based on histological and radiological results. Kim et al revealed the lack of cirrhosis in 33% of NBNC HCC patients, which is consistent with our findings. Several investigations have also demonstrated that fibrosis and cirrhosis are not always required for the development of HCC, particularly for NAFLD-related HCC.14–16
Our findings revealed that the majority of NBNC PLC patients had ICC, which is more common in individuals with biliary inflammatory disorders, particularly intrahepatic biliary lithiasis. Intrahepatic biliary lithiasis (or hepatolithiasis) has been linked to an increased incidence of ICC, particularly among East Asian populations.17 However, the risk of ICC for cholelithiasis and choledocholithiasis is more debatable. The varying definition of cholelithiasis in the literature leads to uncertainty as to the true risk of ICC. A recent meta-analysis found a robust link between these conditions and ICC, with a pooled odds ratio (OR) of 18.58 (95% confidence interval [CI] 11.07–31.18) for CCA and 2.11 (95% CI 1.64–2.73) for choledocholithiasis and cholelithiasis, respectively.18 This was in concordance with our results.
Our findings also showed that two-thirds of the NBNC ICC were female. Sex hormones have been implicated in the development of cholangiocarcinogenesis. Jackson et al revealed an increased risk of gall bladder disease (GBD) related with the utilization of orally-administered combination menopausal hormone treatment.19 Due to the elevated CA199 levels observed in ICC, CA19-9 is a suggested biomarker for the early identification and diagnosis of ICC. Utada et al discovered that the prevalence of CA19-9 (>37 U/mL) was 54.1% among Japanese patients diagnosed with ICC.20 CA19-9 exhibits a high level of sensitivity and specificity in detecting cholangiocarcinoma.
There are some limitations to this study. First, the study had a limited sample size because of focusing on biopsy-proven primary liver cancer and excluding patients with occult HBV infection; thus, risk factors for NBNC-HCC and NBNC-ICC may not be accurately represented. Secondly, alcohol-related HCC were relatively fewer since the status of alcohol use was not included in this study. Third, biases resulting from the selection and referral process are potentially important as these investigations were carried out in single centers. Despite some limitations, we are certain that this study provides useful insights into the clinical features of non-B and non-C (NBNC) primary liver cancers and risk factors for ICC and HCC. A large-scale, multicenter investigation is needed to verify our findings.
In conclusion, our study found that the majority of NBNC PLC patients were ICC, and only a small portion were HCC. It is crucial to note that female patients with biliary inflammatory diseases and higher CA199 levels had a higher risk of ICC, and patients with metabolic risk factors and higher AFP levels had an increased tendency to develop HCC. Additional research should be performed to verify this conclusion.
Institutional Review Board Statement
The Second Xiangya Hospital of Central South University Ethics Committee (LYF20240137) had approved this study. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
Data Sharing Statement
The authors can certify that all relevant data is included in the article and make materials available upon request from the corresponding author.
Informed Consent Statement
The requirement of informed consent was waived due to the retrospective nature of the study, the data was anonymized, and the absence of any risk.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no financial or non-financial interests with other people or organizations that could inappropriately influence this work.
References
1. Rahib L, Smith BD, Alizenberg R, et al. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014;74(11):2913–2921. doi:10.1158/0008-5472.CAN-14-0155
2. Ananthakrishnan A, Gogineni V, Saeian K. Epidemiology of primary and secondary liver cancers. Semin Intervent Radiol. 2006;23(1):047–063. doi:10.1055/s-2006-939841
3. de Martel C, Georges D, Bray F, et al. Global burden of cancer attributable to infections in 2018: a worldwide incidence analysis. Lancet Glob Health. 2020;8(2):e180–e190. doi:10.1016/S2214-109X(19)30488-7
4. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
5. Tateishi R, Matsumura T, Okanoue T, et al. Hepatocellular carcinoma development in diabetic patients: a nationwide survey in Japan. J Gastroenterol. 2021;56(3):261–273. doi:10.1007/s00535-020-01754-z
6. Calle EE, Rodriguez C, Walker-Thurmond K, et al. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of US adults. N Engl J Med. 2003;348(17):1625–1638. doi:10.1056/NEJMoa021423
7. El-Serag HB, Tran T, Everhart JE. Diabetes increases the risk of chronic liver disease and hepatocellular carcinoma. Gastroenterology. 2004;126(2):460–468. doi:10.1053/j.gastro.2003.10.065
8. Wang Z, Sheng -Y-Y, Dong Q-Z, et al. Hepatitis B virus and hepatitis C virus play different prognostic roles in intrahepatic cholangiocarcinoma: a meta-analysis. World J Gastroenterol. 2016;22(10):3038–3051. doi:10.3748/wjg.v22.i10.3038
9. Jeong S, Luo G, Wang Z-H, et al. Impact of viral hepatitis B status on outcomes of intrahepatic cholangiocarcinoma: a meta-analysis. Hepatol Int. 2018;12(4):330–338. doi:10.1007/s12072-018-9881-y
10. Tao L-Y, X-d H, Xiu D-R. Hepatitis B virus is associated with the clinical features and survival rate of patients with intrahepatic cholangiocarcinoma. Clin Res Hepatol Gastroenterol. 2016;40(6):682–687. doi:10.1016/j.clinre.2016.04.001
11. Wongjarupong N, Assavapongpaiboon B, Susantitaphong P, et al. Non-alcoholic fatty liver disease as a risk factor for cholangiocarcinoma: a systematic review and meta-analysis. BMC Gastroenterol. 2017;17(1):149.
12. Kim J, Kang W, Sinn DH, et al. Potential etiology, prevalence of cirrhosis, and mode of detection among patients with non-B non-C hepatocellular carcinoma in Korea. Korean J Intern Med. 2020;35(1):65–78. doi:10.3904/kjim.2018.040
13. Abu-Saad K, Murad H, Barid R, et al. Development and efficacy of an electronic, culturally adapted lifestyle counseling tool for improving diabetes-related dietary knowledge: randomized controlled trial among ethnic minority adults with type 2 diabetes mellitus. Med Internet Res. 2019;21(10):e13674. doi:10.2196/13674
14. Kwak HW, Park JW, Koh YH, et al. Clinical characteristics of patients with cryptogenic hepatocellular carcinoma in a hepatitis B virus-endemic area. Liver Cancer. 2016;5(1):21–36. doi:10.1159/000367756
15. Noureddin M, Rinella ME. Nonalcoholic fatty liver disease, diabetes, obesity, and hepatocellular carcinoma. Clin Liver Dis. 2015;19(2):361–379. doi:10.1016/j.cld.2015.01.012
16. Marengo A, Rosso C, Bugianesi E. Liver cancer: connections with obesity fatty liver, and cirrhosis. Annu Rev Med. 2016;67(1):103–117. doi:10.1146/annurev-med-090514-013832
17. Kim HJ, Kim JS, Joo MK, et al. Hepatolithiasis and intrahepatic cholangiocarcinoma: a review. World J Gastroenterol. 2015;21(48):13418–13431. doi:10.3748/wjg.v21.i48.13418
18. Clements O, Eliahoo J, Kim JU, et al. Risk factors for intrahepatic and extrahepatic cholangiocarcinoma: a systematic review and meta-analysis. J Hepatol. 2020;72(1):95–103. doi:10.1016/j.jhep.2019.09.007
19. Jackson SS, Pfeiffer RM, Gabbi C, et al. Menopausal hormone therapy and risk of biliary tract cancers. Hepatology. 2022;75(2):309–321. doi:10.1002/hep.32198
20. Utada M, Ohno Y, Tamaki T, et al. Long-term trends in incidence and mortality of intrahepatic and extrahepatic bile duct cancer in Japan. J Epidemiol. 2014;24(3):193–199. doi:10.2188/jea.JE20130122
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.